the effects of stress management on adaptation and
TRANSCRIPT

The Effects of Stress Management on Adaptation
and Biobehavioral Processes in Women Undergoing
Treatment for Non-Metastatic Breast Cancer
Michael H. Antoni, Ph.D.
Department of Psychology
Div of Health Psychology
Director, Center for Psycho-
Oncology
Leader, Biobehavioral Oncology
Research Program, Sylvester
Cancer Center
University of Miami

Acknowledgments NCI
R01 CA64710
NCI R01CA131451
P50CA84944
Sylvester Cancer Center
• Robert Derhagopian, MD
• Frederick L. Moffat, MD
• Tammy Enos Sifre, PhD
• Kristin Kilbourn, PhD
• Susan Alferi Fox, PhD
• Patti Arena, PhD
• Jessica Lehman, PhD
• Amy Boyers, PhD
• Jennifer Culver, PhD
• Susan Yount, PhD
• Suzanne Harris, PhD
• Dean Cruess, PhD.
• Stefan Gluck, MD, Ph.D.
• Bonnie McGregor, PhD
• Alicia Price, PhD
• Vida Petronis, PhD
• Roselyn Smith-Gonas, PhD
• Kurrie Wells, MS
• Cassy Vaughn, MS
• Kenya Urcuyo, MS
• Sophie Guellati, PhD
• Sarah Wimberly, Ph.D.
• Aisha Kazi, Ph.D.
• Kristin Phillips, Ph.D.
• Janny Rodriguez, MEd
• Nicole Whitehead, Ph.D.
• Jarrard Goodwin, M.D.
• Bonnie B. Blomberg, Ph.D., Microbiology/Immunology, University of Miami School of Medicine, Miami
• Suzanne Lechner, Ph.D., Psychiatry, University of Miami School of Medicine, Miami
• Charles S. Carver, Ph.D., Psychology, University of Miami, Coral Gables
• Susan Lutgendorf, PhD, Psychology, University of Iowa, Iowa City, IA
• Steven W. Cole, PhD, Medicine, UCLA, Los Angeles, California
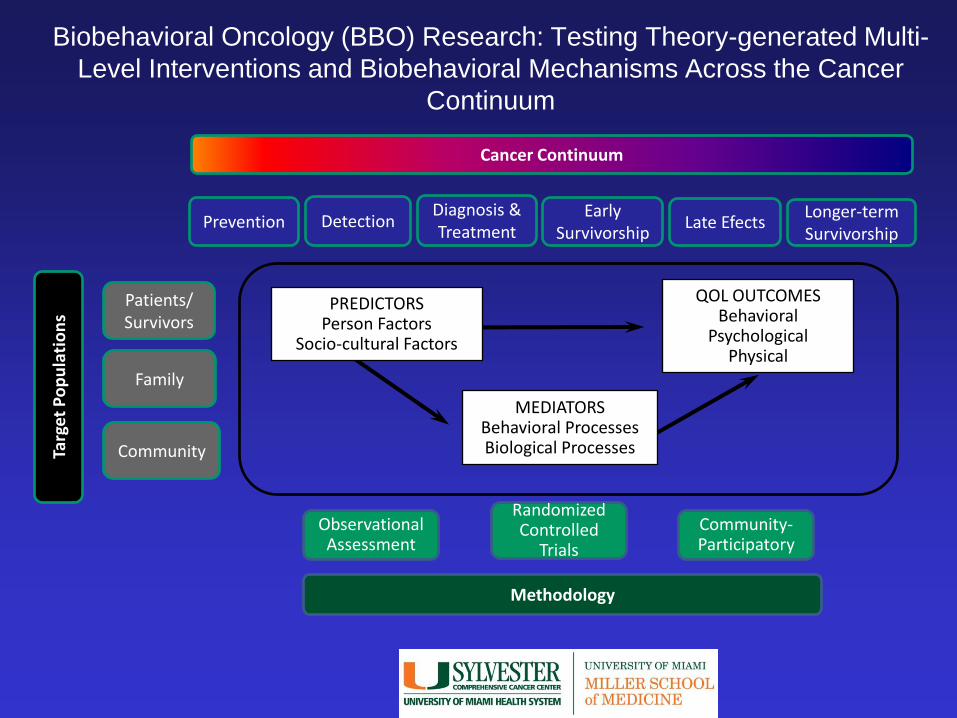
Biobehavioral Oncology (BBO) Research: Testing Theory-generated Multi-
Level Interventions and Biobehavioral Mechanisms Across the Cancer
Continuum
Prevention Detection Diagnosis & Treatment
Early Survivorship
Late Efects Longer-term Survivorship
Cancer Continuum
Targ
et P
op
ula
tio
ns
Patients/ Survivors
Family
Community
Methodology
Observational Assessment
Randomized Controlled
Trials
Community-Participatory
PREDICTORS Person Factors
Socio-cultural Factors
QOL OUTCOMES Behavioral
Psychological Physical
MEDIATORS Behavioral Processes Biological Processes

Family effects across continuum
Cancer detection
Cancer treatment
Persisting symptoms
and late effects
Longer-term Survivorship
Behavioral and psychological interventions for physical, social
and psychological adaptation
Behavioral interventions for symptom mgmt, late effects and optimizing
survivorship
Community Translation of intervention for minority
populations
Cancer prevention
Early survivor-
ship
Behavioral Intervention for risk reduction & screening behavior
Biobehavioral Intervention Research Goals: Behaviorally Intervening Across
the Cancer Continuum

Cognitive Behavioral Stress Management and
Breast Cancer Research at UM (1992-2013)
Post-
Adj
Stage I-IIla
BRCA
Pre-
Adj
Stage I-II
Stage I-IIIa
Dismantle
CBSM
Abbrev
CBSM
E.g., Stress Management for
Women with Breast Cancer
• Rationale
– Breast Cancer (BCa) is a stressor
– Challenges of surgery and adjuvant tx
– Patient assets can facilitate adjustment
– CBSM can fortify these assets in
women with BCa
– Improving Psychosocial Adaptation
may Affect Physiological Adaptation
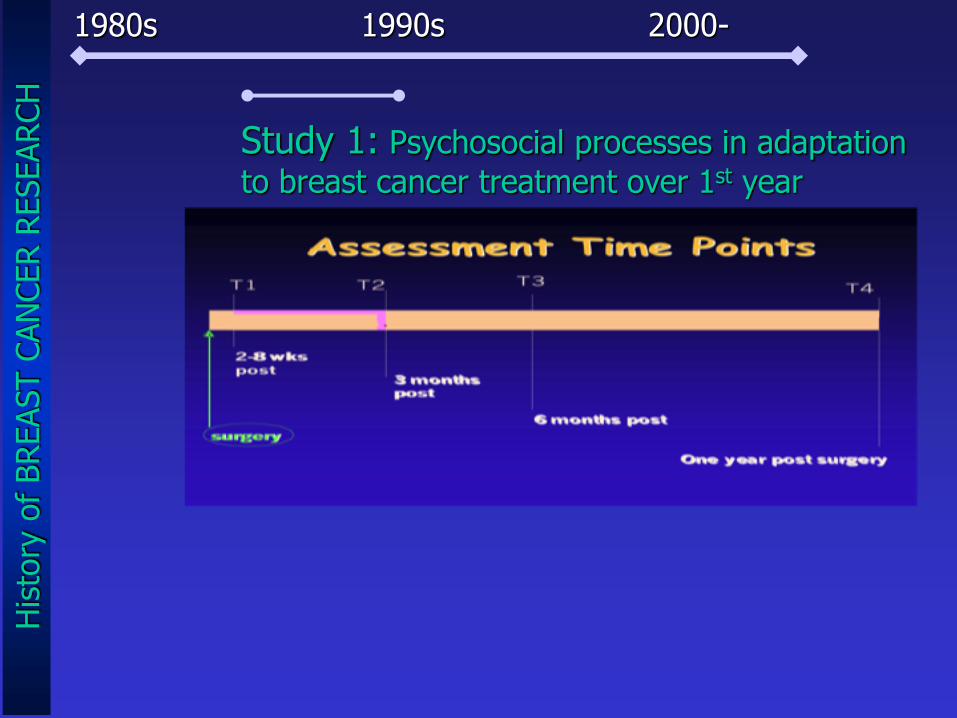
1980s 1990s 2000-
Study 1: Psychosocial processes in adaptation
to breast cancer treatment over 1st year
His
tory
of
BREAST C
AN
CER R
ESEARCH

Why Stress Management for
Women with BRCA?
• What are the challenges?
– Life goals are threatened
– Self-image is questioned
– Physical side-effects of adjuvant tx compromise QOL
Spencer et al. (1998) Health Psychology

Stress Management for
Women with BRCA
• What are the challenges?
– Life goals are threatened
– Self-image is questioned
– Physical side-effects of adjuvant tx compromise QOL
• What characteristics relate to better/worse
adjustment after treatment?

Pre-surgical Accept & optimism
Post-surgical distress
3-mo. denial & disengagement
6-mo. distress
–
+
+

Social Support and
Distress
• Greater social support pre and post-surgery predicts less distress in months after
• Spousal support just after surgery is important
• But support from other women is also important in the months that follow
(Alferi et al., 2001; Petronis et al., 2002)
Stress Management for Women with BCa
QUESTIONS AND OBSERVATIONS
• What are the challenges of BCa? – Life goals are threatened
– Self-image is questioned
– Physical side-effects of adjuvant tx compromise QOL
• What characteristics relate to better/worse
Adaptation and Health outcomes after treatment? – Optimism
– Adaptive coping
– Social support
• Can these assets be built by intervention?
• Cognitive Behavioral Stress Management (CBSM)
CHALLENGES: Petronis et al., 2002; Spencer et al., 1999. ADAPTATION: Alferi et al., 2001; Carver et al., 1993; Stanton et al., 1993 HEALTH: Levy et al., 1991; Watson et al., 1999; Fawzy et al., 1993; Cutrona et al.; Lutgendorf & Antoni, 2007
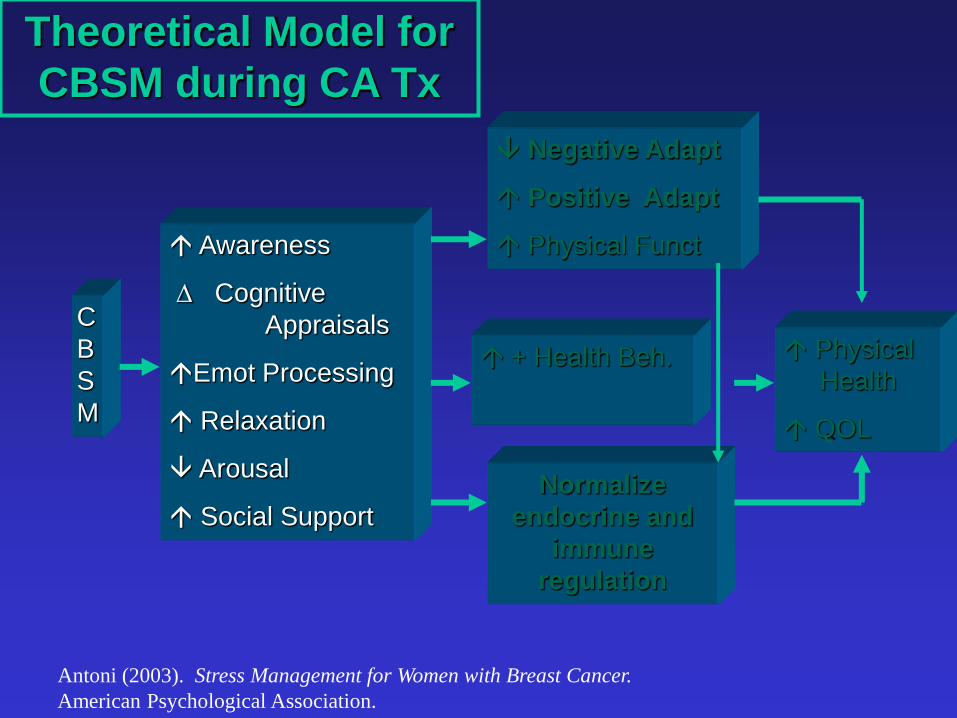
C
B
S
M
Awareness
Cognitive
Appraisals
Emot Processing
Relaxation
Arousal
Social Support
Physical
Health
QOL
Normalize
endocrine and
immune
regulation
+ Health Beh.
Negative Adapt
Positive Adapt
Physical Funct
Theoretical Model for
CBSM during CA Tx
Antoni (2003). Stress Management for Women with Breast Cancer.
American Psychological Association.

CBSM: Aims, strategies,
techniques Aims Strategies Techniques
Increase awareness of
stress response
Provider information (i.e.,
stress response); provide
in-session experiences
Didactic and written
information, self-monitoring
exercises
Teach anxiety
reduction skills
Provide relaxation training PMR, guided imagery,
autogenics, deep breathing
exercises
Modify cognitive
appraisals
Teach CBSM techniques Cognitive restructuring,
rational thought replacement
Build coping skills and
increase emotional
expressiveness
Provide cognitive,
behavioral, and
interpersonal skills training;
facilitate disclosures
Coping skills training,
assertion training, anger
management
Reduce social isolation Build social support
network
Group support, raising
awareness of social network
Antoni (2003). Stress Management for Women with Breast Cancer.
American Psychological Association.


CBSM Intervention:
Relaxation Component
• Progressive muscle relaxation
• Guided imagery
• Autogenic training
• Meditation
• Breathing exercises

Components of CBSM: CBT
• AWARENESS
– Physical
– Emotional
– Cognitive
– Social
• COPING RESPONSES
– Coping repertoire
• (direct, indirect)
– Coping Appraisals
– Coping execution
steps
• APPRAISALS
– Automatic thoughts
– Refuting and replacing
– P-E transactions
• USE OF COPING RESOURCES
– Social support sources
– Social support seeking
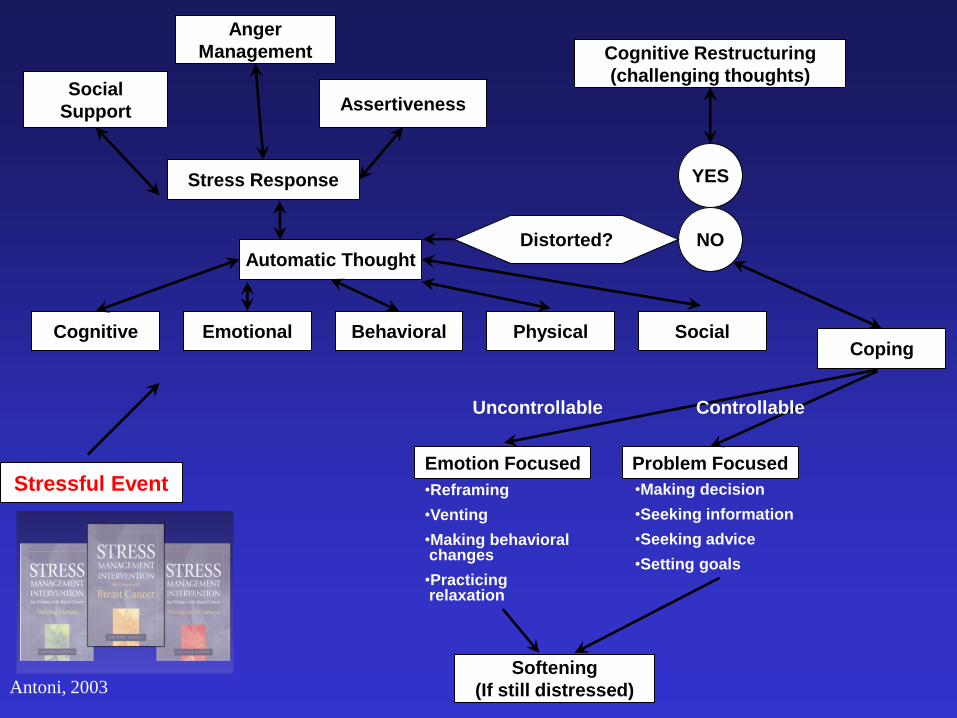
Anger
Management
Social
Support Assertiveness
Stress Response
Cognitive Restructuring
(challenging thoughts)
YES
NO Automatic Thought
Cognitive
Emotion Focused
Softening
(If still distressed)
Coping Social Physical Behavioral Emotional
Distorted?
Problem Focused
Uncontrollable Controllable
•Reframing
•Venting
•Making behavioral changes
•Practicing relaxation
•Making decision
•Seeking information
•Seeking advice
•Setting goals
Stressful Event
Antoni, 2003
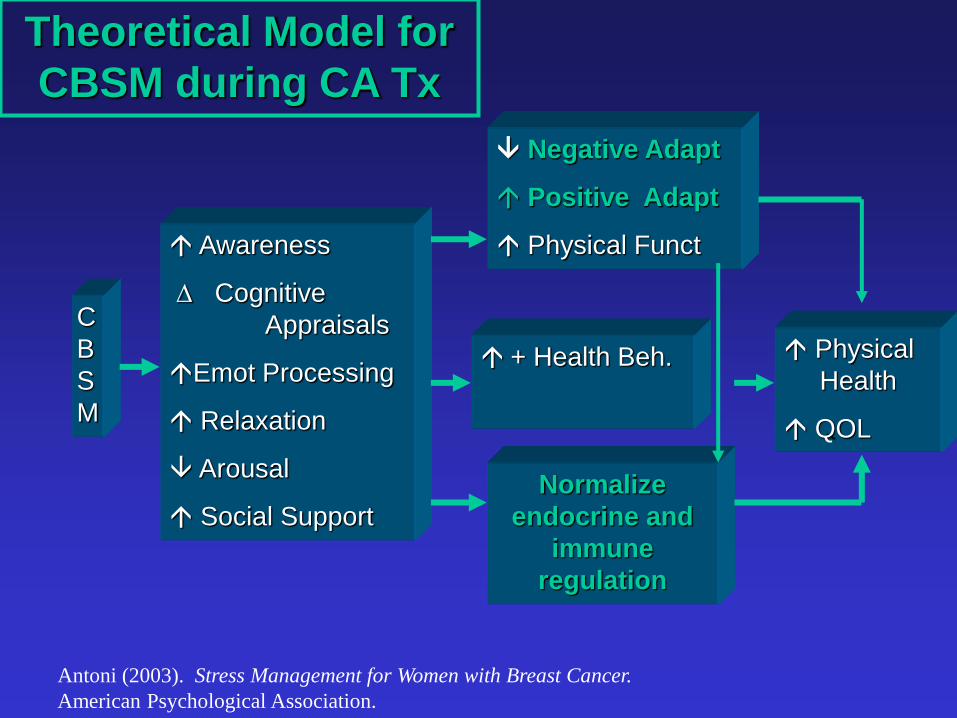
C
B
S
M
Awareness
Cognitive
Appraisals
Emot Processing
Relaxation
Arousal
Social Support
Physical
Health
QOL
Normalize
endocrine and
immune
regulation
+ Health Beh.
Negative Adapt
Positive Adapt
Physical Funct
Theoretical Model for
CBSM during CA Tx
Antoni (2003). Stress Management for Women with Breast Cancer.
American Psychological Association.

