the impact of the covid-19 pandemic on maternal and
TRANSCRIPT

Kotlar et al. Reprod Health (2021) 18:10 https://doi.org/10.1186/s12978-021-01070-6
REVIEW
The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping reviewBethany Kotlar1, Emily Gerson2, Sophia Petrillo3, Ana Langer1 and Henning Tiemeier1,4*
Abstract
Introduction: The Covid-19 pandemic affects maternal health both directly and indirectly, and direct and indirect effects are intertwined. To provide a comprehensive overview on this broad topic in a rapid format behooving an emergent pandemic we conducted a scoping review.
Methods: A scoping review was conducted to compile evidence on direct and indirect impacts of the pandemic on maternal health and provide an overview of the most significant outcomes thus far. Working papers and news articles were considered appropriate evidence along with peer-reviewed publications in order to capture rapidly evolving updates. Literature in English published from January 1st to September 11 2020 was included if it pertained to the direct or indirect effects of the COVID-19 pandemic on the physical, mental, economic, or social health and wellbeing of pregnant people. Narrative descriptions were written about subject areas for which the authors found the most evidence.
Results: The search yielded 396 publications, of which 95 were included. Pregnant individuals were found to be at a heightened risk of more severe symptoms than people who are not pregnant. Intrauterine, vertical, and breastmilk transmission were unlikely. Labor, delivery, and breastfeeding guidelines for COVID-19 positive patients varied. Severe increases in maternal mental health issues, such as clinically relevant anxiety and depression, were reported. Domes-tic violence appeared to spike. Prenatal care visits decreased, healthcare infrastructure was strained, and potentially harmful policies implemented with little evidence. Women were more likely to lose their income due to the pandemic than men, and working mothers struggled with increased childcare demands.
Conclusion: Pregnant women and mothers were not found to be at higher risk for COVID-19 infection than peo-ple who are not pregnant, however pregnant people with symptomatic COVID-19 may experience more adverse outcomes compared to non-pregnant people and seem to face disproportionate adverse socio-economic conse-quences. High income and low- and middle-income countries alike faced significant struggles. Further resources should be directed towards quality epidemiological studies.
Plain English summary: The Covid-19 pandemic impacts reproductive and perinatal health both directly through infection itself but also indirectly as a consequence of changes in health care, social policy, or social and economic circumstances. The direct and indirect consequences of COVID-19 on maternal health are intertwined. To provide a comprehensive overview on this broad topic we conducted a scoping review. Pregnant women who have symp-tomatic COVID-19 may experience more severe outcomes than people who are not pregnant. Intrauterine and
© The Author(s) 2021. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creat iveco mmons .org/licen ses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creat iveco mmons .org/publi cdoma in/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Open Access
*Correspondence: [email protected] Harvard T.H. Chan School of Public Health, Boston, MA, USAFull list of author information is available at the end of the article

Page 2 of 39Kotlar et al. Reprod Health (2021) 18:10
BackgroundCOVID-19, first documented in Wuhan, China at the end of 2019 [1], has rapidly spread across the globe, infecting tens of millions of individuals [2]. While sex-disaggregated data on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mortalities suggest it poses more severe health outcomes for men than women [3], there are con-cerns that the disease could disproportionately burden women in a social and economic sense. Furthermore, it is a particularly salient question whether pregnant women are more susceptible to infection with SARS-CoV-2 or have more severe disease outcomes. Outside of direct infection, the impact of the pandemic and pandemic-control policies on healthcare infrastructure, societies, and the global econ-omy may also affect maternal health. Pregnant women and new mothers are a unique population, with particular men-tal and physical healthcare needs who are also particularly vulnerable to issues such as domestic violence. Finally, the impact of the COVID-19 pandemic is likely to be context-specific, and differ depending on a variety of country-spe-cific factors. A global pandemic is likely to only reveal its consequences after significant time passes, and literature published before or immediately after policies are imple-mented may not capture all relevant outcomes. The goal of this scoping review is to synthesize the current literature on both the direct consequences of contracting COVID-19 during pregnancy and the indirect consequences of the pandemic for pregnant individuals and mothers, taking into account the myriad ways in which containment and prevention measures have disrupted daily life.
MethodsThis scoping review followed the framework outlined by Arksey and O’Malley [4], in order to map the existing lit-erature on the direct and indirect impacts of COVID-19 on maternal health, incorporating the following 5 stages:
Identify research questionHow has the COVID-19 pandemic directly and indirectly impacted maternal health globally?
Identify relevant types of evidenceLiterature published in English from January 1st, 2020 to September 11, 2020 was included in the search. The search strategy involved the algorithm used by the Maternal Health Task Force’s Buzz, a biweekly e-news-letter presenting current research relevant to maternal health. Hand searches were conducted in PubMed using MeSH terms (see Additional file 1), along with broader searches of “COVID” and “corona” followed by the terms: “pregnant”, “maternal”, “women”, “reproductive”, “eco-nomic”, “social”, “indirect”, “direct.” Google Scholar was also searched using these terms to capture grey litera-ture, such as news articles and working papers that have not yet completed the peer review process. This scoping review aimed to capture rapidly evolving evidence in a timely manner, including issues not yet addressed in well-funded, epidemiological studies. The snowball method of consulting sources’ bibliographies was used for cer-tain articles to supplement referenced evidence. The search strategy as outlined above was not registered with PROSPERO.
Study selectionLiterature was included if published during the time frame outlined above and primarily assessed the direct or indirect effects of the COVID-19 pandemic on mater-nal health. Search terms utilized did not directly address neonatal health, but publications on topics relevant to both populations (transmission, breastfeeding, mater-nity care practices) were also included if returned by the search terms. Case reports, case series, qualitative stud-ies, systematic and scoping reviews, and meta-analyses
breastmilk transmission, and the passage of the virus from mother to baby during delivery are unlikely. The guidelines for labor, delivery, and breastfeeding for COVID-19 positive patients vary, and this variability could create uncertainty and unnecessary harm. Prenatal care visits decreased, healthcare infrastructure was strained, and potentially harm-ful policies are implemented with little evidence in high and low/middle income countries. The social and economic impact of COVID-19 on maternal health is marked. A high frequency of maternal mental health problems, such as clinically relevant anxiety and depression, during the epidemic are reported in many countries. This likely reflects an increase in problems, but studies demonstrating a true change are lacking. Domestic violence appeared to spike. Women were more vulnerable to losing their income due to the pandemic than men, and working mothers strug-gled with increased childcare demands. We make several recommendations: more resources should be directed to epidemiological studies, health and social services for pregnant women and mothers should not be diminished, and more focus on maternal mental health during the epidemic is needed.
Keywords: COVID-19, SARS-CoV-2, Maternal health, Newborn health, Maternal-child transmission, Mental health, Gender equity

Page 3 of 39Kotlar et al. Reprod Health (2021) 18:10
were included. As some publications included were sys-tematic or scoping reviews or meta-analyses, there was some duplication in data on which publications were based. The article containing the more complete descrip-tion of the data was used for data charting. Sources were excluded if they consisted only of recommendations for future research. Predictive research was excluded if it consisted only of speculation referencing past epidem-ics but included if based on quantitative methods. News articles, reports, and other grey literature were included if they contained quantifiable evidence (case reports, survey results, qualitative analyses).After reading full texts and synthesizing relevant evidence, literature was organized thematically. Themes were discussed and decided upon by all four authors. Themes that reflected potential impacts of COVID-19, but for which no quan-titative evidence existed were excluded from the review. Of 200 peer-reviewed articles, 129 were excluded; 7 did not pertain to maternal health or COVID-19, 3 were responses to articles, and 199 were commentaries, edi-torials, or practice guidelines which did not contain rel-evant evidence. Of 196 articles from the grey literature, 172 articles were excluded; 124 did not pertain to mater-nal health or COVID-19, and 48 did not contain objec-tive information. See Fig. 1 for a visual representation of inclusion and exclusion.
Chart the data71 peer-reviewed articles and 24 publications from the grey literature were included from the original search.
Two peer-reviewed articles that contradicted earlier find-ings that were published after September 11, 2020 were added. Publications included represented a wide range of methodologies including case reports, case series, obser-vational studies, letters to the editor, and news articles. The authors developed a rubric of major themes that arose in the literature and recorded standard information including location, sampling method, and size of sample, and key findings of each study (see Table 1). An adap-tive thematic analysis [5] was applied using the following steps. The authors identified themes in the literature by a reading and discussing each article included. Articles were then coded independently by two authors. All four authors discussed each code and grouped codes into final themes.
Collate, summarize, and report resultsNarrative descriptions of the evidence were written for each theme that the authors determined in the above stages. All authors reviewed descriptions for clarity and relevance and some themes were combined post hoc to improve readability and avoid redundancy.
Main textDirect effects on pregnancyDuring pregnancy, people undergo significant physi-ologic and immunologic alterations to support and pro-tect the developing fetus. These changes can increase the risk of infection with respiratory viruses for pregnant individuals and their fetuses. Thus, pregnant individuals
396Publica�ons
iden�fied
200 Peer-reviewed ar�cles
196 Grey literature
129 ar�cles excluded• 7 did not pertain to maternal
health and/or COVID-19• 3 responses• 199 did not contain evidence
(i.e. editorial, commentary)
95 Publica�ons 71
Peer-reviewed ar�cles
172 ar�cles excluded• 124 did not pertain to maternal
health and/or COVID-19• 48 did not contain objec�ve
informa�on (i.e. opinion, specula�on)
24Publica�ons
2 Peer-reviewed ar�cles
upda�ng original finding
97 Publica�ons
Fig. 1 Flowchart of literature selection

Page 4 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
Stud
ies
incl
uded
in th
e sc
opin
g re
view
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Del
ahoy
, Sep
tem
ber 2
020
“Cha
ract
eris
tics
and
Mat
erna
l and
Birt
h O
ut-
com
es o
f Hos
pita
lized
Pr
egna
nt W
omen
with
La
bora
tory
-Con
firm
ed
COVI
D-1
9”
MM
WR,
pop
ulat
ion
sur-
veill
ance
of 1
3 st
ates
Dire
ct e
ffect
s on
pre
g-na
ncy
Uni
ted
Stat
es59
8Pr
egna
nt w
omen
mig
ht b
e at
incr
ease
d ris
k fo
r sev
ere
coro
navi
rus
dise
ase
Wu
et a
l. Ju
ne 2
020
“Clin
ical
Man
ifest
atio
n an
d La
bora
tory
Cha
ract
er-
istic
s of
SA
RS-C
oV-2
In
fect
ion
in P
regn
ant
Wom
en.”
Peer
-rev
iew
ed, r
etro
spec
-tiv
e st
udy
Dire
ct e
ffect
s on
pre
g-na
ncy
Chi
na8
Clo
se m
onito
ring
of
labo
rato
ry p
aram
eter
s in
clud
ing
the
WBC
cou
nt,
LYM
PH c
ount
, and
CRP
, al
ong
with
oth
er im
agin
g fe
atur
es in
che
st C
T sc
ans,
is w
arra
nted
to p
rom
ptly
pr
even
t, di
agno
se, a
nd
trea
t a S
ARS
-CoV
-2 in
fec-
tion
durin
g pr
egna
ncy
Xu e
t al.
Apr
il 20
20“C
linic
al P
rese
ntat
ions
and
O
utco
mes
of S
ARS
-Co
V-2
Infe
cted
Pne
umo-
nia
in P
regn
ant W
omen
an
d H
ealth
Sta
tus
of
Thei
r Neo
nate
s.”
Peer
revi
ewed
, ret
rosp
ec-
tive
stud
yD
irect
effe
cts
on p
reg-
nanc
y, in
trau
terin
e tr
ansm
issi
on
Chi
na5
No
obvi
ous
vert
ical
tr
ansm
issi
on w
as
obse
rved
, lym
phop
enia
an
d eo
sino
peni
a w
ere
obse
rved
mor
e fre
quen
tly
in p
regn
ant C
OVI
D-1
9 pa
tient
s as
com
pare
d to
pr
egna
nt w
omen
with
out
COVI
D-1
9
Smith
et a
l. Ju
ne 2
020
“Mat
erna
l and
Neo
nata
l O
utco
mes
Ass
ocia
ted
with
CO
VID
-19
Infe
ctio
n:
A S
yste
mat
ic R
evie
w.”
Peer
revi
ewed
, sys
tem
atic
re
view
Dire
ct e
ffect
s on
pre
g-na
ncy,
intr
aute
rine
tran
smis
sion
, lab
or a
nd
deliv
ery
Chi
naN
/ACO
VID
-19-
posi
tive
preg
nant
w
omen
pre
sent
with
fe
wer
sym
ptom
s th
an th
e ge
nera
l pop
ulat
ion
and
may
be
RT-P
CR
nega
tive
desp
ite h
avin
g si
gns
of
vira
l pne
umon
ia. T
he
inci
denc
e of
pre
term
bi
rths
, low
birt
h w
eigh
t, C
-sec
tion,
NIC
U a
dmis
sion
ap
pear
hig
her t
han
the
gene
ral p
opul
atio
n

Page 5 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Knig
ht e
t al.
June
202
0“C
hara
cter
istic
s an
d O
utco
mes
of P
regn
ant
Wom
en A
dmitt
ed to
H
ospi
tal w
ith C
onfir
med
SA
RS-C
oV-2
Infe
ctio
n in
U
K: N
atio
nal P
opul
atio
n Ba
sed
Coho
rt S
tudy
.”
Peer
revi
ewed
, pop
ulat
ion
coho
rt s
tudy
Dire
ct e
ffect
s on
pre
g-na
ncy,
intr
aute
rine
tran
smis
sion
Uni
ted
King
dom
427
Mos
t pre
gnan
t wom
en
adm
itted
to h
ospi
tal w
ith
SARS
-CoV
-2 in
fect
ion
wer
e in
the
late
sec
ond
or th
ird tr
imes
ter.
Mos
t ha
d go
od o
utco
mes
, and
tr
ansm
issi
on o
f SA
RS-
CoV-
2 to
infa
nts
was
un
com
mon
. The
hig
h pr
opor
tion
of w
omen
fro
m b
lack
or m
inor
ity
ethn
ic g
roup
s ad
mitt
ed
with
infe
ctio
n ne
eds
urge
nt in
vest
igat
ion
and
expl
anat
ion
Allo
tey
et a
l. Se
ptem
ber
2020
“Clin
ical
Man
ifest
a-tio
ns, R
isk
fact
ors,
and
Mat
erna
l and
Per
inat
al
Out
com
es o
f Cor
o-na
viru
s D
isea
se 2
019
in P
regn
ancy
: Liv
ing
Syst
emat
ic R
evie
w a
nd
Met
a-an
alys
is”
Peer
revi
ewed
, sys
tem
atic
re
view
and
met
a-an
alys
is
Dire
ct e
ffect
s on
pre
g-na
ncy
Glo
bal
11,4
32Pr
egna
nt a
nd re
cent
ly
preg
nant
wom
en a
re le
ss
likel
y to
man
ifest
CO
VID
-19
rela
ted
sym
ptom
s of
fe
ver a
nd m
yalg
ia th
an
non-
preg
nant
wom
en
of re
prod
uctiv
e ag
e an
d ar
e po
tent
ially
mor
e lik
ely
to n
eed
inte
nsiv
e ca
re
trea
tmen
t for
CO
VID
-19.
Pr
e-ex
istin
g co
mor
bidi
-tie
s, hi
gh m
ater
nal a
ge,
and
high
bod
y m
ass
inde
x se
em to
be
risk
fact
ors
for
seve
r cov
id-1
9. P
rete
rm
birt
h ra
tes
are
high
in
preg
nant
wom
en w
ith
covi
d-19
than
in p
regn
ant
wom
en w
ithou
t the
di
seas
e

Page 6 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Pere
ira e
t al.
July
202
0“C
linic
al C
ours
e of
Cor
o-na
viru
s D
isea
se-2
019
in
Preg
nanc
y.”
Peer
revi
ewed
, ret
rosp
ec-
tive
stud
yD
irect
effe
cts
on p
reg-
nanc
y, in
trau
terin
e tr
ansm
issi
on, l
abor
and
de
liver
y, b
reas
tfeed
ing
and
infa
nt c
onta
ct
Spai
n60
Mos
t of t
he p
regn
ant
wom
en w
ith C
OVI
D‐1
9 ha
d a
favo
rabl
e cl
inic
al
cour
se. H
owev
er, o
ne‐
third
of t
hem
dev
elop
ed
pneu
mon
ia, o
f who
m 5
%
pres
ente
d a
criti
cal c
linic
al
stat
us. S
even
ty‐e
ight
per
-ce
nt o
f the
wom
en h
ad a
va
gina
l del
iver
y. N
o ve
rti-
cal o
r hor
izon
tal t
rans
mis
-si
ons
wer
e di
agno
sed
in
the
neon
ates
dur
ing
labo
r or
bre
astfe
edin
g
Blitz
et a
l. Ju
ne 2
020
“Mat
erna
l Mor
talit
y am
ong
Wom
en w
ith C
oron
avi-
rus
Dis
ease
201
9 A
dmit-
ted
to th
e In
tens
ive
Care
U
nit.”
Peer
revi
ewed
, cas
e se
ries
Dire
ct e
ffect
s on
pre
g-na
ncy
New
Yor
k, U
nite
d St
ates
462
Mat
erna
l dea
th o
ccur
red
in
15%
of p
atie
nts
adm
itted
to
the
ICU
s fo
r CO
VID
-19
and
in 2
5% o
f tho
se
who
requ
ired
inva
sive
m
echa
nica
l ven
tilat
ion.
D
eliv
ery
occu
rred
in
half
of th
e pa
tient
s w
ith
COVI
D-1
9 w
ho w
ere
adm
itted
to th
e IC
Us
and
all p
atie
nts
who
requ
ired
inva
sive
mec
hani
cal v
en-
tilat
ion.
His
pani
c w
omen
co
nstit
uted
the
larg
est
raci
al o
r eth
nic
grou
p in
the
stud
y, w
hich
may
re
flect
a d
ispr
opor
tiona
te
burd
en o
f dis
ease
am
ong
min
ority
gro
ups

Page 7 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Che
n et
al.
Mar
ch 2
020
“Clin
ical
Cha
ract
eris
tics
and
Intr
aute
rine
Vert
ical
Tr
ansm
issi
on P
oten
tial
of C
OVI
D-1
9 In
fect
ion
in
Nin
e Pr
egna
nt W
omen
: A
Ret
rosp
ectiv
e Re
view
of
Med
ical
Rec
ords
.”
Peer
revi
ewed
, ret
rosp
ec-
tive
stud
yD
irect
effe
cts
on p
reg-
nanc
y, in
trau
terin
e tr
ansm
issi
on, l
abor
and
de
liver
y, b
reas
tfeed
ing
and
infa
nt c
onta
ct
Chi
na9
The
clin
ical
cha
ract
eris
tics
of C
OVI
D-1
9 pn
eum
onia
in
pre
gnan
t wom
en w
ere
sim
ilar t
o th
ose
repo
rted
fo
r non
-pre
gnan
t adu
lt pa
tient
s w
ho d
evel
oped
CO
VID
-19
pneu
mon
ia.
Find
ings
from
this
sm
all
grou
p of
cas
es s
ugge
st
that
ther
e is
cur
rent
ly n
o ev
iden
ce fo
r int
raut
er-
ine
infe
ctio
n ca
used
by
vert
ical
tran
smis
sion
in
wom
en w
ho d
evel
op
COVI
D-1
9 pn
eum
onia
in
late
pre
gnan
cy
Yang
et a
l. A
pril
2020
“Clin
ical
Fea
ture
s an
d O
utco
mes
of P
regn
ant
Wom
en S
uspe
cted
of
Coro
navi
rus
Dis
ease
20
19.”
Peer
revi
ewed
, pro
spec
tive
case
con
trol
stu
dyD
irect
effe
cts
on p
reg-
nanc
yC
hina
55Th
e cl
inic
al s
ympt
oms
and
labo
rato
ry in
dica
tors
are
no
t obv
ious
for a
sym
pto-
mat
ic a
nd m
ild C
OVI
D-1
9 pr
egna
nt w
omen
. Pul
mo-
nary
CT
scan
plu
s bl
ood
rout
ine
exam
inat
ion
are
mor
e su
itabl
e fo
r find
ing
preg
nanc
y w
omen
with
as
ympt
omat
ic o
r mild
CO
VID
-19
infe
ctio
n, a
nd
can
be u
sed
scre
en-
ing
COVI
D-1
9 pr
egna
nt
wom
en in
the
outb
reak
ar
ea o
f CO
VID
-19
infe
ctio
n

