the january 2013 digital edition of pharmacy practice news
DESCRIPTION
The January 2013 Digital Edition of Pharmacy Practice NewsTRANSCRIPT

Hollywood, Fla. and Las VegasVV —As part of the requirements of the Affordable Care Act, the Centers for Medicare & Medicaid Services (CMS) started imposing potential reimburse-ment penalties on hospitals based on their 30-day heart failure (HF) read-mission rates beginning in October 2012. Concerned about these poten-tial penalties, hospitals have ramped up efforts to forestall readmissions
Heart Failure Programs Take Aim at Readmits
Inspectors from the National Association of Boards of Pharmac
(NABP) and state pharmacy boarddescended on six compoundingpharmacies in four states during thfirst two weeks of December as parof a broad, unified effort to bolstethe safety of customized medicinebeing shipped across state lines.
The inspections were carried ouin California, New Jersey, Texas anUtah as public and political pressurfor increased federal and state regulation of pharmacy compounders continued to mount in the wake of thfungal meningitis outbreak that, bmid-December, had sickened morthan 650 individuals in 19 states anclaimed nearly 40 lives.
The dual inspection campaign is seto continue well into 2013. It is parof the association’s contractual agreement with the Iowa State Board oPharmacy to strengthen surveillancof compounding pharmacies license
In Fight for SafeCompounding, a Salvo From NABP
alth systems continue to mount, of cost-cutting strategies, many rican Society of Health-System
eting. Whether it was billing for of high-cost pancreatic enzymes employee drug benefits—the lat-nnual savings—all of the efforts laudable goal: to conserve pre- health care dollars without
mpromising patient care.
Flushing Out the Waste In Unused Medications
The Overlook Medical Cen-er in Summit, N.J., recouped
more than $500,000 in 2011—d another $350,000 from Janu-
August 2012—by ensuring that reimbursed the hospital for dis-agents and other costly drugs. ible by collaboration between s Finance Department, which
re & Medicaid Services (CMS) n levels of reimbursement for
m single-use vials. (Multidose waste reimbursement.)
Smart Strategies for Savings Presented at ASHP Meeting
In most health systems—even those with well-established electronic medi-
cal records—reporting adverse events is a spotty and not alwaysstandardized process.
New software called KBCoremay change that. In November, the program’s developer, CRG Med-ical, won the Reporting Patient Safety Events Challenge issued by the Office of the National Coordinator for Health Infor-mation Technology (ONC), in part due to the software’s flexibility: It enables users to generate error reports from any mobile
device or within the EMR simply by scan-ning a patient’s bar code. The program
also is garnering positive reviews for the depth of relevant data that userscan rapidly access.
“Most reporting systems I’m famil-iar with don’t take advantage of the
existing electronic data [they contain],” said Matt Grissinger, RPh, the director of
error reporting programs at the Institute for Safe Medication Practices. “We already have the patient ’s name, room number, the medications they’re on, their dosages and so
ADE Tracking May Get BoostFrom New Reporting Software
Printer-friendly versions available online
pharmacypracticenews.com The Pharmacist’s News Source Volume 40 • Number 1 • January 2013
• see ADE TRACKING, page 3
• see SAVINGS, page 17
in this issue
40th ANNIVERSARY YEAR 1972–2012
• see HF READMISSIONS, page 8
• see NECC CRISIS, page 1
21 New rules forreimbursement change the payment landscape.
POLICY
12 Compliance experts say time is now to plan for audits and surveys.
15 Are you measuringup to CMS’ core measures? Here’s how to tell.
OPERATIONS & MGMT
The Book Page
Clinical Skills for Pharmacists:A Patient-Focused
Approach/Edition 3Karen J. Tietze
Visit mcmahonmedicalbooks.com
5 Cleveland Clinic’s drug information FAQ database: a rich resource.
7 ED pharmacists document $225,000 in annual savings.
8 In heart failure, baseline albumin may signal poor renal function.
11 Protocols aim at reducing risk from fibrate–statin combinations.
CLINICAL
Immune Globulins:Therapeutic, Phamaceutical, Cost, and Administration Considerations
See insertafter page 4.
EDUCATIONAL REVIEW
ki G
Las Vegas—As the financial pressures on heafacilities are responding with a wide range
of which were presented during the AmePharmacists 2012 Midyear Clinical Mee
drug waste, putting limits on the use oor having pharmacy leaders manage eter racking up nearly $2 million in an
shared acious
com
FI
tm
andary to
Medicare rcarded portions of biological a
The payments were made possthe pharmacy and the hospital’s
identified Centers for Medicarregulations allowing certain
wasted medications fromvials are not eligible for w
o-y sg
hert er es
utd
re a-n-heby re d
et rte-of ce d
P
19

New FDA-approved IV premix drug labeling from Baxter.To help reduce medication errors due to incorrect drug selection, we redesigned the labeling for some of our most widely used liquid premix medications. We decreased the clutter and placed information in a consistent manner. Contact your Baxter sales representative to see how with change comes clarity.
Drug delivery from Baxter Healthcare Corporation.Doing our part, so you can do yours.
Medication Delivery
111779 12/12
pharmacy workflow I drug delivery I nutrition I iv access I infusion systems I support & service
Baxter is a registered trademark of Baxter International Inc.
Sometimes appearances
are everything.
MCPPN2302.indd 1 12/12/12 8:27 PM

on—yet [unlike KBCore], many systemsmake you re-enter [that information].”
Although several other programs allowpharmacists to document their phonecalls and let users pull patient data rightinto the program, “they’re not adverseevent reporting programs like this oneis,” Mr. Grissinger said.
Jerry Fahrni, PharmD, a product man-ager at Talyst who frequently blogs onnew pharmacy technologies and tweetedthe news about KBCore, also sees thepotential of the new software. “It’s a big deal to have all that information at yourfingertips,” he said. “Every drug’s NDC[National Drug Code] number potentially can be found in the bar code, and by scan-ning it, this system can accurately popu-late the [fields for the] strength of thedrug, the manufacturer and all the otherdata.” The program also allows for theinput of additional information once theinitial report has been submitted.
KBCore was one of 13 submissionsto the ONC Challenge, which evalu-ated reporting systems based on fivefactors: effectiveness; usability anddesign; innovation and creativity;integration with electronic medicalrecords (EMRs) and secure transmis-sion capabilities; and ability to lever-age the nationwide health informationnetwork, an initiative for the exchangeof health care information being devel-oped under the auspices of ONC.
“The platform itself was easy to useand clear to understand; we saw sub-
missions in this and other challenges that involve reporting, and input can be quite messy,” Adam Wong, a manage-ment and program analyst at the ONC, told InformationWeek Healthcare. “If the solution isn’t much easier to use than what already exists, it’s not mov-ing things forward.”
No Gold Standard Yet
Dr. Fahrni agreed that current adverse drug event reporting systems are in need of improvement. Indeed, at present, “there’s no nationally recog-nized gold standard system for adverse event reporting; there’s no software that really stands out,” he said. “In most hospitals today, people will do it manu-ally. There’s no great way to collect that data and get it to a centralized spot.”
Vicki Tamis, PharmD, BCPS, a clini-cal quality informaticist at PeaceHealth
Southwest Medical Center, in Van-couver, Wash., also sees flaws in how most hospitals manage the tracking and reporting of adverse drug events. “We find that people who submit reports into the electronic system don’t always get all the accurate information entered,” Dr. Tamis said. “Depending on the reporting program, sometimes the dos-age information or route of administra-tion isn’t correct.” Thus, the medication error report “is usually just a starting point. Almost every time you have to review a patient’s record for an adverse event or medication safety problem, it can take a lot of detective work to pull the full story together.”
As for the KBCore software, Dr. Tamis said it looked promising. But she noted that it could be improved by adding an automated system response when specific drugs or doses of certain drugs
are given. “It would be nice if somebody could design a product that would auto-matically, if a certain dose of X medica-tion is given, pull in [elements] of analy-sis you would need,” she said.
While praising the KBCore applica-tion, Mr. Grissinger cautioned that any adverse event reporting program is only as good as the reporting culture at each hospital. “You could buy the Cadillac of reporting programs, but if your environ-ment is punitive, it still won’t happen.”
The other complaint ISMP hears fre-quently, he noted, “is that institutionshave a big rollout of a reporting system and then people hear nothing and see no action being taken when they do report events. A program like this can make the process easier, but at the end of the day you have to change the culture.”
—Gina Shaw
WANT TO SUBSCRIBE?CHANGE YOUR ADDRESS?HERE’S HOW
All U.S. hospital pharmacists should re ceive Pharmacy Practice News free of charge. If you are a hospital pharma-cist and do not receive the publication, you must add your professional address or make your address change directly
with Pharmacy Practice News, Circulation Dept., 545 W. 45th St., 8th Floor, New York, NY 10036. You can also fax your request to (212) 977-3645, or send it viaemail, [email protected].
If you are not a hospital pharmacist but would like to re ceive Pharmacy Practice News, please send a check for $70.00 (U.S.) or $90.00 (outside U.S.) for a year’s subscrip-
tion pay able to Pharmacy Practice News to McMahon Pub-lish ing, 545 West 45th St., 8th Floor, New York, NY 10036. Please allow 8 to 12 weeks for delivery of the first issue. In dividual issues are $7.00 (U.S.) or $10.00 (outside U.S.).
McMahon Publishing is a 40-year-old, first-generation,family-owned publishing company dedicated to providingmedical professionals with essential, up-to-date news. As
the second largest publisher of medical newspapers, McMahon produces Anesthesiology News, Clinical Oncology News, Gastroenterology & Endos copy News, General Surgery News, Infectious Disease Special Edition, Pain Medicine News, Phar macy Practice News. Rheumatology Practice News and Specialty Pharmacy Continuum.
EDITORIAL BOARD
ADMINISTRATION
Robert Adamson, PharmD, Livingston, NJ
Ernest R. Anderson Jr., MS, RPh, Boston, MA
ANESTHESIOLOGY/PAIN
Julie A. Golembiewski, PharmD, Chicago, IL
Melvin E. Liter, MS, PharmD, FASHP, Lexington, KY
David S. Craig, PharmD, BCPS, Tampa, FL
Robert L. Barkin, MBA, PharmD, Chicago, IL
BIOTECHNOLOGY
Indu Lew, PharmD, Livingston, NJ
CARDIOLOGY
C. Michael White, PharmD, Storrs, CTs
CNS/PSYCHIATRY
Charles F. Caley, PharmD, Storrs, CT
Lawrence Cohen, PharmD, FASHP, FCCP, Fort Worth, Texas
Larry Ereshefsky, PharmD, San Antonio, TX
COMPLEMENTARY AND ALTERNATIVE MEDICINE
Cathy Rosenbaum, PharmD, Cincinnati, OH
CRITICAL CARE
Judi Jacobi, PharmD, FCCM, Indianapolis, IN
INFECTIOUS DISEASES
Steven J. Martin, PharmD, BCPS, FCCM, Toledo, OH
Peggy McKinnon, PharmD, Lexington, MAMM
David P. Nicolau, PharmD, Hartford, CT
Robert P. Rapp, PharmD, Lexington, KY
INTERNAL MEDICINE
Geoffrey C. Wall, PharmD, FCCP, BCPS, CGP, Des Moines, IA
NUCLEAR PHARMACY
Jeffrey Norenberg, PharmD, Albuquerque, NM
ONCOLOGY
Robert T. Dorr, PhD, RPh, Tucson, AZ
Robert Ignoffo, PharmD, San Francisco, CA
Philip E. Johnson, MS, RPh, FASHP, Tampa, FL
Cindy O’Bryant, PharmD, Aurora, CO
Ali McBride, PharmD, MS, BCPS, St. Louis, MO
Sara S. Kim, PharmD, BCOP, New York, NY
PEDIATRICS
Gretchen Brummel, PharmD, BCPS, Hudson, OH
REIMBURSEMENT
Bonnie E. Kirschenbaum, MS, FASHP, Breckenridge, CO
TECHNOLOGY
Thomas Van Hassel, RPh, Yuma, AZ
EDITORIAL STAFFDavid Bronstein, Editorial Director [email protected]
Sarah Tilyou, Senior [email protected]
Kevin Horty, Don Pizzi, Adam Marcus, Cynthia Gordon, Contributing Editors
James Prudden, Group Editorial Director
Robin B. Weisberg, Manager, r Editorial Services
Elizabeth Zhong, Associate Copy Chief
SALES
David Kaplan, Group Publication [email protected]
Matt Spoto, Senior Account [email protected]
David Nathanson, Account [email protected]
Alina Dasgupta, Junior Sales Associate, Classified [email protected]
ART/PRODUCTION STAFFMichele McMahon Velle, MAX Graphics/Creative Director
Frank Tagarello, Senior Art Director/Managing// Director, rrMAX Graphics
James O’Neill, Senior Systems Manager
Dan Radebaugh, Director of Production and Technical Operations
Marty Barbieri, Production Manager
Brandy Wilson, Circulation Coordinator
McMAHON PUBLISHINGRaymond E. McMahon, Publisher and CEO, Managing PartnerVan Velle, President, PartnerMatthew McMahon, General Manager, PartnerLauren Smith, Michael McMahon, Michele McMahon Velle,
Rosanne C. McMahon, Partners
MCMAHON PUBLISHINGMCMAHONMED.COMSales, Production and Editorial Offices: 545 West 45th Street, 8th Floor, New York, NY 10036. Telephone: (212) 957-5300.Corporate Office: 83 Peaceable Street, Redding CT 06896
Copyright © 2013 McMahon Publishing, New York, NY 10036. All rights reserved. Pharmacy Practice News(ISSN 0886-988x) is published monthly by McMahon Publishing. Periodicals postage paid at New York, NY, andat additional mailing offices. POSTMASTER: Send address changes to Pharmacy Practice News, Circulation Dept.,545 W. 45th St., 8th Floor, New York, NY 10036.
Volume 40 • Number 1 • January 2013 • pharmacypracticenews.com
A family-owned medical publishing and medical education company. McMahon publishes seven clinical newspapers and several annual or semiannual Special Editions.
ADE TRACKINGcontinued from page 1
‘You could buy the Cadillac of [adverse event] reporting programs, but if your
environment is punitive, it still won’t happen.’—Matt Grissinger, RPh
Pharmacy Practice News • January 2013
Medication Safety
Technology 3

Vertical integration with geographic diversity helps ensure continuous production of therapies 1
1
Grifols
Albumin Albutein® 5% Albutein® 25% Plasbumin®-5 Plasbumin®-25Alpha1- Proteinase Inhibitor Prolastin®-CAntihemophilic Factor/von Willebrand Factor Complex Alphanate®
Antithrombin III Thrombate III®
Coagulation Factor IX AlphaNine® SDFactor IX Complex Profi lnine® SDImmune Globulin Intravenous IVIGImmune Globulin InjectionHyperimmune Globulin Therapy Products Hypermunes™:
Rabies Immune Globulin HyperRAB® S/DTetanus Immune Globulin HyperTET® S/DRho(D) Immune Globulin HyperRHO® S/DHepatitis B Immune Globulin HyperHEP B® S/D
A Broad Range of Plasma Protein Therapies
Learn more about how Grifols can meet your hospital’s needs at www.grifols.com
MCPPN2303.indd 1 12/17/12 4:06 PM
The Drug Information (DI) Centerat the Cleveland Clinic serves as
a resource for health care providers at10 hospitals, more than 150 ambulatory clinics, and 15 ambulatory pharmacies inthe Cleveland Clinic Health System. Aninternal electronic database, only acces-sible to the 8 DI pharmacists, stores morethan 10 years of questions presented tothe DI Center and answers the DI phar-macists provided. Often, staff pharma-cists call specifically for the DI pharma-
cists to access the database if they know a question previously was answered.
To share information stored in the internal database, a DI Frequently Asked Questions (FAQs) Database was created to be accessible by pharmacy staff. The database is intended to pro-vide concise information about FAQs as well as hospital-specific clinical prac-tice, information required in emergent situations, and information not readily available. The database is designed to be searchable by category (eg, Cleveland Clinic policy and procedures, crush/administration, vaccines, immunoglob-ulins) or keyword. At first, only the DI staff submitted questions to be added to the database. However, as the database has gained more popularity and has
been more widely used, staff pharma-cists have contacted the DI Center with FAQs and responses to be added.
Each response is written in a concise format and is referenced with the most current information and/or reflects stan-dard clinical practice at the Cleveland Clinic. Responses are added to the DI FAQ Database after a peer-review pro-cess in which 2 DI pharmacists verify the validity and accuracy of the informa-tion. To ensure the DI FAQ database is used as a reference and not in place of a clinical decision-making process, there is a disclaimer that states: “This Fre-quently Asked Questions (FAQ) Database is intended for use as a REFERENCE ONLY. It is specific to adult patients (ie, >18 years) unless specified in the
response. Patient-specific factors (eg, age, weight, renal or hepatic function,comorbid conditions, concomitant medi-cations) should ALWAYS be taken intoaccount, along with the most current drug information, medical literature, andstandards of practice.”
In addition to having all sources list-ed in each response, the date when theresponse was added and the last-updated date are included. This information wasincluded to assist the pharmacist in mak-ing a judgment call on whether there may be more up-to-date information available or if the DI Center should be contacted. All of the responses are given internal numbers for indexing and arein an annual rotation to be reviewed andupdated with new information.
Development of a Drug Information FAQ DatabaseKatie Stabi, PharmDDrug Information Pharmacist (REMS)Department of PharmacyCleveland ClinicCleveland, Ohio
continued on page 6
Can dabigatran capsules be opened for oral or feeding-tube administration?
Dabigatran (Pradaxa, Boehringer Ingelheim) capsules should be
swallowed whole and should NOT be broken, chewed, or opened beforeadministration. The bioavailability ofdabigatran etexilate increases by 75%when the pellets are taken without the capsule shell.
SourcePradacapsuRidgePharm
Log NAnswUpda
Why is ideal body weight used to dose Gammagard Liquid 10% (IV immunoglobulin)?
Gammagard Liquid 10% (IV immunoglobulin [IVIG]; Baxter) is dosed by ideal body weight (IBW) dueto standard Cleveland Clinic Foundation clinical practice. Adjusted body weight should be used if the
total body weight is more than 30% to 40% of the IBW.IVIG has a low volume of distribution (0.09-0.13 L/kg) and is believed to stay primarily in the intravascular
space with little distribution into the fat. There is limited published information available on dosing IVIG by IBW because the original studies used total body weight. However, several sources recommend using adjusted body weight in the obese population and suggest dosing with IBW may be an option for IVIG therapy.
SourcesStandard Cleveland Clinic Foundation Clinical Practice.
Immune Globulin Monograph. Lexicomp Online, Lexi-Drugs Online. Hudson, Ohio: Lexicomp, Inc; January 2012.
Siegel J. Immunoglobulins and obesity. Pharmacy Practice News. 2010;37:8-9.
Herman. Safe administration of intravenous immune globulin (IVIG). World of Drug Information. 2004;15.
Khan S, Grimbacker B, Boecking C, et al. Serum trough IgG level and annual intravenous immunoglobulin dose are not related to body size in patients on regular replacement therapy. Drug Metab Lett. 2011;5:132-136.
Rand K, Gibbs K, Derendorf H, Graham-Pole J. Pharmacokinetics of intravenous immunoglobulin (Gammagard) in bone marrow transplant patients. J Clin Pharmacol. 1991;31:1151-1154.
Log Number: 20968; Answered: 1/24/2012; Updated: 2/24/2012
Can duloxetine capsules be opened for oral or feeding-tube administration?
Duloxetine (Cymbalta, Lilly) delayed-release capsules contain enteric-coated pellets that should be swallowed whole and should NOT be chewed, crushed, or opened. The contents should NOT be sprinkled on food or
mixed with liquid because doing so may affect the enteric coating. Duloxetine is listed on the “Do Not Crush” list by the Institute for Safe Medication Practices, Lexicomp, and Micromedex.
The pellets should NOT be administered via feeding tube because that has not been studied and could poten-tially clog the feeding tube.
Caution: There is an in vitro study that determined a 20-mg duloxetine capsule maintained its potency, purity, and dissolution when mixed with applesauce and apple juice (pH ~3.5). The efficacy and safety for oral administration was NOT tested. However, if this method is to be used, it is important that the pellets maintain their integrity and are NOT crushed, chewed, or broken. This study also found that the duloxetine pellets did NOT maintain potency, purity, and dissolution when mixed with chocolate pudding (pH ~5.5-6.0).
oxetine) delayed-release capsules for oral use [package insert]. Indianapolis, IN: Lilly USA, LLC; September 2011.
ral dosage forms that should not be crushed. Institute for Safe Medication Practices. Oct 2011. http://www.ismp.org/tools/donotcrush.pdf. December 19, 2011.
mp Online, Lexi-Drugs Online. Hudson, Ohio: Lexicomp, Inc; December 2011. (Search “crush.”)
edex Healthcare Series [Internet database]. Greenwood Village, CO: Thomson Reuters (Healthcare) Inc. Updated periodically. “crushed.”)
A, Losin WG. In vitro stability, potency, and dissolution of duloxetine enteric-coated pellets after exposure to applesauce, apple juice, and e pudding. Clin Ther. 2008;30:1300-1308.
g Number: 20670; Answered: 12/19/2011; Updated: 2/15/2012
W(
urceaxa (dabigatran etexilate mesylate) ules for oral use [package insert]. efield, CT: Boehringer Ingelheimmaceuticals, Inc; November 2011.
Number: 20669; wered: 12/19/2011;ated: 2/15/2012
SourcesCymbalta (dul
Mitchell JF. OrAccessed D
Lexicom
Microme(Search “
Wells KAchocolate
Log
Pharmacy Practice News • January 2013
Practice Pearl
Clinical 5

