the genetics of prostate cancer: clinical implications pdfs... · the genetics of prostate cancer:...
TRANSCRIPT

1
The Genetics of Prostate Cancer: Clinical Implications
William J. Catalona, MD
Northwestern University Feinberg School of MedicineRobert H. Lurie Comprehensive Cancer Center
Chicago, Illinois
Additional Disclosure
• Collaborator with deCODE genetics, Inc.
• Non-paid consultant with no financial interest or support
Facts
• Cancer is caused by interplay of genetic and environmental factors
• The contribution of genetic factors varies between tumors
• Shared genetic factors may increase the risk for more than 1 type of cancer
Early Family Linkage Studies
• Prostate cancer clusters in families
• Most segregation analyses suggested hereditary prostate cancer could be best explained by at least 1 rare dominant susceptibility gene, but this has not yet proven to be the case

2
Early linkage studies of PCa families postulated the existence of several possible susceptibility genes
RNAseLRNAseL
PCaPPCaP
EphB2EphB2
ELAC2ELAC2
HPC20HPC20 HPCXHPCX
MSR1MSR1
HPC1pHPC1pVDRVDR
CYP3A gene clusterCYP3A gene cluster
Early Targeted Studies
• However, further targeted studies and genome-wide scans revealed difficulties in replication
• Confirmatory studies have yielded mixed results
Clinical Studies
Based on Candidate Genes
UPM-3 (Now called PCA3)
• A gene that is 30-100-fold upregulated in prostate cancer
• Can be detected in prostatic fluid samples• Theoretically, it could be used like urinary
cytology (i.e., could detect cancer without performing a biopsy)
• Practically it might assist in selecting patients for repeat biopsy
3
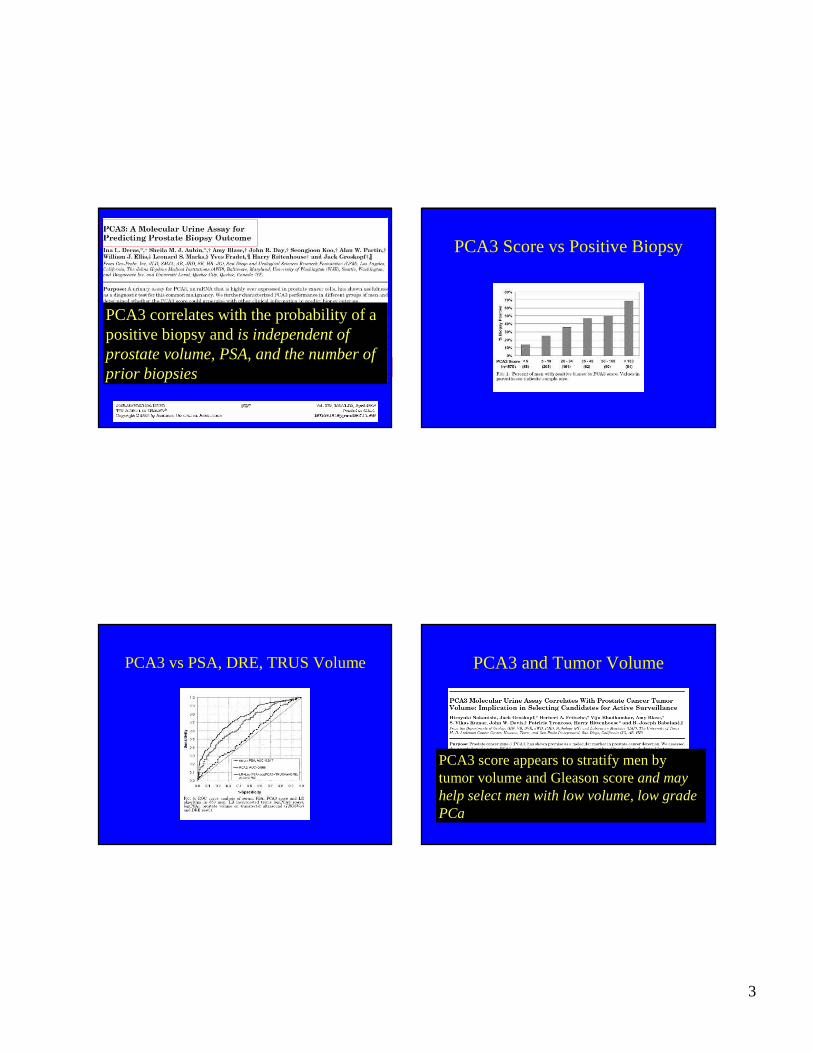
PCA3 correlates with the probability of a positive biopsy and is independent of prostate volume, PSA, and the number of prior biopsies
PCA3 Score vs Positive Biopsy
PCA3 vs PSA, DRE, TRUS Volume PCA3 and Tumor Volume
PCA3 score appears to stratify men by tumor volume and Gleason score and may help select men with low volume, low grade PCa

4
PCA3: Tumor Volume and Gleason Sum
PCA3 in post-DRE urine of PCa patients correlated with pathologic findings of extracapsular tumor extension
Multi-Center Validation EPCA-2
• Nuclear protein specifically expressed in prostate cancer
• ELISA for 2 epitopes (2.19 and 2.22)• In serum samples from patients, shows
results that are complementary to PSA• Identifies men with organ-confined and
non-organ confined prostate cancer and prostate cancer vs non-prostate cancer.