Page 8 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Khan
et a
l. M
arch
202
0“Im
pact
of C
OVI
D-1
9 In
fect
ion
on P
regn
ancy
O
utco
mes
and
the
Risk
of
Mat
erna
l-to-
Neo
nata
l In
trap
artu
m T
rans
mis
-si
on o
f CO
VID
-19
durin
g N
atur
al B
irth.
”
Lett
er to
the
edito
r, ca
se
serie
sD
irect
effe
cts
on
preg
nanc
y, la
bor a
nd
deliv
ery
Chi
na3
Non
e of
the
3 w
omen
in
this
stu
dy h
ad d
ied
of
COVI
D-1
9 in
fect
ion
as o
f M
arch
1, 2
020.
No
vert
ical
tr
ansm
issi
on o
f CO
VID
-19
was
foun
d in
the
third
tr
imes
ter o
f pre
gnan
cy
amon
g in
fant
s de
liver
ed
via
the
vagi
nal r
oute
. M
oreo
ver,
we
did
not fi
nd
evid
ence
of m
ater
nal-
to-n
eona
tal i
ntra
part
um
tran
smis
sion
of C
OVI
D-1
9 vi
a va
gina
l del
iver
y
Lokk
en e
t al.
May
202
0“C
linic
al C
hara
cter
istic
s of
46
Preg
nant
Wom
en
with
a S
ever
e A
cute
Re
spira
tory
Syn
drom
e Co
rona
viru
s 2
Infe
ctio
n in
Was
hing
ton
Stat
e.”
Peer
revi
ewed
, ret
rosp
ec-
tive
stud
yD
irect
effe
cts
on p
reg-
nanc
yW
ashi
ngto
n, U
nite
d St
ates
46Se
vere
cor
onav
irus
dise
ase
2019
dev
elop
ed in
ap
prox
imat
ely
15%
of
preg
nant
pat
ient
s an
d oc
curr
ed p
rimar
ily in
ov
erw
eigh
t or o
bese
w
omen
with
und
erly
-in
g co
nditi
ons.
Obe
sity
an
d co
rona
viru
s di
seas
e 20
19 m
ay s
yner
gist
ical
ly
incr
ease
risk
for a
med
i-ca
lly in
dica
ted
pret
erm
bi
rth
to im
prov
e m
ater
nal
pulm
onar
y st
atus
in la
te
preg
nanc
y. T
hese
find
ings
su
ppor
t cat
egor
izin
g pr
egna
nt p
atie
nts
as a
hi
gher
-ris
k gr
oup,
par
ticu-
larly
thos
e w
ith c
hron
ic
com
orbi
ditie
s

Page 9 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Sava
si e
t al.
Aug
ust 2
020
“Clin
ical
Fin
ding
s an
d D
isea
se S
ever
ity in
H
ospi
taliz
ed P
regn
ant
Wom
en W
ith C
oro-
navi
rus
Dis
ease
201
9 (C
OVI
D-1
9).”
Peer
revi
ewed
, pro
spec
tive
coho
rt s
tudy
Dire
ct e
ffect
s on
pre
g-na
ncy
Italy
77O
ne in
five
wom
en h
ospi
tal-
ized
with
CO
VID
-19
infe
c-tio
n de
liver
ed u
rgen
tly fo
r re
spira
tory
com
prom
ise
or w
ere
adm
itted
to th
e IC
U. N
one,
how
ever
, die
d.
Incr
ease
d pr
eges
tatio
nal
BMI a
nd a
bnor
mal
hea
rt
and
resp
irato
ry ra
tes
on
adm
issi
on w
ere
asso
ci-
ated
with
sev
ere
dise
ase
Men
doza
et a
l. Ju
ne 2
020
“Pre
-Ecl
amps
ia-li
ke
Synd
rom
e In
duce
d by
Se
vere
CO
VID
-19:
A P
ro-
spec
tive
Obs
erva
tiona
l St
udy.”
Peer
revi
ewed
, pro
spec
tive
coho
rt s
tudy
Dire
ct e
ffect
s on
pre
g-na
ncy
Spai
n42
Preg
nant
wom
en w
ith
seve
re C
OVI
D‐1
9 ca
n de
velo
p a
PE‐li
ke
synd
rom
e th
at m
ight
be
dist
ingu
ishe
d fro
m a
ctua
l PE
by
sFlt‐
1/Pl
GF,
LDH
and
U
tAPI
ass
essm
ent.
Hea
lth-
care
pro
vide
rs s
houl
d be
aw
are
of it
s ex
iste
nce
and
mon
itor p
regn
anci
es w
ith
susp
ecte
d pr
e‐ec
lam
psia
w
ith c
autio
n
Ferr
aiol
o et
al.
June
202
0“R
epor
t of P
ositi
ve P
lace
n-ta
l Sw
abs
for S
ARS
-CoV
-2
in a
n A
sym
ptom
atic
Pr
egna
nt W
oman
with
CO
VID
-19.”
Peer
revi
ewed
, cas
e re
port
Intr
aute
rine
tran
smis
sion
Italy
1Th
is w
as a
repo
rt o
f a
posi
tive
plac
enta
l sw
ab
for S
ARS
-CoV
-2 in
an
asym
ptom
atic
wom
an
in th
e th
ird tr
imes
ter
of p
regn
ancy
with
a
posi
tive
rhin
o-ph
aryn
geal
sw
ab fo
r CO
VID
-19,
who
un
derw
ent a
n ur
gent
cae
-sa
rian
sect
ion
for o
bste
tric
in
dica
tions
Hos
ier e
t al.
2020
“SA
RS-C
oV-2
Infe
ctio
n of
th
e Pl
acen
ta.”
Peer
revi
ewed
, cas
e re
port
Dire
ct e
ffect
s on
pre
g-na
ncy,
intr
aute
rine
tran
smis
sion
Uni
ted
Stat
es1
This
repo
rt h
ighl
ight
s a
case
of
acu
te p
lace
ntal
infe
c-tio
n w
ith S
ARS
–CoV
-2
that
may
hav
e po
tent
i-at
ed s
ever
e, e
arly
-ons
et
pree
clam
psia
Gol
den,
The
a, &
Sim
mon
s, Ju
ly 2
020
“Mat
erna
l and
Neo
nata
l Re
spon
se to
CO
VID
-19.”
Peer
revi
ewed
, sco
ping
re
view
Intr
aute
rine
tran
smis
sion
Glo
bal
N/A
At t
his
time,
ver
tical
tran
s-m
issi
on o
f SA
RS-C
oV-2
is
cons
ider
ed u
nlik
ely

Page 10 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Hun
tley
et a
l. A
ugus
t 202
0“R
ates
of M
ater
nal a
nd
Perin
atal
Mor
talit
y an
d Ve
rtic
al T
rans
mis
sion
in
Preg
nanc
ies
Com
pli-
cate
d by
Sev
ere
Acu
te
Resp
irato
ry S
yndr
ome
Coro
navi
rus
2 (S
ARS
-Co
-V-2
) Inf
ectio
n: A
Sy
stem
atic
Rev
iew
.”
Peer
revi
ewed
, sys
tem
atic
re
view
Dire
ct e
ffect
s on
pre
g-na
ncy,
intr
aute
rine
tran
smis
sion
, lab
or a
nd
deliv
ery
Glo
bal
N/A
Ther
e ar
e lo
w ra
tes
of
mat
erna
l and
neo
nata
l m
orta
lity
and
vert
i-ca
l tra
nsm
issi
on w
ith
SARS
-CoV
-2. T
he p
rete
rm
birt
h ra
te o
f 20%
and
the
cesa
rean
del
iver
y ra
te
exce
edin
g 80
% s
eem
s re
late
d to
geo
grap
hic
prac
tice
patt
erns
Wal
ker e
t al.
June
202
0“M
ater
nal T
rans
mis
sion
of
SA
RS-C
OV-
2 to
the
Neo
nate
, and
Pos
sibl
e Ro
utes
for S
uch
Tran
s-m
issi
on: A
Sys
tem
atic
Re
view
and
Crit
ical
A
naly
sis.”
Peer
revi
ewed
, sys
tem
atic
re
view
Intr
aute
rine
tran
smis
-si
on, l
abor
and
del
iver
y,
brea
stfe
edin
g an
d in
fant
co
ntac
t
Glo
bal
655
Neo
nata
l CO
VID‐1
9 in
fec-
tion
is u
ncom
mon
, rar
ely
sym
ptom
atic
, and
the
rate
of
infe
ctio
n is
no
grea
ter
whe
n th
e ba
by is
bor
n va
gina
lly, b
reas
tfed
or
rem
ains
with
the
mot
her
Zhan
g et
al.
July
202
0“S
ever
e A
cute
Res
pira
tory
Sy
ndro
me
Coro
navi
rus
2 (S
ARS
-CoV
-2) I
nfec
tion
Dur
ing
Late
Pre
gnan
cy:
A R
epor
t of 1
8 Pa
tient
s fro
m W
uhan
, Chi
na
Peer
revi
ewed
, cas
e se
ries
Dire
ct e
ffect
s on
pre
g-na
ncy,
intr
aute
rine
tran
smis
sion
, lab
or a
nd
deliv
ery
Chi
na18
The
maj
ority
of p
atie
nts
in
late
term
pre
gnan
cy w
ith
COVI
D-1
9 w
ere
of o
rdi-
nary
type
, and
they
wer
e le
ss li
kely
to d
evel
op in
to
criti
cal p
neum
onia
aft
er
early
isol
atio
n an
d an
ti-vi
ral t
reat
men
t. Ve
rtic
al
tran
smis
sion
of S
ARS
-Co
V-2
was
not
det
ecte
d,
but t
he p
ropo
rtio
n of
ne
onat
al b
acte
rial p
neu-
mon
ia w
as h
ighe
r tha
n ot
her n
eona
tal d
isea
ses
in
new
born
s
Mar
tins-
Filh
o et
al.
Apr
il 20
20“T
o Br
east
feed
or N
ot
to B
reas
tfeed
? La
ck o
f Ev
iden
ce o
n th
e Pr
es-
ence
of S
ARS
-CoV
-2 in
Br
east
milk
of P
regn
ant
Wom
en w
ith C
OVI
D-1
9.”
Peer
revi
ewed
, rap
id
syst
emat
ic re
view
Brea
stfe
edin
g an
d in
fant
co
ntac
tG
loba
lN
/AN
o br
east
milk
sam
ples
w
ere
posi
tive
for S
ARS
-Co
V-2
and,
to d
ate,
ther
e is
no
evid
ence
on
the
pres
ence
of S
ARS
-CoV
-2
in b
reas
t milk
of p
regn
ant
wom
en w
ith C
OVI
D-1
9
Page 11 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
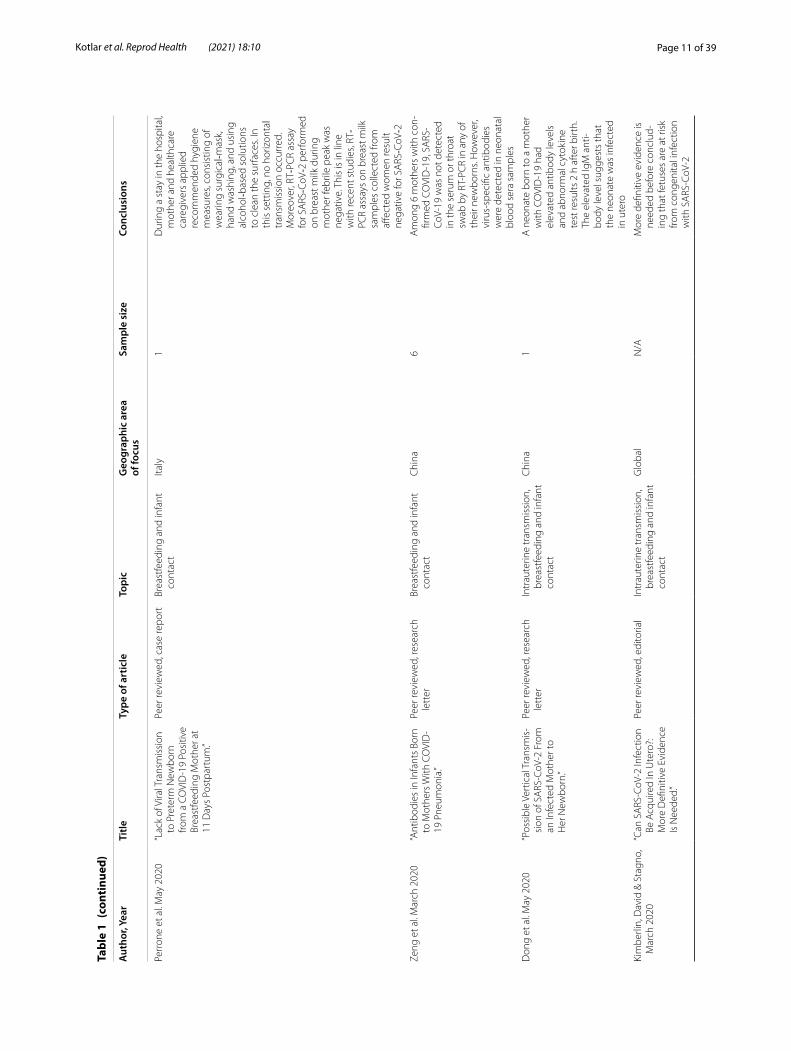
Perr
one
et a
l. M
ay 2
020
“Lac
k of
Vira
l Tra
nsm
issi
on
to P
rete
rm N
ewbo
rn
from
a C
OVI
D-1
9 Po
sitiv
e Br
east
feed
ing
Mot
her a
t 11
Day
s Po
stpa
rtum
.”
Peer
revi
ewed
, cas
e re
port
Brea
stfe
edin
g an
d in
fant
co
ntac
tIta
ly1
Dur
ing
a st
ay in
the
hosp
ital,
mot
her a
nd h
ealth
care
ca
regi
vers
app
lied
reco
mm
ende
d hy
gien
e m
easu
res,
cons
istin
g of
w
earin
g su
rgic
al‐m
ask,
ha
nd w
ashi
ng, a
nd u
sing
al
coho
l‐bas
ed s
olut
ions
to
cle
an th
e su
rfac
es. I
n th
is s
ettin
g, n
o ho
rizon
tal
tran
smis
sion
occ
urre
d.
Mor
eove
r, RT‐P
CR
assa
y fo
r SA
RS‐C
oV‐2
per
form
ed
on b
reas
t milk
dur
ing
mot
her f
ebril
e pe
ak w
as
nega
tive.
Thi
s is
in li
ne
with
rece
nt s
tudi
es, R
T‐PC
R as
says
on
brea
st m
ilk
sam
ples
col
lect
ed fr
om
affec
ted
wom
en re
sult
nega
tive
for S
ARS‐C
oV‐2
Zeng
et a
l. M
arch
202
0“A
ntib
odie
s in
Infa
nts
Born
to
Mot
hers
With
CO
VID
-19
Pne
umon
ia.”
Peer
revi
ewed
, res
earc
h le
tter
Brea
stfe
edin
g an
d in
fant
co
ntac
tC
hina
6A
mon
g 6
mot
hers
with
con
-fir
med
CO
VID
-19,
SA
RS-
CoV-
19 w
as n
ot d
etec
ted
in th
e se
rum
or t
hroa
t sw
ab b
y RT
-PC
R in
any
of
thei
r new
born
s. H
owev
er,
viru
s-sp
ecifi
c an
tibod
ies
wer
e de
tect
ed in
neo
nata
l bl
ood
sera
sam
ples
Don
g et
al.
May
202
0“P
ossi
ble
Vert
ical
Tra
nsm
is-
sion
of S
ARS
-CoV
-2 F
rom
an
Infe
cted
Mot
her t
o H
er N
ewbo
rn.”
Peer
revi
ewed
, res
earc
h le
tter
Intr
aute
rine
tran
smis
sion
, br
east
feed
ing
and
infa
nt
cont
act
Chi
na1
A n
eona
te b
orn
to a
mot
her
with
CO
VID
-19
had
elev
ated
ant
ibod
y le
vels
an
d ab
norm
al c
ytok
ine
test
resu
lts 2
h a
fter
birt
h.
The
elev
ated
IgM
ant
i-bo
dy le
vel s
ugge
sts
that
th
e ne
onat
e w
as in
fect
ed
in u
tero
Kim
berli
n, D
avid
& S
tagn
o,
Mar
ch 2
020
“Can
SA
RS-C
oV-2
Infe
ctio
n Be
Acq
uire
d In
Ute
ro?:
Mor
e D
efini
tive
Evid
ence
Is
Nee
ded.
”
Peer
revi
ewed
, edi
toria
lIn
trau
terin
e tr
ansm
issi
on,
brea
stfe
edin
g an
d in
fant
co
ntac
t
Glo
bal
N/A
Mor
e de
finiti
ve e
vide
nce
is
need
ed b
efor
e co
nclu
d-in
g th
at fe
tuse
s ar
e at
risk
fro
m c
onge
nita
l inf
ectio
n w
ith S
ARS
-CoV
-2