yThe FAQ DI Database is used frequently by the DI staff and was accessed by pharmacy staff more than 2,000 times over a recent 6-month period.
The FAQ DI Database would not be possible without the help of Mandy Leonard, PharmD, r Janine Douglas, PharmD, Matthew Miller, CIS, and the drug information pharmacist peer
reviewers: Marigel Constantiner, RPh, Meghan Lehmann, PharmD, Mandy Leonard, PharmD, AAmy Martin, PharmD, Kara Sink, RPh, Christopher Snyder, RPh, and Marcia Wyman, PharmD.
continued from page 5
Can the zoster vaccine live be given concurrently with the pneumonia vaccine?
The zoster vaccine live (Zostavax, Merck) and the pneumonia vaccine (Pneumovax 23, Merck) can be given to a patient on the same day.Although the manufacturer suggests that prescribers should consider
administering Zostavax and Pneumovax 4 weeks apart, the Advisory Committee on Immunization Practices (ACIP) and the FDA support the administration of the 2 vaccines concomitantly.
The vaccines should be administered using separate syringes at different anatomic sites.
SourcesZostavax (Zoster Vaccine Live) suspension for subcutaneous injection [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; June 2011.
Centers for Disease Control and Prevention. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP)–early release. MMWR Recomm Rep. 2008;57:e1-e31.
Baylor NW. Letter to the editor: Perspective of the U.S. Food and Drug Administration on concomitant administration of Zostavax and Pneumovax. Vaccine. 2011;29:8771.
National Center for Immunization and Respiratory Diseases . General Recommendations on Immunization: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep.2011;60:8-9, 38.
Log Number: 21004; Answered: 1/26/2012; Updated: 4/17/2012What medications containing caffeine can be used to treat postdural puncture headaches?
Apostdural puncture headache (PDPH) is a complication of spinal anesthesia or unintentional dural puncture. A PDPH usually is treated with IV caffeine/
sodium benzoate (500 mg in 1,000 mL normal saline administered over 1 hour, followed by 1,000 mL normal saline infused over 1 hour); a second course of caffeine can be given for unrelieved headache pain in 4 hours. The 500-mg dose of caffeine and sodium benzoate contains 250 mg of anhydrous caffeine and 250 mg of sodium benzoate, which helps increase the solubility of the caffeine.
When caffeine/sodium benzoate is not available, 300 mg of oral anhydrous caffeine as a single dose can be used. Caffeine citrate oral solution is available as 20 mg/mL and contains 10 mg/mL of caffeine base. Therefore, 30 mL ofcaffeine citrate 20 mg/mL oral solution contains 300 mg of anhydrous caffeine.
SourcesLexicomp Online, Lexi-Drugs Online. Hudson, Ohio: Lexicomp, Inc; February 2012; February 15, 2012.
Drug Evaluation: Caffeine. In: Hutchison TA, Shahan DR, Anderson ML, eds. Drugdex System [internet database]. Greenwood Village, CO: Thomson Healthcare; 2012. Updated periodically.
Caffeine and sodium benzoate–caffeine injection, solution [package insert]. Shirley, NY: American Regent, Inc.; September 2008.
Caffeine Citrate–caffeine citrate injection, solution [package insert]. Shirley, NY: American Regent, Inc.; September 2011.
Camann WR, Murray RS, Mushlin PS, Lambert DH. Effects of oral caffeine on postdural puncture head-ache. A double-blind, placebo-controlled trial. Anesth Analg. 1990:70:181-184.
Choi A, Laurito CE, Cunningham FE. Pharmacologic management of postdural puncture headache.Ann Pharmacother. 1996;30:831-839.
Log Number: 21229; Answered: 2/27/2012; Updated: 4/20/2012
How can copper be replenished in a copper-deficient patient?
The most appropriate dose, duration, route, and form of copper supple-mentation in copper-deficient patients (acquired copper deficiency,
copper deficiency myelopathy) have not been studied. It is recommended to first discontinue any zinc therapy and use oral copper therapy, if needed, rather than IV therapy. However, IV therapy may be needed if the oral absorption of copper is blocked or if there is an urgent need due to the patient’s clinical condition.
The preferred route is oral; 2 mg per day of elemental copper is usually sufficient, although doses as high as 9 mg per day have been used. Some sources recommend starting with 6 to 8 mg per day of elemental copper for 1 week, then decreasing the dose by 2 mg each week. Additionally, some sources recommend periodic reassessment of the serum copper level to determine if replacement therapy is adequate, and dose adjustment as needed.
Oral therapy recommendations: Over-the-counter multivitamins are an option for oral therapy. The pharmacy usually stocks Therapeutic M (multivi-tamins, therapeutic with minerals PLUS IRON tablet [THEREMS-M]) tablets,which contain 2 mg of copper. It is important to read product labels to deter-mine the amount of copper in the product. For example, Centrum Kids com-plete chewable tablets contain 2 mg copper per tablet, whereas Centrum Silver tablets contain 0.5 mg copper per tablet. There are no FDA-approved single-ingredient products available, and, per hospital policy, dietary supplements that are not FDA-approved will not be ordered, stocked, or dispensed.
IV therapy recommendations: 2 mg per day of elemental copper infusedover 2 hours for 5 days, then periodically thereafter. IV copper is available as single-entity cupric sulfate (0.4 mg elemental copper/mL) and cupric chloride (0.4 mg elemental copper/mL), with the primary indication for use as an additive in parenteral nutrition. Verify with the IV room that an IV product is available because both products recently have been in short supply.
SourcesKumar N. Copper deficiency myelopathy (Human Swayback). Mayo Clin Proc. 2006;81(10):1371-1384.
Jaiser SR, Winston GP. Copper deficiency myelopathy. J Neurol. 2010;257:869-881.
Product Information. Therems-M vitamin and mineral supplement. Rugby Laboratories, Inc. http://www.watson.com/products/product-database-detail.asp?currentPage=2&group=alpha&c=T. Accessed May 31, 2012.
Centrum.com. Accessed December 20, 2011.
Cleveland Clinic Pharmacy. Policy Number 03-055. Dietary Supplements: Formulary. Effective Date 02/08/07, Dates Revised 02/23/10, 04/02/12.
Log Number: 22114; Answered: 6/21/2012; Updated: 6/21/2012
Are Imovax (human diploid cell rabies vaccine) and RabAvert (purified chick embryo cell rabies vaccine) interchangeable?
Imovax (human diploid cell rabies vaccine, Sanofi Pasteur) and RabAvert (purified chick embryo cell rabies vaccine, Novartis) are generically
equivalent and are considered interchangeable. If available, the same brand should be used for the entire vaccination series. However, vaccination should NOT be deferred due to unavailability of the brand used for previous doses.
A 2-year comparative study showed that the immunogenicity and reactogenicity of the 2 products are comparable. The dose, route, and indications of the 2 products are the same, but their origins, excipients, and side-effect profiles are different.
SourcesGrabenstein JD. ImmunoFacts: Vaccines and Immunologic Drugs–2012 (37th revision). St. Louis, MO: Wolters Kluwer Health; 2011.
Dreesen DW, Fishbein DB, Kemp DT, Brown J. Two-year comparative trial on the immunogenicity and adverse effects of purified chick embryo cell rabies vaccine for pre-exposure immunization. Vaccine. 1989;7:397-400.
Manning SE, Rupprecht CE, Fishbein D, et al. Human rabies prevention–United States, 2008: recommen-dations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2008;57:1-28.
Imovax Rabies (rabies vaccine, HDCV) [package insert]. Swiftwater, PA: Sanofi Pasteur, Inc.; December 2005.
RabAvert (rabies vaccine) [package insert]. Emeryville, CA: Novartis Vaccines and Diagnostics, Inc.; March 2010.
Log Number: 21038; Answered: 1/31/2012; Updated: 3/29/2012
Does Zostavax (zoster vaccine live) need to be readministered if it was given intramuscularly instead of subcutaneously?
The Zostavax (zoster vaccine live) vaccine should be given subcutaneously in the deltoid region of the upper arm and not injected intravascularly or
intramuscularly. However, if Zostavax is given intramuscularly, it does NOT need to be readministered.
SourcesDepartment of Health and Human Services Centers for Disease Control and Prevention. Herpes zostervaccination for health care professionals. http://www.cdc.gov/vaccines/vpd-vac/shingles/hcp-vaccination.htm. Accessed August 14, 2012.
Zostavax (Zoster Vaccine Live) suspension for subcutaneous injection [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; June 2011.
Log Number: 22571; Answered: 8/16/2012; Updated: 8/16/2012
Pharmacy Practice News • January 2013
Practice Pearl
6 Clinical

In tough economic times, it is stillpossible to start an emergency
department (ED) pharmacy and actu-ally save money in the process.
That is the experience reported in a study of an ED pharmacy at Francis-can Saint Margaret Health (FSMH),in Hammond, Ind (Am J Health Syst ((Pharm 2012;69:1682-1686). By shifting existing staff pharmacists to the ED toperform medication reconciliation, thehospital documented $225,000 in costsavings and also improved the accuracy of reconciliation efforts.
From the start, the ED pharmacy initiative at FSMH was focused onmedication reconciliation. But its useof existing pharmacy staff to performthat task was something of a pivot forthe program, lead author Bhavik Nana,PharmD, told Pharmacy Practice News.The hospital initially had receivedapproval to hire three pharmacy techni-cians for the program, but because of economic conditions, the planned posi-tions were eliminated. If an ED pharma-cy were to be established, it would needto begin with no additional funding for technicians or pharmacists.
“That’s basically what we did,” Dr.Nana noted. To launch the program, twopharmacists were secured for the EDprogram from FSMH’s existing full-timeequivalent (FTE) staff. Staffing scheduleswere adjusted, with the pharmacists pro-viding ED services from 11:30 a.m. to 5:30p.m. on weekdays. The manager of thecentral order-entry pharmacy agreed toexpand hours of coverage at no additionalcost. A small, centrally located area in theED became an ED pharmacy workspace.The two pharmacists received training inadmission medication reconciliation andcritical care drugs, and were certified inadvanced cardiac life support and pedi-atric advanced life support.
Commercially available pharmacy intervention software was used to doc-ument interventions. A retrospectivechart review of a random sample of admission medication reconciliations(N=102) showed that 90.2% of recon-ciliations (46 of 51) performed by phar-macists were accurate compared with66.7% of those (34 of 51) performed by nurses (P(( <0.05). A survey of ED admit-ting nurses and physicians found thatthe ED pharmacists were well received.Annualized cost savings attributable topharmacist activities totaled $225,000,including both soft-dollar and hard-dollar cost savings. Soft-dollar cost sav-ings resulted from projected cost avoid-ance, for example, owing to medicationreconciliations; hard-dollar cost sav-ings resulted directly from accepting a pharmacist recommendation, such asfor a drug choice.
Dr. Nana said he is proud of the suc-cesses documented in the study. “This is a challenging time for the health care
field,” he stressed. “One of the chal-lenges health care facilities are facing is [reduced] reimbursement rates. We
have to work harder with the same limited resources. This study is a good
Starting an Emergency Department Pharmacy at Low Cost
• see PHARM COST, page 14
‘This study is a good demonstration of how even in
these [challenging economic] times, new programs
like this can be initiated to help improve patient
care at the hospital.’—Bhavik Nana, PharmD
Unit Dose,Bar Coding,Pharmacy &Nursing SupplyExperts!
800.523.8966 MediDose.com
Medi-Dose/EPS labels are specifically designed for everyneed…from solids to liquids, syringes to ampules, IV linesand bags to insulin and suppositories. Plus, with our MILT® software, you can even add optional bar codes.You name it. At Medi-Dose/EPS, there’s a label for that!
Unit Dose,Bar Coding,Pharmacy &Nursing SupplyExperts!
Scan to see these labels in action! �
Pharmacy Practice News • January 2013
Critical Care
Clinical 7

among those in this vulnerable targetpopulation, and several abstracts pre-sented at recent pharmacy meetingssuggest that pharmacist-led multidisci-plinary efforts, including patient drug education and follow-up, can lower hos-pital readmission rates related to HF.
“Many institutions are trying their bestto come up with methods to meet therequirements, and pharmacists are anintegral part of the solution,” said RobertLee Page II, PharmD, an associate profes-sor of clinical pharmacy and a physicalmedicine clinical specialist in the Divi-sion of Cardiology at the University of Colorado School of Pharmacy and Medi-cine, in Aurora. “Every hospital has itsown different case mix, but these studiesshow we can all learn from each other.”
A Coordinated MultidisciplinaryApproach Works
Responding to the threat of possiblefinancial penalties, researchers at TheNebraska Medical Center, in Omaha,conducted a study involving pharma-cists, nurses and nutritionists to helplower readmission rates. The study included early identification of patientswith HF upon admission, interdisci-plinary education during the inpatientstay and interdisciplinary follow-upphone calls after discharge.
“I was surprised that our efforts notonly improved the patients’ under-standing of the disease process butalso enhanced their resolve and com-mitment to take their medications andpay more attention to their symptoms,”said Brian Trevarrow, PharmD, the leadresearcher, who presented the study atthe American College of Clinical Phar-macy (ACCP) annual meeting.
The educational efforts—whichfocused on the pharmacologic effects on disease pathophysiology, possible sideeffects, dosing, regimen adherence, drug interactions and special instructions—were initiated in January 2011. Pharma-cists, nurses and nutritionists all calledpatients four times: 24 to 48 hours after discharge, within one week, at three tofour weeks and again after 30 days.
The team retrospectively analyzed thereadmissions of 532 patients in 2010(pre-education group) and prospective-ly analyzed the readmissions of 482patients exposed to the education pro-gram in 2011. The two groups of patientshad comparable comorbidities anddemographics and were taking similarmedications. The rate of all-cause read-mission was significantly reduced afterimplementation of the multidisciplinary program, from 28% in 2010 to 20% in2011. The incidence of HF readmissionsalso decreased from 12% to 5%.
The follow-up efforts were ambitious
and rewarding, said Dr. Trevarrow, the coordinator of the Anticoagulation Stewardship and Heart Failure program at the medical center, and a clinical assistant professor at the University of Nebraska College of Pharmacy, in Oma-ha. “Patients [had been] taking medica-tions for years just because they were told to,” said Dr. Trevarrow, noting that after the program was initiated, sev-eral patients thanked him for explaining how the medications work and why it was important to take them.
Patient Education and Follow-Up
A second study presented at the ACCP meeting also underscored the value of helping patients understand the importance of taking their medica-tions and showed lower hospital read-mission rates when pharmacists were involved in patient care during the hos-pital stay as well as after discharge.
During the study, investigators evalu-ated patients admitted to Atlanta Medi-cal Center with a primary or secondary
diagnosis of HF between Aug. 1, 2011 and Jan. 30, 2012, randomizing them into control (n=38) and intervention (n=22) groups. The baseline character-istics, which included ejection fraction, hospital length of stay and comorbidi-ties, were similar between the popula-tions. Control group patients received the standard of care. Intervention group patients received one-on-one medica-tion and disease management discharge counseling from a pharmacist. Patients were called 14 and 28 days after dis-charge. The 30-day readmission rate for patients in the intervention group (9.5%) was approximately 50% lower than for the patients in the control group (21%).
“Heart failure patients are at risk for coming back to the hospital soon after discharge. Because of this pilot study, we now have a program where patients are screened for readmission risk,” said Pamela M. Moye, PharmD, the lead researcher and a clinical assistant professor in the Department of Phar-macy Practice at Mercer University, in
Atlanta. “All patients who are in the mod-erate to high–risk group will have a phar-macy consult and follow-up.”
Pharmacist-ManagedMedication Optimization
A third related ACCP study dealt with the chronic problem of underdos-ing cardiac medications, such as angio-tensin-converting enzyme inhibitors (ACEIs) and β-blockers in the treat-ment of HF. National guidelines recom-mend maximizing therapy to reduce mortality and the number of rehospi-talizations. Pharmacists from the Uni-versity of Illinois at Chicago (UIC) man-aged a clinic for a half-day every other week to help patients maximize theirACEIs and β-blockers. At each visit, the pharmacist reviewed vitals, symptoms, educational needs, laboratory results and medication regimens. ACEIs and β-blockers were titrated as tolerated.
Since the clinic opened in July 2011, the HF pharmacist has made 126 visits to 46 patients, and 64% of cardiologists referred their patients to the clinic for medication optimization. The pro-gram was so successful that within a month, the half-day clinic had to oper-ate every week.
“What’s unique is that it lets me work independently. I don’t need to call a phy-sician before I make a medication adjust-ment,” said Vicki L. Groo, PharmD, the lead researcher and a clinical pharmacistat UIC. Prescriptions and the progressnote are sent to the referring cardiologist for cosignature. The clinic pharmacistsees patients at two-week intervals, witha cardiologist available for additional consultation as needed.
Pharmacist services at the clinic are billed via a hospital-based facility feemodel at a level 3 or 4 technical fee, depending on visit complexity. Dr. Groosaid that because she was already work-ing in the university’s Heart Center, thecosts of implementing this new clinicwere minimal.
The fact that UIC is getting “some reimbursement for pharmacy services … shows that their services are valued,”said Dr. Page, adding, “In order to sustain a program, you need reimbursement.”
VA Hospital Looks for Clues
A study presented at the American Society of Health-System Pharmacists(ASHP) Midyear Clinical Meeting evalu-ated the factors leading to HF readmis-sions at the Jesse Brown Veterans AffairsMedical Center, in Chicago. At the VA medical center, like at UIC, underdosing was a factor contributing to HF readmis-sions. The VA team retrospectively eval-uated patients with a HF diagnosis who were discharged from the medical center between Oct. 1, 2010 and March 1, 2011, comparing those who were readmitted
Baseline Albumin Predicts Worsening Renal Function in Heart Failure Patients
HOLLYWOOD, FLA.—Albumin levels less than or equal to 3 g/dL signal worsen-ing renal failure (WRF) in patients with acute decompensated heart failure
(ADHF), according to a recent University of Michigan study presented at the ACCP annual meeting.
“Our study looked at baseline characteristics to help predict which patientsreceiving continuous infusions of loop diuretics were predisposed to develop WRF, whereas other research has studied what happened during infusion,when it may be too late to prevent WRF,” said Megan Barnes, PharmD, the lead researcher and a clinical pharmacy specialist in cardiology at West PennAllegheny Health System, in Pittsburgh. Aggressive diuresis with loop diuretic infusions often is necessary for symptom relief in patients hospitalized for ADHF, said Dr. Barnes. But it can lead to development of WRF, which has been associated with increased mortality.
Dr. Barnes and her team performed a retrospective observational analysis of 177 patients with ADHF who were receiving continuous infusions of loop diuretics. The study included all patients who were admitted to the Universityof Michigan Health System with ADHF between January 2006 and June 2009and received the infusions. WRF was defined as an increase of at least 0.3 mg/dL from the baseline serum creatinine value.
The mean patient age was 61 years and the median length of loop diuretic infusion was four days. Forty-eight patients (27%) experienced WRF and 34 (19%) died during hospitalization. A myriad of other factors were consideredas predictors of WRF, including advanced age, severity of HF, baseline demo-graphics, comorbidities and medications.
“It’s not surprising that low albumin would be a predictor, because it’s also indicative of nutritional status,” said Robert Page II, PharmD, MSPH, an associ-ate professor of clinical pharmacy and a physical medicine clinical specialist inthe Division of Cardiology at the University of Colorado School of Pharmacyand Medicine, in Aurora. “If patients are nutritionally depleted, it makes sense they may not fare well with high-dose diuretics.”
—D.H.S.
Drs. Barnes and Page reported no relevant fi nancial confl icts of interest.
HF READMISSIONScontinued from page 1
• see HF READMISSIONS, page 11
Pharmacy Practice News • January 2013
Cardiology
8 Clinical