Assessment Time Points
T1
surgery
T4
One year post surgery
T3 T2
2-8 wks
post
B SMART-10 wks.
3 months
post
6 months post

Week Relaxation Stress Management
1 PMR 7 Stress & Awareness
2 PMR 4/D.B. Stress & Awareness/Stress Appraisals
3 D.B./PMR Disease-Specific, Automatic Thoughts
4 Autogenics Auto. Thghts, Distortions, Thght Rep.
5 D.B./Visualiz. Cognitive Restructuring
6 Sunlight Med. Effective Coping I
7 Color Meditation Effective Coping II
8 Meditation Social Support
9 Mindfulness Anger Management
10 Part. Choice Assertion Training & Program Review
Topics of CBSM
(Antoni et al., 2003, 2007; Penedo et al., 2008)
Control Condition
• Std Care Plus Half-day Psychoeducational Seminar
– Groups of 4 – 6 women
– Health Educational on BCa
– Outlined Stress Management Techniques
– Akin to Self-Help Seminar

403 screened for eligibility
204 excluded
55 ineligible
149 declined participation
or failed to appear for T1
199 randomized
107 assigned to control
92 assigned to intervention
85 assessed at T2 (6 mo) 74 assessed at T2 (6 mo)
83 assessed at T3 (12 mo)
74 assessed at T3 (12 mo)
Second NCI Trial: CONSORT DIAGRAM
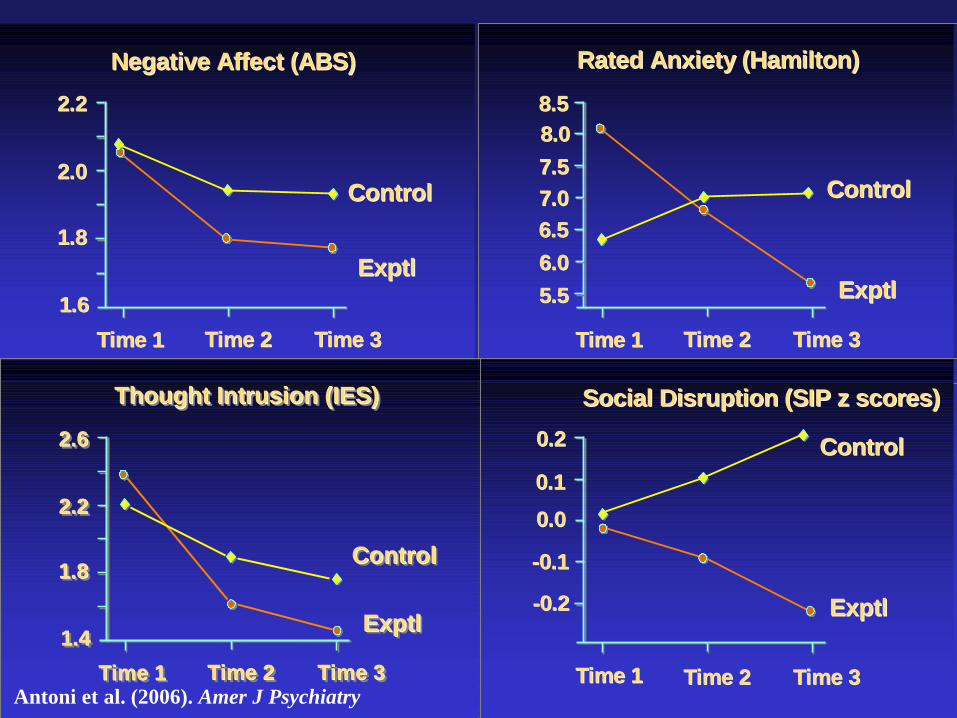
Negative Affect (ABS)Negative Affect (ABS)
ControlControl
ExptlExptl
2.22.2
2.02.0
1.81.8
1.61.6
Time 1Time 1 Time 2Time 2 Time 3Time 3
Rated Anxiety (Hamilton)Rated Anxiety (Hamilton)
ControlControl
ExptlExptl
8.58.5
8.08.0
7.57.5
6.56.5
Time 1Time 1 Time 2Time 2 Time 3Time 3
7.07.0
6.06.0
5.55.5
Social Disruption (SIP z scores)Social Disruption (SIP z scores)
ControlControl
ExptlExptl
0.20.2
0.00.0
--0.10.1
Time 1Time 1 Time 2Time 2 Time 3Time 3
0.10.1
--0.20.2
Thought Intrusion (IES)Thought Intrusion (IES)Thought Intrusion (IES)
ControlControlControl
ExptlExptlExptl
2.62.62.6
2.22.22.2
1.81.81.8
1.41.41.4
Time 1Time 1Time 1 Time 2Time 2Time 2 Time 3Time 3Time 3 Antoni et al. (2006). Amer J Psychiatry

CBSM Reduced
Sleep and Fatigue-
related Disruption
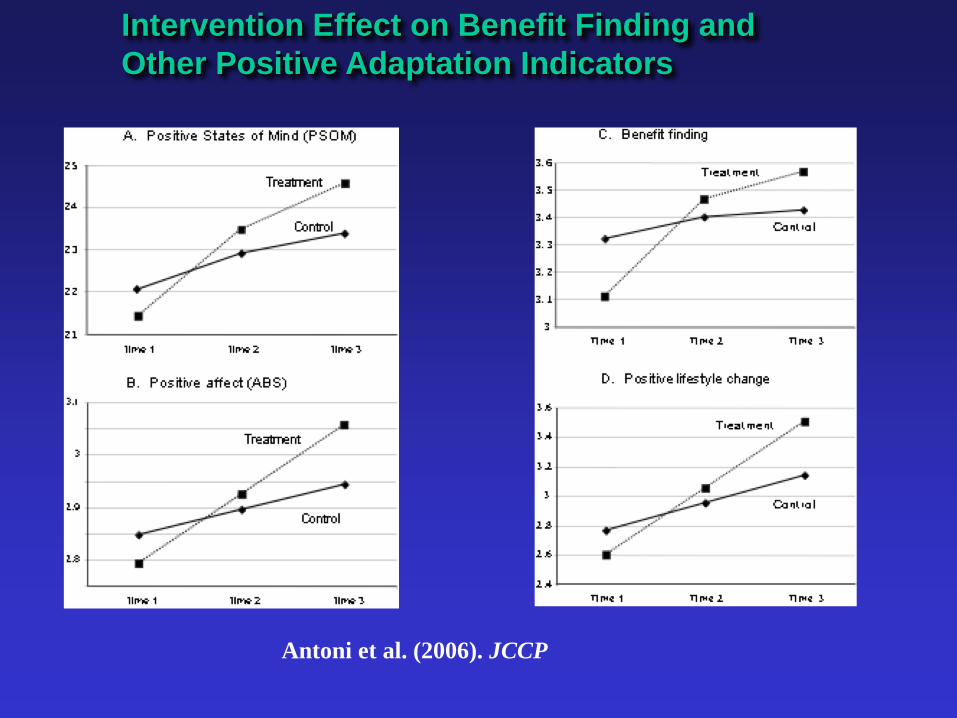
Antoni et al. (2006). JCCP
Intervention Effect on Benefit Finding and
Other Positive Adaptation Indicators

How Did CBSM Work?
• Which elements of CBSM were accounting for these effects?
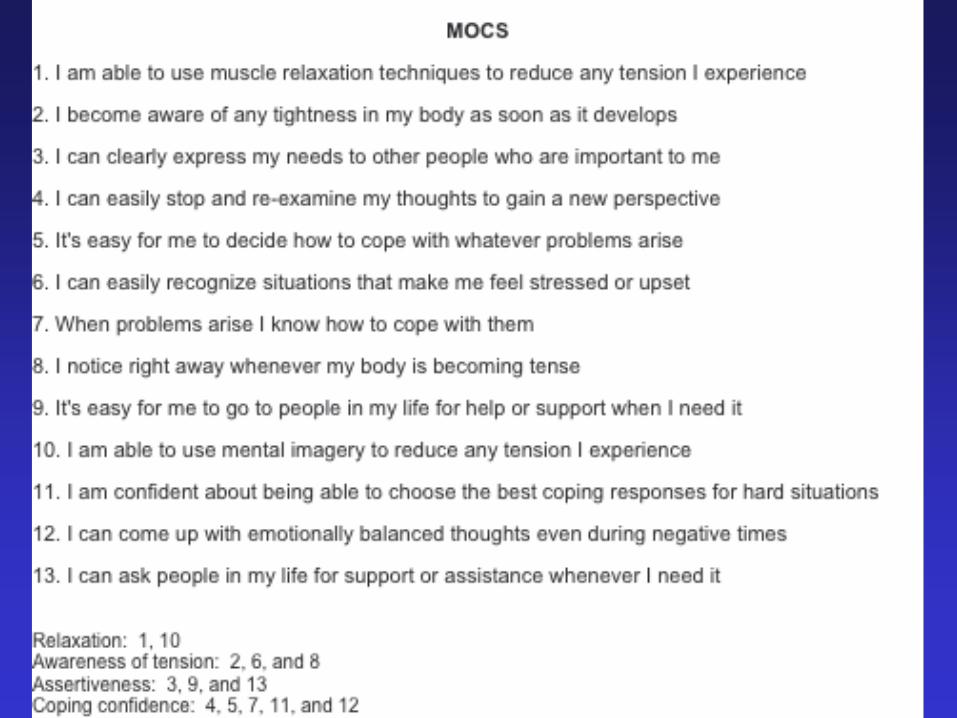
• Measure of Current Status (MOCS, Carver 2004)
– Separate scales for different perceived SM skills
• Relaxation and imagery skills
• Coping and CBT skills
• Ability to use cog restructuring skills
• Ability to act assertively and express needs
– Scales for non-specific effects of group tx
• Cognitive-Affective Processing:
– Emotion Approach Coping (EAC, Stanton 1998)
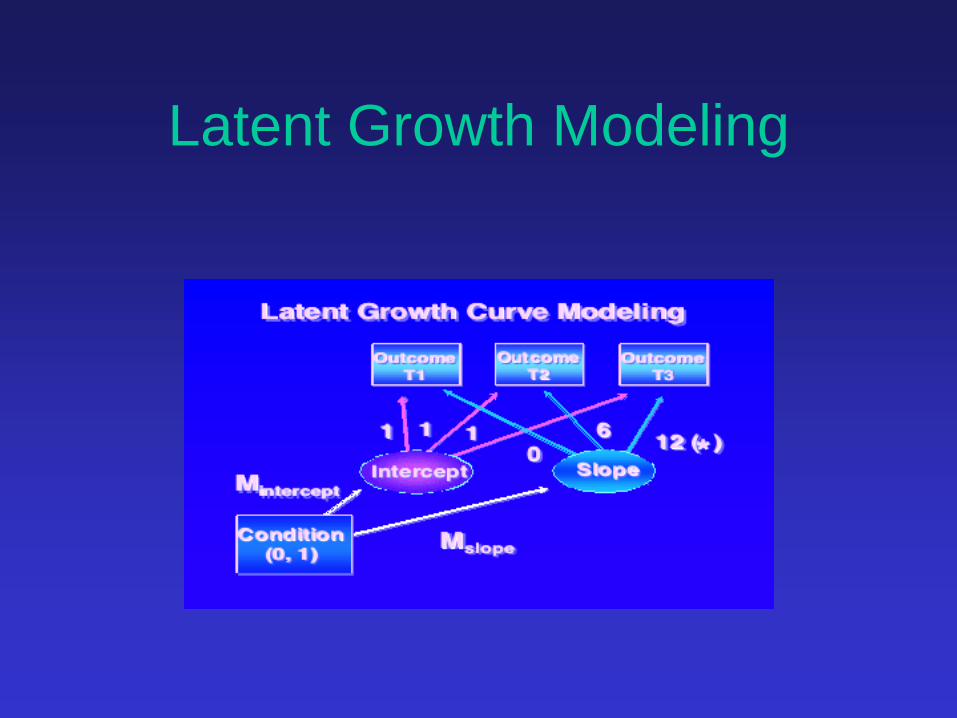
Latent Growth Modeling

How Did CBSM Work?
• Which elements of CBSM were accounting for these effects?
• Measure of Current Status (MOCS, Carver 2004)
– Separate scales for different perceived SM skills
• Relaxation and imagery skills ( p < .01)
• Coping and CBT skills (p < .05)
• Ability to use cog restructuring skills (p < .05)
• Ability to act assertively and express needs (NS)
– Scales for non-specific effects of group tx (NS)
• Emotion Approach Coping (EAC, Stanton 1998) (p < .01)
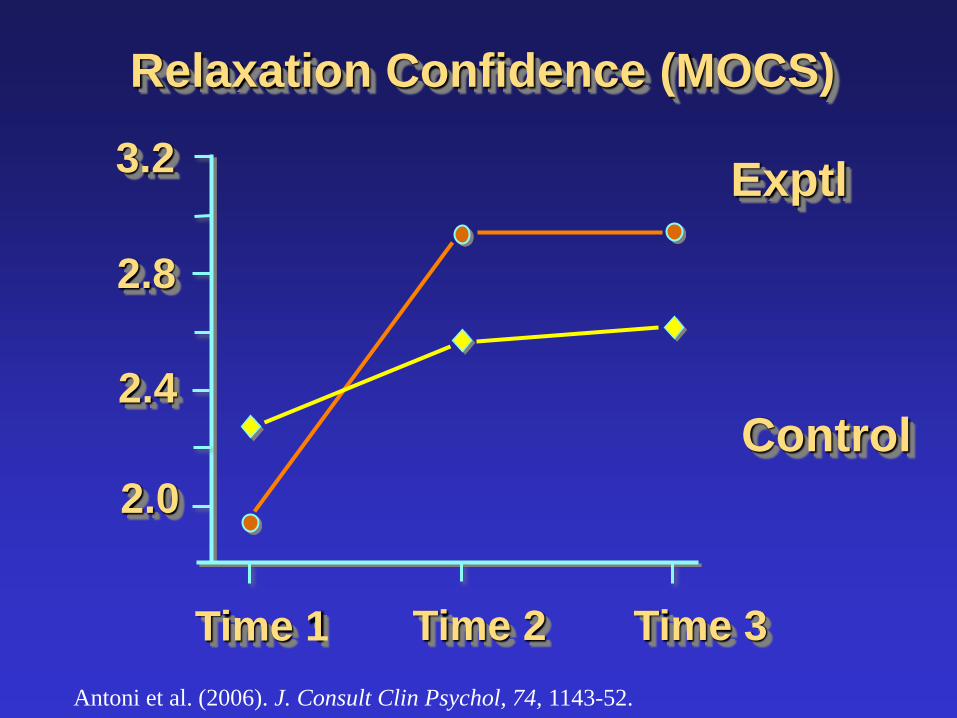
Relaxation Confidence (MOCS)
Control
Exptl 3.2
2.8
2.4
2.0
Time 1 Time 2 Time 3
Antoni et al. (2006). J. Consult Clin Psychol, 74, 1143-52.

CBSM Effects on Emotional
Processing
As s es s m en t Tim e Po in t
4321
Mea
n E
mot
iona
l E
xpre
ssio
n S
core
. 3
. 2
. 1
- . 0
- . 1
- . 2
- . 3
condit ion
co nt r o l
ex pt l

CBSM Effects on slope (z) with mediation by MOCS Relax
(MOCS-R) and Emotional Processing (EAC)
Effect of CBSM w/o Relax w/o Relax & Emot Processing
Positive Adaptation Positive States of Mind (PSOM) 3.17* -0.57 -0.27
ABS Positive Emotions 2.19* -0.82 -0.01
Benefit Finding (17 item) 3.31* -0.61 -0.20
Positive Lifestyle Change 2.64* -0.28 0.20
FACT Emotional Wellbeing 2.96* -0.37 0.32
Negative Adaptation Interviewer-rated Anxiety -2.71* 0.28 -0.23
Interviewer-rated Depression -2.48* 0.46 0.15
IES Intrusive Thoughts -3.64* -1.19 0.04
ABS Emotional Distress -2.48* 0.63 0.13
ABS Depression -2.55* 0.33 0.58
Disrupt. Recreation & Pastimes -2.86* -0.29 -0.45
Disrupt. Social Interaction -2.52* 1.01 -0.48

Up to this point we learned……
• CBSM had beneficial effects on negative and positive adaptation
• Appears to work by instilling confidence in using relaxation skills and facilitating emotional processing
• Supports the CBSM skills + cog/aff processing as important
• But did CBSM affect physiological adaptation?

