the international journol of periodontics & restorative ... · construction. thus, the tr-gtam...
TRANSCRIPT
The International Journol of Periodontics & Restorative Dentistry

221
Vertical Ridge Augmentation:Wtiat is the Limit?
Carlo Tinti MD, DDS'Stefano Parma-Benfenafi MD. DDS. MSD"'Giovanni Polizzi. MD. DDS. " '
The aim of this study is to show the possibility of aohieving more ttian a 4-mm new vertical bone apposition on partialiy edentulous ridges. Sixhealthy, partialiy edentuious patients were treated from July 1993 toSeptember 1993. After accurate radiographie investigation, ali of thepafients were treated using the Bränemari< System. After insertion. 14 fíx-tures were left circumferentiaiiy exposed for 37 mm. Autogenous bonegraft norvested from a bone fliter was placed around the exposed threadsand oompleteiy covered with titanium-reinforced Gore-Tex augmentationmembranes ¡JR-GTAM). Fiaps were caranally displaced to passively coverthe regenerative materiais. Only one af the six memorónos was exposedand it was removed immediateiy. After a 12-montn healing period, themembranes were removed in conjunction with the second-stage surgicalprocedure, in the five cases where the membranes were kept covered, aliof the ovaliable space underneath the JR-GTAM was fíiled with regenera-tive tissue, in ail of fhe oases a histoiogic biopsy was performed. In onecase ali the space was filied with more than 7 mm of bone, in three casesail the space was fiiied with more than 5 mm of bone, in one case the mastcoronai part (approximately I mm) of the regenerative tissue wos repre-sented by connective fissue: fhe remaining tissue was represented bybone. The measurements demonstrated an average af verticai ridge aug-mentation af4.95 mm. In the aniy case where the membrane underwentexposure and was then removed there was no regenerative tissue present.(Int J Periodont Rest Dent 1996,16:221-229.)
•Private Practice, Fiero (Brescia). Italy'Deportment of Penodonfology, University ot Ferrora DentoiSchooi, FerraíQ, italy.
"Privóte Practice, Verona, itoly.
Reprint requests' Dr Cario TintI, Via Covour 3,25020 Fiero (Brescia)
Italy.
In the lost 10 years impianttreatment plonning proposedby the dentist or requested bythe patient hos expanded ex-ponentialiy with the oppiicationof osseointegration to the fuliyor partioily endentulous pofient.However, many patients pre-senting for dental impiant ther-apy are not candidotes forsuch treatment because ofeither an inadequate volumeof bone or a bany onatomythat complicates the place-ment of fixtures, especially insites where ideal implant posi-tioning is mandatory for optimalesthetics.
To obtain predictabie iong-term results, the anatomy quan-tity of bone, ond quaiity of thejawbone at the site of fixtureinstaiiatian are cruciol factors. Aminimum of 7 x 4 mm of bonestructure is required with use ofthe shortest standard Brâne-mark implant^: however, toavoid any undesirable compli-cations during the healingprooess, a minimum buoca-linguai width of ó mm is recom-
Volume 16, Number 3,199Ó
222
mended for complete bonecoverage af the threaded partof the titanium impiant.^-^
Bone regeneration proce-dures can modify, correct, andaugment compromised bonesites resuiting from on excessiverésorption phase foiiowingtooth exfoiiation because oftrauma, deep root fracture,advanced periadontai infiam-matory iesions, or maxillofacialtrauma.
Prior to the ciinical applica-tion of the principie of guidedtissue regeneration (GTR) fodental impiants, extraoral auto-genous bone grafting proce-dures were used to increasethe amount of bone tissue. Theassociated probiems with thesetechniques were the utiiizotionof an exfraoral site, hospifaiizo-fion, and pafient morbidity
in portiolly edentuiouspatients, anatomic structuressuch as the maxiiiary sinus or theaiveoiar nerve may limit thebone height avaiiabie forimplant stability and the ioad-bearing capocity. Differentbone graff maferials may be uti-lized for sinus eievation, andalveolar nerve transportation inthe mandibuiar orch mayIncrease the length of the bonytissue to allow the placement ofimplants of adequafe length.However, both techniques arestiii under clinical evaiuation,and the lotter presents a consis-tent risk at temporary or perma-nent nerve damage. The bio-logic principies of GTR, reported
for the treatment of periodon-toiiy involved feeth, have beenapplied to increase the alveoidrridge width prior to implantplacement, to exclude the inva-sion af nonosteogenic saft tissuecells, and to oilow preferentialenhancement of new bone tis-sue around implants placedinto sites where there is insuffi-cient bone volume,""'^ A betterunderstanding of the principlesof GBR and innavafions in surgi-cal techniques have enhancednew bone formation aroundimplants placed into immediateextraction sockets,^'^''^ indehisced or fenestroted impiantsurfaces,^'°'^ and in treatmentof anguiar bony defects in aperi-implantitis situation.^ inaddition, GBR has enhancedtreatment of other categoriesof defects using ridge regenera-tion, and subsequent or simulta-neous piacement of osseointe-
The expanded polytetraflu-oroethylene (e-PTFE) mem-brane creates initially secludedspace in which the blood clotis prctected from mechanicalinjuries and from the coloniza-tion of celis deriving from thegingivai tissues. As o result, oniycells from the alveolar bonecan repopulate tfie blood clot.