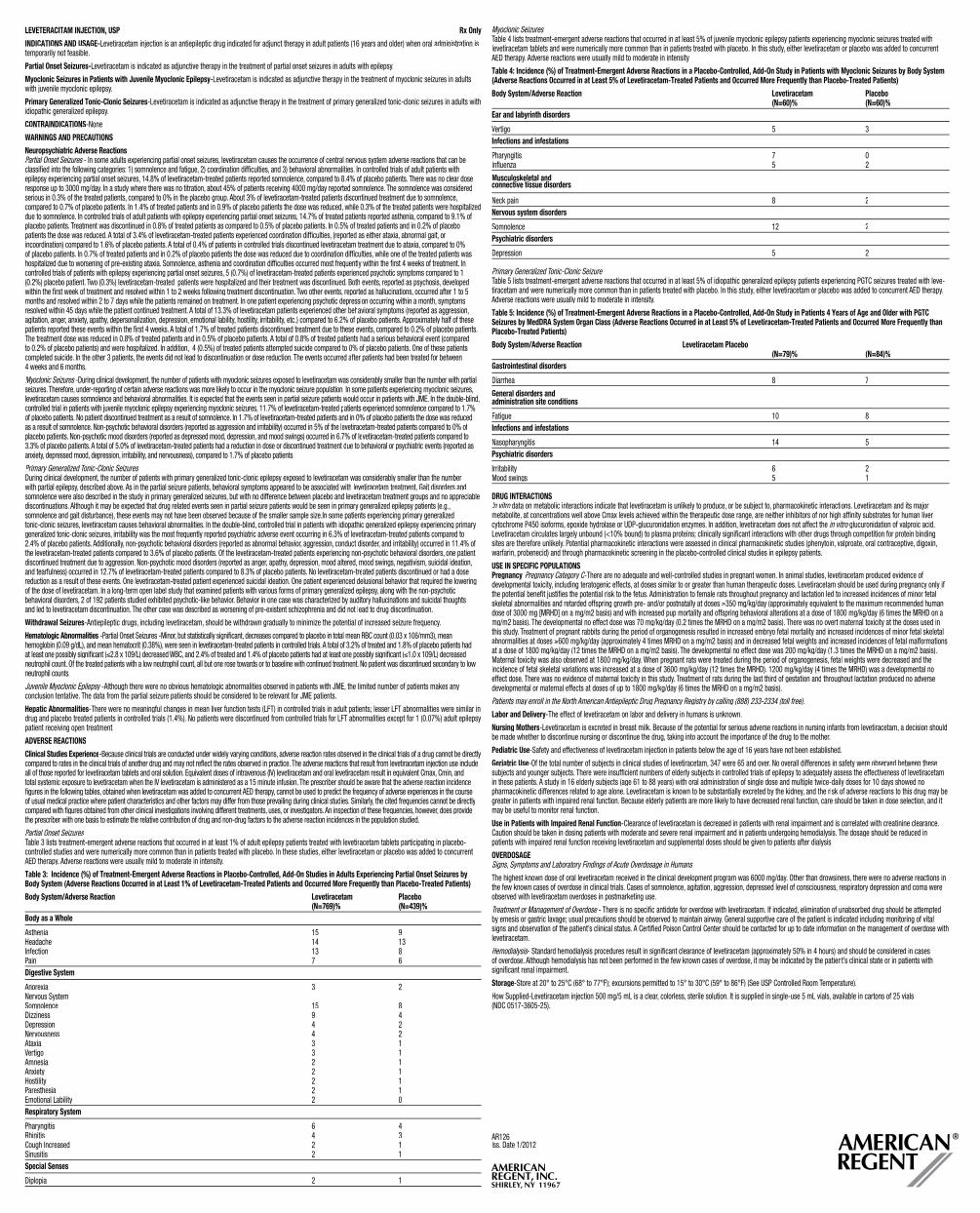
LEVETERACITAM INJECTION, USP Rx Only
INDICATIONS AND USAGE-Levetiracetam injection is an antiepileptic drug indicated for adjunct therapy in adult patients (16 years and older) when oral administration is temporarily not feasible.
Partial Onset Seizures-Levetiracetam is indicated as adjunctive therapy in the treatment of partial onset seizures in adults with epilepsy.
Myoclonic Seizures in Patients with Juvenile Myoclonic Epilepsy-Levetiracetam is indicated as adjunctive therapy in the treatment of myoclonic seizures in adults with juvenile myoclonic epilepsy.
Primary Generalized Tonic-Clonic Seizures-Levetiracetam is indicated as adjunctive therapy in the treatment of primary generalized tonic-clonic seizures in adults with idiopathic generalized epilepsy.
CONTRAINDICATIONS-None
WARNINGS AND PRECAUTIONS
Neuropsychiatric Adverse ReactionsPartial Onset Seizures - In some adults experiencing partial onset seizures, levetiracetam causes the occurrence of central nervous system adverse reactions that can be classified into the following categories: 1) somnolence and fatigue, 2) coordination difficulties, and 3) behavioral abnormalities. In controlled trials of adult patients with epilepsy experiencing partial onset seizures, 14.8% of levetiracetam-treated patients reported somnolence, compared to 8.4% of placebo patients. There was no clear dose response up to 3000 mg/day. In a study where there was no titration, about 45% of patients receiving 4000 mg/day reported somnolence. The somnolence was considered serious in 0.3% of the treated patients, compared to 0% in the placebo group. About 3% of levetiracetam-treated patients discontinued treatment due to somnolence, compared to 0.7% of placebo patients. In 1.4% of treated patients and in 0.9% of placebo patients the dose was reduced, while 0.3% of the treated patients were hospitalizeddue to somnolence. In controlled trials of adult patients with epilepsy experiencing partial onset seizures, 14.7% of treated patients reported asthenia, compared to 9.1% ofplacebo patients. Treatment was discontinued in 0.8% of treated patients as compared to 0.5% of placebo patients. In 0.5% of treated patients and in 0.2% of placebo patients the dose was reduced. A total of 3.4% of levetiracetam-treated patients experienced coordination difficulties, (reported as either ataxia, abnormal gait, or incoordination) compared to 1.6% of placebo patients. A total of 0.4% of patients in controlled trials discontinued levetiracetam treatment due to ataxia, compared to 0%of placebo patients. In 0.7% of treated patients and in 0.2% of placebo patients the dose was reduced due to coordination difficulties, while one of the treated patients was hospitalized due to worsening of pre-existing ataxia. Somnolence, asthenia and coordination difficulties occurred most frequently within the first 4 weeks of treatment. In controlled trials of patients with epilepsy experiencing partial onset seizures, 5 (0.7%) of levetiracetam-treated patients experienced psychotic symptoms compared to 1 (0.2%) placebo patient. Two (0.3%) levetiracetam-treated patients were hospitalized and their treatment was discontinued. Both events, reported as psychosis, developedwithin the first week of treatment and resolved within 1 to 2 weeks following treatment discontinuation. Two other events, reported as hallucinations, occurred after 1 to 5rrmonths and resolved within 2 to 7 days while the patients remained on treatment. In one patient experiencing psychotic depression occurring within a month, symptomsresolved within 45 days while the patient continued treatment. A total of 13.3% of levetiracetam patients experienced other behavioral symptoms (reported as aggression,agitation, anger, anxiety, apathy, depersonalization, depression, emotional lability, hostility, irritability, etc.) compared to 6.2% of placebo patients. Approximately half of these patients reported these events within the first 4 weeks. A total of 1.7% of treated patients discontinued treatment due to these events, compared to 0.2% of placebo patients.The treatment dose was reduced in 0.8% of treated patients and in 0.5% of placebo patients. A total of 0.8% of treated patients had a serious behavioral event (compared to 0.2% of placebo patients) and were hospitalized. In addition, 4 (0.5%) of treated patients attempted suicide compared to 0% of placebo patients. One of these patientscompleted suicide. In the other 3 patients, the events did not lead to discontinuation or dose reduction. The events occurred after patients had been treated for between 4 weeks and 6 months.
Myoclonic Seizures -During clinical development, the number of patients with myoclonic seizures exposed to levetiracetam was considerably smallers than the number with partial rseizures. Therefore, under-reporting of certain adverse reactions was more likely to occur in the myoclonic seizure population. In some patients experiencing myoclonic seizures,levetiracetam causes somnolence and behavioral abnormalities. It is expected that the events seen in partial seizure patients would occur in patients with JME. In the double-blind, controlled trial in patients with juvenile myoclonic epilepsy experiencing myoclonic seizures, 11.7% of levetiracetam-treated patients experienced somnolence compared to 1.7% of placebo patients. No patient discontinued treatment as a result of somnolence. In 1.7% of levetiracetam-treated patients and in 0% of placebo patients the dose was reduced as a result of somnolence. Non-psychotic behavioral disorders (reported as aggression and irritability) occurred in 5% of the levetiracetam-treated patients compared to 0% of placebo patients. Non-psychotic mood disorders (reported as depressed mood, depression, and mood swings) occurred in 6.7% of levetiracetam-treated patients compared to3.3% of placebo patients. A total of 5.0% of levetiracetam-treated patients had a reduction in dose or discontinued treatment due to behavioral or psychiatric events (reported as anxiety, depressed mood, depression, irritability, and nervousness), compared to 1.7% of placebo patients.
Primary Generalized Tonic-Clonic Seizures During clinical development, the number of patients with primary generalized tonic-clonic epilepsy exposed to levetiracetam was considerably smaller than the number with partial epilepsy, described above. As in the partial seizure patients, behavioral symptoms appeared to be associated with levetiracetam treatment. Gait disorders and somnolence were also described in the study in primary generalized seizures, but with no difference between placebo and levetiracetam treatment groups and no appreciable discontinuations. Although it may be expected that drug related events seen in partial seizure patients would be seen in primary generalized epilepsy patients (e.g., somnolence and gait disturbance), these events may not have been observed because of the smaller sample size.In some patients experiencing primary generalized tonic-clonic seizures, levetiracetam causes behavioral abnormalities. In the double-blind, controlled trial in patients with idiopathic generalized epilepsy experiencing primary generalized tonic-clonic seizures, irritability was the most frequently reported psychiatric adverse event occurring in 6.3% of levetiracetam-treated patients compared tof2.4% of placebo patients. Additionally, non-psychotic behavioral disorders (reported as abnormal behavior, aggression, conduct disorder, and irritability) occurred in 11.4% of the levetiracetam-treated patients compared to 3.6% of placebo patients. Of the levetiracetam-treated patients experiencing non-psychotic behavioral disorders, one patient discontinued treatment due to aggression. Non-psychotic mood disorders (reported as anger, apathy, depression, mood altered, mood swings, negativism, suicidal ideation, and tearfulness) occurred in 12.7% of levetiracetam-treated patients compared to 8.3% of placebo patients. No levetiracetam-treated patients discontinued or had a dose reduction as a result of these events. One levetiracetam-treated patient experienced suicidal ideation. One patient experienced delusional behavior that required the lowering of the dose of levetiracetam. In a long-term open label study that examined patients with various forms of primary generalized epilepsy, along with the non-psychotic behavioral disorders, 2 of 192 patients studied exhibited psychotic-like behavior. Behavior in one case was characterized by auditory hallucinations and suicidal thoughts and led to levetiracetam discontinuation. The other case was described as worsening of pre-existent schizophrenia and did not lead to drug discontinuation.
Withdrawal Seizures-Antiepileptic drugs, including levetiracetam, should be withdrawn gradually to minimize the potential of increased seizure frequency.
Hematologic Abnormalities -Partial Onset Seizures -Minor, but statistically significant, decreases compared to placebo in total mean RBC count (0.03 x 10s 6/mm3), mean hemoglobin (0.09 g/dL), and mean hematocrit (0.38%), were seen in levetiracetam-treated patients in controlled trials. A total of 3.2% of treated and 1.8% of placebo patients hadat least one possibly significant ( 2.8 x 109/L) decreased WBC, and 2.4% of treated and 1.4% of placebo patients had at least one possibly significant ( 1.0 x 109/L) decreased neutrophil count. Of the treated patients with a low neutrophil count, all but one rose towards or to baseline with continued treatment. No patient was discontinued secondary to low neutrophil counts.
Juvenile Myoclonic Epilepsy -Although there were no obvious hematologic abnormalities observed in patients with JME, the limited number of patients makes y any conclusion tentative. The data from the partial seizure patients should be considered to be relevant for JME patients.
Hepatic Abnormalities-There were no meaningful changes in mean liver function tests (LFT) in controlled trials in adult patients; lesser LFT abnormalities were similar in drug and placebo treated patients in controlled trials (1.4%). No patients were discontinued from controlled trials for LFT abnormalities except for 1 (0.07%) adult epilepsy patient receiving open treatment.
ADVERSE REACTIONS
Clinical Studies Experience-Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directlycompared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reactions that result from levetiracetam injection use include all of those reported for levetiracetam tablets and oral solution. Equivalent doses of intravenous (IV) levetiracetam and oral levetiracetam result in equivalent Cmax, Cmin, and total systemic exposure to levetiracetam when the IV levetiracetam is administered as a 15 minute infusion. The prescriber should be aware that the adverse reaction incidence figures in the following tables, obtained when levetiracetam was added to concurrent AED therapy, cannot be used to predict the frequency of adverse experiences in the course of usual medical practice where patient characteristics and other factors may differ from those prevailing during clinical studies. Similarly, the cited frequencies cannot be directlycompared with figures obtained from other clinical investigations involving different treatments, uses, or investigators. An inspection of these frequencies, however, does providethe prescriber with one basis to estimate the relative contribution of drug and non-drug factors to the adverse reaction incidences in the population studied.
Partial Onset Seizures Table 3 lists treatment-emergent adverse reactions that occurred in at least 1% of adult epilepsy patients treated with levetiracetam tablets participating in placebo-controlled studies and were numerically more common than in patients treated with placebo. In these studies, either levetiracetam or placebo was added to concurrent AED therapy. Adverse reactions were usually mild to moderate in intensity.
Table 3: Incidence (%) of Treatment-Emergent Adverse Reactions in Placebo-Controlled, Add-On Studies in Adults Experiencing Partial Onset Seizures by Body System (Adverse Reactions Occurred in at Least 1% of Levetiracetam-Treated Patients and Occurred More Frequently than Placebo-Treated Patients)
Body System/Adverse Reaction Levetiracetam Placebo (N=769)% (N=439)%
Body as a Whole
Asthenia 15 9 Headache 14 13 Infection 13 8 Pain 7 6Digestive System
Anorexia 3 2 Nervous System Somnolence 15 8 Dizziness 9 4 Depression 4 2 Nervousness 4 2 Ataxia 3 1 Vertigo 3 1 Amnesia 2 1 Anxiety 2 1 Hostility 2 1 Paresthesia 2 1 Emotional Lability 2 0Respiratory System
Pharyngitis 6 4 Rhinitis 4 3 Cough Increased 2 1 Sinusitis 2 1Special Senses
Diplopia 2 1
Myoclonic Seizures Table 4 lists treatment-emergent adverse reactions that occurred in at least 5% of juvenile myoclonic epilepsy patients experiencing myoclonic seizures treated with levetiracetam tablets and were numerically more common than in patients treated with placebo. In this study, either levetiracetam or placebo was added to concurrent AED therapy. Adverse reactions were usually mild to moderate in intensity.
Table 4: Incidence (%) of Treatment-Emergent Adverse Reactions in a Placebo-Controlled, Add-On Study in Patients with Myoclonic Seizures by Body System (Adverse Reactions Occurred in at Least 5% of Levetiracetam-Treated Patients and Occurred More Frequently than Placebo-Treated Patients)
Body System/Adverse Reaction Levetiracetam Placebo (N=60)% (N=60)%Ear and labyrinth disorders
Vertigo 5 3Infections and infestations
Pharyngitis 7 0 Influenza 5 2
Musculoskeletal and connective tissue disorders
Neck pain 8 2Nervous system disorders
Somnolence 12 2Psychiatric disorders
Depression 5 2
Primary Generalized Tonic-Clonic Seizure Table 5 lists treatment-emergent adverse reactions that occurred in at least 5% of idiopathic generalized epilepsy patients experiencing PGTC seizures treated with leve-tiracetam and were numerically more common than in patients treated with placebo. In this study, either levetiracetam or placebo was added to concurrent AED therapy. Adverse reactions were usually mild to moderate in intensity.
Table 5: Incidence (%) of Treatment-Emergent Adverse Reactions in a Placebo-Controlled, Add-On Study in Patients 4 Years of Age and Older with PGTC Seizures by MedDRA System Organ Class (Adverse Reactions Occurred in at Least 5% of Levetiracetam-Treated Patients and Occurred More Frequently than Placebo-Treated Patients)
Body System/Adverse Reaction Levetiracetam Placebo (N=79)% (N=84)%
Gastrointestinal disorders
Diarrhea 8 7
General disorders and administration site conditions
Fatigue 10 8Infections and infestations
Nasopharyngitis 14 5Psychiatric disorders
Irritability 6 2Mood swings 5 1
DRUG INTERACTIONS In vitro data on metabolic interactions indicate that levetiracetam is unlikely to produce, or be subject to, pharmacokinetic interactio ons. Levetiracetam and its major metabolite, at concentrations well above Cmax levels achieved within the therapeutic dose range, are neither inhibitors of nor high affinity substrates for human liver cytochrome P450 isoforms, epoxide hydrolase or UDP-glucuronidation enzymes. In addition, levetiracetam does not affect the in vitro glucuronidation of valproic acid. Levetiracetam circulates largely unbound (<10% bound) to plasma proteins; clinically significant interactions with other drugs through competition for protein binding sites are therefore unlikely. Potential pharmacokinetic interactions were assessed in clinical pharmacokinetic studies (phenytoin, valproate, oral contraceptive, digoxin, warfarin, probenecid) and through pharmacokinetic screening in the placebo-controlled clinical studies in epilepsy patients.
USE IN SPECIFIC POPULATIONS Pregnancy-Pregnancy Category C-There are no adequate and well-controlled studies in pregnant women. In animal studies, levetiracetam produced evidence of CCdevelopmental toxicity, including teratogenic effects, at doses similar to or greater than human therapeutic doses. Levetiracetam should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Administration to female rats throughout pregnancy and lactation led to increased incidences of minor fetal skeletal abnormalities and retarded offspring growth pre- and/or postnatally at doses 350 mg/kg/day (approximately equivalent to the maximum recommended human dose of 3000 mg [MRHD] on a mg/m2 basis) and with increased pup mortality and offspring behavioral alterations at a dose of 1800 mg/kg/day (6 times the MRHD on a mg/m2 basis). The developmental no effect dose was 70 mg/kg/day (0.2 times the MRHD on a mg/m2 basis). There was no overt maternal toxicity at the doses used in this study. Treatment of pregnant rabbits during the period of organogenesis resulted in increased embryo fetal mortality and increased incidences of minor fetal skeletal abnormalities at doses 600 mg/kg/day (approximately 4 times MRHD on a mg/m2 basis) and in decreased fetal weights and increased incidences of fetal malformations at a dose of 1800 mg/kg/day (12 times the MRHD on a mg/m2 basis). The developmental no effect dose was 200 mg/kg/day (1.3 times the MRHD on a mg/m2 basis). Maternal toxicity was also observed at 1800 mg/kg/day. When pregnant rats were treated during the period of organogenesis, fetal weights were decreased and the incidence of fetal skeletal variations was increased at a dose of 3600 mg/kg/day (12 times the MRHD). 1200 mg/kg/day (4 times the MRHD) was a developmental no effect dose. There was no evidence of maternal toxicity in this study. Treatment of rats during the last third of gestation and throughout lactation produced no adverse developmental or maternal effects at doses of up to 1800 mg/kg/day (6 times the MRHD on a mg/m2 basis).
Patients may enroll in the North American Antiepileptic Drug Pregnancy Registry by calling (888) 233-2334 (toll free).
Labor and Delivery-The effect of levetiracetam on labor and delivery in humans is unknown.
Nursing Mothers-Levetiracetam is excreted in breast milk. Because of the potential for serious adverse reactions in nursing infants from levetiracetam, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use-Safety and effectiveness of levetiracetam injection in patients below the age of 16 years have not been established.
Geriatric Use-Of the total number of subjects in clinical studies of levetiracetam, 347 were 65 and over. No overall differences in safety were observed between these subjects and younger subjects. There were insufficient numbers of elderly subjects in controlled trials of epilepsy to adequately assess the effectiveness of levetiracetam in these patients. A study in 16 elderly subjects (age 61 to 88 years) with oral administration of single dose and multiple twice-daily doses for 10 days showed no pharmacokinetic differences related to age alone. Levetiracetam is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Use in Patients with Impaired Renal Function-Clearance of levetiracetam is decreased in patients with renal impairment and is correlated with creatinine clearance.Caution should be taken in dosing patients with moderate and severe renal impairment and in patients undergoing hemodialysis. The dosage should be reduced in patients with impaired renal function receiving levetiracetam and supplemental doses should be given to patients after dialysis.
OVERDOSAGESigns, Symptoms and Laboratory Findings of Acute Overdosage in Humans
The highest known dose of oral levetiracetam received in the clinical development program was 6000 mg/day. Other than drowsiness, there were no adverse reactions inthe few known cases of overdose in clinical trials. Cases of somnolence, agitation, aggression, depressed level of consciousness, respiratory depression and coma were observed with levetiracetam overdoses in postmarketing use.
Treatment or Management of Overdose - There is no specific antidote for overdose with levetiracetam. If indicated, elimination of unabsorbed drug should be attempte ed by emesis or gastric lavage; usual precautions should be observed to maintain airway. General supportive care of the patient is indicated including monitoring of vital signs and observation of the patient’s clinical status. A Certified Poison Control Center should be contacted for up to date information on the management of overdose with levetiracetam.
Hemodialysis- Standard hemodialysis procedures result in significant clearance of levetiracetam (approximately 50% in 4 hours) and should bess considered in cases of overdose. Although hemodialysis has not been performed in the few known cases of overdose, it may be indicated by the patient’s clinical state or in patients with significant renal impairment.
Storage-Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) (See USP Controlled Room Temperature).
How Supplied-Levetiracetam injection 500 mg/5 mL is a clear, colorless, sterile solution. It is supplied in single-use 5 mL vials, available in cartons of 25 vials (NDC 0517-3605-25).
AR126 Iss. Date 1/2012
MCPPN2204.indd 1 3/15/12 11:06 PM