Page 12 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Eglo
ff et
al.
July
202
0“E
vide
nce
and
Poss
ible
M
echa
nism
s of
Rar
e M
ater
nal–
Feta
l Tra
nsm
is-
sion
of S
ARS
-CoV
-2.”
Peer
revi
ewed
, rev
iew
Intr
aute
rine
tran
smis
sion
Fran
ce17
9A
mon
g 17
9 ne
wbo
rns
test
ed fo
r SA
RS-C
oV2
at
birt
h fro
m m
othe
rs w
ith
COVI
D-1
9, tr
ansm
issi
on
was
sus
pect
ed in
8 c
ases
, 5
with
pos
itive
nas
o-ph
aryn
geal
SA
RS-C
oV-2
RT
-PC
R an
d 3
with
SA
RS-
CoV-
2 Ig
M
Wu
et a
l. M
ay 2
020
“Cor
onav
irus
Dis
ease
20
19 a
mon
g Pr
egna
nt
Chi
nese
Wom
en: C
ase
Serie
s D
ata
on th
e Sa
fety
of
Vag
inal
Birt
h an
d Br
east
feed
ing.
”
Peer
revi
ewed
, sin
gle
cent
er c
ohor
t stu
dyIn
trau
terin
e tr
ansm
issi
on,
brea
stfe
edin
gC
hina
13Va
gina
l del
iver
y m
ay b
e a
safe
del
iver
y op
tion.
How
-ev
er, a
dditi
onal
rese
arch
is
urg
ently
nee
ded
to
exam
ine
brea
st m
ilk a
nd
the
pote
ntia
l ris
k fo
r vira
l co
ntam
inat
ion
Ash
okka
et a
l. Ju
ly 2
020
“Car
e of
the
Preg
nant
W
oman
with
Cor
ona-
viru
s D
isea
se 2
019
in
Labo
r and
Del
iver
y:
Ane
sthe
sia,
Em
erge
ncy
Cesa
rean
Del
iver
y,
Diff
eren
tial D
iagn
osis
in
the
Acu
tely
Ill P
artu
rient
, Ca
re o
f the
New
born
, an
d Pr
otec
tion
of th
e H
ealth
care
Per
sonn
el.”
Peer
revi
ewed
, clin
ical
op
inio
nLa
bor a
nd d
eliv
ery
Glo
bal
N/A
We
pres
ent m
anag
emen
t st
rate
gies
der
ived
from
be
st a
vaila
ble
evid
ence
to
prov
ide
guid
ance
in c
ar-
ing
for t
he h
igh-
risk
and
acut
ely
ill p
artu
rient
Oxf
ord-
Hor
rey
et a
l. A
ugus
t 202
0“P
uttin
g It
All
Toge
ther
: C
linic
al C
onsi
dera
tions
in
the
Care
of C
ritic
ally
Ill
Obs
tetr
ic P
atie
nts
with
CO
VID
-19.”
Peer
revi
ewed
, rev
iew
Labo
r and
del
iver
yU
.SN
/AG
uide
lines
from
var
ious
cl
inic
al s
ocie
ties,
alon
g w
ith d
irect
ion
from
loca
l he
alth
aut
horit
ies,
mus
t be
con
side
red
whe
n ap
proa
chin
g th
e ca
re
of a
n ob
stet
ric p
atie
nt
with
kno
wn
or s
uspe
cted
CO
VID
-19.
With
a ra
pidl
y ch
angi
ng la
ndsc
ape,
a
sim
plifi
ed a
nd c
ohes
ive
pers
pect
ive
usin
g gu
id-
ance
from
diff
eren
t clin
ical
so
ciet
y re
com
men
datio
ns
rega
rdin
g th
e cr
itica
lly-il
l ob
stet
ric p
atie
nt w
ith
COVI
D-1
9 is
nee
ded

Page 13 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Gat
ta, N
unzi
a, R
izzo
, Pilu
&
Sim
onaz
zi, A
pril
2020
“CO
VID
19 d
urin
g Pr
eg-
nanc
y: A
Sys
tem
atic
Re
view
of R
epor
ted
Case
s.”
Peer
revi
ewed
, sys
tem
atic
re
view
Labo
r and
del
iver
yG
loba
l51
At t
he ti
me
of th
e re
port
, 3
preg
nanc
ies
wer
e on
go-
ing;
of t
he re
mai
ning
48
preg
nant
wom
en, 4
6 ga
ve
birt
h by
ces
area
n de
liver
y,
and
2 ga
ve b
irth
vagi
nally
Zaig
ham
& A
nder
sson
, A
pril
2020
“Mat
erna
l and
per
inat
al
outc
omes
with
CO
VID
-19
: A s
yste
mat
ic re
view
of
108
pre
gnan
cies
.”
Peer
revi
ewed
, sys
tem
atic
re
view
Labo
r and
del
iver
yG
loba
l10
891
% o
f the
wom
en w
ere
deliv
ered
by
cesa
rean
se
ctio
n
Che
n et
al.
Apr
il 20
20“C
linic
al C
hara
cter
istic
s of
Pr
egna
nt W
omen
with
Co
vid-
19 in
Wuh
an,
Chi
na.”
Lett
er to
the
edito
r, re
view
Labo
r and
del
iver
yC
hina
118
Of t
he 6
8 pa
tient
s w
ho
deliv
ered
dur
ing
the
stud
y pe
riod,
63
(93%
) und
er-
wen
t a c
esar
ean
sect
ion
Mal
hotr
a et
al.
June
202
0“N
o C
hang
e in
Ces
area
n Se
ctio
n Ra
te d
urin
g CO
VID
-19
Pand
emic
in
New
Yor
k C
ity.”
Lett
er to
the
edito
rLa
bor a
nd d
eliv
ery
U.S
N/A
We
foun
d th
at th
ere
wer
e no
cha
nges
in C
esar
ean
sect
ion
rate
dur
ing
the
COVI
D-1
9 pa
ndem
ic in
N
ew Y
ork
City
COVI
DSu
rg C
olla
bora
tive,
M
ay 2
020
“Ele
ctiv
e su
rger
y ca
ncel
la-
tions
due
to th
e CO
VID
-19
pan
dem
ic: G
loba
l pr
edic
tive
mod
ellin
g to
in
form
sur
gica
l rec
over
y pl
ans”
Peer
revi
ewed
, mod
ellin
g st
udy
Labo
r and
del
iver
yG
loba
lN
/AG
loba
lly, 8
1.7
per c
ent o
f op
erat
ions
for b
enig
n co
nditi
ons,3
7.7
per c
ent
of c
ance
r ope
ratio
ns a
nd
25.4
per
cen
t of e
lec-
tive
caes
area
n se
ctio
ns
wou
ld b
e ca
ncel
led
or
post
pone
d
Nar
ang
et a
l. M
ay 2
020
“SA
RS-C
oV-2
in P
regn
ancy
: A
Com
preh
ensi
ve
Sum
mar
y of
Cur
rent
G
uide
lines
.”
Peer
revi
ewed
, sum
mar
y of
gui
delin
esLa
bor a
nd d
eliv
ery
Glo
bal
N/A
The
sum
mar
y of
gui
delin
es
for t
he m
anag
emen
t of
COVI
D-1
9 in
pre
gnan
cy
acro
ss d
iffer
ent p
erin
atal
so
ciet
ies
is fa
irly
cons
ist-
ent,
with
som
e va
riatio
n in
the
stre
ngth
of r
ecom
-m
enda
tions

Page 14 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Lei e
t al.
Mar
ch 2
020
“Clin
ical
Cha
ract
eris
tics
of
COVI
D-1
9 in
Pre
gnan
cy:
Ana
lysi
s of
Nin
e Ca
ses.”
Retr
ospe
ctiv
e ca
se s
tudy
Brea
stfe
edin
g an
d in
fant
co
ntac
tC
hina
9Se
rial r
eal-t
ime
quan
titat
ive
reve
rse
tran
scrip
tion-
poly
mer
ase
chai
n re
actio
n sh
owed
neg
ativ
e re
sults
in
the
dete
ctio
n of
201
9-no
vel c
oron
aviru
s in
all
sam
ples
obt
aine
d fro
m
amni
otic
flui
d, u
mbi
li-ca
l cor
d bl
ood,
neo
nata
l na
soph
aryn
x, b
reas
t milk
, an
d va
gina
Wan
g et
al.
July
202
0“A
Cas
e Re
port
of N
eona
tal
2019
Cor
onav
irus
Dis
-ea
se in
Chi
na.”
Peer
revi
ewed
, cas
e st
udy
Brea
stfe
edin
g an
d in
fant
co
ntac
tC
hina
1Th
e m
othe
r’s b
reas
t milk
sa
mpl
e w
as n
egat
ive
for
SARS
-CoV
-2 a
s w
ell
Zhu
et a
l. Ju
ne 2
020
“Bre
astfe
edin
g Ri
sk fr
om
Det
ecta
ble
Seve
re A
cute
Re
spira
tory
Syn
drom
e Co
rona
viru
s 2
in B
reas
t-m
ilk.”
Peer
revi
ewed
, ret
rosp
ec-
tive
case
stu
dyBr
east
feed
ing
and
infa
nt
cont
act
Chi
na5
Four
out
of fi
ve (8
0%)
patie
nt`s
bre
astm
ilk
sam
ples
wer
e ne
gativ
e fo
r SA
RS-C
oV-2
RT-
PCR,
whi
ch is
sim
ilar t
o pr
evio
us o
bser
vatio
ns,2
,8
whi
le o
ne (2
0%) p
atie
nt`s
(P
atie
nt 3
) bre
astm
ilk
show
ed S
ARS
-CoV
-2 R
NA
te
st p
ositi
ve
Don
g et
al.
Janu
ary
2020
“Ant
ibod
ies
in th
e Br
east
M
ilk o
f a M
ater
nal
Wom
an w
ith C
OVI
D-1
9.”
Peer
revi
ewed
, cas
e st
udy
Brea
stfe
edin
g an
d in
fant
co
ntac
tC
hina
1A
mat
erna
l wom
an w
as
posi
tive
for S
ARS
-CoV
-2
test
ed in
thro
at s
wab
s bu
t ne
gativ
e te
sted
in o
ther
bo
dy fl
uids
, and
she
had
Ig
G a
nd Ig
A d
etec
ted
in
brea
st m
ilk
Bast
ug e
t al.
July
202
0“V
irola
ctia
in a
n A
sym
p-to
mat
ic M
othe
r with
CO
VID
-19.”
Peer
revi
ewed
, cas
e st
udy
Brea
stfe
edin
g an
d in
fant
co
ntac
tTu
rkey
1Te
mpo
rary
sep
arat
ion
of th
e ne
wbo
rn fr
om a
mot
her
with
con
firm
ed o
r sus
-pe
cted
CO
VID
-19
shou
ld
be s
tron
gly
cons
ider
ed to
re
duce
the
risk
of tr
ans-
mis
sion
to th
e ne
onat
e

Page 15 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Wu
et a
l. A
ugus
t 202
0“P
erin
atal
Dep
ress
ive
and
Anx
iety
Sym
ptom
s of
Pr
egna
nt W
omen
dur
ing
the
Coro
navi
rus
Dis
ease
20
19 O
utbr
eak
in C
hina
.”
Peer
revi
ewed
, mul
ti-ce
nter
, cro
ss-s
ectio
nal
stud
y
Men
tal h
ealth
Chi
na41
24Pr
egna
nt w
omen
ass
esse
d af
ter t
he d
ecla
ratio
n of
co
rona
viru
s di
seas
e 20
19
epid
emic
had
sig
nific
antly
hi
gher
rate
s of
dep
ress
ive
sym
ptom
s th
an w
omen
as
sess
ed b
efor
e th
e ep
i-de
mic
dec
lara
tion.
The
se
wom
en w
ere
also
mor
e lik
ely
to h
ave
thou
ghts
of
self-
harm
. The
dep
ress
ive
rate
s w
ere
posi
tivel
y as
so-
ciat
ed w
ith th
e nu
mbe
r of
new
ly c
onfir
med
cas
es o
f co
rona
viru
s di
seas
e 20
19,
susp
ecte
d in
fect
ions
, and
de
aths
per
day
Sacc
one
et a
l. M
ay 2
020
“Psy
chol
ogic
al Im
pact
of
Coro
navi
rus
Dis
ease
20
19 in
Pre
gnan
t W
omen
.”
Peer
revi
ewed
, cro
ss-s
ec-
tiona
l sur
vey
stud
yM
enta
l hea
lthIta
ly10
0Th
e CO
VID
-19
outb
reak
ha
d a
mod
erat
e to
sev
ere
psyc
holo
gica
l im
pact
on
preg
nant
wom
en
Jung
ari,
June
202
0“M
ater
nal M
enta
l Hea
lth in
In
dia
durin
g CO
VID
-19.”
Peer
revi
ewed
, let
ter t
o th
e ed
itor
Men
tal h
ealth
Indi
aN
/APr
egna
nt w
omen
and
ne
w m
othe
rs a
re a
t an
elev
ated
risk
of s
uffer
-in
g fro
m m
enta
l hea
lth
prob
lem
s. It
has
been
ob
serv
ed th
at th
e un
cer-
tain
ty s
urro
undi
ng C
OVI
D-
19 h
as le
d to
hig
her l
evel
s of
dep
ress
ion
amon
g w
omen
dur
ing
and
afte
r pr
egna
ncy
Gau
sman
& L
ange
r, A
pril
2020
“Sex
and
Gen
der D
ispa
ri-tie
s in
the
COVI
D-1
9 Pa
n-de
mic
.”
Peer
revi
ewed
, com
men
-ta
ryM
enta
l hea
lthG
loba
lN
/AA
lthou
gh c
onta
inm
ent
stra
tegi
es …
may
be
clin
i-ca
lly im
port
ant t
o re
duce
tr
ansm
issi
on, t
hey
may
al
so h
ave
prof
ound
sho
rt-
and
long
-ter
m m
enta
l he
alth
impl
icat
ions
for
wom
en

Page 16 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Ary
al &
Pan
t, D
ecem
ber
2020
“Mat
erna
l Men
tal H
ealth
in
Nep
al a
nd It
s Pr
iorit
iza-
tion
durin
g CO
VID
-19
Pand
emic
: Mis
sing
the
Obv
ious
.”
Peer
revi
ewed
, let
ter t
o th
e ed
itor
Men
tal h
ealth
Nep
alN
/ALa
ck o
f cou
nsel
ing,
unc
er-
tain
ty a
nd in
deci
sive
ness
in
crea
ses
stre
ss d
urin
g pr
egna
ncy.
In a
dditi
on to
th
is, p
regn
ant w
omen
are
w
orry
ing
abou
t CO
VID
19
effec
ts o
n th
eir h
ealth
and
th
eir n
ewbo
rns
Kota
bagi
, For
tune
, Ess
ien,
N
auta
, & Y
oong
, Jul
y 20
20
“Anx
iety
and
Dep
ress
ion
Leve
ls a
mon
g Pr
egna
nt
Wom
en w
ith C
OVI
D-1
9.”
Peer
revi
ewed
, let
ter t
o th
e ed
itor
Men
tal h
ealth
UK
N/A
Med
ian
scor
e ro
se to
a
max
imum
at t
he h
eigh
t of
the
pand
emic
dea
ths
in
the
UK
whe
n “lo
ckdo
wn”
ru
les
wer
e in
stitu
ted
amid
gr
eat u
ncer
tain
ty a
bout
N
atio
nal H
ealth
Ser
vice
ca
paci
ty a
nd C
OVI
D
outc
omes
Chi
vers
et a
l. Se
pter
mbe
r 20
20“P
erin
atal
Dis
tres
s D
urin
g CO
VID
-19:
The
mat
ic
Ana
lysi
s of
an
Onl
ine
Pare
ntin
g Fo
rum
”
Peer
revi
ewed
, qua
litat
ive
them
atic
ana
lysi
sM
enta
l hea
lthA
ustr
alia
N/A
Them
es w
ere
(1) h
eigh
t-en
ed d
istr
ess
rela
ted
to a
hi
gh-r
isk
exte
rnal
env
iron-
men
t; (2
) des
pair
and
antic
ipat
ory
grie
f due
to
depr
ivat
ion
of s
ocia
l and
fa
mily
sup
port
, and
bon
d-in
g rit
uals
; (3)
alte
red
fam
-ily
and
sup
port
rela
tion-
ship
s; (4
) gui
lt-ta
mpe
red
happ
ines
s; an
d (5
) fam
ily
futu
re p
ostp
oned
Koen
en, J
uly
2020
“Pre
gnan
t Dur
ing
a Pa
n-de
mic
?”Bl
og a
rtic
leM
enta
l hea
lthU
.SN
/AO
ver 7
0% o
f wom
en re
port
cl
inic
ally
sig
nific
ant
depr
essi
on o
r anx
iety
, and
ov
er 4
0% s
cree
n po
sitiv
e fo
r pos
t-tr
aum
atic
str
ess
diso
rder
(PTS
D)
Thap
a, M
aina
li, S
chw
ank,
&
Ach
arya
, Jul
y 20
20“M
ater
nal M
enta
l Hea
lth in
th
e Ti
me
of th
e CO
VID
-19
Pan
dem
ic.”
Peer
revi
ewed
, edi
toria
lM
enta
l hea
lthG
loba
lN
/ASt
rict p
ublic
hea
lth m
eas-
ures
dire
cted
tow
ards
m
itiga
ting
the
spre
ad o
f di
seas
e ar
e ne
cess
ary
but
know
n to
hav
e ne
gativ
e ps
ycho
logi
cal e
ffect
s le
ad-
ing
to s
tres
s, an
ger a
nd
conf
usio
n

Page 17 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Prei
s et
al.
Dec
embe
r 202
0“V
ulne
rabi
lity
and
resi
lienc
e to
pan
dem
ic-
rela
ted
stre
ss a
mon
g U
.S.
wom
en p
regn
ant a
t the
st
art o
f the
CO
VID
-19
pand
emic
”
Peer
revi
ewed
, sur
vey
Men
tal h
ealth
, Pre
nata
l ca
reU
.S44
51N
early
one
-thi
rd o
f pr
egna
nt w
omen
hig
hly
stre
ssed
by
the
COVI
D-1
9 pa
ndem
ic
Robe
rton
et a
l. M
ay 2
020
“Ear
ly e
stim
ates
of t
he
indi
rect
effe
cts
of th
e CO
VID
-19
pand
emic
on
mat
erna
l and
chi
ld
mor
talit
y in
low
-inco
me
and
mid
dle-
inco
me
coun
trie
s: a
mod
ellin
g st
udy”
Peer
revi
ewed
, mod
ellin
g st
udy
Pren
atal
car
eG
loba
lN
/AM
odel
est
imat
es a
redu
c-tio
n in
ant
enat
al c
are
by
at le
ast 1
8%, a
nd p
ossi
bly
up to
51.
9%, a
nd a
sim
ilar
redu
ctio
n in
pos
tnat
al
care
Men
ende
z et
al.
May
202
0“A
void
ing
Indi
rect
Effe
cts
of C
OVI
D-1
9 on
Mat
erna
l an
d C
hild
Hea
lth.”
Peer
revi
ewed
, com
men
tPr
enat
al c
are
Glo
bal
N/A
In th
e co
ntex
t of t
he
COVI
D-1
9 pa
ndem
ic,
som
e A
frica
n co
untr
ies
are
chan
ging
rout
ine
AN
C g
uide
lines
to s
pace
(a
nd d
e fa
cto
redu
ce)
the
num
ber o
f con
tact
s to
one
eve
ry 3
mon
ths
inst
ead
of m
onth
ly v
isits
, or
del
ayin
g th
e po
stpa
r-tu
m v
isit
to 3
mon
ths
afte
r del
iver
y (t
here
fore
no
long
er c
onst
itutin
g a
post
part
um v
isit)
Ram
oni,
June
202
0“H
ow C
OVI
D-1
9 Is
Affe
ct-
ing
Ant
enat
al C
are.”
New
s ar
ticle
Pren
atal
car
eN
iger
iaN
/AD
r. A
deye
mi O
kuno
wo,
ad
mitt
ed th
at w
ith
COVI
D-1
9, th
e no
rmal
way
of
car
ing
for p
regn
ant
wom
en h
ad b
een
mod
i-fie
d to
redu
ce th
e sp
read
of
the
dise
ase

