the hyperarousal model of primary insomnia from a
TRANSCRIPT

The hyperarousal model of Primary Insomnia from a
neurobiological perspective.
Name: Martine Groefsema
Student number: 5622735
University of Amsterdam
MSc in Brain and Cognitive Science
Cognitive Neuroscience
Supervisor: dr. W. F. Hofman
Co-assessor: dr L. M. Thalamini

2
Abstract
Despite the growing literature on insomnia, little is known about the underlying
pathophysiology causing the disorder. Previous literature has viewed primary
insomnia mainly as a psychological problem, but more recently studies began to find
more evidence for physiological differences in patients with primary insomnia. The
aim of this review is to discuss the concept of hyperarousal from the higher system to
the molecular processes, and discuss its relevance in the pathology of primary
insomnia. Electrophysiological studies demonstrate increased levels of cortical
arousal in primary insomnia during different stages of sleep. Studies on regional brain
metabolism are limited and are in the need for further research. I conclude that there is
an imbalance between arousing and sleep-inducing brain activity in primary insomnia,
resulting in hyperarousal. However, whether this is the main cause of primary
insomnia can not be concluded. Further research on genetic vulnerability is needed.

3
Content Introduction………………………………………………………………. 4 Chapter 1: Different types and characteristics of insomnia…………….6 Chapter 2: Normal sleep processes……………………………………….8
2.1 Neurophysiology of normal sleep……………………………….9 2.2 Neurobiology of normal sleep…………………………………..10
Chapter 3: Hyperarousal model of insomnia……………………………15
3.1 Neurophysiology of primary insomnia…………………………15 3.2 Neurobiology of primary insomnia…………………………….20
3.2.2 Neurotransmitters…………………………………….22
Chapter 4: Heritability……………………………………………………23
Chapter 5: Treatment……………………………………………………..25
Chapter 6: Discussion……………………………………………………..28 References…………………………………………………………………..31
Appendixes………………………………………………………………….32

4
Introduction
Patients with insomnia experience inadequate nocturnal sleep in some way.
They may describe difficulty falling asleep, frequent awakening, or early morning
awakening with inability to return to sleep. This disorder of initiating and/or
maintaining sleep causes sleep disruption and has major daytime consequences. There
are two types of insomnia; primary and secondary insomnia. Primary insomnia not
attributable to medical, psychiatric, or environmental causes, while secondary
insomnia is. This review will focus on primary insomnia because it has a
homogeneous character because it does not reflect effects of a comorbid disorder.
Primary insomnia affects approximately 3-5% of the general population (Ohayon,
2002) and is therefore an important topic of research.
A form of hyperarousal became the main concept of primary insomnia models.
The hyperarousal model assumes that an underlying state of arousal interferes with
normal biological processes associated with sleep initiation and maintenance (Bonnet
and Arand, 1997). Many different models were designed, mostly based on somatic
(e.g. heart rate) and cognitive arousal (e.g. dysfunctional thoughts). Riemann and
colleagues (2010) summarized the current literature and generated a neurocognitive
model of insomnia, consisting of a cognitive-behavioural and a neurobiological
domain. The authors emphasize that primary insomnia can not only be linked to
alterations on psychological level, but is also associated with measurable deviations of
neuroendocrine as well as electro-and neurophysiological alterations.
In this review the focus will be on the neurobiological domain, because
emerging techniques allowed us to investigate cortical activity more extensively.
Moreover, because primary insomnia is not related to a comorbid disorder, it can be

5
hypothesized that there is some form of genetic vulnerability. This bottom-up
approach assumes a (genetically determined) dysfunction in sleep-wake regulating
neural circuitries originating from the brainstem and leading to sleep disruptions.
With the use of electroencephalography (EEG) and functional magnetic resonance
imaging (fMRI), cortical and even subcortical arousal could be investigated. And the
hyperarousal model can be reviewed with the focus on neurobiological arousal.
One limitation of studying insomnia is the occurrence of many different types.
In the first chapter of this review, the different types and characteristics of insomnia
will be discussed. The second chapter will provide some necessary background
information on normal sleep processes. Neurophysiological as well as neurobiological
processes of normal sleep will be quickly described. The third chapter is the focus of
this review. In this chapter the hyperarousal model will be described, with its evidence
based on electrophysiological and MRI studies. If a hyperaroused state is correlated
with the pathology of primary insomnia, it can be questioned whether this is a
predisposing factor or a consequence of the disorder. Therefore in the fourth chapter
heritability studies of primary insomnia will be discussed. The fifth chapter describes
current treatment of primary insomnia, which is mainly based on changing cognitive
arousal by cognitive behavioural therapy. However, if primary insomnia is caused by
a (genetic) hyperarousal of the neuronal sleep-wake circuitry, other treatment methods
based on a bottom-up approach may be more successful. In the last chapter of the
thesis the evidence will be considered and the main question will be answered: is
hyperarousal the model for explaining the pathology of primary insomnia, based on a
neurobiological perspective? Last, some suggestions for further research will be
proposed.
6
Chapter 1: Different types and characteristics of insomnia.
In research on insomnia it is important to recognize the differences between
the different types (primary and secondary) of insomnia. The general definition of
insomnia is: ‘repeated difficulty with sleep initiation, duration, consolidation, or
quality that occurs despite adequate time and opportunity for sleep, and this results in
some form of daytime impairment’ (DSM-IV, 1994). The book ‘International
classification of sleep disorders’ distinguishes 11 different types of insomnia, of
which 3 types of primary insomnia. This heterogeneity of the disorder makes it
difficult to investigate and understand the psychopathology. Because of the possibility
that the different types of primary insomnia also have different underlying causes, it is
important to distinguish among the different types first.
The first type of primary insomnia is idiopathic insomnia. The definition of
idiopathic insomnia is: ‘a lifelong inability to obtain adequate sleep that is
presumably due to an abnormality of the neurological control of the sleep-wake
system’ (DSM-IV, 1994). So idiopathic insomnia is a long-standing disorder, which
typically begins during childhood, and has no clear environmental causes. The second
type of primary insomnia is called psychophysiological insomnia. The definition of
psychophysiological insomnia is: 'a disorder of somatised tension and learned sleep-
preventing associations that results in a complaint of insomnia and associated
decreased functioning during wakefulness' (DSM-IV, 1994). So psychophysiological
insomnia is a disorder which often begins with a period of stress and can be
developed at any time point in life. Unfortunately, while there are clear distinctions
between idiopathic and psychophysiological insomnia, such as the onset period and
what triggers the pathology, not many studies specified the subtypes of primary
7
insomnia, and included idiopathic insomnia as well as psychophysiological insomnia
patients. And because not many studies made a distinction between these types, this
review includes both idiopathic as psychophysiological primary insomnia too. The
third and last type of primary insomnia is called sleep-state misperception (also
known as paradoxical insomnia). This type will not be included in this review,
because sleep-state misperception insomnia is referred as subjective insomnia since
the dysfunctional sleep can not be objectively measured using physiological
measurements (DSM-IV, 1994). Some studies suggest that sleep-state misperception
may be a transitional state of dysfunction between an objective sleep disorder
(idiopathic and psychophysiological) and normal sleep (Salin-Pascual et al, 1992;
Bonnet & Arand, 1997). However, because the distinct ability of this subtype is still
questionable (Edinger& Krystal, 2003), no studies including these patients are
reviewed.
8
Chapter 2: Normal sleep processes
In order to say something about processes causing sleep disorders, we first
need to consider normal sleep processes. Many different models on normal sleep
regulation have been developed in the last decade. A very common model is the two-
process model by Borbély (1982). The two-process model postulates that two
processes are important in the regulation of sleep, a homeostatic factor (process S)
and a circadian factor (process C). The homeostatic factor rises during wakefulness
and declines during sleep. So this is an appetitive process that is determined by the
amount of time since the last bout of sleep. The longer the time spent awake, the
greater the drive for sleep. On the other hand, the circadian factor (process C) varies
with a 24-hour periodicity and is independent of the amount of preceding sleep or
wakefulness. Together these processes modulate the need for sleep and influence the
balance between central alertness and sleepiness (see figure 1).
A study of Perlis and colleagues (2001) suggested that this two-process model
should be expanded with a second homeostatic ‘process W’. Where the 'process S'
increases with extended wakefulness, the 'process W' is thought to increase with
extended sleep (Perlis et al., 2001). These two processes interact with each other and
deficits can cause sleep initiation and maintenance difficulties. A sleep disorder can
be caused by a decreased sleep propensity (so a low 'process S') or an increased wake
propensity (a hyperarousal or high 'process W'). In this case, primary insomnia can be
hypothesized as a sleep disorder mainly due to an abnormal or increased 'process W'.

