the impact of brief clinical interventions on
TRANSCRIPT
University of ConnecticutOpenCommons@UConn
Doctoral Dissertations University of Connecticut Graduate School
8-20-2013
The Impact of Brief Clinical Interventions onCardiovascular Reactions to Acute StressKatherine O'LearyUniversity of Connecticut, [email protected]
Follow this and additional works at: https://opencommons.uconn.edu/dissertations
Recommended CitationO'Leary, Katherine, "The Impact of Brief Clinical Interventions on Cardiovascular Reactions to Acute Stress" (2013). DoctoralDissertations. 170.https://opencommons.uconn.edu/dissertations/170

Running head: BRIEF CLINICAL INTERVENTIONS
The Impact of Brief Clinical Interventions on Cardiovascular Reactions to Acute Stress
Katherine Elizabeth O’Leary
University of Connecticut, 2013
Stress is a major public health concern due to its’ harmful effects on physical and
mental health. An important goal for clinical health practitioners is to help patients
reduce the psychological and physiological burden of stress. The present study sought to
examine the impact brief clinical interventions have on cardiovascular reactions to acute
stress. Additionally, we explored how depressive and anxiety symptomatology influence
cardiovascular reactivity and recovery, and their moderating effects on treatment
response to interventions. To address these aims, subjects were randomized into one of
three conditions (Acceptance and Commitment Therapy, Autogenic Training, Attention-
only Control group) prior to undergoing an acute psychosocial stress paradigm, the Trier
Social Stress Test (TSST). Psychosocial measures were given at baseline, and heart rate
and blood pressure measurements were obtained at various time points throughout the
protocol. Our results indicated a time by group interaction for heart rate (HR) and
diastolic blood pressure (DBP), demonstrating that brief interventions differentially
affected heart rate and diastolic blood pressure over time. Within the Autogenic Training
group results showed that subjects with higher levels of depressive symptomatology had
lower systolic blood pressure reactivity compared to those with lower levels of depressive
symptoms. Additionally, within the Autogenic Training group, greater recovery in both

BRIEF CLINICAL INTERVENTIONS ii
systolic and diastolic blood pressure was found in subjects with higher levels of social
anxiety. Our results offer important implications for clinical assessment and intervention,
particularly within the field of behavioral medicine.

BRIEF CLINICAL INTERVENTIONS iii
The Impact of Brief Clinical Interventions on Cardiovascular Reactions to Acute Stress
Katherine Elizabeth O’Leary
B.S., Georgetown University, 2005
M.A., Teachers College, Columbia University, 2008
M.A., University of Connecticut, 2010
A Dissertation
Submitted in Partial Fulfillment of the
Requirements for the Degree of
Doctor of Philosophy
at the
University of Connecticut
2013

BRIEF CLINICAL INTERVENTIONS iv
APPROVAL PAGE
Doctor of Philosophy Dissertation
The Impact of Brief Clinical Interventions on Cardiovascular Reactions to Acute Stress
Presented by
Katherine Elizabeth O’Leary, M.A.
Major Advisor __________________________________________
Dean G. Cruess
Associate Advisor ________________________________________
Amy A. Gorin
Associate Advisor ________________________________________
John D. Salamone
Examiner 1 ________________________________________
Marianne L. Barton
Examiner 2 ________________________________________
Juliane R. Fenster
University of Connecticut
2013

BRIEF CLINICAL INTERVENTIONS v
TABLE OF CONTENTS
Abstract……..……………………………………………………………………………...i
Introduction……………………………………………………………………………..…1
Stress……………………………………………..………………………………..1
Allostasis and Allostatic Load…………………………………………….………2
Stress, depression, anxiety, and cardiovascular disease………………......4
Acute Stress Testing………………………………………………………………6
Trier Social Stress Test…………………………………………………....8
Psychological Interventions……………………………………………………...11
Acceptance and Commitment Therapy…………………………………..12
Autogenic Training………………………………………………………15
Present Study…………………………………………………………………….18
Method.…………………………………………………………………………………..19
Participants……………………………………………………………………….19
Procedure………………………………………………………………………...20
Physiological Measures.........................................................................................21
Psychological Measures………………………………………………………….21
Anxiety Sensitivity Index………………………………………………..22
Beck Depression Inventory-II……………………………………………22
Demographic and Medical History Questionnaire………………………23
Liebowitz Social Anxiety Scale………………………………………….23
Spielberger State Trait Anxiety Inventory- Trait………………………...24
Experimental and Control Conditions…………………………………………...24

BRIEF CLINICAL INTERVENTIONS vi
Acceptance and Commitment Therapy condition………………………..24
Autogenic Training condition……………………………………………25
Attention-only Activity condition………………………………………..25
Challenge Task…………………………………………………………………...25
Trier Social Stress Test protocol…………………………………………25
Data Analytic Plan……..…………………………………………………….......26
Results……………………………………………………………………………………28
Participant Characteristics………………………………….……………………28
Descriptive Statistics for Study Measures………………………...……………..29
Baseline physiological measures………………………………………...29
Psychological measures………………………………………………….30
Hypothesis 1: Impact of Brief Clinical Interventions……………………………30
Hypothesis 1a: Depressive and/or Anxiety Symptoms as Treatment
Moderators……………………………………………………………….31
Hypothesis 1b: Association of Depressive and Anxiety Symptoms with
Cardiovascular Reactivity and Recovery………………………………...36
Discussion…………………………………………………………………….………….36
Purpose of the Present Study…………………………………………………….36
Hypothesis 1……………………………………………………………………...38
Hypothesis 1a…………………………………………………………………….40
Hypothesis 1b…………………………………………………………………….43
Limitations……………………………………………………………………….45
Future Directions………………………………………………………………...45
BRIEF CLINICAL INTERVENTIONS vii
References…………………………………………………………………….………….47
Appendix ...………………………………………………………………………………62
Tables……………………………………………………..……………………………...63
Figures……………………………………………………………………………………69

BRIEF CLINICAL INTERVENTIONS 1
Stress
Stress is defined as a real or implied threat to one’s psychological or physical
integrity. It evokes behavioral and physiological responses to psychosocial,
environmental, and physical challenges, and thus can be viewed and measured from a
variety of perspectives (Clark, Bond, & Hecker, 2007; Holmes & Rahe, 1967; Kiecolt-
Glaser, McGuire, Robles, & Glaser, 2002; Lazarus & Folkman, 1984; Logan &
Barksdale, 2008). Stress is a major public health concern. Over the past several decades,
there has been a growing awareness of stress’s detrimental health effects, thereby
necessitating a need for research into the pathways linking stress and health (Kudielka,
Buske-Kirschbaum, Hellhammer, & Kirschbaum, 2004a).
The most common form of stress is acute stress. In moderation acute stress is not
harmful, however, if experienced frequently it can cause psychological and physical
distress. Stress has long been linked to maladaptive functioning and various
psychopathologies, having been found to play a large causal and maintaining role in
psychological disorders (Kessler, 1997; Nugent, Tyrka, Carpenter, & Price, 2011). For
example, individuals prone to experience acute stress are more likely to be over-aroused,
irritable, and anxious. Additionally, acute stress has been found to trigger panic attacks
and psychotic episodes in those predisposed to thought disorders (Chrousos, 2009).
Several epidemiological studies have also emerged evidencing stress as a major
psychosocial risk factor for various medical illnesses, such as cardiovascular disease
(McEwen, 2000; Yusef et al., 2004). Individuals who experience frequent acute stress
are more prone to experience headaches, allergic reactions (e.g., asthma, eczema),
hypertension, pain, and gastrointestinal symptoms (Black & Garbutt, 2002; Chrousos,

BRIEF CLINICAL INTERVENTIONS 2
2009). Currently, however, the exact mechanisms whereby stress exert its’ effects on
human physiological and behavioral systems are not well understood (Epel et al., 2006).
Allostasis and Allostatic Load
The concepts of allostasis and allostatic load are useful frameworks for
investigating the detrimental health effects of stress. Sterling and Eyer (1988) introduced
allostasis as a concept that represents the active, adaptive process of regulatory
physiological systems to physical, psychosocial, and environmental challenges.
Stemming from allostasis theory, allostatic load, according to McEwen and Stellar
(1993), is the wear and tear on the body caused by repeated activation of the stress
response. The concept of allostatic load is used to explain how frequent acute and
chronic stress causes repeated activation of the stress response, resulting in damage and
pathology (Clark et al., 2007; McEwen, 1998; Logan & Barksdale, 2008).
As McEwen (2000) explains there are four main conditions that lead to allostatic
load: repeated frequency of the stress response, failure to habituate to repeated stressors,
failure to turn off the stress response in a timely manner, and inadequate response leading
to hyperactivity of other mediators. Allostatic load is measured through a composite
index of indicators of cumulative strain. It is measured in physiological systems as
chemical imbalances in the autonomic nervous system, central nervous system, and
neuroendocrine immune system, and is thought to lead to disease through a number of
routes. For example, chemical messengers, such as cortisol and epinephrine are released
as part of the stress response. These chemicals can be affected by a variety of lifestyle
factors (e.g., sleep, diet) and are generally beneficial. However, when the body is
overexposed to them, cumulative changes occur. Repeated or dysregulated (i.e., over or
BRIEF CLINICAL INTERVENTIONS 3
under-active) exposure to chemical mediators leads to tissue and organ specific effects,
such as elevated blood pressure and increased heart rate. These specific effects lead to
subsequent outcomes, which are the actual disorders that arise from allostatic load
(McEwen, 2003). Examples of chronic illnesses thought to be associated with allostatic
load are atherosclerosis, obesity, impaired physical capacity, anxiety, depression, and
cognitive decline (Clark et al., 2007; Logan & Barksdale, 2008; Schulkin, 2004; Seeman,
Singer, Rowe, Horwitz, & McEwen, 1997; McEwen, 2004).
Responses to acute stress may be mediated through a variety of behavioral
pathways, including lifestyle factors such as smoking, substance use, obesity, and
socioeconomic status (McEwen, 2000). As we know, the brain perceives stress (whether
real or imagined) and produces behavioral responses to cope with it. These responses are
determined by interpretations by the brain, which are greatly affected by psychosocial
and individual differences, such as anxiety, depression, and social support (Logan &
Barksdale, 2008; McEwen, 2002). For example, one person may perceive a stressful
event as threatening, while another may not. Additionally, one may respond to an event
to avoid a threat, where another may respond in such a way as to increase danger
(McEwen, 2000). In sum, how a person interprets and copes with an event determines
behaviors and habits that are highly influenced by psychosocial and individual
differences. These behaviors make life more or less dangerous in the short-run and
increase allostatic load over time.
In addition to behavioral pathways, direct physiological pathways also contribute
to associations between psychosocial factors and the stress response. Chronic, acute
physical symptoms common in anxiety disorders and depressive illnesses, suggest that

BRIEF CLINICAL INTERVENTIONS 4
physiological stress-related processes, particularly those involving the autonomic nervous
system, greatly influence these conditions (American Psychiatric Association, 2000;
Chrousos, 2009; Chrousos & Gold, 1992; Sullivan, Coplan, Kent, & Gorman, 1999).
Currently, there is a discrepancy among the literature in how psychosocial factors affect
the stress response. For example, some studies have found positive psychological states
and traits, anxiety, neuroticism, and negative affect to be associated with reduced
hypothalamic-pituitary-adrenal (HPA) axis and cardiovascular reactivity to stress and
poor recovery, while other studies have found hyperactive responses due to these factors
(Logan & Barksdale, 2008; McEwen, 1998; McEwen, 2007; Tsigos & Chrousos, 2002).
This inconsistency indicates that psychosocial factors may differentially influence
individual stress responses (Chida & Hamer, 2008).
Stress, depression, anxiety, and cardiovascular disease. Within the allostatic
load literature, the best-studied system in the human body is the cardiovascular system
(McEwen, 1998). Researchers have repeatedly linked stress to cardiovascular disease,
one of the most frequent causes of death in the United States (Armario et al. 2003,
Rosamond et al., 2007). In addition, other psychosocial factors, including depression and
anxiety, have been shown to increase one’s risk for cardiovascular disease. There have
been several large reviews about the links between depression, anxiety, and heart disease.
For example, Kubzansky, Kawachi, Weiss, and Sparrow (1998) found that chronic
anxiety was a major risk factor for coronary heart disease and Glassman and Shapiro
(1997) demonstrated that depression was associated with increased mortality from
coronary heart disease. However, the mechanisms by which these relationships exist are
not as well known (Logan & Barksdale, 2008).

BRIEF CLINICAL INTERVENTIONS 5
Anxiety and depression are believed to affect the heart through three main
pathways: increasing ill-health behaviors, promoting atherogenesis via hypertension
arising from chronic sympathetic nervous system activation and/or dysregulation, and
triggering fatal coronary events. In regards to acute stress, researchers have hypothesized
that repeated episodes of acute psychological stress can result in elevated blood pressure,
heart rate, and inflammatory processes (i.e., markers of allostatic load), increasing
atherosclerotic plaques and stiffness of large arteries causing greater risk for
cardiovascular disease (McEwen, 2002). In fact, epidemiologic studies have found an
association between heightened cardiovascular reactivity in response to stress, extensive
progression of atherosclerosis, and incidence of ischemic heart disease and mortality
(Black & Garbutt, 2002). In sum, it is thought that anxiety and depression make
individuals more susceptible to stress, resulting in repeated exposure to the stress
response and an increase in allostatic load.
Currently, there is uncertainty in the literature over whether increased
cardiovascular reactivity, poor cardiovascular recovery, or both lead to disease states.
Additionally, research has shown mixed results on the effects depressive and anxiety
symptomatology have on reactivity and recovery. For example, studies investigating
cardiovascular responses to acute psychosocial stressors have suggested that depression
and anxiety are related to enhanced cardiovascular reactivity, as evidenced by increased
blood pressure and heart rate (de Rooij, Schene, Phillips, Roseboom, 2010; Kibler & Ma,
2004; Mausbach et al., 2005). Others, however, have found negative associations
implicating a hyporeactivity to acute psychosocial stress (Carroll, Phillips, Hunt, & Der,
2007; Jezova, Makatsori, Duncko, Moncek, & Jakubek, 2004; Salomon, Clift,

BRIEF CLINICAL INTERVENTIONS 6
Karisdottir, & Rottenberg, 2009). For example, Heopniemi et al. (2007) found that
delayed heart rate recovery and lower cardiac autonomic reactivity were associated with
higher carotid atherosclerosis. Mixed results in the literature may be in part due to an
integrated stress response pattern, thereby supporting the concept of allostatic load that
psychosocial factors could lead to different acute stress responses (Chida & Hamer,
2008).
In sum, current explanations of stress have failed to adequately clarify its
association with health and chronic illness. The concept of allostatic load has
applicability to subclinical and clinical psychological symptoms and suggests ways in
which allostasis theory can be applied to the development of clinical interventions to
increase resilience and the likelihood of better health outcomes (Logan & Barksdale,
2008). Further, responses to acute psychological challenge in the laboratory may not be
considered of great clinical importance in and of themselves. However, they adequately
index the way individuals respond to ordinary psychological demands, thus offering a
way to investigate how disturbed stress responses have pathophysiological significance in
everyday life (Chida & Hamer, 2008; Salomon et al., 2009).
Acute Stress Testing
As previously mentioned, acute stress has long been thought to play a role in the
etiology of human psychopathologies, such as anxiety and depressive disorders, as well
as medical illnesses, like cardiovascular disease (Black & Garbutt, 2002; Chrousos, 2009;
Kessler, 1997; McEwen, 2000; Nugent et al., 2011; Yusef et al., 2004). Due to the
clinical significance of acute stress reactions, investigating the various ways stress
impacts pathological and psychopathological mechanisms is of great importance

BRIEF CLINICAL INTERVENTIONS 7
(McEwen , 2007).
In order to investigate these mechanisms, standardized procedures to induce acute
psychosocial stress have been widely developed (Childs, Vicini, & De Wit, 2006). One
useful tool for this type of research has been laboratory-based mental stress testing. This
particular testing involves the measurement of acute physiological responses, such as
cardiac, neuroendocrine, and autonomic nervous system functions, to standardized
stimuli (e.g., public speaking, mental arithmetic tasks, emotionally demanding social
interaction) (Chida & Hamer, 2008; Hellhammer & Schubert, 2012; Kirschbaum, Pirke,
Hellhammer, 1993). Although psychosocial stress testing involves artificial stimuli, it
allows for the induction of consistent physiological responses with good test–retest
reliability and offers a way to eliminate confounds, thereby elucidating causal factors
(Brotman, Golden, & Wittstein, 2007; Chida & Hamer, 2008).
In contrast to protocols that involve physical exertion or pharmaceutical agents,
acute psychosocial stress stimuli exert physiological, behavioral, and subjective stress
responses (Kudielka, Wust, Kirschbaum, & Hellhammer, 2007). In a meta-analysis of
208 studies, Dickerson and Kemeny (2004) found that psychosocial stress tasks perceived
as uncontrollable and that involve social-evaluative threat elicit the largest physiological
response and longest recovery times. Tasks that are defined as uncontrollable are those
in which outcomes are perceived to be unaffected by individual behavioral responses.
Social-evaluative threat involves the perception that others could negatively judge one’s
task performance, thereby impacting social esteem, self-evaluation, and social goals
(Kudielka et al., 2007). The magnitude of changes in physiological parameters has been
shown to depend on intensity of threat, context, and vulnerability, as well as protective

BRIEF CLINICAL INTERVENTIONS 8
factors (Dickerson & Kemeny 2004).
Trier Social Stress Test. A variety of standardized procedures have been
developed to induce acute psychosocial stress in a laboratory setting. One of the most
widely used protocols to study physiological responses to psychosocial stress is the Trier
Social Stress Test (TSST) (Kirschbaum et al., 1993). The TSST involves a public speech
and mental arithmetic task that is performed in front of an evaluative panel and therefore,
involves elements of uncontrollability and social evaluation. It has been used in research
with healthy study participants and clinical populations. For example, the TSST has been
successfully applied in studies with patients suffering from depressive illnesses, anxiety
disorders (e.g., social phobia, posttraumatic stress disorder), burnout, exhaustion,
functional somatic syndromes (e.g., chronic fatigue syndrome, fibromyalgia, irritable
bowel syndrome), pain, and breast cancer survivors (Kudielka et al., 2007). The TSST is
one of the few available protocols that reliably elicits cardiovascular parameters, having
been shown to produce moderate increases in both heart rate and blood pressure
(Dickerson & Kemeny, 2004; Nater et al., 2005). It has also been proven to produce
moderate increases in cortisol and subjective reports of anxiety (Childs et al., 2006;
Kudielka et al., 2004a; Williams, Hagerty, & Brooks, 2004).
The standardized TSST protocol lasts for a total of thirteen minutes. It involves a
brief preparation period (3 minutes) followed by a test period during which subjects are
asked to deliver a free speech (5 minutes). Lastly, subjects are given a time to perform a
mental arithmetic task (5 minutes). They are asked to take over the role of a job applicant
invited for an interview with the company’s selection committee. The selection
committee is comprised of 2-3 males or females unacquainted with the subject and has