Las Vegas—In 2011, the FDA warnedclinicians against using the fibrate gem-fibrozil with simvastatin because of anincreased risk for cardiomyopathy andrhabdomyolysis in patients taking thecombination therapy. Some health sys-tems have responded by issuing a univer-sal ban on all fibrate–statin combinationtreatment. Others have incorporated a hard stop into their clinical decision sup-port systems when these two drugs areco-prescribed.
Regardless of the approach, expertssay that safety protocols to monitorlipids and replace gemfibrozil with anappropriate alternative or switch toanother statin must be part of the mixto guard against adverse drug reactions.Several efforts to accomplish thosemedication management goals were inevidence at the American Society of Health-System Pharmacists (ASHP)Midyear Clinical Meeting.
An Algorithm-Based Approach
In response to the gemfibrozil–simva-statin contraindication, the Pharmacy and Therapeutics Committee at theRalph H. Johnson Veterans Affairs Med-ical Center (RHJ VAMC), in Charleston,S.C., has developed a treatment algo-rithm based on patients’ low-density lipoprotein (LDL) cholesterol and tri-glyceride levels. The algorithm calls forpatients whose LDL is “at goal” (<130mg/dL for primary prevention patientsand <100 mg/dL for secondary preven-tion patients) and whose triglyceridesare less than 150 mg/dL to remain onsimvastatin but be taken off gemfibrozilwith no alternative therapy. Fish oil sup-plementation is given as an alternative topatients with LDL at goal and triglycer-ides of 150-249 mg/dL. Niacin is given topatients with LDL at goal and triglycer-ides of 250-499 mg/dL. Patients whoseLDL is not at goal receive an increaseddose of simvastatin (20 or 40 mg), andthose with a history of pancreatitis ortriglycerides of 500 mg/dL or greaterare kept on gemfibrozil but convertedto rosuvastatin (Crestor, AstraZeneca)
or pravastatin (Pravachol, Bristol-Myers Squibb) at an equivalent or higher dose, as indicated by their LDL level. (Pravas-tatin and rosuvastatin are less likely to interact with gemfibrozil.)
“We wanted to outline [the algo-rithm] for the physicians to make it as easy as possible so they would have to make as few benchmark decisions as possible,” said Molly Haselden, PharmD. In doing so, patients “wouldn’t get lost under the radar or get an inap-propriate combination.”
The protocol also stresses individu-alized care, added Thomas J. Worrall, PharmD, BCPS, an ambulatory care clini-cal pharmacy specialist at RHJ VAMC. The physician and patient work together to come up with the best plan based on history and risk factors, he said. “Anytime a medication is changed for lipids or cho-lesterol, we always monitor it and make additional changes if needed.”
A study of the new algorithm’s effect on a subset of patients, presented by Dr. Haselden and her colleagues at the ASHP meeting, showed a statistically but not clinically significant change in pre- and post-intervention triglycerides (107.5 vs. 159.5 mg/dL; P<0.001) and LDL (81.2 vs. 75.0 mg/dL; P=0.01) among 81 patients whose LDL and triglyceride levels were at goal (150 mg/dL or lower) when they were removed from gemfibrozil in response to the FDA contraindication. The increase in triglycerides “was not clinically significant, as additional thera-py would not be added for a triglyceride level of 159 mg/dL,” said Dr. Worrall.
An additional eight patients whose LDL levels were not at goal at baseline had a significant increase in triglycerides post-intervention (107.6 vs. 156.1 mg/dL; P=0.01); mean LDL did not change sig-nificantly (119.6 vs. 119.1 mg/dL; P=0.82).
Mean total cholesterol, high-density lipoprotein (HDL) and the ratio of aspar-tate aminotransferase to alanine amino-transferase did not change across the total group of 89 patients. Analyses of patients receiving alternative therapies such as fish oil or niacin, or different
statins with gemfibrozil, are under way.Another study presented at the meet-
ing suggested that fish oil might offer an effective alternative to gemfibrozil. In a retrospective chart review of 248 patients on background simvastatin ther-apy, researchers identified 39 patients who were converted to fish oil supple-mentation from gemfibrozil during June to December 2011. Triglycerides and LDL decreased (12.5% and 16.7%, respec-tively) among these patients (mean age, 66.2 years), reported Christine Huber, PharmD, BCPS, a clinical pharmacy spe-cialist in primary care, and Haley J. Mor-rill, PharmD, a resident at Providence VA Medical Center, in Providence, R.I.
Although the findings were not sig-nificant, “it was surprising for us because normally you would expect the LDL to go up,” Dr. Huber said. All patients in the study received the over-the-counter fish oil supplied by the VA pharmacy.
Most of the patients—27 of 39—were prescribed the recommended daily dose of 4,000 mg. “I was surprised that the primary care physicians had selected a recommended dose,” Dr. Huber said, adding that she expected the physicians would start with lower doses. Doses ranged from 1,000 to 4,000 mg. A sub-analysis revealed that patients taking 4,000 mg daily achieved better triglyc-eride control, she said.
For Fish Oil, Rx Is Best?
Robert DiDomenico, PharmD, a car-diovascular clinical pharmacist at the University of Illinois at Chicago College of Pharmacy, noted in an interview that prescription fish oil supplements (Lova-za omega-3-acid ethyl esters, Reliant Pharmaceuticals) may be preferable to over-the-counter products as an alterna-tive to gemfibrozil because they are regu-lated by the FDA. “If you’re identifying a patient who clearly has hypertriglyceri-demia or low HDL and you are purposely trying to raise HDL with one of these products, I might be more inclined to use a brand-name product,” he said. “The alternative is to use the over-the-coun-
ter product and follow the patient closely, and ifyou don’t see tresponse you switch to the b
Dr. DiDomethat the current emphasis on taking patients off gemfibrozil and pro-viding an alternative may be “the wrong side of the coin.” The focus may instead need to shift toward replacing simvas-tatin with another statin, he noted. Sim-vastatin’s availability as a generic has ledto its widespread use, he said, but “are wefocusing on the right drug to switch out?”
He said a good candidate for such a switch is atorvastatin calcium (Lipitor,Pfizer). In addition to being a cost saver—the statin recently became available as a generic—it is slightly more potent than simvastatin and “doesn’t have as many of the hard-and-fast contraindications thatsimvastatin has.”
C. Michael White, PharmD, a profes-sor and the chair of the Department of Pharmacy Practice at the University of Connecticut, in Storrs, and the author of numerous papers on statins, has his own prescription for managing patients onthe lipid-lowering medications—avoiding rash cessations of therapy. “A protocolthat just takes someone with a high risk of pancreatitis due to high triglycerides off gemfibrozil would not be smart,” Dr. White said. Better therapeutic options, he noted, include keeping the patient on gemfibrozil but switching their statin to pravastatin or rosuvastatin, given the latter drug’s lower risk for interacting with gemfibrozil, or keeping the patient on simvastatin but using high-dose fish oil, niacin or fenofibrate (Tricor, Abbott Laboratories) instead of gemfibrozil.
—Susan Birk
Drs. Haselden, Worrall, Huber and Whitereported that they had no relevant fi nancial
confl icts of interest. Dr. DiDomenicoreported that he has served on Roche’s
advisory board.
within 30 days of discharge with thosereadmitted after 30 days or not at all.
Presenting the results at the ASHPmeeting, Blair Kaplan, PharmD, BCPS,and Clare Bergman, PharmD, BCPS,inpatient clinical pharmacists at the VAmedical center, reported that earlier andmore frequent readmissions were morecommon among patients who receivedoral diuretic therapy for less than 24hours before discharge; who were not
prescribed an ACEI or angiotensin-receptor blocker and a β-blocker at dis-charge; and who were not compliant with medications or follow-up care.
Although the investigators noted that the rate of 30-day readmissions at the medical center was low, they acknowl-edged that the results “suggest that there is room for improvement.” Dr. Kaplan told Pharmacy Practice News,“We found that none of the patients who were readmitted during the study period of six months [had been] seen in the newly initiated heart failure
pharmacist clinic. This gives us hope that over time, more patients will have the opportunity to receive medication education and optimization to prevent future hospital readmissions.”
Rural Health Care Approach
These programs can be incorporated even at small rural hospitals, according to another study presented at the ASHP meeting. In the study, conducted at East-ern Maine Medical Center (EMMC), in Bangor, Maine, pharmacists played an integral role within an interdisciplinary
team that educated patients with HF and enhanced continuity of care, result-ing in decreased readmission rates andimproved reimbursement rates.
To be compliant with CMS reimburse-ment requirements, EMMC, which has six affiliated primary care clinics,established a Heart Failure ReadmissionReduction Team, consisting of physi-cians, pharmacists, nurses and admin-istrators from inpatient and outpatientsettings. The Pharmacy Department was responsible for educating patients
Fibrate–Statin Label Changes Call for New Protocols
HF READMISSIONScontinued from page 8
• see HF READMISSIONS, page 22
f the
want,brand.”enico added
Pharmacy Practice News • January 2013
Cardiology
Clinical 11

Chicago—Pharmacy leaders shouldplan ahead to ready their departmentsfor an audit or survey by any of the sev-eral state and federal agencies that couldcome knocking on the door, recom-mended compliance experts at the 2012leadership conference of the American Society of Health-System Pharmacists.
“Being familiar with these organiza-tions and understanding what your roleis in the different types of audits and sur-veys is a requirement for pharmacy lead-ership,” said Patricia C. Kienle, MPA, BSPharm, FASHP, the director of accredita-tion and medication safety for CardinalHealth Pharmacy Solutions, in Laflin, Pa.
Karla M. Miller, PharmD, BCPP, theassistant vice president of pharmacy services and clinical therapeutics for the Hospital Corporation of America Clini-cal Services Group, in Nashville, Tenn,made a similar entreaty at the meeting.“At the heart of all of these organiza-tions is good patient care and protectionof patients,” but each has its own focusand ways of operating, Dr. Miller said ina breakout session on compliance sur-vival strategies. “Be sure you know howto respond to these situations, even theones that are out of your control.”
In addition to surveys by the relative-ly familiar accreditation groups and theCenters for Medicare & Medicaid Ser-vices (CMS), pharmacy leaders couldconceivably find themselves dealing withinvestigations by the Office of InspectorGeneral, the Drug Enforcement Adminis-tration (DEA) or any of the state licensing boards for pharmacy and medicine.
Dr. Miller said that on-site DEA inspec-tions are on the rise. “Make sure execu-tive leadership is aware of [the DEArepresentatives’] presence, get them a private room and a direct contact to
work with” and be prepared to provide the biannual inventory report, inventory records, theft and loss reports, policies for medication diversion prevention, substance abuse in the workplace and controlled substance monitoring, as well as other required documents, she said.
“If you can get those [reports] in front of the DEA, you don’t have much to wor-ry about. It’s when you don’t have these quickly in an orderly manner that they’re going to ask questions,” she said.
CMS has its own areas of recent focus, including its newly implemented reim-bursement penalties for excessive hos-pital readmissions (Pharmacy Practice ((News, December, page 1). Ms. Kienle advised pharmacy leaders to prepare for CMS scrutiny by taking a deeper, closer look at the agency’s Conditions of Par-ticipation (CoP) (http://www.cms.gov/
Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_a_hospi-tals.pdf ). For the three major health care accrediting groups in the United States—the Joint Commission, the American Osteopathic Association (AOA) and Det Norske Veritas (DNV)—the foundation of their standards is the CoP.
Organizations also need to familiarize themselves with the CoP because “CMS is taking a more global approach to what happens in hospitals,” including looking more closely at how the CoP feeds in to the accreditation process, Ms. Kienle said in an interview. Medication-related sections affecting pharmacists are spread throughout the document, not just in the 17 CoP for Pharmaceutical Services. “It’s up to you to know where they are,” added Ms. Kienle, who has served on the Phar-macotherapy Specialty Council of the
Hospital Professional and Technical Advi-sory Committee of the Joint Commission.
“The first half [of the CoP] is almost all about restraints. The second half is all about the operations of the hospital,and the pharmaceutical services piece is key there,” Ms. Kienle said. “There are other things that directly affect our medication perspective, particularly onthe acute care side, that are in other areas [of the CoP] as well. So I would suggest you look at that link and make sure youhave it available to you.”
She added, “Our responsibility in our enterprise is a bigger net than what wedo in the pharmacy. We need to get that message out loud and clear … andsometimes we need to use some of thesefederal standards as support for what wewant to do in our organizations.”
Storing Medications Is Potential Trouble Spot
Standards in the CoP for storage, for example, have changed from requiring that all drugs be locked to requiring thatall drugs and biologics be secured and locked when necessary. That change has“put a big onus on the hospital to define what they think is secure,” Ms. Kienlesaid. “So these are things that should bein your policies. … Do you have a policy that says who has access to medications in your organization? And it needs to beway bigger than pharmacy and nursing because there are lots of other peoplewho have access to specific carved-out areas of meds.”
Ms. Kienle noted that 5% of hospitals receive a validation survey by CMS fol-lowing an accreditation survey. “What they want to do from a validation stand-point is to make sure those accrediting organizations are complying with the
Experts Offer Survey, Audit Survival Tips
Tips for Boosting Compounding Safety
Adhering to a few core strategies can go a long way toward improving the safety of your hospital’s
partnerships with outside sterile compounders and inthe process avoid compliance issues during site sur-veys, according to Patricia C. Kienle, MPA, BS Pharm, FASHP, the director of accreditation and medication safety for Cardinal Health Pharmacy Solutions, in Laf-lin, Pa.. She said that the following approaches couldbe particularly useful:• Ensure that any source used for the provision of
medications meets your health system’s standards.“This isn’t limited to compounding pharmacies; any purchases outside of your known, acceptable ven-dors need to be vetted.”
• Review the contract you have with any compound-ing pharmacy (both sterile and nonsterile).
• Read the ASHP Guidelines on Outsourcing Ster-ile Compounding Services (www.ashp.org/DocLibrary/Bestpractices/MgmtGdlOutsourcing-SterileComp.aspx).
• Assess your internal compliance with United StatesPharmacopeia (USP) Chapter <797>. Accreditation
organizations often ask for the most recent gap anal-ysis if a facility is not USP <797> compliant. Completea new gap analysis if needed (both for nonhazardous as well as hazardous sterile compounding), and share the results with hospital leadership.As with many partnerships or alliances, it is crucial
to review the documentation for any compoundingpharmacy, Ms. Kienle noted. The following records can be particularly revealing and should be on your quality control checklist:• Pharmacy license in the state where the outsourced
pharmacy is located.• DEA registration, if controlled substances are
provided.• Registration with the FDA, as applicable and/
or accreditation by the Pharmacy Compounding Accreditation Board for sterile compounding (does not apply to radiopharmaceuticals).
• Wholesaler or distributor license in the state wherethe outsourced pharmacy is located, if required.
• If the outsourced pharmacy is located in another state, out-of-state wholesaler or distributor license,
if required by your state.• If the outsourced pharmacy is located in another
state, any special license required by your state (e.g., controlled substances, sterile compounding), as applicable.
• Licensure of pharmacists employed by the out-sourced pharmacy.
• Registration/certification of pharmacy technicians employed by the outsourced pharmacy, if applicable.
• Written training program that meets USP <797>requirements and any state requirements, if applicable.
• Summary of results of personnel competence.• Quality monitoring, including sterility testing of
each batch and pyrogen testing if nonsterileingredients are used.
• Sources of ingredients.• Product recall procedures and records.• Proof of liability insurance.• Records of regulatory inspections.
—S.B.
Figure. Medication use system.
b
Planning
Administer
Monitor
Select Store
Dispense
Order
Evaluation
Pharmacy Practice News • January 2013
Compliance
12 Operations & Management

federal standards,” she said. For thatreason, “they don’t survey against [theJoint Commission] or AOA or DNV stan-dards, they survey against the CoP.” Thevast majority of accreditation standardsoverlap with those of CMS, she said,“but there are some subtle differencesor different approaches,” and pharma-cists need to know what those are.
According to Ms. Kienle, hospital andhealth-system pharmacists can expectheightened scrutiny in the wake of therecent fungal meningitis outbreak (relatedarticle, page 1). “You’ve got to believe
when these folks are coming in to survey now and in the near future that this com-pounding issue is going to come up loud and clear,” she said. “The responsibility from a federal perspective is [to ensure] that patients are safe, as it should be. With the atrocious situation that’s occurring with compounding, I think we’re going to see more and more questions in that area.”
The high level of public trust phar-
macists have enjoyed for decades has been tarnished, at least temporarily, by a disaster “that never should have occurred,” she said. In Gallup pub-lic opinion surveys, pharmacists have ranked among the top three most trust-ed groups of professionals for the past nine years. “I’m betting we’re not going to be there this year,” she said.
To prepare for survey questions focused
on compounding (sidebar), pharmacists should ensure that the need for a com-pounded preparation is clinically appro-priate, she advised. “Some compoundshave been used based on convenience or the lack of standardization of concentra-tions in some organizations. Now is the time to assess the appropriateness and evidence-based practices. Organizations that have been unable to standardize[based on physician preference] can nowapproach this issue with a different level of urgency.”
—Susan Birk
EX-AP-0020-201111EX-AP-0039-201201
Pharmacy Practice News • January 2013
Compliance
Operations & Management 13

demonstration of how even in these[challenging economic] times, new pro-grams like this can be initiated to helpimprove patient care at the hospital.”
Study Limitations
Christopher J. Edwards, PharmD,BCPS, a clinical staff pharmacist inemergency medicine at the University of Arizona Medical Center–Univer-sity Campus, in Tucson, pointed to
some shortcomings in the FSMH study. “Reallocation of inpatient staff to the [ED] may not be applicable to all hos-pitals,” Dr. Edwards said. “Pharmacists working in an [ED] should ideally have specialized training.”
Additionally, “I would have liked to see a breakdown of hard versus soft money. They didn’t differenti-ate. Soft money is not as impressive as hard when trying to persuade administrators.”
However, Dr. Edwards said he con-siders the study “interesting because it describes a smaller community hospi-tal—17 beds in the emergency depart-ment. Most of the literature comesfrom large teaching hospitals.”
He also gave kudos to the research-ers for their thorough approach to documentation. “The paper stresses the importance of documentation to present to the administration to jus-tify the cost,” he said. “Documenta-tion, documentation, documentation. Getting your foot in the door is the hardest part.” He added, “You have to present and make a case. The tighter the budget, the more difficult it will be [to convince hospital administrators].”
For FSMH, there are indications that those budget pressures may be lifting, in part due to more recent successes with their ED pharmacy initiative. “In the article, we mentioned approval for 4.5 FTE technicians and these posi-tions are currently in the process of being filled,” Dr. Nana said. “Overall, the hours have been expanded to 20 hours of coverage a day, seven days a week from our initial six hours of coverage, five days a week. In addition, due to the positive results seen, a sis-ter hospital, Franciscan St. Margaret Health–Dyer, has also initiated an ED pharmacy program at their site.”
—George Ochoa
Drs. Nana and Edwards reported no relevant fi nancial confl icts of interest.
PHARM COSTcontinued from page 7
‘Reallocation of
inpatient staff to
the [ED] may not
be applicable to all
hospitals; pharmacists
working in an [ED]
should ideally have
specialized training.’
—Christopher J. Edwards, PharmD, BCPS
Please see brief summary of Prescribing Information on back page.
For more information, visit www.EXPAREL.com
EXPAREL is the only single-doselocal analgesic that…• Provides up to 72 hours1* of analgesia with• Reduced opioid requirements1†
• Without the need for catheters or pumps
EXPAREL is a liposome formulation of bupivacaine indicated for administration into the surgical site to produce postsurgical analgesia.Important Safety Information:EXPAREL is contraindicated in obstetrical paracervical block anesthesia. EXPAREL has not been studied for use in patientsyounger than 18 years of age. Non-bupivacaine-based local anesthetics, including lidocaine, may cause an immediate releaseof bupivacaine from EXPAREL if administered together locally. The administration of EXPAREL may follow the administrationof lidocaine after a delay of 20 minutes or more. Other formulations of bupivacaine should not be administered within 96hours following administration of EXPAREL. Monitoring of cardiovascular and neurological status, as well as vital signs shouldbe performed during and after injection of EXPAREL as with other local anesthetic products. Because amide-type localanesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepaticdisease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at agreater risk of developing toxic plasma concentrations. In clinical trials, the most common adverse reactions (incidence≥10%) following EXPAREL administration were nausea, constipation, and vomiting. *Pivotal studies have demonstrated the safety and efficacy of EXPAREL in patients undergoing bunionectomy or hemorrhoidectomy procedures; additional studies are underway to further demonstratethe safety and efficacy in other procedures.†The clinical benefit of the attendant decrease in opioid consumption was not demonstrated.
Reference: 1. Gorfine SR, Onel E, Patou G, et al. Bupivacaine Extended-Release Liposome Injection for Prolonged Postsurgical Analgesia in Patients Undergoing Hemorrhoidectomy: A Multicenter,Randomized, Double-blind, Placebo-controlled Trial. Dis Colon Rectum. Dec 2011;54(12):1552-1559.
One dose provides postsurgical pain control for up to 72 hours *
Pharmacy Practice News • January 2013
Critical Care
14 Clinical