Leman ES et al J Urol 175:275, abstract 852

5
EPCA-2 in Prostate Cancer and Controls

6
TMPRSS2-ETS Gene FusionFusion of TMPRSS2 and ETS Transcription
Factor Genes in Prostate CancerERG oncogenic transcription factor
ETS1 oncogenic transcription factor
TMPRSS2androgen response gene
Transformation signaling in the presence of androgen
Contemporary Strategies in Active Surveillance: Contemporary Strategies in Active Surveillance: ergerg Fusion Effect on Prostate Cancer MortalityFusion Effect on Prostate Cancer Mortality
FUSION STATUSCumulative Incidence Ratio: 3.644 (p-value=0.0044, 95%CI=(1.497, 8.870))
M. Rubin et al, M. Rubin et al, OncogeneOncogene, 2007, 2007
Urinary Test for Prostate Cancer
Combination of TMPRSS2-ERG and PCA3 significantly improves sensitivity for PCadiagnosis
7
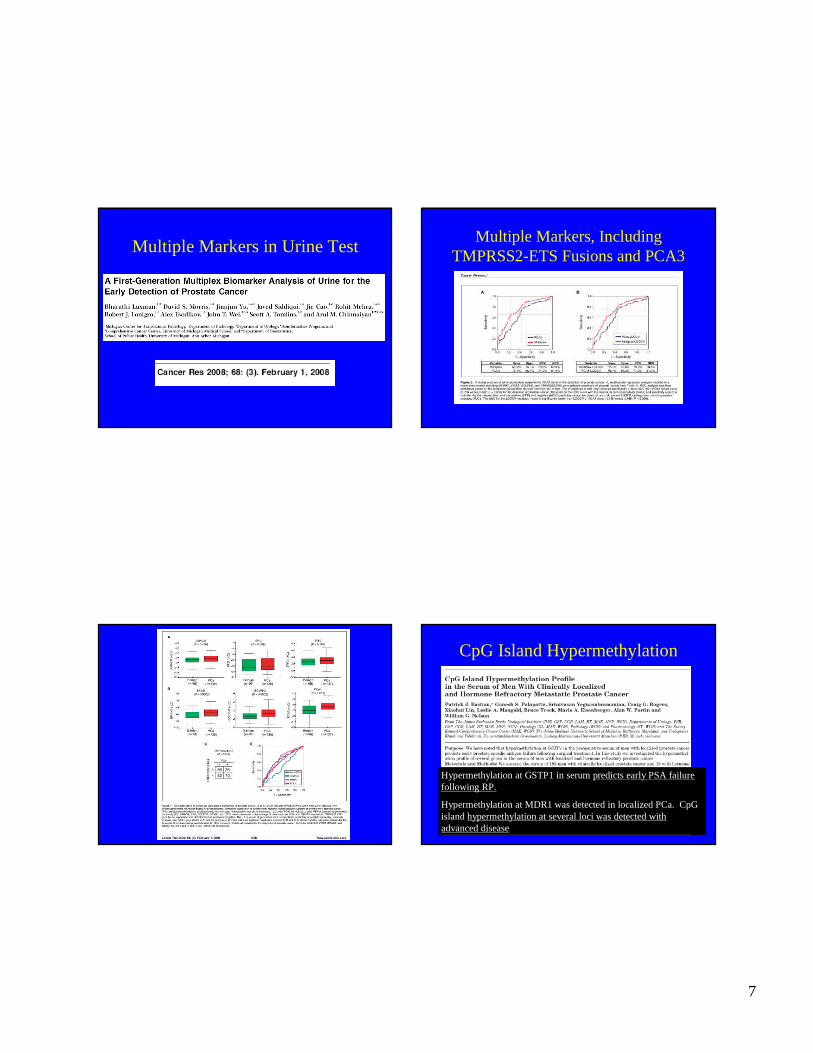
Multiple Markers in Urine TestMultiple Markers, Including
TMPRSS2-ETS Fusions and PCA3
CpG Island Hypermethylation
Hypermethylation at GSTP1 in serum predicts early PSA failure following RP.
Hypermethylation at MDR1 was detected in localized PCa. CpGisland hypermethylation at several loci was detected with advanced disease

8
Hypermethylation of Genes
Gene analysis using PCR is a reliable method for detecting abnormal DNA methylation in voided urine following DRE or prostate needle biopsy.
A serum test based on GSTP1 hypermethylation may help identify men with increased risk of PCa, despite negative prostate biopsy.