The reiationship betweenspace provision and boneregeneratian was studied in the1950s and in the eariy 19ó0s,Severol studies confirmed thisbiologic observation in othertypes af osseous defects. Space
provision for bone regenerationis one af the main problems inGTR procedures, as it definesthe maximum voiume of bonewhich can be regenerated.'^-^The creation and maintenanceof a sufficienf space with anadequate blaod ciot that doesnot interfere with stabilizationmust be estobiished.
it has been clinically proventhat the fewer the residualbony waiis, the more difficult it isto avoid soft tissue and mem-brane coilapse. This is espe-cially true in the presence ofgingival recession, dehiscence,cr fenestration types of bonydefects, where there is no sup-port to the barrier.
Various fiiiing materials havebeen experimented with ondproposed for the creation andmaintenance of space and forprevention of a coilapse ofboth the fiap and the barriermembrane in non-space-mai<-ing detects,^'-^^
Fram clinicai experience itis known that empty spacesbecome rapidly abliterated bya biood ciot containing bothnon-bone-forming and bone-forming ceils after the surgicdlprocedure.
Recentiy, encouraging ex-perimental results have beenreported utiiizing GBR tech-niques in verticdi ridge aug-mentation from flaf corficaibone surfaces. ̂ -̂2''
The internotianai Jaurnai of Periodontics & Restorative Dentistry

223
Many studies hove advo-cated soft tissue pressure andtension to cause membranecollapse in defects, thus iimitingthe regenerative potentiai ofthe bony structures.̂ '̂̂ ^
There ore oniy two studieson jawbone augmentation ofthe vertical dimension^'^' inwhioh the authors utiiizeda new type of e-PTFE mem-brane reinforced with a puretitonium struoture (TR-GTAM, WLGore) ond membrane tixa-tion devices (Memfix system,Straumann). Tito ni um-re in-forced GTAM can be bent andshaped and maintain thedesired form because of thetitanium structure inciuded in itsconstruction. Thus, the TR-GTAMcreates and preserves sufficientspoce between the mem-brane and the bony deteots,allowing new possibilities forvertical ridge augmentationand regeneration in situationsin which the anatomy of thedefect is non-spoce-making.
Jovanovic et al,^^ in a studyon five adult beagie dogs, sug-gested that supracrestal boneregeneration con successfullybe enhanced by a submergedmembrane technique in thedog modei. They olso sug-gested that the TR-GTAM mem-branes were able to maintain alarge protected space withoutthe addition of bone grafts, ondfhaf they produced a largerquantity of bone when com-pared to standard membrones.
Simion et ai,^' in a clinicaland histologio study on fivepatients, suggested that theplacement of implants protrud-ing 3 to 4 mm trom the top of oresorbed bone surface mayresuit in a vertical bone regen-eration gain of 3 to 4 mm inheight, Their histologie exomina-tion showed that ail retrievedminisorews were in direct con-tact with the bone, ond thotthe regeneroted bone wasabie to osseointegrate puretitanium implants,
The aim of this ciinical studywas to demonstrate the possi-bility of achieving more fhon 4mm of new vertical boneapposition on partially edentu-ious ridges using a membronetechnique associated withosseointegrated implants inhumons.
Mettiod and materials
Six potients between 40 and 52years (mean age: 46 years)part ioipated in this clinicalstudy. They were partially eden-tuious, were initiaiiy referred toour dental offices for evoiuationfor implant therapy, and werehighly motivated to undergothis procedure because theywanted to avoid removableportial dentures ot ali costs. Allpatients reported in goodhealth ond received o com-prehensive periodontal evaiuo-tion ond a compiete-mouthradiographie survey.