Page 18 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Ary
al, S
hres
tha,
May
202
0“M
othe
rhoo
d in
Nep
al
durin
g CO
VID
-19
Pan-
dem
ic: A
re W
e H
eadi
ng
from
Saf
e to
Uns
afe?
”
Com
men
tPr
enat
al c
are
Nep
alN
/ATh
ere
is a
pos
sibi
lity
of d
elay
in
see
king
car
e w
hen
preg
nant
mot
hers
are
un
sure
whe
n to
vis
it th
e ho
spita
ls b
ecau
se o
f the
un
cert
aint
y of
ava
ilabi
lity
of th
eir s
ervi
ces
durin
g th
e pa
ndem
ic. F
or w
omen
ha
iling
from
rem
ote
area
s, th
e tr
avel
ban
dur
ing
the
lock
dow
n ca
uses
a d
elay
in
reac
hing
car
e
Palla
ngyo
et a
l. Ju
ne 2
020
“The
Impa
ct o
f Cov
id-1
9 on
Mid
wiv
es’ P
ract
ice
in K
enya
, Uga
nda
and
Tanz
ania
: A R
eflec
tive
Acc
ount
.”
Peer
revi
ewed
, refl
ectiv
e ac
coun
tPr
enat
al c
are
Keny
a, U
gand
a, a
nd
Tanz
ania
N/A
Mid
wiv
es h
ave
repo
rted
lo
w n
umbe
rs a
tten
ding
m
ater
nal h
ealth
clin
ics
and
wom
en a
re a
fraid
to
vis
it th
e ho
spita
ls
for f
ear o
f con
trac
ting
coro
navi
rus…
Thi
s ha
s le
d to
wom
en c
omin
g in
to h
ospi
tals
too
late
, so
met
imes
end
ing
with
un
desi
rabl
e ou
tcom
es e
.g.
still
birt
hs, n
eona
tal a
nd
mat
erna
l dea
th
Popu
latio
n Co
unci
l, A
pril
2020
“Ken
ya: C
OVI
D-1
9 Kn
owl-
edge
, Att
itude
s, Pr
actic
es
and
Nee
ds—
Resp
onse
s fro
m S
econ
d Ro
und
of
Dat
a Co
llect
ion
in F
ive
Nai
robi
Info
rmal
Set
tle-
men
ts (K
iber
a, H
urum
a,
Kario
bang
i, D
ando
ra,
Mat
hare
).”
Surv
eyPr
enat
al c
are,
gen
der
equi
ty in
the
wor
kfor
ceKe
nya
1,76
9M
ore
wom
en re
port
ed
com
plet
e lo
ss o
f inc
ome/
empl
oym
ent c
ompa
red
to m
en. W
omen
wer
e tw
ice
as li
kely
to fo
rgo
esse
ntia
l he
alth
ser
vice
s, in
clud
ing
fam
ily p
lann
ing
serv
ices

Page 19 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Relie
fWeb
, Apr
il 20
20“R
apid
Gen
der A
naly
sis—
COVI
D-1
9: W
est A
frica
—A
pril
2020
—Be
nin.
”
Ana
lysi
sPr
enat
al c
are
Wes
t Afri
ca26
6Be
twee
n so
cial
dis
tanc
ing
slow
ing
dow
n al
l ser
vice
pr
ovis
ions
and
the
fear
of
att
endi
ng c
linic
s, it
is v
ery
hard
for w
omen
to
acc
ess
SRH
R se
rvic
es.
Wom
en a
nd y
outh
hav
e lit
tle a
cces
s to
trad
ition
al
info
rmat
ion
chan
nels
like
TV
and
radi
o be
caus
e m
en c
ontr
ol th
ese
outle
ts
in th
e ho
useh
old
Sem
aan
et a
l. Ju
ne 2
020
“Voi
ces
from
the
Fron
tline
: Fi
ndin
gs fr
om a
The
-m
atic
Ana
lysi
s of
a R
apid
O
nlin
e G
loba
l Sur
vey
of
Mat
erna
l and
New
born
H
ealth
Pro
fess
iona
ls
Faci
ng th
e CO
VID
-19
Pand
emic
.”
Peer
revi
ewed
, glo
bal,
cros
s-se
ctio
nal s
tudy
Pren
atal
car
eG
loba
l71
4H
ealth
care
pro
vide
rs a
re
wor
ried
abou
t the
impa
ct
of ra
pidl
y ch
angi
ng
care
pra
ctic
es o
n he
alth
ou
tcom
es: r
educ
ed a
cces
s to
ant
enat
al c
are,
few
er
outp
atie
nt v
isits
, sho
rter
le
ngth
of s
tay
in fa
cilit
ies
afte
r birt
h, b
anni
ng b
irth
com
pani
ons,
sepa
ratin
g ne
wbo
rns
from
CO
VID
-19
posi
tive
mot
hers
and
po
stpo
ning
rout
ine
imm
uniz
atio
ns
Coxo
n et
al.
Sept
embe
r 20
20“T
he Im
pact
of t
he
Coro
navi
rus
(CO
VID
-19)
Pa
ndem
ic o
n M
ater
nity
Ca
re in
Eur
ope.”
Peer
revi
ewed
, edi
toria
lPr
enat
al c
are
U.K
N/A
Conc
ern
abou
t wha
t co
nstit
utes
saf
e ca
re o
f pr
egna
nt w
omen
and
ne
wbo
rns
has
incr
ease
d,
and
in m
any
sett
ings
, ris
k av
erse
dec
isio
ns h
ave
been
take
n in
mat
erni
ty
care
pro
visi
on w
hich
, it
is a
rgue
d, m
ay in
crea
se
unne
cess
ary
med
ical
in
terv
entio
ns, p
ut w
omen
at
risk
of b
eing
infe
cted
w
ith C
OVI
D-1
9 by
redu
c-in
g pr
ovis
ion
of c
omm
u-ni
ty o
r hom
e-ba
sed
care
, an
d re
duce
or r
ever
se
prog
ress
ion
tow
ards
hig
h qu
ality
mat
erni
ty c
are

Page 20 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Aye
new
et a
l. Ju
ne 2
020
“Ris
k fo
r Sur
ge M
ater
nal
Mor
talit
y an
d M
orbi
d-ity
dur
ing
the
Ong
oing
Co
rona
Viru
s Pa
ndem
ic.”
Prep
rint
Pren
atal
car
eIn
dia
and
Ethi
opia
N/A
Lock
dow
n an
d qu
aran
tine
seco
ndar
y to
CO
VID
-19
pand
emic
cou
ld h
ave
serio
us c
onse
quen
ces
for w
omen
’s he
alth
mor
e th
an e
ver.
Poor
acc
essi
bil-
ity a
nd lo
w li
tera
cy ra
te to
us
e it
is a
noth
er c
halle
nge
to im
plem
enta
tion
tel-
emed
icin
e in
dev
elop
ing
coun
trie
s
Stev
is-G
ridne
ff, H
arid
asan
i G
upta
, Mon
ica
Pron
czuk
“Cor
onav
irus
Cre
ated
an
Obs
tacl
e Co
urse
for S
afe
Abo
rtio
ns.”
New
s ar
ticle
Hea
lthca
re In
frast
ruct
ure
Euro
peN
/AFo
r man
y w
omen
in E
urop
e se
ekin
g ab
ortio
ns, t
he
COVI
D-1
9 pa
ndem
ic
adde
d an
othe
r obs
tacl
e in
an
alre
ady
com
plic
ated
an
d tim
e-se
nsiti
ve c
ours
e
Fred
eris
ken,
June
202
0“S
tate
Act
ion
to L
imit
Abo
rtio
n A
cces
s D
urin
g th
e CO
VID
-19
Pand
emic
.”
New
s ar
ticle
Hea
lthca
re In
frast
ruct
ure
U.S
N/A
The
resp
onse
to th
e CO
VID
-19
pand
emic
has
pr
ompt
ed s
ever
al s
tate
s to
pla
ce re
stric
tions
that
ha
ve e
ffect
ivel
y ba
nned
or
bloc
ked
the
avai
labi
lity
of
abor
tion
serv
ices
UN
FPA
, Apr
il 20
20“Im
pact
of t
he C
OVI
D-1
9 Pa
ndem
ic o
n Fa
mily
Pl
anni
ng a
nd E
ndin
g G
ende
r-Ba
sed
Viol
ence
, Fe
mal
e G
enita
l Mut
ila-
tion
and
Chi
ld M
arria
ge.”
Repo
rtH
ealth
care
Infra
stru
ctur
eG
loba
lN
/AIf
the
lock
dow
n co
ntin
ues
for 6
mon
ths
and
ther
e ar
e m
ajor
ser
vice
dis
rup-
tions
due
to C
OVI
D-1
9, a
n ad
ditio
nal
7 m
illio
n un
inte
nded
pr
egna
ncie
s ar
e ex
pect
ed
to o
ccur
Inte
rnat
iona
l Pla
nned
Pa
rent
hood
Fed
erat
ion,
A
pril
2020
“CO
VID
-19
Pand
emic
Cut
s A
cces
s to
Sex
ual a
nd
Repr
oduc
tive
Hea
lthca
re
for W
omen
aro
und
the
Wor
ld”
New
s ar
ticle
Hea
lthca
re In
frast
ruct
ure
Glo
bal
N/A
5,63
3 st
atic
and
mob
ile
clin
ics
and
com
mun
ity-
base
d ca
re o
utle
ts h
ave
alre
ady
clos
ed b
ecau
se
of th
e ou
tbre
ak, a
cros
s 64
co
untr
ies.
They
mak
e up
14
% o
f the
tota
l ser
vice
de
liver
y po
ints
IPPF
mem
-be
rs ra
n in
201
8

Page 21 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Get
tlem
an &
Raj
, Jul
y 20
20“8
Hos
pita
ls in
15
h: A
Pr
egna
nt W
oman
’s C
risis
in
the
Pand
emic
.”
New
s ar
ticle
Hea
lthca
re In
frast
ruct
ure
Indi
aN
/AH
er b
aby
was
com
ing,
and
he
r com
plic
atio
ns w
ere
grow
ing
mor
e da
nger
ous.
But n
owhe
re w
ould
take
he
r — a
n in
crea
sing
ly
com
mon
sto
ry a
s In
dia’s
he
alth
car
e sy
stem
buc
k-le
s un
der p
ress
ure
Kum
ari,
Meh
ta, &
Cho
ud-
hary
, Jul
y 20
20“C
OVI
D-1
9 ou
tbre
ak a
nd
decr
ease
d ho
spita
lisa-
tion
of p
regn
ant w
omen
in
labo
ur.”
Peer
revi
ewed
, ret
rosp
ec-
tive
anal
ysis
Hea
lthca
re In
frast
ruct
ure
Indi
aN
/AO
ur in
itial
ana
lysi
s of
w
omen
adm
itted
dur
ing
the
lock
dow
n pe
riod
reve
aled
a 4
3·2%
redu
c-tio
n in
hos
pita
lisat
ion
com
pare
d w
ith th
e co
n-tr
ol p
erio
d an
d a
49.8
%
redu
ctio
n co
mpa
red
with
th
e sa
me
cale
ndar
per
iod
from
the
prev
ious
yea
r. Re
ferr
ed o
bste
tric
em
er-
genc
ies
also
dec
reas
ed
by 6
6.4%
Take
mot
o et
al.
July
202
0“M
ater
nal M
orta
lity
and
COVI
D-1
9.”Pe
er re
view
ed, s
yste
mat
ic
revi
ewH
ealth
care
Infra
stru
ctur
eBr
azil
20Ba
rrie
rs to
acc
ess
heal
th-
care
, diff
eren
ces
in
pand
emic
con
tain
men
t m
easu
res
in th
e co
untr
y an
d hi
gh p
reva
lenc
e of
co
ncom
itant
risk
fact
ors
for C
OVI
D-1
9 se
vere
di
seas
e m
ay p
lay
a ro
le
in th
e ob
serv
ed d
ispa
rity
com
pare
d to
wor
ldw
ide
repo
rts
on m
ater
nal
outc
omes
Rafa
eli &
Hut
chin
son,
June
20
20“T
he S
econ
dary
Impa
cts
of C
OVI
D-1
9 on
Wom
en
and
Girl
s in
Sub
-Sah
aran
A
frica
”
Prep
rint,
rapi
d re
view
Hea
lthca
re In
frast
ruct
ure
Sub-
Saha
ran
Afri
caN
/ATh
ere
is s
tron
g ev
iden
ce to
su
gges
t tha
t wom
en a
nd
girls
in S
SAw
ill s
uffer
from
ext
rem
e an
d m
ultif
acet
ed n
egat
ive
seco
ndar
y im
pact
as
a re
sult
of th
eCO
VID
-19
cris
is

Page 22 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Khal
il et
al.
July
202
0“C
hang
e in
the
Inci
denc
e of
Stil
lbirt
h an
d Pr
eter
m
Del
iver
y D
urin
g th
e CO
VID
-19
Pand
emic
”
Peer
revi
ewed
, ret
rosp
ec-
tive
stud
yH
ealth
care
Infra
stru
ctur
eU
.K33
99Th
e in
cide
nce
of s
tillb
irth
was
sig
nific
antly
hig
her
durin
g th
e pa
ndem
ic
perio
d (n
one
asso
ciat
ed
with
CO
VID
-19)
than
du
ring
the
prep
ande
mic
pe
riod
KC e
t al.
Aug
ust 2
020
“Effe
ct o
f the
CO
VID
-19
pand
emic
resp
onse
on
intr
apar
tum
car
e,
still
birt
h, a
nd n
eona
tal
mor
talit
y ou
tcom
es in
N
epal
: A p
rosp
ectiv
e ob
serv
atio
nal s
tudy
”
Peer
revi
ewed
, pro
spec
tive
obse
rvat
iona
l stu
dyH
ealth
care
Infra
stru
ctur
eN
epal
21,7
63Th
e in
stitu
tiona
l stil
lbirt
h ra
te in
crea
sed
from
14
per
1000
tota
l birt
hs b
efor
e lo
ckdo
wn
to 2
1 pe
r 10
00 to
tal b
irths
dur
ing
lock
dow
n, a
nd in
stitu
-tio
nal n
eona
tal m
orta
lity
incr
ease
d fro
m 1
3 pe
r 10
00 li
vebi
rths
to 4
0 pe
r 10
00 li
vebi
rths
Shuc
hman
, May
202
0“L
ow- a
nd M
iddl
e-In
com
e Co
untr
ies
Face
up
to
COVI
D-1
9.”
New
s ar
ticle
Hea
lthca
re In
frast
ruct
ure
Glo
bal
N/A
On
and
off th
e fro
nt li
nes,
doct
ors
are
wat
chin
g in
ala
rm a
s CO
VID
-19
hits
are
as w
ith v
ulne
r-ab
le p
opul
atio
ns a
nd
fragi
le h
ealth
care
sys
tem
s. Pe
ter H
otez
, Dea
n of
the
Nat
iona
l Sch
ool o
f Tro
pi-
cal M
edic
ine
at B
aylo
r Co
llege
of M
edic
ine
in
Hou
ston
, Tex
as, e
xpec
ts
the
pand
emic
to e
xact
a
bigg
er to
ll in
the
Glo
bal
Sout
h th
an in
Nor
th
Am
eric
a or
Eur
ope,
for
seve
ral r
easo
ns
Bong
et a
l. A
pril,
202
0“T
he C
OVI
D-1
9 Pa
ndem
ic:
Effec
ts o
n Lo
w- a
nd
Mid
dle-
Inco
me
Coun
-tr
ies.”
Peer
revi
ewed
, res
earc
h su
mm
ary
Hea
lthca
re in
frast
ruct
ure
Glo
bal
N/A
In th
e ab
senc
e of
spe
cific
, eff
ectiv
e tr
eatm
ent a
nd
give
n a
lack
of r
esou
rces
in
man
agin
g ac
tive
COVI
D-1
9 pa
tient
s, pr
even
tion
and
early
con
-ta
inm
ent o
f the
dis
ease
ap
pear
to b
e th
e m
ost
feas
ible
opt
ion
for L
MIC
s

Page 23 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Hup
aku
& Pe
tron
golo
, 20
20“C
OVI
D-1
9 an
d G
ende
r G
aps:
Late
st E
vide
nce
and
Less
ons
from
the
UK.
”
Peer
revi
ewed
, res
earc
h-ba
sed
polic
y an
alys
is
and
com
men
tary
Gen
der e
quity
in th
e w
orkf
orce
Uni
ted
King
dom
N/A
The
soci
al d
ista
ncin
g an
d lo
ckdo
wns
ass
ocia
ted
with
the
COVI
D-1
9 cr
isis
ha
s hi
t ser
vice
sec
tors
w
ith fr
eque
nt in
tera
ctio
ns
betw
een
cons
umer
s an
d pr
ovid
ers
whi
ch c
anno
t be
don
e fro
m h
ome.
A
t the
sam
e tim
e, it
has
ad
ded
educ
atio
n an
d ch
ildca
re s
ervi
ces
to p
re-
exis
ting
hom
e pr
oduc
tion
need
s
Robe
rtso
n &
Geb
eloff
, A
pril,
202
0“H
ow M
illio
ns o
f Wom
en
Beca
me
the
Mos
t Ess
en-
tial W
orke
rs in
Am
eric
a.”
New
spap
er a
rtic
leG
ende
r equ
ity in
the
wor
kfor
ceU
nite
d St
ates
N/A
Thou
gh d
eem
ed “e
ssen
-tia
l wor
kers
” dur
ing
the
COVI
D-1
9 pa
ndem
ic,
fem
ale
heal
thca
re
wor
kers
face
ineq
ualit
y w
ith re
gard
s to
wag
es,
reso
urce
allo
catio
n, a
nd
gene
ral r
espe
ct a
nd p
res-
tige
com
pare
d to
thei
r m
ale
coun
terp
arts
Jank
owsk
i et a
l. M
ay, 2
020
“Ris
k St
ratifi
catio
n fo
r H
ealth
care
Wor
kers
dur
-in
g Co
VID
-19
Pand
emic
: U
sing
Dem
ogra
phic
s, Co
-Mor
bid
Dis
ease
and
C
linic
al D
omai
n in
Ord
er
to A
ssig
n C
linic
al D
utie
s.”
Prep
rint l
itera
ture
revi
ewG
ende
r equ
ity in
the
wor
kfor
ceG
loba
lN
/AW
e ha
ve g
ener
ated
a to
ol
whi
ch c
an p
rovi
de a
fra
mew
ork
for o
bjec
-tiv
e ris
k st
ratifi
catio
n of
do
ctor
s an
d he
alth
car
e pr
ofes
sion
als
durin
g th
e CO
VID
-19
pand
emic
Wor
ld H
ealth
Org
aniz
a-tio
n, M
arch
, 202
0“S
hort
age
of P
erso
nal
Prot
ectiv
e Eq
uipm
ent
Enda
nger
ing
Hea
lth
Wor
kers
Wor
ldw
ide.”
New
s re
leas
eG
ende
r equ
ity in
the
wor
kfor
ceG
loba
lN
/ATo
mee
t ris
ing
glob
al
dem
and
for p
erso
nal
prot
ectiv
e eq
uipm
ent
(PPE
), W
HO
est
imat
es th
at
indu
stry
mus
t inc
reas
e m
anuf
actu
ring
by 4
0 pe
r ce
nt

