the effects of vibration on muscles in the neck and …141762/fulltext01.pdf · the effects of...
TRANSCRIPT

UMEÅ UNIVERSITY MEDICAL DISSERTATIONS New Series No.1135 – ISSN 0346-6612 – ISBN 978-91-7264-506-6
From the Department of Community Medicine and Rehabilitation Physiotherapy, Umeå University, Sweden
The effects of vibration on muscles in the neck and upper limbs
With focus on occupational terrain vehicle drivers
Charlotte Åström
Umeå 2008

Copyright © Charlotte Åström New Series No.1135 – ISSN 0346-6612 – ISBN 978-91-7264-506-6
Printed in Sweden by Arkitektkopia, Umeå 2008


CONTENTS ABSTRACT .......................................................................... 7
SVENSK SAMMANFATTNING ............................................ 8
ORIGINAL PAPERS ........................................................... 11
INTRODUCTION ................................................................. 12 Work-related musculoskeletal disorders ......................................................... 12 Vibration ............................................................................................................ 12
Exposure in working life ................................................................................ 12 Definition ....................................................................................................... 13 Physiological effects of vibration ................................................................... 14
Terrain vehicles ................................................................................................. 15 Muscle physiology and electromyography ...................................................... 16
The skeletal muscle ........................................................................................ 16 Muscle fatigue ................................................................................................ 17 Electromyograpy ............................................................................................ 17
Vibration exposure and muscle response ........................................................ 18 Rationale for the thesis ..................................................................................... 22 AIMS OF THE THESIS ....................................................... 23
METHODS .......................................................................... 24 Subjects .............................................................................................................. 24
Paper I ............................................................................................................ 24 Paper II and III ............................................................................................... 26 Paper IV .......................................................................................................... 27
DATA COLLECTION METHODS ................................................................ 27 Questionnaire (paper I) ................................................................................... 27 EMG (paper I-IV) ........................................................................................... 28
Vibration exposure ............................................................................................ 29 Paper II and III ............................................................................................... 29 Paper IV .......................................................................................................... 30
Experimental procedure ................................................................................... 31 Paper II and III ............................................................................................... 31 Paper IV .......................................................................................................... 32
Statistical methods ............................................................................................ 34 Paper I ............................................................................................................ 34 Paper II ........................................................................................................... 34 Paper III .......................................................................................................... 35 Paper IV .......................................................................................................... 35

Ethical approval ................................................................................................ 35 RESULTS ........................................................................... 36 Prevalence of hand-arm vibration syndrome and musculoskeletal disorders (Paper I) ............................................................................................................. 36
Hand-arm vibration syndrome ........................................................................ 36 Musculoskeletal disorders .............................................................................. 37 Exposure time ................................................................................................. 39
Fatigue development (Paper II) ....................................................................... 41 Muscle activity during vibration (Paper III) .................................................. 43 Combination of hand-arm vibration and whole-body vibration (Paper IV) 44 Gender differences (paper II-IV) ..................................................................... 49 DISCUSSION ...................................................................... 50 Results ................................................................................................................ 50
Hand-arm vibration syndrome and musculoskeletal disorders in the neck and upper limbs ..................................................................................................... 50 Vibration and fatigue development ................................................................ 51 Changes in muscle activity during vibration exposure ................................... 52 Combination of HAV and WBV .................................................................... 53 Gender effects................................................................................................. 55
Methodological considerations ......................................................................... 56 Epidemiology ................................................................................................. 56 Experimental design ....................................................................................... 56 External validity ............................................................................................. 58
Implications for further research .................................................................... 59 CONCLUSIONS .................................................................. 60
ACKNOWLEDGEMENTS ................................................... 61
REFERENCES .................................................................... 64


ABSTRACT
Introduction: Occupational drivers of terrain vehicles are exposed to several risk factors associated with musculoskeletal symptoms in the lower back as well as in the neck and upper limbs. Vibration has been suggested to be a main risk factor. These drivers are exposed to both whole-body vibration (WBV) and hand-arm vibration (HAV). Aim: This study establishes the association between driving terrain vehicles and musculoskeletal disorders (MSDs) in the neck and upper limbs as well as hand-arm vibration syndrome (HAVS). In addition, this study examines the effect on muscles in the neck and upper limbs of the type of vibration exposure that occurs in occupational driving of terrain vehicles. Methods and results: In Paper I, a cross-sectional questionnaire study on occupational drivers of terrain vehicles, increased Prevalence Odds Ratios (POR) were found for numbness, sensation of cold and white fingers (POR 1.5-3.9) and for MSDs in the neck (POR 2.1-3.9), shoulder (POR 1.8-2.6) and wrist (POR 1.7-2.6). For the shoulders, neck and elbow, there appears to be a pattern of increased odds with increasing exposure time. In Paper II, an experimental study on the trapezius muscle, which included 20 men and 17 women, the mean frequency of the electromyography signal (EMGMNF) decreased significantly more in a three minute sub-maximal contraction without vibration (-3.71Hz and -4.37Hz) compared to with induced vibration (-3.54Hz and -1.48Hz). In Paper III, a higher initial increase of the mean of the root-mean-square of the electromyography signal (EMGRMS) was seen in a three minute sub-maximal contraction with vibration exposure compared to without vibration (0.096% vs. 0.045%). There was a larger mean EMGMNF decrease for NV compared to V in the total three minutes, and a larger decrease also in the first time period was seen for the NV compared to V. A small gender effect was also noticed. In Paper IV, the combination of HAV and WBV was studied in laboratory settings and resulted in a higher trapezius EMGRMS compared to the HAV and WBV separately. Conclusion: Occupational drivers of terrain vehicles are likely to experience symptoms related to HAVS and musculoskeletal symptoms in the neck and upper limbs. Local vibration does not seem to have any negative acute effects on trapezius muscle fatigue. Vibration exposure seems to cause an initial increase in muscle activity in the trapezius that could be related to recruitment on new motor-units. A combination of HAV and WBV causes a larger muscular demand on the trapezius muscle. Keywords: Electromyography, drivers, hand-arm vibration, trapezius, whole-body vibration.
7
SVENSK SAMMANFATTNING Yrkesförare av terränggående fordon, såsom skogsmaskiner, snöskotrar och pistmaskiner utsätts för flera riskfaktorer relaterade till besvär i nacke och armar och undersökningar har även visat att de har dessa besvär i hög utsträckning. En känd riskfaktor för besvär i muskler och leder är exponering för vibrationer. Terrängfordonsförare utsätts dels för vibrationer i händerna från styrdon, sk hand-armvibrationer, men också vibrationer från sätet, sk helkroppsvibrationer. Denna dubbla exponering skulle kunna bidra till de utbredda besvären i nacke och skuldra hos denna yrkesgrupp. Det är känt att vibrationer kan öka muskelaktivitet genom en reflexrespons. Denna ökande belastning på muskulaturen har föreslagits kunna bidra till besvär. Syftet med denna studie var därför att se om det finns något samband mellan terrängfordonskörning och nack- och skulderbesvär, samt vibrationsrelaterade besvär i händer och armar. Syftet var också att i experimentella studier undersöka vibrationers akuta effekt på nackmuskulaturen. Dels hur det påverkar muskeltrötthet och muskelaktivtet, men även hur kombinationen av vibrationer från händer och säte påverkar muskelaktivteten. Resultaten visar att förare av terränggående fordon har en ökad risk för besvär i nacke, skuldror och handleder, samt en ökad risk för vissa vibrationstypiska besvär i händerna såsom domningar, köldkänsla och vita fingrar. De experimentella studierna visade att vibrationer inte ökar på muskeltrötthet under en tre-minutersperiod. Däremot finns det finns vissa skillnader i hur muskelaktiviteten ändras under denna tre-minutersperiod. Då nackmuskulaturen under låg belastning utsätts för vibrationer, ses en tidig ökning av muskelaktiviteten som sedan avtar, medan om samma arbete utförs utan vibrationer så ser ökningen mer jämn ut över tid. En kombination av hand-armvibrationer och helkroppsvibrationer ger upphov till en ökad muskelaktivitet jämfört med hand-armvibrationer och helkroppsvibrationer separat. Dessa resultat visar att lokala vibrationer på kort sikt påverkar muskelaktiviteten, men de verkar inte ha någon negativ effekt muskeltrötthet i nacken. Däremot styrker de hypotesen att dessa förare utsätts för en belastande kombinerad vibrationsexponering som på lång sikt kan vara relaterad till den höga förekomsten av muskulära besvär i nacke och skuldror.
8

ABBREVIATIONS COMB1 HAV+WBV in phase COMB2 HAV+WBV, 180° phase shifted EMG Electromyography EMGMDF The median frequency of the electromyography signal EMGMNF The mean frequency of the electromyography signal EMGRMS The root-mean-square of the electromyography signal ∆EMGMNF The difference between EMGMNF before and after the three minute
sub-maximal trapezius contraction ∆EMGRMS The difference between EMGRMS before and after the three minute
sub-maximal trapezius contraction HAV Hand-arm vibration HAVS Hand-arm vibration syndrome Hz Hertz MSDs Musculoskeletal disorders MU Motor unit MVC Maximum voluntary contraction NV No-vibration condition NV1 First measurement without vibration NV2 Second measurement without vibration POR Prevalence odds ratio RMS Root-mean-square SD Standard deviation SE Standard error TVR Tonic vibration reflex V1 First measurement with vibration
9
V2 Second measurement with vibration WBV Whole-body vibration
10

11
ORIGINAL PAPERS
The thesis is based on the following papers: I. Åström C, Rehn B, Lundström R, Nilsson T, Burström L, Sundelin G. Hand-arm vibration syndrome (HAVS) and musculoskeletal symptoms in the neck and the upper limbs in professional drivers of terrain vehicles—A cross sectional study. Appl Ergon. 2006; 37(6):793-9. II. Åström C, Lindkvist M, Burström L, Sundelin G, Karlsson JS. Changes in EMG activity in the upper trapezius muscle due to local vibration exposure. J Electromyogr Kinesiol. 2007, Epub ahead of print, Dec. III. Åström C, Lindkvist M, Burström L, Karlsson JS, Sundelin G. Trapezius muscle activity during simultaneous exposure to local vibration and static muscle load – a study of acute effects. In manuscript. IV. Åström C, Sundelin G, Karlsson JS, Lindkvist M, Burström L. The effect of combined hand-arm and whole-body vibration exposure on muscular activity in neck, lower back and arms. Submitted. Reprints were made with the kind permission of the publishers.

Introduction ______________________________________________________
INTRODUCTION
Work-related musculoskeletal disorders The high prevalence of work-related musculoskeletal disorders
is one of the most common and expensive public health issues in North America and Europe (1-3). The prevalence has intensified since the mid 20th century. Similar symptom patterns have been given different names besides the term work-related musculoskeletal disorders, for example work-related myalgia, neck-shoulder myalgia and low back pain (4). For a long time, low back pain has been studied, but lately the issue of the increasing number of work-related neck and shoulder complaints have been given more attention (5, 6). The general term musculoskeletal disorders (MSDs) are commonly used in the research field, and henceforth this term will be used in this thesis.
Prevalence of neck pain has been reported to be around 14%-48% in the industrial world (5-10). In 2006, 2.7% of the Swedish men and 5.7% of the Swedish women reported that their work had caused neck pain. The prevalence of work-related shoulder and arm pain was 6.1% for men and 9.8% for women (10). Several studies have investigated risk factors for developing neck and upper limb disorders. A review by Larsson et al. summarized the results from the six last years (11). Gender is considered an important factor; women report a higher prevalence of pain in the upper limbs and in the neck, compared to men (5, 11, 12). Age and smoking are additional risk factors for developing MSDs in the neck and upper limbs. Physical risk factors that have been linked with pain in the neck and shoulders are repetitive movements, high force demands, work posture such as duration of constrained postures, as well as awkward or extreme postures, and exposure to vibration (11). Vibration Exposure in working life
An estimated 480 000 workers (430 000 men and 50 000 women) between the ages of 16-64 were exposed to vibration as a result of their occupation in Sweden during 2005; 7.5% used vibrating hand-held tools during at least ¼ of their working time, and 7.4% were exposed to whole-body vibration (WBV) during at least ¼ of
12

Introduction ______________________________________________________
their working time (12). Approximately 1 million hand-held tools and 800 000 vehicles are used in different professions in Sweden (13). Mechanics and construction workers are examples of occupational users of hand-held tools. Studies have shown a relationship between occupations with hand-arm vibration (HAV) exposure and musculoskeletal symptoms in the neck and upper limbs (14-17). Relationships between occupations with WBV exposure and musculoskeletal symptoms in the neck and upper limbs have also been found (18-20).
Definition Vibration is an oscillatory motion and by definition, it is not a
constant motion but alternately greater and less than some average value. The magnitude of the vibration is determined by the extent of the oscillation, and the frequency of the vibration in determined by the repetition rate of the cycles of oscillation (21). Vibration can be divided into deterministic and random vibration. Random (stochastic) vibration can only be characterized as having some statistical properties, whereas deterministic vibration, such as sinusoidal vibration, can be predicted from knowledge of previous oscillations. Sinusoidal vibration can be used to study the effects of one single frequency of motion, a characteristic that makes it suitable for laboratory studies. Vibration is usually subdivided in local vibration and whole-body vibration (WBV). Local vibration is characterized by vibration transmitted from a vibrating surface to a part of the body. This exposure is usually referred to as hand-arm vibration (HAV) or hand-transmitted vibration since it most commonly occurs with the use of vibrating hand-held tools (22). Typically, WBV occurs when the whole body is supported by a vibrating surface in turn causing the whole body to be affected (21).
The magnitude of a vibration can be expressed in several ways. It can be quantified as the displacement between the peak movement in one direction and the peak movement in the opposite direction (peak-to-peak displacement) or as velocity. However, most standards require that the magnitude of vibration be expressed in terms of acceleration (m/s2). The acceleration can be expressed in terms of peak-to-peak or the peak acceleration, but the measure that is more commonly used is the root-mean-square (RMS) value - the square root of the average value of the square of the acceleration (22).
13