Computerized tomogramsrevealed a minimum quontityof residual bone in o corono-apicai direction. The boneridges were carefully exam-ined, and the desired implantlocation trom a prosthetic pointof view wos determined utiiiz-ing a guiding surgical stent.
Ail patients received anextensive explanation of theprocedures thot would be per-formed and signed a writtenconsent form. A total of 14 den-tal implants (MK II, Nobei-pharma) were piaced.
Voiume 16. Number 3,1996

224
Surgical technique (Figs ¡a tom and 2a to 2e)
All patients were treated toliow-ing an identical surgical proto-col, A crestal incision within thei<eratinized gingiva was used toeievate a buccal mucoperio-steai tull-thickness flap. This inci-sion was extended intrasulcu-larly and anteriorly to the mesiaiiine angle ot the adjacenttooth. Vertical releosing incisionswere made at the distal aspectof the crestai incision, approxi-mateiy 7 to 8 mm distai to theproposed most distal position otthe membrane. The iingual flapwas raised to full ttiickness andcontinued mesially intrasuiou-lary to include three teeth, anda vertical releasing incision ofapproximateiy 3 to 4 mm wasused on the distai aspect. Theperiosteum was then released insuoh a way as to enhonce elas-ticity and ta obtain a coronaliyaccentuated dislodgement otthe linguai flap.
On the vestibuiar side theperiosteai releasing incisionwas started from the most api-cal part of the mesioi reieasingincision and continued untiljoining the most apical part ofthe distal releasing incision. Thistype of incisioh left the flap ten-sion-free at closure.
On the maxillary arch, acrestai incision and two verti-cal buccal reieasing incisionswere used at a reasonable dis-tanoe from the anticipatededge of the membrone ond
were connected by a mesio-distal incision at the base ofthe flap to enhance flap elas-ticity by reieasing the perios-teum, On the paiatal side, acoronaiiy positioned paiataisiiding fidp was performed asdescribed by Tinti and Parma-
Atter positioning the surgi-cai stent made by the prostho-dontists, a totai of 14 MK iiNobelpharma fixfures wereinserted. Stondard implant pro-tocol as described by Adeii etai^ was foilowed, except thotimplants were piaced in anideai position for restoration,and were intentionaiiy allowedto protrude 3 to 7 mm from thebone crest, Countersinks werenot used, Aii the measurementsfor biométrie anaiysis weretaken with a caiibrated perio-dontoi probe from the top ofthe cover screw to the peri-implant bone crest ot the mesiaiand distal aspects before andafter treatment,
During the drilling phase forthe preparation ot the tixture-recipient sites the physioiogicsoiution was suctioned withthe interposition of the bone tii-ter (Quaiity Aspirotors, QualityDent) for the purpose of savingthe bone, Before implant place-ment a round smail-diameterbur was used to perforate thecortical bone to aiiow a idrgernumber of medulidry oovities totavor bleeding, Fourteen fi>cfureswere positioned in six surgicalsites, and the bone particles
taken for the bone tiiters werepositioned all around the fix-tures.
Titanium-reinforced e-PTFEmembrane (TR-GTAM. WL Gore)was used in all patients (Fig Ic),Titanium-reintorced membraneswere bent with fine tweezers toobtain the desired shape for aoiose adaption to the underly-ing bone and to the impiants.The iateral portions weretrimmed with scissors in such away that the outer portion over-iapped the edge of the bonebeyond the detect margins byapproximateiy 4 mm. All thetitanium-reintorced membraneswere additionaliy stabilized tothe bone with Memfix fixationscrews (Fig Ic), When the aug-mentation material was closeto notural teeth, attention wosgiven to prevent interferencewith the healing process of theperiodontal structures. Everyetfort was made to ochieve pri-mary closure of the fiaps andpassive adaption at closure.Horizontal mattress sutures withU stitches were used to createtwo contact surfaces at ieast 3mm thick and were alternatedwith simple interrupted sutures.
