the executive connection of north texas // summer 2014
DESCRIPTION
ÂTRANSCRIPT

SUMMER 2014
THENEWPARKLAND
Developing Fellow ReferencesAdvancing the Health of North TexansACHENTX’s Newest Fellows

4 President’sMessage JohnFloren,FACHE
4 Regent’sMessage MichaelDMurphy,FACHE
5 NationalNews
13 PathtoBecoming aFACHE
17 EventEncore
18 NewFellows&NewMembers
19 UpcomingEvents
F E A T U R E S

A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMERR 2014 3
The ACHE of North Texas e-magazine, The Executive Connection, is published quarterly (Spring, Summer, Fall and Winter) and includes information on the latest regulatory and legislative developments, as well as the quality improvement and leadership trends that are shaping and influencing the healthcare industry. Readers get indepth reporting on the issues and challenges facing hospital and health system leaders today. We make it our job to tell you about the great things the organization and Chapter are doing every day to ensure the health of our community. If you have any news and updates that you want to share with other members, please e-mail your items to [email protected]. Microsoft Word or compatible format is preferable. If you have a graphic or picture that you'd like to include, please send it as a separate file. The following are the types of information that our members shared in past ACHE of North Texas magazines, Advocacy Issues, Legislative Issues, Educational Opportunities, Awards / Achievements, Promotions (Members On the Move), Committee Updates, journal submissions, conference submissions, and workshop participations, sharing mentoring experiences, etc.
Editor-In-Chief John G. Allen, MHA, MPH, FACHE
Managing Director Joan Shinkus Clark, DNP, RN, NEA-BC, CENP, FACHE, FAANContributing Editor Lisa Cox
Contributing Writers Fraser Hay, FACHE John Allen Joan Clark Amanda Bloom Jonathan Leer Amanda O’Neal Brumitt, FACHE Micaela Dulin
Creative Direction Caleb Wills
Advertising/ Subscriptions [email protected]
Questions and Comments: ACHE of North Texas Editorial Office, c/o Executive Connection 250 Decker Drive | Irving, TX 75062 p: 972.413.8144 e: [email protected] w: northtexas.ache.org
2014 Chapter Officers
President Josh Floren, FACHE Texas Health Presbyterian Hospital Plano
Past President Caleb F. O’Rear, FACHE Denton Regional Medical Center
President-Elect Winjie Tang Miao Texas Health Harris Methodist Hospital Alliance
Secretary Dresdene Flynn White, FACHE John Peter Smith Health Network
Treasurer Pam Stoyanoff Methodist Health System
Regent Michael D. Murphy, FACHE Abilene Regional Medical Center
2014 Board of Directors
Teresa Baker, FACHEJohn Peter Smith Health Network
Jessica Fuhrman, FACHEBroadJump
Forney FlemingUniversity of Texas at Dallas
Jay FoxBaylor Medical Center - Waxahachie
Michael Hicks, MD, FACHE Pinnacle Anesthesia Consultants
Janet Holland, MSHA, MBA, FACHE BroadJump
Kristin Jenkins, JD, FACHEDFW Hospital Council Foundation
Kevin Stevenson, FACHE ERDMAN
Demetria WilhiteUniversity of Texas at Arlington
Chip Zahn, FACHESurgical Care Affiliates
Lisa CoxChapter Coordinator

4 A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMER 2014
President’s Message
Did you know?... ACHE offers online resources regarding post graduate fellowships at www.ache.org/ PostGrad. The site is great for organizations seeking to develop a postgraduate fellowship, organizations that want to find the best candidate and students looking for a fellowship opportunity. ACHE and leaders throughout our industry believe that postgraduate fellowships are essential to attract and develop highly qualified healthcare management professionals and we hope you will take moment to check it out.
We look forward to seeing you all over the next few months and as always we welcome your feedback by emailing us at [email protected].
SincerelyJosh Floren, FACHE
hope you have all had a great summer and are looking forward to cooler weather. The fall season
is right around the corner and it’s time to prepare our projections for the year end as well and start planning for the next. For those of you planning to achieve your fellow credential, we have review courses as well as a “lending library” for your Board of Governors exam preparation. We are also still providing reimbursement of the $250 application fee for the first 10 Chapter members who pass the exam before October 31st We hope you will consider advancing to fellow in the College this year.
The North Texas ACHE Chapter has not taken this summer off. Over the past several months we have worked to improve our chapter by setting up many exciting fall events that we believe you will enjoy. If its breakfast with a local CEO, a women in leadership event, a cluster event with the Texas Association for Healthcare Quality or a community service event we have it coming this fall. We have also been working to create a new web image and we are proud to announce that our new website is now active. Please take a moment and visit the new site at www.achentx.org. You will find details on all our upcoming events as well as additional information about our chapter.
I
A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMERR 2014 5
The cluster educational events have been extremely successful in 2014, generating record attendance. Based on this response, we are moving to quarterly educational cluster events in 2015. These cluster events will allow members to get more bang for their buck, obtaining 3 Face to Face credits at one time!
Starting in the late afternoon and ending at 7:30 pm, members can still get home to spend time with their families. The committee is also working on developing a local program council to bring educational events to surrounding communities within the North Texas Chapter. The North Texas Chapter covers 19 counties and the committee wants to provide educational opportunities to more members closer to home.
Please vote for the location that is most appealing to you for the creation of a local program council:Denton / Weatherford / Waxahachie Amanda Bloom and Corey Wilson, Education Committee Chairs
The Shift to Cluster Events and a LPC
Greetings to all of my ACHE Colleagues across northern Texas:
I am pleased to relay to you a number of educational and social events coming soon to northern Texas.