Core measures (CMs) are a set of evidence-based quality indicators
created by the Centers for Medicare &Medicaid Services (CMS) and the JointCommission. They have been shown toreduce the risk for complications, pre-vent recurrences, and otherwise promoteoptimal treatment of patients presenting with specific conditions. Failure to com-ply with the CMs may result in decreasedreimbursement. At Pennsylvania Hospi-tal, we saw an opportunity to leverage a unit-based clinical pharmacist model tohelp achieve and sustain CM compliancegoals. Pharmacist involvement enabledthe hospital to improve compliance in allthe medication-related CMs that weretargeted, with 100% compliance in a majority of the measures.
Implementation Plan
The Department of Pharmacy Servicessaw an opportunity to use its establishedunit-based clinical pharmacist model tohelp achieve and sustain CM compliancegoals. Together with the hospital’s Quali-ty Management Department, they identi-
fied 9 medication-related CMs as oppor-tunities for pharmacist involvement (Table 1). In March 2011, the hospital’s Pharmacy and Therapeutics Committee approved the new pharmacy-initiated program. Before the program’s launch in April 2011, an education plan was devel-oped for pharmacists and house staff. Pharmacists were educated on the areas covered in the CM initiative—acute myocardial infarction (AMI), heart fail-ure (HF), and pneumonia (PN)—and were given an introduction to CMs. House staff were educated about CMs and the potential of pharmacy to help the hospital achieve compliance goals. In November 2011, when stroke was added to the hospital’s CM dashboard, education related to stroke therapeutics was provided to the house staff.
Pharmacy realigned its work-flow model to accommodate the new responsibilities. Unit-based clinical pharmacists identified patients with an “admitting diagnosis” of AMI, HF, PN, or stroke every weekday via an emailed list from clinical data ana-lysts. They also screened patients for CM diagnoses during daily patient care rounds. Pharmacists assessed medi-cation-related CM compliance using patient-specific worksheets created by the pharmacy clinical specialists in internal medicine, infectious disease, and anticoagulation (Figure). After the unit-based clinical pharmacists evalu-ated the patients and discussed them with the multidisciplinary team, they determined which of 3 actions were required, and they proceeded accord-ingly (Table 2).
Clinical pharmacists maintained patient review worksheets to facilitate communication between covering phar-macists, and after discharge the work-sheets served as monitoring tools to
assess monthly pharmacy interventions and trends.
In December 2011, after 8 months of this paper process, the Pharmacy Department implemented a computer-ized pharmacy clinical surveillance pro-gram, Pharmacy One Source Sentri7. This program interfaced with the hos-pital’s electronic charting system and computerized provider order entry sys-tem to extract relevant clinical patient data related to CM areas. With this data, the Pharmacy Department built and generated rules-based report lists. These lists identified patients with spe-cific admitting diagnoses who were not ordered an appropriate medication (eg, “AMI diagnosis without appropriate meds”). The pharmacy created similar lists for each CM set.
Electronic clinical surveillance streamlined the screening process and created a more efficient workflow for the pharmacists. The interface with the hospital’s electronic medication admin-istration record system provided faster real-time patient identification. Phar-macists also documented interventions directly into the surveillance program and added notes to communicate with other pharmacists in the department.
Monitoring of Process
The hospital’s quality management team monitored and reported CM com-pliance monthly at a Core Measures
Task Force meeting. The Pharmacy Department also monitored and report-ed the following data at each meeting:• Number of patients reviewed by the
pharmacists• Number of documentations made
in the patient medical record by pharmacists
• Number of recommendations to the provider
• Provider acceptance rate of recom-mendations made by pharmacistsDuring the first 17 months of the
pharmacy-based initiative, pharma-cists reviewed 2,742 patients, made 218 documentations in patient charts, and made 224 recommendations, with an acceptance rate of 96%. With the addi-tion of pharmacy involvement, the hos-pital was able to improve compliance in the 9 targeted medication-related CMs, with 100% compliance in a majority of the measures.
Keys to Success
Due to the success of the pharmacy CM program, we believe that the same type of service could be replicated at other organizations. The group effortsof the Department of Pharmacy, the Department of Quality and Patient Safety, the performance improvementleadership, and clinical data analysts provided an optimal interdisciplin-ary platform for success. Institutions
Pharmacists Help With CMS Core Measure Adherence Lindsay I. Varga, PharmD, BCPSClinical Pharmacy Specialist in Internal Medicine
Elizabeth Marino Sabo, PharmD,BCPSClinical Pharmacy Specialist in InfectiousDisease
Jacqueline M. von Vital, PharmD, BCPSClinical Pharmacy Specialist in Anticoagulation
Suzanne Y. Brown, MS, RPhDirector of Pharmacy Services
Pennsylvania HospitalPhiladelphia, Pennsylvania
Table 1. Targeted Medication-Related CoreMeasures (as of August 2012)
Measure Set Measure ID No. Measure Short Name
Acute myocardialinfarction (AMI)
AMI-2 Aspirin prescribed at discharge
AMI-3 ACEI or ARB for LVSD
AMI-5 β-Blocker prescribed at discharge
AMI-10 Statin prescribed at discharge
Heart failure (HF) HF-3 ACEI or ARB for LVSD
Pneumonia (PN) PN-6 Initial antibiotic selection
Stroke (STK) STK-1 Venous thromboembolism prophylaxis
STK-2 Discharged on antithrombotic therapy
STK-6 Discharged on statin
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; LVSD, left ventricular systolic dysfunction
Based on reference 1.
• see COMPLIANCE, page 16
Figure. Portion of a patient-specific core measure worksheet for acute myocardial infarction.
Pharmacy Practice News • January 2013
Practice Pearl
Operations & Management 15

should consider several factors to opti-mally replicate the program.
Departmental Partnerships
An integral aspect of this project is the relationship of the Pharmacy Depart-ment with the Department of Quality and Patient Safety and performance improve-ment leadership. Working together allows us to share ideas and optimally identify patients who are appropriate
for CM assessment. The Department of Quality and Patient Safety reviews com-pliance rates on a monthly basis and shares patient cases with the Pharmacy Department.
Staff Education
Education on pathophysiology and therapeutics of disease states, as well as on the background of CMs, is vital in preparing unit-based clinical phar-macists to become contributing mem-bers of the health care team in assess-ing CM compliance.
Workflow and AccountabilityThis project was integrated into our
department’s operational structure,
which includes unit-based clinical phar-macists who are deployed on the floors and closely interact with the patients, nurses, dieticians, and providers on a daily basis. The unit-based clinical phar-macists are held accountable for com-pleting the CM checklists and commu-nicating information to the rest of the health care team.
Standardized Clinical Surveillance Process
Whether a paper or electronic process is used, the establishment of a consis-tent method for identifying and evaluat-ing patients is integral to success.
InterdisciplinaryPatient Care Rounds
The unit-based clinical pharmacist is a member of an interdisciplinary team that meets daily during patient care rounds. During these rounds, valuable information about the patient is pre-sented that allows the team to screen patients using the CM checklists and identify those who would benefit from pharmacy intervention. Without this coordinated effort among the disci-plines, the screening process would be much more challenging.
Ongoing Monitoring And Feedback
Compliance rates and intervention data are gathered and reviewed each month at a Core Measures Task Force meeting. This data also is shared with the unit-based clinical pharmacists and house staff. The pharmacy CM program is dynamic, and pharmacists’ suggestions to improve the program are encouraged and integrated into the program.
Conclusion
Based on our experience at Pennsyl-vania Hospital, we feel that a unit-based clinical pharmacist model can be lever-aged to support a hospital in achiev-ing CM compliance. Success in such a program is best achieved with interdis-ciplinary partnership, staff education, and standardization, as well as ongoing monitoring and feedback.
References1. Centers for Disease Control & Prevention and
The Joint Commission. Specifications Manual for National Hospital Inpatient Quality Measures. Version 4.0. January 2012.
Table 2. Actions Required After Compliance Assessment
Compliance Level Action Required
Patient compliant with all medication CMs No action needed
Patient noncompliant with medication CMsdue to contraindication
Document contraindication inpermanent medical record
Patient noncompliant with medication CMsand no contraindication identified
Communicate with providerand recommend compliance
CM, core measure
COMPLIANCEcontinued from page 15
Register for free@ www.specialtypharmacycontinuum.com
Get the latest news
delivered directly to
your computer and PDA.
The interactive format
has embedded Web site
links that give you instant
access to additional
information as well as
unique searching features
and printing capabilities.
Each installment contains
brief summaries of the
most important articles
from the current month’s
issue, and breaking
news ahead of print.
... to receive the monthly e-newsletter from
at www.specialtypharmacycontinuum.com
Pharmacy Practice News • January 2013
Practice Pearl
16 Operations & Management

According to Carlos Marin, RPh, leadpharmacist in the IV room of the Oncol-ogy Department at Overlook, the initia-tive began when the Finance Depart-ment approached the pharmacy andasked it to track discarded infliximab(Remicade, Janssen). “Every time, wewere able to capture payment for a cer-tain percentage of the waste if we docu-mented it,” he explained.
In a pilot study, Mr. Marin and hiscolleagues identified 11 drugs stocked insingle-dose vials at the hospital’s outpa-tient infusion center and documented any amounts that went unused; they hadthe same success that they’d seen withwasted infliximab.
The targeted drugs are mainly mono-clonal antibodies and chemotherapeutic agents, and the pharmacists responsiblefor order entry in specific areas weretrained on how to document wastedportions of every vial. To make the pro-cess easy and fast, the pharmacy’s order-entry system prompts users to recordthe amount of unused portions of all of the relevant drugs. The system won’t letpharmacists proceed until they supply the requested information, and the extra steps add only a few seconds to the pro-cess, according to Mr. Marin.
The results were eye-opening: In 2011,reimbursements for drug waste for the 11drugs totaled nearly $508,000. Oxalipla-tin and bevacizumab (Avastin, Genen-tech) accounted for 70% of that total. From January to August 2012, the hos-pital recouped another $346,515. Thatamount included waste reimbursementfor several drugs administered mostly inthe inpatient setting, and accounted forabout $8,000 over a two-month period.
“You won’t get full payment for all of the unused portion of a vial, but you willget a percentage of these very expensivedrugs and realize income that otherwisewould not have been there,” Mr. Marinsaid. For example, the hospital submit-ted $491,000 worth of claims to CMSfor wasted bevacizumab, but received$191,724 in reimbursement.
Since the pilot study, the list of drugsscrutinized for waste reimbursement hasexpanded to more than 30 agents. “Wetry to capture those very expensive drugs[for which] reimbursement is very ben-eficial for the hospital, and it’s working out very well,” Mr. Marin said.
Targeting PancreaticEnzyme Therapy
At the Ralph H. Johnson VA Medi-cal Center in Charleston, S.C., KarenC. Downer, PharmD, and her first-yearpharmacy residency program director,Dorothy E. Jenrette, PharmD, saw anopportunity to simultaneously reducecosts and improve patient care by eval-
uating the use of pancreatic enzyme therapy and adjusting (even eliminat-ing) therapy when appropriate. By the end of the initiative, Dr. Downer calcu-lated an overall annual cost avoidance of $92,000 for their facility—a mean of about $2,050 per patient.
After the local pharmacy service noticed that the average cost of enzyme therapy for its facility exceeded costs at comparable VA facilities nationally, the
Pharmacy and Therapeutics Committee approved a pharmacist telephone clinic to evaluate therapy for patients pre-scribed more than 60,000 lipase units daily. Between Sept. 1, 2011 and April 1, 2012, 45 patients received clinical phar-macist intervention.
“I called each patient and worked with them to see if we could get them on an appropriate dose,” Dr. Downer said. “I tried to find a way to reduce their daily
pill burden and still control their disease,and, ultimately, [reduce] the total cost of the prescribed medication.”
Dr. Downer performed a thorough medical chart review and interviewed each patient for any current or past symp-toms of pancreatic disease. She evaluated patients for the frequency and consis-tency of their bowel movements, any his-tory of weight loss and currently pre-scribed proton pump inhibitors. “First, I wanted to gauge how they were doing with their current treatment,” she said. If
SAVINGScontinued from page 1
• see SAVINGS, page 18
Part 1 of a Two-Part Series
BEYOND ABOVE-AND-BEYOND
Pharmacy Practice News • January 2013
Finance
Operations & Management 17

the patients were symptom-free, enzyme doses were gradually lowered by one cap-sule per meal until they reached a per-sonalized dose without having symptoms.
Many patients were able to decrease their doses significantly and keep symp-toms under control. Patients whose symptoms were unstable were referred to the gastroenterology clinic.
All patients received routine follow-up to assess for symptom changes. “I contin-ued to call them until we got them on the lowest dose that kept them stabilized,” Dr. Downer said.
Pill burden was decreased from 6.5 to 2.1 capsules per day (P(( =0.0001) for the entire group, and from 7.9 to 5.5 for patients who remained on therapy after the intervention. In some cases, even patients with confirmed pancre-atitis were weaned completely off the enzymes because they remained asymp-tomatic without therapy. Twenty-eight patients (62%) were able to discontinue therapy completely; 10 (22%) had a dose reduction; and seven (16%) remained on their original dose. The mean daily dose change from 105,444 to 79,111 lipase units daily represented a statistically significant difference for patients who continued therapy (n=17).
Perhaps the most surprising finding was that 25 of the patients had no his-tory of chronic pancreatic disease and were able to discontinue therapy com-pletely. These patients often were taking enzymes for a history of a single acute pancreatic attack or other bowel dis-orders for which enzyme therapy was providing no benefit.
Based on those outcomes, the facil-ity was able to establish criteria for pre-scribing pancreatic enzyme therapy, which includes a confirmed diagnosis of chronic pancreatic disease from a gas-trointestinal specialist or by radiographic findings, and patient symptoms of fat malabsorption evidenced by steatorrhea or weight loss. “The diagnosis should not come from a primary care physician or after one visit to the ED [emergency department] without expert or radio-graphic confirmation,” Dr. Downer said. “The prescription also goes through the pharmacy for approval based on these criteria. These enzymes have become high-cost medications that we monitor monthly to evaluate for appropriate pre-scribing and use.”
Pharmacists Do ItCheaper Than PBMs
By assuming responsibility for phar-macy services normally delegated to its external pharmacy benefit manage-ment (PBM) company, one major hos-pital system created a novel and more cost-effective way to provide pharmacy
benefits for employees enrolled in the system’s health plan.
“Traditionally, we’ve outsourced most of our pharmacy benefit man-agement work,” said Kelley Curtis, PharmD, MBA, corporate director of pharmacy at Sisters of Charity of Leavenworth Health System (SCLHS), in Lenexa, Kan. “Our approach has changed, and now we’ve become very involved with pharmacy benefit con-sulting and development to create our own pharmacy benefit plan that covers
our health system employees and their beneficiaries.”
The health system is composed of 11 SCLHS and Exempla Healthcare facili-ties in four states, and the employee health plan covers more than 19,000 individuals. In 2010, the health system spent more than $15 million on pre-scription medications for its employ-ees, including $7 million for mail order prescriptions.
SCLHS/Exempla met with inpa-tient pharmacy leadership and asked them to identify options that would provide pharmacy benefits to employ-ees, potentially improving health out-comes and lowering drug costs. For example, according to Dr. Curtis, phar-macy administrators worked with the health system’s mail order pharmacy to replace all employee prescriptions sup-plied by the external PBM with drugs purchased at considerable savings with group purchasing organization (GPO) prices. “Usually you have to pay what [the insurer] wants, but we were able to replace the inventory with prescrip-tions purchased under GPO pricing, since our employees are eligible for ‘own-use’ pricing,” she said.
The health system also internalized specialty pharmacy services. Dr. Curtis explained that specialty pharmacy ser-vices had been outsourced to a company that did little to help SCLHS/Exempla employees enroll in prescription assis-tance programs. Many were left to scramble for resources to obtain expen-sive medications, so the health system shifted the responsibility to its own retail infusion center pharmacy, which staffs specialty pharmacy experts. That change alone resulted in a $400,000 savings, along with a notable rise in the num-ber of employees enrolled in prescrip-tion assistance programs. The specialty pharmacy plan cost per day of therapy also dropped considerably: from $82.89
per day in the fourth quarter of 2011(before the plan was brought in house)to $71.35 and $67.94 in the subsequenttwo quarters (after the plan was inter-nalized) (Figure). Other measures thatcontributed to savings included encour-aging prescribers to select medicationsin accordance with evidence-based prac-tice, monitoring employee drug usagefor over- and underutilization and using copay incentives to drive employees touse outpatient pharmacy services in hos-pitals where they are available.
As of September 2012, the system hadsaved an annualized $1,875,000 beforedrug rebates—a 13.4% decrease from theprevious year.
“We’ve handed over many decisionsabout our employees’ pharmacy care tosome of our hospital pharmacy leaders,”Dr. Curtis said. “The human resourcesdepartment at many hospitals doesn’trealize [it has] access to such a high levelof pharmacy benefits specialists right intheir own backyard.”
For other systems that want to followthe SCLHS/Exempla lead, Dr. Curtissaid the pharmacy department shouldinform human resources personnel thatit wants to become involved with thedevelopment of an employee pharmacy plan. “Hospital pharmacy leadershiptends to shy away from [such plans],but we could get a lot more involved.We have thousands of employees andtheir families who could benefit fromour services.”
Savings From LeanProcess Improvement
Significant savings also accrued to theUniversity of Massachusetts MemorialMedical Center, in Worcester, as a resultof its Pharmacy Department’s partici-pation in a system-wide lean processimprovement initiative and concurrentadjustments to medication managementprotocols. By changing its approach todispensing and administering costly oncology drugs, the facility racked upsavings of more than $400,000 from fis-cal year (FY) 2009-2010 to FY 2010-2011,according to Karen Smethers, PharmD,BCOP, the manager of the Oncology Phar-macy and Investigational Drug Services.
The cost for inpatient rituximab(Rituxan, Genentech) alone decreasedfrom baseline by more than $250,000 inFY10 and by $150,000 in FY11. The driv-ing force behind the savings was shift-ing the location of the infusion from
the inpatient setting to the outpatient clinic, where the cost of delivering care is lower and reimbursement is higher, Dr. Smethers noted.
The lean process improvement effort was made possible through the work of various multidisciplinary commit-tees representing pharmacists, physi-cians, nurses, clerical staff, laboratory personnel and hospital administrators, Dr. Smethers added. As a result of that collaboration, several additional cost-cutting strategies were recommended by the medical center’s Oncology Pharmacy and Therapeutics Subcommittee and carried out by caregivers. The strategies included the following:• Promoting evidence-based provision
of care so that patients receive only those oncology drugs determined to be effective for their specific circum-stances according to the most current research. For example, the pharmacy promoted the use of oral immunosup-pressive therapy, such as mycopheno-late and tacrolimus in clinically stable patients, to reduce cost and promote earlier discharge.
• Ensuring that patients arrive at theoncology clinic only after they havereceived prior authorization from their insurance company.
• Encouraging prescribers to practicedose rounding within 5%, which elim-inates waste from partially used vials.
—Steve Frandzel
Drs. Smethers, Downer and Curtis,and Mr. Martin reported no relevant
fi nancial confl icts of interest.
SAVINGScontinued from page 17
‘The [HR] department at many hospitals doesn’t
realize [it has] access to ... a high level of pharmacy
benefits specialists right in their own backyard.’
—Kelly Curtis, PharmD
100
80
60
40
20
0
Co
st (
do
llars
)
Pre-implementation
(Q4 2011) (Q1 2012) (Q2 2012)
Post-implementation
82.89
71.3567.94
Figure. Cost per day, specialty pharmacy benefit.
10082.89
Pharmacy Practice News • January 2013
Finance
18 Operations & Management