1980s 1990s 2000s
Study 1: Psychosocial processes in adaptation
to breast cancer treatment
His
tory
of
BREAST C
AN
CER R
ESEARCH
Study 2: CBSM Effects on Psy Adaptation to
Breast cancer treatment: Main Effects and Mediators
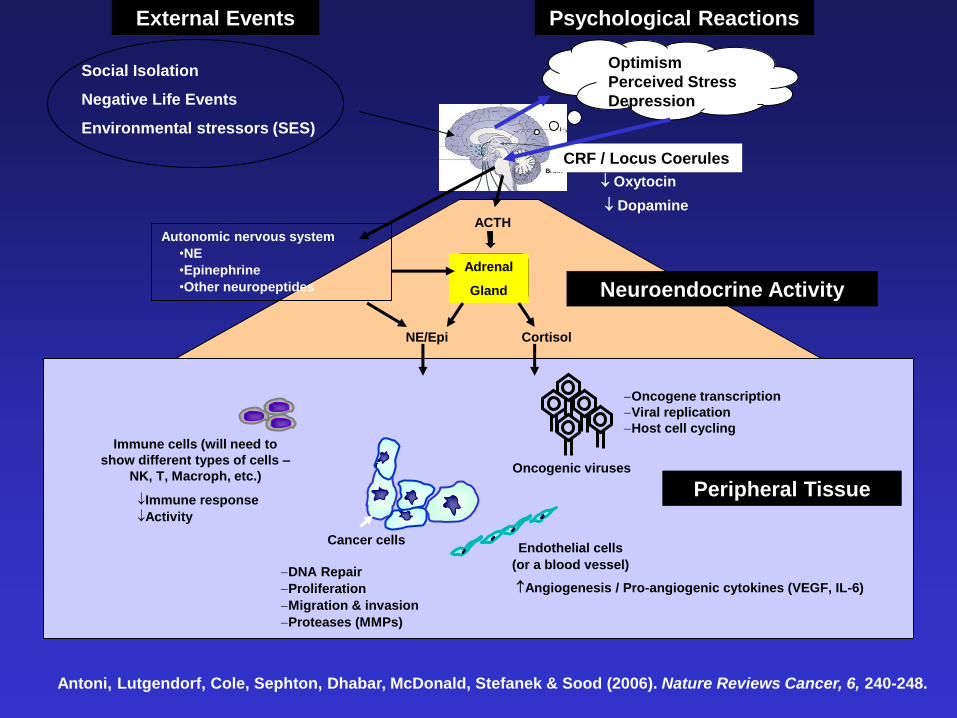
Study 3: CBSM Effects on Psy and Physiol
Adaptation to breast cancer treatment
•Cortisol reduction
•Increased cellular immune function
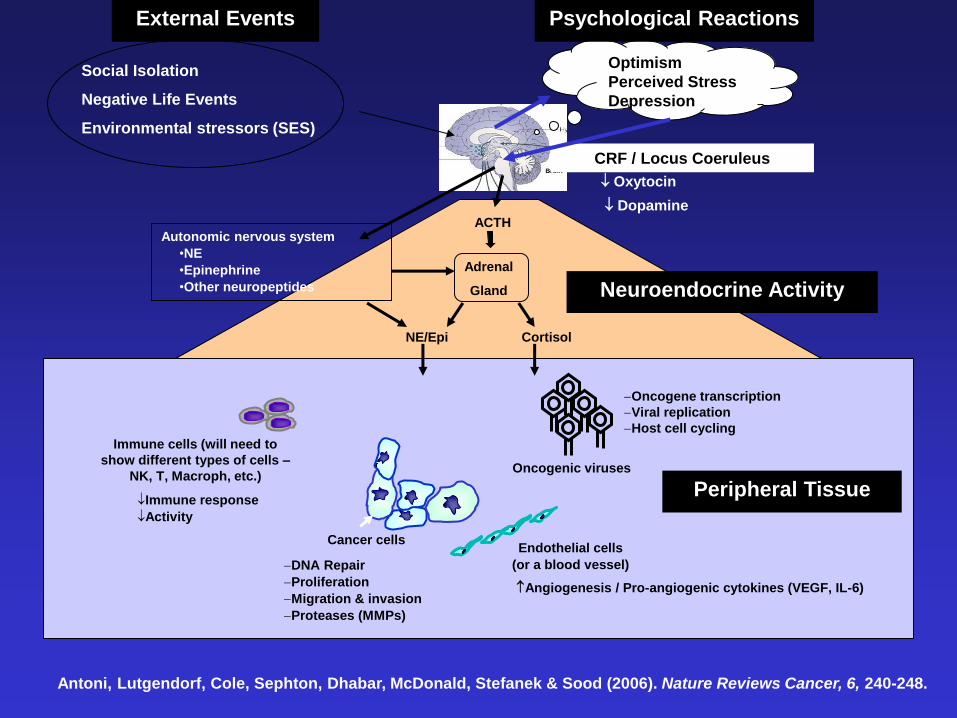
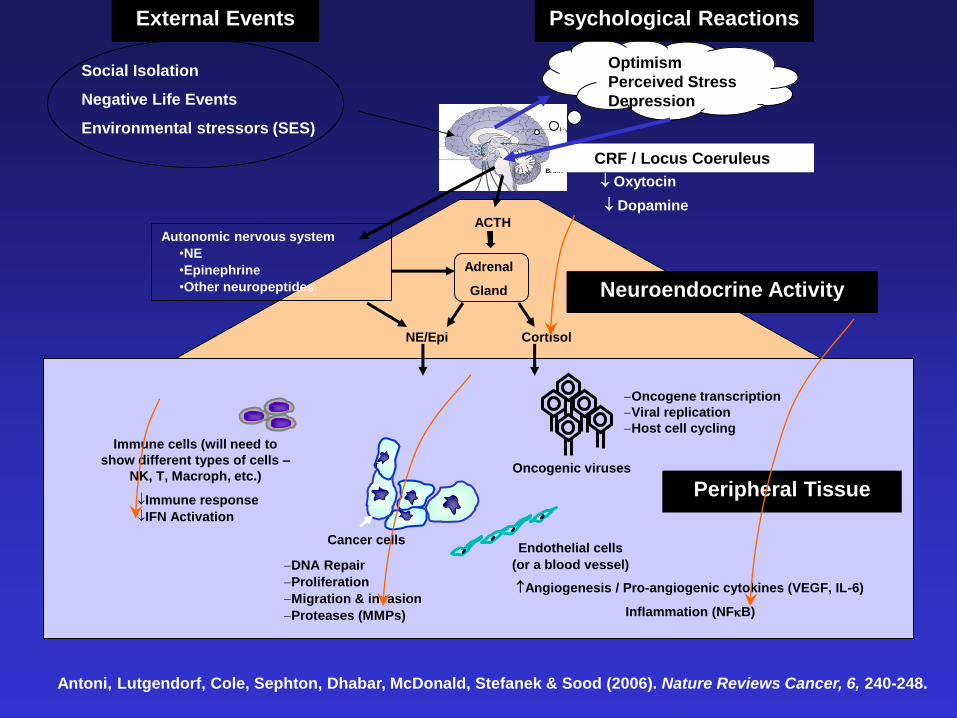
Autonomic nervous system
•NE
•Epinephrine
•Other neuropeptides
Adrenal
Gland
DNA Repair
Proliferation
Migration & invasion
Proteases (MMPs)
Angiogenesis / Pro-angiogenic cytokines (VEGF, IL-6)
ACTH
Cortisol NE/Epi
CRF / Locus Coeruleus
Cancer cells
Immune cells (will need to
show different types of cells –
NK, T, Macroph, etc.)
Dopamine
Endothelial cells
(or a blood vessel)
Oxytocin
Oncogenic viruses
Oncogene transcription
Viral replication
Host cell cycling
Immune response
Activity
Optimism
Perceived Stress
Depression
Social Isolation
Negative Life Events
Environmental stressors (SES)
External Events Psychological Reactions
Neuroendocrine Activity
Peripheral Tissue
Antoni, Lutgendorf, Cole, Sephton, Dhabar, McDonald, Stefanek & Sood (2006). Nature Reviews Cancer, 6, 240-248.
Autonomic nervous system
•NE
•Epinephrine
•Other neuropeptides
Adrenal
Gland
DNA Repair
Proliferation
Migration & invasion
Proteases (MMPs)
Angiogenesis / Pro-angiogenic cytokines (VEGF, IL-6)
ACTH
Cortisol NE/Epi
CRF / Locus Coerules
Cancer cells
Immune cells (will need to
show different types of cells –
NK, T, Macroph, etc.)
Dopamine
Endothelial cells
(or a blood vessel)
Oxytocin
Oncogenic viruses
Oncogene transcription
Viral replication
Host cell cycling
Immune response
Activity
Optimism
Perceived Stress
Depression
Social Isolation
Negative Life Events
Environmental stressors (SES)
External Events Psychological Reactions
Neuroendocrine Activity
Peripheral Tissue
Antoni, Lutgendorf, Cole, Sephton, Dhabar, McDonald, Stefanek & Sood (2006). Nature Reviews Cancer, 6, 240-248.

Elements of CBSM and Putative
Effects on Physiology • Relaxation
– PMR, Imagery, Mindfulness, Breathing
– Decreases tension and anxiety and SNS activation
– SNS-immune communications: NE is ligand for immune cells b-adrenoreceptors down-reg of cellular immune function
• Cognitive Restructuring and Coping Effectiveness Training
– Raise awareness of stress cues
– Change negative/inaccurate stressor appraisals
– Increase pos reframing and acceptance coping
– CBT decreases depression and anxiety which also relate to immune function via HPA and cortisol dysregulation
• Interpersonal Skills Training/Supportive Group
– Assertiveness and anger mgmt to attract /maintain social support
– Group format models seeking and receiving support
– Social support may buffer stress effects on neuroimmune processes

Surgery
T1 T2 T3
CBSM starts
3 mo 9 mo
Adjuvant
therapy
starts
CBSM ends
T4 15 mo
2-8 w.
•Blood*
•Psychological
assessment
•Blood*
•Psychological
assessment
•Blood*
•Psychological
assessment
•Blood*
•Psychological
assessment
3 mo
0
Detailed Design: Blood Draws
Adjuvant
therapy
ends
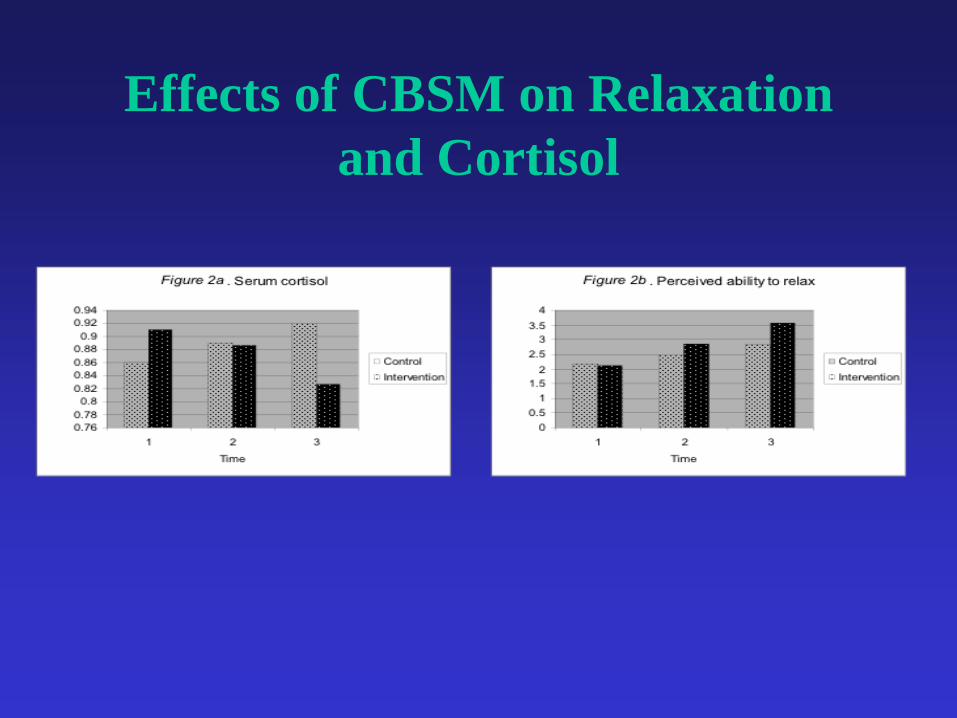
Effects of CBSM on Relaxation
and Cortisol
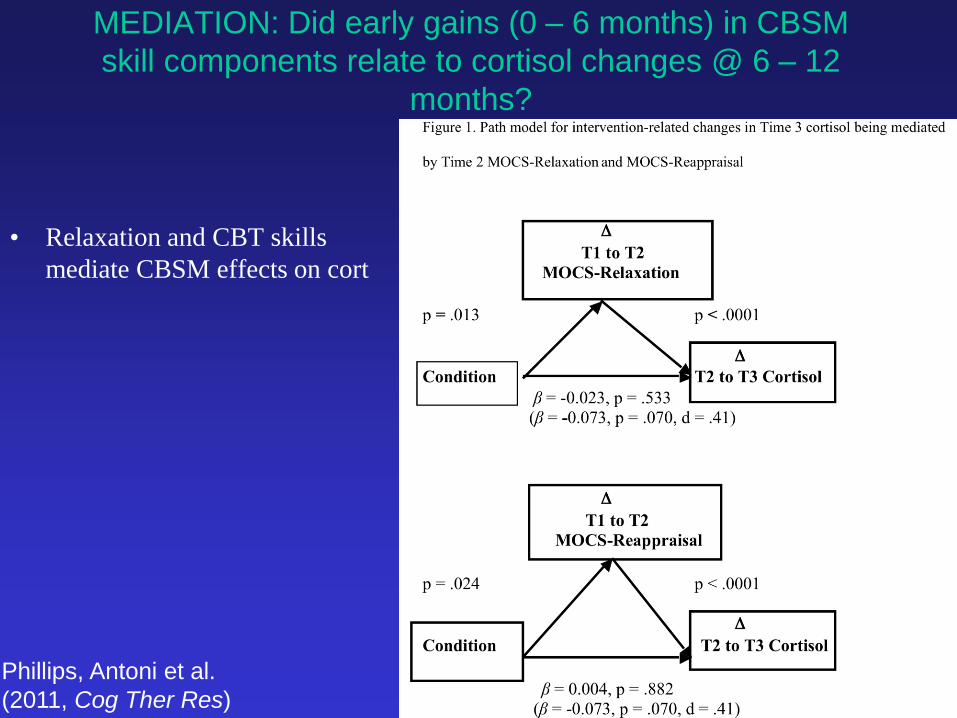
MEDIATION: Did early gains (0 – 6 months) in CBSM
skill components relate to cortisol changes @ 6 – 12
months?
• Relaxation and CBT skills
mediate CBSM effects on cort
Phillips, Antoni et al.
(2011, Cog Ther Res)

Does CBSM also affect cellular
immunity in Women with
BCa? •Prior work had shown Psy Intervention effects on
lymphocyte proliferation in women with BCa
•Other work showed effects of Psy Intervention on NKCC in
patients with MM
•Patients with lower T lymphocyte counts and T-cell
responsivity to mitogen prior to surgery higher risk for
recurrent disease
(Andersen et al., 2004 Fawzy et al., 1990)

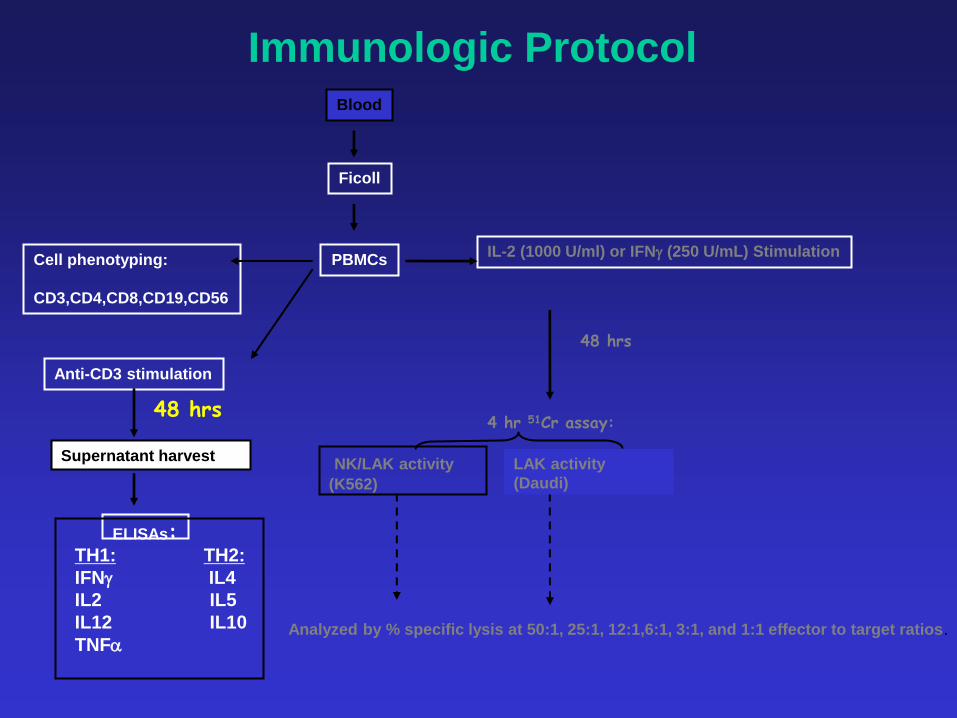
Immunologic Protocol Blood
5 – 6pm
PBMCs
Ficoll
Anti-CD3 stimulation
IL-2 (1000 U/ml) or IFNg (250 U/mL) Stimulation Cell phenotyping:
CD3,CD4,CD8,CD19,CD56
48 hrs
48 hrs 4 hr 51Cr assay:
LPR-tritiated thymidine
TH1: TH2:
IFNg IL4
IL2 IL5
IL12 IL10
TNFa
ELISAs:
NK/LAK activity
(K562)
Analyzed by % specific lysis at 50:1, 25:1, 12:1,6:1, 3:1, and 1:1 effector to target ratios.
LAK activity
(Daudi)