The Texas Midwest Healthcare Executives (TMHE) Chapter is hosting a 12-hour Face-to-Face Educational Program on Sept. 18-19 in Lubbock. The topic is “Emerging Trends in Healthcare: Preparing for Tomorrow Today.” This is a great way to get 12 hours of ACHE Face-to-Face credit right here in Texas. Registration is $550 if done before 9/2, $650 if completed before 9/17, and $700 onsite (but space is limited). For more information, contact Chapter President [email protected] or call Julie at (325) 641-0463.
The ACHE of North Texas Chapter has several events over the next few weeks.
ACHENTX is sponsoring an After-Hours Networking Event at Fort Worth Botanical Gardens on Sept 11.
ACHENTX is also sponsoring a Fall Cluster Event that includes
Regent’s Messageseveral topics on Sept. 18 at Medical City Dallas, and participation will earn 3 hours of ACHE Face-to-Face credit.And ACHENTX is also developing a Board of Governors Review Course that will be at Texas Health Arlington Memorial Hospital on Sept 19. Registration for this educational event is open now.
For more information about any of these ACHENTX sponsored events, go to [email protected].
These are all great opportunities to network with your professional colleagues across north Texas, as well as a means of growing professionally and earn Face-to-Face credits that we all need for ACHE.
I remain honored to serve as your Regent for all three ACHE Chapters that span north Texas: the Texas Midwest Healthcare Executives, ACHE of North Texas, and the East Texas ACHE Forum. Please don’t hesitate to contact me if I can be of service to you.
Michael D. Murphy, FACHERegent for Texas - Northern
6 A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMER 2014
In July2014, Parkland Health & Hospital System received a temporary certificate of substantial completion from the City of Dallas for the new Parkland Hospital. With that
hurdle cleared, Parkland began work on the final punch list and transition planning into the new campus. The completion of the 862-bed facility marks yet another expansion milestone for a hospital that originally opened in 1894. Parkland Hospital is one of the busiest public hospitals in the nation. Located in Dallas County, one of the largest and fastest growing regions in the country, Parkland receives more than 1 million patient visits per year and saw an increase in ambulatory business by more than 200,000 patients last year.
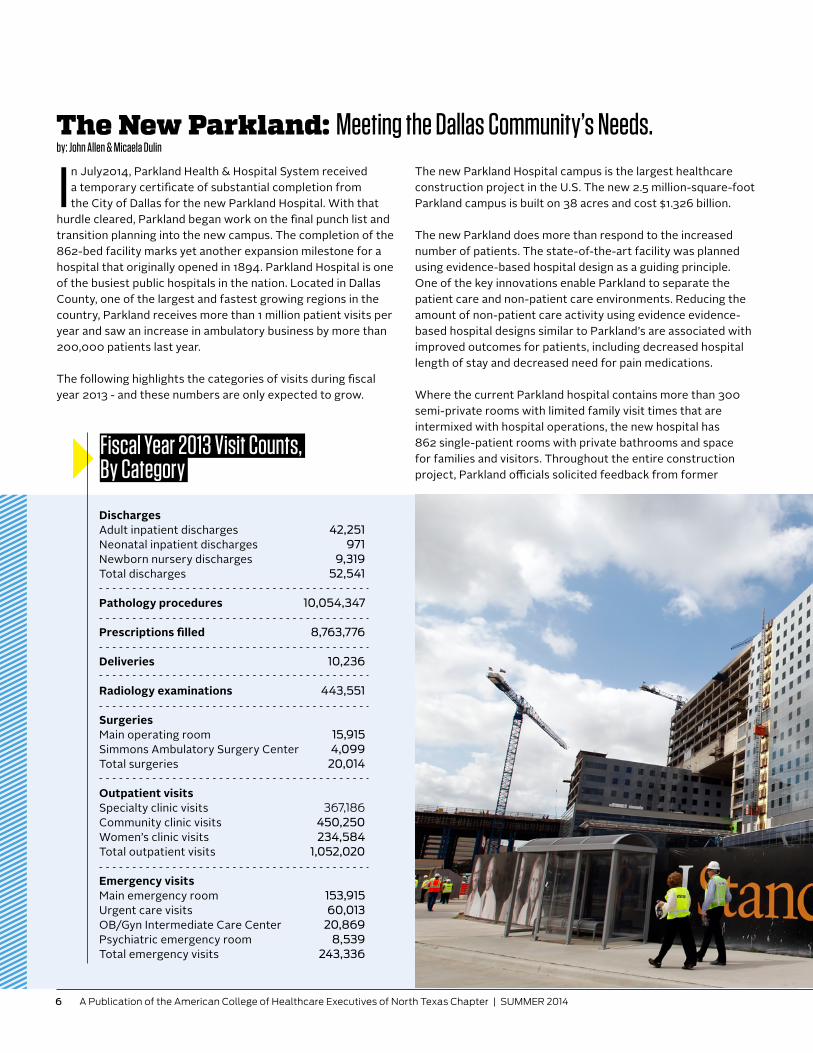
The following highlights the categories of visits during fiscal year 2013 - and these numbers are only expected to grow.
The New Parkland: Meeting the Dallas Community’s Needs.by: John Allen & Micaela Dulin
The new Parkland Hospital campus is the largest healthcare construction project in the U.S. The new 2.5 million-square-foot Parkland campus is built on 38 acres and cost $1.326 billion.
The new Parkland does more than respond to the increased number of patients. The state-of-the-art facility was planned using evidence-based hospital design as a guiding principle. One of the key innovations enable Parkland to separate the patient care and non-patient care environments. Reducing the amount of non-patient care activity using evidence evidence-based hospital designs similar to Parkland’s are associated with improved outcomes for patients, including decreased hospital length of stay and decreased need for pain medications.