by Iowa but located outside its borders.“We’re moving full bore ahead,”
Carmen Catizone, MS, RPh, DPh, the executive director of the association, told Pharmacy Practice News. “The response from the states has been incredible. They’ve said, ‘This is an issue we own and we’re going to move quickly on it.’”
Preliminary findings from the inspec-tions suggest that the New England Com-pounding Center (NECC), whose tainted methylprednisolone was the source of the meningitis outbreak, is by no means the only pharmacy to compound drugs that are seldom if ever tied to a specific pre-scription. Four of the six compounders were found to distribute non-patient-spe-cific, preservative-free sterile injectables, which can be at odds with “traditional” compounding—that is, the preparation of medications prescribed in small quanti-ties for specific individuals. Two of the pharmacies produced very large volumes of non-patient specific sterile drugs, Dr. Catizone reported.
The findings have been sent to Iowa, he said, and the state “is going to be making some determinations.” Dr. Cati-zone praised Iowa’s “innovative” initia-tive. “They were able to think outside the box and say, ‘We can’t hire staff to do this, but we have the funding and we can use it in a way that gets the outcomes accomplished.’” He said other states were weighing similar agreements with NABP.
The NABP approach—to preserve indi-vidual states’ ownership of traditionalpharmacy compounding oversight while broadening their ability to monitor non-resident compounders who ship prod-uct into their states—appears to cross over into FDA turf, which is oversight of interstate-shipped medications.
The FDA, meanwhile, is pressing Congress for new legislation that will reinforce the agency’s hand in policing practices that go beyond prescription-driven compounding. But some phar-macy sources worry that the FDA’s push for new authority may threaten states’ traditional role and raise the risk for a possible “federalization” of compound-ing practice. “I am absolutely terrified that the FDA is going to get in the middle of this, and more importantly, I’m more afraid that Congress is going to get into the middle of this and they’re going to muck this thing up,” said Eric Kastango, RPh, MBA, the president and the CEO of Clinical IQ, speaking at the American Society of Health-System Pharmacists’ Midyear Clinical Meeting last month.
Others have raised doubts about wheth-er a budget-minded Congress would allo-cate funds that the FDA needs to hire more inspectors and expand its national oversight of compounders. The FDA has moved to ease these concerns. In Decem-
ber, agency officials met with pharmacy and health department regulators from all 50 states to solicit input on how feder-al and state agencies might work together to “close gaps” in the “regulatory frame-work,” as Margaret Hamburg, MD, the FDA Commissioner, put it.
Pharmacy board officials who spokeat the two-hour FDA public hearing that followed their early meetings at the agen-cy’s headquarters in Silver Spring, Md., expressed confidence in their capacity to regulate compounding pharmacies in their own states, but some said that
they were challenged by the difficulty of controlling nonresident compounders. “We know what happens in pharma-cies in Arkansas,” said John Clay Kirtley, PharmD, the executive director of the Arkansas State Board of Pharmacy. “We don’t necessarily know about what is happening in specific pharmacies in oth-er states that ship into our state.”
Several board officials noted that insuf-ficient funding often hampers states’ reg-ulatory efforts. Jay Campbell, RPh, JD, the executive director of the North Caro-lina Board of Pharmacy, said that where-
as his board and others in the Southeast region generally have the resources to carry out their missions, others around the country “are dealing with revenue challenges.” He said it was important for state lawmakers to recognize that phar-macy boards must be adequately funded “and not simply be viewed as a revenue stream” for general purposes.
Despite concerns about the potential for federal encroachment on what tradi-tionally has been state regulatory terrain, some board officials saw areas where
• see NECC CRISIS, page 20
NECC CRISIScontinued from page 1
In just fi ve short years, Amneal Pharmaceuticals has become the seventh largest generic pharmaceutical company in the U.S.* Our focus on quality, superb service levels and building strong relationships hasn’t changed. Now, we’re bringing that philosophy to the institutional market. With injectable and unit dose products populating our portfolio, we are fully-equipped to meet the critical need for dependable, high-quality product supply. Amneal’s collaborative, transparent and responsive way of doing business
delivers unsurpassed customer service, consistent quality, convenience and a steady pipeline of essential products to your organization.
At Amneal, we understand that you are committed to providing each and every patient with the best care, in the right form, accurately and in a timely manner. Amneal has proven itself as a vital partner
in that equation.
...To be Steadfastly Focused on Quality, Integrity and Reliable Supply.
* In prescriptions of unbranded generics per IMS, June 2012
Copyright © 2012 Amneal Pharmaceuticals, All Rights Reserved - AMN-PPN-1012
amneal.com
Pharmacy Practice News • January 2013
Sterile Compounding
Policy 19

federal and state collaboration might pre-vent future public health calamities likethe one caused by NECC. Cody Wiberg,PharmD, MS, RPh, the executive directorof the Minnesota Board of Pharmacy, sug-gested that “joint investigations” by theFDA and state boards might be a way toensure better enforcement of federal andstate compounding standards. In moststates, he said, pharmacy boards “are reg-ulatory licensing agencies. We’re not lawenforcement agencies. We can’t initiatecriminal proceedings; the FDA can. Insome of these really horrible situations,[that may] get the attention of folks evenmore” than separate actions by federal orstate regulators alone, he noted.
At the federal level, Senate and Housecommittees have launched investigationsinto the causes of the NECC disaster, lay-ing the groundwork for legislative rem-edies later in 2013. At least two bills havebeen introduced in the House. The onegaining the most attention was initiatedby Rep. Edward J. Markey (D-Mass.),in whose district NECC’s manufacturing facility is located. Under the bill, mostcompounding pharmacies that engage inmass production would be regulated by the FDA as drug manufacturers.
ASHP’s Initial Take on Bills
The impact that the Markey bill orother legislative proposals might haveon hospital pharmacy was a key point of focus during a late-breaking session at theASHP’s Midyear Clinical Meeting, titled“A Compounding Tragedy—A NationalResponse.” Joseph Hill, ASHP’s direc-tor of federal legislative affairs, said thatalthough the Markey bill seems to pro-vide the FDA with regulatory flexibility,the “core issue” is how to define the pointon the continuum of compounding prac-tice where state jurisdiction ends and fed-eral authority kicks in. He said that it was“not so simple” to write legislation thatclarifies the definitions of “compounding considered to be under state jurisdictionversus mass production—what people arecalling manufacturing but may be poten-tially a third category.”
Mr. Hill emphasized that ASHP hadnot yet made any policy determinations.“We want to make sure that when wedo go down the road of addressing any regulatory gaps, we don’t have a knee-jerk reaction” and “we’re not cutting off absolutely necessary practices going onin the health systems.”
One such necessary practice that con-cerns ASHP is anticipatory compound-ing—the preparation of sterile solutionsin advance not for specific patients butbased on known usage patterns—forexample in a hospital operating room.Mr. Hill said the language in the Markey bill seems to define compounding “a bit
more narrowly” when it limits the prac-tice to being “pursuant to a patient pre-scription” and leaves out the phrase “orin anticipation of a prescription.”
If that definition were included in any final legislation, Mr. Hill said, anticipato-ry compounding “would not be automat-ically subject to state regulation,” withthe possibility that it could come underFDA purview. However, he noted thatthe bill does grant the FDA some flexibil-ity to issue waivers to entities to performcertain compounding activities, “such asin anticipation of a patient prescription.”
Addressing the issue of federal versusstate jurisdiction, Christopher J. Topoles-ki, director of federal regulatory affairs atASHP, said that it might be “useful for theFDA and state boards to collaborate fur-ther to identify entities that may be mass-producing and show they are licensedproperly and to share information aboutenforcement actions or disciplinary pro-cedures” not just between themselves butalso with the general public.
Mr. Topoleski noted that the agency had asked to be given “full authority tocollect test samples of compounded prod-ucts and ... records in compounding phar-macies, such as prescriptions received,volume of operations and product testresults.” He said ASHP was concerned“this new authority would essentially federalize regulation of traditional phar-macy compounding. We believe that thisshould remain within the jurisdiction of state boards of pharmacy.”
He also said that the FDA “quite frank-ly does not have the capacity to inspectall compounding pharmacies. Agency collaboration with state boards will benecessary to identify entities engaged inthese activities.”
Mr. Hill said that it was vital for ASHPto continue “talking to Congress as wellas other stakeholders to ensure thatwe’re moving forward.” From a lobbyist’sperspective, he added, “one of the thingswe say a lot is ‘You want to be on the trainrather than under it.’”
Who Is To Blame?
As for who is to blame for the NECCdisaster, Dr. Catizone said it’s easy to pointfingers. However, “every single one of us was responsible for this tragedy,” hestressed. “The regulatory system brokedown, the pharmacy compounding sys-tem broke down, [and] the collaborationbetween FDA and the states broke down.”Because methyl prednisolone purchasersfailed to exercise due diligence, he added,“those transactions [also] broke down.”
In terms of next steps, Dr. Catizonecautioned again focusing too much on thenuances of regulatory policy. “We can’targue [over the definition of compound-ing versus manufacturing] for 20 moreyears,” he said. “Too many patients havebeen killed. We have to act.”
—Bruce and Joan Buckley
NECC CRISIScontinued from page 19
This document provides updated tables for CLSI antimicrobial susceptibility testing (AST) standards M02-A11, M07-A9, and M11-A8.
M100-S23 | Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Third Informational Supplement
M100-S23 Vol. 33, No. 1
Replaces M100-S22 Vol. 31 No. 1
This document provides updated tables for the Clinical and Laboratory Standards Institute antimicrobial susceptibility testing standards M02-A11, M07-A9, and M11-A8.
A standard for global application developed through the Clinical and Laboratory Standards
Institute consensus process.
M100-S23Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Third Informational Supplement
introducing
Quickly find the information you need to make informed patient recommendations.
NOW AVAILABLE as an Interactive Searchable Database for Drug Selection, Interpretation, and Quality Control Procedures!
Count on CLSI’s AST standards to help you deliver reliable results.
Clinicians count on you for accuracy.
Find New or Revised Breakpoints and QC Ranges
Learn How to Put CLSI AST Standards Into Practice
Join us for upcoming webinars: The Basics: Using CLSI Antimicrobial Susceptibility Testing CLSI 2013 AST Update
Learn more at www.aphl.org/clsi.
P: 610.688.0100 www.clsi.orgToll Free (US): 877.447.1888 E: [email protected]
new for 2013
Instantly Access M100-S23 Information— All You Need is a Web Connection
10TH anniversary
Pharmacy Practice News • January 2013
Sterile Compounding
20 Policy

As health care reform moves forward,all pharmacists need to understand
how payment mechanisms for outpatientservices are determined.
Why not just leave this task to your bill-ing and coding team or to some adminis-trative person in your department? Onecompelling factor is the system that theCenters for Medicare & Medicaid Ser-vices (CMS) uses to determine payments.CMS bases its policies primarily on howyour staff decides to choose and use a medication—and the degree to whichyour staff accurately documents thosetreatment decisions. Moreover, new pay-ment mechanisms are built on a platformof data from previous years. So if yoursystems and records are less than stellar,you’ll be contributing to a new programthat underestimates true costs of care.
For these reasons, it should be clearthat reimbursement issues are every-one’s responsibility. So let’s look at 2013and see if we can find opportunities toimprove your involvement in your hos-pital or health system’s reimbursementpractices. In this article, we’ll focus onthe recently released outpatient pro-spective payment system (OPPS) rulesthat cover the medical benefit thatapplies to Part B drugs used by Medicarepatients and that often serve as a base fordecisions made by other payors (http://www.gpo.gov/fdsys/pkg/FR-2012-11-15/pdf/2012-26902.pdf ). (The rules won’tcover Part D medications handled underthe Pharmacy Benefit, nor do they apply to self-administered drugs.)
First, it is important to understandexactly who can be deemed an outpatient.Basically, an outpatient is anyone who isnot admitted to the facility as an inpa-
tient, regardless of where in the facility the person is being treated. This includes the emergency room, the operating room for ambulatory surgery patients, ancil-lary treatment areas such as the gastro-intestinal lab, catheterization lab, radi-
ology, outpatient clinics or the infusion center. (Sound familiar? These sites are some of the same places covered by 340B pricing in eligible facilities.)
The next step is to understand the correct type of codes to use. In a world
of electronic transactions, there are two types of codes—those assigned to prod-ucts, known as health care common pro-cedure coding system (HCPCS) codes,and those used for services (currentprocedural terminology, or CPT codes).Both types are used to transmit the details of the patient visit to the payor.Using the wrong codes or relying on miscellaneous codes results in little tono payment and may trigger an audit; hence the need for accuracy in all of your coding efforts.
Here’s a particularly important caveat to keep in mind: Although most HCPCS codes are listed generically, a few areaunique to the brand name, including IVIG products, as well as these examples:• Q2048 – Doxil brand of liposomal
doxorubicin (billing unit 10 mg):Effective July 1, 2012
• Q2049 – Lipodox brand of liposomal doxorubicin (billing unit 10 mg):Effective July 1, 2012
• J7315 – Mitosol brand of mitomycin ophthalmic: Effective Jan. 1, 2013
The CMS Approach To Reimbursement
CMS pays for Part B drugs in one of four ways (Figure). CMS recognizes thatnew drugs coming to market are very expensive and if they choose to cover them, reimbursement is slightly higher for these “pass-through” drugs for two to three years, as shown in the two left col-umns. Mainstream products that are sep-arately payable are in the third columnand those that have been on the marketfor some time and may be generically available fall into the fourth column. (Intha latter group, the products are often low-cost items and are thus bundled intothe patient visit rather than being sepa-rately reimbursed.)
Additionally, two different sets of rules determine payment rates for drugs usedin a hospital facility and those in a phy-sician office setting. Although both are based on average sales price (ASP), the mark-up has differed over the years that the model has been in place. This yearmarks the first time that the payment rates will be identical in both care set-tings and paid at ASP plus 6%—a 2%increase over 2012 for hospital outpa-tient medications. ASP is the average selling price of manufacturers’ sales of all U.S. purchases for each national drug
It’s Time To Take Charge!
Table 1. A Sampling of Drugs & Biologicals for Which Pass-Through Status Expired Dec. 31, 2012 (abbreviated to drugs only)
CY2013HCPCS
CY 2013 Long Descriptor CY 2013SI
CY 2013APC
C9275 Injection, hexaminolevulinate hydrochloride,100 mg, per study dose
N N/A
J0221 Injection, alglucosidase alfa (Lumizyme),1 mg
K 1413
J0588 Injection, incobotulinumtoxin A, 1 unit K 9278
J0597 Inject, C–1 Esterase inhibitor (human) Berinert 10 units
K 9269
J0775 Injection, collagenase clostridium histolyticum, 0.01 mg
K 1340
J0840 Inject, Crotalidae polyvalent immune fab (ovine), up to 1 g
K 9274
J0897 Injection, denosumab, 1 mg K 9272
J1290 Injection, ecallantide, 1 mg K 9263
J1557 Injection, immune globulin (Gammaplex), intravenous, non-lyophilized (e.g., liquid),500 mg
K 9270
J1741 Injection, ibuprofen, 100 mg (code changefrom C9279)
N N/A
J3095 Injection, telavancin, 10 mg K 9258
J3262 Injection, tocilizumab, 1 mg K 9624
J3357 Injection, ustekinumab, 1 mg K 9261
APC, ambulatory payment classification; CY, calendar year; HCPCS, health care common procedure coding system
• see TAKE CHARGE!, page 22
Figure. OPPS 2013: Drugs and Biologicals Paid in One of Four Ways.ASP, average sales price; AWP, average wholesale price; HCPCS, health care common procedure coding system; OPPS, outpatient prospective payment system; WAC, wholesale acquisition cost
Lower-Cost Packaged Products C osting <$80/Day
New Drugs Not Yet Assigned Unique
HCPCS CodeNew Pass-Through
Drugs
Specified Covered Outpatient Drugs (SCODs) Costing
>$80/Day
“Reimbursement Matters” is a tool
for maintaining your health system’s
fiscal health.Please email
the author [email protected]
with suggestionson reimbursement
issues that youwould like tosee covered. Bonnie Kirschenbaum,
MS, FASHP
Pharmacy Practice News • January 2013
Reimbursement Matters
Policy 21

code (NDC) for one calendar quarter, divided by the total number of units sold in that quarter. It excludes nominal pric-ing and Medicaid “best price,” and for 2013 continues to exclude 340B pricing. It also includes volume and prompt pay discounts, free goods, chargebacks and rebates. It is updated quarterly, so be sure to get on the distribution list (http://www.CMS.gov/McrPartBDrugAvgSalesPrice/01a172012ASPFiles.asp).
A Few More Important Details
The four columns in the Figure (page 21) outline several key reimburse-ment points that need to be heeded:
Pay attention to pass-through sta-tus. CMS carefully determines which drugs are deserving of pass-though status, changes this list at least annu-ally and adds to it during the year as new products come to market. Newly released products may have temporary HCPCS codes (usually starting with C) that change to permanent codes (usually starting with J). Look closely at Federal Register Tables (excerpted in Tables 1 and 2) to see the changes effective Jan. 1, 2013 and ensure that these updates have been made to the drug master files on your pharmacy’s computer system and to the hospital’s charge description master. Don’t leave this very important step to someone else to take care of!
Use billing units correctly. CMS reimburses for the actual doses of the drug administered, not for the whole vial of the drug. The concept of using billing units was introduced several years ago and there’s little tolerance for facilities that haven’t yet figured out how to implement the simple mathe-matical requirements. Essentially every Part B drug that CMS pays for has a bill-ing unit assigned to it (listed in the quar-
terly ASP tables) Divide the dose admin-istered by the billing unit assigned to get the number of billing units that can be billed for and round up to the next whole billing unit as needed. If you billfor too few units, you’re underpaid. If you bill for too many you’re overpaid and in eitheßr case will fail an audit. Example: Drug A comes in a 1,000-mg vial and has a 100-mg billing unit. If the dose is 600-mg, bill for six billing units of 100 mg. If the dose is 650 mg, bill for seven billing units of 100 mg.
Bill for drug waste. This is possible if certain conditions are met. Ask yourself the following four questions and proceed to billing for waste only if the answers to all four questions are “yes,” following the guidelines set up by the Medicare Administrative Contractor (MAC) range you’re in:
Q: Is the drug being used for a Medi-care patient being treated in an outpa-tient area?
Q: Am I using a single-dose vial of the drug?
Q: Does the product have a HCPCS code?
Q: Does the dose fall into the pass-through or separately payable category (not the <$80 per day bundle noted in the Figure)?
Bundled payments. This paymentstrategy comes into play with drugs that cost (determined by ASP) less than $80 per day, an increase from $75 in 2012. These are not separately reimbursable but instead are bundled into the payment the facility receives for the patient visit. CMS assumes that the facility finance team can tease out which portion of the bundle goes to which department within the facility. How are you getting your part of the bundle? Equally important, are you actually reporting the use of these products even though they are not separately reimbursable? If not, you are short-changing the amount that the bun-
dle payment is worth. Worse still, you’relosing the drug administration fee for theproduct because these fees are paid only when the product is billed for as well.
Drug Administration Fees. This vital part of reimbursement experienced a rise in all 2013 fees except one. Checkout the fee tables to ensure that you’reusing the correct CPT codes and that you’ve set up documentation mecha-nisms either electronically or manually to ensure that all necessary data is being captured. Also, make sure that yourpharmacy department is being paid for drug preparation and handling. (Again,those payments need to be teased outof the drug administration fee bundle.)
More Tasks To TackleHere’s a few additional reimburse-
ment-related tasks that you or some-one in your department should be championing: regular charge master reviews; periodic audits of patient bills/claims; development of printed order sheets; embedding billing infor-mation in computerized prescriber order entry systems; reviewing claim denials/write-offs; participating in pre-RAC (recovery audit contractor) or RAC audits and appeals; and com-menting on proposed CMS rules.
Good luck with meeting these reim-bursement challenges in 2013 and beyond!
and establishing a screening criterion to better target patients with HF. Patients were targeted if they were on the cardiac telemetry unit, had a left ventricular ejec-tion fraction less than or equal to 40% and had a primary care provider (PCP) within an affiliated provider group.
“We focused on the worst of the worst patients, those most likely to come back repeatedly,” said lead researcher Dmitri Cohen, PharmD, BCPS, currently a critical care resident at the University Medical Center of Southern Nevada, in Las Vegas. “Before the study, they were getting very little education. During the study, we’d spend 30 minutes to an hour with each patient having detailed conversations.” During each session,
patients were encouraged to take their blood pressure and weight on a daily basis and to notify their PCP of any significant changes. After the sessions,pharmacists emailed notes and sugges-tions to the PCP’s nurse case manager and pharmacist.
The initiative was implemented on Sept. 26, 2011. The team found that 30-day HF readmission rates fell signifi-cantly after implementation, from 17.6% to 19.5% before implementation (2008-2011 data) to 11.7% after (data from first three quarters of 2012), a 33% to 40% reduction (P(( =0.0327).
The special challenges of serving a rural area affected the study, noted Dr. Cohen. “It was a very unhealthy popu-lation of patients. For many of them, exercise was chopping wood once a week,” he said. “They hadn’t been edu-
cated. They didn’t know the symptomsof heart failure, so they were waiting toolong before coming in.”
Patients’ Role Is Crucial
Getting patients to understand their medications, to be committed to taking them as prescribed, to weighing them-selves and to taking their blood pres-sure daily is a huge step forward, accord-ing to C. Michael White, PharmD, thedepartment head and a professor inthe Department of Pharmacy Practiceat the University of Connecticut inStorrs. “The addition of the safety mea-sures is vitally important and new in thisstudy,” he said. “The patients we see with20 pounds of fluid overload are at great-est risk for intubation, nosocomial infec-tions, arrhythmias and death. If they werecaught with more than 2 pounds of weight
loss on a single day or 5 pounds in a week, and treated at that point, their chances for success would be much better.”
These studies illustrate the need for pharmacists to play a more crucial role as hospitals become more responsi-ble for reducing readmission rates, Dr. White noted. He predicted that find-ing clinical care and reimbursement models “that integrate all health care providers who add value to the team in a manner that best utilizes their skills and time availability” is going to be a core feature of a successful system.
—Dana Hawkins-Simons, with additional reporting by Sarah Tilyou
Drs. Page, Trevarrow, Moye, Groo, Kaplan, Bergman, Cohen and White reported no
relevant fi nancial confl icts of interest.
Table 2. A Sampling of Drugs and Biologicals With Pass-Through Status in CY 2013 (abbreviated to drugs only)
CY2012HCPCSCode
CY2013HCPCS Code
CY 2012 Long Descriptor FinalCY 2013SI
FinalCY 2013APC
C9285 C9285 Lidocaine 70 mg/tetracaine70 mg, per patch
G 9285
C9286 J0485 Injection, belatacept, 1 mg G 9286
C9287 J9042 Injection, brentuximab vedotin, 1 mg
G 9287
C9288 J0716 Injection, centruroides (scorpion)immune f(ab)2 (Equine), 1 vial
G 9288
C9289 J9019 Injection, asparaginase Erwinia chrysanthemi, 1,000 IU
G 9289
C9290 C9290 Injection, bupivicaine liposome,1 mg
G 9290
C9292 C9292 Injection, pertuzumab, 10 mg G 9292
C9293 C9293 Injection, glucarpidase, 10 units G 9293
N/A C9294 Injection, taliglucerase alfa,100 units
G 9294
N/A C9295 Injection, carfilzomib, 1 mg G 9295
N/A C9296 Injection, ziv-aflibercept, 1 mg G 9296
J0131 J0131 Injection, acetaminophen, 10 mg G 9283
APC, ambulatory payment classification; CY, calendar year; HCPCS, health care common procedure coding system
TAKE CHARGE!continued from page 21
HF READMISSIONScontinued from page 11
Pharmacy Practice News • January 2013
Reimbursement Matters
22 Policy