The patients were premed-icated with an antibiotic (2g ofamoxicillin 2 hours prior tosurgery), and were prescribed 1g of amoxicillin per day for 1week postoperatively. Thepatients were given appropri-ate anaigesics. They wereexamined at the end of the firstweek for material exposure,
Ttie International Journal ot Periodontios & Restorative Dentistry

225
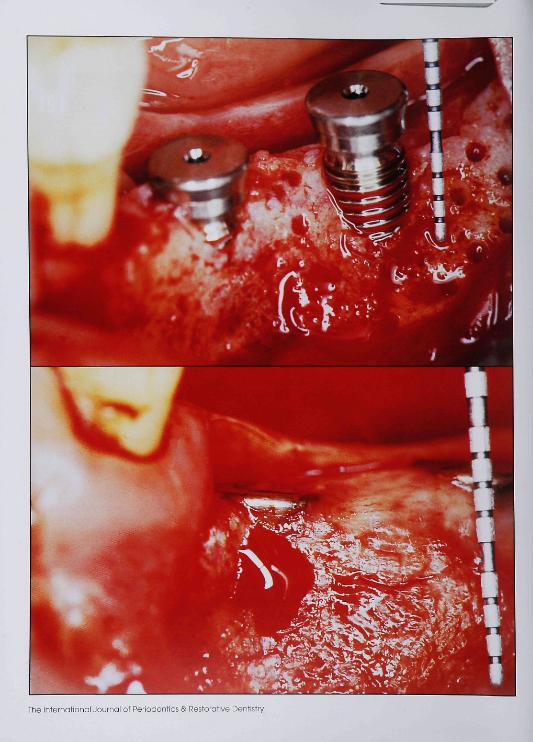
Fig la Edentulous space in the I'ertmandibulor region of a äS-yeor-oldwomon. First ond second mondibularmolOiS were lest several years previous-ly. There is insufHoient bone height toallow traditionai implant placement.
hg 10 IWO iO-mm self-toppingimpiants pioced in ideal prostneticposition. The distai fixture protrudes ó to7 mm from fhe bone orest. The mesiaifixture is not induded on fhe study.
Fig Ic Titonium-ieinfotced GTAM isportioned over the bone defecf andthe protruded impiants and fixed to fhebone with one Memtix fixation screw.The titanium frame gives rigidity to themembrone to maintain space.
Fig Id Ctinicai appearance prior tosfoge 2 surgery offer 12 months ofuneventfui heoiing.
Fig le Periaploal radiograph immedi-ately after positioning the two implonts.
Fig It Periapicai radiograph l yearpostoperative. Newly regenerated cai-cified tissue can be seen.
Fig Ig Membrone removal demon-strates a newiy regenerated ridge andthat the peri-impiant bone defects arefliied with new osseous tissue.
Fig lh Histologie findings from thebiopsy specimen. New regeneratedbone (lomellar) with osteobtostio linesond osteooite oeiis are present.
Volume 16. Number 3, ] 99ó

22Ó
Table 1 Result of GBR treatment in vertical ridge augmentationaround implants in six patients
Patient
1
234
5
6
Healing
UUUUUUUU
MDMDUUUU
Tooth no.
1514134737353637242521222324
Stage 1surgery
457574.544445.5444,5
Stage 2surgery
000
+21000440000
Gain inridge height
(mm)
4577ó4.544005.544
4.5
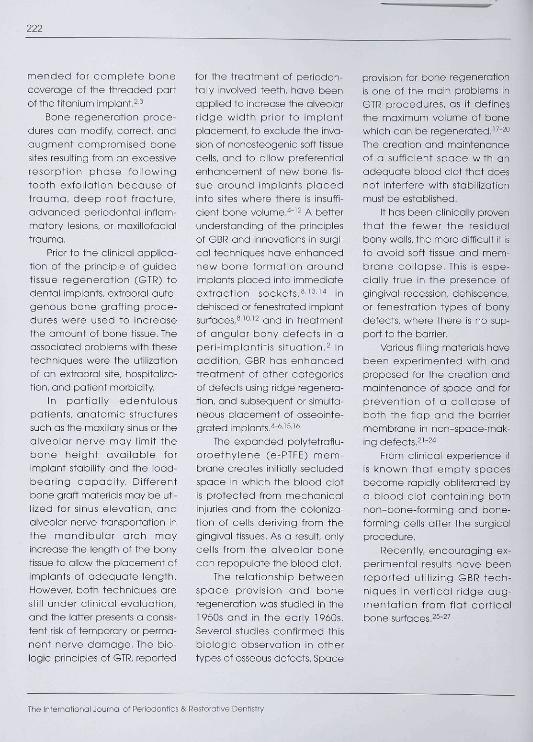
u = Uneventful: MD = membrane dehiscence.Fig 2a Three M/Í il Nobelphormaimpionts placed in ideal prostheticpcsiticn with coronal impiant surfaceextending outside the Pone crestMeasuisments were taken from theresiduol oiveoior crest to the fop cf thecover sorew.
and the sutures were removedin 15 days.