Where the current Parkland hospital contains more than 300 semi-private rooms with limited family visit times that are intermixed with hospital operations, the new hospital has 862 single-patient rooms with private bathrooms and space for families and visitors. Throughout the entire construction project, Parkland officials solicited feedback from former
DischargesAdult inpatient discharges 42,251Neonatal inpatient discharges 971Newborn nursery discharges 9,319Total discharges 52,541
Pathology procedures 10,054,347
Prescriptions filled 8,763,776
Deliveries 10,236
Radiology examinations 443,551
SurgeriesMain operating room 15,915Simmons Ambulatory Surgery Center 4,099Total surgeries 20,014
Outpatient visitsSpecialty clinic visits 367,186Community clinic visits 450,250Women’s clinic visits 234,584Total outpatient visits 1,052,020
Emergency visitsMain emergency room 153,915Urgent care visits 60,013OB/Gyn Intermediate Care Center 20,869Psychiatric emergency room 8,539Total emergency visits 243,336
Fiscal Year 2013 Visit Counts, By Category

1990s when the Dallas County Commissioners commissioned a Blue Ribbon Panel to look at the aging facility. The panel’s findings were unanimous – the 1950s-vintagehospital needed to be replaced. In 2008, Dallas County taxpayers overwhelmingly – by 82 percent – approved a bond to replace the current facility.
In Spring 2009, contractors were brought on board to begin planning the design and construction of the new Parkland hospital. HDR Architects and Corgan Associates were hired to serve as the Parkland master architecture firm and BARA (a joint venture between Balfour Beatty Construction, Austin Commercial, H.J. Russell & Company and Azteca Enterprises) was hired to serve as the Parkland master construction manager.
In January 2011, the hospital schematic design was approved by the Parkland Board of Managers. The hospital construction was started and early release of site work and foundations had already begun in October 2010. HDR Architects and Corgan Associates and BARA employed two Lean principles that were essential to the construction: prefabrication and pull planning. The pre-fabrication process consisted of building structures at a separate site and delivering to the hospital construction site once the structure was assembled. The pull planning process was used to establish milestones for hospital construction.
The prefabrication strategy headed by BARA was focused on building horizontal mechanical, electrical and plumbing modules away from the Parkland construction site. This approach provided cost savings, improved product quality, reduced congestion in the construction zone and improved quality control during module construction. Lou Saksen, Senior Vice President of New Parkland Construction at Parkland, described how more than 800 bathrooms were prefabricated at the logistics center, across the street from the Parkland construction site. “The prefabrication process allowed us to completely develop each bathroom at the logistics center – the tiles and fixtures, and even flood testing. Once the bathrooms were completed, they were ready for delivery and installation at the construction site.”
The pull planning process was used by BARA to establish milestones for the hospital construction project. Planning was broken into four different phases: site, structural, skin
patients and their families to validate their design concepts. Parkland also incorporated increased natural lighting and a wellness garden to further enhance patient satisfaction and recovery by providing enhanced access to nature.
The hospital is one of the first to incorporate on-stage/off-stage areas where hospital staff transport, supplies and hold conferences to discuss patient care with other staff in an area completely away from patients and visitors. This keeps the noise level lowered for patients and reduces the risk of accidental disclosure of confidential patient information.
Parkland has invested $80 million in IT infrastructure and $90 million in medical equipment. The entire facility from hospital beds, to cameras, fire alarms, and operating suites and radiology are being transformed into a digital environment where IT will form the backbone. This is new for many hospitals and Parkland is one of the first to fully implement digital technology in all areas of the facility. Per the words of Ron J. Anderson, MD, former Parkland CEO, “Our institution will be the hospital not of last resort, but the hospital of first choice.”
The genesis for the idea of a new hospital began in the mid-
“I BELIEVE THIS IS PRooF THE PULL PLANNINg PRoCESS WoRKS.”
8 A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMER 2014
and tower construction, each lasting five to six weeks in duration. Subcontractors would apply color-coated sticky notes to a bulletin board to show their progress and establish timelines for completion of each step of the phase. Teams of subcontractors would meet weekly to discuss construction progress based on the sticky notes, including superintendents and foremen. Many superintendents and foremen were new to the pull planning schedule and felt it was easier to understand than a traditional construction schedule. Saksen believes the efficiency of the pull planning process was responsible for the hospital construction being completed ahead of schedule. “The completion deadline for the hospital was August 6, 2014. However, we received our Temporary Certificate of Occupancy on July 22, 2014. I believe this is proof the pull planning process works.”
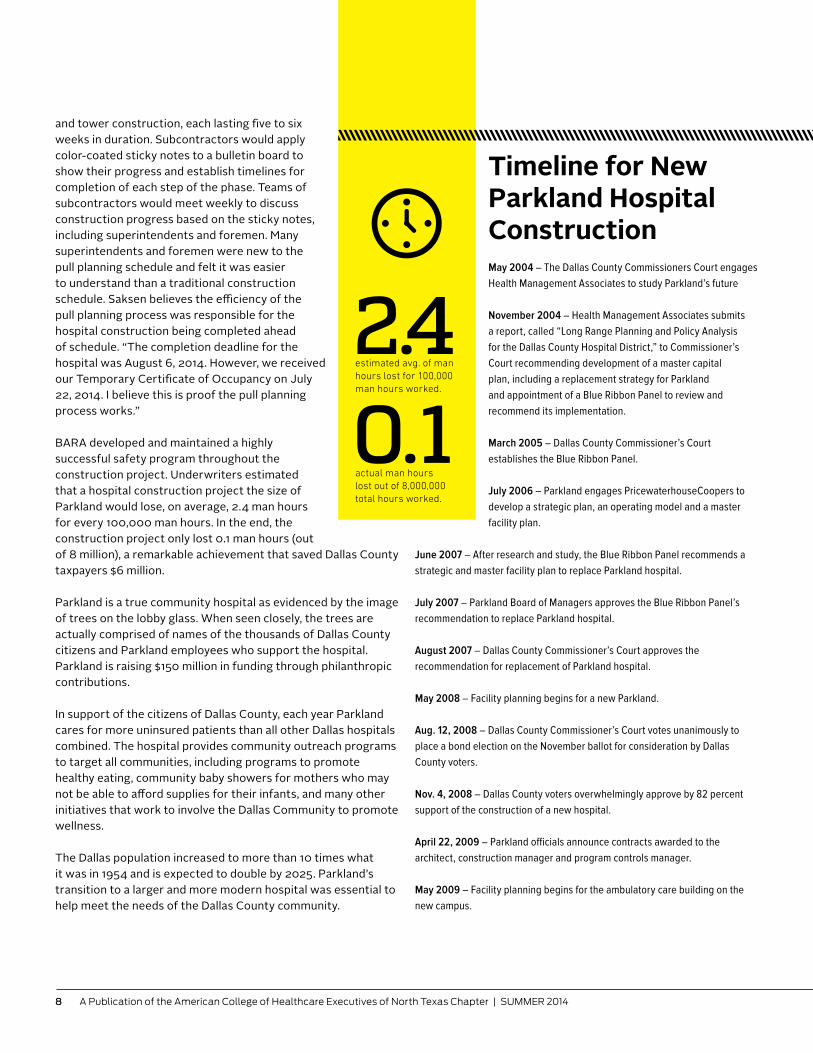
BARA developed and maintained a highly successful safety program throughout the construction project. Underwriters estimated that a hospital construction project the size of Parkland would lose, on average, 2.4 man hours for every 100,000 man hours. In the end, the construction project only lost 0.1 man hours (out of 8 million), a remarkable achievement that saved Dallas County taxpayers $6 million.