BRIEF CLINICAL INTERVENTIONS 9
been trained to respond in an unresponsive, neutral manner. Selection committee
members are introduced to subjects as being trained to monitor nonverbal behavior.
Subjects are informed that their speech will be taped and video recorded for later
analysis. During the speech period, the selection committee members are given
directions to respond to subjects in a standardized way. For example, if a subject ends the
speech in less than five minutes, members are given prepared questions (e.g., what are
your personal strengths? what are your major shortcomings?) The mental arithmetic task
involves asking the subject to serially subtract an uneven number from a larger number as
fast and as accurately as possible. If the subject makes an error, they are asked to restart
(Kirschbaum et al., 1993).
Over the past two decades, the TSST has shown to be a useful tool in basic,
applied, and clinical psychobiological research. Eliciting a range of psychobiological
outcome variables, the TSST protocol has been utilized in a multitude of studies with
children, adults, and the elderly to investigate the stress-disease connection (Kudielka et
al., 2004a). It has even recently been successfully applied in both group and virtual
reality formats (Child et al., 2006; Jonsson et al., 2010). Inducing endocrine and
cardiovascular responses in 70–80% of subjects tested, the TSST procedure has been
shown to significantly increase parameters such as free cortisol, total plasma cortisol,
adrenocorticotropic hormone, catecholamines, growth hormone, prolactin, testosterone,
blood pressure, heart rate, immune parameters, and measures of hemoconcentration and
blood coagulation (Kirschbaum et al., 1993; Kudielka et al., 2007; Nater et al., 2005).
As previously mentioned, the TSST has been utilized in research investigating
cardiovascular reactions to acute psychosocial stress in nonclinical, healthy populations.
BRIEF CLINICAL INTERVENTIONS 10
For example, in a more recent study, Taylor et al. (2010) found a main effect of time
showing a strong increase in heart rate, systolic blood pressure, and diastolic blood
pressure from baseline to peak stress. Additionally, these researchers found that although
cardiovascular parameters decreased after the post-stress task, full recovery was
incomplete, as evidenced by significant baseline to recovery differences. In another
study conducted by Nater et al. (2005), researchers found a significant difference in heart
rate between the TSST and rest conditions and a positive relationship between salivary
alpha amylase and sympathetic tone during stress. In conclusion, the TSST has been
reliably shown to induce acute physiological reactivity and incomplete recovery from
psychosocial stress.
The TSST has also been successful utilized to investigate the impact psychosocial
factors have on cardiovascular reactions to acute psychosocial stress in clinical
populations and subjects with subthreshold psychological symptomatology. For
example, Chida and Hamer (2008) found that depressive mood or hopelessness exhibited
significant associations with increased cardiovascular reactivity. Regarding
cardiovascular recovery after stress, these researchers found that general life stress and
anxiety, neuroticism, and negative affect were associated with poorer cardiovascular
recovery. In contrast, a meta-analysis conducted by Kibler and Ma (2004), reported
small, nonsignificant effect sizes linking depression to blood pressure reactivity and
modest effect sizes for heart rate reactivity. Additionally, York et al. (2007), Carrol et al.
(2007), and Solomon et al., (2009) found a negative association between depressive
symptoms and cardiovascular reactivity to mental stress. In sum, and as previously
mentioned, current research has shown mixed results on the effects psychological

BRIEF CLINICAL INTERVENTIONS 11
symptoms, particularly depression and anxiety, have on physiological stress reactions.
The TSST has been utilized for well over two decades as a tool to study the
mechanisms by which stress impacts physiological systems. Given its success, the next
important step is to investigate whether the TSST protocol can be utilized to investigate
the efficacy of psychosocial interventions (Kudielka et al., 2007).
Psychosocial Interventions
A key goal for clinical health practitioners is to help patients reduce the
psychological and physiological burden of stress. Over the past few decades, researchers
have been investigating whether social, behavioral, and psychotherapeutic interventions
can help practitioners achieve this goal (McEwen, 2007). Studies have focused on
psychosocial interventions aimed at managing stress, increasing resilience to stressful
experiences, and treating physiologic responses to stress to improve health outcomes,
such as cardiovascular function. These nonpharmacological interventions target lifestyle
factors (e.g., sleep, diet, physical activity), as well as interpersonal relationships, self-
efficacy, and self-esteem (Logan & Barksdale, 2008). Others teach relaxation techniques
to help one cognitively, behaviorally, and physiologically cope with, counteract, or alter
the way in which one experiences and recovers from stressful experiences. Psychosocial
interventions can be offered in both long-term and brief formats, and are thought to offer
a useful, nonpharmacological means to prevent the negative effects stress has in both
healthy and clinical populations. Two such psychosocial interventions are Autogenic
Training (Schultz, 1932) and Acceptance and Commitment Therapy (Hayes, Strosahl, &
Wilson, 1999).
Acceptance and Commitment Therapy. Acceptance and Commitment Therapy
BRIEF CLINICAL INTERVENTIONS 12
(ACT) is a therapeutic approach developed by Hayes et al. (1999) that focuses on
increasing flexibility and willingness to experience stressful and anxiety provoking
events and feelings. It is a comprehensive psychotherapy treatment that can be delivered
in both individual and group formats over both short and long-term. ACT is based on
relational frame theory, a contextual theory of language and cognition (RFT; Barnes-
Holmes, Hayes, & Roche, 2001). Having grown out of the cognitive-behavioral
tradition, ACT is considered a third-wave behavioral therapy. However, unlike CBT,
ACT makes no attempts to change unwanted thoughts or feelings; these are not
necessarily viewed as problematic. As ACT teaches, acceptance and willingness, rather
than control, is what leads a person to desired goals and improvements in quality of life.
In order to attain goals and implement behavior change, ACT makes use of experiential
methods and a number of therapeutic strategies (Hayes, Masuda, Bissett, Luoma, &
Guerrero, 2004).
Many, including ACT followers, conceptualize forms of psychopathology as
unhealthy efforts to control emotions, memories, thoughts, and other internal experiences
(Hayes, Wilson, Gifford, Follette & Strosahl, 1996). ACT teaches that attempts to
control unwanted subjective experiences are counterproductive, resulting in an increase
in psychological distress. ACT teaches positive psychological skills to counteract
attempts to control, such as acceptance and cognitive defusion. Acceptance is taught as
an alternative to experiential avoidance and involves an active embrace of private events
without attempts to change their frequency or form. Cognitive defusion attempts to alter
one’s sensitivity to undesirable thoughts (e.g., “I am being judged”) by reducing the
literal quality of the experienced thought (e.g., I am having the thought “I am being

BRIEF CLINICAL INTERVENTIONS 13
judged”). Cognitive defusion techniques attempt to decrease the believability/reality of
thoughts (Hayes, Luoma, Bond, Masuda, & Lillis 2006).
Although a relatively new psychotherapy treatment, ACT has shown empirical
evidence for its effectiveness in treating a variety of psychopathologies (Forman, Herbert,
Moitra, Yeomans, & Geller, 2007; Hayes et al., 2004). In a recent review of the
literature, Hayes et al. (2006) found that the average post-treatment effect size for
randomized controlled clinical trials of ACT ranged from .55 to .99 and average follow-
up effect sizes ranged from .55 to .80. Studies have shown promising results for its
efficacy in treating depression (Forman et al., 2007; Zettle & Hayes, 1986; Zettle &
Rains, 1989), anxiety (Woods, Wetterneck, & Flessner, 2006; Zettle, 2003), thought
disorders (Bach & Hayes, 2002), substance abuse (Hayes et al., 2004), and workplace
stress (Bond & Bunce, 2003).
For example, in a published study relevant to ours, Block (2002) examined the
efficacy of ACT for social anxiety symptoms. In that study, 39 college students with
public speaking anxiety were semi-randomly assigned to six weeks of either ACT,
cognitive-behavioral group therapy, or a no-treatment, waitlist control. Results showed
that scores on social anxiety decreased for both treatment groups compared to the control
condition. In addition, willingness to engage in public speaking situations increased for
both treatment conditions but only the ACT group showed significant decreases in
behavioral avoidance (Block, 2002). Additionally, in another study conducted by
Forman et al. (2007), 101 university counseling center patients reporting moderate to
severe levels of anxiety or depression were randomly assigned to traditional cognitive
therapy or ACT (medium length of treatment = 15-16 sessions). Results indicated that

BRIEF CLINICAL INTERVENTIONS 14
both cognitive therapy and ACT evidenced large, equivalent improvements in depression,
anxiety, functioning difficulties, quality of life, life satisfaction, and clinician-rated
functioning. In regards to mechanisms of action, researchers found that changes in
“observing” and “describing” one’s experiences appeared to mediate outcomes for
cognitive therapy, whereas “experiential avoidance,” “acting with awareness,” and
“acceptance” mediated outcomes for ACT (Forman et al., 2007).
ACT has also been shown to be a useful therapeutic approach in behavioral
medicine populations. ACT has been implemented with chronic pain (McCracken &
Eccleston, 2006), cigarette smoking cessation (Gifford et al., 2004), diabetes (Gregg,
Callaghan, Hayes, Glenn-Lawson, 2007), and epilepsy (Lundgren, Dahl, & Hayes, 2004)
patients. One hypothesized mechanisms by which ACT benefits medical patient
populations is through its emphasis on emotional acceptance rather than suppression.
Research has shown that certain emotion-regulation processes, such as rumination and
worry, increase distress and prolong physiological stress responses. In contrast,
acceptance-oriented coping strategies promote efficient cardiovascular habituation and
recovery from stress (Campbell-Sills, Barlow, Brown, & Hofmann, 2006; Low, Stanton,
& Bower, 2008).
For example, in a recent study conducted by Low et al. (2008), 81 participants
were randomly assigned to write about ongoing stressful experience while either (1)
evaluating the appropriateness of their emotional response, (2) attending to their emotions
in accepting way or, (3) simply describing the objective details of their experience.
Results indicated that writing about emotions in an evaluative way led to less efficient
heart rate habituation and recovery than processing emotions in an accepting manner

BRIEF CLINICAL INTERVENTIONS 15
(Low et al., 2008). In another study by Campbell-Sills et al. (2006), researchers
compared subjective and physiological effects of emotional suppression and acceptance
in 60 subjects diagnosed with anxiety and mood disorders. Subjects were randomly
assigned to either a group that listened to a rationale for suppressing emotions or a group
that listened to a rationale for accepting emotions. Subjective distress, heart rate, skin
conductance level, and respiratory sinus arrhythmia were measured before, during, and
after watching an emotion-provoking film during which the subjects were told to apply
the learned instructions. Results indicated that both groups reported similar levels of
subjective distress during the film but that the acceptance group displayed less negative
affect during the post-film recovery period. Additionally, the suppression group showed
an increased heart rate while the acceptance group showed a decreased heart rate in
response to the film (Cambell-Sills et al., 2006). In sum, there is solid and growing
evidence that ACT is a beneficial intervention for both nonclinical and clinical
populations.
Autogenic Training. Autogenic Training (AT) is a relaxation technique
performed through passive concentration aimed at promoting relaxation and stress relief.
Johannes Schultz, a German psychiatrist and neurologist, first presented AT in the 1930s.
Schultz theorized that mentally connecting with parts of one’s body produces a state
similar to that experienced under hypnosis and found that his technique of AT improved
health and reduced stress in many of his patients (Schultz, 1932). AT was further
developed by Wolfgang Luthe and in its’ current form involves a series of statements
aimed at reducing autonomic arousal (Linden, 1990; Luthe, 1969; Luthe & Schultz,
1959). AT teaches passive concentration on breathing, heartbeat, warmth, and heaviness
BRIEF CLINICAL INTERVENTIONS 16
of body parts, and is normally taught and learned over a period of eight to ten weeks
(Kanji, 1997; Morgan & Jorm, 2008). AT is based on three main principles: reduction of
exteroceptive and proprioceptive afferent stimulation, mental repetition of
psychophysiologically adapted verbal statements, and mental activity conceived as
'passive concentration' (Schulz, 1932; Kanji, 1997). Some believe that AT may be
superior to other behavioral relaxation techniques because it teaches individuals how to
self-regulate physiological responses and, once learned, can be practiced without a
therapist (Cowings, Toscano, Timbers, Casey, & Hufnagel, 2005; Schlamann, Naglatzki,
de Greiff, Forsting, & Gizewski, 2010).
AT offers individuals a way in which to exert calming effects on their mind and
body. A meta-analysis by Stetter & Kupper (2002) on 60 randomized controlled trials
found main effects in the range of medium-to-large effect sizes for pre-post comparisons
of disease specific AT-effects. They also found that unspecific AT-effects, such as
mood, cognitive performance, physiological variables, and quality of life, were larger
than main effects. Analyzing study populations separately, they found positive effects in
the medium effect size range for migraines, hypertension, coronary heart disease, pain
disorder, anxiety disorders, mild-to-moderate depression, and functional sleep disorders.
However, they also observed that AT had not been compared with cognitive or exposure
therapy or psychopharmacological treatments for depression and anxiety, and that
comparison with medical treatments were rare. In sum, Stetter & Kupper (2002) stated
that AT results in medium-to-large clinical main effects that are stable at follow-up, but
further comparison to other efficacious treatments are needed.
In a randomized controlled trial conducted by Kanji, White, & Ernst (2004a)
BRIEF CLINICAL INTERVENTIONS 17
researchers observed the effectiveness of AT in reducing anxiety in a group of nursing
students. The study investigated the differential effects interventions (e.g., AT, attention
control group, time control group) have on anxiety, burnout, and cardiovascular
parameters. They found a greater reduction of state and trait anxiety in the AT group
than in other groups immediately after treatment but no differences between groups for
burnout. They also found that the AT group had the greatest reduction immediately after
treatment in systolic blood pressure, diastolic blood pressure, and heart rate. In regards to
depressive symptoms, Krampen (1999) compared AT with individual psychotherapy and
delayed treatment in 55 adults with depressive disorders. Subjects were randomized to
one of three groups: individual psychotherapy alone, AT and individual psychotherapy,
and waitlist control. In long-term follow-up (3 years), results showed that AT in
combination with individual psychotherapy resulted in more positive effects than
psychotherapy alone, such as lower rates of relapse and treatment reentry, and reductions
in depressive and somatic symptoms. In another study with 134 adults with minor,
subclinical depressive symptoms, Farne and Gnugnoli (2000) found that AT improved
depressive mood after three months significantly more than in the control group. These
results demonstrate that AT may be a beneficial intervention for patients suffering from
minor to moderate psychological pathology.
Studies have also found AT to have positive effects in medical patients with high
blood pressure, early stage cancer, irritable bowel syndrome, migraines, and acute
anxiety, (Aivazyan, Zaitsev, & Yurenev, 1988; Herbert & Gutman, 1983; Hidderley &
Holt, 2004; Kanji, White, & Ernst, 2004b; Kanji, White, & Ernst, 2006; Labbe, 1995;
Shinozaki et al., 2010; Ter Kuile, Spinhoven, Linssen, Zitman, & Van Dyck, 1994;
BRIEF CLINICAL INTERVENTIONS 18
Zsombok, Juhasz, Buravari, Vitrai, & Bagdy, 2003). In regards to cardiovascular
function, Atkinson et al. (2000) found that AT showed a greater reduction immediately
after treatment in blood pressure and heart rate measures compared to a control group. In
59 patients undergoing coronary angioplasty, Kanji et al. (2004b) found significant
reductions in anxiety in AT group at two and five months post surgery. Additionally, in a
pilot study of early stage cancer patients, Hidderley and Holt (2004) found that AT
resulted in a decrease in anxiety and depression, and an increase in immune responses (as
measured by T and B cell markers). In sum, AT has shown to be a beneficial relaxation
intervention in both nonclinical and clinical populations.
As the literature shows, both Acceptance and Commitment Therapy and
Autogenic Training have been applied successfully in a variety of study populations.
However, to date, ACT and AT have yet to be applied in brief formats to investigate the
differential, and possible buffering, effects these interventions have on physiological
stress reactions to acute psychosocial stress.
Present Study
As previously mentioned, allostatic load provides a conceptual and
methodological basis for elucidating behavioral and physiological mechanisms of stress.
It offers a mechanistic framework for investigating how genes, early life experiences,
current environments, interpersonal relationships, and lifestyle factors join to affect the
structure and function of the human body. Most importantly, it offers a basis for
understanding the etiology of systemic illnesses. Allostatic load allows one to consider
the multiple pathways of cause and effect with consideration of interactions between
BRIEF CLINICAL INTERVENTIONS 19
organ systems, for example, the link between cardiovascular disease and anxiety and
depressive symptoms (Juster et al., 2011; McEwen, 2000).
The primary aim of the current study was to investigate physiological stress
reactions to an acute psychosocial stressor and the possible buffering effects brief
interventions have on these reactions. To address this aim, participants were randomized
to one of three intervention conditions (Acceptance and Commitment Therapy (ACT),
Autogenic Training (AT), or Attention-only Control condition) prior to undergoing an
acute psychosocial stress protocol (Trier Social Stress Test; TSST).
In addition, for clinical assessment and intervention purposes, we believed it was
highly warranted to investigate how certain psychological symptoms (e.g., anxiety and
depression) influence acute physiological stress reactions and if they moderate the
treatment response. To address these exploratory aims, participants were asked to
complete a variety of psychosocial measures, including measures of anxiety and
depression, prior to the TSST.
We hypothesized that brief interventions (ACT and AT) would have differential
effects on physiological stress reactions. We believed that the experimental conditions
(ACT and AT) would buffer the stress response and result in lower reactivity and greater
recovery following the TSST. More specifically, we thought Autogenic Training would
be superior to the Acceptance and Commitment Therapy condition, and that both would
be superior to the Control Condition. We also hypothesized that anxiety (social anxiety,
trait anxiety, anxiety sensitivity) and depressive symptoms would impact the
physiological stress response in that higher symptomatology would result in greater
reactivity and lower recovery following the TSST. Lastly, we hypothesized that anxiety
BRIEF CLINICAL INTERVENTIONS 20
and depression would moderate the treatment response.
Method
Participants
Data for the present study was collected as a part of a larger study exploring the
effects brief interventions have on subjective and objective stress reactions. Participants
were drawn from the undergraduate population at the University of Connecticut, Storrs
from Fall 2009 to Spring 2011. Participants were recruited through the Psychology 1100
and 1103 participant pool for which they registered to gain experience regarding the
experimental method while earning credits as unpaid participants in psychological
research. For inclusion, participants were between 18-25 years of age and were able to
provide informed consent. There were no additional inclusion or exclusion criteria. A
total of 123 students consented and data was collected on all of them. The average age
was 19.08 (1.02) years; 66.67% were women, and 67.5% were White.
Procedure
The Institutional Review Board at the University of Connecticut approved the
study, which was a randomized controlled trial utilizing a repeated measures cohort
design. Participation involved one, three-hour visit to the lab. The study was broken
down into three main assessment points (see Appendix A):
Time 1 lasted approximately 75 minutes. Upon arrival to the lab, informed
consent was obtained. Following this process, participants completed a Demographic
and Medical History Questionnaire, along with baseline physiological (heart rate and
blood pressure) and psychological assessments (Anxiety Sensitivity Index, Beck
Depression Inventory-II, Liebowitz Social Anxiety Scale, Spielberger State-Trait Anxiety
BRIEF CLINICAL INTERVENTIONS 21
Inventory- Trait Form). Next participants were randomized to one of three conditions.
The first condition involved an Acceptance and Commitment Therapy intervention, the
second condition involved an Autogenic Training intervention, and the third condition
was an Attention-only Control group (described in further detail below). All interventions
lasted twenty minutes.
Time 2 lasted approximately 45 minutes. It began immediately after the
intervention with a second physiological assessment (heart rate and blood pressure).
Next, participants completed the Trier Social Stress Test (TSST; described in further
detail below).
Time 3 lasted approximately 60 minutes. It began immediately following the
conclusion of the TSST with a third physiological assessment (heart rate and blood
pressure). Participants were then debriefed on the aims of the study. They were informed
that the recording equipment was not turned on and that their performance was not
recorded using any audiovisual equipment. They were also introduced to the two
confederates who made up the selection committee. Subjects were told that these
individuals were undergraduate research assistants who were trained to play roles.
Following the debriefing, all participants engaged in a period of rest before a final
physiological assessment (heart rate and blood pressure) was conducted. At the
conclusion of the study, participants were given time to ask questions and thanked for
their participation.
Physiological Measures
Blood pressure and heart rate were collected non-invasively utilizing a
commercially available monitor (Omron Digital Blood Pressure Cuff; model number
BRIEF CLINICAL INTERVENTIONS 22
HEM-907XL; White & Anwar, 2001). The device was used in accordance with the
directions provided with the equipment. Participants were asked to sit comfortably and
upright in a chair while the monitor’s cuff was placed around their upper arm to
simultaneously measure blood pressure and heart rate. One reading per time point was
made.
Psychological Measures
Anxiety Sensitivity Index. The Anxiety Sensitivity Index (ASI; Reiss, Peterson,
Gursky, & McNally, 1986) is a 16-item self-report questionnaire that assesses fear of
anxiety sensations. Subjects rate scale items on a 5-point scale (0 = very little; 4 = very
much) to indicate to what extent they agree with statements such as: ‘It scares me when I
feel faint,’ ‘It is important for me to stay in control of my emotions,’ and ‘Other people
notice when I feel shaky.’ The scale yields one total summary score ranging from 0 to
64. Various ASI reliability studies revealed a high degree of internal consistency with
Cronbach’s alpha statistics ranging from .80 to .90. The ASI has been shown to measure
a stable personality trait, as one study reported a three-year test-retest correlation of .71
(Maller & Reiss 1992; Reiss 1991). The ASI has also shown excellent diagnostic
criterion validity. Scores have been found to be strongly associated with fearfulness,
panic attacks, and subjective anxiety during biological challenge (Reiss et al., 1986;
Reiss, Peterson, & Gursky, 1988; Peterson & Sacks 1987; Maller & Reiss 1987). In the
present study, the ASI was shown to have good internal consistency (average α = .86).
Beck Depression Inventory-II. The Beck Depression Inventory-II (BDI-II;
Beck, Steer, & Brown, 1996) is a 21-item self-report measure that assesses depressive
symptoms. Subjects rate scale items on a 4-point scale (0-3) to indicate which statement

