the ideal occlusion. ideal morphologic occlusion anterior teeth ap 2-3 mm hor oj vertical 2-4 mm ver...
TRANSCRIPT

The Ideal Occlusion

Ideal Morphologic Occlusion
Anterior Teeth
AP 2-3 mm Hor OJ
Vertical 2-4 mm Ver OB, 50%
Transverse Midlines aligned
Posterior Teeth
Angle I
Contact
Normal buccal overjet

Ideal Functional Occlusion
A. Intercuspal Position: CR jaw position 1. Simultaneous posterior contact2. Axial loading of posterior teeth3. Lighter contact of anterior teeth
B. Anterior Excursive Guidance: 1. Canine Guidance/ or Group Function2. Nonworking: NO contact3. Protrusion: NO posterior contact

My first patient in the clinic!

Biologic Variation of Occlusion

I. Morphologic Variation Brunelle JA et al.: Prevalence and distribution of selected occlusal
characteristics in the US Population, 1988-1991, J Dent Res 1996;75:706-713.
• Third National Health and Nutrition Examination Survey (NHANES III)
• Age: 8-11 & 18-50 y/o• n= 11,000• Hx of ortho tx: 20% • Crowding: Children 48-58% &
Adults 57-67%

A. Sagittal Plane(Children and Youths)
• Angle I Normal: 30%
• Angle I Malocclusion: 55%
• Angle II Malocclusion: 15% • Angle III Malocclusion: 1%

B. Horizontal Plane (Transverse)
• Posterior Crossbite: 9.1%

High Mandibular Plane Angle
• Tall lower face• Smile: maxillary teeth
and gingival visible • Lips postured to seal• Anterior open bite
tendency

Low Mandibular Plane Angle
• Short lower face• Smile: Minimal
maxillary tooth visibility
• Lower lip everted• Deep bite tendency

• Open Bite (≥ 0 mm): < 3%
• Vertical Deep Bite (>5 mm): 16 %
C. Vertical Plane

D. Racial Differences:
• Asian: increased Angle III prevalence
• Afro-American: 10% anterior open bite
• Northern European: increased prevalence of vertical deep bite, increased prevalence Angle II

II. Functional Occlusal Variation

A. CR/IP (CO) Slide
• Slide Prevalence: >90%
• Horizontal Component: Usually 0.5-1.0 mm
• Lateral Component: 25%
(Rieder CE: J Prosthet Dent 39:324-329, 1978; n=323)
1. Working Side Contacts:
Great Variation: Combination of guidance schemes typical. Average # of contacting teeth 2 with one being the canine. (Woda AV et al., J Prosthet Dent 1979;42:335-342.

1. Working Side Contacts:
Great Variation: One sample identified 2% with bilateral canine guidance and 18% with unilateral canine guidance. (Ingerval B, Archs Oral Biol 1977;17:191-200)

Skeletal Variation of Occlusion

Skeletal Effect:
Canine Guidance: tend to have mandibular plane angle < 24o
Group Function: tend to have a mandibular plane angle > 24o
(DiPietro GJ: J Prosthet Dent 38:452-458, 1977; n=112)

2. Nonworking Side Contacts:
• Nonworking contacts identified in > 60% of a sample (Ingervall B, Archs Oral Biol 17:191-200, 1977)

2. Nonworking Side Contacts:
• Nonworking interferences (contact only on the nonworking side) identified in 8% of a study sample (Ingervall B, Archs Oral Biol 17:191-200, 1977)

C. Intercuspal Position Contacts: Ideal
Size: small circular areas ≤ 1 mm diameter
Location: cusp tips to flat fossae & marginal ridges; or balanced inclines.
Number: n=26 or 66
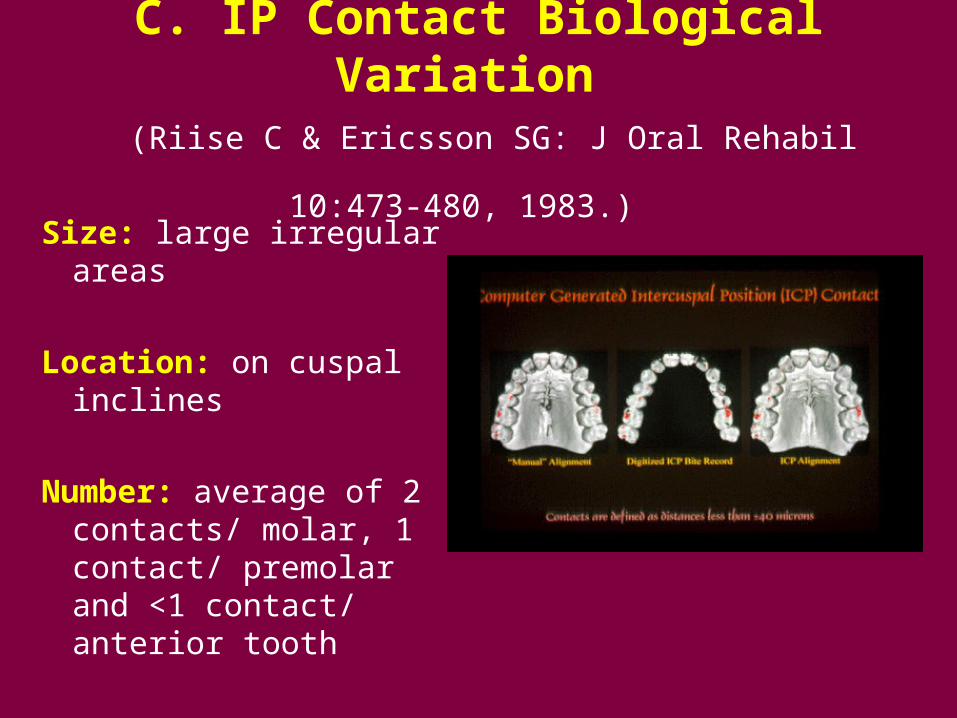
C. IP Contact Biological Variation
(Riise C & Ericsson SG: J Oral Rehabil 10:473-480, 1983.)
Size: large irregular areas
Location: on cuspal inclines
Number: average of 2 contacts/ molar, 1 contact/ premolar and <1 contact/ anterior tooth

Homo sapiens exhibit greater occlusal variation than any other primate

III. Biomechanical System
• Great population variability
• Masticatory system very adaptable to this variation but exhibits greater adaptive capacity with slow developmental change as compared to rapid change, I.e. restorative dentistry.

III. Biomechanical System
Restorative Treatment: We as dentists can not control the biological adaptability but we can control mechanical characteristics. Therefore restorations are fabricated to an ideal occlusion within the scope or extent of the treatment.

Objectives CR Adjustment: Intercuspal Occlusion
• Eliminate CR-IP slide, “create new IP in CR”
• VDO slightly closed from original IP VDO
• Simultaneous posterior contact
• Axial loading of posterior teeth
• Anterior lighter contact

Occlusal Adjustment: A Method
Goal: All centric cusps contacting and every posterior tooth pair holding shimstock.

Thank you!