The patients were oheci<edmonthly, and the use of aremovable prosthesis wasavoided on the surgical site untilstage 2 surgery to prevent onytrauma to the augmented site.
One Ti? membrane becomeexposed offer 11 days and wosimmediateiy removed.
Second-stage surgery—Membrane removal
Affer a 12-month heoiingperiod, aii TR membranes wereremoved exoept for the onethat became exposed at the
surgery for obutment connec-tion, in ali oases a orestai inoisianin a distomesiai direction wasperformed to roise a fiap justbeyond the most apicai marginsof the augmentation material.
After removing the Memfixfixotion screws, the TR mem-brane was raised with smoii sur-gioal piiers from its most apicalportion.
Complete photographicdocumentation and clinicaimeasurements were retaken atthe time of membrane removaland abutment connection.
All the spoce underneaththe TR membranes was com-pieteiy filied with regeneratedtissue (Figs le to lh and 2a to
2d). In one patient the mostcoronol part, approximotely 1mm, contained fibraus connec-tive tissue. The regenerotedmateriai in the remainingspace, OS well as all the spacein the other patients, oppearedOS a hard, bone-iike structure. Asmaii biopsy specimen of newiyregenerated hard tissue wascollected from eoch patient tobe processed far histoiogicexominotion (Figs lh and 2e).These specimens were re-moved, fixed in 10% neutralbuffered formalin for 24 hours,and then dehydrated in onascending series of aicoholrinses. The sections were stainedwith hematoxylin-eosin stoin.
The International Jouinai of Periodontios & Restorative Dentistry
227
Fig 2b Clinical view after flop eleva-tion and TR mernbrane removal.Previous riäge loss is completely regen-erated with newly formed bane.
Fig 2c Raúiogropn immeaioteiv onerfixture pasltioning.
Flg2d Radiograph I year pastopera-tive.
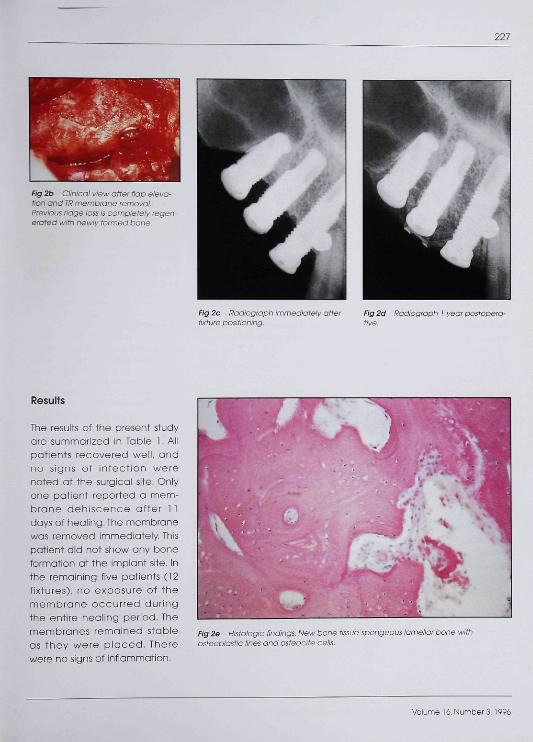
Results
The results af the present studyare summarized in Table 1. Alipatients recovered well, andno signs of infecfion werenoted at fhe surgical site. Oniyone patient reported a mem-brane dehiscence after 1 1days of healing. The membranewas removed immediafely. Thispdtient did not show any boneformation at the implant site. Inthe remaining five patients (12fixtures), no exposure of themembrone occurred duringthe entire healing period. Themembranes remained stableas they were p laced. Therewere no signs of infiammation.
Fig 2e Histologie findings. New bone tissue-spongeous lamellor !osteoblastic lines and osteocite oells.
Volume 16, Number 3,1996

226
During the second-stogesurgical phase at membroneremoval the fixation screwswere removed and the mem-branes were gently dissectedfrom the underlying newlyregenerated tissue.