BRIEF CLINICAL INTERVENTIONS 23
in each group best describes the way they have been feeling during the past two weeks.
Items measure both cognitive (e.g., self-dislike, guilt) affective (e.g., sadness, crying),
and neurovegetative (e.g., appetite, sleep) symptoms. The scale yields one total summary
score ranging from 0-63; higher scores indicate increasing intensity of depressive
symptoms. The BDI-II is one of the most widely used depression rating scales for both
clinical and research purposes. It has demonstrated excellent internal consistency with an
alpha coefficient of .92, excellent concurrent validity, construct validity, and test-retest
reliability across studies (Beck, Steer, Ball, & Ranieri, 1996). In the present study, the
BDI-II had an average α of .33.
Demographics and Medical History Questionnaire. The Demographic and
Medical History Questionnaire was created specifically for this study. It gathers basic
demographic data, such as date of birth, and race and ethnicity, as well as medical
information necessary for analyses of physiological data. Questions include diagnoses of
mental and/or physical illness, medication(s), weight and height, substance use, and
exercise.
Liebowitz Social Anxiety Scale. The Liebowitz Social Anxiety Scale (LSAS;
Liebowitz, 1987) is a 24-item self-report questionnaire that measures respondents’ fear
and avoidance of social situations, such as social interactions (e.g., going to a party,
meeting strangers) and public performances (e.g., giving a prepared oral talk, speaking up
at a meeting). Each item is rated on two 4-point scales, the first measures fear/anxiety
and the second measures avoidance. Scores range from 0 (no fear/never avoid) to 3
(severe fear/usually avoid). The scale yields one total summary score ranging from 0-
144; higher scores indicate increasing intensity of social anxiety. Total scores have been
BRIEF CLINICAL INTERVENTIONS 24
shown to adequately differentiate between individuals with and without social anxiety
disorder (i.e., social phobia). The LSAS has demonstrated adequate reliability and
validity. The scale has shown excellent internal consistency with an alpha coefficient of
.95. It also has good test-retest reliability, as well as good discriminant and convergent
validity (Heimberg et al., 1999; Fresco et al., 2001; Baker et al., 2002). The LSAS was
shown to have good internal consistency in the present study (average α = .85).
Spielberger State-Trait Anxiety Inventory. The Spielberger State-Trait Anxiety
Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1970) is a self-report questionnaire
that consists of two 20-items subscales. The state subscale (“state anxiety”) assesses
momentary anxiety and includes statements such as ‘I feel secure,’ ‘I am jittery,’ and ‘I
feel confused.’ The trait subscale (“trait anxiety”) assesses the stable tendency to
experience anxiety and includes statements such as ‘I lack self-confidence,’ ‘I feel
nervous and restless,’ and ‘I feel rested.’ For the state subscale, subjects are asked to
answer based on how they feel at that present moment. For the trait subscale, subjects are
asked to answer based on how they generally feel. Scores for individual items range
from 1 (not at all/almost never) to 4 (very much so/almost always), with total scale scores
ranging from 20-80. Higher scores indicate higher degrees of anxiety. The STAI is one
of the most frequently used self-report measures of state and trait anxiety with adequate
reliability and validity. The trait subscale has shown good internal consistency (median
alpha coefficient .90) and adequate test-retest reliability (ranging from .73 to .86). The
state subscale has shown good internal consistency as well (median alpha coefficient .93)
and expected low test-retest reliability given it assesses momentary anxiety (scores
ranging from .16 to .62; Spielberger, 1983). In this study, we only utilized the trait
BRIEF CLINICAL INTERVENTIONS 25
subscale (STAI- Trait), which was shown to have excellent internal consistency in the
present study (average α = .92).
Experimental and Control Conditions
ACT intervention. This experimental condition involved exercises drawn from
Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999). This
condition involved the researcher explaining and defining the main principles of ACT
(e.g., experiential avoidance and cognitive fusion). It also utilized time to teach strategies
for coping with anxiety (e.g., acceptance and defusion techniques) and involved
experiential exercises (e.g., envisioning emotions as waves and observing and labeling
thoughts).
AT intervention. This experimental condition involved Autogenic Training (AT;
Schultz, 1932), which is a self-relaxation procedure. This condition involved the
researcher offering a rationale for Autogenic Training. The researcher than lead
participants through a series of statements, which facilitated a passive concentration on
bodily perceptions (e.g., heaviness in the limbs, feelings of warmth) aimed at relieving
tension and stress.
Attention-only Control. This control condition involved an attention-only task.
The researcher read aloud from a fictional book called, “Journey Under the Sea,” which
is a book from “Choose Your Own Adventure” series (Published by Chooseco LLC).
These books are interactive and ask readers to make decisions throughout the story. The
participants were involved in giving their input in choosing the various story lines,
therefore ensuring engagement in the task.
Challenge Task
BRIEF CLINICAL INTERVENTIONS 26
Trier Social Stress Test protocol. As previously described, the Trier Social
Stress Test (TSST; Nater et al., 2005) is a widely utilized standardized protocol for the
induction of psychological stress in a laboratory setting. In this study, the TSST began
with the researcher leading the participant to a different room, where they were
introduced to two confederates sitting at a table (trained undergraduate research assistants
posing as a selection committee). In the room, there was a podium where the participant
was instructed to stand, along with a video camera and a tape recorder. The researcher
explained the task they were about to perform which involved assuming the role of a job
applicant who is invited for an interview. Participants were told that after having a few
minutes to prepare, they would be asked to give a 5-minute speech about why they are
the best person for the job position. Participants were told that the selection committee
was specially trained to monitor nonverbal behavior, that a video recording of their
speech would be conducted, and that a voice frequency analysis of nonverbal behavior
would be performed at a later date. After the instructions were read, participants were led
back to room A, where they were given three minutes to prepare a speech. After their
time was up, they were led back into room B where they were asked to deliver their
speech. After five minutes, the committee interrupted the participant and asked him/her
to serially subtract the number 13 from 1,022 as fast and as accurately as possible. On
every failure the participant had to restart at 1,022 with one member of the committee
interfering with, “Stop – mistake – start over at 1,022, please.” The participant was given
five minutes to complete this task before being led back to room A for further assessment
and debriefing.
Data Analytic Plan
BRIEF CLINICAL INTERVENTIONS 27
All data analyses were performed using SPSS version 19.0 (SPSS, Inc., 2010).
We first conducted exploratory data analyses to assess demographic composition of the
sample and to determine whether variables of interest met assumptions of normality.
Bivariate correlation matrixes were computed using data from the Demographic and
Medical History Questionnaire to determine whether potential covariates should be
controlled for in analyses. ANOVA’s were conducted to assess baseline differences
between measures. Where appropriate, Tukey’s HSD post hoc comparisons were used
for a posteriori comparisons among means. Three participants were excluded: one
participant was excluded based on age, and two others did not complete the study in its
entirety due to the severity of their baseline psychological symptoms and the moderately
stressful nature of the TSST.
To test whether brief interventions have differential effects on physiological stress
reactions over time, 3 (experimental condition) x 4 (time) repeated measures ANOVAs
and ANCOVAs were conducted for heart rate, systolic blood pressure, and diastolic
blood pressure. To test whether depression and/or anxiety moderate the treatment
response, ANCOVAs were conducted utilizing total scores on the ASI, BDI-II, LSAS,
and STAI-Trait as moderator variables, entered as covariates into analyses. To explain
significant three-way interactions, ANCOVAs were conducted to describe depression and
anxiety effects for each treatment group separately. ANCOVAs were also conducted to
demonstrate intervention effects for low and high anxiety and depression separately.
Median splits were utilized to dichotomize psychosocial variables in these analyses.
Reactivity scores were calculated as the change between time 2 and time 3 cardiovascular
measures. Recovery scores were calculated as change scores between time 3 and time 4.
BRIEF CLINICAL INTERVENTIONS 28
Parameter estimates were used to graph 3-way interactions with continuous variables.
This allowed us to best graphically illustrate psychological indices as moderator variables
in a nonclinical sample; high and low BDI-II, STAI-Trait, ASI, and LSAS variables were
defined as follows: high = 1 SD above the mean, low = 1 SD below the mean.
All analyses were first run with four time points including baseline cardiovascular
measures (time 1, time 2, time 3, time 4). Separate analyses were then run on only three
time points (time 2, time 3, time 4) with baseline cardiovascular values as covariates to
control for baseline effects on reactivity and recovery. Next, a series of analyses were
conducted to determine the influence of potentially confounding factors on baseline
cardiovascular measures. Any demographic variable associated with baseline HR, SBP,
or DBP at p ≤ .1 was considered a potential confound, and thus, entered as a covariate in
relevant analyses. In sum, bivariate correlations revealed that exercise was a potential
confound for baseline HR; drug use, alcohol consumption, gender, and BMI were
potential confounds for baseline SBP; and drug use, smoking, and BMI were potential
confounds for DBP. Experimenter and time of day were also used as covariates to
control for between group differences observed in baseline cardiovascular measures.
Analyses were finally run with baseline cardiovascular values and the above-mentioned
relevant physiological covariates. Reported results were corrected by Greenhouse-
Geisser procedure where appropriate (violation of sphericity assumption), indicated by
uneven degrees of freedom (Greenhouse and Geisser, 1959; Vasey and Thayer, 1987).
Throughout, partial eta2 is reported as a measure of effect size.
Lastly, in order to investigate whether depressive and/or anxiety symptoms are
associated with greater reactivity and lower recovery following the TSST, partial
BRIEF CLINICAL INTERVENTIONS 29
correlations were conducted. Intervention group was entered as covariate in all analyses
to control for possible intervention effects. In our analyses, power ranged from 0.4 to 1.0.
Results
Participant Characteristics
Demographic characteristics by group and gender of those included in the
analyses are presented in Tables 1-2. Participants included 120 college undergraduate
students. The average age of participants was 19.08 years (SD = 1.02). Two-thirds were
female (n = 80). All participants reported race/ethnicity as follows: 67.5% White, Non-
Hispanic; 12.5% Black/African American; 11.7% Asian; 6.6% Hispanic/Latino;
Biracial/Multiracial 1.6%. Seventeen individuals (14.2%) reported a mental health
diagnosis (e.g., depression, anxiety) and nine individuals (7.5%) reported a chronic
medical condition (e.g., asthma, diabetes). Thirty-three individuals (27.5%) reported
daily medication use (e.g., birth control, psychiatric medications). Over half the sample
(57.5%) reported alcohol consumption, 5% reported cigarette smoking, and 13.3%
engaged in illicit drug use (e.g., marijuana). Average body mass index was 23.44 kg/m2
(SD = 4.02) and 55% reported engagement in regular physical activity.
Descriptive Statistics for Study Measures
Descriptive statistics for all physiological measures at each time point by group
are detailed in Table 3 and for each time point by gender in Table 4. Statistics for
psychological measures are also included. Baseline statistics are reported below.
Baseline physiological measures. Mean baseline heart rate (bpm) for all
participants (n = 120) was 76.47 bpm (SD = 14.72). ANOVAs were conducted to
determine significant between group differences in baseline heart rate. A significant
BRIEF CLINICAL INTERVENTIONS 30
difference (p ≤ 0.05) was found, such that the AT intervention group (mean = 81.78 bpm)
had a higher mean baseline heart rate compared to the ACT (mean = 73.60 bpm) and
Control (mean = 74.03 bpm) groups.
Mean baseline systolic blood pressure (mmHg) for all participants (N = 120) was
126.11 mmHg (SD = 14.60). ANOVAs were conducted to determine significant between
group differences in baseline systolic blood pressure. No differences between
intervention groups were found.
Mean baseline diastolic blood pressure (mmHg) for all participants (n = 120) was
72.97 mmHg (SD = 8.90). ANOVAs were conducted to determine significant
differences between intervention groups in baseline systolic blood pressure. A significant
group difference (p ≤ 0.05) was found between the AT (mean DBP was 76.43 mmHg, SD
= 8.57) and Control (mean DBP was 69.45 mmHg, SD = 8.76) groups.
Psychological measures. All psychological measures were administered once at
baseline. ANOVAs were conducted and no group differences were found among any of
the psychological measures. Mean score for the BDI-II was 8.34 (SD = 6.87), for the
LSAS was 35.50 (SD = 21.60), for the STAI-Trait was 38.88 (SD = 10.67), and for the
ASI was 19.65 (SD = 9.98).
Hypothesis 1: Impact of Brief Clinical Interventions
For heart rate (HR), repeated measures ANOVAs revealed a main effect of time
(F (2.30, 269.55) = 59.58, p ≤ .001, η2
= .34) as well as a time by group interaction (F
(4.61, 269.55) = 3.82, p = .003, η2
= .06). Post hoc tests indicate a group differences in
HR at baseline among AT and ACT (p = .032), and AT and Control groups (p = .045),
but at no other time point. Thus, after controlling for baseline HR, repeated measures
BRIEF CLINICAL INTERVENTIONS 31
ANCOVAs revealed no effects. However, once relevant covariates (exercise, time of
day, experimenter) were controlled for along with baseline HR, a main effect of time
reemerged (F (1.91, 216.08) = 3.25, p = .04, η2
= .03), demonstrating a significant change
in HR over time.
For systolic blood pressure (SBP), repeated measures ANOVAs revealed a main
effect of time (F (2.88, 337.22) = 53.08, p ≤ .001, η2
= .31). Repeated measures
ANCOVAs, with baseline SBP as a covariate, revealed no main or interaction effects.
Similarly, controlling for relevant covariates (drug use, alcohol, gender, BMI, time of
day, experimenter) along with baseline SBP did not reveal any significant effects.
For diastolic blood pressure (DBP), repeated measures ANOVAs revealed a main
effect of time (F (2.9, 338.72) = 43.86, p ≤ .001, η2
= .27) as well as a time by group
interaction (F (5.79, 338.72) = 2.39, p = .03, η2
= .04). Post hoc tests indicate a group
differences in DBP at baseline among the AT and Control groups (p = .001). Controlling
for baseline DBP revealed no main or interaction effects. Additionally, controlling for
relevant covariates (drug use, smoker, BMI, time of day, experimenter) along with
baseline DBP did not reveal any significant effects.
Hypothesis 1a: Depressive and/or Anxiety Symptoms as Treatment Moderators
Depression (Beck Depression Inventory-II). For HR, repeated measures
ANCOVAs, with total BDI-II score entered as a covariate to test for moderation, revealed
a main effect of time (F (2.27, 258.18) = 20.10, p ≤ 0.001, η2
= .15) as well as a time by
group interaction (F (4.53, 258.18) = 2.47, p = .04, η2
= .04). Post hoc tests indicate a
group differences in HR at baseline among AT and ACT (p = .032), and AT and Control
groups (p = .045), but no group differences at any other time point. Thus, controlling for
BRIEF CLINICAL INTERVENTIONS 32
baseline HR revealed no main or interaction effects. However, once relevant covariates
(exercise, time of day, experimenter) were controlled for along with baseline HR, a main
effect of time reemerged (F (1.89, 208.20) = 3.60, p = .031, η2
= .03), demonstrating a
significant change in HR over time.
For SBP, repeated measures ANCOVAs, with total BDI-II score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.82, 321.99) = 25.77,
p ≤ 0.001, η2
= .18) as well as a 3-way time by group by depression interaction (F (5.65,
321.99) = 2.24 p = .043, η2
= .04), which remained after controlling for baseline SBP (F
(3.8, 214.4) = 2.46, p = .05, η2
= .04); see Figures 1-5. The 3-way interaction
demonstrates that across time points, SBP is affected differently among intervention
groups depending on level of depression. In the AT group, subjects with lower levels of
depressive symptomatology displayed greater SBP reactivity to the TSST compared to
those with higher levels of symptomatology (F (1, 37) = 4.72, p = .036, η2
= .11); see
Figure 1. There was neither a significant difference in SBP reactivity or recovery
between levels of depression in either the ACT or Control conditions nor a significant
difference in SBP between groups at a given level of depression at any time point (p’s >
.1); See Figures 2-5. Once relevant covariates (drug use, alcohol, gender, BMI, time of
day, experimenter) were controlled for along with baseline SBP, the 3-way interaction
was no longer significant (p = .06).
For DBP, repeated measures ANCOVAs, with total BDI-II score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.9, 330.07) = 19.56, p
≤ 0.001, η2
= .15) as well as a time by group interaction (F (5.79, 330.07) = 73.09, p =
.047, η2
= .02). Post hoc tests indicate a group difference in DBP at baseline among the