-4000
-2000
0
2000
4000
6000
8000
Comparison
Group
CBSM
Group
Pro
lifera
tion (
CP
M)
P < .05
Change in Lymphocyte Proliferative
Response 3 Months Post-CBSM
McGregor et al. (2004) J. Psychosomatic Res, 56, 1 – 8
Change in Proliferation T1-T3
6000040000200000-20000-40000
Ch
an
ge
in B
en
efit
Fin
din
g T
1-T
2
2.5
2.0
1.5
1.0
.5
0.0
-.5
-1.0
-1.5
CBSM
Control
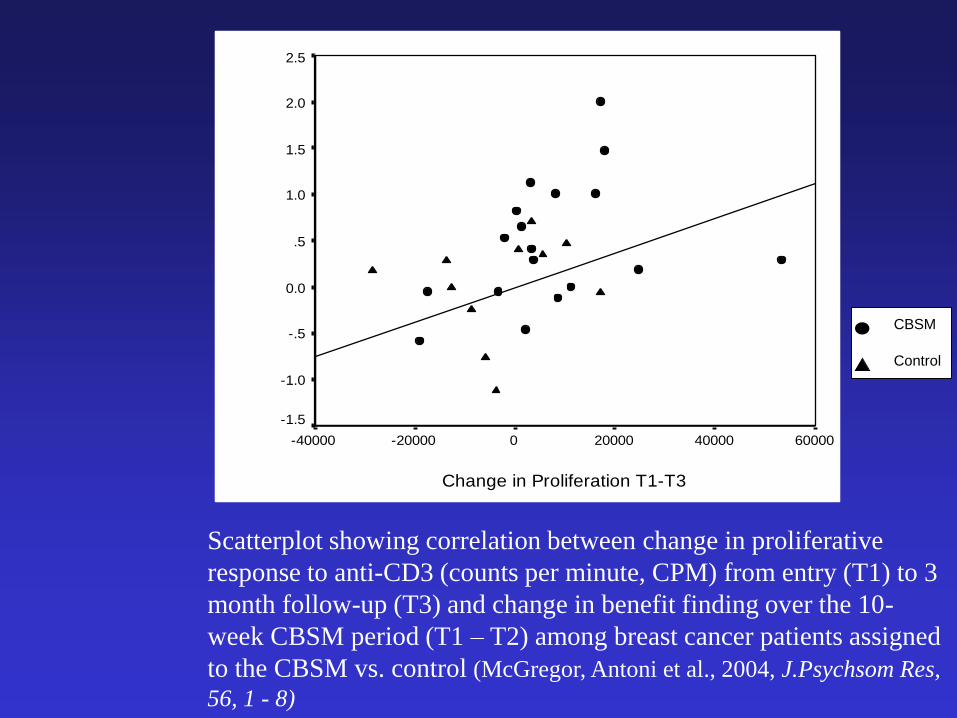
Scatterplot showing correlation between change in proliferative
response to anti-CD3 (counts per minute, CPM) from entry (T1) to 3
month follow-up (T3) and change in benefit finding over the 10-
week CBSM period (T1 – T2) among breast cancer patients assigned
to the CBSM vs. control (McGregor, Antoni et al., 2004, J.Psychsom Res,
56, 1 - 8)
Immunologic Protocol Blood
PBMCs
Ficoll
Anti-CD3 stimulation
IL-2 (1000 U/ml) or IFNg (250 U/mL) Stimulation Cell phenotyping:
CD3,CD4,CD8,CD19,CD56
48 hrs
48 hrs 4 hr 51Cr assay:
Supernatant harvest
TH1: TH2:
IFNg IL4
IL2 IL5
IL12 IL10
TNFa
ELISAs:
NK/LAK activity
(K562)
Analyzed by % specific lysis at 50:1, 25:1, 12:1,6:1, 3:1, and 1:1 effector to target ratios.
LAK activity
(Daudi)
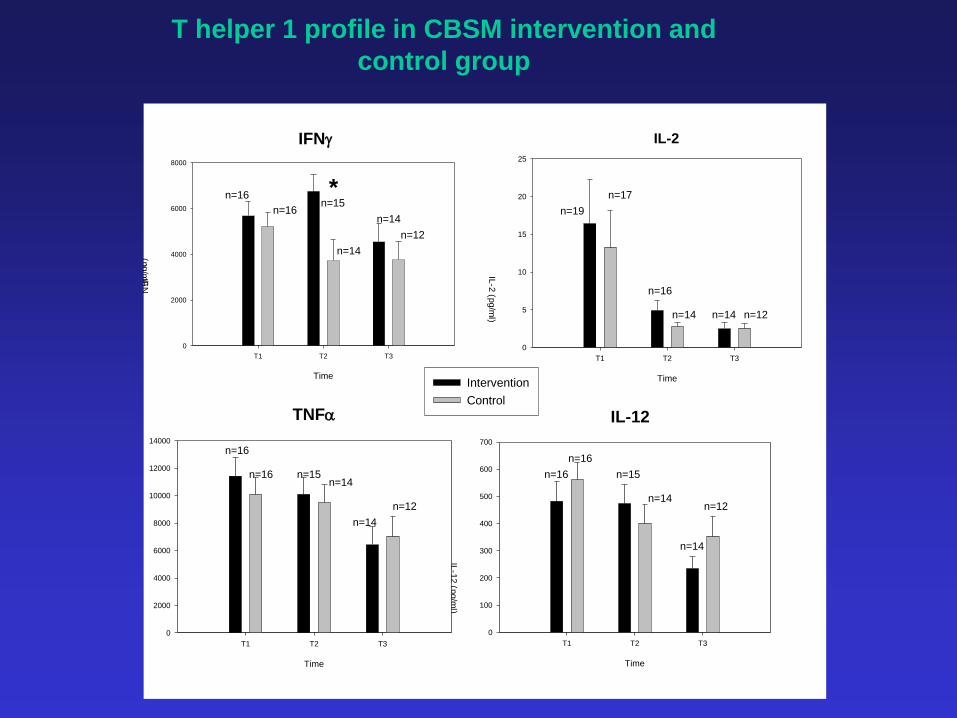
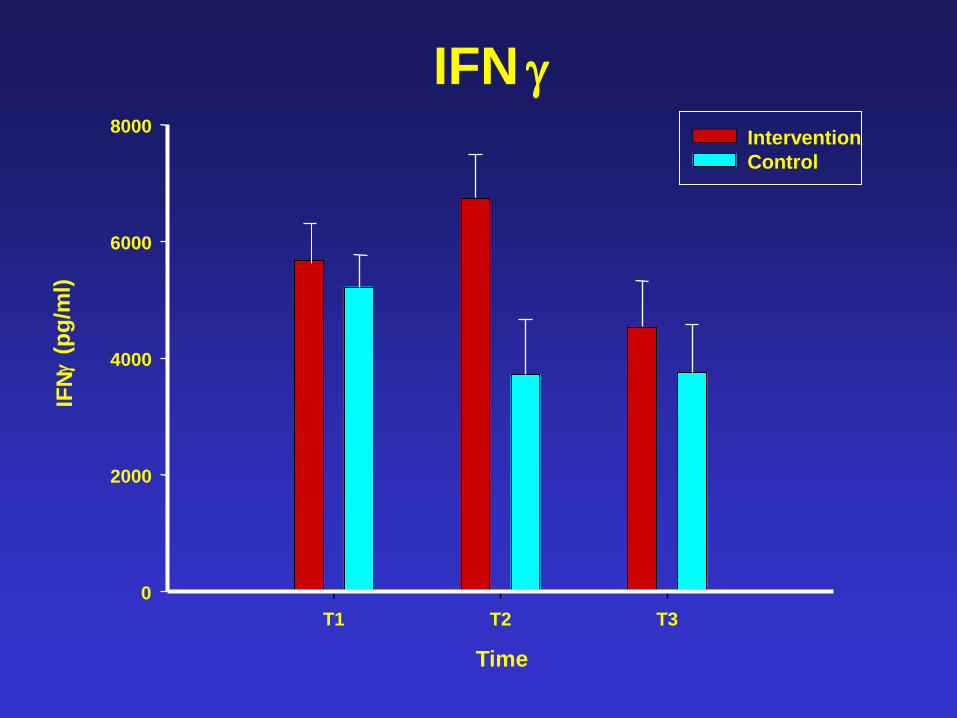
T helper 1 profile in CBSM intervention and
control group
IFN-g IL-2
IL-12 TNFa
*
IFNg
Time
T1 T2 T3
IFN
g (p
g/m
l)
0
2000
4000
6000
8000
IL-2
Time
T1 T2 T3
IL-2
(pg/m
l)
0
5
10
15
20
25
IL-12
Time
T1 T2 T3
IL-1
2 (p
g/m
l)
0
100
200
300
400
500
600
700
Col 12
Col 14
TNFa
Time
T1 T2 T3
TN
Fa
(p
g/m
l)
0
2000
4000
6000
8000
10000
12000
14000
Intervention
Control
* n=16
n=16 n=15
n=14
n=14
n=12
n=19
n=17
n=16
n=14 n=14 n=12
n=16
n=16 n=15 n=14
n=14
n=12
n=16
n=16
n=15
n=14
n=14
n=12
Time
T1 T2 T3
IFN
g (p
g/m
l)
0
2000
4000
6000
8000
IFN g Intervention
Control

Changes in Positive Psy Adaptation (slope) and
Changes in Th1 Cytokine Production (slope)
Measure1 g-IFN IL-2
ABS-Pos Affect .59** --
BF-Spiritual .46* .82**
BF-Lifestyle .71** --
**p < .01 *p < .05
1all measures slope of chg over 3, 6, 12, and 18 months post-surg
ABS: Affect Balance Scale
BF: Benefit Finding

CBSM Intervention after
Surgery for Breast Cancer: Psychological adaptation:
•increased benefit finding and optimism
•decreased anxiety, depression, soc disruption, fatigue, sleep disruption
•increased perceived relaxation skills, CBT and emotion processing important
Physiological adaptation:
•decreases in PM cortisol levels
•increased LPR to anti-CD3 challenge
•increased g-IFN and IL-2 and Th1/Th2 ratio production during LPR
Pattern of effects suggest a faster recovery after adjuvant therapy in CBSM pts vs controls
Antoni et al (2001) Health Psychology, 20, 20-32;
Cruess, Antoni et al (2000) Psychosomatic Medicine, 61, 94.
McGregor et al., (2004) J. Psychosom Res, 56, 1 – 8;
Antoni et al. (2006) Amer J. Psychiatry
Antoni et al., (2006) JCCP; Phillips et al. (2008) Psychosom Med;
Antoni et al. (2009) Brain Beh Imm
Autonomic nervous system
•NE
•Epinephrine
•Other neuropeptides
Adrenal
Gland
DNA Repair
Proliferation
Migration & invasion
Proteases (MMPs)
Angiogenesis / Pro-angiogenic cytokines (VEGF, IL-6)
Inflammation (NFkB)
ACTH
Cortisol NE/Epi
CRF / Locus Coeruleus
Cancer cells
Immune cells (will need to
show different types of cells –
NK, T, Macroph, etc.)
Dopamine
Endothelial cells
(or a blood vessel)
Oxytocin
Oncogenic viruses
Oncogene transcription
Viral replication
Host cell cycling
Immune response
IFN Activation
Optimism
Perceived Stress
Depression
Social Isolation
Negative Life Events
Environmental stressors (SES)
External Events Psychological Reactions
Neuroendocrine Activity
Peripheral Tissue
Antoni, Lutgendorf, Cole, Sephton, Dhabar, McDonald, Stefanek & Sood (2006). Nature Reviews Cancer, 6, 240-248.
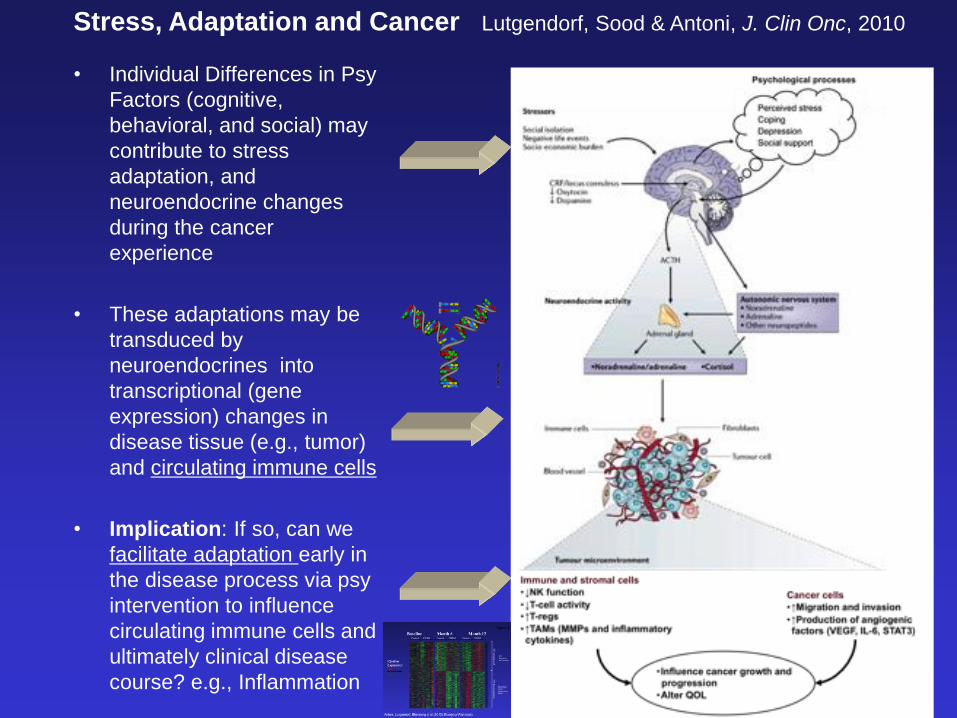
• Individual Differences in Psy
Factors (cognitive,
behavioral, and social) may
contribute to stress
adaptation, and
neuroendocrine changes
during the cancer
experience
• These adaptations may be
transduced by
neuroendocrines into
transcriptional (gene
expression) changes in
disease tissue (e.g., tumor)
and circulating immune cells
• Implication: If so, can we
facilitate adaptation early in
the disease process via psy
intervention to influence
circulating immune cells and
ultimately clinical disease
course? e.g., Inflammation
Stress, Adaptation and Cancer Lutgendorf, Sood & Antoni, J. Clin Onc, 2010

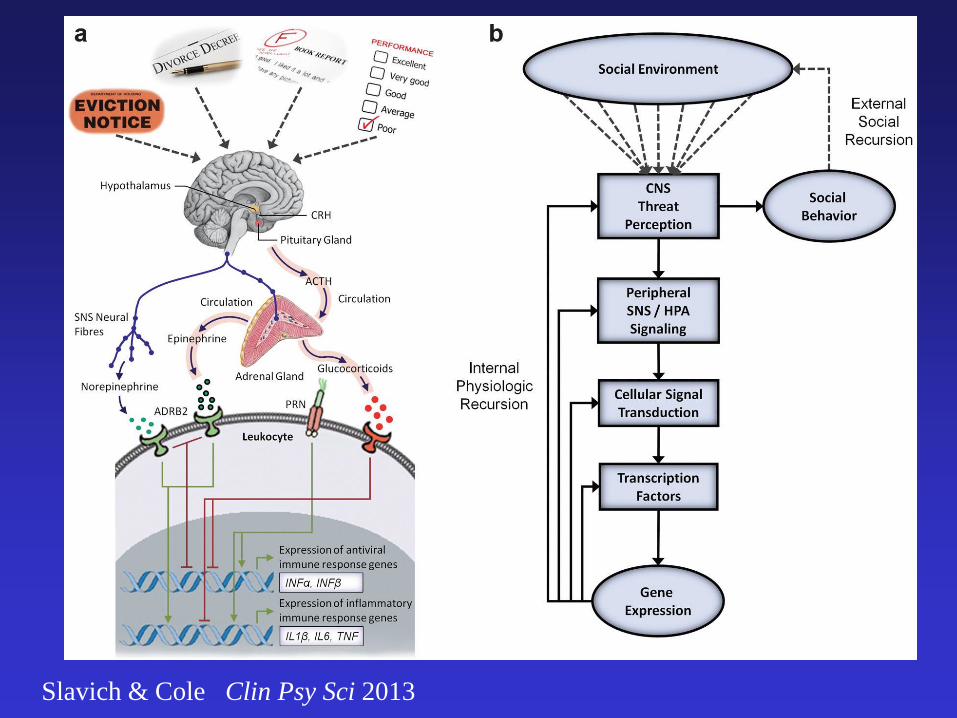
Slavich & Cole Clin Psy Sci 2013

Biobehavioral Pathways Associated with Stress
and Cancer Pathogenesis (Miller & Cole, 2009 Ann Rev Psychol.)
CREB/ATF
GR
NFkB/ IL-1
STRESS •Chronic stress •Depression •Social Adversity
CANCER PATHOGENESIS •Apoptosis/Anoikis •Angiogenesis •Growth & Metastasis
BIOBEHAVIORAL MEDIATORS
•SNS Activation
•HPA dysregulation
•Inflammation
•Cellular Immune Suppression Type I IFN
Slavich & Cole Clin Psy Sci 2013