Parkland is a true community hospital as evidenced by the image of trees on the lobby glass. When seen closely, the trees are actually comprised of names of the thousands of Dallas County citizens and Parkland employees who support the hospital. Parkland is raising $150 million in funding through philanthropic contributions.
In support of the citizens of Dallas County, each year Parkland cares for more uninsured patients than all other Dallas hospitals combined. The hospital provides community outreach programs to target all communities, including programs to promote healthy eating, community baby showers for mothers who may not be able to afford supplies for their infants, and many other initiatives that work to involve the Dallas Community to promote wellness.
The Dallas population increased to more than 10 times what it was in 1954 and is expected to double by 2025. Parkland’s transition to a larger and more modern hospital was essential to help meet the needs of the Dallas County community.
Timeline for New Parkland Hospital ConstructionMay 2004 – The Dallas County Commissioners Court engages Health Management Associates to study Parkland’s future
November 2004 – Health Management Associates submits a report, called “Long Range Planning and Policy Analysis for the Dallas County Hospital District,” to Commissioner’s Court recommending development of a master capital plan, including a replacement strategy for Parkland and appointment of a Blue Ribbon Panel to review and recommend its implementation.
March 2005 – Dallas County Commissioner’s Court establishes the Blue Ribbon Panel.
July 2006 – Parkland engages PricewaterhouseCoopers to develop a strategic plan, an operating model and a master facility plan.
June 2007 – After research and study, the Blue Ribbon Panel recommends a strategic and master facility plan to replace Parkland hospital.
July 2007 – Parkland Board of Managers approves the Blue Ribbon Panel’s recommendation to replace Parkland hospital.
August 2007 – Dallas County Commissioner’s Court approves the recommendation for replacement of Parkland hospital.
May 2008 – Facility planning begins for a new Parkland.
Aug. 12, 2008 – Dallas County Commissioner’s Court votes unanimously to place a bond election on the November ballot for consideration by Dallas County voters.
Nov. 4, 2008 – Dallas County voters overwhelmingly approve by 82 percent support of the construction of a new hospital.
April 22, 2009 – Parkland officials announce contracts awarded to the architect, construction manager and program controls manager.
May 2009 – Facility planning begins for the ambulatory care building on the new campus.
2.40.1actual man hours lost out of 8,000,000 total hours worked.
estimated avg. of man hours lost for 100,000 man hours worked.

June 2013 – Helipads on top of the new building are finished. The helipads are substantially larger than those at the current hospital, designed to provide more room for caregivers who are waiting on air ambulances to land. In addition, the helipads have a built-in de-icing system.
July 2013 – The new 740,000-square-foot Tower Garage is awarded the LEED® Gold Certification from the U.S. Green Building Council’s Leadership in Energy and Environmental Design (LEED) program, which sets voluntary standards for buildings. The garage uses LED lighting and a 32kW photovoltaic solar panel system.
August 2013 – The outside of the new hospital building is fully enclosed, with most future projects taking place inside the hospital walls as crews work to finish out the interior. The blue construction cranes working on the outside of the building are taken down.
October 2013 – The structure of the chapel at new Parkland is completed and the roof and glass are installed. To support worship flexibility, the space can be arranged with the altar and service elements in several orientations.
October 2013 – The foundation is poured for the new logistics building. This 225,000-square-foot facility will house many of the support services for the hospital. It will be the entry point for all hospital supplies and include a truck docking station and a connecting tunnel system to new Parkland.
November 2013 – Construction of patient rooms for the Burn Intensive Care Unit (BICU) is finished in the acute care tower of the new Parkland hospital. The new Parkland BICU includes 12 intensive care and 18 acute care beds; the current center is comprised of nine intensive care and 17 acute care beds.
July 2014 – Parkland receives a Temporary Certificate of Substantial Completion from the City of Dallas. Transition planning for the new campus continues.
Spring 2015 – Patient care will begin in the new location.
August 2009 – Parkland receives AAA bond ratings from both Fitch Ratings and Standard & Poor’s Rating Service. Parkland issues $705 million in bonds, including $680 million in Build America Bonds.
Winter 2009 – Staff begin to relocate from buildings that will be removed to make way for new construction. Staff transition continues through Spring 2010.
Winter 2009 – Planning begins on the new administrative office building.
Winter 2009 – Mock hospital rooms are created to better assist architects in designers in creating the most efficient spaces possible for patient care.September 2010 – Final schematic designs are approved by Parkland.
Summer 2010 – Demolition and grading of land begins to make way for new construction.