9
Figuur 1: Two-process model for normal sleep (from Borbély, 1982). The C refers to the circadian factor and the S to the homeostatic factor.
2.1 Neurophysiology of normal sleep
The beginning of sleep research dates back to 1930s, where the studies mainly
used electroencephalogram (EEG) techniques. Kleitman and Dement (1957) were the
first to specify rapid-eye-movement sleep (REM sleep) and defined the cyclic pattern
of sleep as one cycle of REM-nonREM that lasts 90-100 minutes, with 4-5 cycles
repeating during one night. The non-REM sleep period is more specified by a
distinction of 3 different stages, based on EEG wave patterns. Every stage has a
characteristic EEG frequency and waveform. The first stage is characterized by a
transition from alpha waves (8-13 Hz) to theta waves (4-7 Hz). During stage 2 sleep
spindles (11-16 Hz) and K-complexes can occur. Sleep spindles and K-complexes are
rapid bursts of activity. Going into detail on this phenomenon will be beyond the
scope of this review. The third stage, also called slow-wave-sleep (SWS), is
characterized by an extreme amount of delta waves (0-4 Hz) (Carskadon &
Rechtschaffen, 2000).
For primary insomnia, the transition from wakefulness to sleep, also called the
sleep-onset-period (SOP), is extremely interesting because the inability of patients to
initiate sleep. In normal sleepers, the SOP is characterized by a decrease of high
frequency and an increase of slow frequency EEG activity (De Gennaro et al., 2001).
These results show global differences in EEG patterns. A more precise and localized

10
image of the processes during sleep can be made with the use of functional resonance
imaging (fMRI).
2.2 Neurobiology of normal sleep
Explaining the history of sleep research and describing all neuroimaging
studies on normal sleep processes would be beyond the scope of this review.
However, to get some background knowledge I will briefly summarize the current
literature of brain activation patterns during NREM and REM sleep in healthy
participants.
One main finding of early functional neuroimaging studies of sleep is a global
decrease of cerebral activity during NREM sleep compared to wakefulness, similar to
the EEG measurements (Buchsbaum et al., 1989; Maquet et al., 1992 ; Nofzinger et
al., 2002). Other studies found evidence for regional differences in activity patterns
during sleep. Decreased activity in thalamic structures during NREM sleep compared
to wakefulness has been found (Braun et al., 1997 ; Andersson et al., 1998; Kajimura
et al., 1999; Kjaer et al., 2002; Nofzinger et al., 2002). Second, a decrease in basal
ganglia structures (e.g. the caudate/ putamen) has been found repeatedly (Braun et al.,
1997; Kajimura et al., 1999). Third, a decrease in several frontal cortex areas (Braun
et al., 1997; Kajimura et al., 1999; Nofzinger et al., 2002). And fourth, REM sleep can
be characterized by an increased metabolism within the limbic system, pons and the
visual cortex (Maquet et al., 1996).
If we even zoom in more closely to the midbrain structures, a network that
promotes wakefulness can be defined, the ascending arousal reticular system (ARAS).
Evidence for the existence of an arousal system came from early work of Von
Economo (1930). He discovered that patients with encephalitis lethargica, who sleep
11
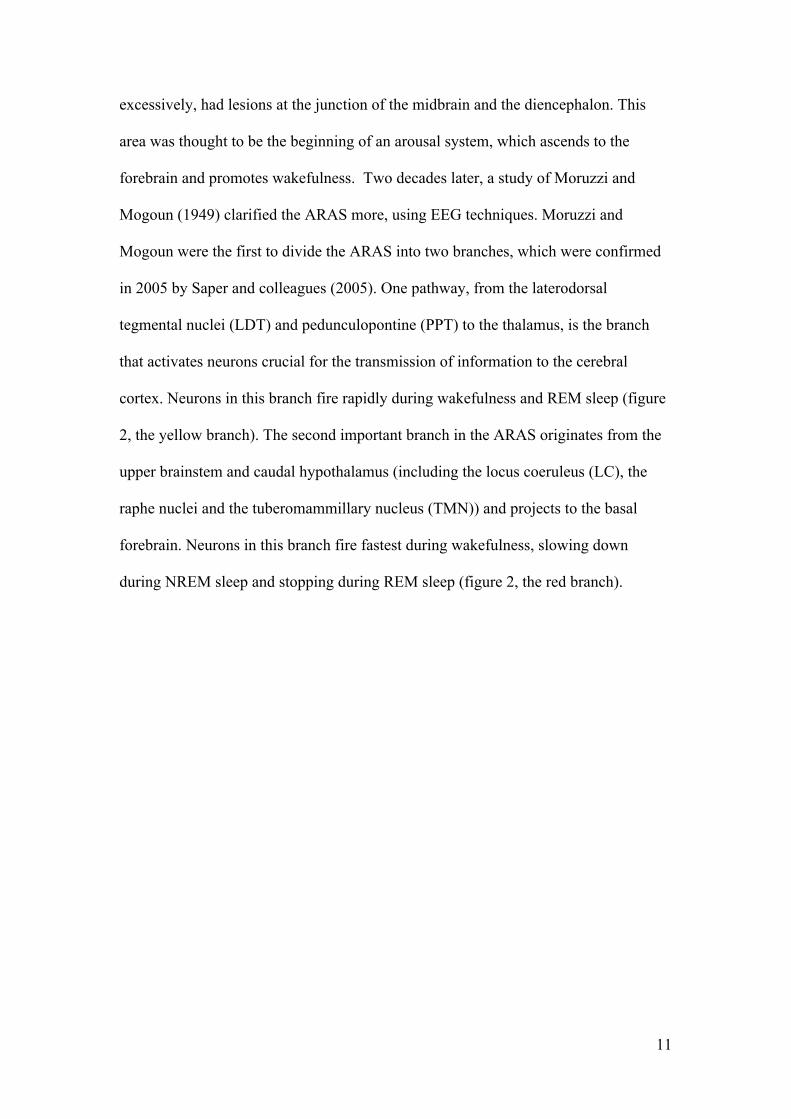
excessively, had lesions at the junction of the midbrain and the diencephalon. This
area was thought to be the beginning of an arousal system, which ascends to the
forebrain and promotes wakefulness. Two decades later, a study of Moruzzi and
Mogoun (1949) clarified the ARAS more, using EEG techniques. Moruzzi and
Mogoun were the first to divide the ARAS into two branches, which were confirmed
in 2005 by Saper and colleagues (2005). One pathway, from the laterodorsal
tegmental nuclei (LDT) and pedunculopontine (PPT) to the thalamus, is the branch
that activates neurons crucial for the transmission of information to the cerebral
cortex. Neurons in this branch fire rapidly during wakefulness and REM sleep (figure
2, the yellow branch). The second important branch in the ARAS originates from the
upper brainstem and caudal hypothalamus (including the locus coeruleus (LC), the
raphe nuclei and the tuberomammillary nucleus (TMN)) and projects to the basal
forebrain. Neurons in this branch fire fastest during wakefulness, slowing down
during NREM sleep and stopping during REM sleep (figure 2, the red branch).