An approximately 1-mm-thick layer of connective tissuewos present after removol ofthe membrane in the mostcoronoi part in only one case.This tissue was removed, leavingonly bone around the impiant.Connective tissue wos notfound oround the implants inany of the other cases.
Measurements were cor-ried out mesially and distallyfrom the highest part of thecover screw to the top of thenewiy formed ridge, The mea-surements demonstrated anaverage circumterential boneformation in verticai regenera-tion of the ridge of 4.95 mm,and in one case the regenero-tion wos over 7 mm.
The histoiogic examinationof the regeneroted tissueunequivocaiiy demonstratedthat it wos healthy, vitai bonewith mature and reguiariyformed bone cells (see Figs lhand 2e). The histoiogic exami-nation of the soft tissue demon-strated that it was connectivetissue with no inflammatoryreaction, no macrophoges, fewcells, and scorce blood vesseis.
Discussion
This sfudy confirmed the capac-ity of fhe GTR technique to verti-colly augment bone from flotcortical bone surfaces, os waspreviously demonstroted inexperiments with both oni-mais^^- '̂ and humons,^' Simionet al^^ found a 4-mm limit of ver-tical regeneration of the ridge.In this study, five of six casesshowed a vertical bone regen-eration of approximately 5 mm,and in one case of more than 7mm,The spoce beiow the mem-brane in all cases presentedhod been filied almost exclu-sively with tissue which both clin-icaliy and histoiogicaily wosshown to be bone. The discrep-ancy in the results shown in thepresent ortiole and that ofSimion may be coused by (1)the omount of time betweenstage 1 ond stage 2 surgery:and (2) the use of autogenousbone graft from fhe fiiter.
Conclusion
The aim of this study was todemonstrate the possibiiity ofsupracrestal bone regenerationof over 4 mm. This gool ap-peared possible when:
1. The fiap completeiy cov-ered fhe membrone andwas piaced without tension.
2. The membrone wos cov-ered for 1 yeor.
3. The membrone was stabi-lized.
4. Autogenous bone was used,5. There were obundant perfo-
rations of the corticai bone,6. iHorizontol maftress sutures
with U stitches were used tocreate two contact sur-faces at ieost 3 mm thick.
Further research is neededto evaiuate the load-bearingcapobility and long-term resuitsof the newly formed tissue.
References
1. Lekholm U, Zarb GA. Potient selectionand preparation. In: Brânemark P-l,Zarb GA, Albrektsson T (eds). Tissue-integrated Prostheses: Osseointe-gration in Clinical Dentistry. Chicogo:Quintessence, 1985: 199-210.
2. Jovanovic SA. Diagnosis and treot-ment of peri-implont disease, CurrOpin Periodont 1994:194-204.
3. Adel l R. Lei<holm U, Rocklet B,Brânemark P-l. A 15-year study ofosseointegrated implants in theIreatment of the edentulous jaw. IntJOrolSurg 1981:10:387-410.
4. Buser D. Brägger U, Lang NP NymonS. Regeneration and enlargement oflaw bone using guided tissue regen-erat ion. Clin Orai Implonts Res1990,1:22-32.
5. Nevins M, Mellonig JT. Enhoncementof the damaged edentulous ridgeto receive denfal impiants: A combi-nation of aiiograft and the Gore-Texmembrane, lnt J Periodont Rest Dent1992J 12:97-111.
The international Journal of Penodontics & Restorative Dentistry

229
ó, Nevins M, Meilonig JT. The odvon-tages ot looaiized ridge augmento-tion prior to impiont placement: Astoged event, Int J Periodont RestDent 1994:14:97-111.
7. Dahiin C, Anderssan L Linde A. Boneaugmentat ion at fenestratedimpiants by an osteopromotivemembrane techniaue. A controliedoiinicai study Clin Oral implants Res1991:2;159-I65,
8. Beoker W, Becker BE, Guided tissueregeneration for impionts piocedInto extraction sockets and forimpiant dehiscences: Surgiool tech-niques and case reports, int JPeriodont Rest Dent 1990:10:377-391.