Oct. 28, 2010 – Groundbreaking marks the beginning of construction for the new hospital.
November 2010 – Construction of the new parking garage begins.
Nov. 8, 2010 – New employee parking lot opens.
Dec. 6, 2010 – New DART Green Line opens, running through the center of the new campus.
July 2011 – Construction of the central utility plant (CUP) begins.
Summer 2011 – Designs begin for outpatient and logistics buildings.
January 2012 – The new 740,000-square-foot Tower Garage opens.
Fall 2012 – Construction begins on outpatient and logistics buildings.
December 2012 – The central utility plant begins utility service to the new Parkland hospital campus.
April 2013 – The Women and Infant’s Specialty Health (WISH) clinic structure is completed. The
size of the current WISH clinic, which occupies 30,000 square feet, restricted patient volumes to about 44,000 for the past several years due to lack of space. The new WISH clinic will be in excess of 100,000 square feet, giving Parkland staff greater capacity to treat more infants and mothers.
The names of Parkland supporters etched in the shape of trees.

What are you doing now?
I joined VHA three years ago after moving from Kansas and am part of an organization that I had been with member hospitals through the years and am now part of team of dedicated employees bringing value and service excellence to its member organizations.
In your opinion, what is the most important issue facing Healthcare today?
I would say that the financial challenges being faced by every healthcare organization today represent the most important challenge and the biggest threat to community healthcare. A secondary threat faced by healthcare leaders is the ability to embrace and determine the necessary changes to identify opportunities and to execute the required strategic, operational and tactical solutions required as a result of revenue reductions. That is where ACHE membership and being active in a chapter can be vital in providing learning opportunities through educational offerings and from other peer healthcare leaders.
How long have you been a member of ACHE?
I first joined ACHE in 1992.
Member SpotlightRex Walk, FACHE, VHA DallasSr. Director, Supply Networks
Why is being a member important to you?
Being a member of ACHE has given me the opportunity to access important educational opportunities and to cultivate meaningful relationships with other healthcare leaders. As a former ACHE Regent, I was able see first-hand both the dedication of the ACHE team and the quality of its membership. Membership in ACHE has provided me with the tools and opportunities the most effective healthcare leader possible.
What advice would you give early careerists or those considering membership?
Due to the complexities and challenges facing every healthcare leader today, I couldn’t imagine not being equipped with the tools and support that ACHE has provided me through the years. Membership in ACHE has truly been one of the best professional values for me in terms of price, relationships and results.
Tell us one thing that people don’t know about you.
Growing up on the flatlands of Western Kansas, we used to chase tornados for fun which has had some relevancy in my healthcare leadership experience.
ACHE of North Texas is pleased to announce the release of its new website!Designed with a fresh new look and user-friendly navigation, you can always keep up to date with the latest information, events, and promotions from the Chapter.
Our new site features integrated social media content, is mobile/tablet friendly, simple to navigate and provides a user friendly experience. The new design allows you to quickly find content and information about the Chapter thanks to the site’s simplified structure.
We hope that you will enjoy browsing the new site. Please send any comments or feedback to this link www.ACHENTX.org.

A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMERR 2014 11
What are you doing now?I am celebrating 16 years as the Chief Executive Officer of recently renamed and branded medical and dental practice now known as Foremost Family Health Centers. We just opened our second medical office in Balch Springs, Texas in January, 2014. Our corporate medical and dental office is in Dallas, Texas, and has been in existence since 1986. We are working on opening a third medical and dental office in 2015.
Foremost Family Health Centers is a designated federally qualified health center (FQHC) which is designed to be a one-stop shop for affordable primary and preventive medical, dental, behavioral health and wellness care services for all ages. We accept most major insurance plans and offer discounts to the uninsured individuals and families if they meet certain eligibility requirements. Our practice is staffed with board certified physicians in family practice, internal medicine, obstetrics and gynecology, pediatrics, podiatry, and psychiatry, and we have a team of dentists and hygienists providing preventive dental care. Additional services include laboratory, x-ray, behavioral health, chronic disease management and exercise programs.
My immediate goals are to identify more areas throughout the DFW Metroplex and open additional offices, secure PCMH designation and Joint Commission Accreditation at each site.
In your opinion, what is the most important issue facing Healthcare today?I see a couple of important issues facing healthcare today. There is still a demand for comprehensive and affordable primary care medical and dental practices which need to be placed in communities accessibleto those who have little to no insurance, and for those who may have a high deductible. Formal partnerships between specialists, hospitals and affordable primary care community health centers, when structured correctly, can decrease unnecessary emergency room visits and increase the compliance with utilization of primary care health centers as medical and dental homes. The second most important issue facing healthcare is shifting the focus of children, adults, and communities to
consistent healthy lifestyle changes, with a goal of improving clinical outcomes.
I am a person who has lived with two long-term chronic diseases (high cholesterol and thyroid disease) diagnosed in my teens, and have had the diagnosis of Type 2 Diabetes for the past 4 years. While these diseases, along with others, run in my family, I still had to make drastic changes in my lifestyle to achieve some sense of normalcy. My actions to keep these conditions under control are motivated by the fact that I am married with 3 children, all of whom both my husband and I plan to see grow up and achieve their life goals. Healthcare quality is personal for me.
How long have you been a member of ACHE?
I have been a member since 2010.
Why is being a member important to you?Membership with ACHE has allowed me to share the information I have learned through webinars, conferences, magazines, luncheons, and networking opportunities with my leadership team (CFO, COO, Medical Officer, HR/Compliance Officer, Dental Officer, Clinical Manager) and
those who are considering membership with ACHE would benefit from speaking with current members to gain additional information on how ACHE has contributed to their business.