12
Contrary to the ARAS, there is a network that promotes sleep. A key role in
this network is assigned to the ventrolateral preoptic nuclei (VLPO), a group of
neurons located in the hypothalamus. The VLPO appears to be strategically well
placed because of its robust connections with hypothalamic regions (Chou et al.,
2002). Moreover, major descending projections from the VLPO to the TMN and more
regions of the ARAS were found, using tracing methods (Sherin et al., 1998). The
neurotransmitters present in the VLPO are mainly gamma-aminobutyric acid
(GABA). GABA is known as the most important and ubiquitous inhibitory
neurotransmitters of the central nervous system. This suggests that the VLPO may
provide inhibitory GABAergic inputs to these cell bodies in the ARAS, and therefore
may play a key role in silencing the ARAS and promoting sleep (see figure 4).
Figuur 2: A schematic drawing showing key components of the ARAS. Red branch: neurons that fire during wakefulness and slow down during NREM/REM. Yellow branch: neurons that fire during wakefulness and REM sleep (from Saper et al., 2005, pg1258)

13
The arousal and sleep promoting networks interact with each other creating the
balance between sleep and wake processes. The transition from wake to sleep occurs
very rapidly and it is therefore called a flip-flop switch, you are either awake or
asleep, but not much time is spent in the transitional state. The question that rises is:
what triggers this switch? Apparently, something makes the balance towards
activation of the one network, or the other. A neuropeptide ‘orexin’ seems to be
highly important. This neuropeptide is produced only in the posterior half of the
lateral hypothalamus (LH). The orexin neurons are mainly active during wakefulness
and can directly reinforce the arousal system (Lee et al., 2005). These orexin neurons
can have an indirect effect on the VLPO (see figure 3). During wakefulness the VLPO
is inhibited through the regions of the ARAS, which are directly reinforced by the
orexin neurons. On the other hand, during sleep, the VLPO inhibits the orexin neurons
Figuur 3: A schematic drawing showing primary projections of the VLPO to the main components of the ascending arousal system (from Saper et al., 2005, pg 1259).

14
and the regions of the ARAS. This inhibition is strengthened by the fact that the
orexin neurons inhibit the ARAS regions even more.
Figuur 4: A schematic drawing of the flip-flop switch model (from Saper, 2005). a) the balance during wakefulness; b) the balance during sleep.
Taken together, these studies suggest that normal sleep can be characterized
by global and regional deactivations. During the SOP, the VLPO and several basal
ganglia areas are key factors in the regulation of sleep. During NREM sleep, the
thalamus, basal ganglia, pons and some prefrontal cortex areas show great
deactivation, and therefore may be important.

15
Chapter 3: Hyperarousal model of insomnia
A hyperaroused state became the main concept of different models on primary
insomnia. This hyperarousal can be found in three different dimensions. For instance
somatic arousal causes you to have heightened sensory response, which can be seen
by increased automatic activity such as elevated heart rate/respiration and the blood
levels of stress hormones increase dramatically as has been found in poor sleepers
repeatedly (Monroe, 1967; Adam et al., 1986; Bonnet, 1995).
Another form of arousal is cognitive arousal. Cognitive arousal is reflected by
intrusive and negative cognitions and their associations with sleep complaints
(Wicklow & Epsie, 2000; Lichstein and Rosenthal, 1980). The last proposed form of
arousal is defined as cortical arousal. In this review I will investigate the current
literature on cortical (hyper)arousal in primary insomnia, this can also be called the
neurobiological aspects of insomnia. This research field has expended dramatically
the last decade, due to new techniques such as EEG and fMRI, which allow us to have
a closer look at the biological basis of hyperarousal.
3.1 Neurophysiology of primary insomnia (cortical arousal)
Research using quantitative EEG (QEEG) techniques provides insights in
cortical arousal in insomnia. For example, cortical electrophysiological signals in the
beta and especially gamma band have been hypothesized as a main feature of coherent
cortical processing of sensory information (Llinás & Ribary, 1993), where an EEG
power increase in this frequency range can be interpreted as a sign of cortical
hyperactivity or hyperarousal. Therefore, analysing EEG patterns in insomniacs can
provide meaningful information, in favour or against the hyperarousal hypothesis.