Chronic Stress/Adversity and
Negative Affect
Inflammation: e.g., NFkB response
elements in promoters of downstream
transcription
Cytokines (IL1A, IL1B, IL1RA, IL6, TNF)
Chemokines (CCLs, CXCLs)
Oxidative stress (Superoxide dismutase, SODs)
Prostaglandin signaling (cyclooxygenase: CoX 2)
Pro-Inflammatory Cytokines and their Sequelae
IL-1-a, IL1-b, IL-6, TNF-a, IL-8, PGs
CRF
Upstream DNA
Transcriptional
Control Pathway
Downstream
Gene Expr for
translation of
RNA
Protein
Synthesis
Stress and Inflammatory Gene Expression in cells making inflammatory proteins
Neuroendocrine regulation:
SNS, HPA

Study Aims
• Aim 1: Determine whether individual differences in
psychological adaptation relate to differences in
leukocyte gene expression among women early in
their treatment for primary (non-metastatic) breast
cancer.
• Aim 2: Test whether a psychological intervention
(CBSM) designed to facilitate adaptation is
associated with changes in leukocyte gene
expression over time

Study Sample and Measures
• Sample: 79 Women undergoing surgery for non-metastatic BCa in prior 2
– 10 wks and not yet started adjuvant therapy
• Psychological Adaptation
– Positive Affect/Negative Affect Balance (Affect Balance Scale, ABS, Derogatis, 1975)
• Other Psy Factors
– Perceived stress management skill efficacy
– Personal growth (benefit finding scale: BFS)
– Fatigue (FSI) and Sleep quality (PSQI)
– QoL/Well-Being (FACT)
• Transcriptional Indicators
– miRNA expression: pro-inflam cytokines, chemokines and tumor promoting transcripts
– Gene Library convergence: pro-inflammatory and wound healing pathways
– Bioinformatically inferred upstream transcripts: NFkB, GATA, STAT, GR
• Criteria for differential expression
– 50% up- or down-regulation (< 5% false discovery rate)
– Traditional p-value
• Covariates
– Sociodemographic (age, race, SES)
– Biomedical (disease stage, ER/PR/HER1Neu, surgery type, days since surg, meds)
Hypotheses
• Hyp 1: Greater Levels of Adaptation (Positive: Negative affective
state = ABS composite score) will relate to a better leukocyte
transcriptional profile
– Less Pro-Inflammatory Signaling (cytokines, chemokines, Cox2/PG, oxidat stress)
– Less Pro-Metastatic Signaling (enzymes for tissue invasion, remodeling and
epithelial-mesenchymal transition [EMT])
• Hyp 2: CBSM will facilitate adaptation and improve leukocyte
transcriptional profile
– Increased Positive Affect
– Decreased Negative Affect
– Increased Affect Balance (Positive – Negative Afect)
– Less Pro-Inflammatory Signaling
– Less Pro-Metastatic Signaling
– Greater Glucocorticoid Receptor Sensitivity
Study Analyses
• Hyp 1: Genomic-Affect Association: Relationships between
baseline affective state (ABS composite score) and expression of
each analyzed transcript were assessed by multiple regression
– controlling for age, race (white vs. non-), and tumor stage, estrogen receptor
(ER)-, and progesterone receptor (PR) status. Genes showing > 50% differential
expression for each 1SD diff in ABS composite scores were identified as
differentially expressed
• Hyp 2: Effects of CBSM on expression of each analyzed transcript
were assessed in a 2 (Group: CBSM vs. Control) x 3 (Time: baseline,
6-, and 12-month follow-up) mixed model factorial design
– controlling for individual differences in age, race, tumor stage, ER status, PR
status, treatment with chemotherapy, and treatment with radiation.
– All analyses were conducted on an intent-to-treat basis with parameters estimated
in the context of mixed effect linear models including all cases

403 screened for eligibility
204 excluded
55 ineligible
149 declined participation
or failed to appear for T1
199 randomized
107 assigned to control
107 treated as assigned
34 provide T1 PBMC samples
92 assigned to intervention
92 treated as assigned
45 provide T1 PBMC samples
CONSORT DIAGRAM
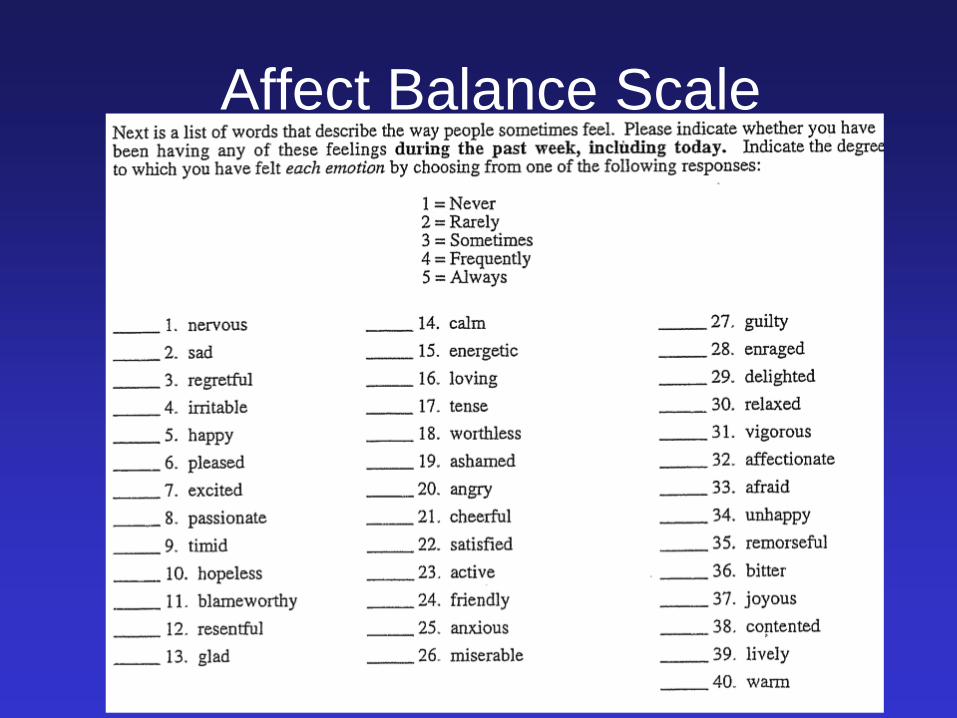
Affect Balance Scale

Transcriptional Indicators Focus on Pro-inflammatory and Pro-Metastatic Signaling
in Circulating PBMCs
• miRNA expression: pro-inflam cytokine, chemokines and tumor
promoting transcripts
• Gene Library convergence: functional significance of genes identified:
pro-inflammatory and wound healing pathways
• Bioinformatically-inferred upstream transcripts controlling gene
expression: NFkB, STAT, GATA
• Bioinformatically-inferred cell populations involved within the PBMC
compartment
Genomic Studies: Microarray Analysis
• PBMCs analyzed with Illumina Human HT-12 v3 Expression BeadChips
• Expression of 27,455 human genes derived from low-level fluorescence
intensity values & quantile normalized w/ Illumina Genome Studio software
• Functional characteristics-GOstat Gene Ontology, GeneCards, EntrezGene
• Activity of specific transcription control pathways* assessed by TELiS
bioinformatic analysis of transcription factor-binding motif (TFBM)
distributions in the promoters of differentially expressed genes:
NF-kB, STAT, GATA, IFN, GR
*transcripts identified as differentially expressed by microarray analysis were re-verified using quantitative RT-PCR with TaqMan
gene expression assays (Applied Biosystems Inc), a one-step enzyme system (Quantitect RT-PCR; Qiagen), and manufacturer’s
specified thermal cycling protocol on a iCycler real-time PCR instrument (BioRad Inc.). Data were analyzed by standard
threshold cycle analysis after normalization to parallel-assayed ACTB mRNA concentrations

Aim 1 Study Analyses
• Genomic-Affect Association: Relationships between baseline
affective state (ABS composite score) and expression of each
analyzed transcript were assessed by multiple regression
– controlling for age, race (white vs. non-), and tumor stage, estrogen receptor
(ER)-, and progesterone receptor (PR) status. Genes showing > 50% differential
expression per 1 SD diff in ABS affect balance composite scores were identified
as differentially expressed

RESULTS:
Affect and Gene Expression • 201 named human genes showed > 50% difference in expression
across the range of ABS composite scores at study entry (2 – 8
wks post-surgery)
• 177 genes were up-regulated in association with affect ratio
reflecting more negative affect, including genes encoding:
– pro-inflammatory cytokines (IL1A, IL1B, IL6, TNF)
– prostaglandin-synthesis enzyme COX2 (PTGS2)
– the oxidative stress response (SOD2)
– inflammatory chemokines and related receptors (CCL3, CCL3L1, CCL4L2,
CCL7, CCL20, CXCL9, CXCL10, CXCR6, CXCR7)
– tissue remodeling and epithelial-mesenchymal transition (LMNA, MMP9)
• Bioinformatic Analysis
GOstat Gene Ontology Analyses (p’s < .0001) for pro-inflammatory and wound-
healing signaling
Upstream Signaling Implicated: NFkB
Inferred Cell Populations: Myeloid
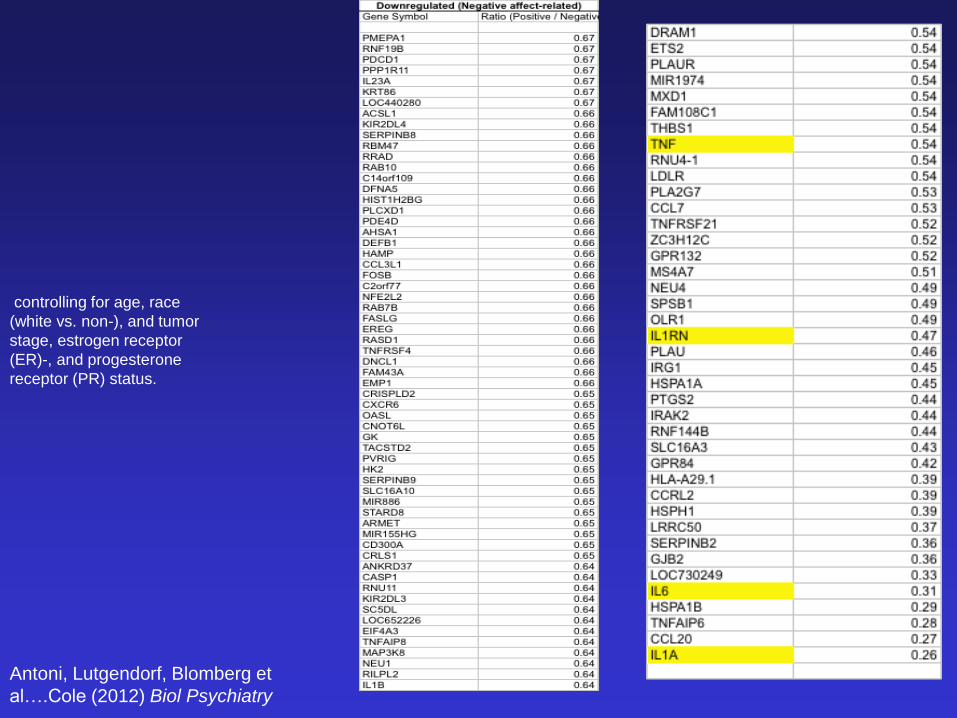
Antoni, Lutgendorf, Blomberg et
al….Cole (2012) Biol Psychiatry
controlling for age, race
(white vs. non-), and tumor
stage, estrogen receptor
(ER)-, and progesterone
receptor (PR) status.

Comparing Mood X Leukocyte Gene Expression
Associations in Different Cancer Populations
Antoni et al. (2012) Biol. Psychiatry
Breast Cancer (N = 79)
Lower PA/Greater NA associated w/ 50% diff in exp of 201 genes:
•Pro-Inflammatory Signaling: –Cytokines [IL1A,IL1B,TNF,IL6,IL1RN]
–Chemokines [CCL2, CCL3, CCL3L1, CCL4L2, CCL7, CCL20, CACL9, CXCL10, CXCR6, CXCR7]
–Oxidative Stress [SOD2]
–COX 2 [COX2/PTGS2]
•Pro-Metastatic Signaling (PBMCs): –MMP9, LMNA
•Gene Ontology Analyses: –Transcripts converging on pro-inflammatory signaling (p < .0001)
•Inferred* Upstream Signaling –NFkB
•Implicated* PBMC Population –Myeloid * Based on TeLiS Bioinformatic Program
Cohen et al. (2012) PLoS One
Metastatic RCC (N = 30)
Depression associated w/ 50% diff in
exp of 177 genes:
•Pro-Inflammatory Signaling: –Cytokines [IL1A,IL1B,TNF,IL6,IL1RN]
–Chemokines [CCL2, CCL3, CCL3L1, CCL4L2,
CCL7, CCL8, CCL20, CCR7, CXCL1, CXCL16]
–Oxidative Stress [SOD2]
–COX 2 [COX2/PTGS2]
•Pro-Metastatic Signaling (tumor) –MMP9, MMP2
•Gene Ontology Analyses: –Transcripts converging on pro-inflammatory signaling (p < .0001)
•Inferred* Upstream Signaling –NFkB
•Implicated* PBMC Population –Myeloid (greater TAMs in depressed)

Study Aims
• Aim 1: Determine whether individual differences in
psychological adaptation relate to differences in
leukocyte gene expression among women early in
their treatment for primary (non-metastatic) breast
cancer.
• Aim 2: Test whether a psychosocial intervention
(CBSM) designed to facilitate adaptation is
associated with changes in leukocyte gene
expression over time

Effects of Intervention Targeting Adaptation: Cognitive
Behavioral Stress Management (CBSM)

403 screened for eligibility
204 excluded
55 ineligible
149 declined participation
or failed to appear for T1
199 randomized
107 assigned to control
107 treated as assigned
34 provide T1 PBMC samples
92 assigned to intervention
92 treated as assigned
45 provide T1 PBMC samples
85 assessed at T2 (6 mo)
28 provide T2 PBMC samples
74 assessed at T2 (6 mo)
34 provide T2 PBMC samples
83 assessed at T3 (12 mo)
23 provide T3 PBMC samples
74 assessed at T3 (12 mo)
34 provide T3 PBMC samples
34 analyzed for gene expression
18 T1 & T2 PBMC samples
6 T1 & T3 PBMC samples
45 analyzed for gene expression
21 T1 & T2 PBMC samples
7 T1 & T3 PBMC samples
CONSORT DIAGRAM


No Between-Group Differences
• Surgery
• Adjuvant type (chemo, radiation)
• Time since surgery
• Endocrine therapy
• Demographics
Study Analyses
• Effects of CBSM on psychological adaptation were first assessed in
the subsample with gene expression data in a 2 (Group: CBSM vs.
Control) x 3 (Time: baseline, 6-, and 12-month follow-up) factorial
design
• Effects of CBSM on expression of each analyzed transcript were
assessed in a 2 (Group: CBSM vs. Control) x 3 (Time: baseline, 6-,
and 12-month follow-up) factorial design
– controlling for individual differences in age, race, tumor stage, ER status, PR
status, treatment with chemotherapy, and treatment with radiation.
– All analyses were conducted on an intent-to-treat basis with parameters estimated
in the context of mixed effect linear models including all cases

Did CBSM Facilitate Psy Adaptation?
• ABS Affect Balance Score (Group x Time effect, p = .0042), with:
• CBSM-treated group showing: (linear time trend over 12 months)
– increased positive affect: +6.8 ± 2.36, p = .0055
– decreased negative affect: -8.22 ± 2.08, p = .0003
– Increased composite affect balance scores: +17.54 ± 4.12, p < .0001
• Control group showed
– negligible change over time on each dimension:
– positive affect: -0.16 ± 1.94, p = .936
– negative affect: -4.64 ± 3.94, p = .245
– overall affect balance: 1.00 ± 3.62, p = .784.

