the great debate in neonatal piccs: catheter tip location ...fannp.org/fannppdf13/a06a the great...
TRANSCRIPT

The Great Debate in Neonatal PICCs: Catheter Tip Location and What IS Central? Elizabeth Sharpe, DNP, ARNP, NNP-BC, VA-BC Neonatal Nurse Practitioner St. Mary’s Medical Center, West Palm Beach, FL
The speaker has disclosed that she is a clinical education consultant for Argon Medical Devices, which could be perceived as having a bearing on her presentation of this subject. She has no significant financial interest or relationship with any other companies or the manufacturer(s) of any commercial product and/or service that will be discussed as part of this presentation.
Session Summary The presenter will review of the latest evidence, including anatomical, hemodynamic and pharmacologic implications of catheter tip location, and the potential risks for serious complications associated with suboptimal tip location. Also, a look at new technological advances.
Session Objectives Upon completion of this presentation, the participant will be able to:
identify the difference between central and non-central catheter tip locations;
identify the implications of catheter tip locations;
name three complications that occur due to movement of the catheter tip location;
identify two risk factors for malposition;
identify at least two preventive strategies to minimize complications.
References Eifinger, F., Brisken, K., Roth, B. & Koebke, J. (2011). Topographical anatomy of central venous system in extremely low-
birth weight neonates less than 1000 grams and the effect of central venous catheter placement. Clinical Anatomy, 24(6): 711-716.
Kugelman, A., Inbar-Sanado, E., Shinwell, E., Makhoul, I., Meiron, L., Zangen, S., Wattenberg, O., Kaplan, T., Riskin, A. & Bader, D. (2008). Iatrogenesis in neonatal intensive care units: Observational and interventional, prospective, multicenter study. Pediatrics, 120(3): 550-555.
Nadroo, A., Lin, J., Green, R., Magid, M. & Holman, I. (2001). Death as a complication of peripherally inserted central catheters in neonates. Journal of Pediatrics, 138(4): 599-601.
Nowlen, T., Rosenthal, G., Johnson, G., Tom, D. & Vargo, T. (2002). Pericardial effusion and tamponade in infants with central catheters. Pediatrics, 110(1): 137-142.
Pettit, J. (2002). Assessment of infants with peripherally inserted central catheters: Part 1. Advances in Neonatal Care, 2(6): 304-315.
A6a FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 1 of 8

Pettit, J. & Wyckoff, M. (2007). Peripherally inserted central catheters guidelines for practice (2nd ed). Glenview, IL: National Association of Neonatal Nurses.
Warren, M., Thompson, K., Popek, E., Vogel, H. & Hicks, J. (2013). Pericardial effusion and cardiac tamponade in neonates: Sudden unexpected death associated with total parenteral nutrition via central venous catheterization. Annals of Clinical & Laboratory Science, 43(2): 163-171.
Session Outline See presentation handout on the following pages.
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 2 of 8