Introduction ______________________________________________________
The frequency of a vibration is expressed as the number of oscillations per second measured as Hertz (Hz). The simplest type of vibration is the sinusoidal vibration because it contains only one frequency. Different vibration frequencies affect the human body in different ways. According to the standards ISO 2631-1 (23) and ISO 5349-1 (24) analysis of the influence on health of WBV should be performed within the frequency range 0.5-80Hz and for HAV within 5-1500Hz. The different frequencies are given different weights corresponding to the sensitivity of the human body (23, 24).
Physiological effects of vibration When a muscle is exposed to vibration, the vibration elicits a
reflex response - the tonic vibration reflex (TVR). This reflex is caused by a vibration induced stretch of the muscle spindle (25). This stretch can be produced by a local vibration to the muscle or tendon as well as from the relative movement of the human body during exposure to WBV. Vibration is transmitted through body parts, lower frequencies more so than higher. Certain vibration frequencies trigger the natural frequency of different body parts, a frequency that results in resonance. The resonance for the human spine has been reported to be 4.5-5.5Hz (26, 27), 1-1.4Hz and 9Hz for the head-neck complex (28) and 4-8Hz for the shoulders (29).
Circulation is also effected by vibration. Exposure to HAV, especially with higher frequencies, causes a vasoconstriction in the blood vessels and a reduction of peripheral blood flow (30). Vibration exposure can also produce cardiovascular effects such as heart-rate variability (31, 32). Several epidemiological studies have shown a relationship between working with vibrating hand-held tools and acute and chronic vascular and neurological symptoms in the hands (22, 33-35). The exposure of the hands and arms to vibration can cause both reduced blood circulation to the fingers and attacks of blanching of one or several fingers. This condition is usually referred to as vibration-induced white finger. Hand-arm vibration syndrome (HAVS) also includes symptoms such as tingling, numbness and muscle and joint symptoms. At first these symptoms are acute and reversible, but with prolonged exposure they can become chronic. The vascular symptoms have been studied the most, but neurological and musculoskeletal symptoms are also included in the HAVS. Biopsy studies have shown changes in the muscular tissue after exposure to vibration both in rats and in humans (36). The HAV does not only
14

Introduction ______________________________________________________
seem to affect the muscles in the hand; pain in the neck, shoulder, elbow and wrist is also associated with working with vibrating hand-held tools (14, 16, 17).
Whole-body vibration (WBV) can affect the human body in several different ways. Motion sickness and discomfort are common health effects (21). WBV also has effects on the cardiovascular function, respiratory system, sensory responses and the skeletal system (22). Increased prevalence of musculoskeletal symptoms in the neck, shoulder, and lower back have been reported in several occupations that include exposure to WBV in the daily routine. Truck drivers have been reported to have high prevalence of lower back, neck and shoulder symptoms (19, 37). Okunribido et al. show that numerous groups of occupational drivers have a high prevalence of low back pain (38). Bus drivers have a prevalence of neck pain as high as 53%, and shoulder pain up to 42% (18).
Terrain vehicles
Whole-body vibration exposure is particularly predominant in vehicles. Drivers of terrain vehicles are exposed to WBV in their everyday work routine and they have a high prevalence of musculoskeletal disorders (20). Terrain vehicles operate in off-road environments and examples of vehicles are snowmobiles, snow-groomers, four wheelers and forest machines such as forwarders and harvesters. There are about 21 000 snowmobiles and 10 000 forest machines used professionally in Sweden, in occupations associated with for example forestry, reindeer herding and alpine ski resorts (13). Occupational drivers in general report a high prevalence of musculoskeletal disorders. In Sweden, 21.7% of occupational drivers reported work-related symptoms and 4.1% had been on sick leave pension for more than five weeks (10). Drivers of terrain vehicles are exposed to high levels of vibration caused by the irregular terrain that they operate in. Shocks and jolts, or short high amplitude vibrations, are a common exposure for these drivers. They are also exposed to both WBV from the seat and HAV from the steering devices in the vehicles. In addition to vibration exposure, drivers of terrain vehicles have several other potential risk factors in their daily routine, such as poor ergonomics, extensive working hours, long-term sitting and psychosocial load.
15
Introduction ______________________________________________________
Muscle physiology and electromyography
The skeletal muscle The main tasks for human skeletal muscles are to produce
movements, to stabilize the body, to move substances within the body and to produce heat. The muscle cell, usually referred to as muscle fibres, consists of myofibrils, which are the contractile element of the skeletal muscle. The myofibrils contain three types of even smaller structures called filaments (myofilaments). The filaments can be either thick or thin. Depending on whether the muscle is contracting or relaxing, the thick and thin filaments overlap one another. The overlapping of the filaments - i.e. the muscle contraction - occurs when the muscle fibres are excited by the central nervous system. Muscle fibres that are innervated by the same nerve fibre (axon) are called motor units (MU), and this is the smallest functional unit of a muscle (39). The number of motor fibres in a MU varies widely, but it has generally been agreed that muscles that are responsible for fine movements and adjustments (such as ocular muscles) have the smallest number of fibres per MU, while larger muscles, such as those in the limbs have larger MUs (40).
Muscle fibres are classified according to their structure and function. There are three general types of muscle fibres; Slow oxidative (type I), fast oxidative-glycolytic (IIA), and fast glycolytic (type IIB) fibres. The type I fibres have a small diameter and a slow contraction velocity. On the other hand, they are very resistant to fatigue. The type IIA are also resistant to fatigue, not to the same extent as the type I, but they have a fast contraction velocity. The type IIB fibres have the largest diameter and are easily fatigued. Their contraction is strong and rapid (39). To increase the muscle force, there are two processes involved: increasing the number of active MUs, which is called recruitment, and increasing the stimulation rate of the motor nerve. Larger MUs are recruited as the synaptic input increases in strength. This is called the Henneman’s size principle: the smaller MUs have lower thresholds and the larger MUs have higher thresholds (41). The smaller MUs do not only have fewer muscle fibres, but their muscle fibres are also smaller in size. The muscle fibre types increases in size, and are recruited in the following order: type I → IIA → IIB. They are de-recruited in the reverse order.
16

Introduction ______________________________________________________
Muscle fatigue Muscle fatigue might be related to the development of
discomfort and injuries in the musculoskeletal system (42-45). Several definitions for the term muscular fatigue exist, but one commonly used definition is that muscular fatigue is “an exercise-induced reduction in maximal voluntary muscle force” (46). Fatigue is usually divided into peripheral and central fatigue. Peripheral fatigue refers to the exercise induced processes leading to a reduction in force and occurs at or distal to the neuromuscular junction. This type of fatigue can be shown by a fall in the twitch or tetanic force produced by the peripheral nerve stimulation with the muscle being at rest. Central fatigue on the other hand refers to more proximal processes. It is usually this type of fatigue that is “an exercise-induced reduction in maximal voluntary muscle force”. The central fatigue can be demonstrated by an increase in the additional force provoked by nerve stimulation during a maximal voluntary contraction. If the nerve stimulation can produce this extra force, the conclusion is that some MUs were not recruited or were not firing fast enough. This superimposed twitch is a sign of central fatigue caused by central processes proximal to the site of motor axon stimulation (46).
Electromyograpy Electromyography (EMG) is a technique to visualize and
analyze the electrical signal derived from the MUs in the muscle when it contracts. This signal can be recorded using either needle EMG or surface EMG (47). With needle EMG, the needle electrode is penetrated through the skin and directly into the muscle. Needle EMG gives more detailed information regarding wave shape of MU’s action potential. Surface EMG electrodes are glued onto the skin which makes this method non-invasive. It gives more “global” information about the muscle and is composed of the summation of hundreds of contributions from the active MUs. Because each contribution is heavily filtered by the tissue between the sources and the electrodes, this method is only applicable on superficial muscles. The EMG signal can be described in different ways. A common parameter to describe the amplitude of the signal is the root-mean-square (EMGRMS) of the EMG signal. To describe the EMG signal in the frequency domain, the mean frequency (EMGMNF) or the median frequency (EMGMDF) can be used (40). EMG is a common method to
17

Introduction ______________________________________________________
use when evaluating possible muscular fatigue. A decrease in the EMGMNF or EMGMDF with a simultaneous increase in the EMGRMS indicates muscular fatigue (43, 48). The increase of the EMGRMS however, can be a more uncertain measure of fatigue, especially in ergonomic field studies, since it can also be due to an increased workload (49, 50). Three explanations to the changes in EMGRMS and EMGMNF have been presented: MU recruitment, MU synchronization and changes in the conduction velocity of muscle fibres. When using EMG indicators of fatigue, it is important to remember that it is only the electrical manifestations of fatigue that are presented, and not the direct measures of mechanical fatigue (the reversible reduction of the ability to generate mechanical force (50). Vibration exposure and muscle response
Some studies have examined the response in spinal muscles to vibration by means of EMG. The following paragraph is a summary of the results from these. For an overview, see Table 1.
It seems clear that seated WBV exposure increases the EMG amplitude, expressed as EMGRMS, in the erector spinae muscle. This has been shown for both lower frequencies from 0.3Hz to 10Hz (51, 52) as well as for higher frequencies (from 30Hz to 40Hz) (53). The EMGRMS seems to increase with increasing vibration magnitude (52, 54, 55). De Oliviera et al. (56, 57) studied EMG response in the back muscles during helicopter flights and did not find any increased muscle activity compared to static sitting or standing. Contrary to De Oliviera’s studies, Thuresson (54) found a 0.5-1% of maximum voluntary electrical activation increase in the upper neck muscles at frequencies around 5Hz for all head worn equipment and neck positions in helicopter pilots. For the lower neck muscles, the activity increased about 1% of maximum voluntary electrical activation at the same frequency when the head was in a flexed position.
Several studies have shown a relationship between sitting posture and EMG response in the spinal muscles when exposed to WBV (58-60). The results of the studies were unanimous: a bent forward posture gives the largest EMG amplitudes in the lumbar and thoracic back muscles during vibration exposure. This result however was not the case for the neck muscles which had increased muscle activity in all tested postures.
Timing of muscle responses to transients, or sudden increases in vibration acceleration, have been studied for the back muscles (58,
18

Introduction ______________________________________________________
61, 62). A non-linear increase of the internal load was predicted with rising amplitudes. The muscle response occurred right at the start and was within the range of stretch reflexes, and the muscle response occurred earlier with increasing amplitudes of the transients. Posture also affects the timing of the muscle response to the transient; a bent forward and an erect posture gave more pronounced responses (58). Some studies have presented a synchronization of muscle activity, which is related to the vibration frequency (52) as well as the sitting posture (59).
Hansson et al. (63) showed an increased development of fatigue in the erector spinae muscle in sitting subjects exposed to WBV. The exposure time was five minutes and was performed both with and without WBV exposure.
19

Introduction ______________________________________________________
20

Introduction ______________________________________________________
21

Introduction ______________________________________________________
22
In conclusion, most EMG studies have investigated back muscles, and most of the studies have only studied WBV. The few studies that have investigated the trapezius muscle activity presented an increased muscle activity that was not affected by alterations in posture. Rationale for the thesis
Occupational drivers of terrain vehicles are exposed to several risk factors related to the development of neck and upper limb disorders. Epidemiological studies have shown an increased prevalence of musculoskeletal disorders in this group. However, the relation between driving terrain vehicles and neck and upper limb disorders is not fully understood. Exposure to vibration has been identified in existing literature as a potential risk factor. The drivers of terrain vehicles have a unique work situation where they are exposed to both whole-body vibration and hand-arm vibration simultaneously. Electromyography studies during exposure to whole-body vibration have mainly focused on the muscles in the lower back, whereas the studies on exposure to hand-arm vibration have focused on muscles in the hands. There is a lack of studies that investigate the exposure of the combination of whole-body vibration and hand-arm vibration. Furthermore, few studies have investigated neck muscle activation during exposure to vibration.

Aims ______________________________________________________
AIMS OF THE THESIS
This thesis investigates how the type of vibration exposure that occurs during occupational driving of terrain vehicles affects the neck and upper limb muscles. Specific aims • To establish the association between typical vibration
symptoms in hands and musculoskeletal symptoms in the neck and upper limbs and exposure to driving terrain vehicles (Paper I).
• To describe the acute effects of local vibration on the fatigue development in the upper trapezius muscle by means of electromyography (Paper II).
• To investigate the muscle activity in the upper trapezius muscle during a sustained sub-maximal contraction with induced vibration as measured by electromyography (Paper III).
• To compare the electromyographic response in the neck, lower back and forearms in a combined HAV and WBV exposure and separate HAV and WBV exposure (Paper IV).
• To establish possible gender differences on the effect of vibration exposure on muscle activity (Paper II-IV).
23

Methods ______________________________________________________
METHODS
The first paper included registered drivers of terrain-vehicles as well as reindeer herders from the northern part of Sweden. The second, third and fourth paper included young, healthy subjects with no history of being exposed to vibration in their occupation. Subjects Paper I
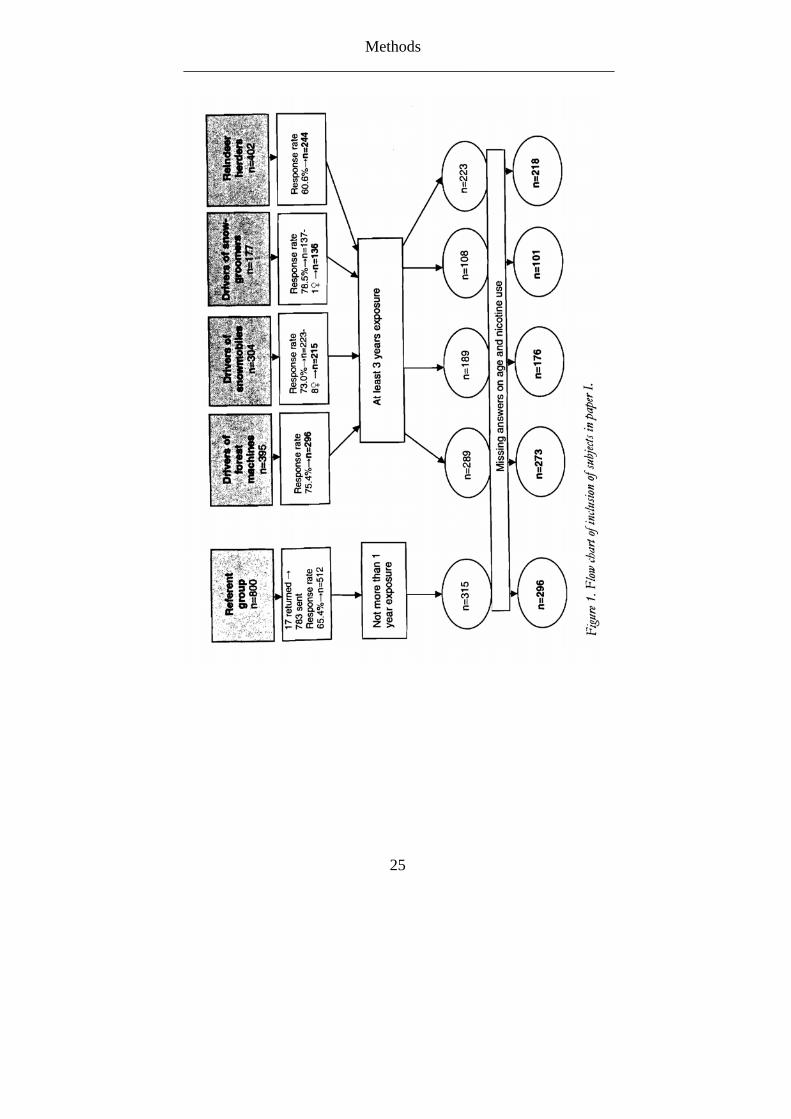
All registered drivers of terrain vehicles and randomly selected reindeer herders in the four most northern counties in Sweden were asked to participate in the questionnaire study. The drivers were registered as drivers of forest machines, workers using snowmobiles and workers using snow-groomers. The questionnaire was also sent to referents randomly selected from the general population in the same region. For a more detailed version of the inclusion procedure, see Figure 1. Only drivers that had worked professionally for at least three years were included in the exposed group. Only the referents that had no more than one year of exposure to driving any kind of terrain vehicle were included in the non-exposed group (referent group).
24
Methods ______________________________________________________
25