16
As noted above, the transition from wakefulness to sleep, also called the sleep onset
period (SOP), entails a shift in the frequency power spectrum of the EEG from high
to low frequencies in healthy individuals (Wright et al., 1995). This period is of
specific interest in the light of primary insomnia. Merica and Gaillard (1992) were
one of the first to study the SOP in insomniac patients. They confirmed the idea that
the SOP of normal sleepers can be characterized by a rapid change in beta and delta
activities. Beta activity decreases and delta activity increases, both in insomniacs as in
healthy controls. However, insomniacs had higher beta and lower delta activity
compared to controls in the SOP and the first minutes of the first NREM cycle. The
differences in delta activity between insomniacs and healthy controls were significant.
The authors of this article suggest that this increased high frequency activity may
explain the tendency of insomnia patients to overestimate their sleep latencies.
Lamarche and Ogilvie (1997) performed a similar study, looking at the SOP in
psychophysiological insomniacs, non-specified psychiatric insomniac and control
sleepers. They extended previous findings by defining the SOP into four quartiles.
The results showed that insomniac exhibit less delta power in the SOP, specifically in
the last quartile. Reduced alpha activity was found during the first quartile of the SOP
in insomniacs, and it did not show a dramatic drop, which is common during normal
sleep. Moreover, they found that increased relative beta power during wakefulness in
primary insomnia patients.
In line with previous findings, Staner and colleagues (2003) found that
patients with primary insomnia did not experience a decrease of their alpha and beta
power during the SOP, and showed lower delta activity in the first 5 minutes of sleep.
They concluded that hyperarousal mainly affects the sleep initiation of primary

17
insomnia patients whereas the homeostatic sleep regulation process seems to be
partially maintained.
In contrast to the study of Staner and colleagues, Merica and Guillard (1998)
questioned whether primary insomnia affected only the SOP, or if this dysregulation
can be seen in other sleep stage too. They were the first who did not limit their EEG
data to an interval at/around sleep onset and also examined the first four NREM/REM
cycles. Consistent with previous studies, increased beta power in insomnia patient
compared to healthy controls was found during the SOP. However, elevated beta
activity was found during the whole night in primary insomnia patients, emphasizing
the importance to investigate the whole sleep pattern instead of focussing only on the
SOP. Moreover, they found increased power in fast frequency bands and a decreased
power in the delta and theta bands in insomnia patients during REM sleep. One major
disadvantage of this study is that the authors did not remove all episodes of
wakefulness within each NREM/REM cycle before performing the power analysis.
They only excluded episodes that contained periods of wakefulness lasting 5 minutes
or more. This may have resulted in group differences for high frequencies, that can be
explained by differences in short periods of wakefulness. However, these results were
the first to show that primary insomnia also affects the REM sleep. Moreover, they
suggest that not only the sleep initiation is dysregulated in primary insomnia, but also
the maintenance of sleep.
In table 1 all the results are summarized. First, beta activity (14-35Hz) is
increased (or drops more slowly) in primary insomnia relative to good sleepers, both
around the SOP as during NREM sleep (Merica et al., 1992;1998; Nofzinger et al.,
1999; Perlis et al., 2001; Lamarche and Ogilvie, 1997). Second, insomnia patients
exhibit reduced levels of alpha power during NREM, wakefulness and sleep onset

18
period (Merica et al., 1998; Lamarche and Ogilvie, 1997), and increased levels of
alpha activity during the SOP (Lamarche and Ogilvie, 1997; Staner et al., 2001).
Third, theta power during NREM and REM sleep was decreased in insomniacs
(Merica et al., 1998). Fourth, delta power appears to be lower in insomniacs during
the SOP, NREM and REM sleep (Lamarche and Ogilvie, 1997; Merica et al., 1998;
Staner et al.,2003). And fifth, higher gamma power was observed during NREM sleep
(Krystal et al., 2002). In conclusion, insomniacs show elevated levels of high
frequency and a reduction of slow frequency EEG activity during all phases of sleep
compared to normal sleepers, which is evidence in favour of the hyperarousal
hypothesis (see table 1).
Table 1: EEG differences in PI compared to healthy sleepers (during first NREM cycle, except for the study of Merica and Gaillard (1998) who investigated the first four NREM/REM cycles). Stage EEG frequency Effect Article
Wakefulness Alpha (8-12 Hz)
Beta (14-35 Hz)
Decreased in PI
Increased in PI
Lamarche and Ogilvie
(1997)
SOP Delta (0-4 Hz) Decreased in PI Merica and Gaillard
(1992),
Lamarche and Ogilvie
(1997) Alpha (8-12 Hz) Increased in PI Lamarche and Ogilvie
(1997)
Staner et al., (2003) Beta (14-35 Hz) Dropped more slowly/
increased in PI
Merica and Gaillard
(1992 ‘ns’; 1998)
Staner et al., (2003)
La Marche and Ogilvie
(1997)

19
NREM
Delta (0-4 Hz) Decreased in PI Staner et al., (2003),
Merica and Gaillard
(2008) Theta (4-7 Hz) Decreased in PI Merica and Gaillard
(2008) Alpha (8-12 Hz) Decreased in PI
Merica and Gaillard
(2008) Beta (14-35 Hz) Increased in PI
Merica and Gaillard (1998) Nofzinger et al., (1999)
Gamma (25-100 Hz) Increased in PI
Krystal et al., 2002
REM Delta (0-4 Hz) Decreased in PI Merica and Gaillard
(2008) Theta (4-7 Hz) Decreased in PI Merica and Gaillard
(2008)
Alpha (8-12 Hz) Increased in PI Merica and Gaillard
(2008) Beta (14-35 Hz) Increased in PI Merica and Gaillard
(1998)
EEG: electroencephalography, SOP: sleep onset period, NREM: non-rapid-eye movement sleep,
REM: rapid-eye-movement sleep
There are several limitations of sleep research using QEEG measurements.
First, some studies focused on a limited portion of the sleep EEG spectrum (e.g.
Staner et al,, 2001) while others focused on a specific sleep period (e.g. Merica and
Gaillard, 1992; Lamarche and Ogilvile 1997). Second, the measurement is susceptible
to confounding artefacts from electromyography (EMG) signals (Goncharova et al.,
2003). And last, in contrast to the excellent temporal resolution of EEG, the spatial
resolution of is very limited. EEG is only able to measure cortical activity (and no
20
subcortical brain structures) and therefore can not give information about more
subcortical brain activity. As in normal sleep, new techniques as MRI allow
researchers to measure brain activity at lower levels, including subcortical brain
circuits and areas. This may give new insights in the underlying brain mechanisms
controlling sleep.
3.2 Neurobiology of primary insomnia (sub-cortical arousal)
If abnormal sleep is a result of a failure of sleep promoting areas, we would
expect to find a decreased activity of the VLPO and several basal ganglia areas. If
abnormal sleep is a result of a failure of wake promoting areas, we would expect to
find an excessive ascending activation through increased activity areas located in the
ARAS (thalamus, basal ganglia, pons and prefrontal cortex). This last expectation is
the main idea of the hyperarousal hypothesis.
To my knowledge only two studies investigated functional abnormalities of
insomniacs, directly looking at brain metabolism with the use of MRI (Nofzinger et
al., 2004; Smith et al., 2002).
Smith et al., (2002) used a single photon emission computed tomography
(SPECT) method, to investigate the brain metabolism in insomniacs. Their results
showed a significant decreased regional cerebral blood flow in the frontal medial
cortex, frontal lateral cortex, basal ganglia, thalamus, pons and temporal, occipital
and parietal cortices during the first cycle of NREM sleep in insomniacs compared to
good sleepers.
And a recent neuroimaging of Nofzinger and colleagues (2004), who used
fluordeoxyglucose positron emission tomography (PET) to assess the regional
cerebral glucose metabolism (CMRglu). Contrary to the results of Smith and

