the knee: clinical evaluation nick iannuzzi, md november 28 th - 2011
TRANSCRIPT

The Knee: Clinical Evaluation
Nick Iannuzzi, MDNovember 28th - 2011

Outline
• Anatomy• History• Differential Diagnoses
– Structured Evaluation
• Practice Physical Exam
2

The Knee
3
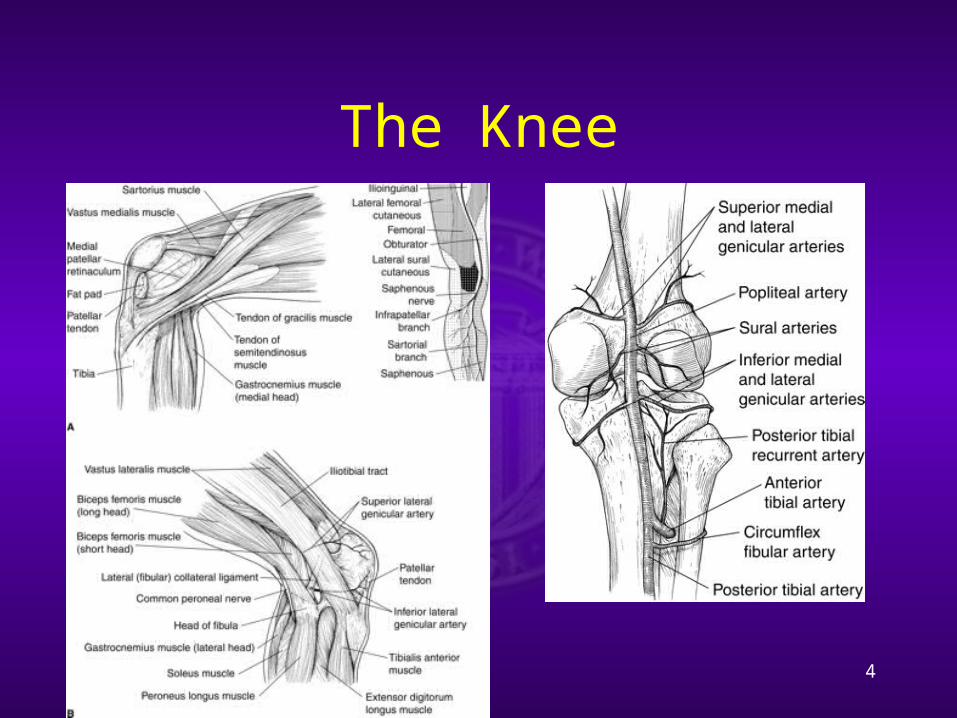
The Knee
4

Exam Maneuvers
• Anterior drawer test• Lachman test• Pivot shift test• Posterior sag sign• Posterior drawer test• Quadriceps active test• Valgus stress test• Varus stress test• Patellofemoral grind test• Apprehension test• Joint line tenderness • McMurray Test• Apley grind test• Bounce home test
5
WHAT?
WHY?
WHEN?

History
Timing? Mechanism? Pain description? Swelling? Mechanical Symptoms? Instability?
Baker et al 1983; Hughston et al 1985, Laprade et al 1997

Differential Diagnoses
• Anterior Knee pain
• Extensor mechanism rupture/failure
• Patellofemoral pain• Patellofemoral
instability• Plica• Arthritis
7

Differential Diagnoses
• Lateral knee pain • Lateral meniscal tear• IT band friction
syndrome• Segond fracture• LCL/PLC tear• Gastrocnemius
strain/tear• Arthritis
8

Differential Diagnoses
• Medial Knee Pain • Medial meniscus tear
• MCL strain/tear• Hamstring strain/tear• Pes anserine bursitis• MPFL disruption• Arthritis
9

Differential Diagnoses
• Posterior knee pain
• Popliteal/Baker’s cyst (meniscal tear)
• Tumors• Claudication• Radiculopathy
10

Differential Diagnosis
• Locked knee • Meniscal tear• OCD lesion
(femur/patella)• Tibial spine
avulsion• Osteochondroma
(tendons incarcerated)
11

Rule #1
Always compare to the other Knee!!
INTERNAL CONTROL

EXAM-Getting Started
Inspection/Palpation-Effusion?-Tender?-Skin Breaks?
Alignment-Varus/Valgus?-Dislocated?
Range of Motion (0-130+) -Mechanical Block-Contractures-Crepitus
“Seek Out Disease, Don’t Hope For Health”-anonymous
WHAT DO YOU SEE??