BRIEF CLINICAL INTERVENTIONS 33
AT and Control groups (p = .001). Once baseline DBP was controlled for, no main or
interaction effects were observed. Similarly, controlling for relevant covariates (drug
use, smoker, BMI, time of day, experimenter), along with baseline DBP, did not result in
any significant effects.
Anxiety Sensitivity (Anxiety Sensitivity Index). For HR, repeated measures
ANCOVAs, with total ASI score entered as a covariate to test for moderation, revealed a
main effect of time (F (2.28, 259.3) = 5.16, p = .004, η2
= .04). Controlling for baseline
HR revealed no main or interaction effects. However, once relevant covariates (exercise,
time of day, experimenter) were controlled for along with baseline HR, a main effect of
time reemerged (F (1.9, 208.64) = 3.13, p = .048, η2
= .03), indicating a significant
change in HR over time.
For SBP, repeated measures ANCOVAs, with total ASI score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.86, 326.06) = 16.96,
p ≤ 0.001, η2
= .13). Once baseline SBP was added as a covariate, however, no main or
interaction effects were observed. Similarly, controlling for relevant covariates (drug
use, alcohol, gender, BMI, time of day, experimenter), along with baseline SBP, did not
result in any significant effects.
For DBP, repeated measures ANCOVAs, with total ASI score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.89, 329.12) = 7.54, p
≤ 0.001, η2
= .06). Once baseline DBP was controlled for, however, no main or
interaction effects were observed. Similarly, controlling for relevant covariates (drug
use, smoker, BMI, time of day, experimenter), along with baseline DBP, did not result in
any significant effects.

BRIEF CLINICAL INTERVENTIONS 34
Social Anxiety (Liebowitz Social Anxiety Scale). For HR, repeated measures
ANCOVAs, with total LSAS score entered as a covariate to test for moderation, revealed
a main effect of time (F (2.3, 255.01) = 9.18, p ≤ 0.001, η2
= .08). Controlling for baseline
HR revealed no main or interaction effects. However, once relevant covariates (exercise,
time of day, experimenter) were controlled for along with baseline HR, a main effect of
time reemerged (F (1.92, 205.01) = 5.02, p = .008, η2
= .05), indicating a significant
change in HR over time.
For SBP, repeated measures ANCOVAs, with total LSAS score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.9, 322.33) = 10.39, p
≤ 0.001, η2
= .09) as well as a 3-way time by group by social anxiety interaction (F (5.81,
322.33) = 2.68, p = .016, η2
= .05). This 3-way interaction remained after controlling for
baseline SBP (F (3.91, 214.86) = 3.46 p = .01, η2
= .06) and after controlling for relevant
covariates (drug use, alcohol, gender, BMI, time of day, experimenter) along with
baseline SBP (F (3.9, 200.77) = 3.8 p = .006, η2
= .07); See Figures 6-10. The 3-way
interaction demonstrates that across time points, SBP is affected differently among
intervention groups depending on level of social anxiety. In the AT group, individuals
with lower levels of social anxiety symptomatology recovered less after the TSST than
those with higher levels of symptomatology (F (1, 37) = 6.17, p = .018, η2
= .14); see
Figure 6. At time 4, there was a significant difference in SBP between levels of social
anxiety symptomatology in the AT group (F (1, 37) = 5.13, p = .029, η2
= .12); see Figure
6. There was neither a significant difference in SBP reactivity or recovery between levels
of social anxiety in either the ACT or Control conditions nor a significant difference in

BRIEF CLINICAL INTERVENTIONS 35
SBP between groups at a given level of social anxiety at any time point (p’s > .1); see
Figures 7-10.
For DBP, repeated measures ANCOVAs, with total LSAS score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.88, 320.10) = 10.0, p
≤ 0.001, η2
= .08) as well as a 3-way time by group by social anxiety interaction (F (5.77,
320.1) = 2.34, p = .034, η2
= .04). This 3-way interaction remained after controlling for
baseline DBP (F (3.92, 215.75) = 2.7, p= .032, η2
= .05); see Figures 11-15. The 3-way
interaction demonstrates that across time points, DBP is affected differently among
intervention groups depending on level of social anxiety. In the AT group, individuals
with lower levels of social anxiety symptomatology recovered less after the TSST than
those with higher levels of symptomatology (F (1, 37) = 4.38, p = .043, η2
= .11); see
Figure 11. There was neither a significant difference in DBP reactivity or recovery
between levels of social anxiety in either the ACT or Control conditions nor a significant
difference in DBP between groups at a given level of social anxiety at any time point (p’s
> .1); see Figures 12-15. Once relevant covariates (drug use, smoker, BMI, time of day,
experimenter) were controlled for along with baseline DBP, the 3-way interaction was no
longer significant (p = .056).
Trait Anxiety (Spielberger State Trait Anxiety Inventory- Trait). For HR,
repeated measures ANCOVAs, with total STAI-Trait score entered as a covariate to test
for moderation, revealed no main or interaction effects. Similarly, controlling for
baseline HR, no main or interaction effects were observed. However, once relevant
covariates (exercise, time of day, experimenter) were controlled for along with baseline
BRIEF CLINICAL INTERVENTIONS 36
HR, a main effect of time was emerged (F (1.91, 209.54) = 3.34, p = .039, η2
= .03),
indicating a significant change in HR over time.
For SBP, repeated measures ANCOVAs, with total STAI-Trait score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.85, 324.61) = 5.71, p
= .001, η2
= .05). Once baseline SBP was added as a covariate, however, no main or
interaction effects were observed. Similarly, controlling for relevant covariates (drug
use, alcohol, gender, BMI, time of day, experimenter), along with baseline SBP did not
result in any significant effects.
For DBP, repeated measures ANCOVAs, with total STAI-Trait score entered as a
covariate to test for moderation, revealed a main effect of time (F (2.88, 328.36) = 4.17, p
= .007, η2
= .04). Once baseline DBP was controlled for, however, no main or interaction
effects were observed. Similarly, controlling for relevant covariates (drug use, smoker,
BMI, time of day, experimenter), along with baseline DBP and STAI-Trait did not result
in any significant effects.
Hypothesis 1b: Association of Depressive and Anxiety Symptoms with
Cardiovascular Reactivity and Recovery
Partial correlations, with group as covariate, revealed no associations between
depression (as measured by total score on the BDI-II) and HR, SBP, or DBP reactivity or
recovery. Additionally, no associations were found between social anxiety (as measured
by total score on the LSAS) or trait anxiety (as measured by total score on the STAI-
Trait) and HR, SBP, or DBP reactivity or recovery. However, HR reactivity was found
to be positively associated with anxiety sensitivity (as measured by total score on the
ASI) (pr = .21, p = .027). No associations were observed between HR recovery and ASI.
BRIEF CLINICAL INTERVENTIONS 37
Discussion
Purpose of the Present Study
Stress is a psychosocial risk factor that has long been linked to medical illness and
various psychopathologies (Kessler, 1997; McEwen, 2003; Nugent et al., 2011). While it
has been well established that behavioral factors (e.g., diet, exercise, substance use) play
a critical role in the onset and maintenance of stress-related illness, the role of internal
biological mechanisms of stress are less understood (Luthar, 2003; McEwen, 2000). As
discussed throughout the introduction, the concepts of allostasis and allostatic load offer a
useful framework for investigating the psychobiological mechanisms affected by stress,
particularly those involving the cardiovascular system (McEwen & Stellar 1993; Sterling
& Eyer, 1988).
In our study we set out to examine cardiovascular stress reactions to an acute
psychosocial stressor and were particularly interested in investigating whether brief
psychosocial interventions would attenuate these reactions. As previously mentioned,
although responses to stressors in a laboratory setting may not be of great clinical
importance, they indicate how a person responds to stressful demands in their everyday
life and offer a useful way to examine disturbed stress responses that may have
pathological consequences (Chida & Hamer, 2008; Salomon et al., 2009). Additionally,
laboratory settings provide a controlled environment whereby direct physiological
outcomes to clinical interventions can be validly acquired. Another aim of our study was
to explore how certain psychological symptoms (e.g., anxiety and depressive
symptomatology) influence acute physiological stress reactions and whether these
symptoms moderate the treatment response to brief interventions. Given the current
BRIEF CLINICAL INTERVENTIONS 38
discrepancy among the literature in regards to how psychosocial factors affect the stress
response, we believe this aim offers important implications for clinical assessment and
intervention.
To our knowledge, this is the first study to examine the effects brief clinical
interventions have on cardiovascular reactions (e.g., heart rate, systolic blood pressure,
diastolic blood pressure) to an acute psychosocial stress paradigm, and whether common
psychosocial factors (e.g., anxiety and depression) moderate the treatment response.
Hypothesis 1
In our study, participants were randomized to one of three intervention conditions.
The first experimental condition was developed based on Acceptance and Commitment
Therapy (ACT), a therapeutic approach that focuses on increasing one’s flexibility and
willingness to accept stressful and anxiety provoking events and feelings (Hayes et al.,
1999). ACT has proven empirical evidence for its effectiveness in treating a variety of
psychopathologies, including depression and anxiety, and has been shown to affect
positive cardiovascular outcomes (Cambell-Sills et al., 2008; Forman et al., 2007; Hayes
et al., 2004; Low et al., 2008; Woods et al., 2006; Zettle, 2003; Zettle & Hayes, 1986;
Zettle & Rains, 1989).
The second experimental condition was Autogenic Training (AT), a self-
relaxation procedure that involves a series of statements aimed at reducing autonomic
arousal (Linden, 1990). AT has shown clinical main effects in the range of medium-to-
large effect sizes in both nonclinical and clinical populations. For example, a number of
studies have shown AT to be a beneficial for the reduction of anxiety and depressive
symptoms, as well as a variety of cardiovascular outcomes, such as heart rate and blood
BRIEF CLINICAL INTERVENTIONS 39
pressure (Kanji, 2004a; Kanji, 2004b; Krampen, 1999, Farne & Gnugnoli, 2000; Stetter
& Kupper, 2002). The third condition, an Attention-only Control group, involved joining
with a research assistant to read an interactive adventure book.
Based on literature demonstrating the positive benefits relaxation and acceptance
techniques have on health outcomes, we hypothesized that brief interventions would have
differential effects on heart rate, systolic blood pressure, and diastolic blood pressure
following a psychosocial stress paradigm. Specifically, we thought the ACT and AT
experimental conditions would attenuate the stress response, resulting in positive
cardiovascular outcomes (e.g., lower reactivity and greater recovery following the TSST).
Further, because we were measuring acute physiological outcomes, we hypothesized that
the AT condition, being a somatic relaxation technique, would be superior to the ACT
condition, and that both experimental conditions would be superior to the Attention-only
Control condition. In support of our hypothesis, results showed a time by group
interaction for heart rate and diastolic blood pressure, indicating that brief interventions
differentially affected heart rate and diastolic blood pressure over time. However, after
controlling for relevant covariates, particularly baseline differences in heart rate and
diastolic blood pressure, these effects were no longer evident. Additionally, contrary to
our hypothesis, we did not observe any effects on systolic blood pressure.
One way of interpreting our results is to suggest that the original time by group
interactions for both heart rate and diastolic blood pressure were driven by baseline
differences between groups. However, another interpretation is that intervention effects,
which could no longer be measured after controlling for baseline time points, drove our
results. For example, in regards to heart rate outcomes, there was a greater reduction in
BRIEF CLINICAL INTERVENTIONS 40
heart rate from baseline to pre-TSST in the AT group compared to the ACT and Control
groups. This suggests that there was a greater intervention effect for the AT group
compared to the other groups. However, because we had to control for baseline
differences in subsequent analyses, and therefore remove time 1, the intervention effect
could no longer be displayed. Therefore, it may be that the observed time by group
interaction was in fact due to the AT intervention effect rather than baseline differences
in heart rate.
In regards to diastolic blood pressure, the same interpretations must be
considered. Again, it may be that the group by time interaction was driven by baseline
differences in diastolic blood pressure. However, another possibility is that intervention
effects, which could no longer be measured after controlling for baseline time points,
drove our results. On further examination, the AT group again showed a significant
intervention effect compared to the ACT and Control groups, which was evidenced by a
lowering of diastolic blood pressure from baseline to pre-TSST. However, because we
had to control for baseline differences in subsequent analyses, and therefore remove time
1, this effect could no longer be demonstrated. Therefore, as with heart rate, it may be
that the intervention effects of the AT group rather than baseline differences in diastolic
blood pressure drove the observed time by group interaction.
Hypothesis 1a
Our second hypothesis was that anxiety and depressive symptomatology would
moderate the treatment response. This hypothesis was more exploratory in nature since
there is no literature, to our knowledge, investigating whether psychosocial factors
moderate cardiovascular outcomes to brief clinical interventions.
BRIEF CLINICAL INTERVENTIONS 41
We hypothesized that anxiety and depression levels would moderate the treatment
response to brief clinical interventions. In regards to depressive symptomatology and
systolic blood pressure, our hypotheses were supported. Results showed a significant
three-way interaction indicating that across time points, SBP was affected differently
among intervention groups depending on level of depression. Within the Autogenic
Training group, subjects with higher levels of depressive symptomatology had lower SBP
reactivity to the TSST than those with less symptomatology. There were no significant
differences between levels of depression in SBP reactivity, recovery, or across any time
points within either the ACT or Control conditions. This finding provides evidence that
AT may be most beneficial for individuals with higher levels of depression. Once
relevant covariates were controlled for, the three-way interaction was no longer
significant (p = .06).
In regards to social anxiety symptomatology and systolic and diastolic blood
pressure, our hypotheses were also supported. Results showed a significant three-way
interaction indicating that across time points, after controlling for all relevant covariates,
SBP was affected differently among intervention groups depending on level of social
anxiety. Within the AT group, subjects with higher levels of social anxiety
symptomatology had greater SBP recovery following the TSST than those with less
symptomatology. Additionally, within the AT group, subjects with higher levels of
social anxiety symptomatology had significantly lower SBP than those with less
symptomatology at time 4. There were no significant differences between levels of social
anxiety in SBP reactivity, recovery, or across any time points within either the
Acceptance and Commitment Therapy or Control conditions. Overall, this finding

BRIEF CLINICAL INTERVENTIONS 42
provides evidence that AT may be most beneficial for individuals with higher levels of
social anxiety.
Additionally, results showed a significant three-way interaction indicating that
across time points, DBP is affected differently among intervention groups depending on
level of social anxiety. This finding held after controlling for baseline differences in
diastolic blood pressure. Within the AT group, subjects with higher levels of social
anxiety symptomatology had greater DBP recovery following the TSST than those with
less symptomatology. There were no significant differences between levels of social
anxiety in DBP reactivity, recovery, or across any time points within either the ACT or
Control conditions. This finding also provides evidence that AT may be beneficial for
individuals with higher levels of social anxiety. However, once other relevant covariates
were controlled for along with baseline DBP, the three-way interaction was no longer
significant (p = .056).
In sum, our results show that depressive and social anxiety symptomatology
moderated the effectiveness of our brief clinical interventions, as measured by
cardiovascular outcomes. Analyzing these findings together it is evident that subjects
with greater levels of social anxiety and those with greater levels of depressive symptoms
benefited more from the Autogenic Training intervention than those with lower levels. It
is an interesting finding that individuals with higher levels of psychopathology showed
greater cardiovascular benefits from AT. Because the intervention was brief, and
therefore less potent than if it had been practiced on several occasions, some may have
expected individuals with lower levels of psychopathology to benefit the most from it.
One interpretation for our findings is that nonclinical subjects with greater social
BRIEF CLINICAL INTERVENTIONS 43
anxiety (and depression) were more motivated to participate in the intervention, and thus,
learned and benefited more from it, thereby affecting cardiovascular outcomes. There is
a vast literature on the importance of motivation for the acquisition and transfer of
techniques and skills taught in psychosocial interventions (see Ryan et al., 2011 for a
review). In fact, motivation has been found to be so important for learning and transfer
that an empirically supported directive therapeutic style, Motivational Interviewing, has
been developed to focus on helping patients increase it (Miller, 1983; Miller & Rollnick,
1991; Miller & Rollnick, 2002; Hettema, Steele, & Miller, 2005). Based on motivational
theories (e.g., Self-Determination Theory; Deci & Ryan, 1985), it is reasonable that
individuals with greater intrinsic motivation, perhaps those with more symptoms of
psychopathology, would be more likely to fully engage in a brief version of Autogenic
Training, which is directly aimed at reducing the symptoms they are experiencing.
Hypothesis 1b
As discussed in the introduction, current research has shown mixed results for the
effects depression and anxiety have on physiological stress reactions. For example,
studies investigating physiological responses to acute psychosocial stressors have
suggested that depression and anxiety are related to enhanced cardiovascular reactivity,
as evidenced by increased blood pressure and heart rate (de Rooij et al., 2010; Kibler &
Ma, 2004; Mausbach et al., 2005). However, other researchers have found negative
associations implicating a hyporeactivity to acute psychosocial stress (Carroll et al.,
2007; Jezova et al., 2004; Salomon et al., 2009). In addition, it is important to note that
there is a lack of research investigating the relationship between depressive and anxiety