9. Datilin C, Lektioim U, Linde A,Membrane-induoed bone aug-mentation at titanium implants. Areport on 10 fixtures followed from 1to 3 years after loading, int JPeriodont Rest Dent 1991,11:273-261,
10, Jovonovic SA, Spiekermann H,Richter JE, Bone regenerationaround titanium dental implants indehisced defect sites: A clinicaistudy, Int J Oral Maxiliofac Implants1992:7:233-245,
11, Mellanig JT, Triplet J. Guided tissueregeneration and endosseous den-tal implants. Int J Periodont RestDent 1993:13:109-119,
12, Paimer RM, Floyd PD, Paimer PJ,Smith 6J, Jahonssan OB, AibrektssonT Healing of impiant dehisoencedefects with and wittiout expand-ed palytetrafiuofoethyiene mem-branes: A controiied clinioai andtiistologicai study, Oiin Orai impiantsRes 1994:5:98-104.
13, Lazzara RJ, Immediate impiantpiacement into extraction sites:Surgjoai and restorative advan-tages, int J Periadont Rest Dent1989:9:333-343.
14. Becker B, LynohS, LekhoimU, et ai.Acomparison ot three methods forpromoting bone formation araundimpiants piaced into immediateextraction sockets: e-PTFE mem-brane aione, or witti eittier PDGFand iGF-i, or DFDB, J Periodonloi1992:03:929-940.
15. Simion M, Baidoni M, Zaffe D.Jawbone eniargement using imme-diate impiant placement ossociat-ea with a split-crest technique andguided tissued regeneration, intJ Periodont Rest Dent 1992:12:463-473,
16. TInti C, Parma-Benfenati S, MantriniF, Spaoe-making metal structures fornon-resorbabie membrones mguided bone regeneration aroundimplants. A twa case report, int JPeriodont Rest Dent (accepted),
17. Tinti C, yinoenzi G, Oocchetto PGuided tissue regeneration inmuoogingivai surgery J Periodontoi1993:64:118il-1191,
18. Dahlin C, Albeerius R Linde A.Osteopromotion for oranioplasty JNeurosurg 1991:74:487-491.
19. Honey JM, Nilveus RE, MoMiilan PJ,Wikesjo UM, Periadontol repair indogs' Exponded polytetraflouroeth-yiene barrier membranes supportwound stabilizatian and enhancebone regeneratian. J Periodontoi1993:04:883-890,
20. Sigursson TJ, Hordwick R, Bogle GC.Wikesjo UM, Periodontal repoir indogs: Spooe provision by reinforcede-PTFE membranes enhances boneand oementum regeneratian iniorge supraaiveoiar defects. JPeriadontoi 1994:65:350-356.
21. StatiL Fraum S, Humon infrobonylesion responses to debridement,porous hydroxyapatite implants,and Teflon barrier membranes.Seven histoiogio case reports, JPeriodontoi 1991:62:005-610,
22. Oortellini P Pini Proto G, Baldi C,Ciauser C. Guided tissue regenera-tion vjith ditferent materials, int JPeriodontal Rest Dent 1990:10:137-151.
23. Schaliorn R, McCiain P Combinedosseous composite grafting, rootconditioning, and guided tissueregeneration, Int J Periodontal RestDent 1988:8(4):8-31.
24. Simion M. Dohlin C, Trisi R Piateiii A,Qualitotive ond quantitative com-parative study on different fillingmatericis used in bone regenera-tion, int J Periodontai Rest Dent1994:14:199-215.
25. Lindhe A, Thoren C, Dciniin C,Sandberg E. Oreatian of new boneby an osteopromotive membranetechnique: An experimental studyin rats. J Oroi Moxillofao Surg1993:51:892-889.
26. Sohmid J, Hammerie CHF, Sticti H.Lang NP Supraplant, o novelimplant system bosed on the princi-pie of guided bone regeneration, Apreiiminary study in the rabbit, OiinOrol impiants Res 1991:2:199-202.
27. Jovanovic SA Schenk RK. OfSini M,Kenney EB. Suprocrestoi bone for-mation o round dentai implants: Anexpérimentai dog study, int J OraiMaxiliofao Implants 1995,10:23-31.
28 Sctienk RK, Buser D, Hordwick WR,Dahiin C. Healing pattern ot boneregeneration in membrane-protect-ed defects: A histoiogic study in theoanine mandibie, Int J OralMoxiilofoc impiants 1994:9:13-29,
29. Simion M, Trisi P Pioteili A. Vertioolridge augmenfotian using amembrane teciinique associatedwith osse ointe g rated implants. IntJ Periodont Rest Dent 1994:14:497-511,
30. Tinti O, Parma-Bentenati S, Coronailypositioned paiatai sliding fiap. IntJ Periodont Rest Dent 1995:15:299-310
Volume 16, Number 3,1996