EXAM-Overview
Inspection/PalpationAlignmentRange of Motion (0-130+)
Tracking
Extensor Mechanism
Stability-Provocative Tests
GAIT Analysis

ACL – Anterior Drawer
15
Knee at 90 degrees
Anteriorly translate the tibia with thumbs palpating relationship between femoral condyles and tibia
Sensitivity 22-41% (acute injuries); 50-95% (chronic injuries)

ACL - Lachman Exam
Position: -Supine -Knee flexed 0-15 deg
Force Applied: Anterior
Grading Scale:Grade I: 1-5mmGrade II: 6-10mmGrade III: >10mm
Sens 80-99%, Spec 95%
Gross Anterior Displacement: ACL+PLC
Hamstrings RelaxedFeel for Endpoint

ACL - Pivot Shift
Position: -Supine -Knee ExtensionFlexion
Force: Valgus, IR Pathomechanics:
-SUBLUXEDReduced -ITT reduces tibia @ 20-30 flexion
Pathoanatomy: -Positive: Glide, Shift, Gross
Sens 35-99%, Spec 98%
*Key Testable Exam Finding

PCL – Posterior Sag Sign
• Position supine– Hip flexed 45 degrees– Knee flexed 90
degrees
• Normally, tib plateau extends 1cm beyond femoral condyles
• Sens 79%, Spec 100%
18

PCL - Posterior Drawer
Position: -Supine -Knee flexed 90 deg
Force Applied: Posterior Pathomechanics:
-Post translation tibial plateau-Tibial Plat comp to Femoral Condyle
Pathoanatomy:
-G I/IIPCL injury -G IIIPCL + PLC injury
Sens 50-100%, Spec 99%
Negative in all normal knees, Cooper 1991
Gollehon et al 1987, Grood et al 1988, Noyes 1996
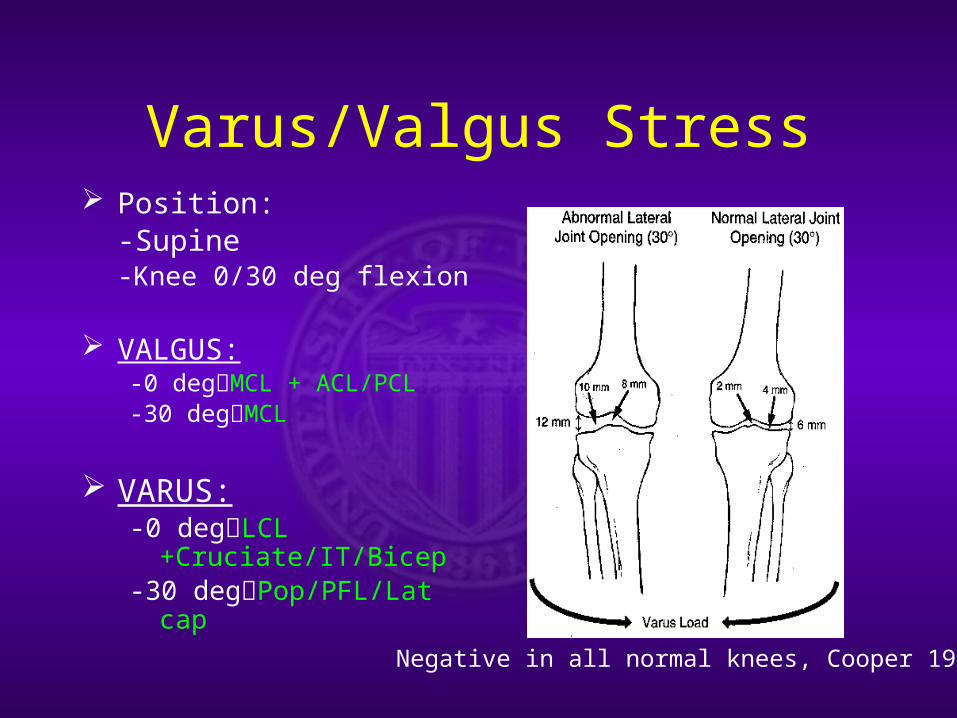
Varus/Valgus Stress Position:
-Supine-Knee 0/30 deg flexion
VALGUS:-0 degMCL + ACL/PCL-30 degMCL
VARUS:-0 degLCL
+Cruciate/IT/Bicep-30 degPop/PFL/Lat cap
Negative in all normal knees, Cooper 1991

PLC/PCL - ER stress (Dial) Position:
-Prone -Hip Neutral (0 deg flexion)-Knee Flexed 30/90
Force: ER Pathomechanics:
-Tibial ER on Femur
Pathoanatomy: >10 deg of Asymmetry 30 degPLC Injury90 degPLC + PCL Injury
TMA-Transmalleolar AxisNegative in all normal knees, Cooper 1991

PLC/PCL - External Rotation Recurvatum
Position:-Supine-Hip neutral (0 deg flexion)-Knee extended
Force: Lift FF anterior Pathomechanics:
-Knee hyperextends-External rotation-Varus
Pathoanatomy:-PLC injury- ±PCL/ACL tear
Negative in all normal knees, Cooper 1991

Meniscus – Joint Line Tenderness
• Can palpate medial and lateral joint lines of tibia at ~90 degrees flexion
• Medial meniscus more prominent with IR
• Lateral meniscus more prominent with ER
• Sens 55-85%, Spec 30-67%
23
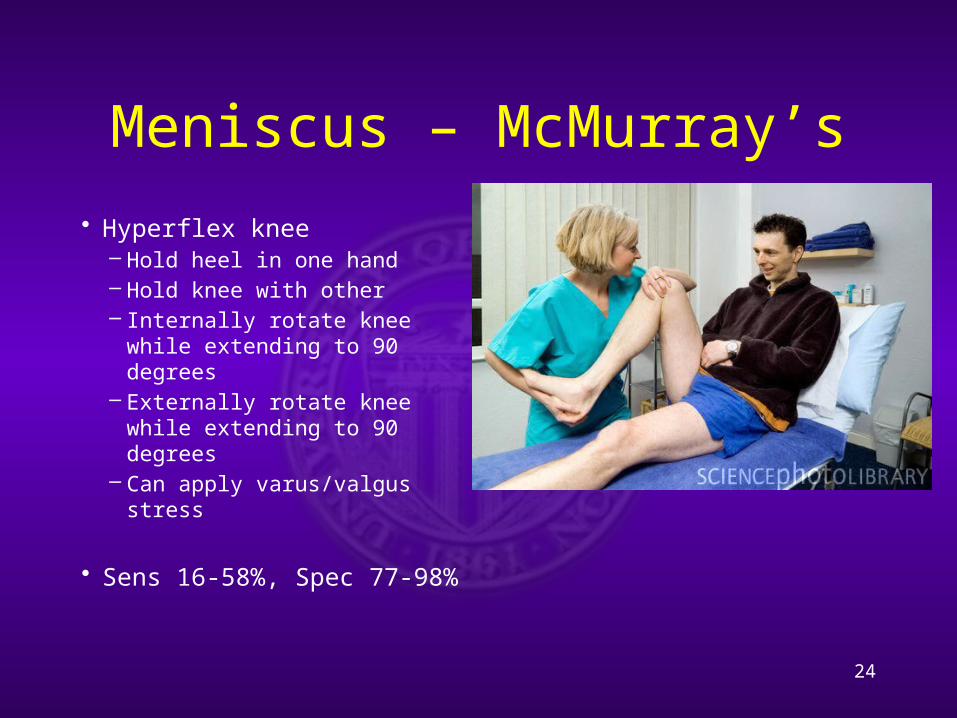
Meniscus – McMurray’s
• Hyperflex knee– Hold heel in one hand– Hold knee with other– Internally rotate knee while
extending to 90 degrees– Externally rotate knee while
extending to 90 degrees– Can apply varus/valgus
stress
• Sens 16-58%, Spec 77-98%
24

Patellofemoral Instability – Q angle
• Angle formed by – Line drawn from
ASIS to center of patella
– Line drawn from center of patella to tibial tubercle
– Normal is 10-15 deg
25
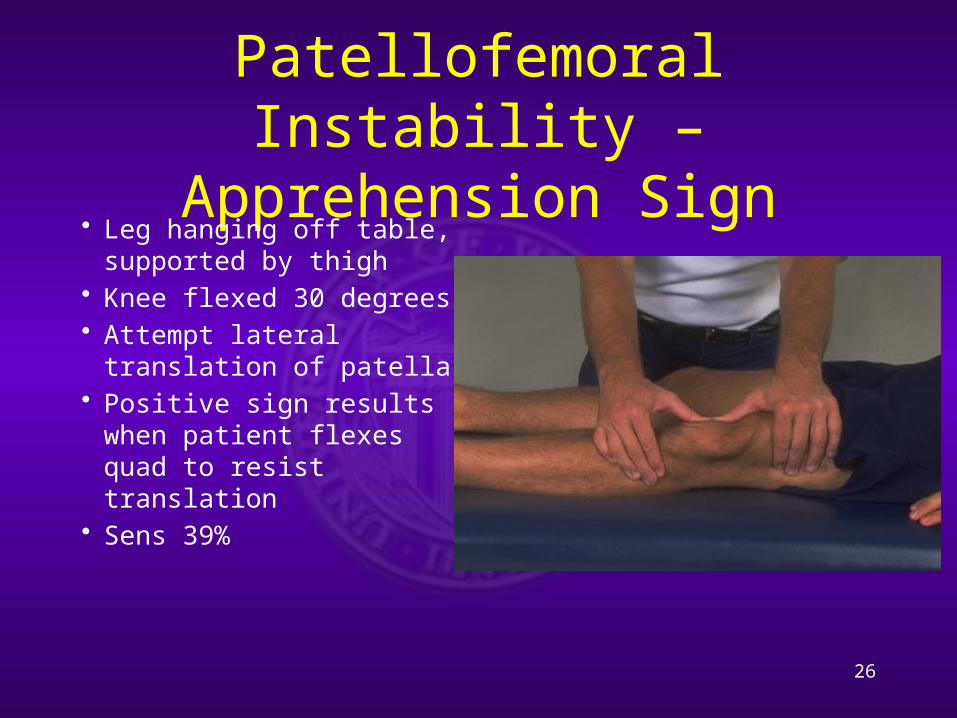
Patellofemoral Instability – Apprehension Sign
• Leg hanging off table, supported by thigh
• Knee flexed 30 degrees• Attempt lateral
translation of patella • Positive sign results
when patient flexes quad to resist translation
• Sens 39%
26
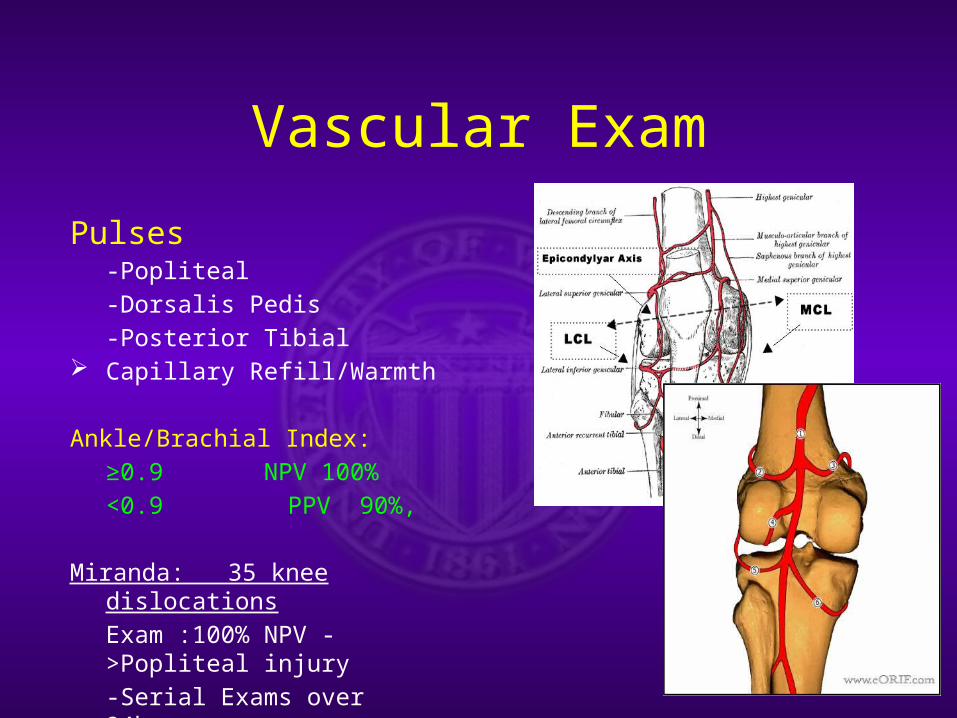
Vascular Exam
Pulses-Popliteal
-Dorsalis Pedis
-Posterior Tibial Capillary Refill/Warmth
Ankle/Brachial Index:
≥0.9 NPV 100%
<0.9 PPV 90%,
Miranda: 35 knee dislocations
Exam :100% NPV ->Popliteal injury
-Serial Exams over 24hrs
POSITIVE: Angiography or OR!!

KNEE Emergencies?
INFECTION
DISLOCATION
VASCULAR INJURY
-Dislocations
-Distal femur/Prox Tibia
Most knee complaints are NOT emergencies!!

Surgical Problems
Pathology Finding
ACL Lachmans
Meniscus McMurray’s
Arthritis Hx/Xray
Infection Pain/Effusion/Labs
Vascular ABI/Hard Signs
CONCLUSIONS
HISTORY
EXAMINE NL KNEE
R/O EMERGENCY
REPETITION IS KEY
PHONE A FRIEND
30IT IS ONLY A VIRTUE IF YOU’RE NOT A SCREWUP!