Methods ______________________________________________________
Table 2. Number of subjects included in paper I (n), age, cumulative exposure time during all years (lifetime) and during the previous year in hours (h) for drivers of terrain vehicles and referents (mean, range) and nicotine use.
Drivers of
Forest Machin s e(n=273)
Snowmobiles (n=176)
Snow- groomers (n=101)
Reindeer Herders (n=218)
Referents (n=296)
Age 49 42 42 45 42 (range) (26-69) (21-65) (23-60) (21-62) (20-61) Exposure time (h) Lifetime 42435 5483 14153 9829 0.5 (range) (172-135860) (80-39080) (1308-50640) (40-80136) (0-64) Previous 12 months 1669 306 624 381 1.1 (range) (0-5104) (0-1600) (32-1540) (0-2252) (0-96) Nicotine use (cigarettes or snuff)
114 67 40 107 107
(%) (41.8) (38.1) (39.6) (49.1) (36.1)
Paper II and III Twenty healthy male volunteers and 20 healthy female
volunteers were included in this laboratory study (Table 3). The participants had no history of musculoskeletal disorders and were asked to avoid hard physical activity the day before the day of measurement. All the volunteers gave their informed consent before the inclusion in the study.
Table 3. Characteristics of subjects in paper II and III, number, age, height, weight and maximum voluntary contraction (MVC), mean (range).
Men (n=20) Women (n=20)
Age (years) 25.7 (21-39) 25.9 (20-37) Height (cm) 183.9 (172-193) 167.0 (158-174) Weight (kg) 79.7 (64-95) 61.2 (48-70) MVC (N) 76 (45-103) 48 (28-72)
26

Methods ______________________________________________________
Paper IV Twelve healthy male volunteers and 10 healthy female
volunteers were included in the experimental study of combined vibration exposure (Table 4). The subjects had no history of musculoskeletal disorders and they were asked to avoid hard physical activity the day before the day of the experiment. All the volunteers gave their informed consent before the inclusion in the study.
Table 4. Characteristics of subjects in paper IV, number, age, height, weight, physical activity level and maximum voluntary contraction (MVC), mean (range). Men (n=12) Women (n=10) Age (years) 23 (20-26) 23 (21-25) Height (cm) 178 (165-189) 168 (160-178) Weight (kg) 75 (61-98) 62 (54-70) Physical activity level 5 (4-6) 5 (4-6) MVC trapezius (N) 76 (45-103) 54 (35-76) MVC erector carpi radialis (N) 17 (10-21) 12 (10-16)
DATA COLLECTION METHODS
Data collection methods included a self-administered questionnaire and experimental electromyography recordings.
Questionnaire (paper I) The mailed questionnaire asked the respondents to rate
symptoms of HAVS in their fingers and hands. There were six items regarding symptoms from left and right side of the body: 1) Numbness in hand or finger during night; 2) Reduced strength in hand; 3) Prone to drop objects; 4) Ache in finger; 5) Sensation of coldness in hand or finger; and 6) White fingers of the type where one or several fingers turns pale when it is damp or cold. The severity of the symptoms was graded from 1 to 4 (1=none, 2=insignificant, 3=some, 4=pretty much). The Swedish version of the Nordic Questionnaire was used to assess musculoskeletal symptoms within the last 12 months in the wrists, elbows, shoulders, and the neck (64). This questionnaire includes items with dichotomized response alternatives regarding symptoms (ache, pain, or discomfort) originating from different regions of the musculoskeletal system.
27

Methods ______________________________________________________
Each individual also estimated their exposure duration in total years, months/years and hours/weeks of driving various terrain vehicles. The cumulative exposure time in hours was calculated from this information. The same was done for cumulative exposure during the last 12 months. Information about the respondents’ age and nicotine use was also collected.
EMG (paper I-IV) In paper II and III, surface EMG was collected from the right
upper trapezius (pars descendens). In paper IV, surface EMG was collected from the right upper trapezius (pars descendens), right extensor carpi radialis longus, and the right lumbar part of erector spinae. Disposable bipolar Ag-AgCl electrodes were used. The electrode pairs (centre-to-centre distance 20mm) were placed along the direction of the muscles. The trapezius electrodes were placed 20 mm lateral to the midpoint of the line between the seventh cervical vertebra and acromion (65); the extensor carpi radialis electrodes were placed at the midpoint between the middle of the bend of the arm and the lateral epicondyle of humerus at a length distance of one-third the forearm length from the elbow to the wrist; the erector spinae electrodes were placed at a two-finger width (approximately 30mm) laterally from the processus spinosus of the L1 vertebrae (66). The skin was shaved and cleaned with alcohol before the electrode attachment. EMG was recorded with a digital wireless data acquisition system (67) with high impedance (>10GΩ) differential inputs. The EMG channels had ± 50mV dynamic range, 0-400Hz bandwidth, and <3µV RMS noise. Each channel was A/D converted at 1000 samples per seconds with 20 bits resolution, and the data was stored on a computer. The data was processed off-line using MATLAB software. In paper II and III, a 20Hz high pass 6th order digital Butterworth filter was applied to the EMG signal. In study IV, a 15Hz high pass and 250Hz low pass 8th order digital Butterworth filters were applied to the data. To suppress the motion artefacts from the EMG due to the vibration of the skin (paper IV), 0.8Hz wide 3rd order Butterworth notch filter centred at 10, 20, 30,…, and 110Hz were applied. There were also some problems with interference from the frequency converter controlling the vibrator’s cooling fan. This was removed using notch filters.
28

Methods ______________________________________________________
Vibration exposure Paper II and III
A small shaker that provided a sinusoidal acceleration of 2.4m/s2 (RMS) (1.7mmp-p) and a frequency of 10Hz in unloaded condition was used for vibration exposure. The vibration was applied approximately orthogonally to the subject’s right shoulder (the central part of the acromion) (Figure 2). This vibration frequency was chosen because it is a common frequency during occupational driving (20). A 15mm diameter circular plastic disc was mounted on the shaker, and the shaker was attached to a coil spring suspended linear bearing unit. When the subjects lifted their shoulders as they were instructed (elevated 2cm) the contact force from the shaker was about 5N.
Figure 2. Experimental set-up, paper II and III.
29
Methods ______________________________________________________
Paper IV A sinusoidal vibration with a frequency of 10Hz was generated
using a single signal generator (Hewlett & Packard 33120A) and two separate power amplifier and electrodynamic shaker assemblies. For the HAV exposure a Ling Dynamic System (LDS) 300 and LDS 7/600 were used and for WBV exposure a LDS MPA 1 and LDS 712 were used. The phase between the HAV and the WBV exposure could be inverted using a double pole switch between the MPA 1 and the LDS 712. The magnitude of the frequency-weighted acceleration was 5.0m/s2 for the HAV and 1.1m/s2 for the WBV. These measurements correspond to the exposure limit values established in the European vibration directive (68). The actual vibration magnitudes were measured using accelerometers (Brüel & Kjaer 4368 and 4384), one mounted on the seat and one mounted on the handle bar. The measured accelerations were amplified (Brüel & Kjaer 2635) before they were monitored on a digital oscilloscope (Tektronix).
30

Methods ______________________________________________________
Experimental procedure Paper II and III
First, the subjects performed a standing MVC of a shoulder elevation. A sling with a padded loop around their right shoulder was attached to a force transducer and the subjects were instructed to lift their right shoulder up as forcefully as possible. To ensure that the subjects did not bend their body to the opposite side to produce more force, the test leader stood behind the subject. The highest of three attempts was chosen as MVC. For normalisation of the EMG, the subjects then performed a sub-maximal contraction (30% of MVC) in the same position. The subjects were then seated on a stool and were instructed to sit in an upright position facing forward with their arms hanging beside their torso and their feet placed on a horizontal supporting surface. Weights (about 10% of MVC per weight) were held in the hands by the subjects to increase the muscle load in the trapezius. The weights were kept during the whole experiment, except during the resting period.
EMG was recorded during 15s when the subjects lifted both the shoulders up to the shaker (2cm) without vibration. Next the subjects kept this position for three minutes and directly after, EMG was recorded again for 15s without induced vibration. EMG was measured during the whole three minute period as well. The subjects also rated the perceived exertion of the upper trapezius muscle after the three minutes using the Borg 6-20 scale (69). The three minute periods were repeated four times, twice with the induced vibration (V1 and V2) and twice without (NV1 and NV2). There was 10 minutes of rest between each of the four trials and the order of the four trials was randomized. The 15s measuring period before and after the three minutes was always performed without vibration. For an illustration of the experimental procedure see Figure 3.
31

Methods ______________________________________________________
Figure 3. Experimental procedure paper II and III. The order of all four periods was randomized.
Paper IV Fine-tuning the phase was done with a simple RC filter with
variable resistance. The subjects were seated on a wooden seat without a back rest that was mounted on the large LDS 712 shaker (Figure 4). The posture was measured and controlled, and was 90 degrees to the hips and knees. A hard plastic bicycle-like straight handlebar with a 35mm-diameter handles and 390mm handles (centre-to-centre distance) was mounted on the HAV shaker. The handlebar was placed so that a 60-degree shoulder flexion with straight elbows was attained. The subjects applied a grip force of 40N during the whole exposure time. This was monitored with an I-scan system (Tekscan) including a 5101 model sensor. The subjects were asked neither to lean on nor to lift the handles so that they only lifted the weight of their arms. To control this, the applied push/pull force on the handlebar was measured with a load cell (Tedea Huntleigh,
15s EMG recordning
15s EMG recordning
15s EMG recordning
Paper III Paper II Paper II
Period 1
Period 2
Period 4
Period 3
180s static muscle load with vibration exposure (V1)
180s static muscle load with vibration exposure (V2)
180s static muscle load without vibration exposure (NV1)
15s EMG recordning
15s EMG recordning
15s EMG recordning
15s EMG recordning
15s EMG recordning
180s static muscle load without vibration exposure (NV2)
32

Methods ______________________________________________________
1022, 35kg) mounted between the handlebar and shaker. Using a pointer instrument, both the subjects and the test leader could monitor the load cell force. EMG was recorded for 30s of exposure, five periods in total, with two minutes of rest in between each recording period. The exposures were hand-arm vibration from the handles (HAV), whole-body vibration from the seat (WBV), HAV+WBV in phase (COMB1), HAV+WBV, 180° phase shifted (COMB2), and one period without vibration exposure (NV). The order of all exposures was randomized. The experimental procedure is presented in Figure 5.
Figure 4. Experimental set-up, paper IV, showing sitting posture, vibration exposure, and electrode placement for the trapezius, erector spinae and extensor carpi radialis.
33

Methods ______________________________________________________
COMB2 HAV WBV
Figure 5. An example of an experimental procedure; no vibration (NV), hand-arm vibration (HAV), whole-body vibration (WBV), HAV+WBV in phase (COMB1), HAV+WBV, 180° phase shifted (COMB2). The order of all exposures was randomized. Statistical methods Paper I
One non-symptom group and one symptom group were created in the exposed group as well as in the referent group for each of the symptoms for determining prevalence odds ratios (POR). For the HAVS symptoms, the non-symptom group included the participants that graded their symptoms as 1 or 2; the participants that graded their symptoms as 3 or 4 created the symptom group. For the musculoskeletal symptoms, the answers were already dichotomized according to the Nordic questionnaire (64). POR comparing the prevalence of symptoms in respective driving group with the referent group was determined by means of multiple logistic regression analysis and was adjusted for age and nicotine use. Significance refers to the 95% confidence interval. SPSS 12.0.1 (SPSS Inc.) was used for the statistical calculations. All the drivers (also those with <3 years of exposure time) were also stratified into four exposure bands (life time exposure in hours of all terrain vehicles) to calculate odds ratios in each exposure band.
Paper II Repeated measures analysis of variance (SPSS version 12.0.1)
was used to examine the effects of vibration. The independent variables were exposure (vibration (V) and no-vibration (NV)), measure (1st/2nd), and gender (men/women). The dependent variables were the difference in EMGMNF and EMGRMS between before and after the three minute sub-maximal trapezius contraction (∆EMGMNF and ∆EMGRMS). Significance was accepted at p ≤ 0.05.
Rest
120s 120s 30s 30s 120s 120s
Rest Rest Rest COMB1 NV
30s 30s 30s
34

Methods ______________________________________________________
35
Paper III Only the first measure of vibration and no-vibration condition
(V1 and NV1) were used in paper III. The EMG parameters were analyzed for a selected 173s segment to avoid possible artefacts in the beginning and end of the recordings. This 173s was divided into three equally long segments. The slopes of the normalized EMGRMS and of the EMGMNF in each period, for each individual were estimated using linear regression (SPSS version 15.0.). The effect of vibration on the regression coefficient was then compared using repeated measures analysis of variance. The independent variables were exposure (vibration (V) and no-vibration (NV)), time period (1st/2nd/3rd), and gender (men/women). The dependent variables were regression coefficient for EMGRMS and EMGMNF. Significance was accepted at p ≤ 0.05.
Paper IV Repeated measures analysis of variance (SPSS version 15.0.) was
used to examine the effects of different vibration exposures on the EMG response in the neck, arms and lower back. The independent variables were exposure (HAV, WBV, COMB1, COMB2) and gender (men/women). Dependent variables were the normalized EMGMDF and EMGRMS (expressed as percentage of NV) of the different muscles. Significance was accepted at p ≤ 0.05. Ethical approval
The Ethical Committee of the Faculty of Medicine at Umeå University approved of the studies (§454/03, dnr 03-400).