BRIEF CLINICAL INTERVENTIONS 44
symptomatology and cardiovascular recovery, rather most studies concentrate on
reactivity.
Our study design offered an opportunity for us to add to the literature regarding
the possible associations between certain key psychosocial factors and cardiovascular
reactivity and recovery. Based on prior research, we hypothesized that after controlling
for treatment group, anxiety and depressive symptomatology would be associated with
greater cardiovascular reactivity and lower recovery following the TSST. Our hypothesis
was partially supported in that heart rate reactivity was found to be positively associated
with anxiety sensitivity (as measured by total score on the ASI). However, no additional
measures were associated with any other cardiovascular parameters.
In our study, mean scores for all four measures (BDI-II, ASI, LSAS, STAI-Trait)
were all in the nonclinical range. Therefore, one interpretation of these results is that
certain associations were not observed because our study included a nonclinical
population that displayed subthreshold symptomatology. Our results imply that lower
levels of psychopathology (i.e., a few symptoms of anxiety or depression), although
meaningful, may not affect physiological parameters as drastically as more severe
pathology.
In further discussion of our results, we did not specifically study individual
differences in regards to psychopathology. For example, a biological predisposition to
certain disorders may engender more physiological effects. Additionally, certain
symptoms of anxiety and depression may elicit cardiovascular responses (e.g.,
somatic/physical symptoms) more than others (e.g., cognitive/affective symptoms). It is
also reasonable to ascertain that age of onset and length of time experiencing certain
BRIEF CLINICAL INTERVENTIONS 45
pathology may have more or less of an effect on physiological parameters.
Unfortunately, because we did not directly study these types of individual differences, we
were not able to test these possibilities. Therefore, one important implication of our
study is that direct consideration of individual differences when investigating
physiological outcomes is imperative.
Limitations
Although there are many strengths of this study, such as its novelty, there are
some important limitations to mention. First, although our subjects were randomly
assigned to groups, there were still baseline differences in two of three cardiovascular
parameters. This indicates that our baseline data might represent anticipation stress
rather than a true baseline condition. Therefore, future research utilizing a similar study
design should take baseline anticipation stress into consideration by adequately
measuring and treating it as a confounding factor. Second, we did not measure
cardiovascular parameters during the TSST; rather we assessed reactivity immediately
following the cessation of the protocol. Although this method has been utilized in
various studies, assessing cardiovascular parameters during the TSST may provide a
more valid measure of reactivity. Third, because of our sample population and sample
size of men, we were not able to investigate possible age and gender differences in
treatment response. Several studies (e.g., Kelly, Tyrka, Anderson, Price, Carpenter,
2008; Kudielka et al, 2004a) have found age and gender differences in responses to social
stress challenges. Therefore, exploring age and gender differences in treatment response
involving objective outcome measures is warranted. Lastly, we did not directly measure
BRIEF CLINICAL INTERVENTIONS 46
motivation and treatment engagement, which can both be considered as possible
confounds decreasing intervention effectiveness.
Future Directions
There is a growing awareness of the detrimental health effects stress has on
individuals. This awareness has led to research endeavors investigating the exact
pathways linking stress and health. Just as important as elucidating these mechanisms,
there is also a need for the development and study of specific interventions to counteract
the effects of stress. Our study has specifically added to this field by showing that brief
clinical interventions involving somatic relaxation, particularly Autogenic Training, may
be beneficial to individuals undergoing acute stress. Additionally, our study
demonstrated that individuals with higher levels of depression and/or anxiety might
benefit the most from these targeted interventions.
Particularly within the field of behavioral medicine, our findings offer important
implications for assessment and treatment. Acute physiological reactivity from stressful
medical and dental procedures is common and may lead to negative outcomes (Cohen,
Fiske, & Newton, 2000; Johnsen et al., 2003; Munafo & Stevenson, 2001; Mavros et al.,
2011; Pignay-Demaria, Lesperance, Demaria, Frasure-Smith, & Perrault, 2003).
Moreover, it is well evidenced that mild and severe forms of anxiety and depressive
disorders are high in medical and dental patient populations and are considered risk
factors for disease (Demertizis & Craske 2006; Moussavi et al., 2007; Sherbourne,
Jackson, Meredith, Camp, & Wells, 1996; Stoudemire, 1996; Wittchen et al., 2002).
Targeting certain individuals more prone to poor outcomes (e.g., those suffering from
mild or severe psychopathology) and administering brief clinical interventions prior to
BRIEF CLINICAL INTERVENTIONS 47
stressful procedures may attenuate and/or prevent negative health outcomes. Future
research investigating the effectiveness brief clinical interventions have on these
populations is not only warranted, but highly feasible.
BRIEF CLINICAL INTERVENTIONS 48
References
Aivazyan, T., Zaitsev, V., & Yurenev, A. (1988). Autogenic training in the treatment and
secondary prevention of essential hypertension: Five-year follow-up. Health
Psychology, 7(Suppl.), 201-8.
al’Absi, M., & Arnett, D. (2000). Adrenocortical responses to psychological stress and
risk for hypertension. Biomedical Pharmacotherapy, 54, 234-44.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders, (Rev. 4th ed.). Washington, DC.
Armario, P., del Rey, R., Martin-Baranera, M., Almendros, M., Ceresuela, L., & Pardell,
H. (2003). Blood pressure reactivity to mental stress task as a determinant of
sustained hypertension after 5 years of follow-up. Journal of Human
Hypertension, 17, 181-6.
Bach, P., & Hayes, S. (2002). The use of acceptance and commitment therapy to prevent
the rehospitalization of psychotic patients: A randomized controlled trial. Journal
of Consulting and Clinical Psychology, 70, 1129-39.
Baker, S., Heinrichs, N., Kim, H., & Hofman, S. (2002). The Liebowitz social anxiety
scale as a self-report instrument: A preliminary psychometric analysis. Behavior
Research and Therapy, 40, 701-15.
Beck, A., Steer, R., & Brown, G. (1996). Manual for the Beck Depression Inventory (2nd
edition). San Antonio, TX: Psychological Corporation.
Beck, A., Steer, R., Ball, R., & Ranieri, W. (1996). Comparison of Beck Depression
Inventories IA and II in psychiatric outpatients. Journal of Personality
Assessment, 67, 588-97.
BRIEF CLINICAL INTERVENTIONS 49
Black, P., & Garbutt, L. (2002). Stress, inflammation and cardiovascular disease. Journal
of Psychosomatic Research, 52, 1-23.
Block, J. (2002). Acceptance or change of private experiences: A comparative analysis in
college students with public speaking anxiety. Doctoral dissertation. University at
Albany, State University of New York.
Bond, F., & Bunce, D. (2003). The role of acceptance and job control in mental health,
job satisfaction, and work performance. Journal of Applied Psychology, 88, 1057-
67.
Brosschot, J., Gerin, W., & Thayer, J. (2006). The perseverative cognition hypothesis: A
review of worry, prolonged stress-related physiological activation, and health.
Journal of Psychosomatic Research, 60, 113–24.
Brotman, D., Golden, S., & Wittstein, I (2007). The cardiovascular toll of stress. Lancet,
370, 1089-100.
Campbell-Sills, L., Barlow, D., Brown, T., & Hofmann, S., (2006). Effects of
suppression and acceptance on emotional responses of individuals with anxiety
and mood disorders. Behaviour Research and Therapy, 44, 1251-63.
Carroll, D., Phillips, A., Hunt, K., & Der, G. (2007). Symptoms of depression and
cardiovascular reactions to acute psychological stress: Evidence from a
population study. Biological Psychiatry, 75, 68-74.
Chida, Y., & Hamer, M. (2008). Chronic psychosocial factors and acute physiological
responses to laboratory-induced stress in healthy populations: A quantitative
review of 30 years of investigations. Psychological Bulletin, 134, 829-85.
BRIEF CLINICAL INTERVENTIONS 50
Childs, E., Vicini, L., & De Wit, H. (2006). Responses to the Trier Social Stress Test
(TSST) in single and grouped participants. Psychophysiology, 43, 366-71.
Chrousos, G. (2009). Stress and disorders of the stress system. Nature Reviews
Endocrinology, 5, 374-81.
Chrousos, G., Gold, P. (1992). The concepts of stress and stress system disorders:
Overview of physical and behavioral homeostasis. Journal of the American
Medical Association, 267, 1244-52.
Clark, M., Bond, M., & Hecker, J. (2007). Environmental stress, psychological stress and
allostatic load. Psychology, Health & Medicine, 12, 18-30.
Cohen, S., Fiske, J., & Newton, J. (2000). Behavioral Dentistry: The impact of dental
anxiety on daily living. British Dental Journal, 189, 385-90.
Cowings, P., Toscano, W., Timbers, A., Casey, C., & and Hufnagel, J. (2005). Autogenic
feedback training exercise: A treatment for airsickness in military pilots. The
International Journal of Aviation Psychology, 15, 395-412.
de Rooij, S., Schene, A., Phillips, D., & Roseboom, T. (2010). Depression and anxiety:
Associations with biological and perceived stress reactivity to a psychological
stress protocol in a middle-aged population. Psychoneurendocrinology, 35, 866-
77.
Deci, E., & Ryan, R. (1985). Intrinsic motivation and self-determination in human
behavior. New York: Plenum Publishing Co.
Demertizis, K., & Craske, M. (2006). Anxiety in primary care. Current Psychiatry
Reports, 8, 291-7.
BRIEF CLINICAL INTERVENTIONS 51
Dickerson, S., & Kemeny, M. (2004). Acute stressors and cortisol responses: A
theoretical integration and synthesis of laboratory research. Psychological
Bulletin, 130, 355-91.
Epel, E., Lin, J., Wilhelm, F., Wolkowitz, O., Cawthon, R., Adler, N., … Blackburn, E.
(2006). Cell aging in relation to stress arousal and cardiovascular disease risk
factors. Psychoneuroendocrinology, 31, 277-87.
Farne, M., & Gnugnoli, D. (2000). Effects of autogenic training on emotional distress
symptoms. Stress Medicine, 16, 259-61.
Forman, E., Herbert, J., Moitra, E., Yeomans, P., & Geller, P. (2007). A randomized
controlled effectiveness trial of Acceptance and Commitment Therapy and
Cognitive Therapy for anxiety and depression. Behavior Modification, 31, 772-
99.
Fresco, D., Coles, M., Heimberg, R., Liebowitz, M., Hami, S., Stein, M., & Goetz, D.
(2001). The Liebowitz Social Anxiety Scale: A comparison of the psychometric
properties of self-report and clinician-administered formats. Psychological
Medicine, 31, 1025-35.
Gifford, E., Kohlenberg, B., Hayes, S., Antonuccio, D., Piasecki, M., Rasmussen-Hall,
M., & Palm, K. (2004). Acceptance theory-based treatment for smoking
cessation: An initial trial of acceptance and commitment therapy. Behavior
Therapy, 35, 689-706.
Glassman, A., & Shapiro, P. (1997). Depression and the course of coronary artery
disease. American Journal of Psychiatry, 155, 4-11.

BRIEF CLINICAL INTERVENTIONS 52
Greenhouse, S., & Geisser, S. 1959. On methods in the analysis for profile data.
Psychometrica, 24, 95–112.
Gregg, J., Callaghan, G., Hayes, S., Glenn-Lawson, J. (2007). Improving diabetes self-
management through acceptance, mindfulness, and values: A randomized
controlled trial. Journal of Consulting and Clinical Psychology, 75, 336-43.
Hayes, S., Barnes-Holmes, D., & Roche, B. (2001). Relational Frame Theory: A Post-
Skinnerian Account of Human Language and Cognition. New York, NY: Kluwer.
Hayes, S., Luoma, J., Bond, F., Masuda, A., & Lillis, J. (2006). Acceptance and
Commitment Therapy: Model, processes and outcomes. Behaviour Research and
Therapy, 44, 1-25.
Hayes, S., Masuda, A., Bissett, R., Luoma, J., & Guerrero, J. (2004). DBT, FAP, and
ACT: How empirically oriented are the new behavior therapy technologies?
Behavior Therapy, 35, 35-54.
Hayes, S., Strosahl, K., & Wilson, K. (1999). Acceptance and Commitment Therapy: An
experiential approach to behavior change. New York: Guilford Press.
Hayes, S., Wilson, K., Gifford, E., Follette, V., & Strosahl, K. (1996). Experiential
avoidance and behavioral disorders: A functional dimensional approach to
diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64,
1152-68.
Hayes, S., Wilson, K., Gifford, E., Bissett, R., Piasecki, M., Batten, S., … Gregg, J.
(2004). A preliminary trial of twelve-step facilitation and acceptance and
commitment therapy with polysubstance-abusing methadone-maintained opiate
addicts. Behavior Therapy, 35,667-88.

BRIEF CLINICAL INTERVENTIONS 53
Hellhammer, J., & Schubert, M. (2012). The physiological response to Trier Social Stress
Test relates to subjective measures of stress during but not before or after the test.
Psychoneuroendocrinology, 37, 119-24.
Heopniemi, T., Elovainio, M., Pulkki, L., Puttonen, S., Raitakari, O., & Keltikangas-
Jarvinen, L. (2007). Cardiac autonomic reactivity and recovery in predicting
carotid atherosclerosis: The cardiovascular risk in young Finns study. Health
Psychology, 26, 13–21.
Herbert, C., & Gutman, G. (1983). Practical group autogenic training for management of
stress- related disorders in family practice. Canadian Family Physician, 29, 109-
17.
Hettema, J., Steele, J., & Miller, W. (2005). Motivational Interviewing. Annual Review of
Clinical Psychology, 1, 91-111.
Hidderley, M., & Holt, M. (2004). A pilot randomized trial assessing the effects of
autogenic training in early stage cancer patients in relation to psychological status
and immune system responses. European Journal of Oncology Nursing, 8, 61-5.
Hocking Schuler, J., & O’Brien, W. (1997). Cardiovascular recovery from stress and
hypertension risk factors: A meta-analytic review. Psychophysiology, 34, 649-59.
Holmes, T., & Rahe, R. (1967). The social readjustment rating scale. Journal of
Psychosomatic Research, 11, 213-8.
Jezova, D., Makatsori, A., Duncko, R., Moncek, F., & Jakubek, M. (2004). High trait
anxiety in healthy subjects is associated with low neuroendocrine activity during
psychosocial stress. Progress in Neuropsychopharmacology & Biological
Psychiatry, 28, 1331-6.
BRIEF CLINICAL INTERVENTIONS 54
Johnsen, B., Thayer, J., Laberg, J., Wormnes, B., Raadal, M., Skaret,
E., … Berg., E.
(2003). Attentional and physiological characteristics of patients with dental
anxiety. Journal of Anxiety Disorders, 17, 75-87.
Jonsson, P., Wallergard, M., Osterberg, K., Hansen, A., Johansson, G., & Karlson, B.
(2010). Cardiovascular and cortisol reactivity and habituation to a virtual reality
version of the Trier Social Stress Test: A pilot study. Psychoneuroendocrinology,
35, 1397-403.
Juster, R., Marin, M., Sindi, S., Nair, V., Ng, Y., Pruessner, J., Lupien, S. (2011).
Allostatic load associations to acute, 3-year and 6-year prospective depressive
symptoms in healthy older adults. Physiology & Behavior, 104, 360-4.
Kanji, N. (1997). Autogenic Training. Complementary Therapies in Medicine, 5, 162-7.
Kanji, N., White, A., & Ernst, E. (2004a). Autogenic training to reduce anxiety in nursing
students: Randomized controlled trial. Journal of Advanced Nursing, 53, 729-35.
Kanji, N., White, M., & Ernst, E. (2004b). Autogenic training reduces anxiety after
coronary angioplasty: A randomized clinical trial. American Heart Journal, 147,
e10.
Kanji, N., White, M., & Ernst, E. (2006). Autogenic training for tension type headaches:
A systematic review of controlled trials. Complementary Therapies in Medicine,
14, 144-50.
Kelly, M., Tyrka, A., Anderson, J., Price, L., Carpenter, L. (2008). Sex differences in
emotional and physiological responses to the Trier Social Stress Test. Journal of
Behavior Therapy and Experimental Psychiatry, 39, 87-98.
BRIEF CLINICAL INTERVENTIONS 55
Kessler, R. (1997). The effects of stressful life events on depression. Annual Review of
Psychology, 48, 191-214.
Kibler, J., & Ma, M. (2004). Depressive symptoms and cardiovascular reactivity to
behavioral stress. International Journal of Behavioral Medicine, 11, 81-7.
Kiecolt-Glaser, J., McGuire, L., Robles, T., & Glaser, R. (2002). Emotions, morbidity,
and mortality: New perspectives from psychoneuroimmunology. Annual Review
of Psychology, 53, 83-107.
Kirschbaum, C., Pirke, K., Hellhammer, D. (1993). The ‘‘Trier Social Stress Test’’- a
tool for investigating psychobiological stress responses in a laboratory setting.
Neuropsychobiology, 28, 76-81.
Krampen, G. (1999). Long-term evaluation of the effectiveness of additional autogenic
training in the psychotherapy of depressive disorders. European Psychologist, 4,
11-8.
Kubzansky, L., Kawachi, I., Weiss, S., Sparrow, D. (1998). Anxiety and coronary heart
disease: A synthesis of epidemiological, psychological, and experimental
evidence. Annals of Behavioral Medicine, 20, 47-58.
Kudielka, B., Buske-Kirschbaum, A., Hellhammer, D., & Kirschbaum, C. (2004a).
Differential heart rate reactivity and recovery after psychosocial stress (TSST) in
health children, younger adults, and elderly adults: The impact of age and gender.
International Journal of Behavioral Medicine, 11, 116-21.
Kudielka, B., Wust, S., Kirschbaum, C., & Hellhammer, D. (2007). The Trier Social
Stress Test (TSST). In G. Fink, Ed., Encyclopedia of stress (2nd
ed.). San Diego:
Academic Press.

BRIEF CLINICAL INTERVENTIONS 56
Labbe, E. (1995). Treatment of childhood migraine with autogenic training and skin
temperature biofeedback: A component analysis. Headache, 35, 10-3.
Lazarus, R., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
Liebowitz, M. (1987). Social Phobia. Modern Problems of Pharmacopsychiatry, 22, 141-
73.
Linden, W. (1990). Autogenic training. New York: Guilford Press.
Logan, J., & Barksdale, D. (2008). Allostasis and allostatic load: expanding the discourse
on stress and cardiovascular disease. Journal of Clinical Nursing, 17, 201-8.
Low, C., Stanton, A., & and Bower, J. (2008). Effects of acceptance-oriented versus
evaluative emotional processing on heart rate recovery and habituation. Emotion,
8, 419-24.
Lundgren, T., Dahl, J., & Hayes, S. (2008). Evaluation of mediators of change in the
treatment of epilepsy with Acceptance and Commitment Therapy. Journal of
Behavioral Medicine, 31, 225-35.
Luthar, S. (Ed.). (2003). Resilience and vulnerability: adaptation in the context of
childhood adversities. New York: Cambridge University Press.
Luthe, W. (1969-1973). Autogenic therapy (Vol. I-VI). New York, NY: Grune &
Stratton.
Maller, R., & Reiss, S. (1987). A behavioral validation of the Anxiety Sensitivity Index
Journal of Anxiety Disorders, 1, 256-272.
Maller, R., & Reiss, S. (1992). Anxiety sensitivity in 1984 and panic disorder in 1987.
Journal of Anxiety Disorders, 6, 241-247.