Limitations of Linkage and Candidate Gene Studies
• Linkage analysis has sufficient power to detect highly penetrant genes but has weak power to find susceptibility genes of small-to-moderate effects
• Candidate gene studies do not test most of the genome
Genetic Variants
• Prior to 2006, no common genetic variant accounted for a substantial proportion of cases
• In 2006, deCODE geneticsdiscovered genetic variants that point to a complex genetic basis, involving multiple susceptibility loci, i.e., “death by 1000 cuts”
9
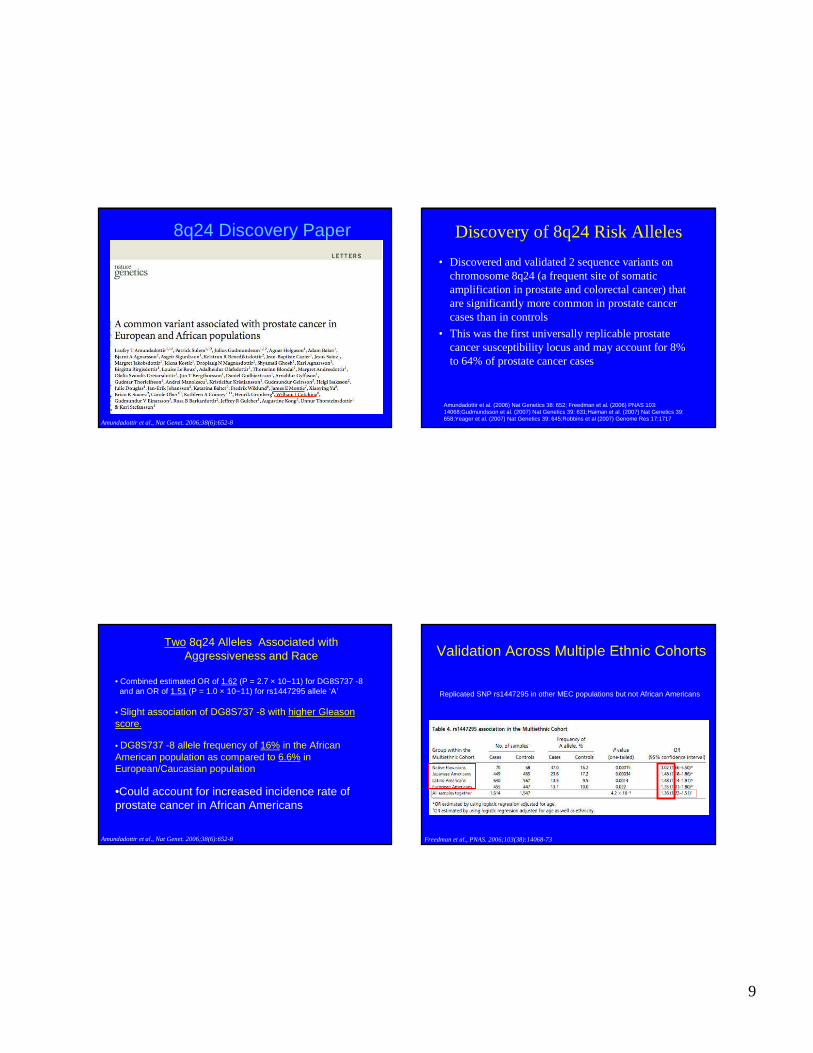
8q24 Discovery Paper
Amundadottir et al., Nat Genet. 2006;38(6):652-8
Discovery of 8q24 Risk Alleles
• Discovered and validated 2 sequence variants on chromosome 8q24 (a frequent site of somatic amplification in prostate and colorectal cancer) that are significantly more common in prostate cancer cases than in controls
• This was the first universally replicable prostate cancer susceptibility locus and may account for 8% to 64% of prostate cancer cases
Amundadottir et al. (2006) Nat Genetics 38: 652; Freedman et al. (2006) PNAS 103: 14068;Gudmundsson et al. (2007) Nat Genetics 39: 631;Haiman et al. (2007) Nat Genetics 39: 658;Yeager et al. (2007) Nat Genetics 39: 645;Robbins et al (2007) Genome Res 17:1717
• Combined estimated OR of 1.62 (P = 2.7 × 10−11) for DG8S737 -8and an OR of 1.51 (P = 1.0 × 10−11) for rs1447295 allele ‘A’
• Slight association of DG8S737 -8 with higher Gleason score.