The Great Debate in Neonatal PICC’s
Catheter Tip Location & What IS Central?
Elizabeth Sharpe, DNP, ARNP, NNP‐BC, VA‐BC
FANNP, October 2013
Disclosures
• Clinical Education Consultant for Argon Medical Devices
k l d f i i• Acknowledgements for Images Permissions
– Argon Medical Devices
– Lumos Catheter Systems
• Transitioning from umbilical lines• Premature infants < 1500 gms• Hyperosmolar ( > 600 mOsm/L) • Irritant medications• pH <5 or >9 (INS 2011)
What are the indications for PICCs?
pH <5 or >9 (INS, 2011) • More than 6 days of hyperosmolar IV therapy (CDC,2011)
• GI, congenital cardiac defects• Limb anomalies, birth injuries
Review
• Chemistry
• Physics
• Anatomy
• Physiology
Osmosis and Cell Volume
IsotonicHypotonic Hypertonic
Courtesy & ©Argon Medical Devices
Medication pH Osmolarity Irritant
Ampicillin250 mg/ml SW100 mg/ml SW
8.0‐10.0 1215 mOsm/L
293 mOsm/L
X
Gentamicin 3.0‐5.5 262 mOsm/L
Meropenem 7.3‐8.3 ~300 mOsm/L X
Phenobarbitol 9.2‐10.2 > 9000 mOsm/L
Piperacillin/ tazobactam
5‐6 270‐445 mOsm/L
Vancomycin 2.5‐4.5 249 mOsm/L X
Acyclovir 10.5‐11.6 278 mOsm/L X
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 3 of 8
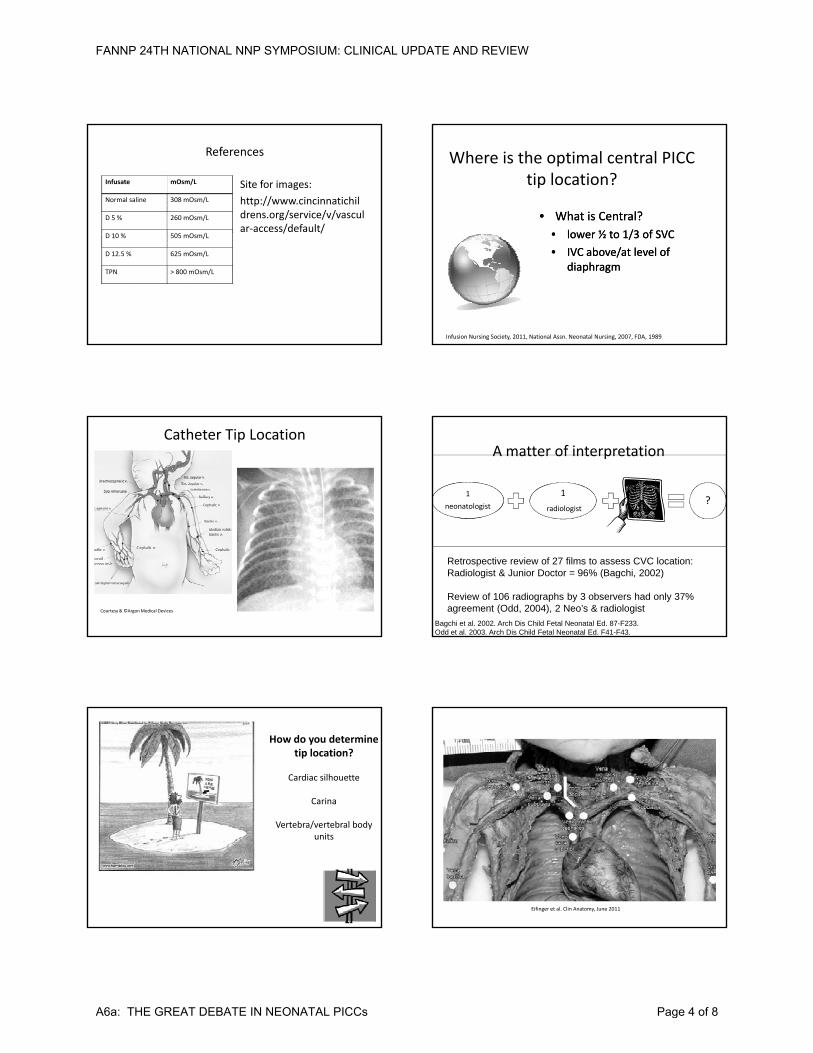
References
Infusate mOsm/L
Normal saline 308 mOsm/L
D 5 % 260 mOsm/L
D 10 % 505 O /L
Site for images:
http://www.cincinnatichildrens.org/service/v/vascular‐access/default/
D 10 % 505 mOsm/L
D 12.5 % 625 mOsm/L
TPN > 800 mOsm/L
Where is the optimal central PICC tip location?
•• What is Central?What is Central?
•• lowerlower ½ to 1/3 of SVC½ to 1/3 of SVC•• lower lower ½ to 1/3 of SVC ½ to 1/3 of SVC
•• IVC IVC above/at level of above/at level of diaphragmdiaphragm
Infusion Nursing Society, 2011, National Assn. Neonatal Nursing, 2007, FDA, 1989
Catheter Tip Location
Courtesy & ©Argon Medical Devices
1
neonatologist
1
radiologist1 Xray1 Xray ?
A matter of interpretation
Bagchi et al. 2002. Arch Dis Child Fetal Neonatal Ed. 87-F233.Odd et al. 2003. Arch Dis Child Fetal Neonatal Ed. F41-F43.
Retrospective review of 27 films to assess CVC location: Radiologist & Junior Doctor = 96% (Bagchi, 2002)
Review of 106 radiographs by 3 observers had only 37% agreement (Odd, 2004), 2 Neo’s & radiologist
How do you determine tip location?
Cardiac silhouette
Carina
Vertebra/vertebral body units
Eifinger et al. Clin Anatomy, June 2011
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 4 of 8

