the hotline is free, confidential, and always available. help a love one, friend, or yourself. you...
TRANSCRIPT

1800-273-TALK (8255)The hotline is FREE, confidential, and always available.
Help a love one, friend, or yourself. You don’t have to be suicidalto use the Hotline; anyone is welcome to call.
A Program of Mountain States Group, Inc.
5 years-Crisis Clinic of King County
8 years- Idaho H&W Mobile Crisis Unit
4 years- St Alphonsus emergency dept.
John R. Reusser, LCSW
mental disorder, past suicide attempts, social isolation, physical illness, unemployment, family conflict, family history of suicide, impulsivity, incarceration, hopelessness, seasonal variation, serotonergic dysfunction, agitation/sleep, childhood abuse, exposure to suicide, homelessness
Suicide Risk Factors
Thomas Joiner, Phd Clinical Faculty Florida State University
Author of Books Including: Why People Die by Suicide, Lonely at the Top, Myths About Suicide
Survivor of Suicide
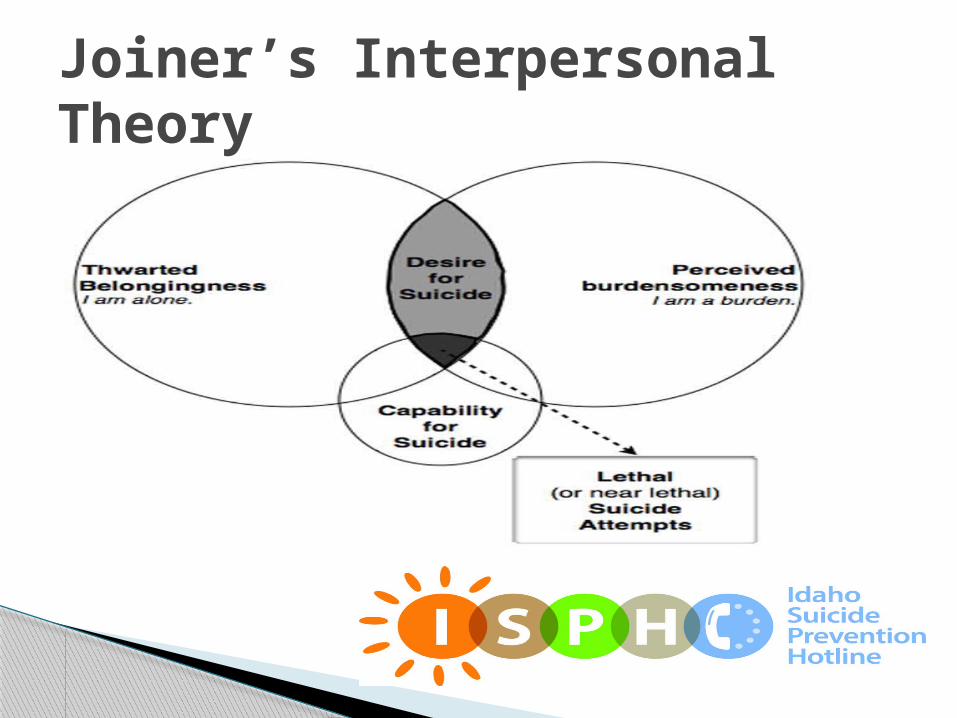
Joiner’s Interpersonal Theory of Suicide
1.Thwarted Belongingness-we have a fundamental need to belong
2. Perceived Burdensomeness-feeling that my suicide would be a relief to others
(together these lead to hopelessness when seen as unchangeable -and active suicidal desire)
3. Acquired Ability for self-harm-in response to repeated exposure to physically painful and/or trauma/ fear-inducing experiences-leading to reduced fear of suicide &increased pain tolerance
Interpersonal Theory-3 parts
Joiner’s Interpersonal Theory
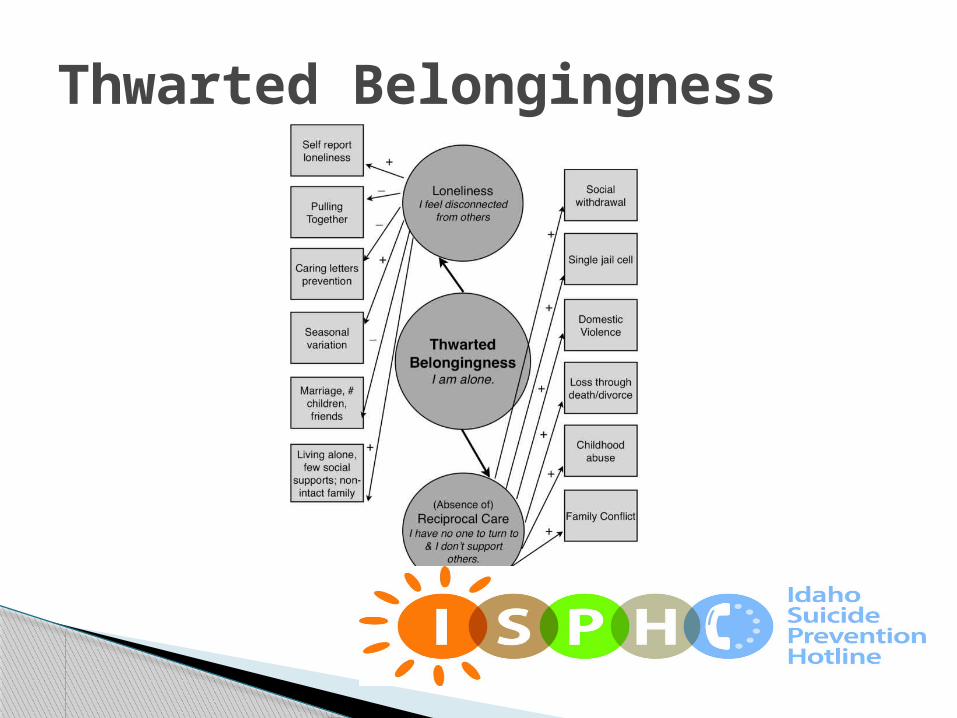
Thwarted Belongingness
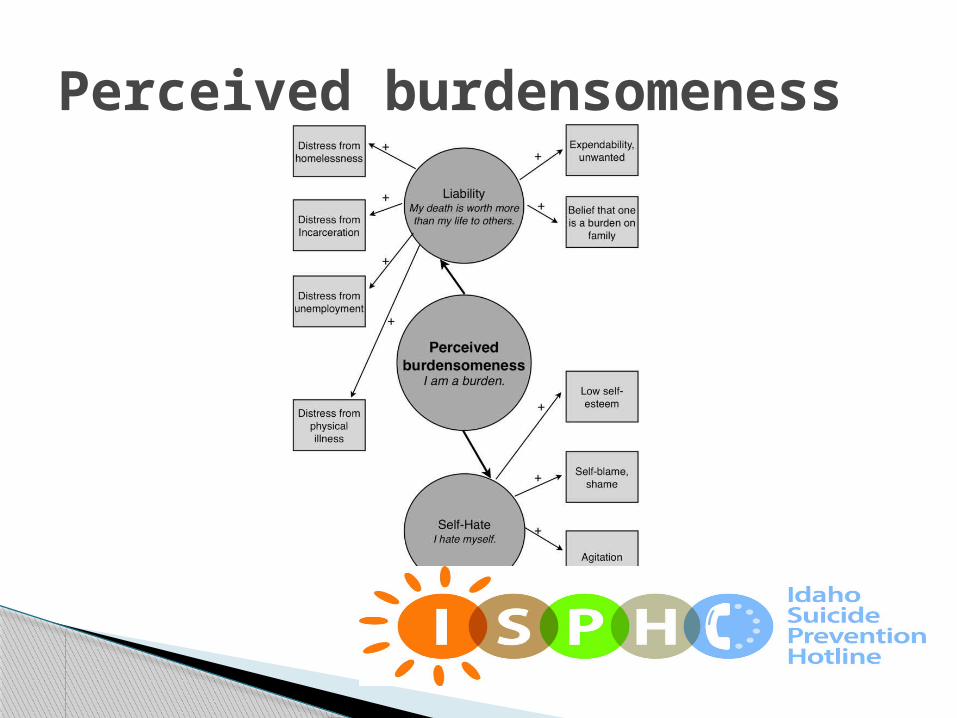
Perceived burdensomeness