CBSM Effects on Adaptation and Other
Psychological Variables
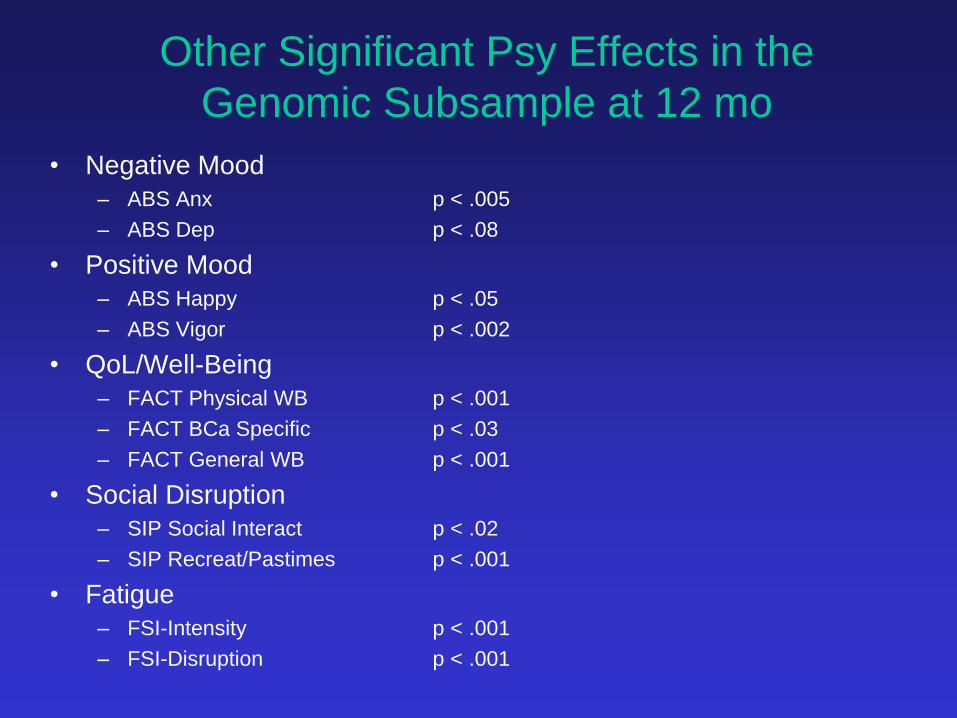
Other Significant Psy Effects in the
Genomic Subsample at 12 mo
• Negative Mood
– ABS Anx p < .005
– ABS Dep p < .08
• Positive Mood
– ABS Happy p < .05
– ABS Vigor p < .002
• QoL/Well-Being
– FACT Physical WB p < .001
– FACT BCa Specific p < .03
– FACT General WB p < .001
• Social Disruption
– SIP Social Interact p < .02
– SIP Recreat/Pastimes p < .001
• Fatigue
– FSI-Intensity p < .001
– FSI-Disruption p < .001
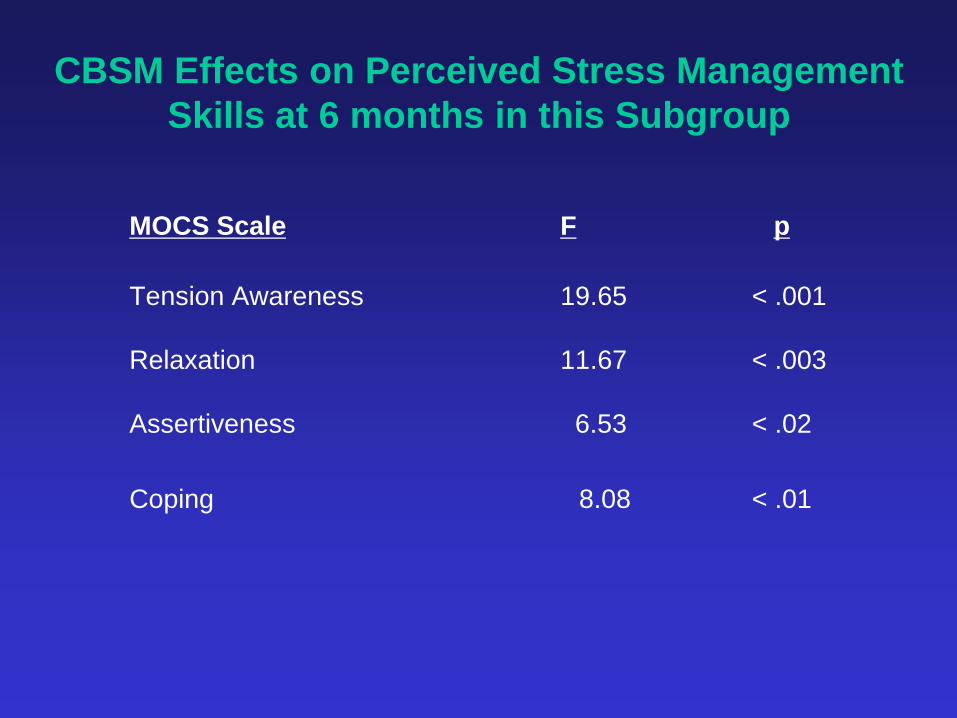
CBSM Effects on Perceived Stress Management
Skills at 6 months in this Subgroup
MOCS Scale F p
Tension Awareness 19.65 < .001
Relaxation 11.67 < .003
Assertiveness 6.53 < .02
Coping 8.08 < .01

Study Analyses
• Effects of CBSM on psychological adaptation were first assessed in
the subsample with gene expression data in a factorial design
• Effects of CBSM on expression of each analyzed transcript were
assessed in a 2 (Group: CBSM vs. Control) x 3 (Time: baseline, 6-,
and 12-month follow-up) factorial design
– controlling for individual differences in age, race, tumor stage, ER status, PR
status, treatment with chemotherapy, and treatment with radiation.
– All analyses were conducted on an intent-to-treat basis with parameters estimated
in the context of mixed effect linear models including all cases
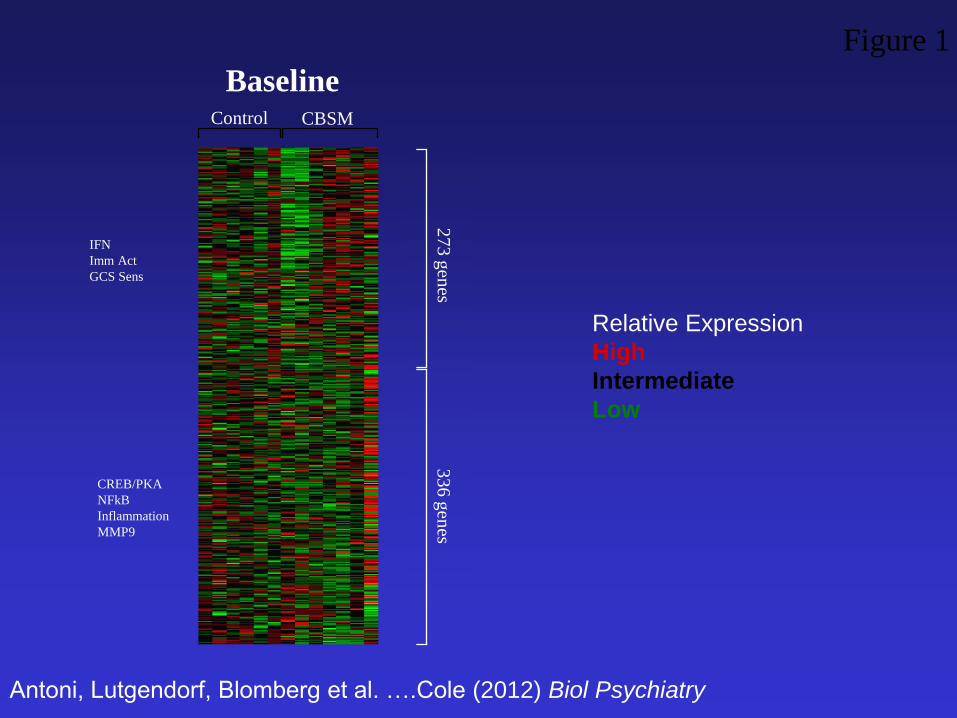
CBSM Control
Baseline
Figure 1
Antoni, Lutgendorf, Blomberg et al. ….Cole (2012) Biol Psychiatry
IFN
Imm Act
GCS Sens
CREB/PKA
NFkB
Inflammation
MMP9
27
3 g
enes
33
6 g
enes
Relative Expression
High
Intermediate
Low

CBSM Control CBSM Control
Baseline Month 6
Figure 1
27
3 u
preg
ulated
3
36
do
wn
regu
lated
Antoni, Lutgendorf, Blomberg et al….Cole (2012) Biol Psychiatry
IFN
Imm Activ
GCS Sensitiv
CREB/PKA
NFkB
Inflammation
MMP9

CBSM Control CBSM Control CBSM Control
Baseline Month 6 Month 12
Figure 1
27
3 u
preg
ulated
3
36
do
wn
regu
lated
IFN
Imm Activ
GCS Sensitiv
CREB/PKA
NFkB
Inflammation
MMP9
Antoni, Lutgendorf, Blomberg et al (2012) Biological Psychiatry

2 X 3 RANOVAs: Effects of CBSM on
Reversing Stress-Related Genomic Expression
• 62 transcripts showed significantly greater down-regulation in CBSM-
treated patients relative to controls, including genes encoding:
– pro-inflammatory cytokines (IL1A, IL1B, IL6)
– the prostaglandin-synthesis enzyme COX2 (PTGS2)
– inflammatory chemokines and their receptors (CCL2, CCL3, CCL3L1,
CCL3L3, CCL4L1, CCL4L2, CCL7, CXCL1, CXCL2, CXCR7),
– mediators of tissue remodeling and epithelial-mesenchymal transition (G0S2,
LMNA, MMP9, OSM).
GOstat Gene Ontology analyses (p’s < .0001)
• 29 genes showed significantly greater up-regulation in CBSM-treated
patients vs. controls, including genes involved in:
– Type I interferon response (IFIT1, IFIT2, IFIT3, IFI44, IFI44L, ISG15, MX2,
OAS2, OAS3),
– Type II interferon signaling (IFN-g), and interferon signal transduction (STAT1,
STAT2).
GOstat Gene Ontology analyses (p’s < .0001)
Antoni, Lutgendorf, Blomberg et al…..Cole (2012) Biological Psychiatry

2 X 3 RANOVAs: Effects of CBSM on
Reversing Stress-Related Genomic Expression
(N = 79)
• INFLAMMATION: 62 transcripts showed significantly greater down-
regulation in CBSM-treated patients relative to controls, including
genes encoding:
– pro-inflammatory cytokines (IL1A, IL1B, IL6, TNF)
– the prostaglandin-synthesis enzyme COX2 (PTGS2)
– inflammatory chemokines and their receptors (CCL2, CCL3, CCL3L1,
CCL3L3, CCL4L1, CCL4L2, CCL7, CXCL1, CXCL2, CXCR7),
– mediators of tissue remodeling and epithelial-mesenchymal transition (G0S2,
LMNA, MMP9, OSM).
• ANTI-VIRAL IMMUNITY: 29 genes showed significantly greater up-
regulation over time in CBSM-treated patients vs. controls, including
transcripts involved in:
– Type I interferon response (IFIT1, IFIT2, IFIT3, IFI44, IFI44L, ISG15, MX2,
OAS2, OAS3),
– Type II interferon signaling (IFN-g), and interferon signal transduction (STAT1,
STAT2).
Antoni, Lutgendorf, Blomberg et al…..Cole (2012) Biological Psychiatry

2 X 3 Mixed Model Effects of CBSM on Negative
Mood-Related Genomic Expression (Highlighted changes in those genes associated with baseline Negative Affect)
• 62 transcripts showed significantly greater down-regulation in CBSM-
treated patients relative to controls (> 50% differential chg), including
genes encoding:
– pro-inflammatory cytokines (IL1A, IL1B, IL6, TNF)
– the prostaglandin-synthesis enzyme COX2 (PTGS2)
– inflammatory chemokines and their receptors (CCL2, CCL3, CCL3L1,
CCL3L3, CCL4L1, CCL4L2, CCL7, CXCL1, CXCL2, CXCR7),
– mediators of tissue remodeling and epithelial-mesenchymal transition (G0S2,
LMNA, MMP9, OSM).
GOstat Gene Ontology analyses (p’s < .0001)
Thirty-one (50%) of the total 62 CBSM-downregulated transcripts also
appeared on the list of genes upregulated in association with negative
affect at baseline (greater than the <1% overlap expected by chance;
binomial p < .0001).
pro-inflammatory transcriptional activation effects hold in ancillary analyses that controlled for additional
treatment-related variables: chemotherapy or radiation (within 3 weeks before each study visit), primary
surgery type (lumpectomy, mastectomy, or bilateral mastectomy), and use of pain medications, anxiolytics, or
antidepressants (downregulation of pro-inflammatory genes, GO:0006954; GO:0009611; both p < .0001;
Antoni, Lutgendorf, Blomberg et al…..Cole (2012) Biological Psychiatry

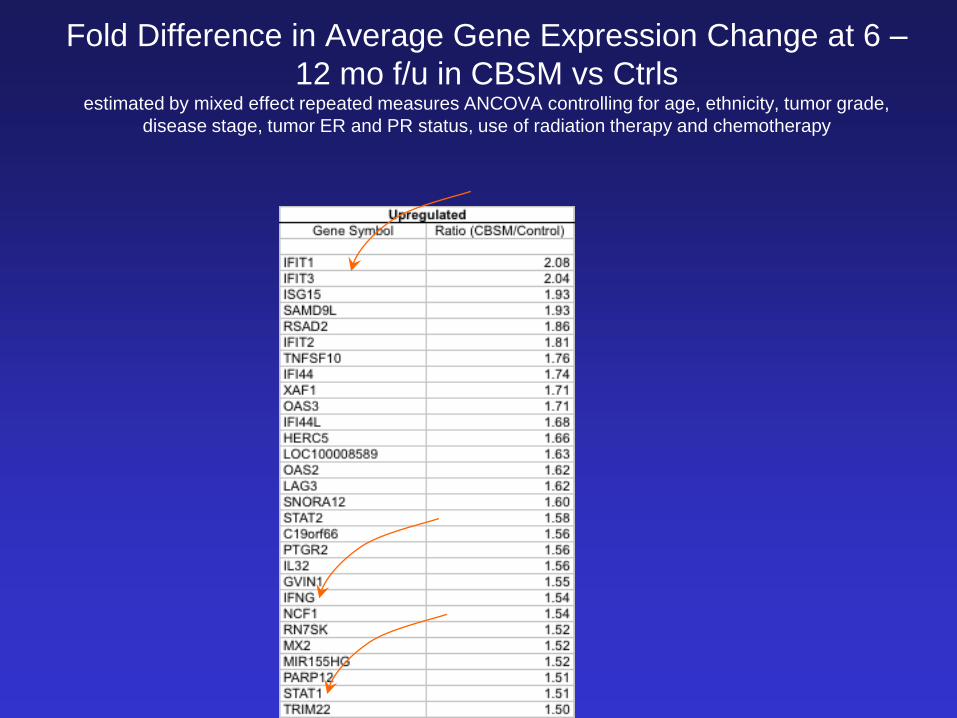
Fold Difference in Average Gene Expression Change at 6 –
12 mo f/u in CBSM vs Ctrls estimated by mixed effect repeated measures ANCOVA controlling for age, ethnicity, tumor grade,
disease stage, tumor ER and PR status, use of radiation therapy and chemotherapy

2 X 3 RANOVAs: Effects of CBSM on
Reversing Stress-Related Genomic Expression
• INFLAMMATION: 62 transcripts showed significantly greater down-
regulation in CBSM-treated patients relative to controls, including genes
encoding:
– pro-inflammatory cytokines (IL1A, IL1B, IL6)
– the prostaglandin-synthesis enzyme COX2 (PTGS2)
– inflammatory chemokines and their receptors (CCL2, CCL3, CCL3L1, CCL3L3,
CCL4L1, CCL4L2, CCL7, CXCL1, CXCL2, CXCR7),
– mediators of tissue remodeling and epithelial-mesenchymal transition (G0S2, LMNA,
MMP9, OSM).
• ANTI-VIRAL IMMUNITY: 29 genes showed greater up-regulation over
time in CBSM-treated patients vs. controls, including transcripts involved
in:
– Type I interferon response (IFIT1, IFIT2, IFIT3, IFI44, IFI44L, ISG15, MX2, OAS2,
OAS3),
– Type II interferon signaling (IFN-g), and signal transduction (STAT1, STAT2).
– These mirror prior CBSM effects on IFN-g production in women with BCA
Antoni, Lutgendorf, Blomberg et al…..Cole (2012) Biological Psychiatry; Antoni et al (2009), BBI
Fold Difference in Average Gene Expression Change at 6 –
12 mo f/u in CBSM vs Ctrls estimated by mixed effect repeated measures ANCOVA controlling for age, ethnicity, tumor grade,
disease stage, tumor ER and PR status, use of radiation therapy and chemotherapy

Antoni, Lutgendorf, Blomberg et al…..Cole (2012)

Antoni, Lutgendorf, Blomberg et al…..Cole (2012) Biological Psychiatry

Genomic Studies: Microarray Analysis Pre-Post
• PBMCs analyzed with Illumina Human HT-12 v3 Expression BeadChips
• Expression of 27,455 human genes derived from low-level fluorescence
intensity values & quantile normalized w/ Illumina Genome Studio software
• Genes > 50% difference in average expression in CBSM vs control
identified as differentially expressed (False Discovery Rate ≤ 5%)
• Functional characteristics-GOstat Gene Ontology, GeneCards, EntrezGene
• Activity of specific transcription control pathways* assessed by TELiS
bioinformatic analysis of transcription factor-binding motif (TFBM)
distributions in the promoters of differentially expressed genes:
NF-kB, STAT1, GATA, GC Receptor (GR)
• Transcript origin analysis was employed to identify the specific leukocyte subsets
predominately mediating CBSM effects on the overall PBMC pool transcriptome.
*transcripts identified as differentially expressed by microarray analysis were re-verified using quantitative RT-PCR with TaqMan
gene expression assays (Applied Biosystems Inc), a one-step enzyme system (Quantitect RT-PCR; Qiagen), and manufacturer’s
specified thermal cycling protocol on a iCycler real-time PCR instrument (BioRad Inc.). Data were analyzed by standard
threshold cycle analysis after normalization to parallel-assayed ACTB mRNA concentrations

Chronic Stress/Adversity and
Negative Affect
Inflammation: e.g., NFkB
response elements in promoters
of downstream transcription
Cytokines (IL1A, IL1B, IL1RA, IL6, TNF)
Chemokines (CCLs, CXCLs)
Oxidative stress (Superoxide dismutase, SODs)
Prostaglandin signaling (cyclooxygenase: CoX 2)
Pro-Inflammatory Cytokines and their Sequelae
IL-1-a, IL1-b, IL-6, TNF-a, IL-8
CRF
Upstream
Transcriptional
Control Pathway
Downstream
Gene
Expression
Protein
Synthesis
Stress and Inflammatory Gene Expression
Neuroendocrine regulation:
SNS, HPA

Fold Difference in TFBM Expression over 6 – 12mo
(log CBSM vs Control)
Interferon
Imm Act
GCS Sens
NFkB
Inflammation
Antoni, Lutgendorf, Blomberg et al…..Cole, Biological Psychiatry (2012)

Fold Difference in TFBM Expression over 6 – 12mo
(log CBSM vs Control)
Interferon
Imm Act
GCS Sens
NFkB
Inflammation
Antoni, Lutgendorf, Blomberg et al…..Cole, Biological Psychiatry (2012)

Stress-related Neuroendocrines can modulate cell-
signaling and inflammatory protein synthesis

Cells Involved in Up-Regulation and Down-
Regulated Genes?
Transcript Origin Analysis was
employed to identify the specific
leukocyte subsets predominately
mediating CBSM effects on the
overall PBMC pool transcriptome.
Antoni, Lutgendorf, Blomberg et
al…..Cole (2012) Biological Psychiatry

CBSM Effects on CREB/ATF (SNS) BL 12mo
and GCS gene expression Ctrl CBSM Ctrl CBSM
suggest impact on on stress pathways
IFN
Imm Act
GCS Sens
Antoni, Lutgendorf, Blomberg et al….Cole
(2012) Biol Psychiatry
CREB/PKA
NFkB
Inflammation
MMP9
CBSM Effects on NFkB and IFN
expression suggest decreased
inflammation and increased Type I
IFN signaling
Transcription Factor Binding Motifs (TFBMs) *Ratio CBSM: Ctrl

Antoni, Lutgendorf, Blomberg…..Cole (2012) Biol Psychiatry, 71, 366-72
Antoni (2013). Brain, Behavior and Immunity, 30, S88 – S98.