Diameter/Length 700 grams 900 grams Term Adult
Basilic 1.1 +/‐ 0.3 mm 6 mm
Cephalic 1.2 +/‐ 0.2 mm 8 mm
Subclavian 2.6 +/‐ 0.4 mm 19 mm
Brachiocephalic 3.3 +/‐ 0.5 mm 19 mm
Brachiocephalic to cavoatrial junction
1.5 cms
Vessel & catheter sizes
cavoatrial junction
Superior Vena Cava ~ 4 mm/1.5 cm
4.1 +/‐ 0.7 mm 6‐8 mm/1.5‐2.5 cm
20 mm/7cms
Cardiovascular surgeons, Dr. Robert Anderson, Eifinger et al, 2011, Clinical Anatomy
Catheter Measurement
1 Fr or 29 g 0.33 mm
2 Fr or 26 g 0.67 mm
3 Fr or 19 g 1.1 mm
Vessel diameters are in millimetersVessel lengths are in centimeters
• “The CVC tip should remain outside the cardiac silhouette but still within the vena cavae:
– Approximately 1 cm outside the cardiac silhouette in premature infants
– Approximately 2 cm in term infants
• Retrospective case reviews of 61 patients
• Mean gestational age 30 weeks
• Mean birth weight 1 kg
Nowlen et al. Pediatrics Vol. 110 No. 1 July 2002
• Complication rates related to catheter tip placement
– N= 1266 PICCs in 1053 patients
– Mean age 6.49 +/‐ 2 years
– Central (SVC, RA, IVC at/above diaphragm)
• Central group had 3.8% of complications
– Noncentral (all other tip locations)
• Noncentral group had 28.8% of complications
• Patients with catheter tips in noncentral locations were 8x more likely to experience a complication!
Racadio, Doellman, Johnson, Bean & Jacobs, Pediatrics, 2001
Complication Central(SVC, RA, IVC > diaphragm)N = 1096
Noncentral(subclavian, brachiocephalic)N = 169
Phlebitis 1.5% 10.0%
Occlusion 1.7% 6.5%
Pediatric Complication Rates: Central vs. Noncentral.
Leaking .1% 11.2%
Mechanical .3% 1.2%
Infection .2% 0
Total 3.8% 28.8%
Racadio et al. Pediatrics 2001
The noncentral group had shorter mean PICC duration than the central group (9.3 days vs. 16.4 days) and was 8 times more likely to develop a complication
Should we settle?
• Complications associated with central and non‐central venous catheters in a NICU
– N= 91 noncentral (PINCCs) and 889 central (PICCs) in 750 neonates
– Complication rates: PINCCs 44% vs PICCs 25.2%
– Phlebitis, infection, leakage, occlusion, infiltration
– Most common complication in PINCCs was infiltration
• PINCCs were more than twice as likely to develop a complication compared to PICCs
Colacchio, Deng, Northrup, Bizzarro, J Perinatology, 2012
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 5 of 8