Acquired capability for self-harm
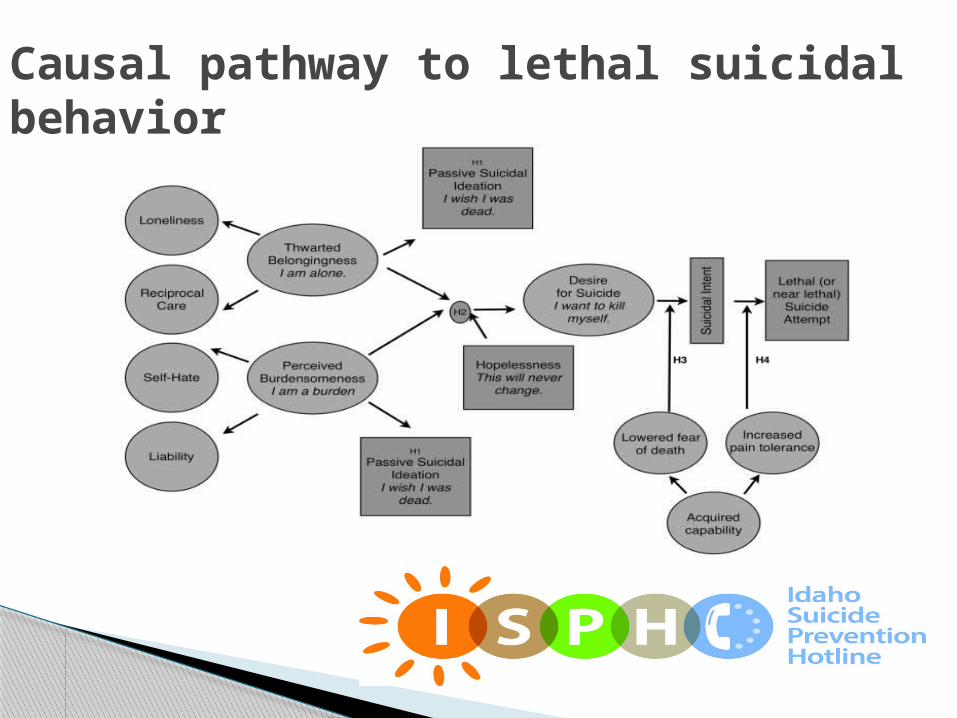
Causal pathway to lethal suicidal behavior

90% of people who die by suicide had a diagnosable psychiatric disorder at the time of their death. Many were under the care of a primary care physician or other medical specialist.
One study found that 20% of older patients who committed suicide had visited their primary care physician on the same day as their suicide, 40% had visited their primary care physician within one week and 70% within one month.
Suicide and primary care settings
Provides education Straightforward roles for everyone in your
practice setting Common sense tools for staff and patients Resources for treatment and ongoing
monitoring/follow up for patients with thoughts to suicide.
WICHE Toolkit- helping suicidal patients in primary care settings

Getting started-
Educating Clinicians & Office Staff

1.Communicate with staff about the new suicide prevention initiative in your office.
2. Meet to develop the “Office Protocol” for potentially suicidal patients. See the “Office Protocol Development Guide” instruction sheet in the Toolkit.
3. Schedule trainings for staff members according to individuals’ prevention responsibilities determined in Step 2.
Quick start guide steps 1-3

4. Develop a referral network to facilitate the collaborative care of suicidal patients. Use the “Developing Mental Health Partnerships” materials in the Toolkit.
5.Read the Toolkit’s “Primer”. Providers may wish to study the last two sections on Suicide Risk Assessment and Intervention first. The first three sections may then be reviewed in order to gain knowledge about Prevalence, Comorbidity, Epidemiology, and Prevention.
6.Order community and patient education tools, such as suicide prevention posters/brochures.
Quick start guide steps 4-6