SAMSCA® (tolvaptan) tablets for oral use
WARNING: INITIATE AND RE-INITIATE IN A HOSPITAL AND MONITOR SERUM SODIUMSAMSCA should be initiated and re-initiated in patients only in a hospital where serum sodium can be monitored closely.Too rapid correction of hyponatremia (e.g., >12 mEq/L/24 hours) can cause osmotic demyelination resulting in dysarthria, mutism, dysphagia, lethargy, affective changes, spastic quadriparesis, seizures, coma and death. In susceptible patients, including those with severe malnutrition, alcoholism or advanced liver disease, slower rates of correction may be advisable.INDICATIONS AND USAGE:
Important Limitations
CONTRAINDICATIONS:Urgent need to raise serum sodium acutely: SAMSCA has not been studied in a setting of urgent need to raise serum sodium acutely.Inability of the patient to sense or appropriately respond to thirst:
Hypovolemic hyponatremia:
Concomitant use of strong CYP 3A inhibitors:
Anuric patients: WARNINGS AND PRECAUTIONS:Too Rapid Correction of Serum Sodium Can Cause Serious Neurologic Sequelae (see BOXED WARNING): Osmotic
Gastrointestinal Bleeding in Patients with Cirrhosis:
Dehydration and Hypovolemia:
in response to thirst.Co-administration with Hypertonic Saline:
Drug Interactions:Other Drugs Affecting Exposure to Tolvaptan:CYP 3A Inhibitors:concentrations [see Dosage and Administration (2.3), Drug Interactions (7.1)]
[see Contraindications (4.4)] CYP 3A Inducers:
increased [see Dosage and Administration (2.3), Drug Interactions (7.1)].P-gp Inhibitors:cyclosporine [see Dosage and Administration (2.3), Drug Interactions (7.1)].Hyperkalemia or Drugs that Increase Serum Potassium:
ADVERSE REACTIONS:Clinical Trials Experience:
Table 1. Adverse Reactions (>2% more than placebo) in Tolvaptan-Treated Patients in Double-Blind, Placebo-Controlled Hyponatremia Trials
System Organ ClassMedDRA
Preferred Term
Tolvaptan 15 mg/day-60 mg/day
(N = 223)n (%)( )
Placebo
(N = 220)n (%)
Gastrointestinal Disorders
ConstipationGeneral Disorders and Administration Site Conditions
a
AstheniaPyrexiaMetabolism and Nutrition Disorders
bb
Anorexia c
Renal and Urinary Disordersdd
a b c d
reactions
SAMSCA® (tolvaptan)
Blood and Lymphatic System
Investigations: Prothrombin time prolonged; Gastrointestinal Disorders: Ischemic colitis; Metabolism and Nutrition Disorders: Diabetic ketoacidosis; Musculoskeletal and Connective Tissue Disorders: Rhabdomyolysis; Nervous System: Cerebrovascular accident; Renal and Urinary Disorders: Urethral hemorrhage; Reproductive System and Breast Disorders (female): Vaginal hemorrhage; Respiratory, Thoracic, and Mediastinal Disorders: Pulmonary embolism, respiratory failure; Vascular disorder: Deep vein thrombosis.DRUG INTERACTIONS:Effects of Drugs on Tolvaptan:Ketoconazole and Other Strong CYP 3A Inhibitors:
[see Dosage and Administration (2.3) and Contraindications (4.4)].Moderate CYP 3A Inhibitors:
[see Dosage and Administration (2.3) and Warnings and Precautions (5.5)].Grapefruit Juice: [see Dose and Administration (2.3) and Warnings and Precautions (5.5)].P-gp Inhibitors:
[see Dose and Administration (2.3) and Warnings and Precautions (5.5)].Rifampin and Other CYP 3A Inducers:
[Dosage and Administration (2.3) and Warnings and Precautions (5.5)].Lovastatin, Digoxin, Furosemide, and Hydrochlorothiazide:
Effects of Tolvaptan on Other Drugs:Digoxin:
Warfarin, Amiodarone, Furosemide, and Hydrochlorothiazide:
Lovastatin:
change.Pharmacodynamic Interactions:
USE IN SPECIFIC POPULATIONS:[see Clinical Pharmacology (12.3)].
Pregnancy: Pregnancy Category C.
[see Nonclinical Toxicology (13.3)].Labor and Delivery: Nursing Mothers:
of SAMSCA to the mother.Pediatric Use:Geriatric Use:
plasma concentrations.Use in Patients with Hepatic Impairment:
Use in Patients with Renal Impairment:
[seeContraindications 4.5) and Clinical Pharmacology (12.3)].Use in Patients with Congestive Heart Failure:
OVERDOSAGE:
50
considered.
PATIENT COUNSELING INFORMATION:[see FDA-Approved Medication Guide (17.3)].
Concomitant Medication:counter drugs since there is a potential for interactions.Strong and Moderate CYP 3A inhibitors and Pg-p inhibitors:
[see Dosage and Administration (2.3), Contraindications (4.4), Warnings and Precautions (5.5) and Drug Interactions (7.1)].Nursing:
SAMSCA is a registered trademark of Otsuka Pharmaceutical Co., Ltd., Tokyo, 101-8535 Japan
© 2012 Otsuka Pharmaceutical Co., Ltd.
MCPPN2221.indd 1 4/19/12 4:23 PM

of physicians surveyed (N=57) would recommend SAMSCA to a colleague1
In this same survey (patient cases; N=150), physicians weresatisfied or very satisfied with SAMSCA 90% of the time1100%
©2012 Otsuka America Pharmaceutical, Inc. March 2012 0712A-4220K
UNMET NEED. FILL IT.
15 mgNDC: 59148-020-50
30 mgNDC: 59148-021-50
Unique oral treatment for clinically significant hypervolemic
and euvolemic hyponatremia
VVATERFREECLEARANCE
VV22
Order SAMSCA® (tolvaptan)
Indication and important limitations • SAMSCA is indicated for the treatment of clinically significant hypervolemic and euvolemic hyponatremia (serum sodium <125 mEq/L
or less marked hyponatremia that is symptomatic and has resisted correction with fluid restriction), including patients with heart failure, cirrhosis, and Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
• Patients requiring intervention to raise serum sodium urgently to prevent or to treat serious neurological symptoms should not be treated with SAMSCA. It has not been established that raising serum sodium with SAMSCA provides a symptomatic benefit to patients
Important safety information SAMSCA should be initiated and re-initiated in patients only in a hospital where serum sodium can be monitored closely. Too rapid correction of hyponatremia (e.g., >12 mEq/L/24 hours) can cause osmotic demyelination resulting in dysarthria, mutism, dysphagia, lethargy, affective changes, spastic quadriparesis, seizures, coma and death. In susceptible patients, including those with severe malnutrition, alcoholism or advanced liver disease, slower rates of correction may be advisable.
Contraindications: Urgent need to raise serum sodium acutely, inability of the patient to sense or appropriately respond to thirst, hypovolemic hyponatremia, concomitant use of strong CYP 3A inhibitors, anuric patients.
• Subjects with SIADH or very low baseline serum sodium concentrations may be at greater risk for too-rapid correction of serum sodium. In patients receiving SAMSCA who develop too rapid a rise in serum sodium or develop neurologic sequelae, discontinue or interrupt treatment with SAMSCA and consider administration of hypotonic fluid. Fluid restriction should generally be avoided during the first 24 hours
• Dehydration and hypovolemia can occur, especially in potentially volume-depleted patients receiving diuretics or those who are fluid restricted. In patients who develop medically significant signs or symptoms of hypovolemia, discontinuation is recommended
• Gastrointestinal bleeding in patients with cirrhosis: Use in cirrhotic patients only when the need to treat outweighs this risk
• Avoid use with: CYP 3A inhibitors and CYP 3A inducers. Reduced dose of SAMSCA may be needed if used with P-gp inhibitors
• Co-administration with hypertonic saline is not recommended
• Monitor serum potassium in patients with levels >5 mEq/L and in those receiving drugs known to increase serum potassium
Commonly observed adverse reactions: (SAMSCA vs placebo) thirst (16% vs 5%), dry mouth (13% vs 4%), asthenia (9% vs 4%), constipation (7% vs 2%), pollakiuria or polyuria (11% vs 3%) and hyperglycemia (6% vs 1%).
Reference: 1. Market Rx 2010.
Please see Brief Summary of FULL PRESCRIBING INFORMATION, including Boxed WARNING, on the following page.Manufactured by Otsuka Pharmaceutical Co., Ltd., Tokyo, 101-8535 Japan. Distributed and marketed by Otsuka America Pharmaceutical, Inc., Rockville, MD 20850.Samsca is a registered trademark of Otsuka Pharmaceutical Co., Ltd., Tokyo, 101-8535 Japan.
For more information about SAMSCA, visit samsca.com or call 1-877-726-7220.
MCPPN2222.indd 1 4/19/12 4:26 PM

Immune Globulins:Therapeutic, Pharmaceutical, Cost, and Administration Considerations
JERRY SIEGEL, PHARMD, FASHPClinical Associate Professor The Ohio State University College of PharmacyColumbus, Ohio
For the past several years, the availability
of immune globulin (Ig) products has
been very good, so product shortages
have not played a major role in product choice.
This allows cli-nicians to match
the best product to the patient based on clinical condi-tion and comorbidities.
New products have become available, providing more treatment
options. For example, Bivigam (Biotest), a 10% liquid product for intravenous use, was approved in Decem-ber 2012 and is expected to be released in early 2013.Also, there are now 4 Ig products indicated for subcu-taneous use: Gammagard Liquid (Baxter), Gammaked (Grifols), and Gamunex-C (Grifols) come in 10% concen-trations and can be administered intravenously or subcu-taneously (PID only), and Hizentra (CSL Behring) comes in a 20% concentration. It should be noted that dosing adjustments are required for all SC agents when con-verting from IV.
Another area of change for Igs is the use of these products for various new indications. Two products, Gammaked and Gamunex-C, are approved for use in patients with chronic inflammatory demyelinating poly-neuropathy (IV only). Gammagard Liquid is approved to treat multifocal motor neuropathy.
A common question regarding Ig products relates to whether they all are the same. Although clinicians have considered all Ig products to have comparable efficacy, they are not pharmaceutically equivalent. It is imperative that Ig products not be interchanged without full consid-eration of the pharmaceutical differences.
The reasons for switching products may be clinical in nature and related to tolerability; they may be fiscal and based on contracting issues; or they may be due to product availability. It is best
to consider product changes as if the patient is naive to Ig use, with increased monitoring and conservative infusion times.
Whereas Tables 1 to 5 may help facilitate these decisions, it is important to understand the clinical impact of changing products. Although all of the products contain primarily IgG, trace amounts of other Igs—IgA and IgM—as well as widely different stabilizing agents, may affect tolerability. The differ-ences in salt, sugar, and overall osmolarity of these products are particularly important when patients have various comorbidities, such as renal dysfunction, diabetes mellitus, vascular disease, or heart failure. Differences between lyophilized and liquid products may result in changes in product concentration and infusion rate, as well as tolerability.
The tables may be helpful in providing optimal care for patients receiving Ig products. They should be used as a general guide to help determine the product that is best suited for a particular patient population. Because there is variation from batch to batch, the exact numbers represent averages of selected batch-es; any one batch of any Ig product may have rang-es outside these average numbers. When comparing administration rates, clinicians need to keep in mind that each patient has a maximum tolerated rate. This rate is based on patient tolerability and may be differ-ent for each product. Ig must be administered slow-ly initially and titrated as tolerated. The rate should be adjusted based on comorbidities as well. The infusion should be slowed or stopped if adverse events (AEs) become evident during the infusion. (See the prescrib-ing information for each agent for more information about AEs.)
hav
This allows cli-nicians to match
the best product to thepatient based on clinical condi-tion and comorbidities.
New products have becomeavailable providing more treatment
1INDEPENDENTLY DEVELOP ED BY M C M AH ON P U BL ISHIN G PHA RMACY PRACTICE N E WS • JA N UA RY 2013
PRINTER-FRIENDLY VERSION AVAILABLE AT PHARMACYPRACTICENEWS.COM

Footnotes on page 7; Key on page 8.
Editor’s Note: Bivigam was approved in late December 2012, but at press time it was not yet available.
Table 1. Therapeutic Considerations
Producta Manufacturer
FDA-Approved Indications IgA Content
pH (after reconsti-tution) Plasma Source
Half-life, db
Viral Inactivation/Removal
IgG Sub-class,c %
IgG1
Bivigam Biotest PharmaceuticalsMedical info: (800) 458-4244www.bivigam.com
PID ≤200 mcg/mL 4.0-4.6 NA 30 Cold ethanol frac-tionation, 35 nm virus filtration, SD
NA
Carimune NF CSL BehringCustomer service: (800) 683-1288 Medical info: (800) 504-5434www.cslbehring.com
ITP, PID 1,000-2,000 mcg/mL (6%)
6.4-6.8 Plasmapheresis, US donors (>16,000)
23 pH 4.0/pepsin, nanofiltration, TSE removal
60.5
Flebogamma 5% DIFFlebogamma 10% DIF
Instituto Grifols SA Barcelona, Spain Customer service: (888) GRIFOLSwww.grifols.com
PID <3.2 mcg/mLc,d 5.6±0.1 (5%)d
5.5±0.1 (10%)d
US source IQPP-certified plasma from FDA-registered sites
4-week dosing: 32±5 (5%),37±13 (10%)
Pasteurization (60°C, 10 h), SD, dual nanofiltration (35+20 nm), fraction I and II+III precipitation, 4% PEG precipitation, pH 4.0 treatment, TSE removal
66.6
Gammagard Liquid 10%
Baxter Healthcare Corp Direct inquiries: (800) 423-2090 www.baxter.com
MMN, PID 37 mcg/mL 4.6-5.1 Plasma from FDA-registered sites
35 SD, low pH, nanofiltration
60.9
Gammagard S/D 5%
Baxter Healthcare Corp Direct inquiries: (800) 423-2090 www.baxter.com
CLL, ITP, KD, PID
<2.2 mcg/mL, <1 mcg/mLe
6.4-7.2 Plasmapheresis, 10,000 donors
37.7±15 SD 67
Gammaked Grifols Therapeutics IncDistributed by Kedrion BiopharmaCustomer service/medical info: (855) 353-7466www.gammaked.comwww.kedrion.com
CIDP, ITP, PIDf
47±13 mcg/mLc,d
4.1c,d US source IQPP- certified plasma from FDA-registered sites
35 pH 4.2, caprylate chromatography purified, TSE removal
62.8
Gammaplex Bio Products Laboratory(distributed by FFF Enterprises)Customer service: (800) 843-7477 www.fffenterprises.com
PID <10 mcg/mL 4.8-5.1 Plasma from FDA-registered sites
41±14 SD, nanofiltration, terminal low pH incubation
64
Gamunex-C Grifols Therapeutics IncCustomer service: (800) 243-4153Medical info: (800) 520-2807 www.gamunex-c.com
CIDP, ITP, PIDf
47±13 mcg/mLc,d
4.1c,d US source IQPP-certified plasma from FDA-registered sites
35 pH 4.2, caprylate chromatography purified, TSE removal
62.8
Hizentra 20% CSL Behring Customer service: (800) 683-1288 Medical info: (800) 504-5434www.cslbehring.comwww.hizentra.com
PID ≤50 mcg/mL 4.6-5.2 Plasmapheresis, US donors
NA pH 4.0 incubation, nanofiltration, depth filtration, virus filtration, TSE reduction
68.7
Octagam 5% Octapharma Pharmazeutika Octapharma USA Customer service: (866) 766-4860 www.octapharma.com
PID ≤200 mcg/mLg
5.1-6.0 US source and recovered plasma
41 Cold ethanol, SD, pH 4.0 incubation for 24 h at 37°C
65
Privigen 10% CSL Behring Customer service: (800) 683-1288 Medical info: (800) 504-5434 www.cslbehring.com; www.privigen.com
ITP, PID ≤25 mcg/mL 4.6-5.0 Plasmapheresis, US donors (≥60,000)
36.6 pH 4.0 incubation, 20 nm virus filtration, depth filtration, TSE removal
67.8
INDEPENDENT LY DEVELOP ED BY M C M AH ON P UBL ISHIN G2