• DG8S737 -8 allele frequency of 16% in the African American population as compared to 6.6% in European/Caucasian population
•Could account for increased incidence rate of prostate cancer in African Americans
Two 8q24 Alleles Associated withAggressiveness and Race
Amundadottir et al., Nat Genet. 2006;38(6):652-8
Replicated SNP rs1447295 in other MEC populations but not African Americans
Validation Across Multiple Ethnic Cohorts
Freedman et al., PNAS. 2006;103(38):14068-73
10
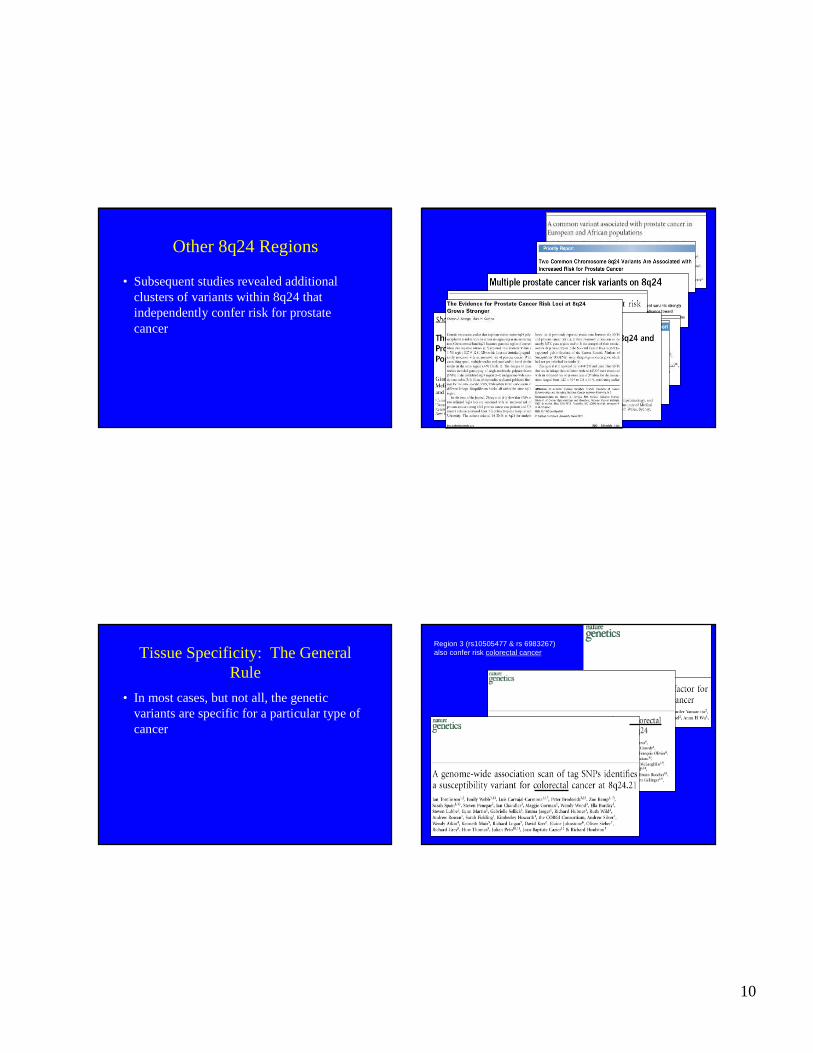
Other 8q24 Regions
• Subsequent studies revealed additional clusters of variants within 8q24 that independently confer risk for prostate cancer
Tissue Specificity: The General Rule
• In most cases, but not all, the genetic variants are specific for a particular type of cancer
Region 3 (rs10505477 & rs 6983267) also confer risk colorectal cancer

11
Known Genes in 8q24 • The genomic regions of 8q24 are gene poorand have a high
recombination rate• The only reported “gene” is a retro-transposed gene,
AF268618(POU5F1) that encodes for a transcription factor, OCT4, proposed as a stem cell marker – embryogenesis and in some tumors
• Two known genes nearby are c-MYCand FAM 84B(NSE2), but no associationwith these genes has been found
• deCODE found no differences in expression in carriers and non-carriers of any of the above or of 1447295 (A), HapC, rs16901979