Results ______________________________________________________
RESULTS
Prevalence of hand-arm vibration syndrome and musculoskeletal disorders (Paper I)
The excluded subjects in paper I did not differ from the final study population (Table 5). Table 5. Number of excluded drivers of terrain vehicles and referents (n), age, cumulative exposure time during all years (lifetime) and during the previous year in hours (h) (mean, range) and nicotine use.
Drivers of
Forest Machines (n=23)
Snowmobiles (n=35)
Snow-groomers (n=35)
Reindeer Herders (n=26)
Referents (n=216)
Age 52 43 37 51 40 (range) (32-68) (21-63) (20-63) (29-61) (19-61) Exposure time (h) Lifetime 25788 2459 3896 1142 1585 (range) (0-66012) (0-29520) (432-23828) (0-16840) (0-26464) Previous 12 months 1158 221 507 8.5 97 (range) (0-2160) (0-1124) (40-1080) (0-80) (0-1768) Nicotine use (cigarettes or snuff)
9 9 16 6 74
(%) (39.1) (25.7) (45.7) (23.1) (34.3)
Hand-arm vibration syndrome The drivers and the reindeer herders had a high prevalence of
numbness (17-30%), sensation of cold in hand or fingers (16-24%), and white fingers (12-20%). Numbness was the most dominant symptom of HAVS in the referent group (13%). No obvious differences between left and right side were found. In general, the drivers and reindeer herders had higher prevalence for the symptoms of HAVS compared to the referent group (Table 6). All the exposed groups had increased odds for numbness and sensation of cold on at least one side (POR 1.5-3.9). All the drivers except for the snow-groomers had increased odds for white fingers in at least one hand
36

Results ______________________________________________________
(POR 1.9-3.5). The drivers of snow-groomers also had increased odds for ache in fingers in the right hand (POR 2.6). No increased odds were found for poor strength or for prone to drop objects in any of the groups (Table 7).
Musculoskeletal disorders Prevalence of musculoskeletal symptoms in the neck (43-61%),
shoulder (26-43%) and wrist (15-30%) were high in the driver groups and reindeer herders compared to the referents (12-31%) (Table 6). Increased odds of musculoskeletal symptoms in the neck were found for all driver groups and the reindeer herders (POR 2.1-3.9) (Table 7). All driver groups had increased odds of symptoms in at least one shoulder (POR 1.8-2.6). Increased odds of symptoms in the right elbow were found only in drivers of snow-groomers (POR 2.0). The POR of musculoskeletal symptoms in the wrist was significantly increased in all the drivers except drivers of forest machines (POR 1.7-2.6) (Table 7).
Table 6. Prevalence (%) of HAVS and MSD in the neck and upper limbs for all the exposed groups and the referent group.
Drivers of
Forest – machines
(n=273)
Snowmobiles
(n=176)
Snow- groomers
(n=101)
Reindeer herders (n=218)
Referents
(n=296) Left Right Left Right Left Right Left Right Left Right
Numbness 22 20 19 17 28 30 28 27 13 13 Poor strength
10 10 7 9 12 16 15 16 11 11
Prone to drop objects
8 7 3 3 4 4 6 7 6 6
Ache in finger
11 11 10 8 15 14 10 11 10 7
Sensation of cold
19 21 17 16 22 22 22 24 12 9
White fingers
19 20 12 13 13 13 16 16 9 7
Wrist 17 15 17 22 26 29 25 30 12 15 Elbow 12 16 11 15 5 17 11 16 8 11 Shoulder 43 43 26 34 42 41 38 39 22 25 Neck 56 43 61 49 31
37

Results ______________________________________________________
38

Results ______________________________________________________
Exposure time There were significantly higher odds ratios in the higher
exposure quartiles compared to the lowest concerning numbness, coldness in hand, or finger on the right side, and white fingers in the right hand. However, there was no clear pattern of increasing odds ratios between the three higher exposure quartiles (Table 8). There were significantly higher odds ratios in the higher exposure quartiles compared to the lowest in the musculoskeletal symptoms in the neck, shoulder, and wrist in both sides and in the elbow on the right side. For the shoulders and the neck as well as the right elbow a pattern of increasing odds with increasing exposure time was apparent (Table 8).
39

Results ______________________________________________________
40

Results ______________________________________________________
Fatigue development (Paper II) Because of insufficient quality in the EMG recording for three
of the subjects, these were removed from the analysis in paper II. Most of the 37 subjects exhibited a decreased EMGMNF during the 180s-sustained sub-maximal contraction (NV1: 29 subjects; NV2: 36 subjects; V1: 31 subjects; V2: 23 subjects). The mean EMGMNF decreased in both vibration (V1: -3.54; V2: -1.48Hz) and no-vibration condition (NV1: -3.71; NV2: -4.37Hz), but significantly more in the no-vibration condition (p=0.010) (Figure 6 and Table 9). The mean EMGRMS increase was larger for the contraction without vibration (5.23% and 6.12%) compared to with vibration (4.01% and 3.54%); however, this was not statistically significant. The repeated measure analysis showed a significant effect of vibration on ∆EMGMNF. It also revealed an interaction between vibration and 1st/2nd measure (Table 10). There were no difference in the Borg ratings between V and NV.
Figure 6. Mean EMGMNF (Hz) and EMGRMS (% of 30% MVC) for the whole group, before and after the three minute sub-maximal trapezius contraction, 1st and 2nd measure, with (V1, V2) and without vibration (NV1, NV2).
41

Results ______________________________________________________
Table 9. Means of EMGMNF and EMGRMS for vibration and no-vibration, first (1st) and second (2nd) measure, before (b) and after (a) the three-minute sub-maximal trapezius contraction. Men (n=20) Women (n=17) 1st 2nd 1st 2nd b a b a b a b a Vibration EMGMNF
(Hz) Mean SD
77.5 13.2
74.4 12.5
75.4 12.9
73.1 11.9
76.6 12.1
72.5 11.8
73.2 9.4
72.7 9.3
EMGRMS (% of 30% MVC) Mean SD
74.6 22.4
76.3 22.6
78.2 28.7
81.0 27.3
73.1 35.5
82.4 48.1
79.1 39.4
89.2 49.6
No- vibration
EMGMNF (Hz) Mean SD
77.4 13.6
73.6 12.2
76.4 12.5
71.6 11.7
75.6 9.6
71.9 8.5
76.6 10.8
72.7 11.8
EMGRMS (% of 30% MVC) Mean SD
79.5 34.2
81.7 31.3
79.1 28.1
79.7 29.4
77.5 45.8
83.5 50.1
75.5 35.5
82.5 45.5
Table 10. Summary of the repeated measures analysis of variance comparing exposure condition; vibration (V) and no-vibration (NV), first and second measure (1st/2nd) and gender (men/women). Dependent variables are ∆EMGRMS and ∆EMGMNF for the trapezius. Measures F df p Anova for ∆EMGMNF Within subjects effect Condition= V/NV Condition= 1st/2nd measure V/NV*1st/2nd measure Between subjects effect Gender = Men/Women
9.484 1.466 7.507
3.564
1 1 1
1
0.004* 0.234 0.010*
0.612
Anova for ∆EMGRMS Within subjects effect Condition= V/NV Condition= 1st/2nd measure V/NV*1st/2nd measure Between subjects effect Gender = Men/Women
1.210 0.011 0.089
0.263
1 1 1
1
0.279 0.917 0.767
0.067
*p<0.05
42

Results ______________________________________________________
Muscle activity during vibration (Paper III) There was no difference between V and NV in the mean
EMGRMS of the total 173s recording (Table 11 and Table 12). However, the mean regression coefficient of EMGRMS for the different time periods revealed a higher initial regression coefficient during the vibration exposure vs. without vibration (0.096% vs. 0.045%) (Table 12). This was however not significant in the repeated measures analysis (Table 11). The repeated measures analysis showed no significant effect of vibration concerning the regression coefficient of the EMGMNF, but there was a larger mean EMGMNF decrease for NV compared to V. By dividing the data with time a slight larger decrease in the first period could be seen for the NV compared to V (Table 13). Table 11. Summary of the repeated measures analysis of variance comparing exposure condition; vibration (V) and no-vibration (NV), time period (1st/2nd/3rd) and gender (men/women). Dependent variables are regression coefficient of EMGRMS and EMGMNF for the trapezius.
Measures F df p Anova for regression coefficient EMGRMS Within subjects effect
V/NV 0.001 1 0.973 V/NV*gender 0.006 1 0.940 V/NV* 1st/2nd/3rd period 0.942 2 0.394 V/NV* 1st/2nd/3rd period*gender 0.457 2 0.635 Between subjects effect Gender (men/women)
1.037
1
0.315
Anova for regression coefficient EMGMNF Within subjects effect
V/NV 1.346 1 0.253 V/NV*gender 0.701 1 0.408 V/NV* 1st/2nd/3rd period 0.493 2 0.613 V/NV* 1st/2nd/3rd period*gender 3.037 2 0.054 Between subjects effect Gender (men/women)
35.798
1
0.322
*p<0.05
43

Results ______________________________________________________
Table 12. Mean of regression coefficient on normalized EMGRMS (%V/s) divided by exposure (V/NV), time (1st, 2nd, 3rd) and gender (men/women). Exp Mean SE Period Mean SE Gender Period Mean SE V
0.041
0.015
1
0.096
0.029
Men
1
0.063
0.041
2 0.014 0.023 2 0.034 0.032 3 0.011 0.026 3 0.001 0.037 Women 1 0.129 0.041 2 -0.005 0.032 3 0.022 0.037
NV
0.040
0.011
1
0.045
0.021
Men
1
-0.001
0.030
2 0.048 0.036 2 0.043 0.051 3 0.026 0.032 3 0.049 0.046 Women
1 0.091 0.030 2 0.054 0.051 3 0.003 0.046
Table 13. Mean of regression coefficient on EMGMNF (Hz/s) divided by exposure (V/ NV), time (1st, 2nd, 3rd) and gender (men/women). Exp Mean SE Period Mean SE Gender Period Mean SE V
-0.016
0.005
1
-0.031
0.007
Men
1
-0.034
0.010
2 -0.013 0.007 2 -0.023 0.009 3 -0.003 0.008 3 -0.008 0.011 Women 1 -0.027 0.010 2 -0.002 0.009 3 0.001 0.011
NV
-0.023
0.004
1
-0.042
0.009
Men
1
-0.058
0.013
2 -0.025 0.007 2 -0.015 0.010 3 -0.004 0.007 3 0.001 0.009 Women
1 -0.026 0.013 2 -0.034 0.010 3 -0.008 0.009
Combination of hand-arm vibration and whole-body vibration (Paper IV)
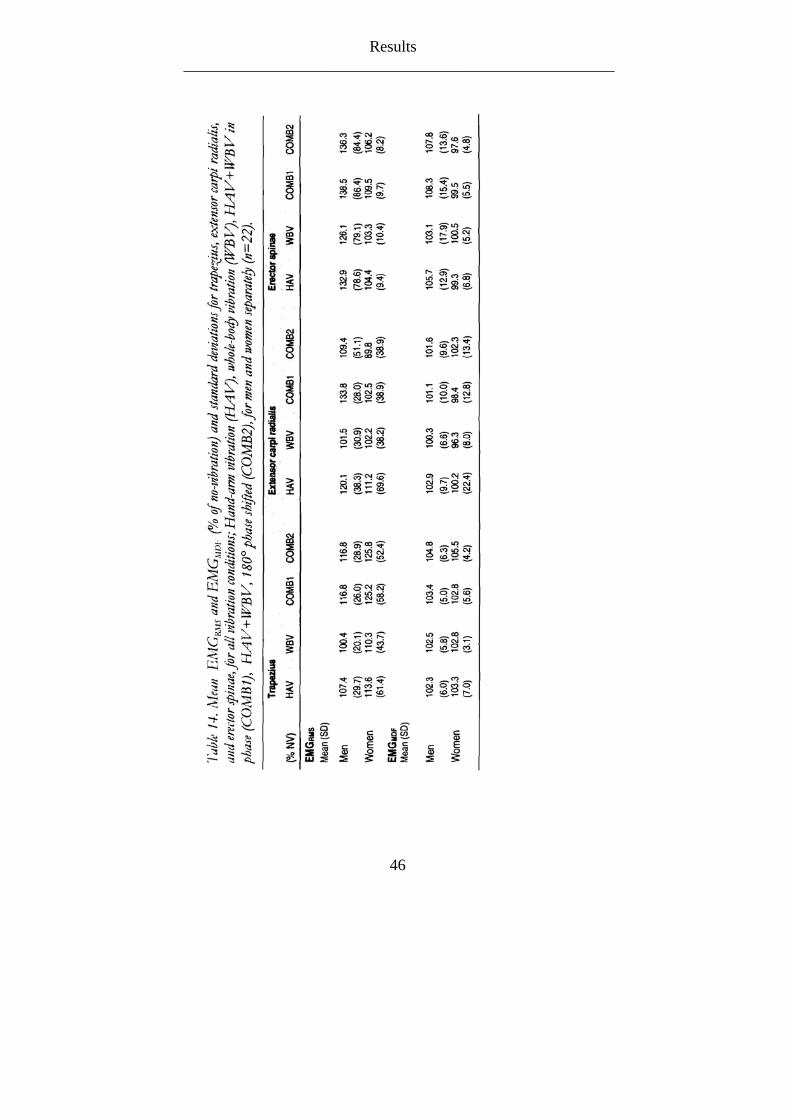
The mean EMGRMS and EMGMDF for men and women separately are presented in Table 14, and on group level in Figure 7 and Figure 8. For the trapezius there was a higher EMGRMS for the COMB1 and COMB2 compared to the HAV and WBV separately. The WBV did not differ from the no-vibration condition (Figure 7). There was a similar pattern for the trapezius muscle concerning the EMGMDF. The COMB1 and COMB2 had a higher EMGMDF than the other exposures with the COMB2 having the highest EMGMDF
44