21
colleagues (2002), Nofzinger and colleagues (2004) showed that in the transition from
wakefulness to NREM sleep insomniacs showed increased global glucose metabolism
compared to healthy controls. Secondly, insomniacs exhibited less reduction of
relative CMRglu in the ARAS, hypothalamus, insular cortex, amygdala,
hippocampus, anterior cingulate cortex and the medial prefrontal cortex during
NREM sleep. Third, PI patients show an increased metabolism in the frontal cortex,
superior temporal cortex, parietal and occipital cortices, and in the thalamus,
hypothalamus, and brainstem reticular formation during wakefulness. These results
were the first to directly show a dysfunctional deactivation or an inhibition of the
arousal mechanisms at the transition from wakefulness to (NREM) sleep in humans
with primary insomnia. The differences in metabolism during wakefulness may be
responsible for the daytime impairments of insomnia, and are shown to be a related to
sleep deprivation (Thomas et al., 2000).
Differences between these two studies can be caused by several aspects.
Despite the advantages of MRI techniques, studying sleep parameters with the use of
a MRI scanner does not come without disadvantages. Two major problems of
studying sleep in the MRI scanner are: difficulties with co registration of the
polysomnography (a measurement of brain waves (EEG), eye movement, muscle
activity, of heart rhythm, used to define sleep stages) and functional imaging data.
And secondly, it is hard to capture tomography during sleep from uniform sleep
stages. Due to the magnetic field, the EEG signal can easily be disrupted, if the
subjects were able to sleep at all in the noisy MRI environment (Smith et al., 2002).
These general limitations of using the MRI scanner in sleep research may have
influenced the results of both studies in different ways.

22
Another possible explanation of the different results may due to different
measurement techniques. Nofzinger and colleagues (2004) used PET recordings,
where Smith and colleagues (2002) used SPECT recordings. Both techniques use an
injection of a different short-lived radioactive tracer isotope, which decays by
emitting a positron. On the one hand, SPECT imaging is a fast scan completed, but
lacks the spatial resolution of PET imaging. Where on the other hand PET imaging
allows a more refined analysis at the neuroanatomical level, but involves a much
longer uptake window, because of the slow tracer. This results in much longer
scanning times (Meikle et al., 2006). Since blood flow is known to decline with
increasing duration of NREM sleep, these small differences due to different
techniques makes it difficult to compare the studies and to get a uniform picture of the
alternations in brain metabolism in primary insomnia.
3.2.2 Neurotransmitters
As pointed out before, sleep is a consequence of several brain areas connecting
with each other in a network. This occurs under the influence of neurotransmitters,
hormones, receptors and connections. The neurotransmitter GABA may have a key
role in promoting sleep by inhibiting midbrain areas of the ARAS. If insomnia
patients exhibit hyperarousal, this may be caused by decreased GABA to inhibit the
brain areas located in the ARAS. In patients with primary insomnia, reduced daytime
overall average brain GABA levels, averaged from basal ganglia, thalamus, and
parietal, occipital, and temporal white matter and cortical regions, were observed
(Winkelman et al., 2008). Remarkably, GABA levels correlated with both subjective
and objective sleep measures. Longer wake time after sleep onset was associated with

23
lower levels of GABA. To our knowledge, this is the only investigation focussing on
neurotransmitters in primary insomnia.
Chapter 4: Heritability
If evidence is found for the occurrence of hyperarousal in primary insomnia, it
can be questioned if hyperarousal is a contribution to insomnia or a consequence of it.
This leads us to the question: are there predisposing factors in insomnia?
There are a couple studies who investigated this topic. Bastien and colleagues
(2000) evaluated the familial incidence of sleep disturbances among individuals with
sleep complaints. They found that 35% of patients consulting for insomnia had a
positive family history of sleep disturbances, with trends suggesting a higher
frequency among patients with primary insomnia, an early age of onset and sleep
onset insomnia. Particularly the mother was the most afflicted family member.
Similar results were found by Beaulieu-Bonneau and colleagues (2007), who reported
that 34.9% of their participants had at least one first-degree relative, with past or
current insomnia. And again, the mother was the most frequently afflicted (19.7%).
Two major disadvantages of the study of Bastien and colleagues (2000) were
that the data were obtained by self-report and the absence of a control group. This
way the results are based on subjective judgements instead of direct assessments and
individuals with past or current insomnia are more likely to report a positive family
history of insomnia than individuals without any history of insomnia (Beaulieu-
Bonneau et al., 2007). A study by Dauvilliers and colleagues (2005) did include a
control group. They compared familial insomnia in three groups, primary insomnia,

24
psychiatric insomnia and a non-insomnia control groups. They results showed reports
of familial insomnia in 72.7%, 43.3% and 24.1% respectively. Similar to previous
studies, the mother was the relative most frequent affected and there was a tendency
to younger age at onset observed in familial and primary insomnia. From these studies
it can be concluded that there is strong evidence for heritability in primary insomnia if
we look at behavioural scores. This leads us to the question: ‘What is the genetic
component of primary insomnia?’.
Ambrosius and colleagues (2008) performed a classical twin study in
monozygotic and dizygotic twin pairs on the genetic effect of sleep EEG in healthy
participants. They found that the relative contributions of the delta, theta, alpha and
sigma frequency bands were significantly correlated to the genetic background. In
other words, the monozygotic twin pairs showed significantly higher within-pair
concordance in spectral power of these frequencies, compared to dizygotic twin pairs.
These results showed that the spectral composition of non-REM sleep in humans is
significantly influenced by genetics. And because it has been found that insomnia is
characterized by specific EEG pattern, these results suggest that a hyperaroused EEG
pattern may be the main cause of primary insomnia.
Sadly, no studies have investigated a possible genetic component in brain
alternations of the neuronal sleep-wake circuitry. This would be of specific interest in
the light of the hyperarousal hypothesis.