• The distal end of a fragile site8C (FRA8C) has been mapped to this region, as well as several integration sites of HPV
POU5F1P1
MYC
128.0-129.0 Mb
4 Significant Regions of 8q24 Associated with Prostate Cancer Susceptibility
Ch 8
REGION 1128.54-128.62
REGION 2128.14-128.28
REGION 3
128.47-128.54
Amundadottir et al. (2006) Nat Genetics 38: 652Freedman et al. (2006) PNAS 103: 14068Gudmundsson et al. (2007) Nat Genetics 39: 631Haiman et al. (2007) Nat Genetics 39: 658Yeager et al. (2007) Nat Genetics 39: 645Robbins et al (2007) Genome Res 17:1717Salinas et al (2008) CEBP 17:1203
SNPs
rs16901979 (A)rs16901979 (A)
rs6983267 (G)rs6983267 (G)
rs1447295 (A)rs1447295 (A)
rs13254738rs6985361
Broad11934905
rs7000448
rs10090154
rs17837688
rs4242382
rs4008482
breast
colorectal & prostate
REGION 4
bladder
Gudmundsson et al., Nat Genet. 2007b;39(8):977-83
17q: The Second Major RegionUK “Practical” Reports 7 Risk Variants on Chromosome 3,6,7,10,11,19 and X
Of the 53 SNPs significant at the P < 10-6 level, 20 were on 8q24 and 6 were on chromosome 17
12
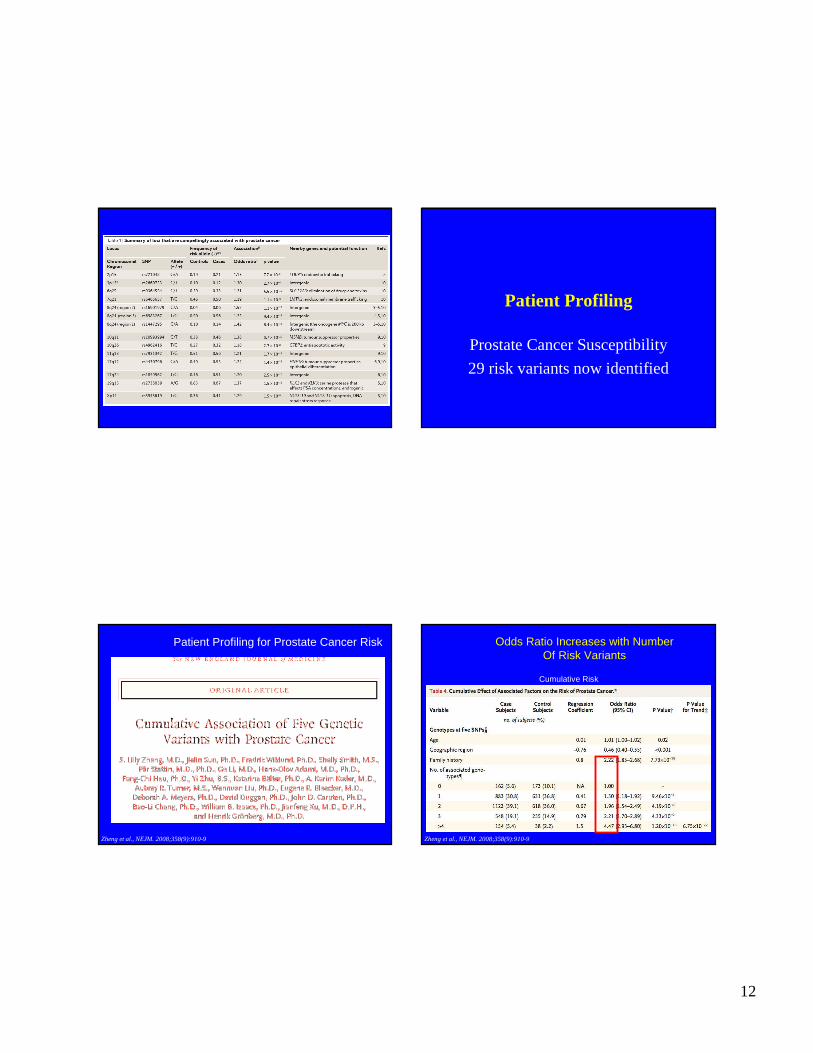
Patient Profiling
Prostate Cancer Susceptibility
29 risk variants now identified
Patient Profiling for Prostate Cancer Risk
Zheng et al., NEJM. 2008;358(9):910-9
Cumulative Risk