• The last Idaho hotline closed in 2006
• Idaho - last state in the US to be without a statewide
suicide hotline
• Planning efforts –Technical Work Group
• 2011 UWTV Community Assessment –quality mental health
support
• Initial Funders and Supporters
• 2013 UWTV Community Impact- access to quality mental
health services
ISPH History

• Launch
• Current Model
• Quality Program
• Research Based
• Accreditation
• Training
• Volunteers
ISPH Facts

Volunteers: Lifeblood of Hotline
• Suicide in Idaho
• Staff Information
• Program Outcomes- Call Summary
• Populations and Areas of Idaho Impacted
• Caller Needs/Issues
ISPH Outcomes & Impact
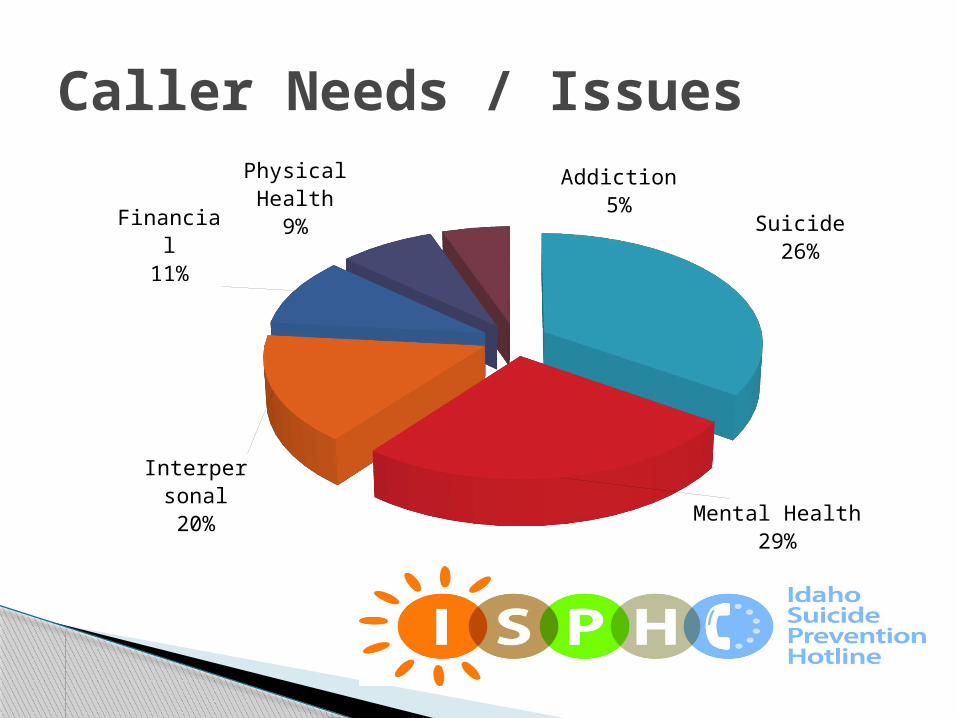
Caller Needs / Issues
Suicide26%
Mental Health29%
Inter-personal
20%
Financial11%
Physical Health
9%
Addiction5%

• 12% of total call volume for 2013
• Collaboration with local resources, IDVS, Veterans Administration & National Veteran’s Crisis Line
Supporting Veterans, Military Members & Their Families

• United Way of Treasure Valley• Idaho State University: Planning Grant, Americorps Position• Speedy Foundation• Idaho Division of Veterans Services• ID Dept. of Health and Welfare, Division of Behavioral
Health• Saint Alphonsus • Suicide Prevention Action Network (SPAN) Idaho• JA and Kathryn Albertson Foundation• Saint Luke’s Health System• Lion’s Club Sight and Hearing Foundation• 211 Idaho, Schools, colleges and universities, police and
emergency responders, hospitals, service providers
Partners, Funders, Collaborators

• The Interpersonal Theory of Suicide- Thomas Joiner Order the WICHE Toolkit http://www.sprc.org
• www.idahosuicideprevention.org
www.facebook.com/idahosuicide prevention
• ISPH outreach- Nancy Pounds
• General info- John Reusser
• Volunteer interest-Nina Leary
Info/ contacts