“
“
Member SpotlightJoyce Tapley, MHA, CHCOChief Executive OfficerForemost Family Heath Centers
continued on page 8

12 A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMER 2014
The Rainbow Healthcare Leaders Association is a national organization with a mission to enhance the representation of lesbian, gay, bisexual and transgender healthcare executives and to promote high-quality care for LGBT individuals and their families. RHLA is committed to focusing on disparities in care and
National Newsother mid-level supervisors in our company. As a part of my succession plan, I have identified opportunities for internal staff members who are interested in internal promotional opportunities to obtain the information from ACHE, so they can understand the level of information available.
I also utilize many of the articles in the decisions that we make in our company.
What advice would you give early careerists or those considering membership?I would suggest that those who are considering membership with ACHE would benefit from speaking with current members to gain additional information on how ACHE has contributed to their business. The ACHE website is designed in a way to provide good information about the association. Attending a local event is also another way to understand the benefits of membership. The best way to know is to join, particularly if the individual is in the healthcare profession. I have been very pleased with all that the association has to offer.
Tell us one thing that people don’t know about you. I am aware that in this profession and position, I am the spokesperson for the company in many venues. I continually challenge myself by accepting opportunities to speak on the radio, on TV, as a key note speaker, a motivational speaker for youth, and by attending conferences as a conference session speaker. It’s getting easier. Fortunately, after most of my speaking engagements, I can ask for feedback (usually from my husband who is very honest with me) on how I can improve so that I do not appear to be nervous.
Member Spotlight (cont’d)Joyce Tapley
Postgraduate Fellowship Area of ache.org Provides a Vital Resource to Healthcare organizations and Entrants
preparing the next generation of LGBT healthcare executives. RHLA and ACHE have a shared interest in fostering the development of diverse healthcare leadership.
Join RHLA now and you will have access to the RHLA Mentorship Program and RHLA Forums, both of which will enable you to connect with other members in a meaningful and confidential environment. Members can share and receive feedback on business and personal issues that are important in their lives as they navigate their careers in healthcare.
For more information about RHLA membership or any of its programs, visit rhla.org.
Join the Rainbow Healthcare Leaders Association
Postgraduate fellowships are essential to attract and develop highly qualified healthcare management professionals. ACHE offers robust online resources on postgraduate fellowships at ache.org/PostGrad for organizations seeking to develop a postgraduate fellowship, organizations that want to find the
best candidate and new healthcare management entrants looking for a fellowship opportunity. The site includes the Directory of Fellowships in Health Services Administration for organizations to post their fellowship opportunities and for students to find opportunities they want to pursue. Additionally, resources for organizations looking to start a fellowship include sample manuals, templates and checklists. ACHENTX.org
VISIT US ONLINE
› Reach out to your employer to see if there are any Fellows in your organization. Then, cultivate those relationships.
› Ask your friends and colleagues if they know a Fellow they could introduc you to.
› Search your LinkedIn connections for the FACHE credential.
› Attend Chapter events and get to know Fellows through networking. Keep an eye on the name tags as they often indicate FACHE.
› Utilize the member directory to reach out to local Fellows that you have common interests with.
› Apply to have a Fellow as a Mentor. Our chapter facilitates a formal mentorship program from April – October. Look for information in January.
our Chapter is reimbursing the $250 application fee for the first 10 applicants that meet the criteria. Learn more here.
The Path to Becoming a FACHEBy Amanda o’Neal-Brummitt, FACHE
Is the requirement to have three Fellow references holding you back from applying? Don’t let it be a barrier to your success. Getting to know Fellows is easy if you are willing to exert a little bit of effort. Here are six ways to meet Fellows in our area:
Once you meet a Fellow you think will serve as a good reference, simply ask. Let them know that you want to apply and need references.
They will likely want to get to know you a little better before giving a reference. Make it easy for them. Offer to meet with them at their office or take them for a cup of coffee. Be respectful of their time. Then, follow-up and ask for the reference.
Hopefully, these tips will help you get started on obtaining your references. Best of luck!
ACHENTX.org

14 A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMER 2014
1. Remove scope of practice barriers to allow for all licensed professionals to practice to the full extent of their education and licensure.
2. Expand opportunities for nurses to lead and diffuse collaborative health improvement efforts.
3. Implement nurse residency programs for newly licensed and advance practice nurses to facilitate their transition into practice.
4. Increase the proportion of nurses with a BS in Nursing to 80% by 2020.
5. Double the number of nurses with a doctorate by 2020 to assure faculty to educate new nurses.
6. Ensure that nurses engage in lifelong learning
7. Prepare and enable nurses to lead change to advance health of populations at all levels of the continuum.
8. Build an infrastructure for the collection and analysis of interprofessional health care workforce data to allow for better knowledge and workforce planning at regional, state and national levels.
In this issue we are highlighting local efforts to implement the recommendations. Two area nurse executives responded to some specific questions. Elaine Nelson, MSN, RN, NEA-BC, chief nursing officer at Texas Health Harris Methodist Fort Worth (THFW) and Mary Robinson, PhD, RN, NEA-BC, chief nursing officer at Texas Health Harris Methodist Southwest (THFW).
Which of the eight recommendations from the IOM report are you implementing in your setting?
(Nelson) At THFW, we are actively working on six of the eight recommendations. We have expanded the practice of APRNs into managing care on our observation unit as well our discharge clinic and senior clinic. APRNs are responsible for managing patients with specific protocols for set diagnoses. Working closely with the physicians and other professionals, the APRNS are a valuable resource to all caregivers. Additionally, nurses across the organization are dedicated to leading and diffusing collaborative health improvement efforts such as faith community nursing and other dedicated community nurses that provide care in our mobile units in the underserved communities. Stroke and trauma staff also lead efforts in the community with elders for prevention around falls and early detection of strokes.
At THR, we have implemented a national residency program that provides educational experiences for newly graduated nurses transitioning into professional roles. Through our Texas Health Resources University, we also have robust educational offerings, certification reviews, and host other venues so that our nurses can engage in lifelong learning.