Odds Ratio Increases with NumberOf Risk Variants
Zheng et al., NEJM. 2008;358(9):910-9
13
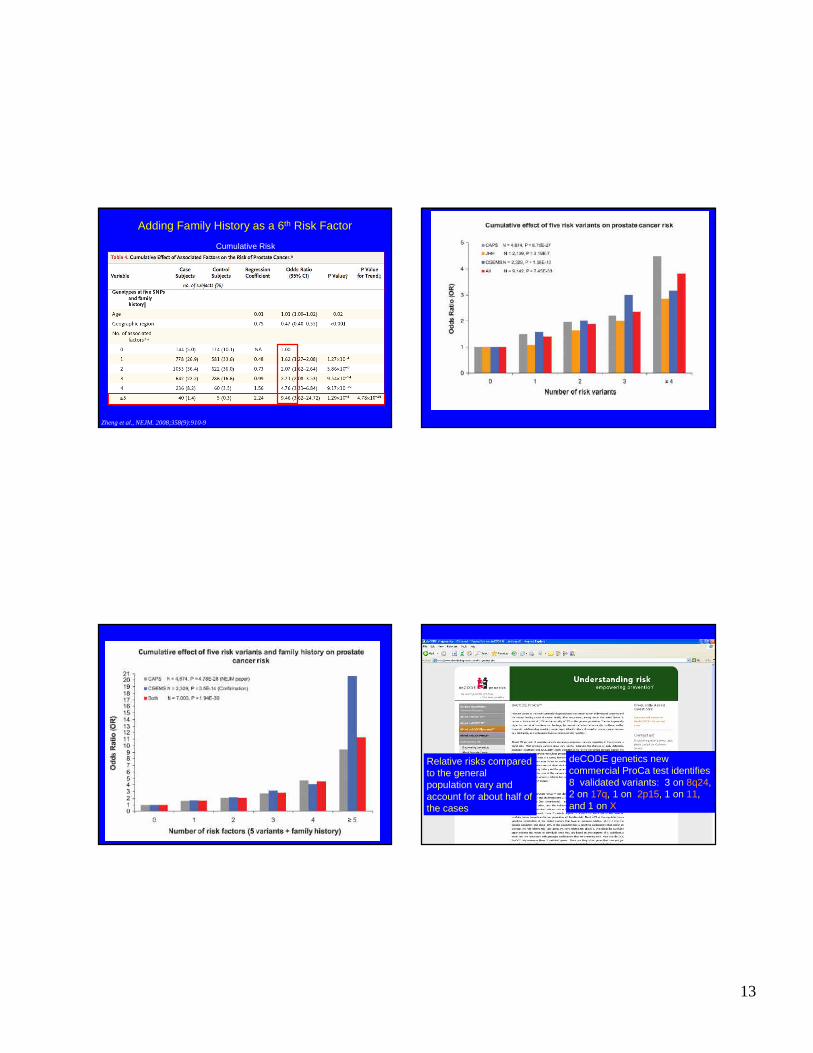
Cumulative Risk
Adding Family History as a 6th Risk Factor
Zheng et al., NEJM. 2008;358(9):910-9
deCODE genetics new commercial ProCa test identifies 8 validated variants: 3 on 8q24, 2 on 17q, 1 on 2p15, 1 on 11, and 1 on X
Relative risks compared to the general population vary and account for about half of the cases

14
Genetic Risk Alleles Improve Performance of PSA Isoforms
+ Aggressive Disease– Amundadottir et al. Nat Genet, 38: 652, 2006– Freedman et al. Proc Natl Acad Sci U S A, 103:14068, 2006– Suuriniemi et al. Cancer Epidem Biomarkers Prev, 16: 809, 2007– Wang et al. Cancer Res, 6: 2905, 2007– Cheng et al. Eur J Hum Genet, 16: 496, 2008– Helfand et al. J Urol, (in press), 2008– Gudmundsson et al. Nat Genet, 40: 281, 2008– Beebe-Dimmer et al. Int J Cancer, 122: 2876, 2008
- Aggressive Disease– Zanke, et al. Nat Genet, 39: 989, 2007 – Zheng et al. N Engl J Med, 358: 910, 2008 – Eeles et al. Nat Genet, 40: 316, 2008– Thomas et al. Nat Genet, 40: 310, 2008– Severi et al. Cancer Epidemiol Biomarkers, 16: 210, 2007
Profiling for Aggressive Disease
15
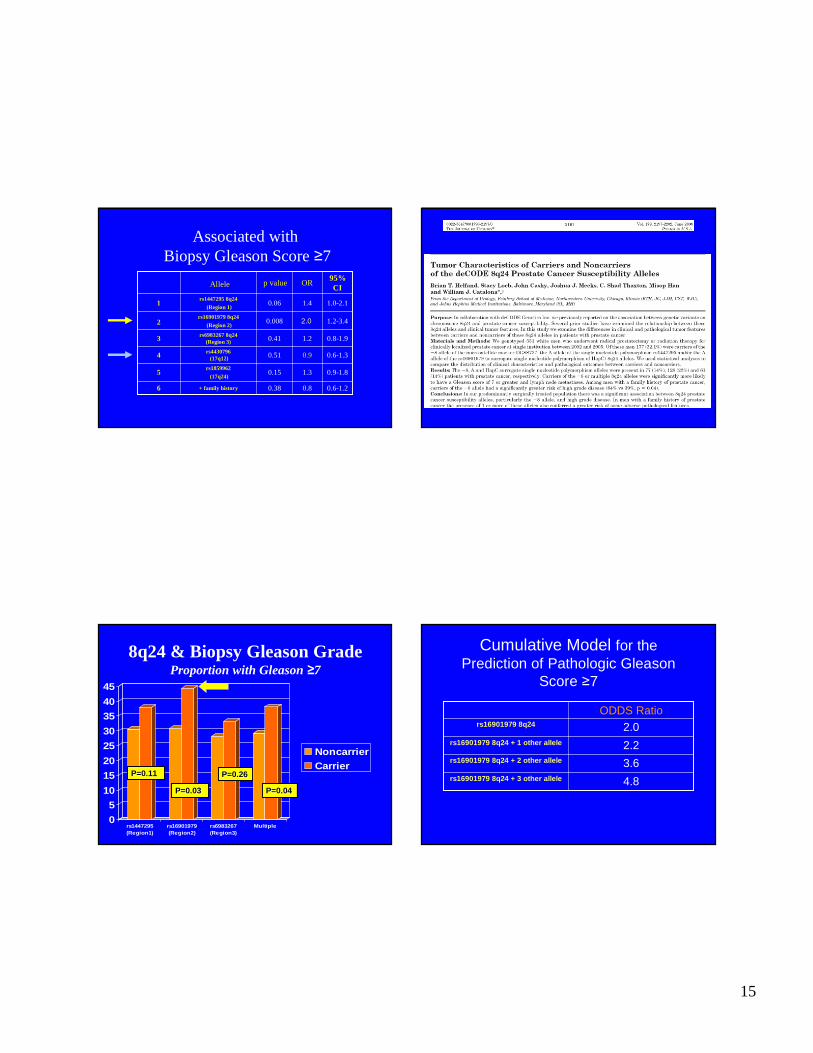
Associated withBiopsy Gleason Score ≥7
0.6-1.20.80.38+ family history6
5
4
3
2
1
0.9-1.81.30.15rs1859962
