the fiscal sustainability of long-term care and its impact on health systems - tim muir, oecd
TRANSCRIPT

The fiscal sustainability of long-term care and its impact on health systems
4th Meeting of the Joint Network on Fiscal Sustainability of Health Systems
16-17 February 2015
Tim Muir Policy Analyst Health and Social Policy Divisions Directorate for Employment, Labour and Social Affairs
• “Care for people needing support in many facets of living over a prolonged period of time” (OECD, 2011)
• Typically this refers to ADL care, but it can also mean IADL care and other things (meeting social needs, some medical care).
• OECD distinguishes “health” components (ADL, nursing care, palliative care) from “social care” (IADL, residential care) for accounting purposes.
What is long-term care?

Fiscal sustainability is the top concern for OECD governments
Source: Help Wanted? (OECD, 2011)

Fiscal sustainability is the top concern for OECD governments
Source: Help Wanted? (OECD, 2011)

Policy-makers continue to consider the trade-offs between cost and coverage
Cost and affordability • Austerity policies
• Concerns about sustainability with ageing populations and/or rising costs
• Rising expenditure in other areas of health care, putting pressure on public finances
• Political limits on levels of taxation
Adequacy of protection • Making sure people get
the care they need
• Keeping out-of-pocket costs manageable
• Reducing pressure on families and carers

TRENDS IN LTC SPENDING AND KEY DRIVERS

There is huge variation in what countries currently spend on LTC
• Prices: higher staff qualifications or overheads in some countries mean that unit costs are higher
• Out-of-pocket costs: in some countries people pay significant proportions of LTC costs themselves
• Role of family: families are expected to take care of older people in some countries, while the state does it in other
Variation is driven by differences in prices, coverage and social norms
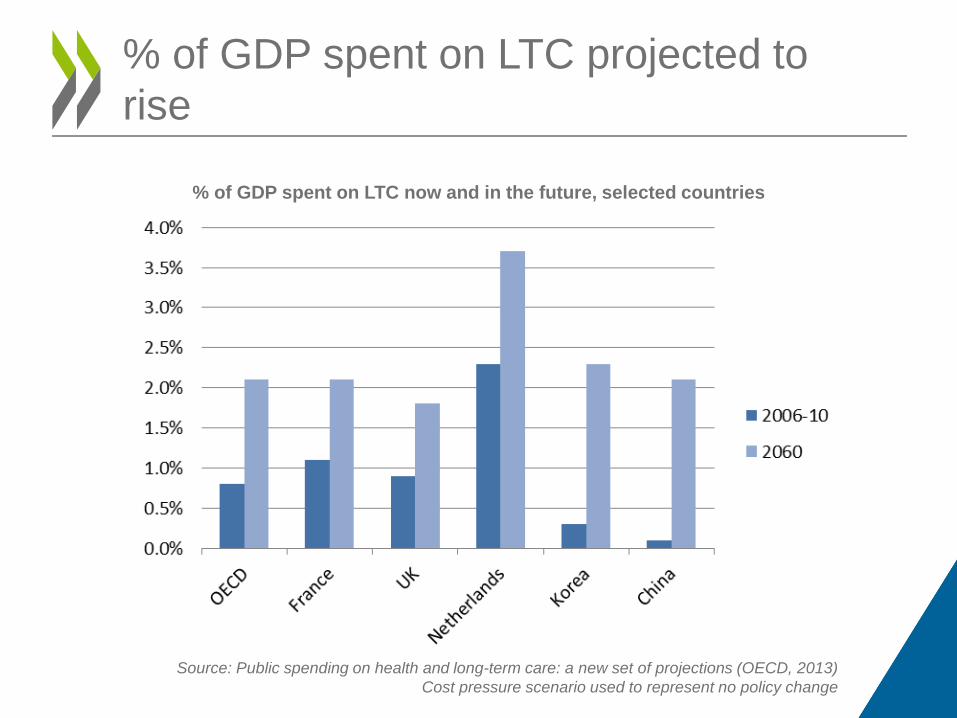
% of GDP spent on LTC projected to rise
% of GDP spent on LTC now and in the future, selected countries
Source: Public spending on health and long-term care: a new set of projections (OECD, 2013) Cost pressure scenario used to represent no policy change