Results ______________________________________________________
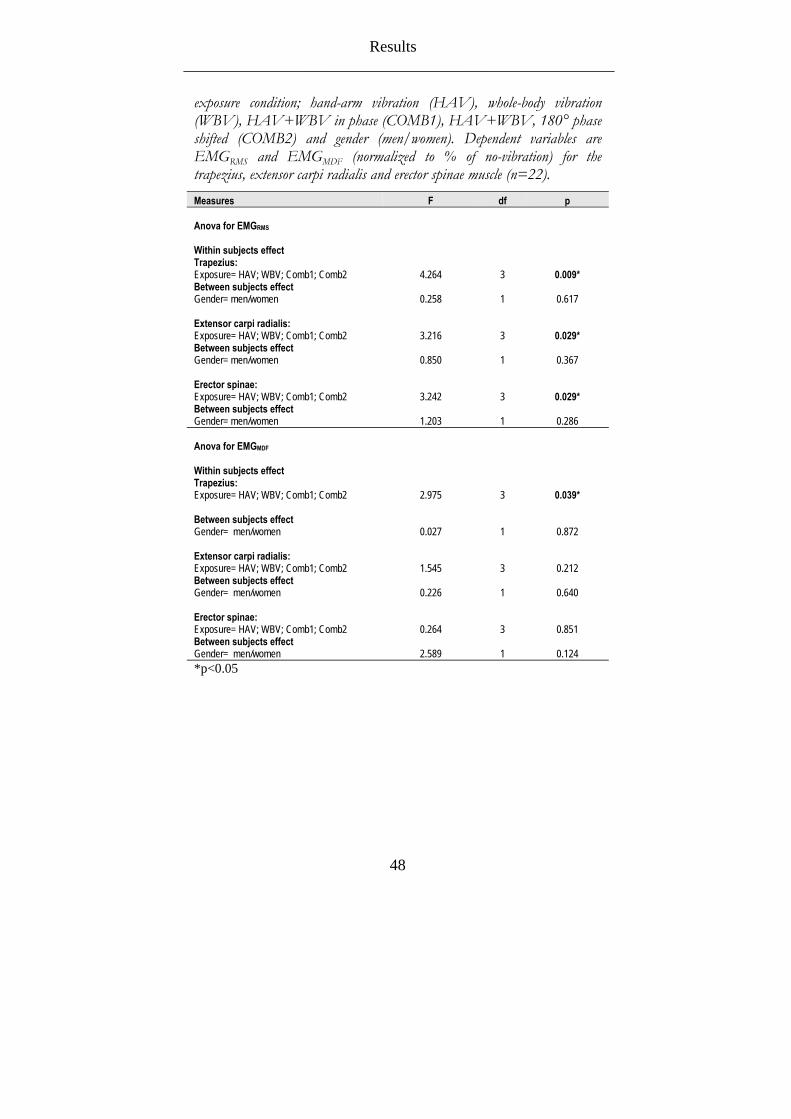
(Figure 8). There was a higher EMGRMS for HAV and COMB1 for the extensor carpi radialis, whereas the WBV and COMB2 showed no higher values compared to the condition without any vibration exposure (Figure 7), and similar patterns appeared for the EMGMDF but for the COMB2 instead of COMB1 (Figure 8). For the erector spinae muscle, there was a generally high increase in EMGRMS and EMGMDF for all exposures compared to the no-vibration condition, but with a higher increase for the COMB1 and COMB2 (Figure 7, Figure 8). The repeated measures analysis showed a significant effect of exposure on EMGRMS in all measured muscles, whereas only in the trapezius for the EMGMDF (Table 15).
45
Results ______________________________________________________
46

Results ______________________________________________________
0
20
40
60
80
100
120
140
Trapezius Extensor carpiradialis
Erector spinae
Muscle
RM
S (%
of n
o vi
brat
ion)
HAV
WBV
COMB1
COMB2
Figure 7. Mean EMGRMS (% of no-vibration) for the trapezius, extensor carpi radialis, and erector spinae, for all vibration conditions; Hand-arm vibration (HAV), whole-body vibration (WBV), HAV+WBV in phase (COMB1), HAV+WBV, 180° phase shifted (COMB2) (n=22).
94
96
98
100
102
104
106
Trapezius Extensor carpiradialis
Erector spinae
Muscle
MD
F (%
of n
o vi
brat
ion)
HAVWBVCOMB1
COMB2
Figure 8. Mean EMGMDF (% of no-vibration) for the trapezius, extensor carpi radialis, and erector spinae, for all vibration conditions; Hand-arm vibration (HAV), whole-body vibration (WBV), HAV+WBV in phase (COMB1), HAV+WBV, 180° phase shifted (COMB2) (n=22).
Table 15. Summary of the repeated measures analysis of variance comparing
47
Results ______________________________________________________
exposure condition; hand-arm vibration (HAV), whole-body vibration (WBV), HAV+WBV in phase (COMB1), HAV+WBV, 180° phase shifted (COMB2) and gender (men/women). Dependent variables are EMGRMS and EMGMDF (normalized to % of no-vibration) for the trapezius, extensor carpi radialis and erector spinae muscle (n=22). Measures F df p Anova for EMGRMS
Within subjects effect Trapezius: Exposure= HAV; WBV; Comb1; Comb2
4.264
3
0.009* Between subjects effect Gender= men/women
0.258
1
0.617
Extensor carpi radialis: Exposure= HAV; WBV; Comb1; Comb2
3.216
3
0.029*
Between subjects effect Gender= men/women
0.850
1
0.367
Erector spinae: Exposure= HAV; WBV; Comb1; Comb2
3.242
3
0.029*
Between subjects effect Gender= men/women
1.203
1
0.286
Anova for EMGMDF
Within subjects effect Trapezius: Exposure= HAV; WBV; Comb1; Comb2
2.975
3
0.039*
Between subjects effect Gender= men/women
0.027
1
0.872
Extensor carpi radialis: Exposure= HAV; WBV; Comb1; Comb2
1.545
3
0.212
Between subjects effect Gender= men/women
0.226
1
0.640
Erector spinae: Exposure= HAV; WBV; Comb1; Comb2
0.264
3
0.851
Between subjects effect Gender= men/women
2.589
1
0.124
*p<0.05
48
Results ______________________________________________________
49
Gender differences (paper II-IV) There were too few women in the cross-sectional material on
HAVS and MSDs for a gender analysis to be done. The analysis of muscle fatigue and vibration showed no gender difference on the effect of vibration. There was, however, a higher EMGRMS increase in general for the women compared to the men (Table 9). This was similar for the V and the NV. In paper III, there were some differences in the EMGRMS increase in different time periods between men and women. The women had an initial increase in EMGRMS in both V and NV but the regression coefficient was larger for the V (0.129% vs. 0.091%) (Table 12). The men had a regression coefficient of the EMGRMS in the first period that was half the size of the women’s initial increase during V (0.063%) and almost no initial change at all at all during NV (-0.001%) (Table 12). A slight gender effect was also apparent concerning the EMGMNF. The men had a large initial EMGMNF decrease during NV compared to V (-0.058Hz/s vs. -0.034Hz/s), whereas the initial EMGMNF decrease did not differ between NV and V for the women (-0.026Hz/s vs. -0.027Hz/s) (Table 13). Concerning the combination of WBV and HAV, there was no gender effect found on the effect of exposures. However, some differences were seen in EMGRMS between men and women in the different muscles. The women had a higher trapezius EMGRMS generally in all exposures, whereas the men had a higher EMGRMS in the erector carpi radialis and the erector spinae (Table 14).

Discussion ______________________________________________________
DISCUSSION
Results Hand-arm vibration syndrome and musculoskeletal disorders in the neck and upper limbs
A higher prevalence of HAVS symptoms for the drivers of terrain vehicles compared to unexposed referents was found. Similar results have been reported (70) on drivers of snowmobiles with an age-adjusted prevalence of white fingers of 18%, a percentage similar to the snowmobile drivers in this thesis (left side: 19%; right side: 17%). The prevalence of numbness in the hands in Anttonen and Virokanna’s study was 49%, while only around 12% was seen in the present study. A study on traffic police motorcyclists showed an increased prevalence of finger blanching (4.2% compared to 0% in the control group) and finger numbness (19.3% compared to 4.1%) (71) which is lower than what was found in the drivers in the present study. Police motorcyclists operate in a more regular terrain, and therefore the vibration exposure would not be the same for this group compared to terrain vehicle drivers.
Age and nicotine use could not explain the results in the present study and therefore vibration exposure from the steering device could be contributing to the symptoms. HAV levels in terrain vehicles have been measured and exposure levels that could cause HAVS have been found (72, 73).
High prevalence of MSD in the neck, shoulders and arms was also found in the present study, a finding that is similar to Mirbod et al. (71) who reported a prevalence of 13.4% of shoulder pain and 45.4% of shoulder stiffness in police motorcyclists. The musculoskeletal symptoms are more difficult to directly relate to vibration exposure since these symptoms are related to a number of known risk factors. Some of these risk factors are present in driving environments such as poor ergonomics, low-level static load, long duration of sitting, and stress. However, vibration is one risk factor as well, and HAV might be transmitted from the hands directly up to the neck. The WBV from the seat is transmitted up through the spine. This could cause a higher muscular demand of the stabilising muscles in the neck and possibly cause a more static muscle use. The vibration could also cause the driver to grasp the handlebar or
50

Discussion ______________________________________________________
steering device harder because of reduced sensation in the hand and because of this increase the static muscle load in the arms, shoulders and neck.
Vibration and fatigue development The study on local vibration in the trapezius muscle during a
sub-maximal shoulder elevation shows that vibration induced in the trapezius muscle during a fatiguing task results in a smaller EMGMNF decrease compared to the same fatiguing task without induced vibration. This might indicate that the induced vibration reduced the level of fatigue or that it slowed the fatigue development down. Contrary to our results, Hansson et al. (63) showed a larger decrease of EMGMNF in the erector spinae muscle during a five minute vibration exposure compared to static sitting, concluding the result with vibration increasing the fatigue development in the muscle. Coorevits et al. (74) studied vibration and its effects on localized muscle fatigue in the back and found a larger decrease in the EMGMNF during no-vibration condition as in the present study. A study on arm flexors during fatiguing contractions reports similar results and suggests a more efficient and effective recruitment of high threshold MUs during fatiguing contractions with vibration exposure (75). Muscle fibres that are mainly used in low level work load like the shoulder elevation in the present study are the small type I (slow oxidative) (76). Vibration induced into a muscle or a tendon is believed to affect mainly the recruitment of the type IIB fibres (fast glycolytic) (77). Vibration to the patellar tendon has been reported to decrease the recruitment threshold and firing rates of MUs (78). Martin et al. (79) showed that an increase in the TVR in frequencies below 100Hz results principally from an increase in motor neuron depolarization with the firing frequency of Ia afferents, which leads to a recruitment of MUs of increasing threshold. One hypothesis could be that this central effect increases the recruitment of type IIb fibres making it responsible for a larger rotation of MUs. This larger variation of fibre types being used when vibration is induced might activate a smaller proportion of the type I muscle fibres than would normally be the case during a low level static contraction, resulting in the trapezius muscle not being fatigued to the same extent. It might be argued that the type IIb muscle fibres are less fatigue resistance than the type I, and therefore there is a possibility that the results could have been the opposite if the exposure time would have been
51

Discussion ______________________________________________________
longer. Nevertheless, an increased rotation of MUs should have a positive effect on muscular fatigue.
Increased discharge rate of MUs in muscles in the hand has been found after 30 minutes of vibration exposure and is suggested to be necessary for performing the constant-force task due to the vibration-induced decrease in the force capacity of the muscle (80). The smaller decrease of EMGMNF after vibration found in the present study might be an after-effect like the one described above. A combination of the increased variation in fibre type activation and after effects on discharge rates might also be the case. Histological experiments have reported that there are differences in how short-term vibration affects the type I and the type II muscle fibres, which supports the theory that there is an increased recruitment of type II muscle fibres during vibration (36).
An increase in peripheral circulation in the trapezius muscle might also be contributing to the smaller EMGMNF decrease after vibration exposure. Some studies have shown an increased blood flow with vibration exposure (81); however, others have shown a decrease in the peripheral circulations (30, 82). Clearly, the effect of vibration on peripheral circulation depends on the frequency of the vibration (30). Different muscles might also exhibit differing effects when exposed to vibration.
In the present study, the EMGRMS was higher in the vibration condition compared to the condition without vibration, although this was not significant. Similar results have been reported (79, 83) in the finger and wrist flexor muscles and been described as an effect of the tonic vibration reflex. The effect of this reflex has mostly been presented for vibration exposures of higher frequencies (40-150Hz). However, Seidel (52) showed TVR during whole-body vibration with the frequencies of 1–30Hz.
Changes in muscle activity during vibration exposure
A larger EMGRMS increase in the trapezius muscle in the first time period for the vibration condition compared to the no-vibration condition was found. Hansson et al. (63) studied the effect of vibration exposure in the back muscles in seated subjects during a five minute period. The results in the thoracic part of the erector spinae muscle in Hansson’s study were similar to the present study with a larger increase in EMGRMS initially, which then decreased towards the
52