Page 24 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Alo
n et
al.
2020
“The
Impa
ct o
f CO
VID
-19
on G
ende
r Equ
ality
.”W
orki
ng p
aper
Gen
der e
quity
in th
e w
orkf
orce
Uni
ted
Stat
esN
/ATh
e ec
onom
ic d
ownt
urn
caus
ed b
y th
e cu
rren
t CO
VID
-19
outb
reak
has
su
bsta
ntia
l im
plic
atio
ns
for g
ende
r equ
ality
, bot
h du
ring
the
dow
ntur
n an
d th
e su
bseq
uent
reco
very
John
ston
, Moh
amm
ed, &
va
n de
r Lin
den,
202
0“E
vide
nce
of E
xace
rbat
ed
Gen
der I
nequ
ality
in
Chi
ld C
are
Obl
igat
ions
in
Can
ada
and
Aus
tral
ia
Dur
ing
the
COVI
D-1
9 Pa
ndem
ic.”
Peer
revi
ewed
, res
earc
h ar
ticle
Gen
der e
quity
in th
e w
orkf
orce
Cana
da &
Aus
tral
ia77
46H
ouse
hold
s in
Can
ada
and
Aus
tral
ia h
ave
exhi
bite
d si
mila
r tre
nds
in th
e ge
nder
ed a
lloca
tion
of
addi
tiona
l chi
ld c
are
resp
onsi
bilit
ies
resu
lting
fro
m p
olic
y re
spon
ses
to
the
COVI
D-1
9 pa
ndem
ic
Mal
ik &
Nae
em, 2
020
“Impa
ct o
f CO
VID
-19
Pand
emic
on
Wom
en:
Hea
lth, l
ivel
ihoo
ds &
do
mes
tic v
iole
nce.”
Peer
revi
ewed
, pol
icy
revi
ewG
ende
r equ
ity in
the
wor
kfor
cePa
kist
anN
/ATh
e go
vern
men
t sho
uld
map
out
a p
lan
of a
ctio
n to
cou
nter
the
shor
t and
lo
ng-t
erm
effe
cts
of th
e co
rona
viru
s on
wom
en
keep
ing
in v
iew
thei
r he
alth
, liv
elih
oods
, and
do
mes
tic v
iole
nce
UN
Wom
en, M
ay, 2
020
The
Priv
ate
Sect
or’s
Role
in
Miti
gatin
g th
e Im
pact
of
COVI
D-1
9 on
Vul
nera
ble
Wom
en a
nd G
irls
in
Nig
eria
Peer
revi
ewed
, res
earc
h br
ief
Gen
der e
quity
in th
e w
orkf
orce
East
ern
and
Sout
hern
A
frica
N/A
The
Nig
eria
n pr
ivat
e se
ctor
ha
s as
sum
ed a
lead
ing
role
in th
e fig
ht a
gain
st
the
COVI
D-1
9 pa
ndem
ic
in th
e co
untr
y. C
ACO
VID
ai
med
to a
lso
help
mob
i-liz
e pr
ivat
e se
ctor
thou
ght
lead
ersh
ip, r
aise
pub
lic
awar
enes
s an
d bu
y-in
for
COVI
D-1
9 pr
even
tion,
and
pr
ovid
e di
rect
sup
port
to
stre
ngth
en th
e he
alth
-ca
re s
ecto
r’s c
apac
ity to
re
spon
d to
the
cris
is
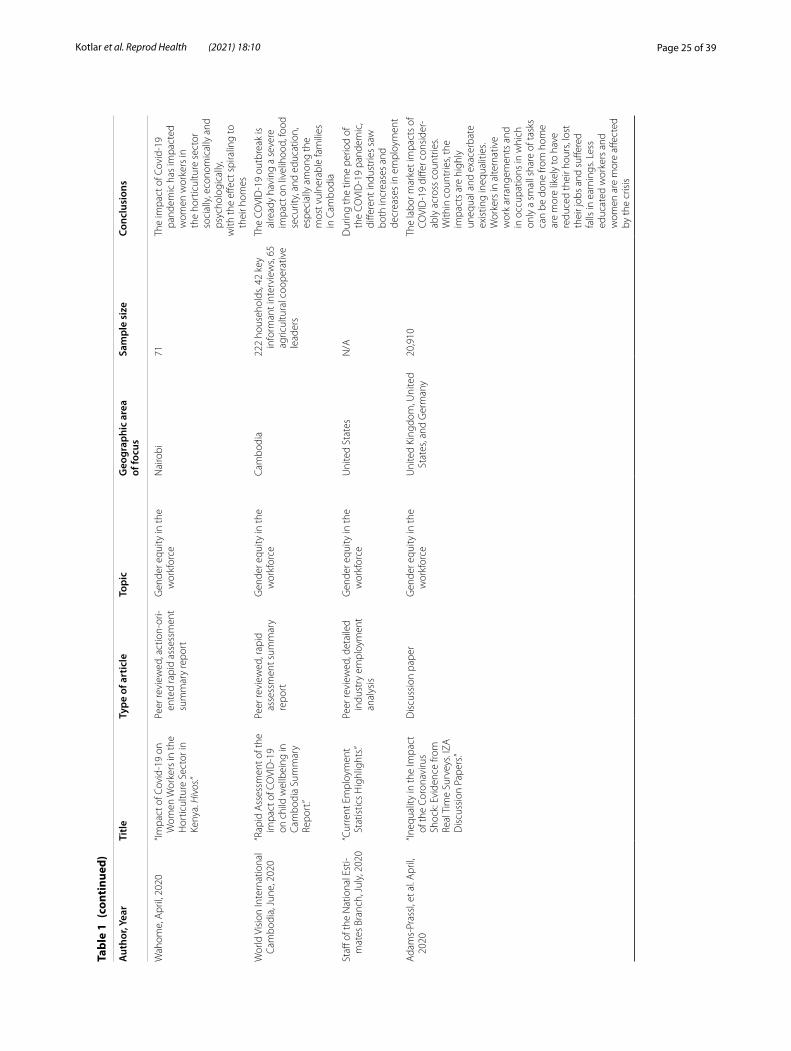
Page 25 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Wah
ome,
Apr
il, 2
020
“Impa
ct o
f Cov
id-1
9 on
W
omen
Wor
kers
in th
e H
ortic
ultu
re S
ecto
r in
Keny
a. H
ivos
.”
Peer
revi
ewed
, act
ion-
ori-
ente
d ra
pid
asse
ssm
ent
sum
mar
y re
port
Gen
der e
quity
in th
e w
orkf
orce
Nai
robi
71Th
e im
pact
of C
ovid
-19
pand
emic
has
impa
cted
w
omen
wor
kers
in
the
hort
icul
ture
sec
tor
soci
ally
, eco
nom
ical
ly a
nd
psyc
holo
gica
lly,
with
the
effec
t spi
ralin
g to
th
eir h
omes
Wor
ld V
isio
n In
tern
atio
nal
Cam
bodi
a, Ju
ne, 2
020
“Rap
id A
sses
smen
t of t
he
impa
ct o
f CO
VID
-19
on c
hild
wel
lbei
ng in
Ca
mbo
dia
Sum
mar
y Re
port
.”
Peer
revi
ewed
, rap
id
asse
ssm
ent s
umm
ary
repo
rt
Gen
der e
quity
in th
e w
orkf
orce
Cam
bodi
a22
2 ho
useh
olds
, 42
key
info
rman
t int
ervi
ews,
65
agric
ultu
ral c
oope
rativ
e le
ader
s
The
COVI
D-1
9 ou
tbre
ak is
al
read
y ha
ving
a s
ever
e im
pact
on
livel
ihoo
d, fo
od
secu
rity,
and
edu
catio
n,
espe
cial
ly a
mon
g th
e m
ost v
ulne
rabl
e fa
mili
es
in C
ambo
dia
Staff
of t
he N
atio
nal E
sti-
mat
es B
ranc
h, Ju
ly, 2
020
“Cur
rent
Em
ploy
men
t St
atis
tics
Hig
hlig
hts.”
Peer
revi
ewed
, det
aile
d in
dust
ry e
mpl
oym
ent
anal
ysis
Gen
der e
quity
in th
e w
orkf
orce
Uni
ted
Stat
esN
/AD
urin
g th
e tim
e pe
riod
of
the
COVI
D-1
9 pa
ndem
ic,
diffe
rent
indu
strie
s sa
w
both
incr
ease
s an
d de
crea
ses
in e
mpl
oym
ent
Ada
ms-
Pras
sl, e
t al.
Apr
il,
2020
“Ineq
ualit
y in
the
Impa
ct
of th
e Co
rona
viru
s Sh
ock:
Evi
denc
e fro
m
Real
Tim
e Su
rvey
s. IZ
A
Dis
cuss
ion
Pape
rs.”
Dis
cuss
ion
pape
rG
ende
r equ
ity in
the
wor
kfor
ceU
nite
d Ki
ngdo
m, U
nite
d St
ates
, and
Ger
man
y20
,910
The
labo
r mar
ket i
mpa
cts
of
COVI
D-1
9 di
ffer c
onsi
der-
ably
acr
oss
coun
trie
s. W
ithin
cou
ntrie
s, th
e im
pact
s ar
e hi
ghly
un
equa
l and
exa
cerb
ate
exis
ting
ineq
ualit
ies.
Wor
kers
in a
ltern
ativ
e w
ork
arra
ngem
ents
and
in
occ
upat
ions
in w
hich
on
ly a
sm
all s
hare
of t
asks
ca
n be
don
e fro
m h
ome
are
mor
e lik
ely
to h
ave
redu
ced
thei
r hou
rs, l
ost
thei
r job
s an
d su
ffere
d fa
lls in
ear
ning
s. Le
ss
educ
ated
wor
kers
and
w
omen
are
mor
e aff
ecte
d by
the
cris
is

Page 26 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Vive
iros
& Bo
nom
i, Ju
ne,
2020
“Nov
el C
oron
aviru
s (C
OVI
D-1
9): V
iole
nce,
Re
prod
uctiv
e Ri
ghts
and
Re
late
d H
ealth
Ris
ks fo
r W
omen
, Opp
ortu
nitie
s fo
r Pra
ctic
e In
nova
tion”
Peer
revi
ewed
, com
men
-ta
ryD
omes
tic v
iole
nce
Glo
bal
Now
is th
e tim
e fo
r vio
lenc
e pr
even
tion
lead
ers
to
advo
cate
for b
old
actio
n.
This
incl
udes
prio
ritiz
ing
the
need
s of
wom
en
(esp
ecia
lly m
inor
itize
d w
omen
) in
med
ical
, soc
ial
and
lega
l set
tings
usi
ng
inno
vativ
e in
terv
entio
n an
d se
rvic
e en
gage
men
t (e
.g.,
e-fil
ing
for p
rote
ctio
n or
ders
, virt
ual a
dvoc
acy
serv
ices
), ur
ging
pol
icy
mak
ers
to p
ass
legi
slat
ion
to s
uppo
rt w
omen
, and
sh
inin
g an
acc
ount
abili
ty
spot
light
on
lead
ersh
ip
Wan
qing
, Mar
ch, 2
020
“Dom
estic
Vio
lenc
e Ca
ses
Surg
e D
urin
g CO
VID
-19
Epid
emic
.”
Mag
azin
e ar
ticle
Dom
estic
vio
lenc
eC
hina
N/A
Rate
s of
dom
estic
vio
lenc
e in
Chi
na in
crea
sed
durin
g th
e CO
VID
-19
pand
emic
, man
y of
whi
ch
wer
e at
trib
utab
le to
th
e ep
idem
ic it
self,
but
du
e to
the
focu
s on
the
pand
emic
, the
nee
ds o
f vi
ctim
s w
ere
negl
ecte
d
Euro
new
s, M
arch
, 202
0“D
omes
tic V
iole
nce
Case
s Ju
mp
30%
dur
ing
Lock
-do
wn
in F
ranc
e.”
New
s ar
ticle
Dom
estic
vio
lenc
eFr
ance
N/A
Dom
estic
vio
lenc
e ca
ses
in F
ranc
e in
crea
sed
follo
win
g th
e on
set o
f a
natio
nwid
e lo
ckdo
wn
due
to C
OVI
D-1
9
UN
Wom
en, A
pril,
202
0“C
OVI
D-1
9 an
d En
ding
Vi
olen
ce a
gain
st W
omen
an
d G
irls.”
Issu
e br
ief
Dom
estic
vio
lenc
eG
loba
lN
/AIt
is c
ritic
al to
add
ress
the
incr
ease
of v
iole
nce
agai
nst w
omen
dur
ing
COVI
D-1
9 th
roug
h ac
cel-
erat
ed a
nd c
once
rted
e
orts
of g
over
nmen
ts,
inte
rnat
iona
l and
nat
iona
l ci
vil s
ocie
ty o
rgan
izat
ions
an
d U
N a
genc
ies.
The
need
s of
wom
en a
nd g
irls
who
face
mul
tiple
form
s of
dis
crim
inat
ion
need
to
be p
riorit
ized

Page 27 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Siga
l, et
al.
Apr
il, 2
020
“‘Ano
ther
Pan
dem
ic’:
In
Latin
Am
eric
a, D
omes
tic
Abu
se R
ises
am
id L
ock-
dow
n.”
New
s ar
ticle
Dom
estic
vio
lenc
eLa
tin A
mer
ica
N/A
Lock
dow
ns a
roun
d La
tin
Am
eric
a ar
e he
lpin
g sl
ow
the
spre
ad o
f CO
VID
-19,
bu
t are
hav
ing
a da
rker
an
d le
ss-in
tend
ed c
onse
-qu
ence
: a s
pike
in c
alls
to
help
lines
sug
gest
s a
rise
in d
omes
tic a
buse
, in
a re
gion
whe
re a
lmos
t 20
mill
ion
wom
en a
nd g
irls
suffe
r sex
ual a
nd p
hysi
cal
viol
ence
eac
h ye
ar
Gra
ham
-Har
rison
, et a
l. M
arch
, 202
0“L
ockd
owns
aro
und
the
Wor
ld B
ring
Rise
in
Dom
estic
Vio
lenc
e.”
New
s ar
ticle
Dom
estic
vio
lenc
eG
loba
lN
/AD
omes
tic v
iole
nce
agai
nst
wom
en a
nd c
hild
ren
has
incr
ease
d as
a re
sult
of
the
quar
antin
e du
ring
the
COVI
D-1
9 pa
ndem
ic
Bosm
an, A
ugus
t, 20
20“D
omes
tic V
iole
nce
Calls
M
ount
as
Rest
rictio
ns
Ling
er: ‘N
o O
ne C
an
Leav
e.’”
New
spap
er a
rtic
leD
omes
tic v
iole
nce
Uni
ted
Stat
esN
/ATh
e co
rona
viru
s ha
s cr
eate
d ne
w te
nsio
ns. S
tayi
ng a
t ho
me
has
wor
sene
d ab
u-si
ve s
ituat
ions
. She
lters
w
orry
abo
ut th
e sp
read
of
the
viru
s
Wom
en’s
Safe
ty N
SW,
Apr
il, 2
020
“New
Dom
estic
Vio
lenc
e Su
rvey
in N
SW S
how
s Im
pact
of C
OVI
D-1
9 on
th
e Ri
se.”
Peer
revi
ewed
, med
ia
rele
ase
Dom
estic
vio
lenc
eA
ustr
alia
80Su
rvey
s of
fron
tline
w
omen
’s do
mes
tic
viol
ence
wor
kers
dur
ing
the
COVI
D-1
9 pa
ndem
ic
reve
al in
crea
sed
over
all
clie
nts
utili
zing
thei
r se
rvic
es, i
ncre
ased
com
-pl
exity
of c
lient
nee
ds,
esca
late
d or
wor
sene
d vi
olen
ce, i
ncre
ased
vi
olen
ce s
peci
fical
ly
rela
ting
to C
OVI
D-1
9,
and
incr
ease
d vi
olen
ce
repo
rted
for t
he fi
rst t
ime

Page 28 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
Nde
di, A
pril,
202
0“F
ram
ewor
k in
End
ing
Viol
ence
Aga
inst
wom
en
and
Girl
s w
ith th
e A
dven
t of t
he C
OVI
D 1
9 fro
m a
n A
frica
n Pe
rspe
c-tiv
e.”
Evid
ence
-bas
ed fr
ame-
wor
kD
omes
tic v
iole
nce
Afri
caN
/ATh
ere
is a
nee
d to
incr
ease
of
kno
wle
dge
and
awar
e-ne
ss-s
uppo
rt fo
r com
mu-
nity
mob
iliza
tion.
It is
als
o im
port
ant t
o en
gage
with
te
leco
m m
obile
com
pa-
nies
to d
eliv
er m
essa
ges
and
prov
ide
serv
ices
like
in
terv
entio
ns c
halle
ngin
g vi
olen
t mas
culin
ities
and
C
SOs
advo
cacy
on
endi
ng
gend
er-b
ased
vio
lenc
e w
ith th
e CO
VID
-19.
Fin
ally
, th
e pr
ovis
ion
of q
ualit
y es
sent
ial s
ervi
ces
adap
ted
to th
e cu
rren
t pan
dem
ic
cont
ext i
s es
sent
ial
Muk
herje
e et
al.
June
, 20
20“V
ulne
rabi
lity
of M
ajor
In
dian
Sta
tes
Due
to
COVI
D-1
9 Sp
read
and
Lo
ckdo
wn.
”
Ana
lysi
s of
sta
te- a
nd
natio
nal-
leve
l hea
lth
data
sou
rces
Dom
estic
vio
lenc
eIn
dia
N/A
Ther
e ar
e m
any
stat
es in
In
dia,
incl
udin
g G
ujar
at,
that
hav
e a
high
er
perc
enta
ge o
f wom
en
expe
rienc
ing
dom
estic
vi
olen
ce w
ith d
runk
ard
husb
and
as c
ompa
red
to
the
natio
nal a
vera
ge. T
he
lock
dow
n is
like
ly to
affe
ct
thes
e se
ctio
ns o
f wom
en
muc
h ad
vers
ely
as th
ey
are
lock
ed a
t hom
e w
ith
thei
r abu
sers
who
are
lik
ely
to g
et m
ore
viol
ent
in th
e ab
senc
e of
liqu
or.
The
Nat
iona
l Com
mis
-si
on fo
r Wom
en (N
CW
) on
17t
h A
pril,
202
0 sa
id it
re
gist
ered
587
dom
estic
vi
olen
ce c
ompl
aint
s be
twee
n M
arch
23
and
Apr
il 16
—a
sign
ifica
nt
surg
e fro
m 3
96 c
om-
plai
nts
rece
ived
in th
e pr
evio
us 2
5 da
ys b
etw
een
Febr
uary
27
and
Mar
ch 2
2

Page 29 of 39Kotlar et al. Reprod Health (2021) 18:10
Tabl
e 1
(con
tinu
ed)
Aut
hor,
Year
Title
Type
of a
rtic
leTo
pic
Geo
grap
hic
area
of
focu
sSa
mpl
e si
zeCo
nclu
sion
s
DeB
olt e
t al.
Nov
embe
r 20
20a
“Pre
gnan
t wom
en w
ith
seve
re o
r crit
ical
cor
ona-
viru
s di
seas
e 20
19 h
ave
incr
ease
d co
mpo
site
m
orbi
dity
com
pare
d w
ith n
onpr
egna
nt
mat
ched
con
trol
s.”
Peer
revi
ewed
, mul
ti-ce
nter
, ret
rosp
ectiv
e,
case
–con
trol
stu
dy
Dire
ct e
ffect
s on
pre
g-na
ncy
38U
.SPr
egna
nt w
omen
with
se
vere
and
crit
ical
cor
o-na
viru
s di
seas
e 20
19 a
re
at a
n in
crea
sed
risk
for
cert
ain
mor
bidi
ties
whe
n co
mpa
red
with
non
preg
-na
nt c
ontr
ols
Zam
bran
o et
al.
Oct
ober
20
20a
“Upd
ate:
Cha
ract
eris
tics
of
Sym
ptom
atic
Wom
en o
f Re
prod
uctiv
e A
ge w
ith
Labo
rato
ry-C
onfir
med
SA
RS-C
oV-2
Infe
ctio
n by
Pre
gnan
cy S
tatu
s—U
nite
d St
ates
, Jan
uary
22
–Oct
ober
3, 2
020”
MM
WR
popu
latio
n, s
ur-
veill
ance
Dire
ct e
ffect
s on
pre
g-na
ncy
400,
000
U.S
In a
n an
alys
is o
f app
roxi
-m
atel
y 40
0,00
0 w
omen
ag
ed 1
5–44
yea
rs w
ith
sym
ptom
atic
CO
VID
-19,
in
tens
ive
care
uni
t adm
is-
sion
, inv
asiv
e ve
ntila
tion,
ex
trac
orpo
real
mem
-br
ane
oxyg
enat
ion,
and
de
ath
wer
e m
ore
likel
y in
pr
egna
nt w
omen
than
in
nonp
regn
ant w
omen
a Stu
dy a
dded
in a
fter
Sep
tem
ber 1
1 to
refle
ct u
pdat
es in
the
know
ledg
e.