BRIEF CLINICAL INTERVENTIONS 57
Mausbach, B., Dimsdale, J., Ziegler, M., Mills, P., Ancoli-Israel, S., Patterson, T., &
Grant, I. (2005). Depressive symptoms predict norepinephrine response to a
psychological stressor task in alzheimer’s caregivers. Psychosomatic Medicine,
67, 638-42.
Mavros, M., Athanasiou, S., Gkegkes, I., Polyzos, K., Peppas, G., & Falagas, M. (2011).
Do psychological variables affect early surgical recovery? PLoS One, 6, 1-6.
McCracken, L., & Eccleston, C. (2006). A comparison of the relative utility of coping
and acceptance-based measures in a sample of chronic pain sufferers. European
Journal of Pain, 10, 23-9.
McEwen, B. (1998). Protective and damaging effects of stress mediators. New England
Journal of Medicine, 338, 171-9.
McEwen, B. (2000). Allostasis and allostatic load: Implications for
neuropsychopharmacology. Neuropsychopharmacology, 22, 108-24.
McEwen, B. (2002) Sex, stress and the hippocampus: allostasis, allostatic load and the
aging process. Neurobiology of Aging, 23, 921-39.
McEwen, B. (2003). Mood Disorders and allostatic load. Biological Psychiatry, 201,
200-7.
McEwen, B. (2004) Protection and damage from acute and chronic stress: allostasis and
allostatic overload and relevance to the pathophysiology of psychiatric disorders.
Annals of the New York Academy of Sciences, 1032, 1-7.
McEwen, B. (2007). Physiology and neurobiology of stress and adaptation: Central role
of the brain. Physiological Reviews, 87, 873-904.
BRIEF CLINICAL INTERVENTIONS 58
McEwen, B., & Stellar, E. (1993). Stress and the individual. Archives of Internal
Medicine, 153, 2093-101.
Miller, W. (1983). Motivational interviewing with problem drinkers. Behavioral
Psychotherapy, 11, 147-72.
Miller, W., & Rollnick, S. (1991). Motivational Interviewing: Preparing People to
Change Addictive Behavior. New York: Guilford.
Miller, W., & Rollnick, S. (2002). Motivational Interviewing: Preparing People for
Change, Vol. 2. New York: Guilford.
Morgan, A., & Jorm, A. (2008). Self-help interventions for depressive disorders and
depressive symptoms: A systematic review. Annals of General Psychiatry, 7, 13.
Moussavi, S., Chatterji, S., Verdes, E., Tandon, A., Patel, V., & Ustun, B. (2007).
Depression, chronic diseases, and decrements in health: Results from the World
Health Surveys. Lancet, 370, 851–8.
Munafo, M., & Stevenson, J. (2001). Anxiety and surgical recovery: Reinterpreting the
literature. Journal of Psychosomatic Research, 51, 589-96.
Nater, U., Rohleder, N., Gaab, J., Berger, S., Jud, A., Kirschbaum, C., et al. (2005).
Human salivary alpha-amylase reactivity in a psychosocial stress paradigm.
International Journal of Psychophysiology, 55(3), 333-42.
Nugent, N., Tyrka, A., Carpenter, L., & Price, L. (2011). Gene-environment interactions:
Early life stress and risk for depressive and anxiety disorders.
Psychopharmacology, 214, 175-96.
Peterson, R., & Sacks, C. (1987). Predictors of reaction to self-reported panic attacks in
college students. Paper presented at the Association for Advancement of Behavior

BRIEF CLINICAL INTERVENTIONS 59
Therapy Convention, Boston, MA: November, 1987.
Pignay-Demaria, V., Lespérance, F., Demaria, R., Frasure-Smith, N., & Perrault, L.
(2003). Depression and anxiety and outcomes of coronary artery bypass surgery.
The Annals of Thoracic Surgery, 75, 314-21.
Reiss, S. (1991). Expectancy model of fear, anxiety, and panic. Clinical Psychology
Review, 11, 141-53.
Reiss, S., Peterson, R., & Gursky, D. (1988). Anxiety sensitivity, injury sensitivity, and
individual differences in fearfulness. Behavior Research and Therapy, 26, 341-
45.
Reiss, S., Peterson, R., Gursky, D., & McNally, R. (1986). Anxiety sensitivity, anxiety
frequency, and the prediction of fearfulness. Behavior Research and Therapy, 24,
1-8.
Rosamond, W., Flegal, K., Friday, G., Furie, K., Go, A., Greenlund, K.,… Hong Y.
(2007). Heart disease and stroke statistics - 2007 update: A report from the
American Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Circulation, 115, e69–171.
Ryan, R., Lynch, M., Vansteenkiste, M., & Deci, E. (2011). Motivation and autonomy in
counseling, psychotherapy, and behavior change: A look at theory and practice.
The Counseling Psychologist, 39, 193– 260.
Salomon, K., Clift, A., Karisdottir, M., & Rottenberg, J. (2009). Major depressive
disorder is associated with attenuated cardiovascular reactivity and impaired
recovery among those free of cardiovascular disease. Health Psychology, 28, 157-
65.
BRIEF CLINICAL INTERVENTIONS 60
Shinozaki, M., Kanazawa, M., Kano, M., Endo, Y., Nakaya, N., Hongo, M., & Fukudo,
S. (2010). Effect of Autogenic Training on General Improvement in Patients with
Irritable Bowel Syndrome: A Randomized Controlled Trial. Applied
Psychophysiological Biofeedback, 35, 189-98.
Schlamann, M., Naglatzki, R., de Greiff, A., Forsting, M., & Gizewski, E. (2010).
Autogenic Training alters cerebral activation patterns in fMRI. International
Journal of Clinical and Experimental Hypnosis, 58, 444-56.
Schulkin, J. (2004). Allostasis, homeostasis, and the costs of physiological adaptation.
Cambridge University Press, New York.
Schultz J. (1932) Autogenic Training. Thieme Verlag, Stuttgart.
Schultz, J., & Luthe, W. (1959). Autogenic training—A psychophysiological approach in
psychotherapy. New York: Grune & Stratton.
Seeman, T., Singer, B., Rowe, J., Horwitz, R., & McEwen, B. (1997). Price of
adaptation-allostatic load and its health consequences: MacArthur studies of
successful aging. Archives of Internal Medicine, 157, 2259-68.
Sherbourne, C., Jackson, C., Meredith, L., Camp, P., & Wells, K. (1996). Prevalence of
comorbid anxiety disorders in primary care outpatients. Archives of Family
Medicine, 5, 27-34.
Spielberger, C. (1983). Manual for the State-Trait Anxiety Inventory STAI (Form Y). Palo
Alto, CA: Mind Garden.
Spielberger, C., Gorsuch, R., & Lushene, R. (1970). STAI: Manual for the State-Trait
Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
BRIEF CLINICAL INTERVENTIONS 61
Sterling, P., & Eyer, J. (1988). Allostasis: A new paradigm to explain arousal pathology.
In S. Fisher & J. Reason (Eds.), Handbook of life stress, cognition and health (pp.
629 – 649). New York: John Wiley & Sons.
Stetter, F., & Kupper, S. (2002). Autogenic training: A meta-analysis of clinical outcome
studies. Applied Psychophysiology and Biofeedback, 27, 45-98.
Stoudemire, A. (1996). Epidemiology and psychopharmacology of anxiety in medical
patients. Journal of Clinical Psychiatry, 57, 73-5.
Sullivan, G., Coplan, J., Kent, J., & Gorman, J. (1999). The noradrenergic system in
pathological anxiety: A focus on panic with relevance to generalized anxiety and
phobias. Biological Psychiatry, 46, 1205-18.
Taylor, S., Seeman, T., Eisenberg, N., Kozanian, T., Moore, A., & Moons, W. (2010).
Effects of a supportive or an unsupportive audience on biological and
psychological responses to stress. Journal of Personality and Social Psychology,
98, 47-56.
Ter Kuile, M., Spinhoven, P., Linssen, A., Zitman, F., & Van Dyck, R. (1994). Autogenic
training and cognitive self-hypnosis for the treatment of recurrent headaches in
three different subject group. Pain, 58, 331-40.
Tsigos, C., & Chrousos, G. (2002). Hypothalamic-pituitary-adrenal axis, neuroendocrine
factors and stress. Journal of Psychosomatic Research, 53, 865-71.
Vasey, M., & Thayer, J. 1987. The continuing problem of false positives in repeated
measures ANOVA in psychophysiology: A multivariate solution.
Psychophysiology, 24, 479–86.
White, W., & Anwar, Y. (2001). Evaluation of the overall efficacy of the Omron office
BRIEF CLINICAL INTERVENTIONS 62
digital blood pressure HEM-907 monitor in adults. Blood Pressure Monitoring, 6,
107-10.
Williams, R., Hagerty, B., & Brooks, G. (2004). Trier Social Stress Test: A method for
use in nursing research. Nursing Research, 53, 277–280.
Wittchen, H., Kessler, R., Katja, B., Krause, P., Hofler, M., & Hoyer, J. (2002).
Generalized anxiety and depression in primary care: Prevalence, recognition, and
management. Journal of Clinical Psychiatry, 63, 24-34.
Woods, D., Wetterneck, C., & Flessner, C. (2006). A controlled evaluation of acceptance
and commitment therapy plus habit reversal for trichotillomania. Behaviour
Research and Therapy, 44, 639-56.
York, K., Hassan, M., Li, Q., Li, H., Fillingim, R., & Sheps, D. (2007). Coronary artery
disease and depression: Patients with more depressive symptoms have lower
cardiovascular reactivity during laboratory-induced mental stress. Psychosomatic
Medicine, 69, 521-8.
Yusef, S., Hawken, S., Ounpuu, S., Dans, T., Avezum, A., Lanas, F., … Lisheng, L.
(2004). Effect of potentially modifiable risk factors associated with
myocardial infarction in 52 countries (the INTERHEART study): case-control
study. Lancet, 364, 937-52.
Zettle, R. (2003). Acceptance and commitment therapy (ACT) vs. systematic
desensitization in treatment of mathematics anxiety. Psychological Record, 53,
197-215.
Zettle, R., & Hayes, S. (1986). Dysfunctional control by client verbal behavior: The
context of reason giving. Analysis of Verbal Behavior, 4, 30-8.

BRIEF CLINICAL INTERVENTIONS 63
Zettle, R., & Rains, J. (1989). Group cognitive and contextual therapies in treatment of
depression. Journal of Clinical Psychology, 45, 436-45.
Zsombok, T., Juhasz, G., Buravari, A., Vitrai, J., & Bagdy, G. (2003). Effect of autogenic
training on drug consumption in patients with primary headache: An 8-month
follow-up study. Headache, 43, 251-7.

BRIEF CLINICAL INTERVENTIONS 64
Appendix A. Diagram of Participant Involvement in Larger Study
Time 2 (~45 mins)
Pre-Trier Assessment
(~30 mins)
-Physiological
Measures
-Process Measures
Trier Social Stress Test
(~15 mins)
-Instructions
-Anticipation
-Free Speech
-Subtraction
Time 3 (~60 mins)
Post-Trier Assessment
(~20 mins)
-Physiological
Measures
-Process Measures
Debriefing (~15 mins)
Rest Period (~15 mins)
-Physiological
Measures
Wrap Up (~10 mins)
-Questions
Time 1 (~75 mins)
Informed Consent
(~15 mins)
Baseline Assessment (~40
mins)
-Physiological
Measures
-Psychological
Measures
Intervention Sessions
(~20 mins)
-Group 1: ACT
-Group 2: AT
-Group 3: Control

BRIEF CLINICAL INTERVENTIONS 65
Table 1
Participant Characteristics by Group
ACT AT Control Total n
n
40
40
40
120
120
Age (SD)
19.32 (1.16)
18.95 (.90)
18.95 (.96)
19.08 (1.02)
120
Mental Health
Condition (%) 6 (15%) 8 (20%) 3 (7.5%) 17 (14.2%) 120
Medical
Condition (%) 2 (5%) 4 (10%) 3 (7.5%) 9 (7.5%) 120
Daily Medication
(%)
12 (30%)
11 (27.5%)
10 (25%)
33 (27.5%)
120
Illicit Drug Use
(%)b,c
7 (17.5%)
5 (12.5%)
4 (10%)
16 (13.3%)
120
Cigarette Smoker
(%)
2 (5%)
4 (10%)
0
6 (5%)
120
BMI (kg/m2)b,c
23.73 (4.59) 23.16 (3.83) 23.43 (3.67) 23.44 (4.03)
119
Physical Exercise
(%)a
21 (52.5%)
23 (57.5%) 22 (55%) 66 (55%) 120
Race and Ethnicity
White
Black
Asian
Hispanic
Biracial/Multiracial
25 (62.5%)
5 (12.5%)
4 (10%)
6 (15%)
0
28 (70%)
5 (12.5%)
6 (15%)
1 (2.5%)
0
26 (65%)
3 (7.5%)
4 (10%)
5 (12.5)
2 (5%)
79 (65.8%)
13 (10.8%)
14 (11.7%)
12 (10%)
2 (1.7%)
120
Consume Alcohol
(%)b
22 (55%)
23 (57.5%)
24 (60%)
69 (67.5%)
120
Time of Daya
AM (9-12 PM)
Early PM (12-3 PM)
Late PM (3-6 PM)
16 (40%)
9 (22.5%)
15 (37.5%)
8 (20%)
22 (55%)
10 (25%)
11 (27.5%)
15 (37.5)
14 (35%)
35 (29.2%)
46 (38.3%)
39 (32.5)
120
aCorrelates with baseline HR (p ≤ 0.1);
bCorrelates with baseline SBP (p ≤ 0.1);
cCorrelates with baseline DBP (p ≤ 0.1)