25
Chapter 5: Treatment
Current treatment options for primary insomnia are mainly based on
behavioural aspects, including stimulus control therapy, sleep restriction therapy,
relaxation therapy, cognitive behaviour therapy, sleep hygiene education (Principles
and practice of sleep medicine, pp. 726-737). The aim of cognitive behaviour therapy
for insomnia (CBT-I), which is considered the treatment of choice for primary
insomnia, is to change maladaptive sleep habits, reduce autonomic arousal and alter
dysfunctional beliefs as for instance rumination (Morin et al., 1994; Murtagh et al.,
1995). However, there is a significant group of patients (about 20%) that does not
respond to cognitive behaviour therapy (CBT) (Morin et al., 1994, Harvey et al.,
2003) and the patients that do respond, show an average improvement but not
sufficient to categorize them as ‘good sleepers’ (Harvey et al., 2003). I suggest that in
the light of the hyperarousal view it would be of interest to think about a treatment
approach that works from bottom-up instead of normal CBT, that is based on a top-
down view. Regulating the specific neurobiological alternations in insomnia patients
may result in a more successful treatment approach.
There are two different methods to achieve a bottom-up approach in treatment.
One of them is by using pharmacological interventions. Current pharmacological
treatment interferes with the function of neurotransmitters in the ARAS by
counteracting the result of wake-promoting systems. For instance, specific targets can
be regulated by adding a histamine H1-antagonist (e.g. Doxepin or Diphenhydramine)
to counteract histamine from the TMN or a serotonin 5-HT2a-receptor antagonist (e.g.
Trazodone) to block serotonin in the DR (Szabadi, 2006). Another method can be to
inhibit the wake-promoting system itself, instead reacting on the results of an active
26
ARAS. A benzodiazepine receptor agonist (BZRA) mimics the action of the VLPO
by inhibiting the ARAS through increased activity of GABA (Gottesman, 2002)
The main disadvantage of pharmacological treatment is that some drugs are
not prescribed for long-term use, because of their side effects (Ringdahl et al., 2004;
Kripke, 2006). Moreover, there is a risk for substance dependence. Even with relative
save drugs such as Zolpidem and Zopiclone, which are both prescribed for treatment
of insomnia (Hakak et al., 2003). Furthermore, not all sedatives show greater
improvement compared to CBT in older adults, who are more vulnerable for side
effects (Sivertson et al., 2006).
A possible new treatment to focus on the hyperarousal instead of cognitive
arousal, but without clear pharmacological side effects, is EEG neurofeedback.
Neurofeedback is a new method based on training a patients’ self regulation (Othmer
et al., 1999). The patient receives feedback of his EEG recordings and is trained to
normalize the functioning of the brain by inhibiting or reinforcing specific frequency
bands. In the light of hyperarousal as a leading cause of primary insomnia, and
significant EEG evidence for this, this treatment may be successful by training the
patients to regulate their cortical arousal. This may result in a decreased arousal and
therefore positive effect on primary insomnia. Because primary insomnia is
considered a 24-h disorder (Bonnet & Arand, 1995) training of wake EEG can result
in changes of the sleep EEG (Sterman et al., 1970). Thus neurofeedback may be a
successful new treatment possibility. Cartoos and colleagues (2010) performed an
exploratory study on the effects of neurofeedback and showed a significant
improvement in total sleep time after neurofeedback training. Further research on this
treatment method is needed.

27
Concluding, neurofeedback may be in interesting new treatment technique by
reducing the cortical hyperarousal in primary insomnia. However one shortcoming of
this technique is that no study investigated the effects of neurofeedback on subcortical
hyperarousal and the regulation of metabolism in for instance the ARAS system.
Based on the current evidence I suggest a combined treatment of neurofeedback and
pharmacological treatment for primary insomnia.

28
Chapter 6: Discussion
In this review, I summarized the current literature on the hyperarousal
hypothesis of sleep in primary insomnia, with the use of EEG or MRI methods. I
questioned whether there is evidence for a hyperarousal model on neurobiological
basis. I discussed the literature from cortical to subcortical levels of arousal. First
EEG studies were described, and after that the scarce literature on MRI studies was
described.
In EEG studies, elevated levels of high frequency and a reduction of slow
frequency EEG activity has been repeatedly found during all phases of sleep, in
insomnia patients compared to normal sleepers. Technical limitations result in an
inability to adequately localize regional activity throughout the brain. This resulted in
the need for another, more advanced, measurement technique. However, despite this
limitation, these results clearly support the hyperarousal hypothesis.
From MRI studies no clear conclusions can be drawn because currently
available data are limited and inconsistent. The results of the two current studies
(Smith et al, 2002; Nofzinger et al, 2004) are contradictive. A possible explanation for
this clear difference may lie within the changing of brain metabolism over time. To
date, no fMRI study recorded more than the first part of the first NREM cycle. Perlis
and colleagues (2001) showed that the heightened beta activity in insomniacs during
the SOP rapidly attenuates across the sleep-wake transition. This decline was found to
be significantly greater in patients with primary insomnia and leads to a brief period
of hypoarousal. With this difference in arousal over time, it is possible that the 2-min
time window of the study of Smith accidently recorded this temporary hypoarousal.
This emphasises the importance of future research on a whole night cycle with fMRI.

29
Such research can give more insight in the question whether primary insomnia
patients are generally hyperaroused during NREM sleep, as found by Nofzinger and
colleagues (2004) or if they show periods or hyperarousal alternating with periods of
hypoarousal.
A dysfunction of the sleep-wake circuitry may be a result of difference in
neurotransmitters. To date, only one study investigated differences in the amount of
neurotransmitters in primary insomnia. Winkelman and colleagues (2008) found
global decreased GABA in primary insomnia patients, suggesting a failure to inhibit
wake-promoting areas.
In the light of treatment possibilities, we propose a new treatment method. The
current behavioural treatments (Principles and practice of sleep medicine, pp. 726-
737) have proven to be successful in reducing arousal by changing mostly thoughts
and rumination. However, because primary insomnia can be caused by (sub)cortical
instead of cognitive arousal, other treatment methods may be more successful.
Pharmacological treatment has proven to be successful, and a new proposed method is
neurofeedback, which focuses on reducing cortical arousal. I suggest a combination
of these two treatment modalities. When combined, pharmacological treatment is used
to change the arousal on neurotransmitter level, where simultaneously neurofeedback
can result in reducement of cortical arousal. Together these two therapies may be the
most successful treatment method of primary insomnia.
The available data generally support the hyperarousal theory of insomnia with
increased cortical activity during NREM sleep. However, the key brain areas
responsible for the hyperarousal remain unclear. Further research on the
identification of regional brain activation should allow development of increasingly
specific medical treatments, to control abnormal activation.

30
Moreover, differences on neurotransmitter level and the temporal
characteristics of hyperarousal should be investigated. As said before, the study of
Perlis and colleagues (2001) suggest that hyperarousal may be a dynamic, instead of
static process. Therefore, a whole night fMRI study looking at the hyperarousal over
time would be very useful.
In this review I conclude that hyperarousal is key factor in the pathology of
primary insomnia, based on neurophysiological evidence. Moreover, the literature
suggests a hyperarousal of the ARAS as underlying factor of primary insomnia. But
due to limited research this hypothesis can not be confirmed (yet).