We are promoting BSN nursing and already have 61% of the workforce who have achieved that education. Many more are in baccalaureate programs and will complete the work well in advance of 2020. One hundred percent of our managers have a BSN and many have achieved or are working on their masters in nursing (MSN). In terms of doctoral degrees, THFW strongly advocates continued education and is sensitive to increasing the number of doctorally prepared nurses to meet the needs of future nursing students. THR provides excellent tuition reimbursement benefits to encourage increasing numbers of nurses to achieve their doctorate. I am currently a doctoral
Texas Team: Advancing the Health of North Texans Part IIby: Joan Shinkus Clark DNP, RN, NEA-BC, CENP, FACHE, FAAN
Elaine Nelson, MSN, RN, NEA-BCMary Robinson, PhD, RN, NEA-BC
In the last issue of the ACHE North Texas Newsletter, the work of the Texas Team was highlighted in response to the Institute of Medicine (IOM) Future on Nursing report and the national call to action to implement the eight recommendations in the report. The eight recommendations included:

student at Texas Tech and graduate in May of 2015.
Could you talk about one or two initiatives you are working on?
Increase proportion of nurses with BS in Nursing to 80% by 2020.(Robinson) At Texas Health we are implementing both systemwide and local strategies, driven by overall systemwide goals memorialized in the Texas Health Nursing Operations Plan as well as our Hospital Operations Plan. Through analysis of systemwide status around those with completed baccalaureates in nursing as well as those in process, we are able to set systemwide goals for educational achievement. THR has worked closely with the area schools of nursing, both associate and baccalaureate programs, to create opportunities for streamlined transition of nurses from associate degree to BSN. A group at the system level has met to identify the educational minimum requirements needed to hire on as a THR Nurse, with clear expectations upon hire that any associate degree nurses hired are expected to return to school and complete their bachelor’s degree within an allotted time frame.
Our local Professional Reward and Recognition Council has evaluated the current percentages of nurses who have a BSN and established annual goals that specify incremental improvements toward the 2020 80% performance metric. Action plans are written at both the system and hospital level with the hospital actions building on the system work. Nurse Managers are expected to have discussions with incumbent RN’s working with them to establish reasonable goals for achievement of the BSN as well as follow-up discussions regarding progress towards goals.
Expand opportunities for nurses to lead and diffuse collaborative health improvement efforts.
(Robinson) THR and THSW have created a unique model that has built on the role of the Clinical Nurse Leader (CNL) to expand opportunities to lead and diffuse collaborative health improvement efforts. Over the past 5 years, THR has partnered with Texas Christian University to bring the Clinical Nurse Leader role to Texas and Texas Health Resources. These
masters prepared advanced generalists are working within the hospital setting to manage a microsystem of patients with the ultimate goal of improving patient outcomes as well as their overall health when possible. The CNL program and Care Transitions program are strategic efforts to improve Value and Quality as well as to move the care of the patient beyond the walls of the hospital. The CNL in partnership with other team members helps to coordinate care within the hospital but also partners with Care Transition Managers and other members of the health care team to align patient’s care needs once they leave the hospital. Care transitions coaches are available to work with patients outside the walls to assist them in navigating their healthcare needs and aligning them with appropriate resources. The CNL plays a unique role in this collaborative effort.
What obstacles do you have internally to achieving these recommendations?
(Nelson)The biggest obstacle lies in removing scope of practice barriers specifically in regards to APRNs. Assisting physicians to understand that the APRNs are an adjunct to care and can facilitate care in an effective and efficient manner is crucial to having them practice at the top of their license.
(Robinson) Obstacles to achieving the BSN recommendation are related to managing the message to staff about requirements and helping them to achieve expectations. The current nurses who do not have a BS may not have the resources and time or even desire to go back to school so I see that as a major challenge in achieving this goal. We will need to work closely with our nurses to help them identify the steps it will take for them to achieve the goal and facilitate and encourage movement toward the goal.
Obstacles to achieving nurses leading and diffusing collaborative health improvement efforts largely lie in the disconnect between funding for illness related events versus health related events and then just getting all parties together to collaborate and move ideas and processes forward.
Any advice for ACHE members on how to prioritize these activities in order to meet the goals?
(Nelson) Doing a gap analysis on current state and developing benchmarks to monitor progress will be important over the coming years. The recommendations can be seen as a step approach. As nurses increase their education levels and expertise, opportunities must be provided that encourage and allow nurses to lead change and practice at the top of their license...Action plans that will build on the recommendations and address gaps are going to be crucial to achieve success.
“Obstacles to achieving the BSN recommendation are related to managing the message to staff about requirements and helping them to achieve expectations.”
continued on page 16
achieving these recommendations, this is important work in the months and years to come in assuring that our patients and communities receive the best care possible by nurses. As some of our local nurse leaders have advised, achievement is a multi-year process and assuring that plans are in place now to move your organization towards achievement of these recommendations will be critical as payment and reform move simultaneously in the direction of value over volume.
(Robinson) Several of these initiatives are inter-related so working on one helps with others in many cases. I would strongly recommend having strategic initiatives focused on achievement of these goals followed by action plans formulated with the input of front line staff artuiculating the steps that would be needed to achieve these. Dashboards and visual reminders of progress towards goals are always helpful.
Thanks to the leaders for their insights. Whether you are a nurse executive or supporting the nurse executive in
The Networking and Membership Committee is excited to announce that as a result of comments and suggestions from our constituents, we are taking a more proactive approach to delivering events that better fulfill your needs. Our committee has been meeting and is committed to providing events that are more geographically located in the centralized areas across the service area of the ACHE of North Texas chapter. With these suggestions the chapter recorded one of the highest attendances for our “Breakfast with the CEO” series at Baylor Regional Medical Center at Grapevine with President Steve Newton, FACHE. As we look forward to the next year for 2014-2015 we are still committed to providing these events, with additional ideas and thoughts being presented to include community service projects, holiday parties, and specialized events for certain members of our organization (i.e. Early Careerists, Senior Executives, etc.). The committee also wants to reach out to the chapter to gather ideas and suggestions for event locations, topics addressed by our guest speakers, and how to better improve our reach in the service area we cover to recruit new members. Please consider your colleagues in each of your wonderfully diverse organizations by asking them if they are members of ACHE. If not, we would ask that you share with them the benefits of membership and inviting them to one of our many events throughout the year.