Page 30 of 39Kotlar et al. Reprod Health (2021) 18:10
and their children may be at heightened risk for infection with SARS-CoV-2 [2].
In general, pregnant individuals with COVID-19 do not seem to display more severe disease symptoms than non-pregnant individuals. Most cases among pregnant people are asymptomatic or mildly symptomatic [6]. For symp-tomatic cases, the most common clinical presentations included fever, cough, and dyspnea [7–11]. Laboratory findings consistently included lymphopenia, leukopenia, thrombocytopenia, and elevated levels of C-reactive pro-tein and transaminases [7, 12–14]. Others reported an increased D-dimer level and neutrophil/lymphocyte ratio and a decreased white blood cell count [8, 9]. Chest com-puted tomography (CT) scans revealed abnormal imag-ing features, namely ground-glass opacities, in the lungs of pregnant individuals with COVID-19 [7, 10, 15], but the clinical significance of these imaging findings and the laboratory parameters is not clear.
Adverse outcomes resulting from maternal infection with SARS-CoV-2 during pregnancy are infrequent. In studies from January to September 2020, most cases of COVID-19 among pregnant individuals documented during surveillance in the United States did not progress to severe disease, and intensive care unit (ICU) admission involving mechanical ventilation was seldom required [6]. Results were similar in two studies of pregnant women admitted hospitals in China [7, 16]. However, recently two studies have contradicted these early results. A multicenter, retrospective case control study published in November 2020 compared pregnant women admitted in Philadelphia for severe or critical coronavirus disease to reproductive-aged nonpregnant women admitted for severe or critical coronavirus disease found that preg-nant participants were more likely to be admitted to the ICU, to be intubated, to require mechanical ventilation, and were at increased risk of composite morbidity [17]. Similarly, an analysis of 400,000 women in the United States between 15 and 44 years of age with symptomatic COVID-19 published in October 2020 found that preg-nant women were more likely to experience ICU admis-sion, intubation, mechanical ventilation, and death [18].
Publications including data from a variety of contexts and designs found that the most commonly reported adverse outcome was preterm delivery [11–13, 19]; and increased prevalence of low birthweight and Cesarean-section (C-section) delivery were also observed [10, 20]. Other obstetric complications and outcomes including maternal death, stillbirth, miscarriage, preeclampsia, fetal growth restriction, coagulopathy, and premature rupture of membranes were rare, but apparent [8]. Epide-miological studies did not show that COVID-19 directly increased risks for these outcomes, although a study in London [21] suggests that stillbirths may become more
common as a direct or indirect consequence of the pan-demic. A prospective cohort study by Mendoza et al. found that pregnant individuals with severe COVID-19 may develop a preeclampsia-like syndrome with-out abnormal ratios of soluble fms-like tyrosine kinase 1 to placental growth factor (sFlt-1/PIGF) and uterine artery pulsatile index (UtAPI) scores typical of normal preeclampsia [22]. Placental infection with the virus was observed; however, these cases were largely asymp-tomatic or mildly symptomatic [23, 24]. In a review of cases, Golden and Simmons hypothesized that these pla-cental abnormalities were not a direct result of COVID-19 infection [25].
Intrauterine transmissionThe literature on maternal–fetal transmission of SARS-CoV-2 is highly speculative and requires additional evidence to confirm postulated mechanisms of trans-mission. Thus far, studies do not support intrauterine infection with COVID-19 resulting from vertical trans-mission in pregnant individuals with clinically or micro-biologically diagnosed cases of the virus during the third trimester [14, 26–28]. Few cases of neonatal infection potentially acquired in utero were observed. For example, samples from six pregnant women with COVID-19 and their neonates in Wuhan, China were tested, and SARS-CoV-2 RNA was undetectable in samples of cord blood, throat and nasopharyngeal swabs, urine, feces, amniotic fluid, and placental tissue [14, 29, 30]. Yet, the reliability of these positive neonatal test results was questioned as tests were not performed immediately following deliv-ery. Elevated IgM antibodies in neonates with SARS-CoV-2 infection born to SARS-CoV-2-positive mothers were identified at two hospitals in Wuhan, China [31, 32] However, Kimberlin and Stagno raised doubts about intrauterine transmission as IgM antibodies are too large to cross the placenta. Also, IgM assays used to diagnose congenital infection are often unreliable [33]. Low lev-els of SARS-CoV-2 RNA were found in blood samples collected in two large cohort studies in Wuhan, China [34, 35]. The occurrence of placental infection with the virus [23, 24] and the presence of COVID-19 antibodies in neonatal blood suggest some mechanism of vertical transmission [25].
Despite this, transmission of the virus through blood is questionable. Egloff et al. hypothesized that transcytosis (transcellular transport) of the virus, infected blood cell transport, and virus or infected cells in the cervicovagi-nal compartment were unlikely avenues for transmission in most pregnant women with COVID-19. According to these data, the maternal–fetal transmission risk is probably very low, possibly under 1% following mater-nal SARS-CoV-2 infection during pregnancy [36]. Yet,

Page 31 of 39Kotlar et al. Reprod Health (2021) 18:10
it is widely recognized that further research involving larger population-based longitudinal studies is needed to determine the plausibility of incidental maternal–fetal transmission.
Labor and deliveryA few case series including an analysis of 108 births occurring in New York City, suggest no increased risk of infection for the neonate when birth occurs vagi-nally. Despite early reassuring evidence that there is no increased risk of infection for the neonate when birth occurs vaginally [37], clinical guidelines differ in their recommendations on mode of delivery [38, 39].
Estimates of C-section rates among women infected with SARS-CoV-2 differed but suggest a potentially sig-nificant increase in operative delivery. A systematic review conducted by Della Gatta et al. reported that 90.2% of women diagnosed with COVID-19 delivered via C-section [40] A systematic review by Zaigham and Andersson reported 91% of the women delivered via C-section [41] This is similar to early estimates from Wuhan, China; Chen et al. found a C-section occurrence of 93% [42]. The reasons for this practice are unclear, but it may be attributable to more aggressive management of labor and delivery during the onset of the pandemic. However, a recent analysis of women delivering at New York City hospitals between March 8 and April 2, 2020 found C-section rates not higher than average (31.3% for women with confirmed COVID-19, compared to 33.9% of those who tested negative) [43]. Some scien-tists and healthcare providers speculated that C-section rates are reduced in LMICs due to indirect impacts of the COVID-19 pandemic on the healthcare system [44]. As of the completion of this paper, no evidence to support this exists.
Particularly in the beginning of the pandemic, hos-pitals implemented policies regarding support persons and postpartum stays that isolated women during labor and delivery. A comprehensive review of care guidelines from international perinatal societies and institutions found that most either recommended no visitors or one asymptomatic support person, and expedited discharge was recommended by the American College of Obstet-rics and Gynecology, the Catalan Health Service, and the Society for Maternal and Fetal Medicine [45]. Given the documented benefits of labor support [46], reducing access may increase the incidence of C-section delivery and decrease maternal satisfaction with labor and deliv-ery experiences. Furthermore, expedited discharge may reduce the ability of healthcare providers to identify and treat postpartum complications.
Breastfeeding and infant contactThe possibility of transmission of novel coronavirus through breast milk is unclear. The published evidence on the presence of SARS-CoV-2 in breastmilk consisted of case reports and case series of postpartum women who tested positive for the coronavirus during pregnancy. Of milk samples collected from 37 women, the majority tested negative for SARS-CoV-2 [26, 32, 39, 47, 48], with the exceptions of Zhu et al. and Wu et al. who found one positive sample among 5 samples from 5 women [49], and among 3 samples from 3 women, respectively [37]. These preliminary findings suggested that transmission of SARS-CoV-2 through breast milk was unlikely.
Dong et al. reported the presence of IgG and IgA SARS-CoV-2 antibodies in breast milk samples taken from a woman with a positive throat swab test for COVID-19 [50]. This suggested that breast milk could have protec-tive effects against infection with COVID-19, though more evidence is needed for confirmation.
Public health and medical organizations released guid-ance regarding breastfeeding for mothers with confirmed SARS-CoV-2 infection that weighed infection risk with the known and documented benefits of breastfeeding and early bonding. The WHO and UNICEF recommended continued breastfeeding, rooming in, skin to skin contact, and kangaroo care utilizing infection control practices. Specifically, the “WHO recommends that mothers with suspected or confirmed COVID-19 should be encour-aged to initiate or continue to breastfeed. Mothers should be counselled that the benefits of breastfeeding substan-tially outweigh the potential risks for transmission.” In contrast, the Centers for Disease Control and Prevention, while encouraging the continuation of breastfeeding in general, stated, “temporary separation of the newborn from a mother with confirmed or suspected COVID-19 should be strongly considered to reduce the risk of trans-mission to the neonate” [51].
Mental healthPregnant women and new mothers are more likely to experience mental illness than non-pregnant individuals [52]. Several COVID-19-related studies in India, China, and Italy of the intrapartum and postpartum periods considered clinically relevant anxiety and depression and their symptoms through self-reports and clinical assess-ments. Additional maternal mental health issues includ-ing substance use disorders and hostility aggression have yet to be studied in depth.
The pandemic significantly impacted maternal mental health. Feelings of anxiety and depression were associ-ated with maternal fear of vertical transmission of the virus to their infants, limited accessibility of antenatal

Page 32 of 39Kotlar et al. Reprod Health (2021) 18:10
care resources, and lack of social support [53, 54]; these experiences also created a source of stress for pregnant and postpartum women without COVID [27, 55]. Social distancing and isolation/quarantine procedures imple-mented during the pandemic increased risk of psy-chological problems among pregnant women and new mothers [53–55].
During pregnancy, self-reported rates of clinically rel-evant anxiety and depressive symptoms were higher among pregnant women relative to their retrospectively self-assessed pre-pandemic levels and when compared to non-pregnant individuals in a multicenter cross-sectional study performed in China by Y. Wu et al. In the same study, thoughts of self-harm were also more frequent than before the pandemic [52]. Additionally, based on a small case series, Kotabagi et al. proposed a positive cor-relation between both clinically relevant maternal anxi-ety and depression and the number of COVID-19-related deaths in the population [56]. The unpredictability of COVID-19, along with deprivation of social and family support, increased perinatal distress [57]. A global sur-vey of pregnant and postpartum women by Koenen and colleagues found that 40% of women screened positive for post-traumatic stress disorder (PTSD); over 70% of women also reported clinically significant depression or anxiety [58]. These findings are highly plausible, but must be seen against the background that carefully controlled epidemiological studies are scarce. To establish time trends in psychiatric or trauma prevalence is notoriously difficult as the same population must be assessed with the same measures in the same setting before and during the crises.
The postpartum period was less well-studied than the intrapartum period. Several authors speculated that lim-ited health resources and increased prevalence of home deliveries without trained obstetric clinicians contributed to depression and distress among all pregnant women and new mothers [53, 59]. Jungari reasoned that height-ened levels of clinically relevant depression likely arose from maternal fear of infection for both themselves and their infants, social isolation, and uncertainty surround-ing viral spread, but empirical evidence was lacking [54].
Prenatal and postnatal careThe COVID-19 pandemic required postponement of many non “essential” health services to prevent transmis-sion within clinics, which led to significant reductions in the obtention of antenatal and postnatal care. In the US, an online survey of 4451 pregnant women found nearly a third reported elevated levels of stress, with alterations to prenatal appointments cited as a major reason for this elevation. [60]. A modelling study on the indirect effects of the pandemic in 118 LMIC estimated a reduction in
antenatal care by at least 18%, and possibly up to 51.9%, and a similar reduction in postnatal care [61].
This estimate was supported by countries’ changes in perinatal care guidelines [62]. A consultant Obstetrician and Gynecologist at the Lagos University Teaching Hos-pital stated that those in early pregnancy were urged to come in once in eight weeks rather than once in four, and the number of antenatal care visits decreased from 10 to 15 to an average of 6 [63]. Women also chose to forego visits due to lack of transportation, familial pressure to isolate, and personal fears of the virus [64]. Mater-nal health workers, such as midwives in Kenya, Uganda and Tanzania, reported low numbers attending mater-nal health clinics, and more women coming into hospi-tals late, without sufficient antenatal care [65]. A survey by the Population Council sampling heads of households across five Nairobi urban slums found that 9% of partici-pants forewent health services such as antenatal care and immunization/nutrition services for children [66]. Fur-ther, a rapid gender analysis by CARE West Africa found consistent reports of false rumors about the virus and a general mistrust of health workers, leading to some men, especially in rural areas, forbidding their wives from seeking health services. In Mali, most female respondents said they were not accessing health services, out of fear of the virus and confusion about which services were still being offered [67].
A global, cross-sectional study of maternal and new-born health professionals by Semaan et al. found a sig-nificant reduction in antenatal care services utilized as clinics reduced hours, number of visitors permitted, and in-person visits during pregnancy [68]. In some areas of the UK, women were provided with blood pressure machines and urinalysis sticks to conduct their own antenatal checks. Some antenatal care was offered via telemedicine, however this varied regionally. Respond-ents from the UK expressed concerns about the impacts of reduced contact on the quality of maternity care, and participants in LMICs recognized women’s inadequate access to communication infrastructure, as telehealth was far more elusive in rural areas, particularly for women [69, 70].
Healthcare infrastructureThe temporary closure of outpatient clinics during shel-ter at home orders left many women without access to time-sensitive maternal and reproductive health care, from routine gynecological checkups to prenatal care to abortion. Classifying abortion care as “non-essential” severely restricted access regionally or nationwide in many countries during periods of lockdown [71, 72]. The UN Population Fund estimates that if COVID-19 related disruption continued for 6 months, 47 million women in

Page 33 of 39Kotlar et al. Reprod Health (2021) 18:10
114 LMIC will be unable to use modern contraceptives, and an additional 7 million unintended pregnancies will occur globally [73]. Beyond temporary measures, many clinics closed their doors entirely. By April, 5,633 static and mobile clinics and community-based care outlets closed across 64 countries, according to an International Planned Parenthood Federation survey of its national members [74]. Facilities that remained open were over-whelmed, particularly in LMICs, where many hospitals were already overcrowded. Further, pregnant individuals in many LMICs, with particularly dire numbers in India, were turned away from hospitals or denied ambulances and forced to endure labor on the streets or at home [75, 76]. To mitigate this, hospitals limited the number of peo-ple per room and the duration of their stay and reduced postpartum stays. However, this mitigation could nega-tively impact access to and quality of care.
Semaan et al. revealed that many maternal and new-born healthcare providers worldwide did not receive training in COVID-19 from their health facility, and 53% of participants in LMICS and 31% in HICs did not feel knowledgeable in how to care for a COVID-19 maternity patient; 90% of participants reported higher stress levels [68]. This lack of training and confidence hindered qual-ity of care, with the additional burden of staff and supply shortages. Supply chain breakdowns have left many facil-ities without access to medications or blood products, which are critical to treating postpartum hemorrhage [70, 73, 74].
While some maternal deaths observed during the pan-demic were directly caused by COVID-19, a significant portion may have been attributable to underlying fac-tors. Using evidence from a case series of 20 COVID-19-related maternal deaths, Takemoto et al. proposed that inadequacy of the Brazilian healthcare system was responsible for Brazil’s high rate of maternal mortality [77]. In Brazil, antenatal care resources were already lim-ited, and even fewer were available during the pandemic as many were repurposed for the care of COVID-19 patients. Likewise, the system failed to address existing public health issues which increased the risk of mater-nal mortality resulting from COVID-19 among pregnant individuals. Women and girls in Sub-Saharan Africa were also expected to experience significant secondary conse-quences from the COVID-19 pandemic, leading to a rise in maternal mortality during the pandemic. [78].
Studies in both Nepal and the United Kingdom of preg-nant individuals found the incidences of stillbirth and neonatal mortality were significantly higher during the pandemic period than the pre-pandemic period. Those experiencing stillbirth and infant mortality did not show symptoms of COVID-19, suggesting these outcomes may instead be due to the reallocation of medical resources
towards COVID-19 patients and the subsequent reduc-tion in hospitalization for labor management and peri-natal care visits [79, 80]. Likewise, another observation is attributed to reduced care: the consistent reductions in preterm birth were seen across various time windows surrounding the implementation of COVID-19 mitiga-tion measures in different countries such as Netherlands, Ireland and Denmark [81] Authors discussed reduced air pollution and maternal stress during pregnancy as poten-tial causal factors; however, a large minority of preterm births, was iatrogenic, suggesting healthcare provider behavior may be a contributing factor. When routine pre-pandemic care was offered, obstetricians may have induced delivery more often due to more close surveil-lance of pregnancies, usually for maternal or fetal health concerns (e.g. following deviations in cardiotocogra-phy). Delivery is more likely to be induced late-preterm, which in the study accounted for all of the prevalence differences [81]. Changes in care-seeking behavior and care availability due to the COVID-19 pandemic may in some contexts lead to potential improved outcomes (reduced preterm delivery), however, this may come with an increase in stillbirth. It is certainly is a major research challenge with potential lessons for obstetric care.
The long-term impacts of the COVID-19 pandemic on maternal health were yet to be determined, but modelling studies indicated potentially grim outcomes particularly for LMICs. Weak healthcare systems in these countries were unable to mount the necessary response to the pan-demic, which allowed the virus to spread rapidly [82]. The public health and healthcare sectors in LMICs were chronically under-funded and under-resourced, leaving them ill-prepared to meet the demands of the pandemic and implement the response measures recommended by leading public health organizations [83]. These shortcom-ings of the healthcare systems in LMICs threatened both the physical and mental health of pregnant and postpar-tum people.
Gender equity in the workforceThe social distancing and lockdown measures of the COVID-19 pandemic caused significant consequences for business sectors where interactions between indi-viduals were frequent and often unavoidable. Women were over-represented in these industries; data from the UK Labour Force Survey revealed that approxi-mately 46% and 39% of working women and men, respectively, were employed in critical sectors, while 19% and 13%, respectively, were employed in locked-down sectors [84]. Safety measures to reduce viral spread revealed that many jobs could be carried out remotely; however, certain essential positions required employees to continue to show up in-person and risk