31
Appendix 1: Definitions of subtypes of insomnia, according to the ICSD.
Psychophysiological insomnia (307.42-0)
Learned insomnia, conditioned insomnia, functionally autonomous insomnia,
psychophysiological arousal, chronic somatised tension, internal arousal without
psychopathology.
Psychophysiological insomnia is a disorder of somatised tension and learned sleep-
preventing associations that results in a complaint of insomnia and associated
decreased functioning during wakefulness. Psychophysiological insomnia is an
objectively verifiable insomnia that develops as a consequence of two mutually
reinforcing factors: (a) somatised tension and (b) learned sleep-preventing
associations. Individuals who have psychophysiological insomnia typically react to
stress with somatised tension an agitation. The meaning of stressful events (other than
insomnia) is typically denied an represses, but manifests itself as increased
physiological arousal (e.g., increased muscle tension, increased vasoconstriction, etc.)
Idiopathic insomnia (780.52-7)
Childhood insomnia, lifelong insomnia, insomnia associated with problems within the
sleep-wake system, excessive arousal, inadequately developed sleep system.
Idiopathic insomnia is a lifelong inability to obtain adequate sleep that is presumably
due to an abnormality of the neurological control of the sleep-wake system.

32
References
Adam, K., Tomeny, M., Oswald, I. (1986). Physiological and psychological
differences between good and poor sleepers. Journal of psychiatric research, 20(4),
301-316.
Ambrosius, U., Lietzenmaier, S., Wehrle, R., Wichniak, A., Kalus, S., Winkelmann,
J., Bettecken, T., Holsboer, F., Yassouridis, A., Friess, E. (2008). Heritability of
sleep electroencephalogram. Biological Psychiatry, 64, 344-348.
American Psychiatric Association (APA). Diagnostic and statistical manual of mental
disorder. 4th ed. Washington, DC: APA; 1994.
American Sleep Disorders Association, The international classification of sleep
disorders: diagnostic and coding manual-revised. Rochester, M.N: Americal Sleep
Disorders Association 1997.
Andersson, J.L., Onoe, H., Hetta, J., Lidstrom, K., Valind, S., Lilja, A., et al. (1998).
Brain networks affected by synchronized sleep visualized by positron emission
tomography. Journal of Cerebral Blood Flow & Metabolism, 18 (7), 701-715.
Beaulieu-Bonneau, S., LeBlanc, M., Mérette, C., Dauvilliers, Y., Morin, C.M. (2007).
Family history of insomnia in a population-based sample. Sleep, 30(12), 1739-
1745.
Bonnet, M.H., Arand, D.L. (1995). 24-hour metabolic rate in insomniacs and matched
normal sleepers. Sleep, 8, 581–8.
Bonnet, M.H., Arand, D.L. (1997). Hyperarousal and insomnia. Sleep medicine
reviews, 1(2), 97-108.
Bonnet, M.H., Arand, D.L. (1997). Psysiological activation in patients with sleep state
misperception. Psychosomatic medicine, 59(5), 533-540.
Borbély, A.A., (1982). A two process model of sleep regulation. Human
Neurobiology, 1: 195-204.
Braun, A.R., et al. (1997). Regional cerebral blood flow throughout the sleep-wake
cycle. An H2(15)O PET study. Brain, 120(Pt7), 1173-1197.

33
Buchsbaum, M.S., Gillin, J.C., Wu, J., Hazlett, E., Sicotte, N., Dupont, R.M. et al.
1986. Regional cerebral glucose metabolic rate in human sleep assessed by
positron emission tomography. Life Sciences, 45(15), 1349-1356.
Cartoos, A., De Valck, E., Arns, M., Breteler, M.H.M., Cluydts, R. (2010). An
exploratory study on the effects of tele-neurofeedback and tele-biofeedback on
objective and subjective sleep in patients with primary insomnia. Applied
Psychophysiological Biofeedback, 35, 125-134.
Chou, T.C., Bjorkum, A.A., Gaus, S.E., Lu, J., Scammell, T.E., Saper, C.B. (2002).
Afferents to the vertrolateral preoptic nucleus. The Journal of Neuroscience, 22(3),
977-990.
Dauvilliers, Y., Morin, C., Cervena, K., Carlander, B., Touchon, J., Besset, A.,
Billiard, M. (2005). Family studies in insomnia. Journal of Psychosomatic
Research, 58, 271-278.
Dement, W.C., Kleitman, N. (1957). Cyclic variations in EEG during sleep and their
relation to eye movements, body motility and dreaming. Clinical Neurophysiology,
9:673–390.
De Gennaro, L., Ferrara, M., Bertini, M., (2001). The boundary between wakefulness
and sleep : quantitative electroencephalographic changes during the sleep onset
period. Neuroscience, 107, 1-11.
Chairman, T.M.J. (1990). ICSD – International classification of sleep disorders:
Diagnostic and coding manual. Diagnostic Classification Steering Committee,
Rochester, Minnesota: American Sleep Disorders Association.
Edinger, J.D., Krystal, A.D. (2003). Subtyping primary insomnia: is sleep state
misperception a distinct clinical entity? Sleep Medicinereviews, 7(3), 203-214.
Goncharova, I.I., McFarland, D.J., Vaughan, T.M., Wolpaw ,J.R.. EMG
contamination of EEG: spectral and topographical characteristics (2003). Clinical
Neurophysiology, 114(9), 1580-1593.
Gottesman, C. (2002). GABA mechanisms in sleep. Neuroscience, 111, 231-239.
Hakak, G., Müller, G.W., Wittchen, H.U., Pittrow, D., Kirch, W. (2003). Abuse and
dependence potential for the non-benzodiazepine hypnotics zolpidem and
zoplicone: a review of case reports and epidemiological data. Addiction, 98, 1371-
1378.
Harvey, A.G., Tang, N.K.Y. (2003). Cognitive behavior therapy for primary
insomnia: can we rest yet? Sleep Medicine Review, 7, 237-62.