More on tip location• PICC tip position and risk of associated complications in neonates
– N=319 infants: Central 203, Noncentral 116
– Central catheters had lower rates of complication 30 vs 46 6% vs noncentralcomplication 30 vs. 46.6% vs noncentral catheters
– Midclavicular placement: between lateral and medial border of clavicle
– Midclavicular placement was 3x more likely to develop infiltration or mechanical complications
Jain, Deshpande, Shah, J Perinatology AOP, 2012
Risk factors related to tip location
• Noncentral PICC tip locations, age < 1 year and PICU exposure were risk factors for PICC removal.
• N = 2574 PICCs in 1807 patients (median age 5 )years)
• Central = SVC or IVC
• Noncentral catheters were more likely to have complications needing removal than central (43.8% vs. 16.2%)
Jumani, Advani, Reich, Gosey & Milstone, JAMA Pediatrics 2013
The latest on Tip Position• N = 237 PICCs in 200 neonates, 207 central, 30 noncentral
• Central = SVC or IVC
• Noncentral + subclavian, CAJ, RA, iliac, axillary ivein
• Mean dwell time: 11.7 days in central vs. 9.8 days in noncentral
• Noncentral had higher incidence of removal due to extravasation.
Costa, Bueno, Alves & Kimura, JOGNN, 2013
Importance of Radiographic Monitoring
• Catheter tip position should be confirmed by x-ray or other imaging modality and rechecked periodically (FDA, 1989)
• Catheters with tips located outside the• Catheters with tips located outside the SVC/IVC are from 2 to 8 x more likely to develop a complication (Colacchio et al., 2012, Jain et al., 2012, Racadio et al, 2001)
Implications for Practice
• Radiographic monitoring and consistent patient positioning support accurate catheter tip confirmation.
• Accurate knowledge of the catheter tip• Accurate knowledge of the catheter tip location is crucial in prevention of catheter-related complications, as catheters whose tips are located outside the SVC/IVC have increased risk of complications.
Keys to Consistent Monitoring of Catheter Tip Location
• Consistent positioning of the extremity to bring catheter tip to deepest location
– Upper extremity adducted if basilic vein
Upper extremity abducted if cephalic vein– Upper extremity abducted if cephalic vein
– Lower extremity flexed
• In situ patient dynamics can impact catheter tip location
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 6 of 8

What can you do when the catheter is unable to be inserted into central placement?
• If catheter tip is in brachiocephalic or subclavian, may use as a peripheral as a temporarymeasure if
Midclavicular
p yblood returns and catheter flushes
• May withdraw catheter to appropriate midline placement.
• Peripheral limitations ( no > D12.5)
NANN Guidelines for Practice, 2007
Common malpositions
• Withdrawal of catheter– Advantages: Removal from undesirable location, ?
– Disadvantages:
• Break into sterile site, manipulate catheter, increase risks for infection, skin trauma, inadvertent overdislodgement, stress
Malposition Management
• Sacrifices optimal tip location in superior vena cava (INS, AVA, NANN, FDA)
• Repositioning Maneuvers– Advantages: less traumatic, less invasive, less stress, can achieve optimal tip location
– Disadvantages: Are there any?
– Gravity + hemodynamic flow + infusion induced movement
• In situ patient dynamics
– Coughing, crying
– Changes in thoracic or abdominal cavity pressures
– Unfavorable positioning (consider counter‐gravity)
• Iatrogenic mechanical dynamics
– High frequency oscillator/jet ventilation
Risk factors for malposition
High frequency oscillator/jet ventilation
– Infusion induced catheter movement due to forceful flushing
• Securement failure
– Improper or inadequate securement, loose dressing
Pearls for Placement: Turn head towards ipsilateral side for upper extremity insertion. Level the bed.
After catheter adjusted, is a follow up x‐ray required?
• Yes!
• “Verify new catheter tipcatheter tip location via radiologic means after all repositioning efforts”
• FDA, INS 2011, NANN 2007
Pearls for PICC Placement
• Premeditate to medicate?• Coordinate with planned extubation or ventilatory
support changes• Coordinate with volume expansion, after fluid status
optimized• Coordinate after blood products support (PRBCs,
platelets)• Place before anticipated surgery• Place before hypothermia protocol initiated• Timing is everything!
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 7 of 8

Thank you!
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A6a: THE GREAT DEBATE IN NEONATAL PICCs Page 8 of 8