Diphtheria Toxinc
Streptococcus pneumoniaec
Haemo philus influ enzae Type Bc
Streptoly-sin Oc CMVc HAVc
HBV (Surface Anti-body)c
Herpes Simplex Type 1c
Polio Type 2cIgG2 IgG3 IgG4 Type 1 Type 3
NA NA NA NA NA NA NA NA NA NA NA NA NA
30.2 6.6 2.8 3.6 IU/mL (NT)
313 (EIA) 180 (EIA) 1:60 (CF) 300 IU/mL (HAI)
1:512 (IFA); 1:2,560 (EIA)
1:348 (RIA)
1:64 (RIA) 1:128 (CF)
1:64 (NT)
28.5 (5%), 27.9 (10%)
2.7 (5%), 3.0 (10%)
2.2 (5%), 2.5 (10%)
7.0±1.0 IU/mL (5%),13.7±1.4IU/mL (10%)
NA NA 15±1 mg/L (5%)
NA 30±6 PEI units/mL (5%), 69±16 U/mL (10%)
21±4 IU/mL (5%)
88.0± 41.8 IU/g Ig (5%), 80.7± 23.0 IU/g Ig (10%)
NA NA
32.1 5 2.1 4.0 units/mL (NT)
NA 21.2 mcg/mL (EIA)
1:2,320 (EIA) NA 68 PEI units/mL (EIA)
16.4 IU/mL (RIA)
≥0.20 IU/mL (EIA)
VZV: 32 units/mL (NT)
Type 1: 1:190 mIU/mL (NT)
25 5 3 2-5 IU/mL (NT); J5 lipid A 1:273
17.5 mcgAbN/mL (EIA)
8.5 mcg/mL (EIA)
11 mcg/mL (EIA)
1,150 IU (HH)
37 PEI mcg/mL (EIA), 1:2,480 (NT)
1:267 (RIA)
820 mIU/mL (RIA)
1:1,000 (EIA)
1:305 (NT)
29.7 4.8 2.7 7±2 AU/mL 87.4±22.2 mcg/mL
26.1±7.7 mcg/mL
13.0±2.4 mcg/mL
16,846±
13,648 Todd units/mL
57 PEI units/mL
1:139 65±19 IU/g Ig
NA 1:22 ±
0.35
30 5 1 2.2 IU/mL 2.3 mcg/mL
NA 791 mcg/mL 185 IU/mL 431 U/mL
20 IU/mL
4.7 IU/mL
5,129 AU/mL
NA
29.7 4.8 2.7 7±2 AU/mL 87.4±22.2 mcg/mL
26.1±7.7 mcg/mL
13.0±2.4 mcg/mL
16,846±
13,648 Todd units/mL
57 PEI units/mL
1:139 65±19 IU/g Ig
NA 1:22 ±
0.35
26.6 2.7 2 ≥2.5 IU/mL NA NA NA ≥1,000 IU/mL
NA NA ≥0.4 IU/mL
NA NA
30 3 2 5-30 IU/mL NA NA NA 600-800 IU/mL
33-40 IU/mL
21-25 IU/mL
51 IU/g 1:8,192 1:160-1:320 (NT)
28.7 2.3 1.2 4.9 (3.8-7.3) IU/mL
NA NA 36.1 (26.4-45.0) IU/mL
1,746 (1,310-2,010) IU/mL
76.4 (51.2-116.8) IU/mL
NA 5.3 (3.0-10.1)IU/mL
NA NA
3IN D E PE N D E N TLY D E VE LOPE D BY MCMA HON PUBL ISHING

Footnotes on page 7; Key on page 8.
Table 2. Pharmaceutical Considerations
Producta Method of Preparation
Available Dosing Forms Form
Gamma Globulin, % Monomers, %
Bivigam Cohn-Oncley,i cold ethanol fractionation, SD IV Liquid NA NA
Carimune NF Kistler-Nitschmann,i pH 4.0 + trace pepsin, nanofiltration
IV Lyophilized ≥96 92
Flebogamma 5% DIFFlebogamma 10% DIF
Cohn-Oncley,i ion-exchange chromatography, acid pH treatment, PEG precipitation, SD,pasteurization, dual nanofiltration (35+20 nm)
IV Liquid 99.6±0.2 (5%),c,d
99.6±0.1 (10%)c,d
>99.95 monomers + dimers (5%),c,d >99.89 monomers + dimers (10%)c,d
Gammagard Liquid Cohn-Oncley,i anion-exchange chromatography, SD, nanofiltration, ultrafiltration, low pH incubation
IV, SC Liquid ≥98 ≥95 monomers + dimers
Gammagard S/D 5%
Cohn-Oncley,i ultrafiltration, anion-exchange chromatography, SD
IV Lyophilized ≥90 96.4
Gammaked Cold ethanol fractionation, anion-exchange chromatography, caprylate chromatography purified, low pH incubation
IV, SC (PID only)
Liquid ≥98 100 monomers + dimersc,d
Gammaplex Cold ethanol fractionation, ion-exchange chromatography, SD, nanofiltration (20 nm), ultrafiltration, terminal low pH incubation
IV Liquid >99 ≥99 monomers + dimers
Gamunex-C Cold ethanol fractionation, anion-exchange chromatography, caprylate chromatography purified, low pH incubation
IV, SC (PID only)
Liquid ≥98 100 monomers + dimersc,d
Hizentra Cold ethanol fractionation, octanoic acid fractionation, anion-exchange chromatography, pH 4.0 incubation, depth filtration, nanofiltration (20 nm)
SC Liquid ≥98 ≥90 monomers + dimers
Octagam Cold ethanol fractionation, ultrafiltration, anion-exchange chromatography, SD, pH 4.0 incubation
IV Liquid ≥96 ≥90 monomers + dimers
Privigen Cold ethanol fractionation, octanoic acid fractionation, anion-exchange chromatography, pH 4.0 incubation, depth filtration, nanofiltration (20 nm)
IV Liquid ≥98 ≥98 monomers + dimers
INDEPENDENT LY DEVELOP ED BY M C M AH ON P UBL ISHIN G4

IgM Content Albumin PEGSodium Content Stabilizer Osmolality/Osmolarity Shelf Lifeh Reconstitution Time
NA NA NA NA Glycine NA 24 mo refrigerated
Not applicable (liquid solution)
Trace 0 0 0% water, 0.9% saline
5% sucrose In sterile water: 3%, 192 mOsm/kg; 6%, 384 mOsm/kg; 12%, 768 mOsm/kg In NS: 3%, 498 mOsm/kg; 6%, 690 mOsm/kg; 12%, 1,074 mOsm/kg
24 mo Several minutes
<2 mcg/mL (5%), <6 mcg/mL (10%)
<2 mcg/mL (5%), <5 mcg/mL (10%)
Not detectable
Trace (<3.2 mmol/L)
5% sorbitol (polyol)
327±4.5 mOsm/kg (5%)c,d 342±7.2 mOsm/kg (10%)c,d
24 mo RT Not applicable (liquid solution)
Trace NA Not detectable
Not detectable Glycine 240-300 mOsm/kg 36 mo refrigerated; 12 mo RT
Not applicable (liquid solution)
Trace <3 mg/mL <2 mg/mL 0.85% 2% glucose 636 mOsm/L (5%), 1,250 mOsm/L (10%)j
24 mo <5 min at RT; >20 min if cold
Trace <20 mcg/mL 0 Trace (<7 mEq/L)
Glycine 264±4 mOsm/kgc,d 36 mo refrigerated; 6 mo RT
Not applicable (liquid solution)
<0.02 mcg/mLk 0k 0k 30-50 mmol/L Sorbitol, glycine 480 mOsm/kg 24 mo Not applicable (liquid solution)
Trace <20 mcg/mL 0 Trace (<7 mEq/L)
Glycine 264±4 mOsm/kgc,d 36 mo refrigerated; 6 mo RT
Not applicable (liquid solution)
Trace ≤2% NA ≤10 mmol/L Proline 380 mOsm/kg 30 mo RT Not applicable (liquid solution)
≤0.1 mg/mL 0 0 0 10% maltosel 310-380 mOsm/kg 24 mo RT or refrigerated
Not applicable (liquid solution)
3 mg/L Trace 0 Trace Proline 240-440 mOsm/kg 36 mo RT Not applicable (liquid solution)
5IN D E PE N D E N TLY D E VE LOPE D BY MCMA HON PUBL ISHING

Key on page 8.
Table 3. Cost Considerations
Producta Supply Storage Distribution Return Policy Warranty Packaging or Labeling Enhancements
Bivigam 5, 10 g 2°C-8°C, 24 mo; do not freeze
NA NA Tamper-evident seal, label with integrated hanger, peel-off label, latex-free stopper
Carimune NF 3, 6, 12 g
≤30°C Wholesaler or direct
Shipping error; defective or damaged product; no out-of-date products
Tamper-evident seal, RSS bar code, peel-off label with lot number, expiration date
Flebogamma 5% DIF Flebogamma 10% DIF
2.5, 5, 10, 20 g (5%),5, 10, 20 g (10%)
2°C-25°C, 24 mo; do not freeze
Wholesaler or direct from Grifols USA (888) GRIFOLS
Shipping error; defective or damaged product; no out-of-date products
Tamper-evident seal with hologram, prior handling recognition, integral suspension band, laser-etched vials with UIN, bar code, peel-off label with product, lot number
Gammagard Liquid 1, 2.5, 5, 10, 20, 30 g
2°C-8°C, 36 mo; ≤25°C, 12 mo
Wholesaler or direct
No Tamper-evident cap, RSS bar code, peel-off label with lot number, expiration date
Gammagard S/D 5% 2.5, 5, 10 g
≤25°C; do not freeze
Wholesaler or direct
No Tamper-evident cap, peel-off label with lot number, expiration date
Gammaked 1, 2.5, 5, 10, 20 g
2°C-8°C, 36 mo; ≤25°C, 6 mo; do not freeze
Wholesaler Shipping error; defective or damaged product; no out-of-date products
Latex-free packaging, tamper-evident vials, peel-off label with lot number, expiration date
Gammaplex 5, 10 g 2°C-25°C, 24 mo; do not freeze
Wholesaler Shipping error; defective or damaged product; no out-of-date products
Latex-free, single-use vial, tamper-evident cap, peel-off label with lot number, expiration date
Gamunex-C 1, 2.5, 5, 10, 20 g
2°C-8°C, 36 mo; ≤25°C, 6 mo; do not freeze
Wholesaler or direct
Shipping error; defective or damaged product; no out-of-date products
Latex-free packaging, tamper-evident vials, peel-off label with lot number, expiration date
Hizentra 5, 10, 20 mL
≤25°C, 30 mo
Wholesaler or direct
Shipping error; defective or damaged product; no out-of-date products
Latex-free packaging, single-use tamper-evident vials, peel-off label with lot number, expiration date
Octagam 1, 2.5, 5, 10, 25 g
2°C-25°C, 24 mo; do not freeze
Wholesaler or direct
Shipping error; defective or damaged product; no out-of-date products
Tamper-evident, latex-free packaging, peel-off label with lot number, expiration date
Privigen 5, 10, 20 g
≤25°C, 36 mo
Wholesaler or direct
Shipping error; defective or damaged product; no out-of-date products
Latex-free, single-use vial, tamper-evident seal, RSS bar code, peel-off label with lot number, expiration date
INDEPENDENT LY DEVELOP ED BY M C M AH ON P UBL ISHIN G6

FOOTNOTES
a All agents are contraindicated for IgA defi ciency with antibodies to IgA.
b Varies with disease state, immune status, and age of the patient.
c Average of sample lots.
d Data on fi le at Grifols.
e As of Dec. 2012, Baxter has discontinued Gammagard S/D 5%; the low IgA product will remain available for patients with known reactions to IgA or IgA defi ciency with antibodies; special request only.
f DO NOT USE Gammaked or Gamunex-C subcutaneously for ITP or CIDP.
g With additional purifi cation steps added in 2010, current release lots contain <100 mcg/mL. Data on fi le at Octapharma.
h Under appropriate storage conditions.
i Cohn-Oncley is the original method of cold ethanol fractionation; Kistler-Nitschmann is the specifi c cold ethanol fraction ation method used by the manu facturer (CSL Behring).
j Limit infusion rate to <3.3 mg IgG/kg per minute (2 mL/kg/h) for 10% solutions.
k Data on fi le at Bio Products Laboratory.
l Maltose does not signifi cantly affect serum glucose or insulin levels and can be safely administered to diabetic patients. Certain BGMS falsely interpret maltose, icodextrin, galactose, and xylose as glucose and can provide falsely elevated glucose readings. If insulin is administered as a result of these readings, hypoglycemia can occur. The BGMS that use test strips containing GDH-PQQ and GDO can provide these false readings. See PI for full details.
m Some infusion rates were converted from
those listed in the prescribing information for consistency and reader convenience.
n Certain severe adverse drug reactions may be related to the rate of infusion. Slowing or stopping the infusion usually allows the symptoms to disappear promptly.
o Unless specifi c compatibility information is available, do not mix with other drugs or solutions.
p Patients at high risk for thromboembolic events include patients who are elderly, overweight, or immobilized; patients with a history of hypertension, cardiovascular disease, or thrombotic disorders, or those who are >65 or dehydrated.
q Log reduction factor values obtained through prescribing information; most are available on respective websites.
r Data on fi le at Octapharma.
Table 4. IVIG Administration Ratesm
IVIGaInitial Infusion Rate
Maintenance Infusion Rate
Maximum Infusion Raten Commentso
Bivigam 0.5 mg/kg/min Increase by 0.8 mg/kg/min every 20 min if tolerated up to 6 mg/kg/min
6 mg/kg/min No filter required; administer at the minimum infusion rate practical to patients >65 and those at risk for renal failure or thrombotic eventsp
Carimune NF 0.48 mL/kg/h 1-2 mL/kg/h 3 mL/kg/h No filter required; compatible with NaCl, D5W; increased risk for renal and thrombotic adverse effectsp
Flebogamma 5% DIF Flebogamma 10% DIF
0.6 mL/kg/h Increase gradually as tolerated to:6 mL/kg/h (5%), 4.8 mL/kg/h (10%)
6 mL/kg/h (5%), 4.8 mL/kg/h (10%)
No filter required; administer at the minimum infusion rate practical to patients >65 and those at risk for renal failure or thrombotic eventsp
Gammagard Liquid 0.5 mL/kg/h for 30 min
4 mL/kg/h; increase gradually as tolerated
5 mL/kg/h No filter required; compatible with D5W but not NaCl; patients at risk for renal dysfunction or thrombotic events shouldbe gradually titrated up to a more conservative maximum rate <2 mL/kg/hp
Gammagard S/D 5% 0.5 mL/kg/h for 30 min
1-2 mL/kg/h; increase rate every 15 min as tolerated
4 mL/kg/h (5%), 8 mL/kg/h (10%)
15-micron filter required and supplied with administration set; compatible with sterile water
Gammaked 0.6 mL/kg/h,1.2 mL/kg/h (CIDP)
4.8 mL/kg/h 4.8 mL/kg/h No filter required; avoid NaCl even in evacuated containers; administer at minimum infusion rate practical to patients >65 or at risk for renal or thrombotic eventsp
Gammaplex 0.6 mL/kg/h Increase gradually as tolerated every 15 min to: 4.8 mL/kg/h
4.8 mL/kg/h 15- to 20-micron in-line filter recommended; administer at minimum infusion rate practical to patients at risk for renal dysfunction or thrombotic eventsp
Gamunex-C 0.6 mL/kg/h, 1.2 mL/kg/h (CIDP)
4.8 mL/kg/h 4.8 mL/kg/h No filter required; do not dilute with NaCl, but NaCl flush is ok; incompatible with heparin (refer to full PI for details); administer at minimum infusion rate practical to patients >65 or at risk for renal or thrombotic eventsp
Octagam 0.6 mL/kg/h for 30 min
1.2 mL/kg/h for 30 min, then 2.4 mL/kg/h
<4 mL/kg/h No filter required or supplied; if an in-linefilter is used, the pore size should be 0.2-200 microns; for patients at risk for renal dysfunction or thrombotic events, administer at the minimum infusion rate practical, not to exceed 0.07 mL/kg/minp
Privigen 0.3 mL/kg/h As tolerated, up to maximum recommended rate
2.4 mL/kg/h (ITP), 4.8 mL/kg/h (PID)
No filter required; administer at minimum infusion rate practical to patients at risk for renal dysfunction or thrombotic eventsp
7IN D E PE N D E N TLY D E VE LOPE D BY MCMA HON PUBL ISHING
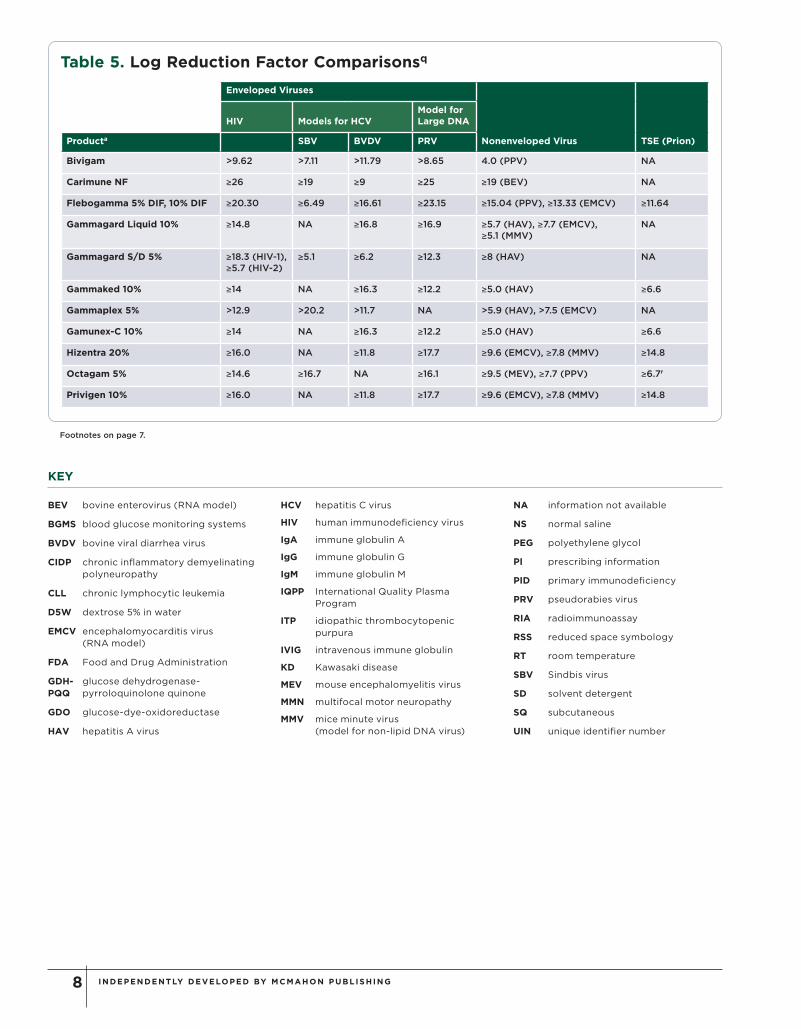
KEY
BEV bovine enterovirus (RNA model)
BGMS blood glucose monitoring systems
BVDV bovine viral diarrhea virus
CIDP chronic infl ammatory demyelinating polyneuropathy
CLL chronic lymphocytic leukemia
D5W dextrose 5% in water
EMCV encephalomyocarditis virus (RNA model)
FDA Food and Drug Administration
GDH- glucose dehydrogenase-PQQ pyrroloquinolone quinone
GDO glucose-dye-oxidoreductase
HAV hepatitis A virus
HCV hepatitis C virus
HIV human immunodefi ciency virus
IgA immune globulin A
IgG immune globulin G
IgM immune globulin M
IQPP International Quality Plasma Program
ITP idiopathic thrombocytopenic purpura
IVIG intravenous immune globulin
KD Kawasaki disease
MEV mouse encephalomyelitis virus
MMN multifocal motor neuropathy
MMV mice minute virus (model for non-lipid DNA virus)
NA information not available
NS normal saline
PEG polyethylene glycol
PI prescribing information
PID primary immunodefi ciency
PRV pseudorabies virus
RIA radioimmunoassay
RSS reduced space symbology
RT room temperature
SBV Sindbis virus
SD solvent detergent
SQ subcutaneous
UIN unique identifi er number
Footnotes on page 7.
Table 5. Log Reduction Factor Comparisonsq
Enveloped Viruses
Nonenveloped Virus TSE (Prion)
HIV Models for HCVModel for Large DNA
Producta SBV BVDV PRV
Bivigam >9.62 >7.11 >11.79 >8.65 4.0 (PPV) NA
Carimune NF ≥26 ≥19 ≥9 ≥25 ≥19 (BEV) NA
Flebogamma 5% DIF, 10% DIF ≥20.30 ≥6.49 ≥16.61 ≥23.15 ≥15.04 (PPV), ≥13.33 (EMCV) ≥11.64
Gammagard Liquid 10% ≥14.8 NA ≥16.8 ≥16.9 ≥5.7 (HAV), ≥7.7 (EMCV), ≥5.1 (MMV)
NA
Gammagard S/D 5% ≥18.3 (HIV-1), ≥5.7 (HIV-2)
≥5.1 ≥6.2 ≥12.3 ≥8 (HAV) NA
Gammaked 10% ≥14 NA ≥16.3 ≥12.2 ≥5.0 (HAV) ≥6.6
Gammaplex 5% >12.9 >20.2 >11.7 NA >5.9 (HAV), >7.5 (EMCV) NA
Gamunex-C 10% ≥14 NA ≥16.3 ≥12.2 ≥5.0 (HAV) ≥6.6
Hizentra 20% ≥16.0 NA ≥11.8 ≥17.7 ≥9.6 (EMCV), ≥7.8 (MMV) ≥14.8
Octagam 5% ≥14.6 ≥16.7 NA ≥16.1 ≥9.5 (MEV), ≥7.7 (PPV) ≥6.7r
Privigen 10% ≥16.0 NA ≥11.8 ≥17.7 ≥9.6 (EMCV), ≥7.8 (MMV) ≥14.8
INDEPENDENT LY DEVELOP ED BY M C M AH ON P UBL ISHIN G8