Page 34 of 39Kotlar et al. Reprod Health (2021) 18:10
exposure. While there was a lack of research on wom-en’s role as essential workers, 2019 research by Boniol et al. found that women comprise 70% of the healthcare workforce worldwide [85]. A New York Times analy-sis of US census data crossed with the federal govern-ment’s essential worker guidelines also found that 1 in 3 jobs held by women were designated as essential [86].
While working an essential job provided job security, it also increased the risk of SARS-CoV-2 transmission, particularly in the healthcare workforce, given the high contact nature of medical care, the higher risk individu-als who sought it, and the lack of PPE many hospitals faced [87, 88]. Data show that women tend to bear a larger burden than men of addressing household needs and providing childcare [89]. The burden of domestic work has increased during the Covid-19 pandemic. Approximately nationally representative survey data from Canada and Australia revealed the average Cana-dian woman with children spent nearly 50 more hours per week on childcare during the pandemic than did the average man, and the average Australian woman with children spent nearly 43 more hours on childcare. Although this disparity in unpaid care work existed prior to the pandemic, childcare needs have increased for many households [90].
In LMICs, the majority of employed women worked in the informal sector, where they did not have access to services such as paid sick leave, maternity leave, or unemployment benefits [61, 91]. Data from UN Women has found that in Kenya, 60 percent of all job losses recorded since the crisis were held by women [92]. Fur-ther, a rapid qualitative assessment by Hivos East Africa found that thousands of females, who are often the main household earners in East Africa, have been laid-off due to the pandemic [93], and surveys by Population Coun-cil and World Vision International Cambodia found that a higher percentage of women than men have completely lost their income or earning potential [66, 94].
In several but not all HICs, women were still more likely to become unemployed during the COVID-19 cri-sis. The U.S. Bureau of Labor Statistics reported that in April 2020 alone, women accounted for 55% of the 20.5 million jobs lost in America, and that job loss was more prevalent and occurred at a more rapid rate for women than men [95]. A study by Adams-Prassl et al. on large geographically representative samples of individuals in the US, UK, and Germany found that in the UK and US, women faced a higher likelihood than men of losing their jobs or report lower earnings during the pandemic in comparable jobs, even when controlling for job char-acteristics such as college degree [96]. Conversely, gen-der did not serve as a significant predictor of job loss in Germany.
Domestic violenceLockdown measures required individuals to stay inside for extended periods of time, and early data demon-strated notable spikes in domestic violence (DV). Police data were consulted as evidence of increased violence, and surges in DV cases were noted in several countries [97–101]. In addition, DV hotlines and charities in many countries also experienced higher influxes of calls since January 2020 [97, 98, 100, 102, 103]. Non-representative surveys from Women’s Safety New South Wales and Foundation Lance d’Afrique Burundi revealed increased requests for help by survivors to female frontline workers [104, 105]. The Chief Justice of Kenya announced that in the first two weeks of April alone, gender-based violence cases increased by over a third [78]. Similarly, data from India’s National Commission for Women shows that domestic violence complaints more than doubled after Prime Minister Modi announced lockdown on March 24, 2020 [92].
There is a lack of representative epidemiological data on increased DV, and the existing data did not specify if the victims were pregnant or mothers. The breadth of reported cases is alarming, and this increase in DV is expected to be detrimental to maternal health outcomes [105–107]. The actual number of DV incidents is likely higher than reported as lockdown measures and fears of virus spread limited community support for women seeking freedom from abusers [101, 108, 109].
DiscussionThis study represents a comprehensive scoping review of the direct and indirect impacts of the COVID-19 pan-demic on maternal health. By using broad search terms and inclusion criteria, we were able to review literature on social and economic impacts of the pandemic as well as the physical and mental health impacts. However, this study did not include literature in languages other than English, which likely skews results towards countries in which English is the primary language. It was diffi-cult to locate published information on LMICs pertain-ing to maternal health. We attempted to mitigate this by including grey literature and news articles from a variety of sources. Finally, while a scoping review methodology allowed us to rapidly synthesize literature, it does not represent as rigorous a process as a systematic review or meta-analysis.
While early results suggested otherwise, recent studies with large sample sizes utilizing control groups suggest that pregnant people experiencing symptoms of COVID-19 are at higher risk of adverse outcomes than those who are not pregnant [17, 18]. Additionally, the non-medical impact of the COVID-19 pandemic is already apparent in this vulnerable population. While short and

Page 35 of 39Kotlar et al. Reprod Health (2021) 18:10
medium-term consequences of these impacts are emerg-ing, the long-term consequences are currently unknown and will require careful research to be elucidated.
To date, studies of the effects of the COVID-19 pan-demic have, perhaps understandably, given time con-straints and availability of data, lacked rigorous methods. To adequately assess these effects, we require research that carefully controls for pre-COVID-19 levels of the different outcomes of interest (e.g. depressive symptoms, C-Section) and population characteristics (e.g. comor-bidity, socio-economic status) to more validly assess time trends. While reducing the frequency of prenatal visits in high income countries (HIC) may not necessar-ily be associated with worse birth outcomes, reducing the basic antenatal care in low- and middle-income countries (LMIC) is likely to impact maternal and neonatal health [110, 111]. Continued surveillance and reporting are critical to ascertain whether maternal mortality and mor-bidity have increased during the pandemic and which populations were affected most severely.
The Covid-19 pandemic has created a multitude of questions regarding the optimal policies to reduce the spread of SARS-Cov-2 while minimizing the unintended detrimental consequences to family wellbeing and gender equity. Salient among these are: in what circumstances should schools and daycares resume care and in what format? Which models of antenatal and delivery care produce optimal outcomes? Which economic relief poli-cies protect gender equity in the workplace and family wellbeing? Heterogeneous and inconsistent application of policies and models for healthcare and childcare deliv-ery both within and across countries, while potentially not ideal for pandemic response, provide a near-natural experiment that helps to explore these questions.
At the same time, policies impacting pregnant and parenting people have been implemented with little evidence. Several of these policies have the potential to significantly harm pregnant individuals’ health and undermine their rights. Most concerning are those that limit emotional support during labor and delivery, man-date early infant separation, and shorten postpartum stays. While the clinical rationale behind high C-sec-tion rates among pregnant individuals diagnosed with Covid-19 are unclear, these rates are alarming given that no evidence exists that C-section delivery lowers risk of transmission of SARS-CoV-2 or improves maternal health [81, 112].
These concerns lead us to provide several clear policy recommendations we believe either have sufficient evi-dence to merit implementation or must be pursued because of ethical and human rights considerations. The first two pertain to healthcare policy. Given the evidence on the paucity of severe outcomes from SARS-CoV-2
infection in newborns, we urge the CDC to align with the WHO’s strong recommendation to keep the mother/infant dyad together even if the mother has a confirmed infection of SARS-CoV-2. Precautions, of course, are warranted, but our opinion is that the overwhelming evi-dence behind the benefits of early bonding and breast-feeding outweigh the risk of infection in the newborn.
Second, whenever possible, healthcare organizations should consider the mental health impacts of any poli-cies implemented to reduce risk of transmission. Early and convincing evidence currently exists that mater-nal mental health issues have increased during the pan-demic. Policies that limit or eliminate the ability to give birth with a support person present or that are likely to increase distress, potentially exacerbating underly-ing mental health issues, should be avoided. With many healthcare organizations shortening postpartum hospital stays or providing postpartum visits through telemedi-cine, there is also the risk that screening for postpartum depression or other mental health issues will be forgotten or glossed over. Healthcare providers should be vigilant of the increased mental health needs of their pregnant and parenting patients.
Finally, daycare and school closures are causing incred-ible stress and destabilization to caregivers, especially women, who often bear the brunt of childcare duties. These closures along with other workplace related con-sequences of the pandemic pose a serious threat to gen-der equity in the workforce. Without serious mitigation through policy, this threat is potentially far-reaching. We strongly recommend that governments prioritize the resumption of schooling under safe conditions and child-care when easing shelter in place or other pandemic-related restrictions. Failure to do so is likely to worsen any short-term losses in women’s employment given women’s disproportionate burden of childcare, and to put vulnerable single-mother and low income households at risk of poverty and food insecurity.
ConclusionWhile rigorous studies have not yet been conducted, early evidence from this scoping review shows that many of the social and economic consequences of the COVID-19 crisis likely affect women more than men. The low risk of mother to child transmission in-utero or via breast milk is well documented. It seems that pregnancy may constitute a particularly vulner-able period for COVID-19, but this requires further confirmation through well designed and implemented research. An increased risk of distress and psychiatric problems during pregnancy and postnatally during the pandemic is likely, but also in this case high-quality evi-dence is lacking. Likewise, a rise in the prevalence of

Page 36 of 39Kotlar et al. Reprod Health (2021) 18:10
domestic violence is plausible and supported by several studies, but we need more representative data. Stud-ies of maternal morbidity and mortality are also lack-ing. Rigorous epidemiological studies must document the health impact of infection with SARS-CoV-2 dur-ing pregnancy as well as the changes in health care service and accessibility and their impact on maternal health. This review, however, provides good evidence that mothers with children are more likely to suffer job and income losses during the pandemic than men and women without children. Single mothers in particular are likely to suffer from food insecurity. These socio-economic consequences for women are similar across many high- and low-income countries.
Supplementary InformationThe online version contains supplementary material available at https ://doi.org/10.1186/s1297 8-021-01070 -6.
Additional file 1. Pubmed MeSH Terms Utilized for Peer-Reviewed Articles.
AbbreviationsCOVID-19: Coronavirus Disease 2019; DV: Domestic violence; LMIC: Low- and middle-income countries; HIC: High income countries; PTSD: Post-traumatic stress disorder; C-section: Cesarean section; SARS-CoV-2: Severe acute respira-tory syndrome coronavirus 2.
AcknowledgementsNone.
Authors’ contributionsBK designed the study, reviewed literature, and drafted the manuscript. EG and SP retrieved and summarized the literature, reviewed the literature and drafted the manuscript. AL advised on the review and reviewed the final manuscript. HT designed the study, supervised the review process and reviewed the draft and final manuscripts. All authors read and approved the final manuscript.
FundingThis project was supported by the Health Resources and Services Adminis-tration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number and title for grant amount (T76 MC000010, Maternal and Child Health Training Grant). This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
Availability of data and materialsFull review algorithm will be made available.
Ethics approval and consent to participateNot applicable in review.
Consent for publicationNot applicable in review.
Competing interestsThe authors declare that they have no competing interests.
Author details1 Harvard T.H. Chan School of Public Health, Boston, MA, USA. 2 George Wash-ington University, Washington, DC, USA. 3 Brown University, Providence, Rhode
Island, USA. 4 Department of Social and Behavioral Science, Harvard T.H. Chan School of Public Health, 677 Huntington Ave., Boston, MA 02115, USA.
Received: 13 October 2020 Accepted: 4 January 2021
References 1. WHO Coronavirus Disease (COVID-19) Dashboard | WHO Coronavirus Dis-
ease (COVID-19) Dashboard. (n.d.). Retrieved December 29, 2020, https ://covid 19.who.int/table
2. Muralidar S, Ambi SV, Sekaran S, Krishnan UM. The emergence of COVID-19 as a global pandemic: Understanding the epidemiol-ogy, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie. 2020;179:85–100. https ://doi.org/10.1016/j.bioch i.2020.09.018.
3. Pradhan A, Olsson P-E. Sex differences in severity and mortality from COVID-19: are males more vulnerable? Biol Sex Differ. 2020. https ://doi.org/10.1186/s1329 3-020-00330 -7.
4. Arksey H, O’Malley L. Scoping studies: towards a methodological frame-work. Int J Soc Res Methodol. 2005;8(1):19–32.
5. Braun V, Clarke V. What can “thematic analysis” offer health and wellbe-ing researchers? Int J Qual Stud Health Well-Being. 2014. https ://doi.org/10.3402/qhw.v9.26152 .
6. Delahoy MJ. Characteristics and Maternal and Birth Outcomes of Hospitalized Pregnant Women with Laboratory-Confirmed COVID-19—COVID-NET, 13 States, March 1–August 22, 2020. Morbidity and Mortality Weekly Report: MMWR; 2020. p. 69.
7. Wu C, Yang W, Wu X, Zhang T, Zhao Y, Ren W, Xia J. Clinical manifesta-tion and laboratory characteristics of SARS-CoV-2 infection in pregnant women. Virologica Sinica. 2020;35(3):305–10. https ://doi.org/10.1007/s1225 0-020-00227 -0.
8. Xu L, Yang Q, Shi H, Lei S, Liu X, Zhu Y, Wu Q, Ding X, Tian Y, Hu Q, Chen F, et al. Clinical presentations and outcomes of SARS-CoV-2 infected pneumonia in pregnant women and health status of their neonates. Sci Bull. 2020. https ://doi.org/10.1016/j.scib.2020.04.040.
9. Smith V, Seo D, Warty R, Payne O, Salih M, Chin KL, Ofori-Asenso R, et al. Maternal and Neonatal Outcomes Associated with COVID-19 Infec-tion: a Systematic Review. PLoS ONE. 2020;5(6):e0234187. https ://doi.org/10.1371/journ al.pone.02341 87.
10. Knight M, Bunch K, Vousden N, Morris E, Simpson N, Gale C, O’Brien P, Quigley M, Brocklehurst P, Kurinczuk JJ. Characteristics and Outcomes of Pregnant Women Admitted to Hospital with Confirmed SARS-CoV-2 Infection in UK: National Population Based Cohort Study. BMJ. 2020;369:2107. https ://doi.org/10.1136/bmj.m2107 .
11. Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, Kew T, Debenham L, Llavall AC, Dixit A, Zhou D, Balaji R, Lee SI, Qiu X, Yuan M, Coomar D, van Wely M, van Leeuwen E, Kostova E, Kunst H. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020. https ://doi.org/10.1136/bmj.m3320 .
12. Pereira A, Cruz-Melguizo S, Adrien M, Fuentes L, Marin E, Perez-Medina T. Clinical Course of Coronavirus Disease-2019 in Pregnancy. Acta Obstetricia et Gynecologica Scandinavica. 2020;99(7):839–47. https ://doi.org/10.1111/aogs.13921 .
13. Blitz MJ, Rochelson B, Meirowitz N, Prasannan L, Rafael TJ, et al. Maternal mortality among women with coronavirus disease 2019. Am J Obstetr Gynecol. 2019. https ://doi.org/10.1016/j.ajog.2020.06.020.
14. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, Li J, Zhao D, Xu D, Gong Q, Liao J, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospec-tive review of medical records. Lancet. 2020;395(10226):809–15. https ://doi.org/10.1016/S0140 -6736(20)30360 -3.
15. Yang H, Sun G, Tang F, Peng M, Gao Y, Peng J, Xie H, Zhao Y, Jin Z. Clini-cal features and outcomes of pregnant women suspected of coronavi-rus disease 2019. J Infect. 2020;81(1):e40-44. https ://doi.org/10.1016/j.jinf.2020.04.003.
16. Khan S, Peng L, Siddique R, Nabi G, Xue M, Liu J, Han G. Impact of COVID-19 infection on pregnancy outcomes and the risk of maternal-to-neonatal intrapartum transmission of COVID-19 during natural

Page 37 of 39Kotlar et al. Reprod Health (2021) 18:10
birth. Infect Control Hosp Epidemiol. 2020;41(6):748–50. https ://doi.org/10.1017/ice.2020.84.
17. DeBolt CA, Bianco A, Limaye MA, Silverstein J, Penfield CA, Roman AS, Rosenberg HM, Ferrara L, Lambert C, Khoury R, Bernstein PS. Pregnant women with severe or critical coronavirus disease 2019 have increased composite morbidity compared with nonpregnant matched controls. Am J Obst Gynecol. 2019. https ://doi.org/10.1016/j.ajog.2020.11.022.
18. Zambrano LD, Ellington S, Strid P, Galang RR, Oduyebo T, Tong VT, Woodworth KR, Nahabedian III JF, Azziz-Baumgartner E, Gilboa SM, Meaney-Delman D. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22–October 3, 2020. Morbid-ity and Mortality Weekly Report. 2020. https ://doi.org/10.15585 /mmwr.mm694 4e3
19. Lokken EM, Walker CL, Delaney S, Kachikis A, Kretzer NM, Erickson A, Resnick R, Vanderhoeven J, Hwang JK, Barnhart N, Rah J. Clinical characteristics of 46 pregnant women with a severe acute respiratory syndrome coronavirus 2 infection in Washington State. Am J Obstet Gynecol. 2020.
20. Savasi VM, Parisi F, Patanè L, Ferrazzi E, Frigerio L, Pellegrino A, Spinillo A, Tateo S, Ottoboni M, Veronese P, Petraglia F. Clinical findings and dis-ease severity in hospitalized pregnant women with coronavirus disease 2019 (COVID-19). Obstetr Gynecol. 2020;136(2):252–8.
21. Khalil A, von Dadelszen P, Draycott T, Ugwumadu A, O’Brien P, Magee L. Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. JAMA. 2020;324(7):705–6. https ://doi.org/10.1001/jama.2020.12746 .
22. Mendoza M, Garcia-Ruiz I, Maiz N, Rodo C, Garcia-Manau P, Serrano B, Lopez-Martinez RM, Balcells J, Fernandez-Hidalgo N, Carreras E, Suy A. Preeclampsia-like syndrome induced by severe COVID-19: a prospec-tive observational study. BJOG. 2020. https ://doi.org/10.1111/1471-0528.16339 .
23. Ferraiolo A, Barra F, Kratochwila C, Paudice M, Vellone VG, Godano E, Varesano S, Noberasco G, Ferrero S, Arioni C. Report of positive placen-tal swabs for SARS-CoV-2 in an asymptomatic pregnant woman with COVID-19. Medicina. 2020;56(6):306.
24. Hosier H, Farhadian S, Morotti R, Deshmukh U, Lu-Culligan A, Campbell K, Yasumoto Y, Vogels C, Casanovas-Massana A, Vijayakumar P, Geng B. SARS-CoV-2 infection of the placenta. medRxiv. 2020..
25. Golden TN, Simmons RA. Maternal and Neonatal Response to COVID-19. Am J Physiol Endocrinol Metab. 2020;319(2):E315-9. https ://doi.org/10.1152/ajpen do.00287 .2020.
26. Huntley BJ, Huntley ES, Di Mascio D, Chen T, Berghella V, Chauhan SP. Rates of maternal and perinatal mortality and vertical transmission in pregnancies complicated by severe acute respiratory syndrome coro-navirus 2 (SARS-Co-V-2) infection: a systematic review. Obstetr Gynecol. 2020;136(2):303–12.
27. Kotlar B, Gerson E, Petrillo S, Langer A, Tiemeier H. Maternal Transmis-sion of SARS-COV-2 to the Neonate, and Possible Routes for Such Transmission: A Systematic Review and Critical Analysis. BJOG. 2020. https ://doi.org/10.1111/1471-0528.16362 .
28. Zhang L, Dong L, Ming L, Wei M, Li J, Hu R, Yang J. Severe acute respiratory syndrome coronavirus 2(SARS-CoV-2) infection during late pregnancy: a report of 18 patients from Wuhan China. BMC Pregn Childbirth. 2020;20(1):394. https ://doi.org/10.1186/s1288 4-020-03026 -3.
29. Martins-Filho PR, Santos VS, Santos HP. To breastfeed or not to breast-feed? Lack of evidence on the presence of SARS-CoV-2 in breastmilk of pregnant women with COVID-19. Revista Panamericana de Salud Pública. 2020;44: e59. https ://doi.org/10.26633 /RPSP.2020.59.
30. Perrone S, Giordano M, Meoli A, Deolmi M, Marinelli F, Messina G, Lugani P, Moretti S, Esposito S. Lack of viral transmission to preterm newborn from a COVID-19 positive breastfeeding mother at 11 days postpartum. J Med Virol. 2020. https ://doi.org/10.1002/jmv.26037 .
31. Zeng H, Xu C, Fan J, Tang Y, Deng Q, Zhang W, Long X. Antibod-ies in Infants Born to Mothers With COVID-19 Pneumonia. JAMA. 2020;323(18):1848–9. https ://doi.org/10.1001/jama.2020.4861.
32. Dong L, Tian J, He S, Zhu C, Wang J, Liu C, Yang J. Possible vertical trans-mission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020;323(18):1846–8. https ://doi.org/10.1001/jama.2020.4621.
33. Kimberlin DW, Stagno S. Can SARS-CoV-2 infection be acquired in utero?: more definitive evidence is needed. JAMA. 2020;323(18):1788–9. https ://doi.org/10.1001/jama.2020.4868.
34. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z. Clinical Features of Patients Infected with 2019 Novel Corona-virus in Wuhan China. Lancet. 2020;395(10223):497–506.
35. Wang W, Yanli X, Gao R, Roujian L, Han K, Guizhen W, Tan W. Detec-tion of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020;323(18):1843–4. https ://doi.org/10.1001/jama.2020.3786.
36. Egloff C, Vauloup-Fellous C, Picone O, Mandelbrot L, Roques P. Evidence and possible mechanisms of rare maternal-fetal transmission of SARS-CoV-2. J Clin Virol. 2020;128:104447. https ://doi.org/10.1016/j.jcv.2020.10444 7.
37. Wu Y, Liu C, Dong L, Zhang C, Chen Y, Liu J, Zhang C, et al. Coronavirus Disease 2019 among pregnant chinese women: case series data on the safety of vaginal birth and breastfeeding. BJOG. 2020;127(9):1109–15. https ://doi.org/10.1111/1471-0528.16276 .
38. Ashokka B, Loh MH, Tan CH, Su LL, Young BE, Lye DC, Biswas A, Illanes SE, Choolani M. Care of the pregnant woman with coronavirus disease 2019 in labor and delivery: anesthesia, emergency cesarean delivery, differential diagnosis in the acutely ill parturient, care of the newborn, and protection of the healthcare personnel. Am J Obstetr Gynecol. 2020;223:66–74. https ://doi.org/10.1016/j.ajog.2020.04.005.
39. Oxford-Horrey C, Savage M, Prabhu M, Abramovitz S, Griffin K, LaFond E, Riley L, Easter SR. Putting it all together: clinical considerations in the care of critically ill obstetric patients with COVID-19. Am J Perinatol. 2020;37(10):1044–51. https ://doi.org/10.1055/s-0040-17131 21.
40. Della Gatta AN, Rizzo R, Pilu G, Simonazzi G. COVID19 during preg-nancy: a systematic review of reported cases. Am J Obst Gynecol. 2020.
41. Zaigham M, Andersson O. Maternal and perinatal outcomes with COVID-19: a systematic review of 108 pregnancies. Acta Obstet Gynecol Scand. 2020;99(7):823–9. https ://doi.org/10.1111/aogs.13867 .
42. Chen L, Li Q, Zheng D, Jiang H, Wei Y, Zou L, Feng L, Xiong G, Sun G, Wang H, Zhao Y. Clinical characteristics of pregnant women with Covid-19 in Wuhan, China. N Engl J Med. 2020.
43. Malhotra Y, Miller R, Bajaj K, Sloma A, Wieland D. No Change in Cesarean Section Rate during COVID-19 Pandemic in New York City. Eur J Obst Gynecol Reprod Biol. 2020. https ://doi.org/10.1016/j.ejogr b.2020.06.010.
44. COVIDSurg Collaborative. . Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br J Surg. 2020. https ://doi.org/10.1002/bjs.11746 .
45. Narang K, Ibirogba ER, Elrefaei A, Trad AT, Theiler R, Nomura R, Picone O, Kilby M, Escuriet R, Suy A, Carreras E. SARS-CoV-2 in pregnancy: a com-prehensive summary of current guidelines. J Clin Med. 2020;9(5):1521. https ://doi.org/10.3390/jcm90 51521 .
46. Continuous support for women during childbirth—Bohren, MA - 2017 | Cochrane Library. (n.d.). Retrieved December 29, 2020, from https ://doi.org/10.1002/14651 858.CD003 766.pub6/full?cooki esEna bled.
47. Lei D, Wang C, Li C, Fang C, Yang W, Chen B, Wei M, Xu X, Yang H, Wang S, Fan C. Clinical characteristics of COVID-19 in pregnancy: analysis of nine cases. Chin J Perinatal Med. 2020 Mar 16;23(3):225–31.
48. Wang S, Guo L, Chen L, Liu W, Cao Y, Zhang J, Feng L. A case report of neonatal 2019 coronavirus disease in China. Clin Infect Dis. 2020;71(15):853–7. https ://doi.org/10.1093/cid/ciaa2 25.
49. Zhu C, Liu W, Su H, Li S, Shereen MA, Lv Z, Niu Z, Li D, Liu F, Luo Z, Xia Y. nBreastfeeding risk from detectable severe acute respiratory syndrome coronavirus 2 in Breastmilk. J Infect. 2020. https ://doi.org/10.1016/j.jinf.2020.06.001.
50. Dong Y, Chi X, Hai H, Sun L, Zhang M, Xie WF, Chen W. Antibodies in the breast milk of a maternal woman with COVID-19. Emerg Microbes Infect. 2020;9(1):1467–9. https ://doi.org/10.1080/22221 751.2020.17809 52.
51. Bastug A, Hanifehnezhad A, Tayman C, Ozkul A, Ozbay O, Kazancioglu S, Bodur H. Virolactia in an asymptomatic Mother with COVID-19. Breastfeeding Med. 2020;15(8):488–91. https ://doi.org/10.1089/bfm.2020.0161.
52. Wu Y, Zhang C, Liu H, Duan C, Li C, Fan J, Li H, Chen L, Xu H, Li X, Guo Y. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am J Obstetr Gynecol. 2020;223(2):240. https ://doi.org/10.1016/j.ajog.2020.05.009.