BRIEF CLINICAL INTERVENTIONS 66
Table 2
Participant Characteristics by Gender
Male Female All n
n
40
80
120
120
Age (SD)
18.98 (1.03)
19.13 (1.02)
19.08 (1.02)
120
Mental Health
Condition (%)
3 (7.5%)
14 (17.5%)
17 (14.2%)
120
Medical
Condition (%)
2 (5.0%)
7 (8.8%)
9 (7.5%)
120
Daily Medication (%)
6 (15.0%)
27 (33.8%)
33 (27.5%)
120
Illicit Drug Use (%)b,c
9 (22.5%)
7 (8.8%)
16 (13.3%)
120
Cigarette Smoker (%)
2 (5.0%)
4 (5.0%)
6 (5.0%)
120
BMI (kg/m2)b,c
23.55 (4.04)
23.39 (4.04)
23.44 (4.02)
119
Physical Exercise (%)a
26 (65.0%)
40 (50.0%)
66 (55.0%)
120
Race and Ethnicity
White
Black
Asian
Hispanic
Biracial/Multiracial
30 (75.0%)
2 (5.0%)
6 (15.0%)
1 (2.5%)
1 (2.5%)
51 (63.75%)
13 (16.25%)
8 (10.0%)
7 (8.75%)
1 (1.25%)
81 (67.5%)
15 (12.5%)
14 (11.7%)
8 (6.6%)
2 (1.6%)
120
Consume Alcohol (%)b
26 (65.0%)
43 (53.8%)
69 (57.5%)
120
Time of Daya
AM (9-12 PM)
Early PM (12-3 PM)
Late PM (3-6 PM)
12 (30%)
16 (40%)
12 (30%)
23 (28.7%)
30 (37.5%)
27 (33.8%)
35 (29.2%)
46 (38.3%)
39 (32.5%)
120
aCorrelates with baseline HR (p ≤ 0.1);
bCorrelates with baseline SBP (p ≤ 0.1);
cCorrelates with baseline DBP (p ≤ 0.1)
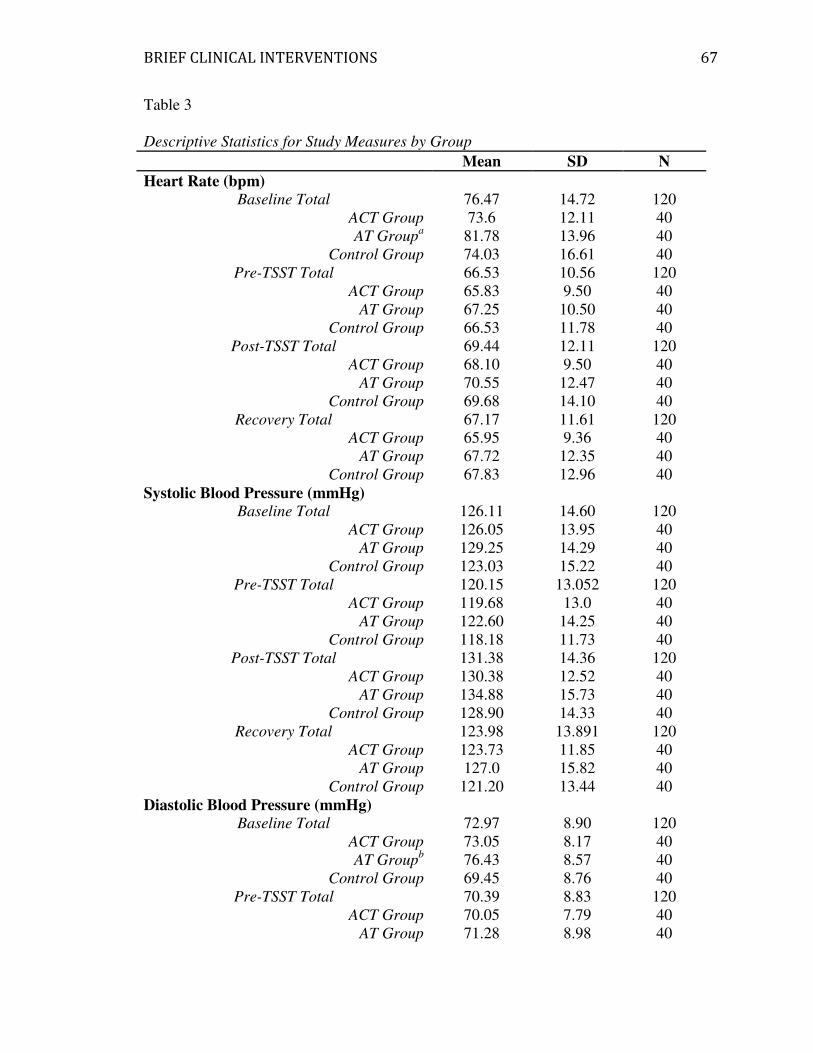
BRIEF CLINICAL INTERVENTIONS 67
Table 3
Descriptive Statistics for Study Measures by Group
Mean SD N
Heart Rate (bpm)
Baseline Total
ACT Group
AT Groupa
Control Group
76.47
73.6
81.78
74.03
14.72
12.11
13.96
16.61
120
40
40
40
Pre-TSST Total
ACT Group
AT Group
Control Group
66.53
65.83
67.25
66.53
10.56
9.50
10.50
11.78
120
40
40
40
Post-TSST Total
ACT Group
AT Group
Control Group
69.44
68.10
70.55
69.68
12.11
9.50
12.47
14.10
120
40
40
40
Recovery Total
ACT Group
AT Group
Control Group
67.17
65.95
67.72
67.83
11.61
9.36
12.35
12.96
120
40
40
40
Systolic Blood Pressure (mmHg)
Baseline Total
ACT Group
AT Group
Control Group
126.11
126.05
129.25
123.03
14.60
13.95
14.29
15.22
120
40
40
40
Pre-TSST Total
ACT Group
AT Group
Control Group
120.15
119.68
122.60
118.18
13.052
13.0
14.25
11.73
120
40
40
40
Post-TSST Total
ACT Group
AT Group
Control Group
131.38
130.38
134.88
128.90
14.36
12.52
15.73
14.33
120
40
40
40
Recovery Total
ACT Group
AT Group
Control Group
123.98
123.73
127.0
121.20
13.891
11.85
15.82
13.44
120
40
40
40
Diastolic Blood Pressure (mmHg)
Baseline Total
ACT Group
AT Groupb
Control Group
72.97
73.05
76.43
69.45
8.90
8.17
8.57
8.76
120
40
40
40
Pre-TSST Total
ACT Group
AT Group
70.39
70.05
71.28
8.83
7.79
8.98
120
40
40
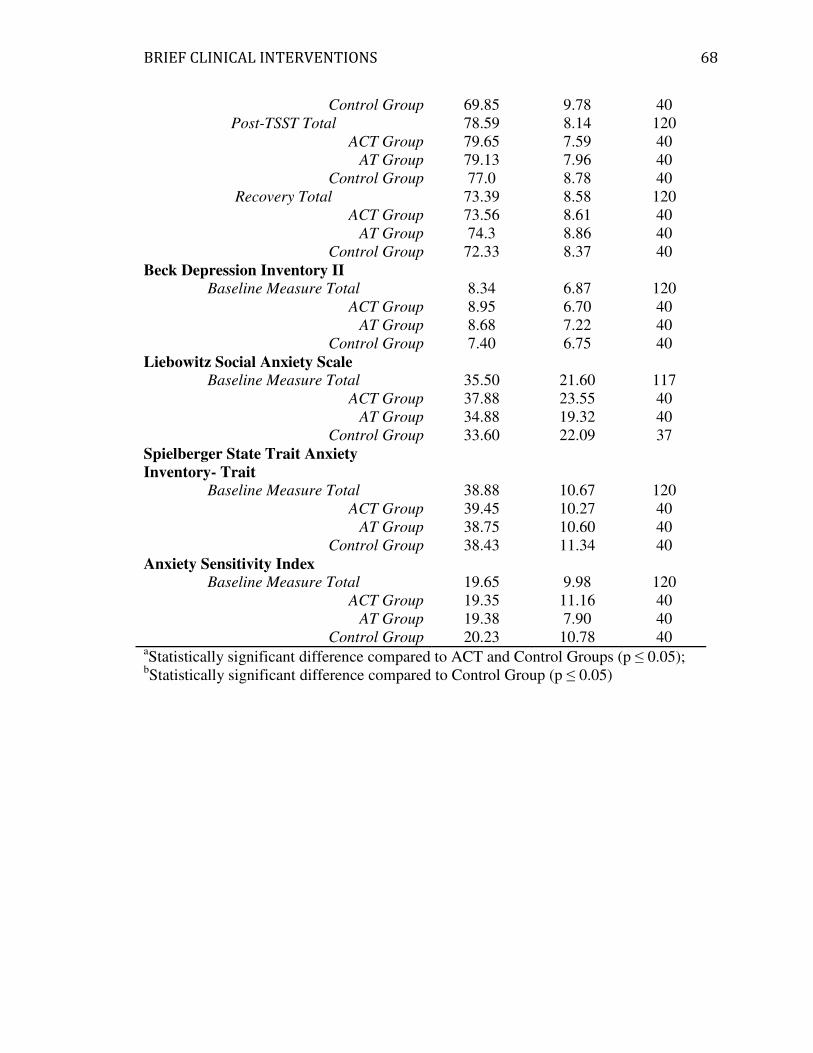
BRIEF CLINICAL INTERVENTIONS 68
Control Group 69.85 9.78 40
Post-TSST Total
ACT Group
AT Group
Control Group
78.59
79.65
79.13
77.0
8.14
7.59
7.96
8.78
120
40
40
40
Recovery Total
ACT Group
AT Group
Control Group
73.39
73.56
74.3
72.33
8.58
8.61
8.86
8.37
120
40
40
40
Beck Depression Inventory II
Baseline Measure Total
ACT Group
AT Group
Control Group
8.34
8.95
8.68
7.40
6.87
6.70
7.22
6.75
120
40
40
40
Liebowitz Social Anxiety Scale
Baseline Measure Total
ACT Group
AT Group
Control Group
35.50
37.88
34.88
33.60
21.60
23.55
19.32
22.09
117
40
40
37
Spielberger State Trait Anxiety
Inventory- Trait
Baseline Measure Total
ACT Group
AT Group
Control Group
38.88
39.45
38.75
38.43
10.67
10.27
10.60
11.34
120
40
40
40
Anxiety Sensitivity Index
Baseline Measure Total
ACT Group
AT Group
Control Group
19.65
19.35
19.38
20.23
9.98
11.16
7.90
10.78
120
40
40
40 aStatistically significant difference compared to ACT and Control Groups (p ≤ 0.05);
bStatistically significant difference compared to Control Group (p ≤ 0.05)

BRIEF CLINICAL INTERVENTIONS 69
Table 4
Descriptive Statistics for Study Measures by Gender
Mean SD N
Heart Rate (bpm)
Baseline Total
Male
Female
76.47
75.95
76.72
14.72
16.25
13.99
120
40
80
Pre-TSST Total
Male
Female
66.53
65.62
66.99
10.56
11.18
10.28
120
40
80
Post-TSST Total
Male
Female
69.44
69.95
69.19
12.11
14.03
11.12
120
40
80
Recovery Total
Male
Female
67.17
67.08
67.21
11.61
12.44
11.25
120
40
80
Systolic Blood Pressure (mmHg)
Baseline Total
Malea
Female
126.11
137.45
120.44
14.60
14.44
10.97
120
40
80
Pre-TSST Total
Malea
Female
120.15
131.35
114.55
13.052
12.64
9.08
120
40
80
Post-TSST Total
Malea
Female
131.38
144.07
125.04
14.36
12.92
10.29
120
40
80
Recovery Total
Malea
Female
123.98
134.18
118.87
13.891
11.70
12.0
120
40
80
Diastolic Blood Pressure (mmHg)
Baseline Total
Male
Female
72.97
73.97
72.48
8.90
10.74
7.86
120
40
80
Pre-TSST Total
Male
Female
70.39
71.05
70.06
8.83
9.05
8.76
120
40
80
Post-TSST Total
Male
Female
78.59
79.53
78.13
8.14
8.16
8.14
120
40
80
Recovery Total
Male
Female
73.39
73.8
73.19
8.58
10.41
7.58
120
40
80
Beck Depression Inventory II
Baseline Measure Total
Male
8.34
6.98
6.87
5.24
120
40

BRIEF CLINICAL INTERVENTIONS 70
Female 9.03 7.49 80
Liebowitz Social Anxiety Scale
Baseline Measure Total
Male
Female
35.50
32.23
37.2
21.60
18.52
23.0
117
40
77
Spielberger State Trait Anxiety
Inventory- Trait
Baseline Measure Total
Malea
Female
38.88
36.05
40.29
10.67
9.1
11.16
120
40
80
Anxiety Sensitivity Index
Baseline Measure Total
Malea
Female
19.65
16.75
21.1
9.98
8.31
10.46
120
40
80 aStatistically significant difference compared to Females (p ≤ 0.05)

BRIEF CLINICAL INTERVENTIONS
Figure 1
Autogenic Training Group: Depression and Systolic Blood Pressure
Figure 1. This figure helps demonstrate the 3
depression). It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Autogenic
Training group.
CLINICAL INTERVENTIONS
Autogenic Training Group: Depression and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group
It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Autogenic
71
way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Autogenic
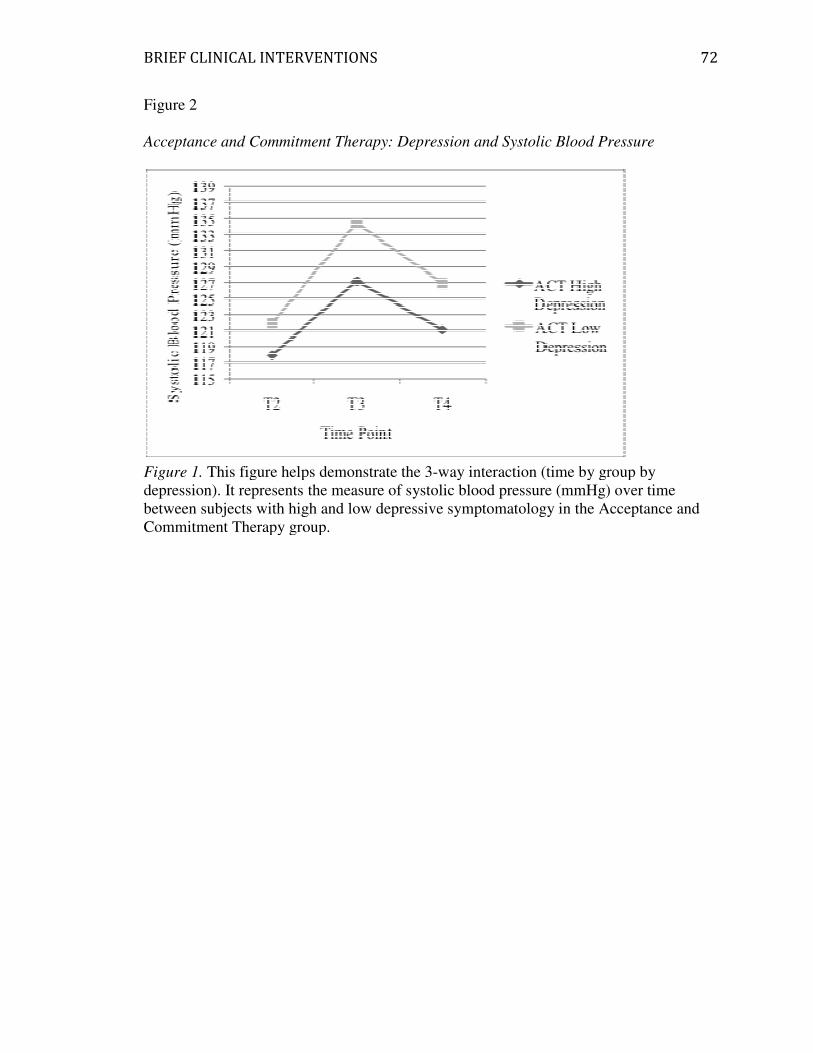
BRIEF CLINICAL INTERVENTIONS
Figure 2
Acceptance and Commitment Therapy:
Figure 1. This figure helps demonstrate the 3
depression). It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low
Commitment Therapy group.
CLINICAL INTERVENTIONS
Acceptance and Commitment Therapy: Depression and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Acceptance and
Commitment Therapy group.
72
Depression and Systolic Blood Pressure
way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
depressive symptomatology in the Acceptance and

BRIEF CLINICAL INTERVENTIONS
Figure 3
Control Group: Depression and Systolic Blood Pressure
Figure 3. This figure helps demonstrate the 3
depression). It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Control group.
CLINICAL INTERVENTIONS
Control Group: Depression and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group
It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Control group.
73
way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
between subjects with high and low depressive symptomatology in the Control group.
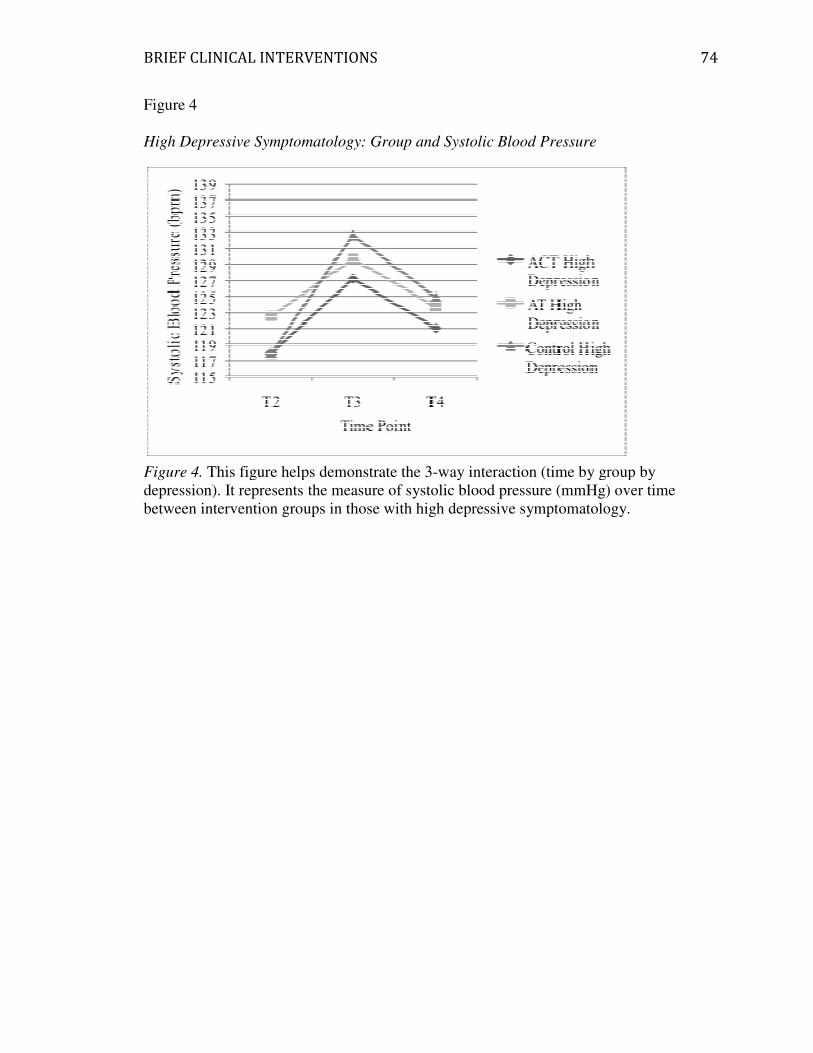
BRIEF CLINICAL INTERVENTIONS
Figure 4
High Depressive Symptomatology: Group and Systolic
Figure 4. This figure helps demonstrate the 3
depression). It represents the measure of systolic blood pressure (mmHg) over time
between intervention groups in those with high depressive
CLINICAL INTERVENTIONS
High Depressive Symptomatology: Group and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
between intervention groups in those with high depressive symptomatology.
74
way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
symptomatology.
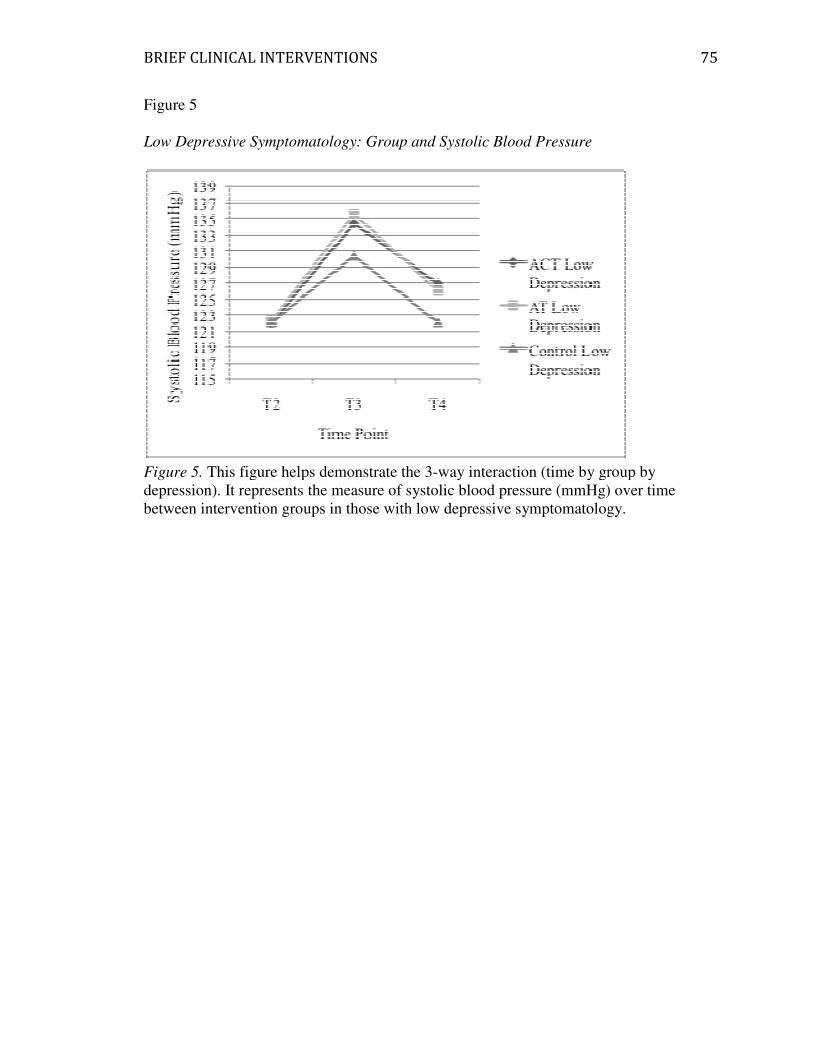
BRIEF CLINICAL INTERVENTIONS
Figure 5
Low Depressive Symptomatology: Group and Systolic Blood Pressure
Figure 5. This figure helps demonstrate the 3
depression). It represents the measure of systolic blood pressure (mmHg) over time
between intervention groups in those with
CLINICAL INTERVENTIONS
Low Depressive Symptomatology: Group and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
between intervention groups in those with low depressive symptomatology.
75
way interaction (time by group by
It represents the measure of systolic blood pressure (mmHg) over time
depressive symptomatology.
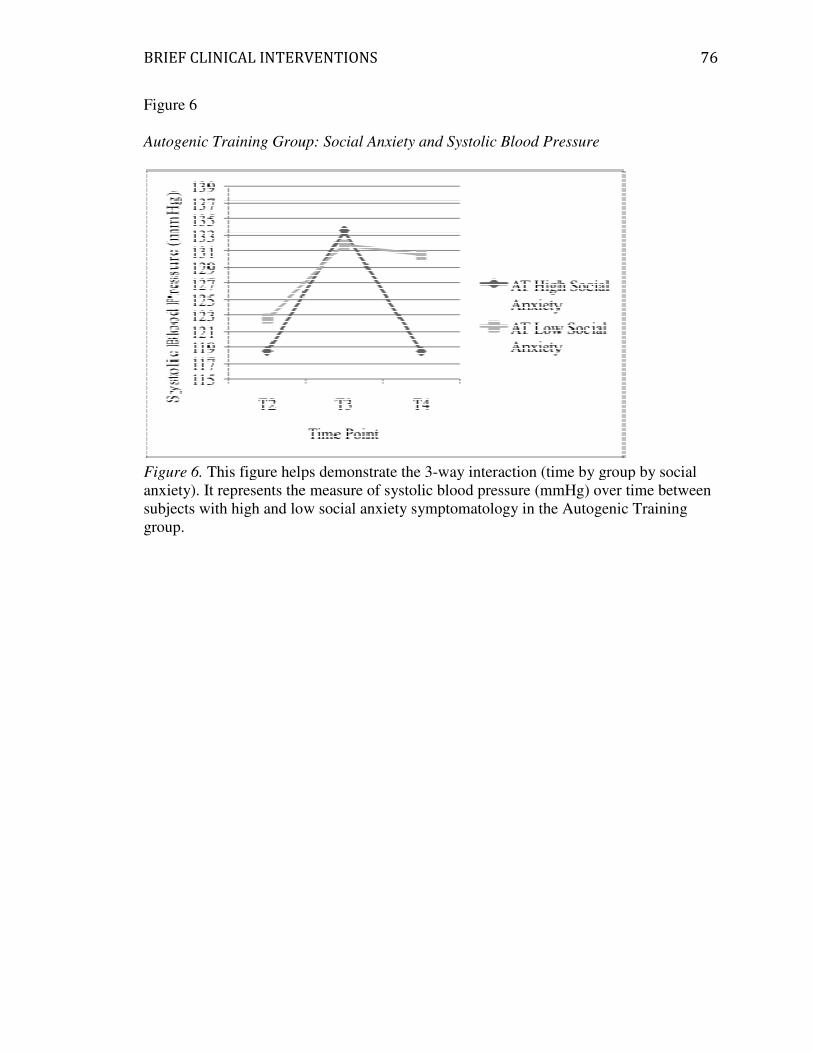
BRIEF CLINICAL INTERVENTIONS
Figure 6
Autogenic Training Group: Social Anxiety and Systolic Blood Pressure
Figure 6. This figure helps demonstrate the 3
anxiety). It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Autogenic
group.
CLINICAL INTERVENTIONS
Autogenic Training Group: Social Anxiety and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Autogenic
76
way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Autogenic Training
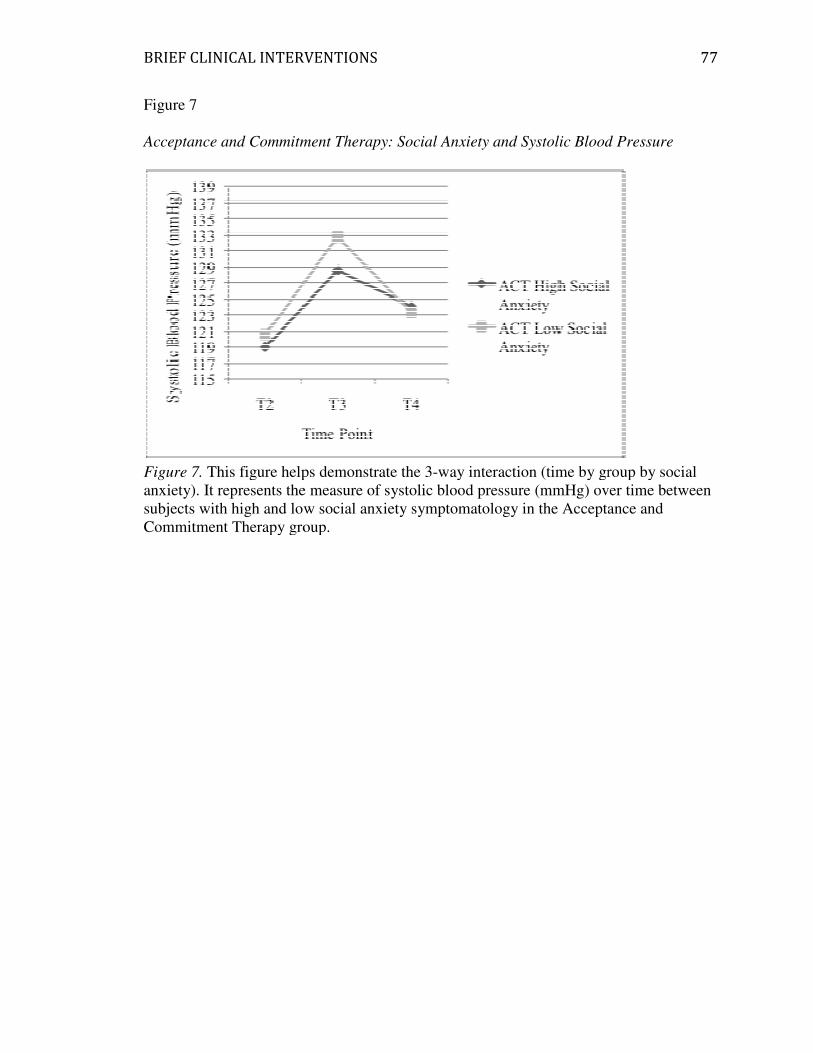
BRIEF CLINICAL INTERVENTIONS
Figure 7
Acceptance and Commitment Therapy: Social Anxiety and Systolic Blood Pressure
Figure 7. This figure helps demonstrate the 3
anxiety). It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Acceptance and
Commitment Therapy group.
CLINICAL INTERVENTIONS
Acceptance and Commitment Therapy: Social Anxiety and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Acceptance and
Commitment Therapy group.
77
Acceptance and Commitment Therapy: Social Anxiety and Systolic Blood Pressure
way interaction (time by group by social
the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Acceptance and