Matrix Metalloproteases (MMPs)
Secreted into the extracellular
matrix (ECM) by stromal
leukocytes such as macrophages
Capable of degrading many
kinds of ECM protein and
facilitating invasion and
migration.
One of the most studied in
metastasis and angiogenesis
MMP-2 and MMP-9 promote
angiogenesis and invasion and
are associated with shorter
disease free survival (Kamat et
al, 2006).

Conclusions
• Psychological processes (adaptation and stress mgmt
interventions) – may be associated with biological indicators that
– may predict breast cancer disease activity and clinical outcomes
• That is a lot of “Maybes”
• Is it: – Psy Biological Disease Outcome..”my stress makes me inflamed & sicker”
– Disease Biological Psy…”I am stressed and inflamed as my disease worsens”
– Biological Psy and Disease Outcome…”my treatments make me stressed and
inflamed so I skip them and get sicker”
– None of the above? All of the above?.....”these are all random happenstances”
• Limits – Microarray analyses need confirmation by protein tests
– Our understanding of biology of breast cancer is still evolving
– Our findings can be over-interpreted so caution is in order in our claims

Examining Leukocyte Transcription
Provides BIG data • Does Facilitating Adaptation relate to gene expression in
PBMCs for:
– Inflammation? (NFkB, STAT cytokine/chemokine/PGs)
– HPA regulation? (GR) affects anti-inflammatory control
– Disease progression promoters? MMP-9, LMNA, G0S2
– Myeloid cells (monocytes and DCs) likely mediators
• $$$ Questions: Are these differences in expression tied to:
– QOL and symptom management?
– Faster recovery from surgery or adjuvant therapy?
– Ability to tolerate larger dosage of adjuvant tx?
– Success of cancer treatments vs resistance?
– Clinical disease outcomes (recurrence, mortality)?

Lutgendorf, Sood & Antoni, J. Clin Onc, 2010
Tracking Gene Gangs in the Hood………
Tracking patterns of gene
expression changes in
cells in the
“neighborhood of tumors”
may give us a window
into how stress affects
body’s ability to stay
healthy, less inflamed
and better defended
If so then we can observe
how stress management
affects these processes
as well over the long
term!
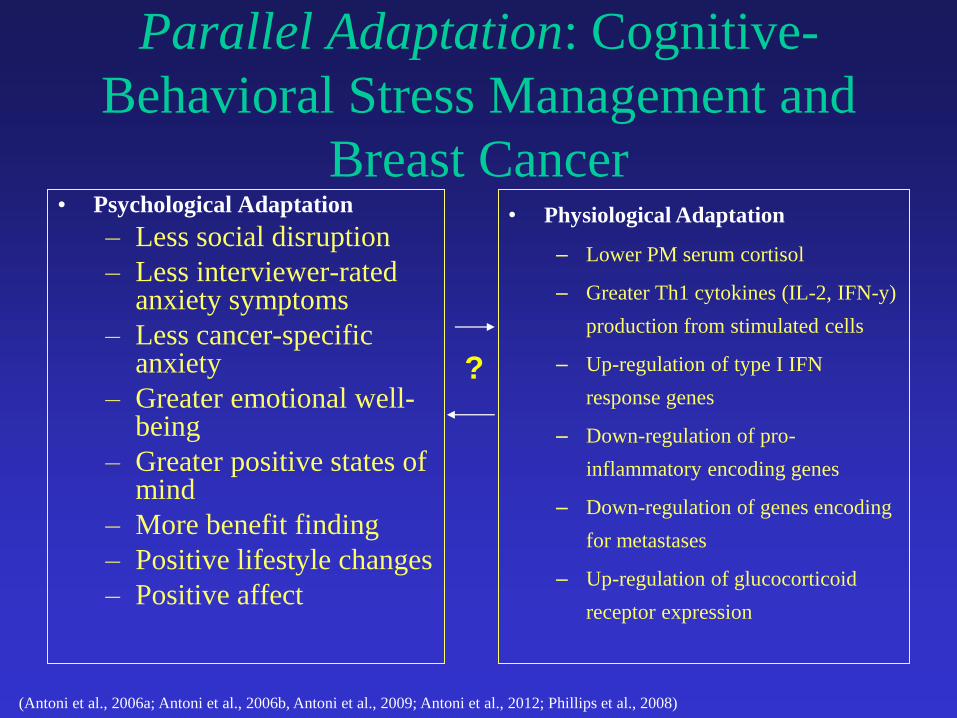
Parallel Adaptation: Cognitive-
Behavioral Stress Management and
Breast Cancer • Psychological Adaptation
– Less social disruption
– Less interviewer-rated anxiety symptoms
– Less cancer-specific anxiety
– Greater emotional well-being
– Greater positive states of mind
– More benefit finding
– Positive lifestyle changes
– Positive affect
(Antoni et al., 2006a; Antoni et al., 2006b, Antoni et al., 2009; Antoni et al., 2012; Phillips et al., 2008)
• Physiological Adaptation
– Lower PM serum cortisol
– Greater Th1 cytokines (IL-2, IFN-y)
production from stimulated cells
– Up-regulation of type I IFN
response genes
– Down-regulation of pro-
inflammatory encoding genes
– Down-regulation of genes encoding
for metastases
– Up-regulation of glucocorticoid
receptor expression
?

Immune Findings Mirror Other Recent Work Using
Psychosocial Interventions In Bca Women Post-Surgery
• 16-wk + Monthly Booster CBT + Lifestyle Change
(Andersen et al. 2004, 2007)
• 8-wk Mindfulness Based Stress Mgmt
(Witek-Janusek….. Mathews, 2008)
• 8-wk CBT
(Savard, Simard, Ivers, & Morin, 2005)
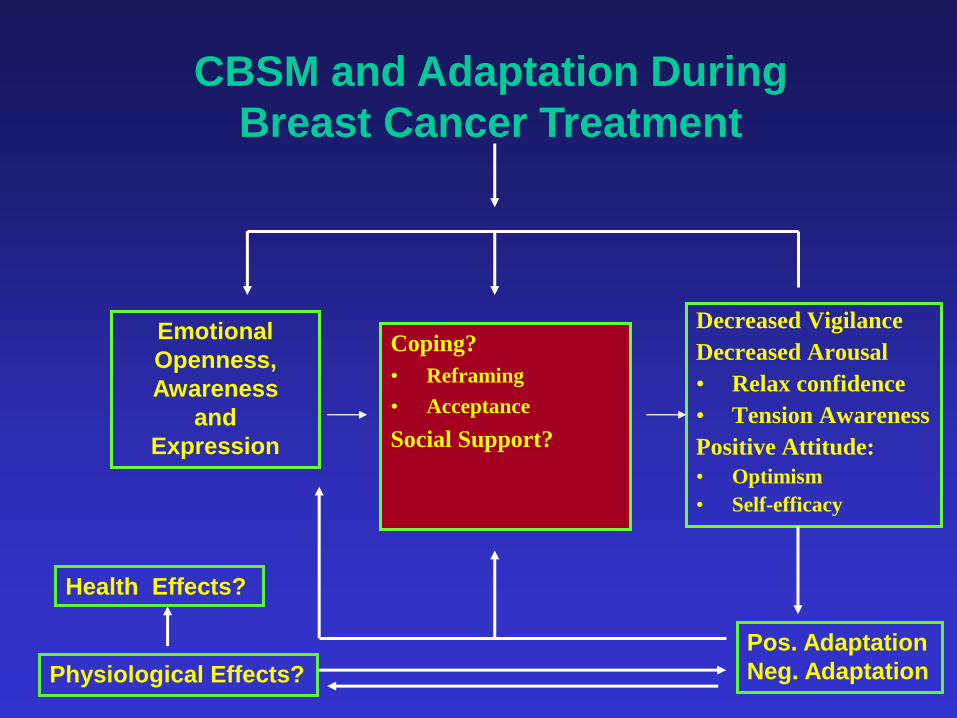
Coping?
• Reframing
• Acceptance
Social Support?
Decreased Vigilance
Decreased Arousal
• Relax confidence
• Tension Awareness
Positive Attitude:
• Optimism
• Self-efficacy
Emotional
Openness,
Awareness
and
Expression
Pos. Adaptation
Neg. Adaptation
CBSM and Adaptation During
Breast Cancer Treatment
Physiological Effects?
Health Effects?

Model for Psychosocial Intervention Effects on
Psychological Adaptation, Biobehavioral Processes and
Cancer Pathogenesis and Clinical Outcomes
CREB/ATF
GR resistance
NFkB/ IL-1
PSYCHOLOGICAL ADAPTATION
•Chronic distress •Negative affect •Social Adversity
CANCER PATHOGENESIS •Apoptosis/Anoikis •Angiogenesis •Growth & Metastasis
BIOBEHAVIORAL PROCESSES
•SNS Activation
•HPA dysregulation
•Inflammation
•Cellular Immune Suppression
Type I IFN
PSY INTERVENTION •Cognitive
•Appraisals •Coping
•Behavioral •Relaxation •Health behaviors
•Interpersonal •Assertiveness •Anger Mgmt •Social Support
CLINICAL OUTCOMES
•Recurrence •Mortality •Co-Morbidity
Antoni (2013). Brain, Behavior and Immunity.

Model’s Implications in Breast
Cancer
• Individual Differences in Psy Factors may contribute to
stress adaptation during the cancer experience
• Adaptation may accompany neuroendocrine changes
• Neuroendocrine changes transcriptional changes in
circulating immune (stromal) cells that could interact with
tumor to promote disease progression
• Implication: If so, can we facilitate adaptation early in the
disease process via psychosocial intervention to influence
circulating immune cells and ultimately clinical disease
course?
Gaps Remaining
• Integrating Changes in Psychological and
Physiological Adaptation with Longer-Term
Clinical Outcomes
• Identifying Intervention Moderators?
• Best Timing for Delivering CBSM in the
context of care?
• Briefer Forms Effective?
• What are essential ingredients?
• Alternative Methods Effective for
Delivering to Underserved Populations?

Gaps Remaining
• Integrating Changes in Psychological and
Physiological Adaptation with Longer-Term
Clinical Outcomes
• Identifying Intervention Moderators?
• Best Timing for Delivering CBSM in the
context of care?
• Briefer Forms Effective?
• What are essential ingredients?
• Alternative Methods Effective for
Delivering to Underserved Populations?

Long-Term Study: Aim 1
• Examine whether women with breast
cancer assigned to the 10-week CBSM
group differ from those in the 1-day
psycho-educational control group on
psychological status at 5year follow-up:
– Depression
– Vigor and fatigue
– Social disruption

CBSM and depression: long-term
(Stagl et al., 2013, SBM)
0 2 4 6 8 10 12
CBSM
Control
9.53
11.7
Differences in Depression on CES-D in 5-year follow up of
Breast Cancer Survivors
*
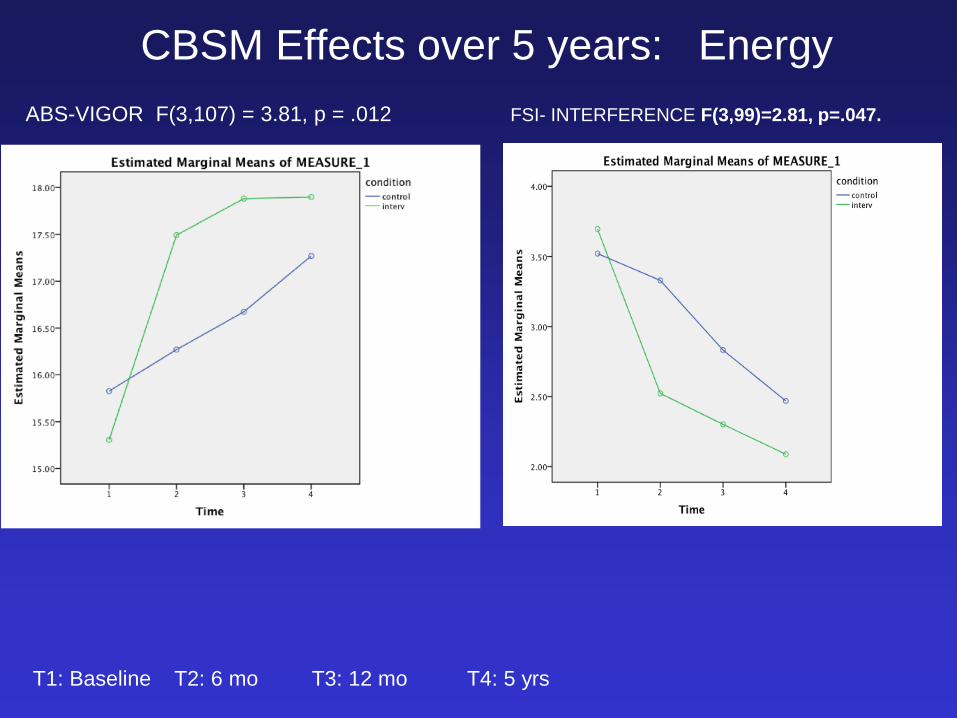
CBSM Effects over 5 years: Energy
ABS-VIGOR F(3,107) = 3.81, p = .012 FSI- INTERFERENCE F(3,99)=2.81, p=.047.
T1: Baseline T2: 6 mo T3: 12 mo T4: 5 yrs

SIP-RECREATIONS /PASTIMES F(3,105) = 3.14, p = .030
CBSM Effects over 5 years:
Social Disruption
T1: Baseline T2: 6 mo T3: 12 mo T4: 5 yrs

12 Month Pre-post CBSM Chg Predicts 5yr Status
• Greater 12mo change 5yr Outcome
– ABS-NA, ABS-PA, FSI-fatigue, FACT, PM cort, IFN-g - CES-D ABS Depression
– ABS-NA, BS-PA, FACT, leukocyte pro-inflamm gene express1 - FSI-fatigue
– ABS-NA, ABS-PA, PSQI, leukocyte pro- inflamm/pro-met2 - ABS-Vigor
– ABS-NA, ABS-PA - ABS-PA
1greater 12-mo reductions in pro-inflammatory [cytokine and chemokine) leukocyte gene expression
(e.g., TNF-a, IL-1b) predicted greater 5-yr ABS vigor (b = -.35) and ABS affect balance (b = -
.44), and less FSI fatigue disruption (b = .40).
2greater 12-mo reductions in MMP-9 and LMNA gene expression related to greater 5-yr ABS-Vigor
and greater emotional well-being (b = -.41 to -.65).
Findings held controlling for covariates (e.g., sociodemographic, adjuvant treatment).

Long-Term Study: Aim 2
• Examine whether women with breast cancer assigned to the 10-week CBSM group differ from those in the 1-day psycho-educational control group on clinical disease endpoints at 8-15 year follow-up:
– disease free interval
– breast cancer specific mortality
– all-cause mortality

Methods
Sample:
• 240 women post-surgery for non-metastatic stage 0-IIIb breast cancer accrued between 1998-2005.
• Randomized to 10-week group based Cognitive-Behavioral Stress Management Intervention (CBSM) or a 1-day Psycho-educational Control Seminar (PE)
• CBSM =120; PE = 120
• Currently 8-15 years post study enrollment
• Tumor Registry link and Chart Reviews ongoing
Gaps Remaining
• Integrating Changes in Psychological and
Physiological Adaptation with Clinical
Outcomes
• Identifying Intervention Moderators?
• Best Timing for Delivering CBSM in the
context of care?
• Briefer Forms Effective?
• What are essential ingredients?
• Alternative Methods Effective for
Delivering to Underserved Populations?