Discussion ______________________________________________________
end of the five minutes. The effects of the tonic vibration reflex have been shown to be more pronounced in the initial 10 seconds of vibration exposure in the biceps brachii muscle (84). Increased muscle activity initially during vibration exposure followed by a decline has been presented (85). Griffin et al. (86) studied vibration and fatigue in the triceps brachii muscle and found an initial decrease in the firing rate as could be expected during sustained contraction, but after applying vibration an increased firing rate was seen. The type of MUs that are mostly affected by vibration are characterized by a high recruitment threshold in voluntary isometric contractions, a high firing rate during the initial phase of MVCs, and a rapid decline in firing rate during sustained MVCs (85). The smaller EMGMNF decrease during vibration in the first time period compared to without vibration found in the present study are not coherent with results by Coorevits et al. (74) where the EMGMNF decreased more initially when exposed to vibration.
Combination of HAV and WBV A combined HAV and WBV exposure increased the muscle
activity as measured by EMGRMS and EMGMDF in the trapezius. HAV and WBV separately also increased the EMGRMS compared to no-vibration, but not to the same extent as the two combinations of HAV and WBV. There was some increased EMGRMS in the extensor carpi radialis during HAV and one of the combined exposures. Increased muscle activity in shoulder muscles (87), biceps brachii (88) as well as the forearm muscles (87) during exposure to local vibration has been shown by others. The muscle activity in erector spinae increased for all exposures, but no clear difference in muscle activity during the combined vibration exposure compared to the HAV and WBV was found in the present study. Studies have shown increased muscle activity in the back muscles when exposed to vibration (52, 53). The vibration exposure in these studies, however, was not identical with the one chosen in the present study. Both amplitude and frequency have been reported to be of importance when looking at its effects on muscle activity measured with EMG (52, 55, 58, 60, 89).
The vibration that was used in the present study, with a lower frequency, is transmitted through body parts. Head transmissibility in seated subjects exposed to 10Hz WBV have been reported being between 0.52 (least severe posture) and 1.14 (most severe posture)
53

Discussion ______________________________________________________
(60, 90). Trunk transmissibility has been reported to be up to 1.7 for 10Hz vibration (60). With the double vibration that was investigated in this study, two sources of vibration existed, the handles and the seat. Therefore, the vibration is transmitted from both the hands through the arms up to the neck and from the buttocks up to the neck through the spine. This might cause a high absorbed vibration magnitude in the trapezius muscle with larger reflex muscle activation as a consequence. Studies have shown that higher vibration magnitudes cause a higher muscle response (52). Concerning the combination of HAV and WBV in anti-phase, it could cause an increased stretch in the trapezius muscle with a larger reflex activation as a consequence. This anti-phase condition could cause more constant and static muscle activation in the trapezius and result in a higher EMGRMS that might contribute to development of muscle fatigue with increasing exposure duration. Resonance has been reported in the lower back for frequencies at 3-4Hz, 6Hz, and 10-12Hz when applying impact to the hand-arm system for standing subjects (91). This resonance was lower than when the impact was applied at the feet, and the authors concluded the results as an attenuation of the vibration by the hand-arm system before it reaches the lumbar spine. The highest EMG amplitude was found in this study during the combined HAV and WBV, indicating that the trapezius absorbs energy from the HAV before it reaches the lumbar spine and the WBV before it reaches the hand-arm system.
The proprioception is known to be affected by vibration exposure. Vibration exposure is believed to modulate postural orientation and postural equilibrium. This can result in changes in the centre of pressure in standing and increases body sway (92). Vestibular response to low frequency vibration has also been suggested to elicit a muscle response (52). The postural sway (mainly in the anterior-posterior direction) as well as the illusion of body segments moving are affected by exposure to local vibration (93, 94). Studies have shown that this disturbed proprioception arises regardless of which muscle is vibrated as long as the muscle is related to postural control (95). The above mentioned studies were performed on standing subjects and with exposure local vibration. However, postural control can also be effected by seated WBV (93). The combined HAV and WBV in anti-phase might cause conflicting illusory movements because of the two different sensory inputs. If so, this could cause a higher muscular demand for the trapezius to stabilize the head and for erector spinae to stabilise the upper body.
54

Discussion ______________________________________________________
Gender effects The cross sectional study did not include a sufficient number of
women for a gender analysis. This is simply due to the fact that there are few women in professions that include driving terrain vehicles. No gender effects were found on the effect of vibration in the study of vibration and muscular fatigue in the trapezius. However, some effects were found on the EMGRMS in general. A larger increase in the EMGRMS both with and without induced vibration was found for the women compared to the men. As mentioned, the recruitment of type IIb muscle fibres is mainly affected by vibration (77). Women, however, have a larger over all portion of type I fibres (96), so this would not explain the larger increase in EMGRMS. The higher EMGRMS for women was also present for both with vibration and without. Some studies have suggested a difference in the distribution of muscle fibres between men and women. Women have a larger portion of type IIb fibres in the descending part of the trapezius (especially in the lower part of it) and men have a larger portion of type II fibres in the upper part of the descending portion of the trapezius (97, 98). The electrodes in the present study were placed on the lower part or the descending portion (65), and this might explain why a larger EMGRMS increase was found in the women. It might also explain the effects that were found in the study of muscle activity during vibration (Paper III) where the women had a larger initial EMGRMS increase during V compared to the men. In the study of the combined HAV and WBV no gender effects on the differences in muscular response between the exposures were found. There were however, some differences in amplitude of the EMG in the different muscles. The women seemed to use their trapezius to a higher degree than the men, and the men had a higher activity in their forearms and lower back. Experimental studies have shown that women tend to use their trapezius muscle more than men when performing work with their arms. Although the posture in the present experiment was controlled, individual muscle activation strategies could have occurred (14).
55

Discussion ______________________________________________________
Methodological considerations Epidemiology
The cross-sectional design has its limitations, especially since it cannot draw conclusions about single causative effects. A longitudinal study is more suitable for this. The drivers have various ergonomic situations that are likely to affect the occurrence of MSDs. These factors were not taken into account in the first paper. The study group consisted of different driving groups that not only have different ergonomic environments, but also differences in seasonal work, cold exposure, and work routines.
To be included in the exposed group, the subjects had to have at least three years of exposure, where each year had to include more than eight hours of exposure to terrain vehicles. This is a very short exposure time, and it can be argued if eight hours of driving would have any effect on the health. However, most of the drivers that were included in the study reported far more hours/year of driving. Over-estimation, however, can be a problem in retrospective exposure assessments. The respondents were not asked whether they used vibrating hand-held tools, which would influence their symptoms, especially of HAVS.
Experimental design An interaction between the first and second measure was found
for the effect on the ∆EMGMNF. The initial EMGMNF was lower for the second vibration exposure than for the other trials (V1, NV1 and NV2). One could hypothesize that the vibration was a new and unacquainted stimulus that the subjects were not used to; therefore they tensed their muscles more the first time (V1). The difference was within the normal range of variance in EMGMNF measures in laboratory settings (99). There are some difficulties with standardizing a shoulder elevation and different muscle strategies might occur. To reduce this as much as possible, it was visually controlled by the same test leader during the whole experiment.
In paper III, no statistically significant differences were found in the EMG parameters between the vibration and the no-vibration condition. One reason for this could be that the study included an insufficient number of subjects. However, most of the EMG-studies
56

Discussion ______________________________________________________
performed in musculoskeletal research include less than 20 subjects and 40 subjects must be considered to be in the upper range.
The low load of 10% of MVC in paper II and III could be argued. Since such low loads are common in occupational settings, it must be considered highly relevant for the present research questions. One of the strengths in the experimental studies was the fact that each subject was its own control and that all measures were done the same day. Therefore, the problem of repeatability in contraction, sitting posture, and EMG electrode placement did not exist. Vibration exposure affects grip force. To control this, the grip force was monitored and held constant.
As mentioned in the introduction, a commonly used definition for muscular fatigue is “an exercise-induced reduction in maximal voluntary muscle force” (46). This definition requires that the MVC is observed, until the force no longer can be maintained, known as the failure point. However, concerning sub-maximal contractions, the involved muscles are continuously fatigued from the onset of the contraction without a failure point occurring. This development of muscular fatigue in sub-maximal contractions can be observed by the changes in the EMG signal, such as a shift towards lower frequencies (43). In the present thesis, a failure point in desired force is not investigated, but the above-mentioned changes in the EMG signal were noted. Although some studies argue the use of EMG for assessing muscle fatigue (100), this method was chosen for practical reasons as well as for the possibility to be compared to other studies.
Significant effects of movement artefacts in the data were found in pilot studies prior to paper IV. This was filtered using notch filters. The interference from the cooling fan was filtered in a similar way. The problem with removing movement artefacts is that parts of the true EMG signal will also be removed. However, after the pilot tests, it was concluded that not removing the artefacts would cause a larger error than if they were removed. Method development, for the management of the vibration-evoked movement artifacts would be beneficial. It is important to fully understand and be able to separate movement artefacts from the true synchronized muscle activity that has been suggested in previous studies. Laboratory and simulation experiments could be used to acquire an understanding of this problem.
57

Discussion ______________________________________________________
External validity Because the cross-sectional study included a large number of
the occupational drivers of terrain vehicles in northern Sweden, general conclusions about their increased risks for musculoskeletal symptoms and HAVS can be drawn. Other countries might have different conditions, such as different terrain and vehicles. One must also remember that the epidemiological data here cannot give an answer to the effect of vibration on HAVS and MSDs in the neck and upper limbs, but only the association between driving vehicles with large vibration levels and HAVS and MSDs.
Because the exposure time was only three minutes in the paper II and III and 30s in paper IV, only conclusions about acute effects can be drawn. With increasing exposure time, the results could be different. Only one frequency and amplitude was chosen for each experiment: however, these were based on common work life exposure levels both for HAV and WBV (20). Still, it is important to remember that the papers II-IV are based on experimental data, not field data. In the actual working situation, other risk factors occur, such as long exposure duration, ergonomic factors, and mental stress. Also, in an actual driving situation the grip force varies, and this was standardized and kept constant in the experiment. It is possible that the effect vibration has on the grip force is an important factor in increasing muscle load in the neck and upper limbs for the occupational drivers of terrain vehicles. However, to try to distinguish the effect of vibration, this standardization was necessary. The authentic vibration exposure also consists of several short, high amplitude periods - shocks and jolts. These are also believed to affect musculoskeletal problems.
The experimental studies were performed on young healthy subjects with no experience of occupational driving of terrain vehicles. Being accustomed with vibration exposure as well as possible changes in the muscles caused by long-term vibration exposure might have given different results compared to the ones in the present study. However, to study the vibration on muscular activity the chosen population was believed to be the most suitable.
58

Discussion ______________________________________________________
59
Implications for further research Due to the high prevalence of musculoskeletal disorders in drivers of terrain vehicles, it is critically important to further investigate these types of vibration exposures. Laboratory studies with longer exposure duration as well as vibration including shocks and jolts would give important information that might be linked to the development of musculoskeletal symptoms in the neck and upper limbs. Field studies in drivers of different terrain vehicles are of great interest for understanding the muscle activity during authentic driving. Here ergonomic factors, shocks, stress, etc. could be considered. In addition, to further evaluate gender effects, more typical female professions with vibration exposure must be studied.

Conclusion ______________________________________________________
CONCLUSIONS
These studies demonstrate the following: • Driving terrain vehicles is related to experiencing symptoms
related to hand-arm vibration syndrome, such as numbness sensation of cold and white fingers. Driving terrain vehicles is also related to experiencing musculoskeletal symptoms in the neck, shoulders and wrists. These symptoms seem to be associated with the exposure time (Paper I).
• Short-term exposure to local vibration has no negative effect on the level of fatigue of the upper trapezius muscle as measured by EMG (Paper II).
• Vibration causes an early increase of muscle activity during a sustained, sub-maximal trapezius contraction (Paper III).
• A combination of HAV and WBV gives a higher muscle activity in the trapezius muscle compared to HAV and WBV exposure separately. This might help explain the high prevalence of symptoms in the neck in drivers of terrain and off-road vehicles (Paper IV).
• Clear gender effects do not seem to exist regarding the effect of vibration on muscle activity (Paper II, III, IV).
60

Acknowledgements ______________________________________________________
ACKNOWLEDGEMENTS
Research, just like life, is very much about team work. I could not, and I would not have wanted to finish this thesis on my own. Therefore there are some people that I in one way or another would like to thank; Gunnevi Sundelin, my main supervisor. For your great experience and knowledge in research. For constant support in my project but also for your support in everything related to being a PhD-student. For offering me perfect conditions to learn and to develop. For this I am forever grateful. Lage Burström, my co-supervisor. For your expertise in the field of vibration and for always prioritizing supervision. But also for showing that a good place to grow as a researcher is in a humble and fun environment. Our “Skrivardagar” was an example of this. Stefan Karlsson, my co-supervisor. Without your knowledge in the field of EMG, this project would not have been possible to carry out. Also for inspiring me to critically dissect scientific results, others as well as my own, but also to dare to express new ideas and free speculations. Markus Lindkvist, my co-worker in the lab and co-author. For your unique combination of intelligence and practical skills, humour and sincerity, but also for your pedagogic skills, that comes completely free from prestige. This is rare, and I have valued it during our sometimes long hours in the lab. Monika Edström, my co-worker in the lab. For making weeks of data collection easy and fun. Always things in order, always things on time and with an amazing ability to interact with the test subjects. Also, thank you for all the practical help during my thesis writing. All participants in my studies. Thank you for your contribution to research.
61

Acknowledgements ______________________________________________________
Börje Rehn, for being a good first role model in research when supervising me in my 10-p project, and for continuous interest in my research. Bertil Nordmark, for excellent preparation of the laboratory and for all the assistance. Annelise Müller, for the illustrative images in my papers. Hans Stenlund, Leif Nilsson and Lennart Nilsson, for statistical assistance. My two partners in crime, Sonya ”Hönken” Hörnqvist, Bodil ”Bollis” Björ. My wonderful friends, what would my PhD-time here have been without you to laugh with…and at… I am truly going to miss you, but I will keep amusing you with stories of my funny adventures, even if it’s going to be from a distance. All my PhD-colleagues at the department of Physiotherapy. Thanks for ALL your support and friendship. All my colleagues at the department of Physiotherapy and Occupational Therapy. Without you, work would have been awfully boring. My co-delegates in FUN, for introducing me in a part of research life that not all PhD-student get the opportunity to see. Colleagues in the vibration network and co-authors, Ronnie Lundström and Tohr Nilsson. Other colleagues in the vibration network, Jens Wahlström, Jessica Ljungkvist, and Pernilla Hedlund. All my old friends from Piteå, Matte, Jonny, Annchalotte, Wille, Kicko, Eva, Jenny, Sofia. Thanks for not caring the least about statistical significances, external validity, or about how many of my papers are published. Thanks for being there, thanks for making me happy.
62

Acknowledgements ______________________________________________________
63
My Umeå friends, Jenny, Andreas, Åsa, Une, Anna and Johanna. Thanks for all the wonderful dinners, parties, long walks, training, gossip, etc. In my world, Umeå WAS you. All my friends from all around the world that with their friendship and generosity made my years in Umeå extremely colourful; Lisandro, Tania, Vinicius, Ingela, Kurt, Joan, Nadia, Josefin, Anthony. My family, my mother and Jan-erik. First of all, thanks for ALL the practical help with pretty much everything. But also thanks for the upbringing that made me stay grounded, become independent and to dare to think that everything is possible. My two sisters, Malin and Jeanette, for always being there, for all the hours on the phone and all the fun. My father and Eivor. For always believing in me. My extended family, my grandfather and Vivi, aunt Maud and Janne and cousin Tommy. Thanks for all the dinners and gatherings, and for comments like ”But what do you do…. I mean really.?” It’s refreshing with some common sense in this sometimes strange academic world. Ty, for being you, for being in my life. Financial support for this work was gratefully received from Centre for Environmental Research in Umeå (CMF), The Royal Swedish Academy of Agriculture and Forestry (KSLA), The foundation of mutual accident insurance company “Land och Sjö”, LSR Memorial Foundation, and JC Kempe Memorial Foundation.