BRIEF CLINICAL INTERVENTIONS
Figure 8
Control Group: Social Anxiety and Systolic Blood
Figure 8. This figure helps demonstrate the 3
anxiety). It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the
CLINICAL INTERVENTIONS
Control Group: Social Anxiety and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Control group.
78
way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
Control group.
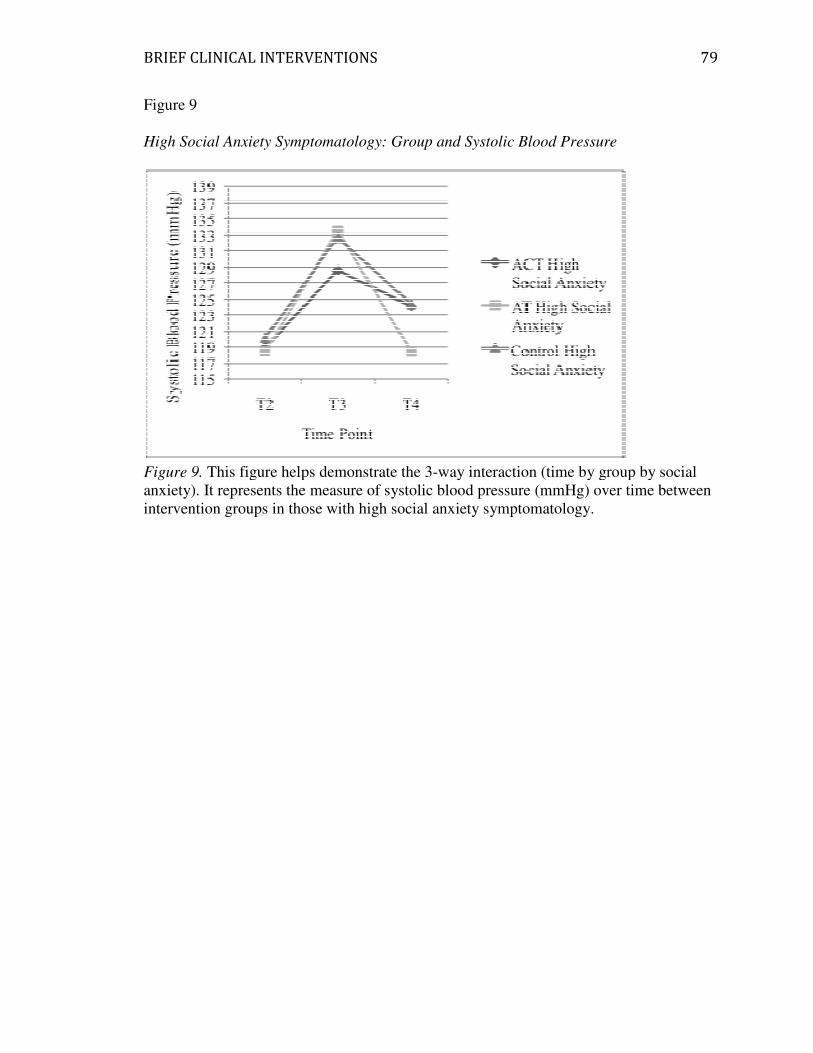
BRIEF CLINICAL INTERVENTIONS
Figure 9
High Social Anxiety Symptomatology: Group and Systolic Blood
Figure 9. This figure helps demonstrate the 3
anxiety). It represents the measure of systolic blood pressure (mmHg) over time between
intervention groups in those with high social anxiety
CLINICAL INTERVENTIONS
High Social Anxiety Symptomatology: Group and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
intervention groups in those with high social anxiety symptomatology.
79
Pressure
way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
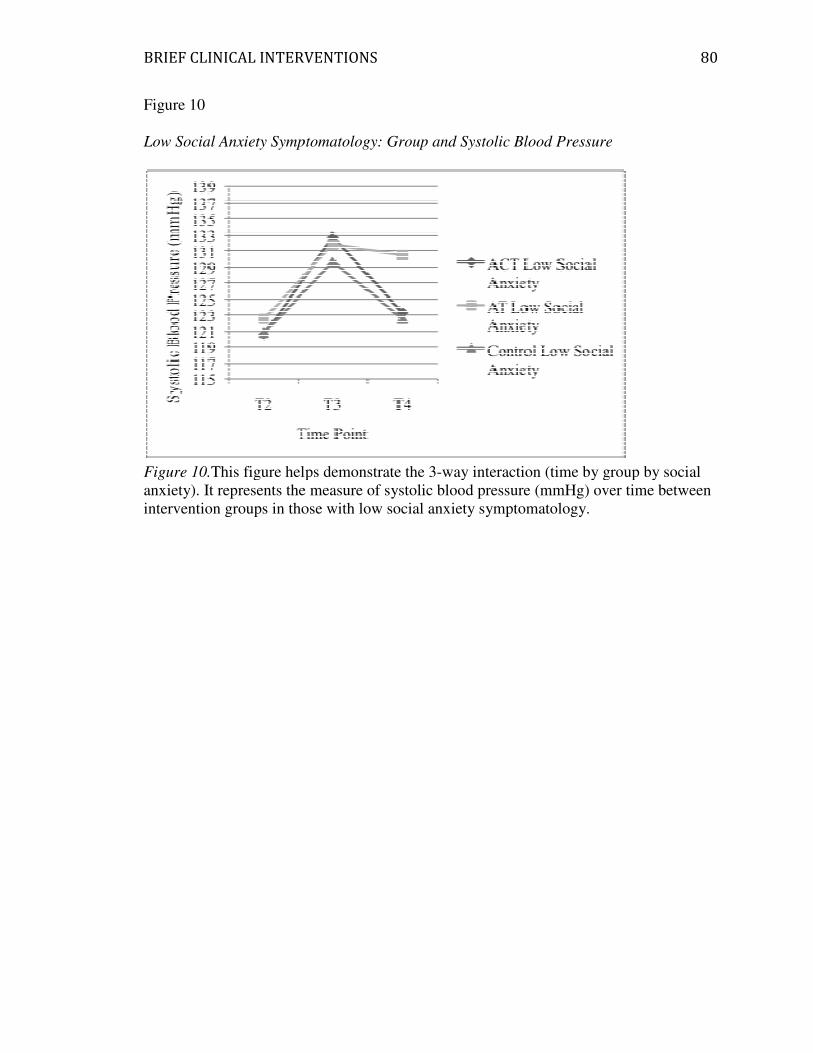
BRIEF CLINICAL INTERVENTIONS
Figure 10
Low Social Anxiety Symptomatology: Group and Systolic Blood Pressure
Figure 10.This figure helps demonstrate the 3
anxiety). It represents the measure of systolic blood pressure (mmHg) over time between
intervention groups in those with
CLINICAL INTERVENTIONS
Low Social Anxiety Symptomatology: Group and Systolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between
intervention groups in those with low social anxiety symptomatology.
80
Low Social Anxiety Symptomatology: Group and Systolic Blood Pressure
way interaction (time by group by social
It represents the measure of systolic blood pressure (mmHg) over time between

BRIEF CLINICAL INTERVENTIONS
Figure 11
Autogenic Training: Social Anxiety and Diastolic Blood Pressure
Figure 11. This figure helps demonstrate the 3
anxiety). It represents the measure of
subjects with high and low
group.
CLINICAL INTERVENTIONS
: Social Anxiety and Diastolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of diastolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Autogenic Training
81
way interaction (time by group by social
blood pressure (mmHg) over time between
symptomatology in the Autogenic Training

BRIEF CLINICAL INTERVENTIONS
Figure 12
Acceptance and Commitment Therapy: Social Anxiety and Diastolic Blood Pressure
Figure 12. This figure helps demonstrate the 3
anxiety). It represents the measure of
subjects with high and low
Commitment Therapy group.
CLINICAL INTERVENTIONS
Acceptance and Commitment Therapy: Social Anxiety and Diastolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of diastolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Acceptance and
group.
82
Acceptance and Commitment Therapy: Social Anxiety and Diastolic Blood Pressure
way interaction (time by group by social
blood pressure (mmHg) over time between
Acceptance and

BRIEF CLINICAL INTERVENTIONS
Figure 13
Control Group: Social Anxiety and Diastolic Blood Pressure
Figure 13. This figure helps demonstrate the 3
anxiety). It represents the measure of
subjects with high and low
CLINICAL INTERVENTIONS
Control Group: Social Anxiety and Diastolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by
It represents the measure of diastolic blood pressure (mmHg) over time between
subjects with high and low social anxiety symptomatology in the Control group
83
way interaction (time by group by social
blood pressure (mmHg) over time between
Control group.
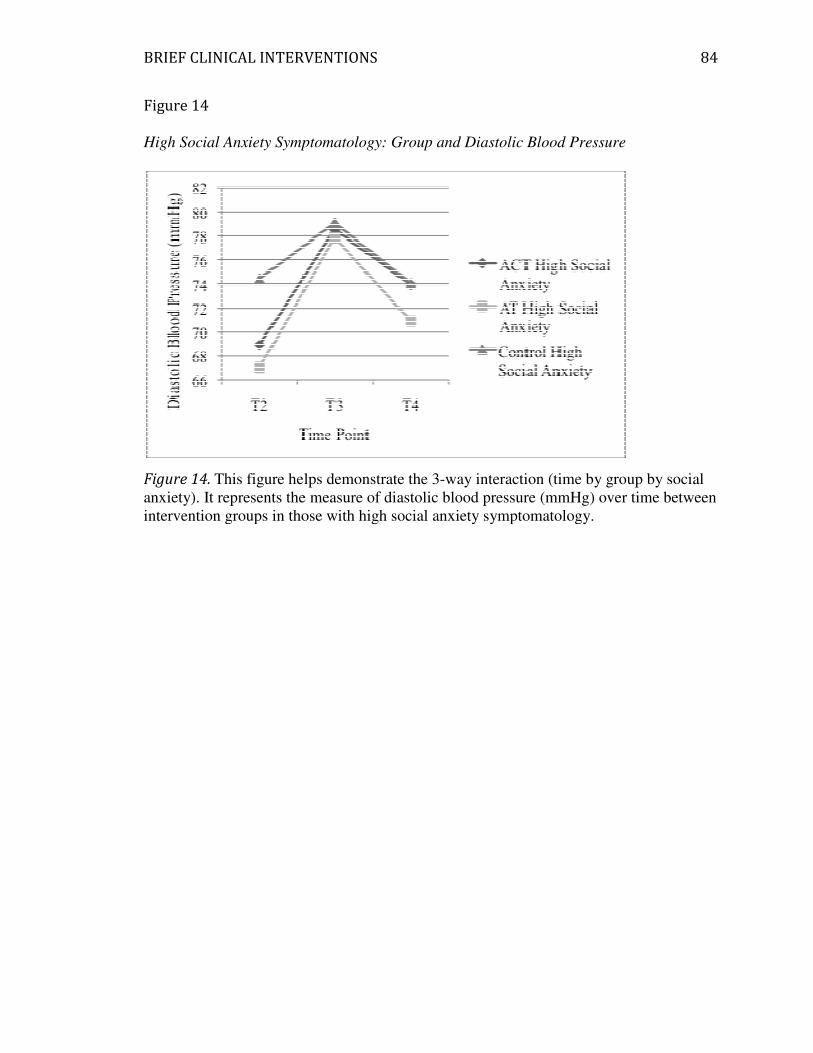
BRIEF CLINICAL INTERVENTIONS
Figure 14
High Social Anxiety Symptomatology: Group and
Figure 14. This figure helps demonstrate the 3
anxiety). It represents the measure of
intervention groups in those with high social anxiety symptomatology.
CLINICAL INTERVENTIONS
Social Anxiety Symptomatology: Group and Diastolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of diastolic blood pressure (mmHg) over time between
intervention groups in those with high social anxiety symptomatology.
84
Blood Pressure
way interaction (time by group by social
blood pressure (mmHg) over time between

BRIEF CLINICAL INTERVENTIONS
Figure 15
Low Social Anxiety Symptomatology: Group and
Figure 15. This figure helps demonstrate the 3
anxiety). It represents the measure of
intervention groups in those with
CLINICAL INTERVENTIONS
Social Anxiety Symptomatology: Group and Diastolic Blood Pressure
This figure helps demonstrate the 3-way interaction (time by group by social
It represents the measure of diastolic blood pressure (mmHg) over time between
intervention groups in those with low social anxiety symptomatology.
85
Blood Pressure
way interaction (time by group by social
blood pressure (mmHg) over time between