34
Kajimura, N., Uchiyama, M., Takayama, Y., Uchida, S., Uema, T., Kato, M., et al.
(1999). Activity of midbrain reticular formation and neocortex during the
progression of human non-rapid eye movement sleep. Journal of Neuroscience,
19(22), 10065-10073.
Kjaer, T.W., Law, I., Wiltschiotz, G., Paulson, O.B., Madsen, P.L. (2002). Regional
cerebral blood flow during light sleep-a H(2)(15)O-PET study. Journal of Sleep
Research, 11, 201-207.
Kripke, D.F,. Risks of chronic hypnotic use. In: Lader M, Cardinali DP, Pandi-
Perumal SR, editors. Sleep and sleep disorders – a neuropsychopharmacological
approach. New York: Springer; 2006. p. 141–5.
Krystal, A.D., Edinger, J.D., Wohlgemuth, W.K., Marsh, G.R., (2002). NREM sleep
EEG frequency spectral correlates of sleep complaints in primary insomnia
subtypes. Sleep, 25(6), 630-40.
Lamarche, C.H., Ogilvie, R.D. (1997). Electrophysiological changes during the sleep
onset period of psychological insomniacs, psychiatric insomniacs, and normal
sleepers. Sleep, 20, 724-33.
Lee., M.G., Hassani, O.K., Jones, B.E. (2005). Discharge of identified
orexin/hypocretin neurons across the wake-sleep cycle. Journal of Neuroscience,
25, 6716-6720.
Lichstein, K.L., Rosenthal, T.L. (1980). Insomniacs’ perceptions of cognitive versus
somatic determinants of sleep disturbance. Journal of Abnormal Psychology, 89(1),
105-107.
Maquet P, Dive D, Salmon E, Sadzot B, Franco G, Poirrier R, et al. (1992). Cerebral
glucose utilization during stage 2 sleep in man. Brain Research, 571(1), 149-153.
Maquet, P., Peters, J., Aerts, J., Delfiore, G., Degueledre, C., Luxen, A., et al. (1996).
Functional neuroanatomy of human reapid-eye-movement sleep and dreaming.
Nature 383(6596), 163-166.
Meikle, S.R., Beekman, F.J., Rose, S.E. (2006). Complementary molecular imaging
technologies: High resolution SPECT, PET and MRI. Drugs Discovery Today:
Techonolgies, 3(2), 178-194.
Merica, H., Gaillard, J. (1992). The EEG of the sleep onset period in insomnia: a
discriminant analysis. Physiology and Behavior, 52, 199-204.
Merica, H., Blois, R., Gaillard, J. (1998). Spectral characteristics of sleep EEG in
chronic insomnia. European Journal of Neuroscience, 10, 826-34.
35
Monroe, L.J. (1967). Psychological and physiological differences between good and
poor sleepers. Journal Abnormal Psychology, 72, 255-64.
Morin, C.M., Culbert, J.P., Schwartz, S.M. (1994). Nonpharmacological interventions
for insomnia: A meta-analysis of treatment efficacy. American Journal of
Psychiatry, 151, 1172-1180.
Moruzzi, G., Magoun, H.W. (1949). Brain stem reticular formation and activation of
the EEG. Electroenceohalography and Neurophysiology, 1(4), 455-73.
Murtagh, D.R.R., Greenwood, K.M. (1995). Identifying effective psychological
treatments for insomnia: A meta-analysis. Journal of Consulting and Clinical
Psychology, 63, 79-89.
Nofzinger, E.A., Buysee, D.J., Miewald, J.M., Meltzer, C.C., Price, J.C., Sembrat,
R.C., et al. (2002). Human regional cerebral glucose metabolism during non-rapid
eye movement sleep in relation to waking. Brain, 125(part 5), 1105-1115.
Nofzinger, E.A., Buysse, D.J., Germain, A., Price, J.C., Miewald, J.M., Kupfer, D.J.
(2004). Functional neurimaging evidence for hyperarousal in insomnia. American
Journal of Psychiatry, 161: 2126-2129.
Nofzinger, E.A., Mintun, M.A., Wiseman, M., Kupfer, D.J., Moore, R.Y. (1997)
Forebrain activation in REM sleep: an FDG PET study. Brain Research, 770, 192-
201.
Nofzinger, E.A., Nowell, P.D., Buysee, D.J., Vasco, R.C., Thase, M.E., Frank, E.,
Kupfer, D.J., Reynolds, C.F. (1999). Towards a neurobiology of sleep disturbance
in primary insomnia and depression: a comparison of subjective, visually scored,
period amplitude, and power spectral densisity sleep measures. Sleep, 22 (supp. 1),
S99.
Othmer, S., Othmer, S.F., Kaiser, D.A. (1999). EEG biofeedback: an emerging model
for its global efficiency. In: Evans, J.R., Abarbanel, A., editors. Introduction to
quantitive EEG and neurofeedback. San diego: Academic press, 3-27.
Perlis, M.L., Merica, H., Smith, M.T., Giles, D.E., (2001). Beta EEG activity and
insomnia. Sleep Medicine Reviews, 5 (5), 365-376.
Perlis, M.L., Smith, M.T., Andrews, P.J., Orff, H., Giles, D.E. (2001). Beta/gamma
EEG activity in patients with primary and secondary insomnia and good sleeper
controls. Sleep, 24, 10-7.

36
Riemann, D., Spiegelhalder, K., Feige, B., Voderholzer, U., Berger, M., Perlis, M.,
Nissen, C. (2010). The hyperarousal model of insomnia: a review of the concept
and its evidence. Sleep Medicine Reviews, 14, 19-31.
Ringdahl, E.N., Pereira, S.L., Delzell, E. (2004). Treatment of primary insomnia.
JABFM, 17(3), 212-219.
Salin-Pascual, R.J., Roehrs, T.A., Merlotti, L.A., Zorick, F., Roth, T. (1992). Long-
term study of the sleep of insomnia patients with sleep state misperception and
other insomnia patients. American Journal of Psychiatry, 149, 904-908.
Saper., C.B., Scammell, T.E., Lu, J. (2005). Hypothalamic regulation of sleep and
circadian rhythms. Nature, 437, 1257-1263.
Sherin, J.E., Elmguist, J.K., Torrealba, F., Saper, C.B., (1998). Innervation of
histaminergic tuberomammillary neurons by GABAergic and galaninergic neurons
in the verntrolateral preoptic nucleus of the rat. Journal of Neuroscience, 18(12),
4705-21.
Staner, L., Cornette, F., Maurice, D., Viardot, G., Le Bon, O., Haba, J., et al (2003).
Sleep microstructure around sleep onset differentiates major depressive insomnia
from primary insomni. Journal of Sleep Research, 12, 319-30.
Sterman, M.B., Howe, R.C., MacDonald, L.R. (1970). Facilitation of spindle-burst
sleep by conditioning of electroencephalographic activity while awake. Science,
167, 1146-8.
Szabadi, E. (2006). Drugs for sleep disorders: mechanism and therapeutic prospects.
Brain Journal of Clinical Pharmacology, 61, 761-6.
Thomas M, Sing H, Belenky G, Holcomb H, Mayberg H, Dannals R, Wagner H,
Thorne, D., Popp, K., Rowland, L., Welsh, A., Balwinski, S., Redmond, D. (2000).
Neural basis of alertness and cognitive performance impairments during sleepiness.
1. Effects of 24 h of sleep deprivation on waking human regional brain activity.
Journal of Sleep Research, 9(4), 335-52.
Von Economo, C., (1930). Sleep as a problem of localization. Journal of Nervous and
Mental Disease, 71, 249-259.
Wicklow, A., Epsie, C.A., (2000). Intrusive thoughts and their relationship to
actigraphic measurement of sleep: towards a cognitive model of insomnia.
Behavioural Research and Therapy, 38, 679-93.