References ______________________________________________________
REFERENCES
1. Baldwin ML. Reducing the costs of work-related musculoskeletal disorders: targeting strategies to chronic disability cases. J Electromyogr Kinesiol 2004;14(1):33-41. 2. Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol 2004;14(1):13-23. 3. Borghouts JA, Koes BW, Vondeling H, Bouter LM. Cost-of-illness of neck pain in The Netherlands in 1996. Pain 1999;80(3):629-36. 4. Johansson H, Windhorst U, Djupsjöbacka M, Passatore M. Chronic Work-Related Myalgia - Neuromuscular Mechanisms behind Work-Related Chronic Muscle Pain Syndromes. Gävle: Gävle University Press; 2003. 5. Roquelaure Y, Ha C, Leclerc A, Touranchet A, Sauteron M, Melchior M, et al. Epidemiologic surveillance of upper-extremity musculoskeletal disorders in the working population. Arthritis Rheum 2006;55(5):765-78. 6. Leroux I, Dionne CE, Bourbonnais R, Brisson C. Prevalence of musculoskeletal pain and associated factors in the Quebec working population. Int Arch Occup Environ Health 2005;78(5):379-86. 7. Hagen KB, Magnus P, Vetlesen K. Neck/shoulder and low-back disorders in the forestry industry: relationship to work tasks and perceived psychosocial job stress. Ergonomics 1998;41(10):1510-8. 8. Cote P, Cassidy JD, Carroll L. The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine 1998;23(15):1689-98. 9. Guez M, Hildingsson C, Nilsson M, Toolanen G. The prevalence of neck pain: a population-based study from northern Sweden. Acta Orthop Scand 2002;73(4):455-9. 10. Gummesson C, Isacsson SO, Isacsson AH, Andersson HI, Ektor-Andersen J, Ostergren PO, et al. The transition of reported pain in different body regions--a one-year follow-up study. BMC Musculoskelet Disord 2006;7:17. 11. Larsson B, Sogaard K, Rosendal L. Work related neck-shoulder pain: a review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract Res Clin Rheumatol 2007;21(3):447-63. 12. Sweden S. Arbetsorsakade besvär 2006; 2006.
64

References ______________________________________________________
13. Burstrom L. Konsekvenser av EU-förslaget till "Physiocal agent" direktiv angående vibrationer i arbetslivet. Umeå: Arbetslivsinstitutet; 2001. 14. Wahlstrom J, Burstrom L, Hagberg M, Lundstrom R, Nilsson T. Musculoskeletal symptoms among young male workers and associations with exposure to hand-arm vibration and ergonomic stressors. Int Arch Occup Environ Health 2008;81(5):595-602. 15. Bovenzi M, Zadini A, Franzinelli A, Borgogni F. Occupational musculoskeletal disorders in the neck and upper limbs of forestry workers exposed to hand-arm vibration. Ergonomics 1991;34(5):547-62. 16. Kihlberg S, Hagberg M. Hand-arm symptoms related to impact and nonimpact hand-held power tools. Int Arch Occup Environ Health 1997;69(4):282-8. 17. Palmer KT, Griffin MJ, Syddall HE, Pannett B, Cooper C, Coggon D. Exposure to hand-transmitted vibration and pain in the neck and upper limbs. Occup Med (Lond) 2001;51(7):464-7. 18. Magnusson ML, Pope MH, Wilder DG, Areskoug B. Are occupational drivers at an increased risk for developing musculoskeletal disorders? Spine 1996;21(6):710-7. 19. Robb MJ, Mansfield NJ. Self-reported musculoskeletal problems amongst professional truck drivers. Ergonomics 2007;50(6):814-27. 20. Rehn B. Musculoskeletal Disorders and Whole-body Vibration Exposure. Umeå: Umeå University; 2004. 21. Griffin MJ. Handbook of Human Vibration. London: Academic Press Limited; 1996. 22. Griffin MJ, Welsh AJ, Bovenzi M. Acute response of finger circulation to force and vibration applied to the palm of the hand. Scand J Work Environ Health 2006;32(5):383-91. 23. ISO. Mechanical vibration and shock - evaluation of human exposure to whole-body vibration Part 1: General requirements. Geneva, Switzerland, 1997. 24. ISO. Mechanical vibration - Measurement and evaluation of human exposure to hand-transmitted vibration - Part 1: General requirements. Geneva, Switzerland, 2001. 25. Eklund G, Hagbarth KE. Motor effects of vibratory muscle stimuli in man. Electroencheph. clin. Neurophysiol. 1965;19:619. 26. Wilder DG, Woodworth BB, Frymoyer JW, Pope MH. Vibration and the human spine. Spine 1982;7(3):243-54.
65

References ______________________________________________________
27. Panjabi MM, Andersson GB, Jorneus L, Hult E, Mattsson L. In vivo measurements of spinal column vibrations. J Bone Joint Surg Am 1986;68(5):695-702. 28. Fard MA, Ishihara T, Inooka H. Identification of the head-neck complex in response to trunk horizontal vibration. Biol Cybern 2004;90(6):418-26. 29. Hazarin B, Grzesik J. The transmission of vertical whole-body vibration to the body segments of standing subjects. Journal of Sound and Vibration 1998;215(4):775-787. 30. Bovenzi M, Lindsell CJ, Griffin MJ. Acute vascular responses to the frequency of vibration transmitted to the hand. Occup Environ Med 2000;57(6):422-30. 31. Harada N, Kondo H, Kimura K. Assessment of autonomic nervous function in patients with vibration syndrome using heart rate variation and plasma cyclic nucleotides. Br J Ind Med 1990;47(4):263-8. 32. Bjor B, Burstrom L, Karlsson M, Nilsson T, Naslund U, Wiklund U. Acute effects on heart rate variability when exposed to hand transmitted vibration and noise. Int Arch Occup Environ Health 2007;81(2):193-9. 33. Bovenzi M. A follow up study of vascular disorders in vibration-exposed forestry workers. Int Arch Occup Environ Health 2008;81(4):401-8. 34. Bovenzi M, Della Vedova A, Nataletti P, Alessandrini B, Poian T. Work-related disorders of the upper limb in female workers using orbital sanders. Int Arch Occup Environ Health 2005;78(4):303-10. 35. Jang JY, Kim S, Park SK, Roh J, Lee TY, Youn JT. Quantitative exposure assessment for shipyard workers exposed to hand-transmitted vibration from a variety of vibration tools. AIHA J (Fairfax, Va) 2002;63(3):305-10. 36. Necking L. Vibration-induced muscle injury in the hand. Malmö: Lund; 2003. 37. Koda S, Yasuda N, Sugihara Y, Ohara H, Udo H, Otani T, et al. [Analyses of work-relatedness of health problems among truck drivers by questionnaire survey]. Sangyo Eiseigaku Zasshi 2000;42(1):6-16. 38. Okunribido OO, Magnusson M, Pope MH. The role of whole body vibration, posture and manual materials handling as risk factors for low back pain in occupational drivers. Ergonomics 2008;51(3):308-29.
66

References ______________________________________________________
39. Tortora GJ, Grabowski SR. Principles of Anatomy and Physiology. 8th ed. New York: Harper Collins College Publishers INC.; 1996. 40. Basmajian J, DeLuca CJ. Muscles Alive - Their Functions Revealed by Electromyography. 5 ed. Baltimore: Williams & Williams; 1985. 41. Henneman E. Relation between size of neurons and their susceptibility to discharge. Science 1957;126(3287):1345-7. 42. Chaffin DB. Localized muscle fatigue--definiton and measurement. J Occup Med 1973;15(4):346-54. 43. De Luca CJ. Myoelectrical manifestations of localized muscular fatigue in humans. Crit. Rev. Biomed. Eng. 1984;11(4):251-279. 44. Edwards RH, Hill DK, Jones DA, Merton PA. Fatigue of long duration in human skeletal muscle after exercise. J Physiol 1977;272(3):769-78. 45. Sjogaard G, Sogaard K. Muscle injury in repetitive motion disorders. Clin Orthop Relat Res 1998(351):21-31. 46. Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev 2001;81(4):1725-89. 47. Pattichis CS, Schofield I, Merletti R, Parker PA, Middleton LT. Introduction to this special issue. Intelligent data analysis in electromyography and electroneurography. Med Eng Phys 1999;21(6-7):379-88. 48. Merletti R, Knaflitz M, DeLuca CJ. Electrically evoked myoelectric signals. Crit Rev Biomed Eng 1992;19(4):293-340. 49. Dimitrova NA, Dimitrov GV. Interpretation of EMG changes with fatigue: facts, pitfalls, and fallacies. J Electromyogr Kinesiol 2003;13(1):13-36. 50. Hägg G, Luttman A, Jäger M. Methodologies for evaluating electromyographic field data in ergonomics. J Electromyogr Kinesiol 2000;10:301-312. 51. Seroussi RE, Wilder DG, Pope MH. Trunk muscle electromyography and whole body vibration. J Biomech 1989;22(3):219-29. 52. Seidel H. Myoelectric reactions to ultra-low frequency and low-frequency whole body vibration. Eur J Appl Physiol Occup Physiol 1988;57(5):558-62. 53. Wos H, Svensson LB, Norlander S. Implementation of double-pulsed holography in evaluation of whole-body vibration. Ergonomics 1991;34(11):1357-64.
67
References ______________________________________________________
54. Thuresson M. On neck load among helicopter pilots - effect of head worn equipment, whole body vibration and neck position. Stockholm: Karolinska Institutet; 2005. 55. Bluthner R, Seidel H, Hinz B. Myoelectric response on back muscles to vertical random whole-body vibration with different magnitudes at different postures. Journal of Sound and Vibration 2002;253(1):37-56. 56. De Oliviera CG, Simpson DM, Nadal J. Lumbar back muscle activity of helicopter pilots and whole-body vibration. Journal of Biomechanics 2001;34:1309-1315. 57. De Oliveira CG, Nadal J. Back muscle EMG of helicopter pilots in flight: effects of fatigue, vibration, and posture. Aviat Space Environ Med 2004;75(4):317-22. 58. Blüthner R, Seidel H, Hinz B, Schust M. Timing of back muscles during whole-body vibration with transients - its significance for the internal spinal load. In: UK groupmeeting on human respons to vibration 17-19; 1997; University of Southampton, England; 1997. 59. Zimmermann CL, Cook TM, Goel VK. Effects of seated posture on erector spinae EMG activity during whole body vibration. Ergonomics 1993;36(6):667-75. 60. Zimmermann CL, Cook TM. Effects of vibration frequency and postural changes on human responses to seated whole-body vibration exposure. Int Arch Occup Environ Health 1997;69(3):165-79. 61. Dupuis H, Hartung E, Haverkamp M. Acute effects of transient vertical whole-body vibration. Int Arch Occup Environ Health 1991;63(4):261-5. 62. Blüthner R, Hinz B, Menzel B, Seidel H. Back muscle response to transient whole-body vibration. International Journal of Industrial Ergonomics 1993;12:49-59. 63. Hansson T, Magnusson M, Broman H. Back muscle fatigue and seated whole body vibrations: an experimental study in man. Clinical Biomechanics 1991;6:173-178. 64. Kuorinka I, Jonsson B, Kilbom Å, Vinteberg H, Biering-Sörensen F, Andersson G, et al. Standardised nordic Questionnaires for the analysis of musculoskeletal symptoms. Applied Ergonomics 1987;18:233-237. 65. Jensen C, Vasseljen O, Westgaard RH. The influence of electrode position on bipolar surface electromyogram recordings of the upper trapezius muscle. Eur J Appl Physiol Occup Physiol 1993;67(3):266-73.
68

References ______________________________________________________
66. Hermens H, Freriks B, Merletti R, Stegemann D, Blok J, Rau G, et al. SENIAM; European recommendations for surface electromyography.: Roessing: Research and Development.; 1999. 67. Karlsson JS, Bäcklund T, Edström U. A New Wireless Multi-Channel Data System for Acquisition and Analysis of Physiological Signals. In: Proceedings of the 17th International Symposium on Biotelemetry; 2003; Brisbane, Australia; 2003. 68. Council E. Directive 2002/44/EC of the European parliament and of the Council of 25 June 2002 on the minimum health and safety requirements regarding the exposure of workers to the risks rising from physical gents (vibration) (sixteenth individual Directive within the meaning of Article 16(1) of Directive 89/391/EEC). Off J Europ Communities 2002;L 177:13-19. 69. Borg GA. Perceived exertion. Exerc Sport Sci Rev 1974;2:131-53. 70. Anttonen H, Virokannas H, Niskanen J. Hand-arm vibration and terrain vehicles. Central European Journal of Public Health 1995;53(3):29-34. 71. Mirbod SM, Yoshida H, Jamali M, Masamura K, Inaba R, Iwata H. Assessment of hand-arm vibration exposure among traffic police motorcyclists. Int Arch Occup Environ Health 1997;70(1):22-8. 72. Burström L, Olofsson B. Hand-armvibrationer i terränggående fordon. Umeå: National Institute for Working Life; 2001. Report No.: 2001:4. 73. Goglia V, Gospodaric Z, Kosutic S, Filipovic D. Hand-transmitted vibration from the steering wheel to drivers of a small four-wheel drive tractor. Appl Ergon 2003;34(1):45-9. 74. Coorevits P, Danneels L, Ramon H, Druyts H, De Craecker W, Cambier D, et al. Surface EMG analysis of the effects of whole-body vibrations on localized back muscle fatigue. In: 3rd international Conference on Whole-Body Vibration injuries; 2005; Nancy, France; 2005. 75. McBride JM, Porcari JP, Scheunke MD. Effect of vibration during fatiguing resistance exercise on subsequent muscle activity during maximal voluntary isometric contractions. J Strength Cond Res 2004;18(4):777-81. 76. Henneman E, Olson CB. Relations between Structure and Function in the Design of Skeletal Muscles. J Neurophysiol 1965;28:581-98.
69