(17q24)
0.6-1.30.90.51rs4430796(17q12)
0.8-1.91.20.41rs6983267 8q24(Region 3)
1.2-3.40.008rs16901979 8q24
(Region 2)
1.0-2.11.40.06rs1447295 8q24
(Region 1)
95% CI
ORp valueAllele
2.02.0
8q24 & Biopsy Gleason GradeProportion with Gleason ≥7
0
5
10
15
20
25
30
35
40
45
rs1447295(Region1)
rs16901979(Region2)
rs6983267(Region3)
Multiple
NoncarrierCarrier
P=0.11P=0.11
P=0.03P=0.03
P=0.26P=0.26
P=0.04P=0.04
Cumulative Model for the Prediction of Pathologic Gleason
Score ≥7
4.8rs16901979 8q24 + 3 other allele
3.6rs16901979 8q24 + 2 other allele
2.2rs16901979 8q24 + 1 other allele
2.0rs16901979 8q24
ODDS Ratio
16
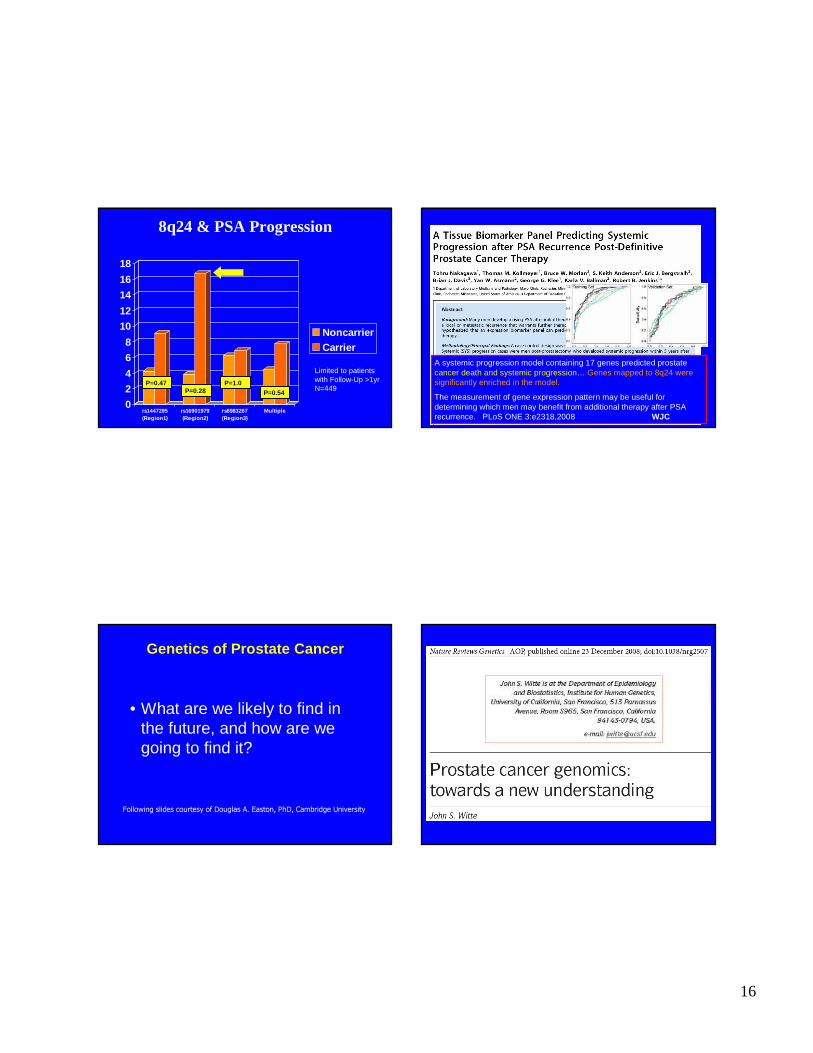
8q24 & PSA Progression
0
2
4
6
8
10
12
14
16
18
rs1447295(Region1)
rs16901979(Region2)
rs6983267(Region3)
Multiple
NoncarrierCarrier
Limited to patientswith Follow-Up >1yrN=449
PP=0.47=0.47PP=0.28=0.28
PP=1.0=1.0
PP=0.54=0.54
A systemic progression model containing 17 genes predicted prostate cancer death and systemic progression… Genes mapped to 8q24 were significantly enriched in the model.
The measurement of gene expression pattern may be useful for determining which men may benefit from additional therapy after PSA recurrence. PLoS ONE 3:e2318,2008 WJC
Genetics of Prostate Cancer
• What are we likely to find in the future, and how are we going to find it?