Identifying Intervention Moderators?
• Consider CBSM effects in context of:
– Person (ethnicity, SES, age, personality, social
context)
– Treatment (surg type and adjuvant)
– Disease (e.g., use Tissue Bank to measure
genomic, hormonal and immune markers)
• Clinicopathological: tumor sz, nodal status, grade, LVI tumor
lymphatic vessels and ER/PR status
• Tissue-derived: p27, pai-1, VEGF, IGF-1

DX Surgery
Specimen Repository
Core
•Tissue
•Blood
•History
Informed
consent
experimental control
(2-8 weeks) Group start T1 Randomize
Study Timeline Prior to the
Start of Intervention
prog. markers cells serum clinico-path.

Gaps Remaining
• Integrating Changes in Psychological and
Physiological Adaptation with Clinical
Outcomes
• Identifying Intervention Moderators?
• Best Timing for Delivering CBSM in the
context of care?
• Briefer Forms Effective?
• What are essential ingredients?
• Alternative Methods Effective for
Delivering to Underserved Populations?

Does Timing Within Treatment
Matter?
Can Stress Management Intervention Facilitate
Positive Adjustment after Adjuvant Therapy
for Breast Cancer has ended?
NCI grant P50CA84944. M. Antoni, P.I.
Examining the effects of CBSM at 3 - 24
months after adjuvant therapy has been
completed

Assessment Time Points
T1
surgery
T4
1 -2 year post surgery
T3 T2
2-8 wks
post
B SMART-10 wks.
3 months
post
6 months post

Testing Timing: Can Stress Management
Intervention Facilitate Positive Adjustment 3 – 24
months after Adjuvant Therapy for Breast Cancer
has ended?
Outcomes Grp X Time
PSYCHOSOCIAL
Increased Benefit Finding p = .046 Increased Post traumatic Growth (PTGI) p = .006 Increased Spirituality p = .020
Increased FACT-B p = .080
PHYSIOLOGICAL
Decreased Urinary Free Cortisol p = .048 Increased NKCC p = .031
Intervention Components
CBSM-specific
Relaxation confidence p = .001
Tension awareness p = .057
Non-CBSM –specific
Connection w/other CA pts p = .027
NCI CA84944-P50 M. Antoni, P.I.

Effects of CBSM in BRCA: Is timing important?
Physiol Post-surg (101) Post-surg (199) Post-Adj (126)
Cortisol Y Y Y
NK/LAK Y Y
LPR Y
TH1 cyto Y
Psych
Neg Mood Y Y
Pos Mood/BF Y Y Y
Fatigue Y
QOL/sleep Y Y Antoni et al. 2001 Antoni et al. 2006 a,b;
2009; Phillips et al.,
2008
Ironson et al., 2004
Gaps Remaining
• Integrating Changes in Psychological and
Physiological Adaptation with Clinical
Outcomes
• Identifying Intervention Moderators?
• Best Timing for Delivering CBSM in the
context of care?
• Briefer Forms Effective?
• What are essential ingredients?
• Alternative Methods Effective for
Delivering to Underserved Populations?

Other Ongoing Work In CBSM
• Can CBSM be delivered effectively:
– In abbreviated components?
– In the community?
– In different languages?
– Over the telephonevideophoneTablet/Web
Dismantling CBSM into its Active
Components
• Observations of Prior CBSM groups
– Attendance: effects for [5] = [10] > [1 – 2] sessions
– Mediators: Relaxation Confidence, Cognitive appraisal skills and
Emotional Expression
• Ongoing NCI Trial (2R01 CA064710 Antoni, PI) “Dismantling Study”
– 5wk CBT only (group)
– 5wk Relaxation Training only (group)
– 5wk Health Education (attention) only (group)

5-Week Intervention
W
k
RT
1 PMR-7
2 PMR-4, Beach Scene Imagery
3 Passive PMR, Special Place
Imagery
4 Light Imagery
5 Meditation
Streamlined Interventions
5-Week Intervention
Wk CBT
1 Stress Symptoms & Appraisals
2 Distortions & Reappraisals
3 Coping, Acceptance/Softening
4 Social Support & Anger
Management
5 Assertiveness & Review
5-Week Control Group
EE
Info about BCa, treatment, side effect management, healthy lifestyle, & Q.O.L.
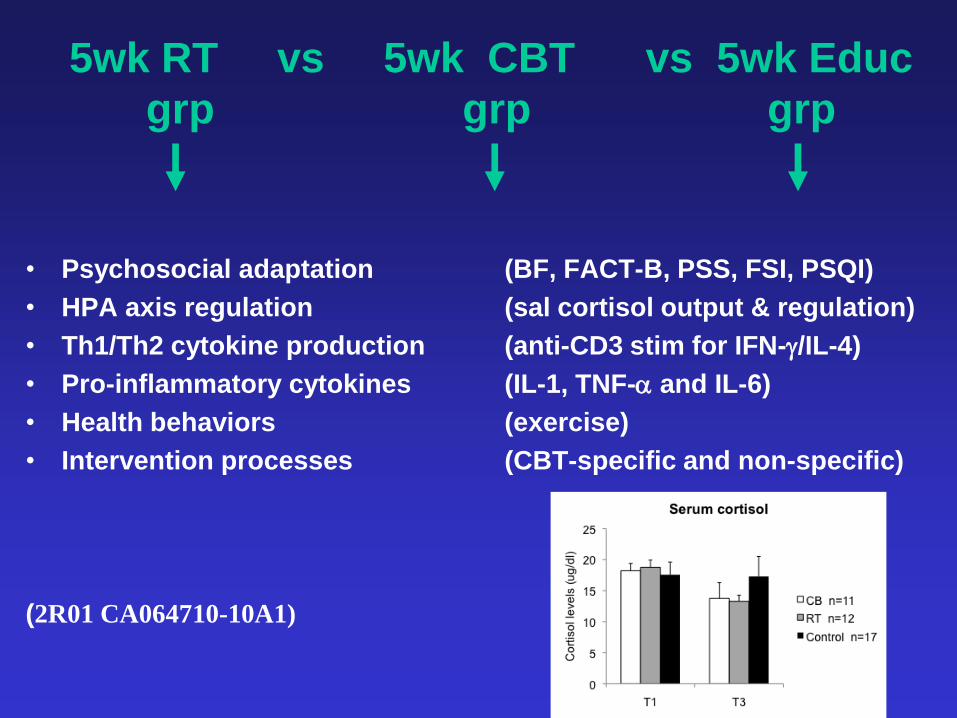
5wk RT vs 5wk CBT vs 5wk Educ
grp grp grp
• Psychosocial adaptation (BF, FACT-B, PSS, FSI, PSQI)
• HPA axis regulation (sal cortisol output & regulation)
• Th1/Th2 cytokine production (anti-CD3 stim for IFN-g/IL-4)
• Pro-inflammatory cytokines (IL-1, TNF-a and IL-6)
• Health behaviors (exercise)
• Intervention processes (CBT-specific and non-specific)
(2R01 CA064710-10A1)

Specificity of Effects after 5-wk Training
Period
RT CB EE Target: Tension/Arousal Cognitive/Affective Health Information
Effects:
• Anxiety Depression/Neg Affect None
ABS Anx -ABS Dep None
Relaxation Efficacy -FACT Emot Well-being None
• Recreations Pastimes (SIP) Intrusive Thoughts (IES) None
-Hobbies/Social Activities -Cancer-related thts
• Positive Mood Positive Mood None
– Happiness -Happiness
– Joy -Joy
– Affection -Affection
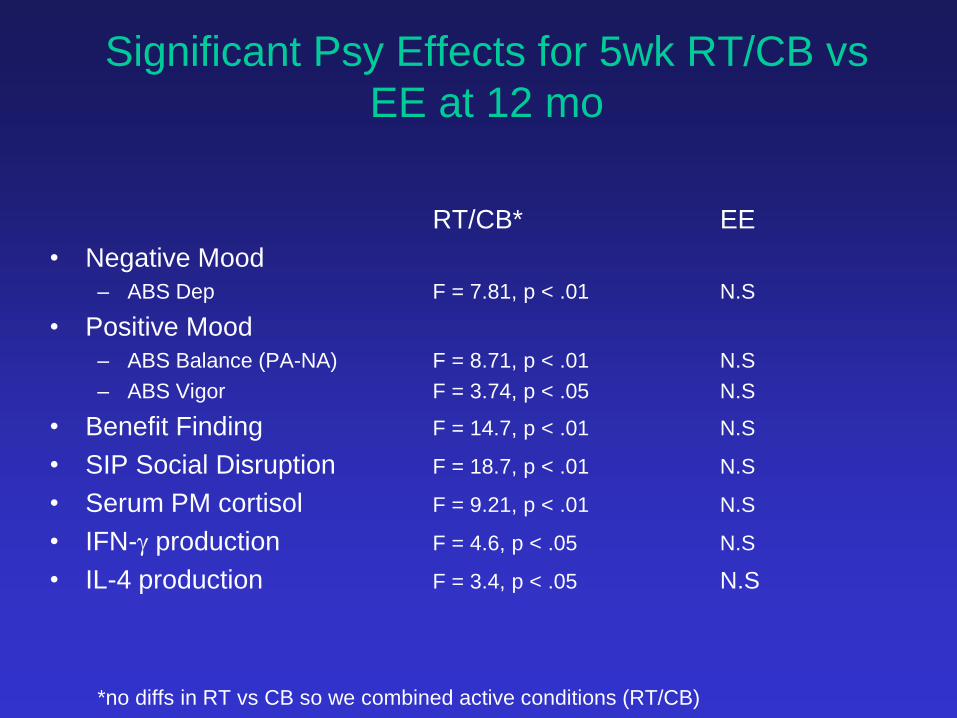
Significant Psy Effects for 5wk RT/CB vs
EE at 12 mo
RT/CB* EE
• Negative Mood
– ABS Dep F = 7.81, p < .01 N.S
• Positive Mood
– ABS Balance (PA-NA) F = 8.71, p < .01 N.S
– ABS Vigor F = 3.74, p < .05 N.S
• Benefit Finding F = 14.7, p < .01 N.S
• SIP Social Disruption F = 18.7, p < .01 N.S
• Serum PM cortisol F = 9.21, p < .01 N.S
• IFN-g production F = 4.6, p < .05 N.S
• IL-4 production F = 3.4, p < .05 N.S
*no diffs in RT vs CB so we combined active conditions (RT/CB)

Significant Psy Effects for 5wk RT/CB vs
5wk EE vs 10wk CBSM @ 12 mo
5wks 10wks
RT/CB EE CBSM
• Negative Mood
– ABS Dep ** N.S ***
• Positive Mood
– ABS Balance ** N.S ***
– ABS Vigor * N.S ***
• Benefit Finding ** N.S ***
• SIP Soc Disruption ** N.S ***
• Serum PM cortisol ** N.S **
• IFN-g production * N.S **
Combined active 5wk conditions (RT/CB), 5wk Enhanced Health Education (EE), 10wk Cognitive
Behavioral Stress Management (CBSM). ***p < .001 **p < .01 *p < .05 on RANOVAs
Delivering CBSM in the Community: Project CARE (Lechner, P.I., Antoni, co-PI, Kobetz, co-PI) NCI R01CA131451
• Minority Breast Cancer Patients underserved and understudied
• Partnered with Community Organizations in Overtown and other Miami regions of minority and underserved populations
• Formative research to tailor CBSM-based intervention
• Community-Based Participatory Research methods used to train assessors to collect physiologic and psychosocial measures in home
• CBSM groups conducted in community (church & community centers)
• Pre-post-F/U of psychosocial, physiological and symptom cluster outcomes – PSS, Mood, QOL
– Fatigue, sleep, symptoms
– Salivary cortisol, HRV

Can You Hear Me Now?: Can CBSM groups be Delivered Over
the Phone?
• Patients with advanced disease not able to attend groups
• Some patients have transportation issues
• Some prefer to maintain anonymity
• Worked with Psychiatry and Engineering to develop Telecare-based technology with conference calling to allow access to CBSM via phone: “TELEPHONE GROUPS”

E.g., Patients Participate in “Tele-Groups” at Home
• 10 one-hour modules delivered in conference call on CTIS or cell phone
• Each module contains relaxation and cognitive-behavioral stress reduction (CBT) components
• System provides menus for review of 10 CBT modules during and after session
• Menu also allows user to play back audio of relaxation exercises
• The system collects real-time usage data on a per call basis to measure “dose” received
• Other Menu buttons: – Calling group leader or members – Contacting PCa support organizations

Communication Technology On
the Horizon
• Using Videophone Technology/Internet to deliver
CBSM in group-based form at home to patients (and
partners) who cannot attend clinic-based groups due
to advanced disease, mobility issues/personal
preference:
– Chronic Fatigue Syndrome
1R01NS072599-01
-Advanced Prostate Cancer
NCI R01

ANSWER CALL Press this button to answer an incoming call or to end video.
FULL SCREEN Press this button to expand the video to full screen.
GO BACK Press this button to return to the previous screen.
HELP Press this button to bring up the help menu with topics you can view.
NO MIC Press this button to turn off the microphone. Others will not hear you.
NO VIDEO Press this button to turn off the video camera. Others will not see you.
SEE YOURSELF Press this button to view yourself on screen and adjust the image.
SERVICES Press this button to bring up the system menu with topics you can view.
VOLUME Press this button to adjust the volume. Clicking on the plus side of the
button increases the volume. Clicking on the minus side decreases it.

CBSM Videophone
Programming
• CBSM Modules 1 – 10 Video Reviews
• Relaxation and Interpersonal Skills
Video Enactments
• Expert Videos
• Daily Stress Ratings Prompting
• System captures usage (adherence and
dosage data)
• Prototype for Web-Based (SKYPE)
• Transitioning from Videophone to Tablet

Demonstration Videos
Assertiveness
Deep Breathing Special Place
Imagery
Progressive Muscle
Relaxation
Mindfulness
Meditation
Ongoing and Future Work In CBSM
• Can CBSM be delivered effectively:
– In abbreviated components?
– In the community?
– In different languages?
– Over the telephonevideophoneTablet/Web

Stress Management Studies at UM (1986-
2013)
HIV
MSM Hetero
Men
Inner-City
Women
Asymp
Dx Notif
Symp
Pre-HAART
HAART
Asymp. HIV+
AIDS
HAART
Eng
Lang
Spa
Lang
Spa
Lang
Eng
Lang
HPV +
SIL
Post-
Adj
Stage I-IIla
BRCA
Pre-
Adj
Stage I-II
Stage I-IIIa
Dismantle
CBSM
Abbrev
CBSM
PRCA
Post
Surg
Post
Radiation
Advanced
Disease
Eng
Lang
Spa
Lang
Eng
Lang
Spa
Lang
Eng
Lang
CFS
SMART
ENERGY
TELE
CBSM
TELE-
CBSM Community-based
CBSM

1970s/80s 1990s 2000s 2010s
Phase 1: Stress/Stress Management Effects on
QoL in Cancer Patients
His
tory
of
Bio
beh
avio
ral
Res
earc
h
Phase 2: Stress/Stress Mgmt Effects
on “Adaptation” to Medical Treatment
Phase 3: Stress/Stress Mgmt
Effects on Neuroimmune
Indicators of Unknown Duration
Phase 4: Stress/Stress
Mgmt Effects on Molecular
Interactions/ Processes
Controlling Cell Function
Over Longer Periods?
Developing and Testing Psychosocial Interventions in
Clinical Disease: “Drilling Down and Reaching Out”
• Combining “Mechanism Research” with “Clinical Efficacy Research” is Efficient Science
• Using microarray and bioinformatics technology we now see that Stress Management may produce molecular “footprints” in leukocytes pursuant to changes in neuroendocrine regulation over sustained periods
• These changes portend improved ability to respond to stress and optimize quality of life across the cancer continuum over the long term
• Using Community-based Approaches and Telecommunication Technology Reaches Populations Most in Need
Acknowledgments NCI
R01 CA64710
NCI R01CA131451
P50CA84944
Sylvester Cancer Center
• Robert Derhagopian, MD
• Frederick L. Moffat, MD
• Tammy Enos Sifre, PhD
• Kristin Kilbourn, PhD
• Susan Alferi Fox, PhD
• Patti Arena, PhD
• Jessica Lehman, PhD
• Amy Boyers, PhD
• Jennifer Culver, PhD
• Susan Yount, PhD
• Suzanne Harris, PhD
• Dean Cruess, PhD.
• Stefan Gluck, MD, Ph.D.
• Bonnie McGregor, PhD
• Alicia Price, PhD
• Vida Petronis, PhD
• Roselyn Smith-Gonas, PhD
• Kurrie Wells, MS
• Cassy Vaughn, MS
• Kenya Urcuyo, MS
• Sophie Guellati, PhD
• Sarah Wimberly, Ph.D.
• Aisha Kazi, Ph.D.
• Kristin Phillips, Ph.D.
• Janny Rodriguez, MEd
• Nicole Whitehead, Ph.D.
• Jarrard Goodwin, M.D.
• Bonnie B. Blomberg, Ph.D., Microbiology/Immunology, University of Miami School of Medicine, Miami
• Suzanne Lechner, Ph.D., Psychiatry, University of Miami School of Medicine, Miami
• Charles S. Carver, Ph.D., Psychology, University of Miami, Coral Gables
• Susan Lutgendorf, PhD, Psychology, University of Iowa, Iowa City, IA
• Steven W. Cole, PhD, Medicine, UCLA, Los Angeles, California