Page 38 of 39Kotlar et al. Reprod Health (2021) 18:10
53. Saccone G, Florio A, Aiello F, Venturella R, De Angelis MC, Locci M, Bifulco G, Zullo F, Sardo AD. Psychological impact of coronavirus disease 2019 in pregnant women. Am J Obstetr Gynecol. 2019. https ://doi.org/10.1016/j.ajog.2020.05.003.
54. Jungari S. Maternal Mental Health in India during COVID-19. Public Health. 2020;185:97–8. https ://doi.org/10.1016/j.puhe.2020.05.062.
55. Aryal S, Pant SB. Maternal mental health in Nepal and its prioritization during COVID-19 pandemic: missing the obvious. Asian J Psychiatry. 2020;54:102281. https ://doi.org/10.1016/j.ajp.2020.10228 1.
56. Kotabagi P, Fortune L, Essien S, Nauta M, Yoong W. Anxiety and depres-sion levels among pregnant women with COVID-19. Acta Obstetricia et Gynecologica Scandinavica. 2020;99(7):953–4. https ://doi.org/10.1111/aogs.13928 .
57. Chivers BR, Garad RM, Boyle JA, Skouteris H, Teede HJ, Harrison CL. Perinatal distress During COVID-19: thematic analysis of an online parenting forum. J Med Internet Res. 2020;22(9):e22002. https ://doi.org/10.2196/22002 .
58. Koenen KC. Pregnant During a Pandemic? Psychology Today. 2020. https ://www.psych ology today .com/us/blog/menta l-healt h-aroun d-the-world /20200 7/pregn ant-durin g-pande mic?eml
59. Thapa SB, Mainali A, Schwank SE, Acharya G. Maternal Mental Health in the Time of the COVID-19 Pandemic. Acta Obstetricia et Gynecologica Scandinavica. 2020;99(7):817–8. https ://doi.org/10.1111/aogs.13894 .
60. Thomas C, Morris SM, Clark D. Place of death: preferences among can-cer patients and their carers. Soc Sci Med. 2004;58(12):2431–44. https ://doi.org/10.1016/j.socsc imed.2020.11334 8.
61. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income coun-tries: a modelling study. 2020. https ://www.thela ncet.com/pdfs/journ als/langl o/PIIS2 214-109X(20)30229 -1.pdf
62. Menendez C, Gonzalez R, Donnay F, Leke RG. Avoiding indirect effects of COVID-19 on maternal and child health. Lancet Global Health. 2020.
63. Ramoni R. How COVID-19 Is Affecting Antenatal Care. Daily Trust. 2020, sec. News. https ://daily trust .com/how-covid -19-is-affec ting-anten atal-care.
64. Aryal S, Shrestha D. Motherhood in Nepal during COVID-19 pandemic: are we heading from safe to unsafe?. J Lumbini Med College. 2020. https ://doi.org/10.22502 /jlmc.v8i1.351.
65. Pallangyo E, Nakate MG, Maina R, Fleming V. The impact of Covid-19 on midwives’ practice in Kenya, Uganda and Tanzania: a reflective account. Midwifery. 2020. https ://doi.org/10.1016/j.midw.2020.10277 5.
66. Population Council. Kenya: COVID-19 Knowledge, Attitudes, Practices and Needs—Responses from Second Round of Data Collection in Five Nairobi Informal Settlements (Kibera, Huruma, Kariobangi, Dandora, Mathare). Poverty, Gender, and Youth, 2020. https ://doi.org/10.31899 /pgy14 .1013.
67. ReliefWeb. Rapid Gender Analysis - COVID-19 : West Africa – April 2020 - Benin. 2020. https ://relie fweb.int/repor t/benin /rapid -gende r-analy sis-covid -19-west-afric a-april -2020.
68. Semaan AT, Audet C, Huysmans E, Afolabi BB, Assarag B, Banke-Thomas A, Blencowe H, Caluwaerts S, Campbell OM, Cavallaro FL, Chavane L. Voices from the frontline: findings from a thematic analysis of a rapid online global survey of maternal and newborn health professionals facing the COVID-19 pandemic. BMJ Global Health. 2020;5(6):e002967. https ://doi.org/10.1136/bmjgh -2020-00296 7.
69. Coxon K, Turienzo CF, Kweekel L, Goodarzi B, Brigante L, Simon A, Lanau MM. The Impact of the Coronavirus (COVID-19) pandemic on maternity care in Europe. Midwifery. 2020;88:102779–102779. https ://doi.org/10.1016/j.midw.2020.10277 9.
70. Ayenew B, Pandey D, Yitayew M, Etana D, Binay Kumar P, Verma N. Risk for Surge Maternal Mortality and Morbidity during the Ongoing Corona Virus Pandemic. Med Life Clin. 2020;2(1):1012.
71. Stevis-Gridneff M, Alisha HG, Monica P. Oronavirus Created an Obstacle Course for Safe Abortions. New York TImes. 2020. https ://www.nytim es.com/2020/06/14/world /europ e/coron aviru s-abort ion-obsta cles.html.
72. Sobel L, Ramaswamy A, Frederiksen B, Salganicoff A. State Action to Limit Abortion Access During the COVID-19 Pandemic. KFF(blog), 2020. https ://www.kff.org/coron aviru s-covid -19/issue -brief /state -actio n-to-limit -abort ion-acces s-durin g-the-covid -19-pande mic/.
73. UNFPA. Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-Based Violence, Female Genital Mutilation and Child Marriage. UNFPA, 2020.
74. Federation, International Planned Parenthood. COVID-19 Pandemic Cuts Access to Sexual and Reproductive Healthcare for Women around the World. News Release. Published Online April 9, 2020, n.d.
75. Jeffrey G, Raj S. 8 Hospitals in 15 Hours: A Pregnant Woman’s Crisis in the Pandemic.” New York Times. 2020. https ://www.nytim es.com/2020/06/21/world /asia/coron aviru s-india -hospi tals-pregn ant.html.
76. Kumari V, Mehta K, Choudhary R. COVID-19 outbreak and decreased hospitalisation of pregnant women in labour. Lancet Global Health. 2020;8(9):e1116–7. https ://doi.org/10.1016/S2214 -109X(20)30319 -3.
77. Takemoto ML, Menezes MO, Andreucci CB, Knobel R, Sousa L, Katz L, Fonseca EB, Nakamura-Pereira M, Magalhães CG, Diniz CS, Melo AS. Clinical characteristics and risk factors for mortality in obstetric patients with severe COVID-19 in Brazil: a surveillance database analysis. BJOG. 2020. https ://doi.org/10.1080/14767 058.2020.17860 56.
78. Rafaeli T, Hutchinson G. The Secondary Impacts of COVID-19 on Women and Girls in Sub-Saharan Africa, (n.d.). Resource Centre. Retrieved December 29, 2020, from https ://resou rcece ntre.savet hechi ldren .net/node/18153 /pdf/830_covid 19_girls _and_women _ssa.pdf
79. Khalil A, Von-Dadelszen P, Draycott T, Ugwumadu A, O’Brien P, Magee L. Change in the incidence of stillbirth and preterm delivery during the COVID-19 Pandemic. JAMA. 2020;324(7):705–6. https ://doi.org/10.1001/jama.2020.12746 .
80. KC, A., Gurung, R., Kinney, M. V., Sunny, A. K., Moinuddin, M., Basnet, O., Paudel, P., Bhattarai, P., Subedi, K., Shrestha, M. P., Lawn, J. E., & Målqvist, M. . Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Global Health. 2020;8(10):e1273–81. https ://doi.org/10.1016/S2214 -109X(20)30345 -4.
81. Been JV, Ochoa LB, Bertens LC, Schoenmakers S, Steegers EA, Reiss IK. Impact of COVID-19 mitigation measures on the incidence of preterm birth: A national quasi-experimental study. MedRxiv. 2020. https ://doi.org/10.1101/2020.08.01.20160 077.
82. Shuchman M. Low-and middle-income countries face up to COVID-19. Nature Medicine. 2020;26(7):986–8. https ://doi.org/10.1038/d4159 1-020-00020 -2.
83. Bong CL, Brasher C, Chikumba E, McDougall R, Mellin-Olsen J, Enright A. The COVID-19 pandemic: effects on low-and middle-income countries. Anesthesia Analgesia. 2020. https ://doi.org/10.1213/ANE.00000 00000 00484 6.
84. Hupkau C, Petrongolo B. COVID-19 and Gender Gaps: Latest Evidence and Lessons from the UK. VoxEU. Org22. 2020.
85. Boniol M, McIsaac M, Xu L, Wuliji T, Diallo K, Campbell J. Gender equity in the health workforce: Analysis of 104 countries, viewed 27 April 2020. 2019. https ://apps.who.int/iris/bitst ream/handl e/10665 /31131 4/WHO-HIS-HWF-Gende r-WP1-2019.1-eng.pdf?seque nce=1&isAll owed=y
86. Robertson C, Gebeloff R. How Millions of Women Became the Most Essential Workers in America. The New York Times, 2020. https ://www.nytim es.com/2020/04/18/us/coron aviru s-women -essen tial-worke rs.html.
87. Jankowski J, Davies A, English P, Friedman E, McKeown H, Rao M, Sethi S, Strain WD. Risk Stratification for Healthcare Workers during CoViD-19 Pandemic: Using Demographics, Co-Morbid Disease and Clinical Domain in Order to Assign Clinical Duties. Medrxiv. 2020.
88. World Health Organization. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. World Health Organization. 2020. https ://www.who.int/news-room/detai l/03-03-2020-short age-of-perso nal-prote ctive -equip ment-endan gerin g-healt h-worke rs-world wide.
89. Alon TM, Doepke M, Olmstead-Rumsey J, Tertilt M. The Impact of COVID-19 on Gender Equality. National Bureau of Economic Research, 2020.
90. Johnston RM, Mohammed A, van der Linden C. Evidence of exac-erbated gender inequality in child care obligations in Canada and Australia during the COVID-19 pandemic. Politics Gender. 2020. https ://doi.org/10.1017/S1743 923X2 00005 74.

Page 39 of 39Kotlar et al. Reprod Health (2021) 18:10
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
91. Malik S, Naeem K. Impact of COVID-19 Pandemic on Women: Health, livelihoods & domestic violence. Sustainable Development Policy Insti-tute. 2020. http://www.jstor .com/stabl e/resre p2435 0
92. UN Women. The Private Sector’s Role in Mitigating the Impact of COVID-19 on Vulnerable Women and Girls in Nigeria. 2020. https ://www.weps.org/resou rce/priva te-secto rs-role-mitig ating -impac t-covid -19-vulne rable -women -and-girls -niger ia
93. Wahome C. Impact of Covid-19 on Women Workers in the Horticulture Sector in Kenya. Hivos. 2020. https ://www.hivos .org/asset s/2020/05/Hivos -Rapid -Asses sment -2020.pdf
94. World Vision International Cambodia. Rapid Assessment of the impact of COVID-19 on child wellbeing in Cambodia Summary Report. 2020. https ://www.wvi.org/publi catio ns/cambo dia/rapid -asses sment -summa ry-repor t-impac t-covid -19-child rens-well-being -cambo dia
95. Staff of the National Estimates Branch. Current Employment Statistics Highlights. U.S. Bureau of Labor Statistics, 2020. https ://www.bls.gov/web/empsi t/ceshi ghlig hts.pdf.
96. Adams-Prassl A, Boneva T, Golin M, Rauh C. Inequality in the Impact of the Coronavirus Shock: Evidence from Real Time Surveys. IZA Discus-sion Papers. 2020. https ://www.iza.org/publi catio ns/dp/13183 /inequ ality -in-the-impac t-of-the-coron aviru s-shock -evide nce-from-real-time-surve ys
97. Novel Coronavirus (COVID-19): Violence, Reproductive Rights and Related Health Risks for Women, Opportunities for Practice Innovation. 2020 https ://www.ncbi.nlm.nih.gov/pmc/artic les/PMC72 75128 /
98. Wanqing Z. Domestic Violence Cases Surge During COVID-19 Epidemic. Sixth Tone, 2020. https ://www.sixth tone.com/news/10052 53/domes tic-viole nce-cases -surge -durin g-covid -19-epide mic.
99. Euronews. Domestic Violence Cases Jump 30% during Lockdown in France. euronews, 2020. https ://www.euron ews.com/2020/03/28/domes tic-viole nce-cases -jump-30-durin g-lockd own-in-franc e.
100. Women, U. N. COVID-19 and Ending Violence against Women and Girls. New York. 2020.
101. Sigal L, Ramos Miranda NA, Martinez AI, Machicao M.Another Pandemic: In Latin America, Domestic Abuse Rises amid Lockdown. Reuters, 2020. https ://www.reute rs.com/artic le/us-healt h-coron aviru s-latam -domes ticvi ol/anoth er-pande mic-in-latin -ameri ca-domes tic-abuse -rises -amid-lockd own-idUSK CN229 1JS.
102. Graham-Harrison E, Giuffrida A, Smith H, Ford L. Lockdowns around the World Bring Rise in Domestic Violence. The Guardian. 2020, sec. Society. https ://www.thegu ardia n.com/socie ty/2020/mar/28/lockd owns-world -rise-domes tic-viole nce.
103. Bosman J. Domestic Violence Calls Mount as Restrictions Linger: ‘No One Can Leave. New York Times. 2020. https ://www.nytim es.com/2020/05/15/us/domes tic-viole nce-coron aviru s.html.
104. Women’s Safety NSW. “New Domestic Violence Survey in NSW Shows Impact of COVID-19 on the Rise.” Women’s Safety NSW, April 3, 2020. https ://www.women ssafe tynsw .org.au/wp-conte nt/uploa ds/2020/04/03.04.20_New-Domes tic-Viole nce-Surve y-in-NSW-Shows -Impac t-of-COVID -19-on-the-Rise.pdf.
105. Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. 2016;191:62–77. https ://doi.org/10.1016/j.jad.2015.11.014.
106. Kaur R, Garg S. Addressing domestic violence against women: an unfinished agenda. Indian J Commun Med. 2008;33(2):73–6. https ://doi.org/10.4103/0970-0218.40871 .
107. Dennis CL, Vigod S. The relationship between postpartum depression, domestic violence, childhood violence, and substance use: epidemio-logic study of a large community sample. Violence Against Women. 2013 Apr;19(4):503–17. https ://doi.org/10.1177/10778 01213 48705 7.
108. Kem J. Framework in Ending Violence Against women and Girls with the Advent of the COVID 19 from an African Perspective. 2020. Available at SSRN 3575288.
109. Mukherjee S, Dasgupta P, Chakraborty M, Biswas G, Mukherjee S. Vulnerability of Major Indian States Due to COVID-19 Spread and Lock-down. 2020.
110. Carter Ebony B, Tuuli Methodius G, Caughey Aaron B, Odibo Anthony O, Macones George A, Cahill Alison G. Number of prenatal visits and pregnancy outcomes in low-risk women. J Perinatol. 2016;36(3):178–81. https ://doi.org/10.1038/jp.2015.183.
111. Gajate-Garrido G. The impact of adequate prenatal care on urban birth outcomes: an analysis in a developing country context. Econ Dev Cult Change. 2013;62(1):95–130. https ://doi.org/10.1086/67171 6.
112. Panagiotakopoulos L. SARS-CoV-2 infection among hospitalized pregnant women: Reasons for admission and pregnancy characteris-tics—Eight US health care centers, March 1–May 30, 2020. Morbidity and Mortality Weekly Report: MMWR; 2020. p. 69.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub-lished maps and institutional affiliations.