Following slides courtesy of Douglas A. Easton, PhD, Cambridge University
17
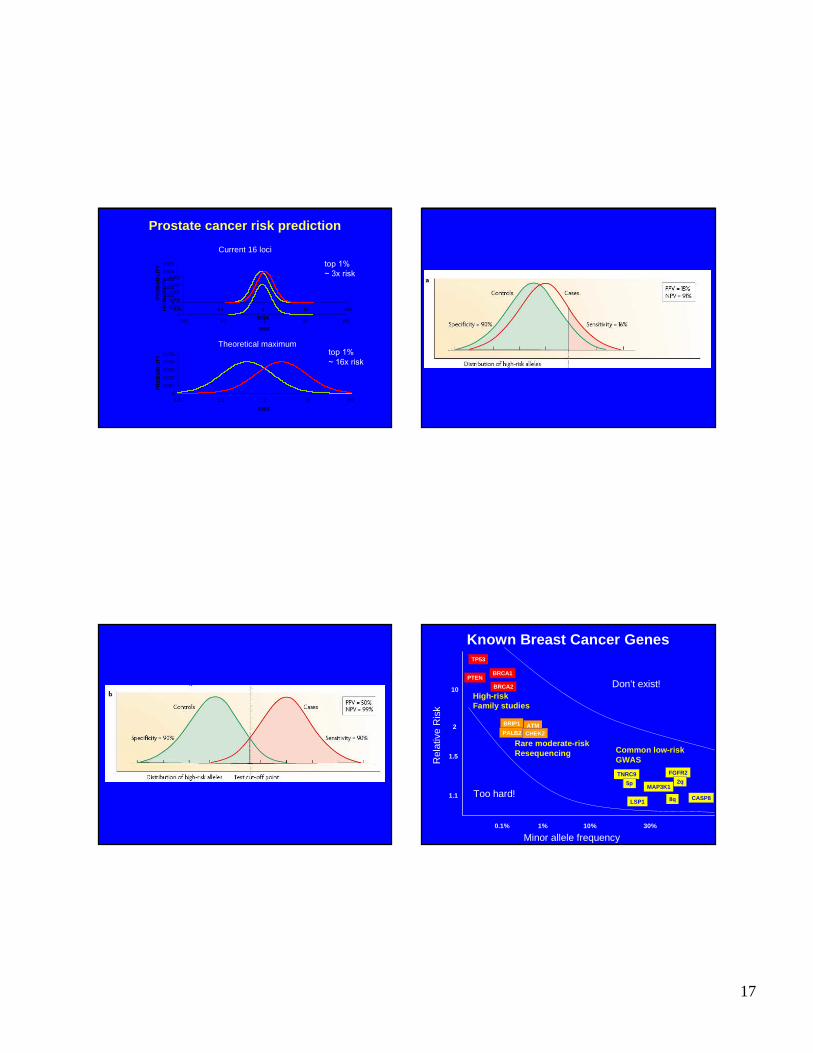
Prostate cancer risk prediction
0
0.001
0.002
0.003
0.004
0.005
0.01 0.1 1 10 100
RISK
PR
OB
AB
ILIT
Y
Theoretical maximum
Current 16 loci
0
0.001
0.002
0.003
0.004
0.005
0.01 0.1 1 10 100
RISK
PR
OB
AB
ILIT
Y
0
0.001
0.002
0.003
0.004
0.005
0.01 0.1 1 10 100
RISK
PR
OB
AB
ILIT
Y top 1%~ 3x risk
top 1%~ 16x risk
Known Breast Cancer Genes
1% 10% 30%
1.1
1.5
2
Minor allele frequency
Rel
ativ
e R
isk
10
0.1%
BRCA1
BRCA2
TP53
PTEN
High-riskFamily studies
BRIP1
PALB2ATMCHEK2
Rare moderate-riskResequencing
Don’t exist!
Too hard!
Common low-riskGWAS
CASP8
FGFR2TNRC9
LSP1
MAP3K1
8q
2q5p

18
Prostate Cancer Susceptibility Loci
1% 10% 30%
1.1
1.5
2
Risk allele frequency
Rel
ativ
e R
isk
10
0.1%
High-riskLinkage studies
Rare low/moderate riskResequencing
Common low riskAssociation studies
11q13
MSMBKLK2/3
3p12
6q25
BRCA2
2p15
JAZF1
BRCA1?
NBS1
CHEK2?
8q
8q
TCF2
8q 17q
LMTK2
Xp11
Prostate Cancer Loci to Find?
1% 10% 30%
1.1
1.5
2
Minor allele frequency
Rel
ativ
e R
isk
10
0.1%
11q13
MSMBKLK2/3
3p12
6q252p15
JAZF1
8q
8q
TCF28q 17q
LMTK2
Xp11New/combined scans/follow-ups
Better arrays
Resequencing
Large Genome-Wide Scans Detect More Small-Effect Variants
• In a collaborative study with deCODE genetics (33,000 cases and 45,000 controls), we identified SNPs associated with cancer at multiple sites (lung 1.15, bladder 1.12, prostate 1.07, and cervix 1.31)
• Thus, we have identified genetic variants that confer susceptibility to several cancers that have strong environmental components to their risk
RafnarRafnar T et al, T et al, Nat Genet.Nat Genet. 2009 Feb;41(2):2212009 Feb;41(2):221--7. 7. EpubEpub 2009 Jan 182009 Jan 18
Implications
• Many new genetic prostate cancer markers
• May provide insights into prostate carcinogenesis and strategies for prevention and treatment
• Some will contribute significantly to patient care