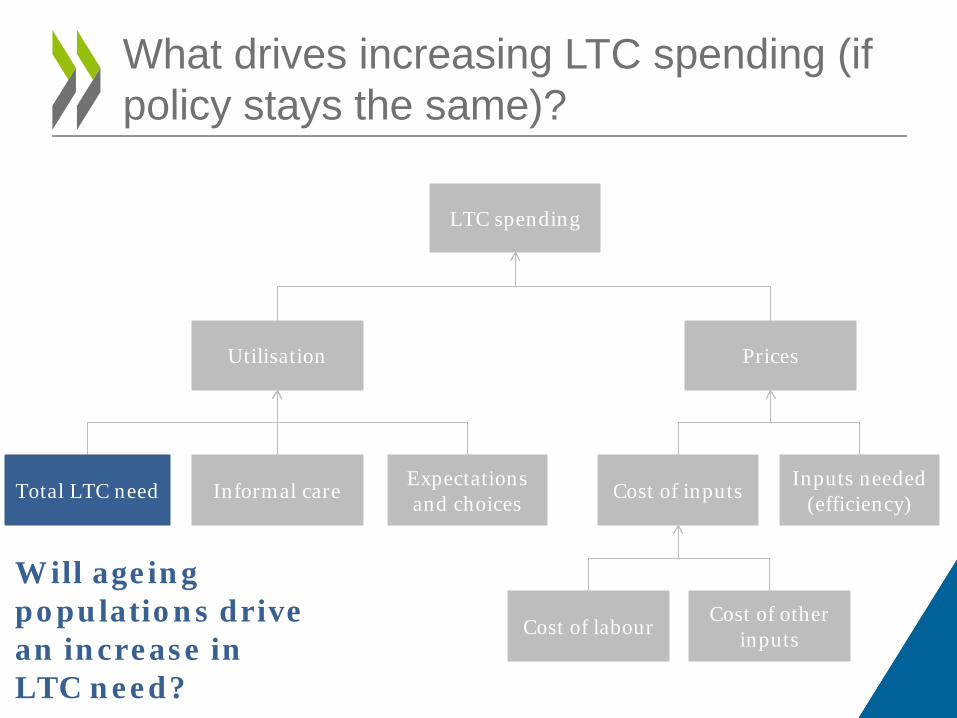
What drives increasing LTC spending (if policy stays the same)?
LTC spending
Utilisation Prices
Total LTC need Expectations and choices Informal care
Cost of labour Cost of other inputs
Inputs needed (efficiency) Cost of inputs
What drives increasing LTC spending (if policy stays the same)?
LTC spending
Utilisation Prices
Expectations and choices Informal care
Cost of labour Cost of other inputs
Inputs needed (efficiency) Cost of inputs Total LTC need
Will ageing populations drive an increase in LTC need?

Older people account for an increasing proportion of the world’s population

Other things being equal, more older people means more disability
Dementia prevalence in Europe by age band assumed constant over time
The number of people with dementia in Europe by age and year
Source: OECD analysis of data from Alzheimer's Europe and the United Nations

But other things are not equal if “healthy ageing” holds
Constant age-specific prevalence
Healthy ageing adjustment
Constant time to death prevalence
We can make different assumptions about disability trends…
More optimistic assumptions Lower total need Less cost pressure
• Evidence suggests falling age-specific rates for many conditions e.g. dementia
• OECD projections assume healthy ageing
• Ageing to increase LTC spend by 0.1% of GDP by 2030 and 0.3% of GDP by 2060 – only about a fifth of total projected expenditure growth
• Informal care Increasing geographical mobility and participation in labour force reduce informal care and increase costs
• Expectations Rising incomes and living standards mean higher expectations of care in old age
• Cost of labour Wages rise along with wider economy, but few efficiency opportunities due to labour-intensive nature of work
So what are the other drivers of rising costs?

IMPLICATIONS OF LTC BUDGETING DECISIONS

• Prevention Potential to reduce total needs, but evidence of effectiveness limited
• Improve efficiency Could meet needs more cheaply, but limited opportunities in a labour-intensive service
But these are unlikely to be enough, so some countries are considering if they can…
• Reduce public coverage Meet a lower proportion of needs from public budgets
Policy decisions can change the trajectory of public spending

Reducing public coverage pushes costs elsewhere or leaves needs unmet
Reduced public coverage for LTC
Needs are met in other ways
Some needs are not met
Formal services purchased privately
• Higher out-of-pocket costs • Risk of poverty, asset depletion
More care provided by families
• Opportunity cost • Increased chance of mental health issues • Families drop out of labour force
Needs met in health systems
• Bed blocking in hospitals • Increased health costs
People go without care
• Lower quality of life • More falls, injuries, acute episodes • Increased activity in health systems

Reducing public coverage pushes costs elsewhere or leaves needs unmet
Reduced public coverage for LTC
Formal services purchased privately
• Higher out-of-pocket costs • Risk of poverty, asset depletion
More care provided by families
• Opportunity cost • Increased chance of mental health issues • Families drop out of labour force
Needs met in health systems
• Bed blocking in hospitals • Increased health costs
People go without care
• Lower quality of life • More falls, injuries, acute episodes • Increased activity in health systems
Clear links to health budgeting – but evidence on the strength of these links is weak
Needs are met in other ways
Some needs are not met

A coherent view of health and LTC could potentially reduce these issues
Budgeting processes
Commissioning / delivery of
services
Integration Cooperation
• Single budget for health and LTC
• Reflect interactions between services in budget planning
• Joint commissioning of health and LTC
• Flexibility to move funding between the two
• Greater consideration of interactions in commissioning / delivery of services
But it is not clear how best to structure these solutions – or how effectively they would reduce cost-shifting.

• Is your country experiencing rising demand for long-term care, is this sustainable under current models and what can (and should) be done to control costs?
• Given the links between health and long-term care services, how does your country ensure that budgeting processes take a coherent view of health and long-term care?
Questions for discussion