References ______________________________________________________
77. Ushiyama J, Masani K, Kouzaki M, Kanehisa H, Fukunaga T. Difference in aftereffects following prolonged Achilles tendon vibration on muscle activity during maximal voluntary contraction among plantar flexor synergists. J Appl Physiol 2005;98(4):1427-33. 78. Grande G, Cafarelli E. Ia Afferent input alters the recruitment thresholds and firing rates of single human motor units. Exp Brain Res 2003;150(4):449-57. 79. Martin BJ, Park HS. Analysis of the tonic vibration reflex: influence of vibration variables on motor unit synchronization and fatigue. Eur J Appl Physiol Occup Physiol 1997;75(6):504-11. 80. Shinohara M. Effects of prolonged vibration on motor unit activity and motor performance. Med Sci Sports Exerc 2005;37(12):2120-5. 81. Kerschan-Schindl K, Grampp S, Henk C, Resch H, Preisinger E, Fialka-Moser V, et al. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin Physiol 2001;21(3):377-82. 82. Bovenzi M, Griffin MJ, Ruffell CM. Vascular responses to acute vibration in the fingers of normal subjects. Cent Eur J Public Health 1995;3 Suppl:15-8. 83. Park HS, Martin BJ. Contribution of the tonic vibration reflex to muscle stress and muscle fatigue. Scand J Work Environ Health 1993;19(1):35-42. 84. Mottram CJ, Maluf KS, Stephenson JL, Anderson MK, Enoka RM. Prolonged vibration of the biceps brachii tendon reduces time to failure when maintaining arm position with a submaximal load. J Neurophysiol 2006;95(2):1185-93. 85. Bongiovanni LG, Hagbarth KE. Tonic vibration reflexes elicited during fatigue from maximal voluntary contractions in man. J Physiol 1990;423:1-14. 86. Griffin L, Garland SJ, Ivanova T, Gossen ER. Muscle vibration sustains motor unit firing rate during submaximal isometric fatigue in humans. J Physiol 2001;535(Pt 3):929-36. 87. Rohmert W, Wos H, Norlander S, Helbig R. Effects of vibration on arm and shoulder muscles in three body postures. Eur J Appl Physiol Occup Physiol 1989;59(4):243-8. 88. Bosco C, Cardinale M, Tsarpela O. Influence of vibration on mechanical power and electromyogram activity in human arm flexor muscles. Eur J Appl Physiol Occup Physiol 1999;79(4):306-11. 89. Bluthner R, Seidel H, Hinz B. Examination of the myoelectric activity of back muscles during random vibration--methodical
70

References ______________________________________________________
71
approach and first results. Clin Biomech (Bristol, Avon) 2001;16 Suppl 1:S25-30. 90. Griffin MJ. Vertical vibration of seated subjects: effects of posture, vibration level, and frequency. Aviat Space Environ Med 1975;46(3):269-76. 91. Pope MH, Magnusson M, Hansson T. The upper extremity attenuates intermediate frequency vibrations. J Biomech 1997;30(2):103-8. 92. Capicikova N, Rocchi L, Hlavacka F, Chiari L, Cappello A. Human postural response to lower leg muscle vibration of different duration. Physiol Res 2006;55 Suppl 1:S129-34. 93. Slota GP, Granata KP, Madigan ML. Effects of seated whole-body vibration on postural control of the trunk during unstable seated balance. Clin Biomech (Bristol, Avon) 2008;23(4):381-6. 94. Wierzbicka MM, Gilhodes JC, Roll JP. Vibration-induced postural posteffects. J Neurophysiol 1998;79(1):143-50. 95. Roll JP, Vedel JP, Ribot E. Alteration of proprioceptive messages induced by tendon vibration in man: a microneurographic study. Exp Brain Res 1989;76(1):213-22. 96. Simoneau JA, Bouchard C. Human variation in skeletal muscle fiber-type proportion and enzyme activities. Am J Physiol 1989;257(4 Pt 1):E567-72. 97. Lindman R, Eriksson A, Thornell LE. Fiber type composition of the human male trapezius muscle: enzyme-histochemical characteristics. Am J Anat 1990;189(3):236-44. 98. Lindman R, Eriksson A, Thornell LE. Fiber type composition of the human female trapezius muscle: enzyme-histochemical characteristics. Am J Anat 1991;190(4):385-92. 99. Falla D, Dall'Alba P, Rainoldi A, Merletti R, Jull G. Repeatability of surface EMG variables in the sternocleidomastoid and anterior scalene muscles. Eur J Appl Physiol 2002;87(6):542-9. 100. Vollestad NK. Measurement of human muscle fatigue. J Neurosci Methods 1997;74(2):219-27.

Dissertations ______________________________________________________
Dissertations written by physiotherapists, Umeå University 1989–2008 Birgitta Bergman Being a physiotherapist - Professional role, utilization of time and vocational strategies. Umeå University Medical Dissertations, New Series no 251, 1989 (Department of Physical Medicine and Rehabilitation) Inger Wadell Influences from peripheral sense organs on primary and secondary spindle afferents via gamma-motoneurones - A feedback mechanism for motor control and regulation of muscle stiffness. Umeå University Medical Dissertations, New Series no 307, 1991 (Department of Physiology) Jessica Elert The pattern of activation and relaxation during fatiguing isocinetic contractions in subjects with and without muscle pain. Arbete och hälsa 1991:47. Diss. 1992 (sammanfattning). (Departments of Clinical Physiology, National Institute of Occupational Health and Physical Medicine and Rehabilitation) Gunnevi Sundelin Electromyography of shoulder muscles - The effects of pauses, drafts and repetitive work cycles. Arbete och Hälsa, 1992:16. Diss. (sammanfattning). (Departments of Anatomy, National Institute of Occupational Health, Division of Work and Environmental Physiology, Divisions of Occupational Medicine and Applied Work Physiology and Occupational Medicine) Birgit Rösblad Visual and proprioceptive control of arm movement - Studies of development and dysfunction. Diss. (sammanfattning) 1994 (Department of Paediatrics) Charlotte Häger-Ross To grip and not to slip - Sensorimotor mechanisms during reactive control of grasp stability. Umeå University Medical Dissertations, New Series no 429, 1995 (Department of Physiology) Lars Nyberg Falls in the frail elderly – Incidence, characterics and prediction with special reference to patients with stroke and hip fractures. Umeå Medical Dissertations, New Series no 483, 1996 (Department of Geriatric Medicine) Margareta Barnekow-Bergkvist Physical capacity, physical activity and health -A population based fitness study of adolescents with an 18-year follow-up. Umeå University Medical Dissertations, New Series no 494, 1997 (Departments of Physiology and Technology, National Institute for Working Life and Epidemiology and Public Health)
72

Dissertations ______________________________________________________
Britta Lindström Knee muscle function in healthy persons and patients with upper motor neurone syndrome. Umeå University Medical Dissertations, New Series no 505, 1997 (Departments of Physical Medicine and Rehabilitation and Clinical Neuroscience) Monica Mattsson Body Awareness - applications in physiotherapy. Umeå University Medical Dissertations, New Series no 543, 1998 (Departments of Psychiatry and Family Medicine) Hildur Kalman The structure of knowing. Existential trust as an epistemological category. Umeå studies in the humanities, 145, 1999 (Department of Philosophy and Linguistics) Lillemor Lundin-Olsson Prediction and prevention of falls among elderly people in residential care. Umeå University Medical Dissertations, New Series no 671, 2000 (Departments of Community Medicine and Rehabilitation, Physiotherapy and Geriatric Medicine) Christina Ahlgren Aspects of rehabilitation – with focus on women with trapezius myalgia Umeå University Medical Dissertations, New Series no 715, 2001 (Department of Public Health and Clinical Medicine, Occupational Medicine) Ann Öhman Profession on the move - changing conditions and gendered development in physiotherapy. Umeå University Medical Dissertations, New series No 730, 2001 (Departments of Community Medicine and Rehabilitation, Physiotherapy and Public Health and Clinical Medicine, Epidemiology) Hamayun Zafar Integrated jaw and neck function in man: studies of mandibular and head-neck movements during jaw opening-closing tasks. (Department of Odontology, Clinical Oral Physiology and Centre for Musculoskeletal Research, National Institute for Working Life, Umeå) Kerstin Söderman The female soccer player – Injury pattern, risk factors and intervention. Umeå University Medical Dissertations, New series no 735, 2001 (Departments of Surgical and Perioperative Sciences, Sports Medicine, and Community Medicine and Rehabilitation, Physiotherapy) Lena Grönblom-Lundström Rehabilitation in light of different theories of health. Outcome for patients with low-back complaints – a theoretical discussion. Umeå University Medical Dissertations, New series no 760, 2001 (Departments of Public Health and Clinical Medicine, Epidemiology, and Community Medicine and Rehabilitation, Social Medicine)
73

Dissertations ______________________________________________________
Kerstin Waling Pain in women with work-related trapezius myalgia. Intervention effects and variability. Umeå University Medical Dissertations, New series no 762, 2001 (Departments of Public Health and Clinical Medicine, Occupational Medicine, and Community Medicine and Rehabilitation, Physiotherapy) Eva-Britt Malmgren-Olsson Health problems and treatment effects in patients with non-specific musculoskeletal disorders. A comparitson between Body Awareness Therapy, Feldenkrais and Individual Physiotherapy. Umeå University Medical Dissertations, New series no 774, 2002 (Department of Community Medicine and Rehabilitation, Physiotherapy and Department of Psychology) Jane Jensen Fall and injury prevention in older people living in residential care facilities. Umeå University Medical Dissertations, New series no 812, 2003 (Department of Community Medicine and Rehabilitation, Physiotherapy and Geriatric Medicine) Anncristine Fjellman-Wiklund Musicianship and teaching. Aspects of musculoskeletal disorders, physical and psychosocial work factors in musicians with focus on music teachers. Umeå University Medical Dissertations, New series no 825, 2003 (Department of Community Medicine and Rehabilitation, Physiotherapy) Börje Rehn Musculoskeletal disorders and whole-body vibration exposure among professional drivers of all-terrain vehicles. Umeå University Medical Dissertations, New series no 852, 2004 (Department of Public Health and Clinical Medicine, Occupational Medicine) Martin Björklund Effects on repetitive work on proprioception and of stretching on sensory mechanisms. Implications for work-related neorumuscular disorders. Umeå University Medical Dissertations, New series no 877, 2004 (Departments of Surgical and Perioperative Sciences, Sports Medicine Unit, Umeå University, The Center for Musculoskeletal Reseach, University of Gävle, Umeå, and Alfta Forskningsstiftelse, Alfta) Karin Wadell Physical training in patients with chronic obstructive pulmonary disease – COPD. Umeå University Medical Dissertations, New series no 917, 2004 (Departments of Community Medicine and Rehabilitation, Physiotherapy; Public Health and Clinical Medicine, Respiratory Medicine and Allergy, Surgical and Perioperative Sciences, Sports Medicine)
74

Dissertations ______________________________________________________
Peter Michaelson Sensorimotor characteristics in chronic neck pain. Possible pathophysiological mechanisms and implications for rehabilitation. Umeå University Medical Dissertations, New series no 924, 2004 (Departments of Surgical and Perioperative Sciences, Sports Medicine Unit, University of Umeå, Southern Lappland Research Department, Vilhelmina, Centre for Musculoskeletal Research, University of Gävle, Umeå) Ulrika Aasa Ambulance work. Relationships between occupational demands, individual characteristics and health related outcomes. Umeå University Medical Dissertations, New series no 943, 2005 (Department of Surgical and Perioperative Sciences, Sports Medicine and Surgery, University of Umeå and Centre for Musculoskeletal Research, University of Gävle) Ann-Katrin Stensdotter Motor Control of the knee. Kinematic and EMG studies of healthy individuals and people with patellofemoral pain. Umeå University Medical Dissertations, New series no 987, 2005 (Departments of Community Medicine and Rehabilitation, Physiotherapy) Tania Janaudis Ferreira Aspects of muscle function and training with oxygen in patients with chronic obstructive pulmonary disease – COPD. Umeå University Licentiate Thesis, 2005 (Department of Community Medicine and Rehabilitation, Physiotherapy) Erik Rosendahl Fall prediction and a high-intensity functional exercise programme to improve physical functions and to prevent falls among older people living in residential care facilities. Umeå University Medical Dissertations, New Series No 1024, 2006 (Department of Community Medicine and Rehabilitation, Geriatric Medicine and Physiotherapy) Michael Stenvall Hip fractures among old people. Their prevalence, consequences and complications and the evaluation of a multi-factorial intervention program designed to prevent falls and injuries and enhance performance of activities of daily living. Umeå University Medical Dissertations, New Series No 1040, 2006 (Department of Community Medicine and Rehabilitation, Geriatric Medicine and Physiotherapy) Petra von Heideken Wågert Health, physical ability, falls and morale in very old people: the Umeå 85+ Study. Umeå University Medical Dissertations, New Series No 1038, 2006 (Department of Community Medicine and Rehabilitation, Geriatric Medicine and Physiotherapy)
75

Dissertations ______________________________________________________
76
Gerd Flodgren Effect of low–load repetitive work and mental load on sensitising substances and metabolism in the trapezius muscle. Umeå University Medical Dissertations, New series no 1130, 2007 (Department of Surgical and Perioperative Sciences, Sports Medicine Unit, Umeå University, Centre of Musculoskeletal Research, University of Gävle, Umeå, and the Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, Umeå Sweden) Staffan Eriksson Falls in people with dementia. Umeå University Medical Dissertations, New series no 1135, 2007 (Department of Community Medicine and Rehabilitation, Physiotheraphy and Geriatric Medicine, Umeå University, Umeå, Sweden) Jonas Sandlund Position-matching and goal-directed reaching acuity of the upper limb in chronic neck pain: Associations to self-rated characteristics. Umeå University Medical Dissertations, New series no 1182, 2008 (Department of Surgical and Perioperative Sciences, Sports Medicine Unit, Umeå University, Centre of Musculoskeletal Research, University of Gävle, Umeå)