Thank you,Networking and Membership Committee
Exciting New Events From the Networking and Membership Committee
Advancing the Health of North Texans Part II (cont’d)
ACHE’s Job CenterThe American College of Healthcare Executives’ Job Center is a complimentary online resource designed to bring together the right candidate and the right job. It is a member only resource for job seekers, but is open to both member and non-member employers interested in listing positions. The Job Center features more than 2,300 position listings with nearly 4,000 active job seekers and was enhanced in early 2013 to include many new features.
Job seekers now benefit from improved search functionality, new job notification options, enhanced job detail pages, and a mobile-friendly version. Employers can utilize new job activity information reports, options to upload a company logo to appear on job listings, and resume alerts to notify you when new candidates meet your criteria.
We hope you make use of this popular ACHE resource. We are especially interested in increasing the number of early careerist opportunities, as launching a career in today’s competitive healthcare management marketplace presents challenges for many of our early career members.
To take a look at the ACHE Job and Resume Bank click ACHE-JobBank.
If you have further questions, contact Marisol Santiago at [email protected] or (312) 424-9446.
EVENT ENCoRE

A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMERR 2014 17
June 26:Navigating Executive Level Career Advancement in the Era of Healthcare Reform Hosted by Texas Health Presbyterian Hospital Dallas
July 10: After Hours Networking Event at the Ballpark
EVENT ENCoRE

WELCoME ACHENTX’S NEWEST MEMBERSAshley Anderson, Fort WorthMartin Barker, DallasToy H. Bartley, DallasSharita N. Butler, AllenJessica Ceballos, Grand PrairieMass R. Cham, Royse CityJanet Glaze, ArlingtonLance Henry, Farmers BranchLauren Homayoun, PlanoJessica R. Johnson, RN, Grand PrarieThomas Kallstrom, IrvingDonny Kalluvilayil, The ColonyReigen Lox, FriscoBhushan Mahajan, IrvingMegan V. Mattingly, DallasMichael Walsh, RN, FriscoKynet Watkins, Dallas
Fred Andrews, Fort WorthEve Asuelime, ArlingtonTammy Bauer, Fort WorthScott Casey, Fort WorthRebecca David, DallasMichael Dixon, Southlake
Robinne Dodd, KellerRobert K. Dugger, JD, DallasMicky Fokken, Fort WorthGreg Fuhrmann, Fort WorthJoanna Hailey, RockwallJeffrey S. Lang, KellerBenjamin I. Lueck, IrvingLina Nicolas, MD, SouthlakeDavid J. Nowacki, DallasTolu Opeloye Sr., CypressToby Radabaugh, Highland Village1Lt Bilal Rizvi, San AntonioAllana Rohrscheivb, Ann ArborCarolyn C. Scott, SouthlakeClaire Simpson, Fort WorthMin Sohne, EulessThomas Southam, The ColonyJames M. Stewart, DallasJonathan T. Ward, ArlingtonMichelle A. White, Argyle
Barbra F. Bidot, AddisonJeremy Eaves, DallasAdam S. Fielding, Willow Park
Mark C. Gibson, JustinCarrie Hecht, AledoDawn Himes, FriscoJohn Hines, RichardsonScott A. Jones, DallasEdmond S. Katz, AtlantaAllen R. Luna, DallasNicole A. Martinez, Fort WorthJohnathan McIver, PlanoAndrew N. Meyercord, DallasMichelle Mudge-Riley, McKinneyHiep Nguyen, RN, Haltom CitySayna noei, WaxahachieJoseph Osborne, DallasWayne E. Plummer Jr., Fort WorthKatherine D. Price, Baton RougeBianca K. Richardson, Fort WorthNancy L. Schaefer, ArlingtonVeli R. Shah, DallasDarren L. Smith, DallasStephen Sokolyk, MD, RichardsonTamera Walters, KrumDeborah White, Glenn HeightsAmy Yazbeck, McKinney
JUNE
JULY
AUGUST
ACHENTX’SNEWESTFELLOWS
William Cooksey, RNMarcus Jackson Sr.Greg Kennedy
Paul M. MusgraveRon NorrisJulia A. Roberts, RN
Byron J. SernaValerie ShoupMichael R. Williams, MD

A Publication of the American College of Healthcare Executives of North Texas Chapter | SUMMERR 2014 19
Wednesday, October 8thWomen in Leadership: Leaving a LegacyLocation: La Cima Club | Las Colinas Time 7.30-9.30AM
Thursday, October 16thListening to Employers: How Health Systems Can Support Population Health Management 1.5 Face to Face Credits Apply Location: Texas Health Arlington Memorial Hospital Time: 5.30-7.30PM
Wednesday, October 29thBreakfast with the CEOLocation: Parkland Health & Hospital System Time: 7.30-9.30AM
Friday, November 7thImproving Hospital Physician Relations: A Journey from Autonomy to PartnershipTime: 9.00am – 3.00pmLocation: Baylor Sammons Cancer Center | Dallas
Thursday, December 4thHoliday Networking Event and Toy DriveLocation: TopGolf | The ColonyTime: 6.30-8.30
ACHE of North Texas thanks the following Corporate Sponsors for assisting the organization’s mission. By sponsoring various events throughout the year, these sponsors are provided local and national exposure with an opportunity to showcase their organization, brand, career opportunities, products and services to the ACHE membership and its affiliates.
For the latest updates on Chapter events, programs and promotions please check our website or watch your inbox for the event guide.
Upcoming Events: