the little yellow - chromosome · the little yellow book aguidetorarechromosomedisorders by dr...
TRANSCRIPT

TheLittle Yellow
Book
A Guide to Rare Chromosome Disordersby
Dr Beverly Searle BSC(HONS) PHD CBIOL MSB andProfessor Maj Hultén PHD MD FRCPATH
11229:8876 17/6/13 15:12 Page ii

The Little Yellow Book, Vol 1
Published by The Rare Chromosome Disorder Support Group
Rare Chromosome Disorder Support GroupRegistered Charity Number 1110661Registered in England and Wales Company Number 5460413Registered Office:Valiant House, 3 Grange Mills, Weir Road, London SW12 0NE
Designed and printed by GREENGilbert
Written by Dr Beverly Searle BSC(HONS) PHD CBIOL MSBand edited by Professor Maj Hultén PHD MD FRCPATH
Copyright © Unique – Rare Chromosome Disorder Support Group2013
All rights reserved. No part of this publication may be reproduced inany form whatsoever, stored in any retrieval system or transmitted inany form or by any means without prior permission in writing fromthe publisher.
ISBN 0-9541253-0-4
11229:8876 17/6/13 15:12 Page iii
Dear Parent,
Welcome to Unique. We hope that through membershipof the group you will feel supported in caring for yourvery special child who has a rare chromosomal disorder.
Perhaps your child is still a baby or has passed thebaby stage but has only just been diagnosed. Howeverold your child, discovering that he or she has a rarechromosomal disorder can come as a great shock. Youmight be feeling a mixture of emotions; sadness,confusion, numbness, anger, guilt, “why me?”, isolationor bewilderment. Perhaps your reaction to your childhas surprised you. You might be feeling overwhelmed atyour lack of knowledge about your child’s condition ordespairing that your child’s condition hasn’t even got aproper name. Whatever your feelings, rest assured thatother members of Unique, including the group’sorganisers, have experienced at least some, if not all, ofthem. We know how much it can help to talk to peoplewho understand what you are going through and evenwhat you are talking about. You are not alone.
We have prepared this booklet to give you a basicunderstanding of chromosomes and rare chromosomedisorders and to tell you a little bit about ourselves andthe group. Please feel free to use the group’s services. Ifyou have a question, we will do our very best to answerit or point you in the direction of someone who can.
Very best wishes,
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
1
welcome to unique
11229:8876 17/6/13 15:12 Page 1

history of unique....................................................................................................3
the unique team.......................................................................................................5
consequences of rare chromosomal disorders..........15
what can unique do to help?........................................................... 18
all about chromosomes and genes............................................20Cells, Chromosomes, DNA and Genes
Chromosome and DNA Analysis
Symbols used in Karyotypes and Molecular
Cytogenetics
rare chromosomal disorders..............................................................33NUMERICAL DISORDERS
Polyploidy
Aneuploidy
STRUCTURAL DISORDERS
Translocations
Balanced Reciprocal Translocations and
Unbalanced Translocations
Robertsonian Translocations
Insertions
Deletions and microdeletions
Rings
Duplications and microduplications
Inversions
Isochromosomes and sSMCs
Uniparental disomy (UPD)
further reading and information................................................40
donations, fundraising, grants and covenants.......41
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
2
contents
11229:8876 17/6/13 15:12 Page 2

Unique has been a source of mutual support and self-help to families of children with a rare chromosomedisorder since it was founded by Edna Knight MBEin the UK in 1984 as the Trisomy 9 Support Group.
In 1989, with the support of the In Touch Trust andContact a Family, the group expanded to includefamilies whose children have any rare chromosomedisorder. In 1993 the group was granted CharityStatus and the new logo Unique was adopted.
In 1996, Unique launched its comprehensivecomputerised database to collect information aboutall aspects of how specific rare chromosomedisorders affect individual members over a lifetime.In January 1999, Unique was awarded a 3 year grantby the National Lottery Charities Board to fund afull-time Development Officer and a part-timeFamily Support Officer. In April 1999, the group’sfirst website was launched and membership stood atjust 1192 families.
In 2003, other short-term grants allowed the groupto employ a full-time Information Officer to researchand produce family-friendly information guides onspecific rare chromosome disorders. At the sametime, a part-time Assistant Information Officer wasemployed to produce information on topics such asbehaviour, communication, education and so on. Apart-time Finance and Fundraising Officer joined usin 2004.
By early 2013, group membership had risen steeplyto over 10,000 families, representing over 14,000individuals with a rare chromosome disorder in over90 countries worldwide. With at least 100 newfamilies now joining us each month, the rate of
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
3
our history
11229:8876 17/6/13 15:12 Page 3

growth of our membership shows no signs ofslowing down! As more sophisticated methods ofanalysing people’s chromosomes and DNA, likemicroarrays and next generation sequencing, manymore previously undiagnosed people will bereceiving a diagnosis of a rare genetic or genomicdisorder. Consequently we expect our membershipto continue to rise rapidly for the foreseeable future.Of necessity, our team has had to grow to keep pacewith the huge increase in our workload.
Over these many years, we have worked very hard toraise awareness of Unique among families andindividuals affected by rare chromosome disorders.We have also been spreading awareness of rarechromosome disorders to professionals and to thegeneral public so that they too have an appreciationof the extraordinary challenges our members face.However, securing grants to pay for this work isbecoming much more difficult with fewer fundingopportunities available and many more charitiescompeting for the same grants. Please help us withdonations and fundraising so that we can continueour essential work.
Unique has adopted and works to an equalopportunities policy and is registered under the DataProtection Act (registration number Z9206140).
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
4
11229:8876 17/6/13 15:12 Page 4

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
5
Unique has a voluntary Trustee Board comprising amajority of parents who, along with other Trustees,use their wide and varied professional expertise toensure the group is run to the highest standards. TheBoard supports the group’s officers who carry out theday to day frontline work.
Edna Knight MBE– The Group’s Founder,Life President and Trustee
� I helped to establish Unique from the beginning. I havefour daughters, two with a duplication of part of theshort arm of chromosome 9 - Wendy (17.7.65) and Julie(26.10.71). My youngest daughter Claire (6.8.82) has abalanced insertional translocation like myself, whilstmy second daughter Linda has normal chromosomes.Wendy and Julie are doing well after very slow starts.They have reading skills and are able to travel alone onbuses locally. Wendy attends a sheltered developmentcentre and goes out to large local companies andcolleges for work experience. Julie works with supportfrom the Shaw Trust. I am pleased with their progress sofar and they are still progressing and learning to do newthings. Their development, skills and achievements havecontinued to expand well into their 20s, 30s and 40s.
As a Trustee, I keep a watchful eye on the progress ofUnique and liaise with the staff team and fellow Trustees,without whom the group could not run. With theemployment of Beverly Searle as Chief Executive Officer,a considerable element of the burden of running the groupwas lifted from me. I am here to help with the smoothrunning of the group and to encourage others. There are agreat many diverse activities within Unique such ascoordinating the compilation and dispatch of the thrice-yearly newsletter, collating information for the regular
the unique team
Claire, Edna, Linda,Wendy and Julie.
11229:8876 17/6/13 15:12 Page 5
conference and working with many other members onvarious tasks. Most importantly though I am here both toensure that the organisation keeps to its own guidelinesand to run a group that is both informative and sensitiveto the needs of parents.�
Beverly Searle– Chief Executive Officer
� I was appointed to the post of Development Officer inApril 1999 and in 2003 I was made DevelopmentDirector. More recently I became Chief Executive Officer. Iworked for Unique in a voluntary capacity for some yearsas Database coordinator and was a member of themanagement committee from the early 1990’s. I joined thegroup shortly after the birth of my daughter, Jenny, inFebruary 1990. Jenny had a complete deletion of the shortarm of chromosome 18; she was profoundly learning andphysically disabled and had complex health needs. Jenny’selder brother Jonathan has a mild heart defect, althoughhis chromosomes are normal. In 2011, Jonathan qualifiedas a medical doctor.
Before I had my children, I worked for many years as aresearch scientist, being awarded the degree of PhD for myresearch into aspects of the biochemistry and genetics ofyeast. What a coincidence then that one of my childrenshould be born with a chromosomal defect! After thechildren were born, I worked part time as a freelanceabstractor of current literature for apharmacological/medical publishing company.
After Jenny’s birth, I devoted a great deal of my time andenergy to promoting the needs of families with disabledchildren. As one time Vice-Chair of Action for Carers(Surrey) and a founder member of the East Surrey Carer’sSupport Association, I have had a lot of experienceworking with Social Services and Health Authorityrepresentatives. I also served for four years as a Non-Executive Director of a NHS Trust for People withLearning Disabilities.
Most enjoyably, though, I have been involved in therunning of Unique. My husband Trevor is a computersoftware specialist and together we developed Unique’smembers’ database and the group’s website.
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
6
Trevor, Beverly and Jenny.
11229:8876 17/6/13 15:12 Page 6
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
7
When I first had Jenny, I was very upset and reallythought that was the end of any decent life for us. It wasdifficult at times but I can honestly say that in most ways,my life has changed immeasurably for the better and Ihave met some wonderful people because of Jenny. As forJenny, despite her disabilities, she was a delightful youngwoman and her sweet nature shone through. Sadly we losther when she was 21 years old but felt very lucky andprivileged to have had her in our lives.
I am responsible to the Trustees for the day to dayrunning of Unique and development of our services; Imanage our staff team, respond to enquiries from newfamilies and professionals and aim to raise the profile ofrare chromosome disorders and the work of Unique.�
Prisca Middlemiss– Senior Information Officer
�One of my earliest childhood memories is of my fathercoming home from work and announcing that thenumber of human chromosomes had at last been correctlycounted. A Swede, Albert Levan, and an Indonesian,Joe-Hin Tjio, had overturned the prevailing wisdom thathumans, like chimpanzees and gorillas, had 24 pairs ofchromosomes. Using improved techniques, as Maj Hulténso charmingly recounts, these scientists had shown thatwe actually have 23 pairs. As an academic physiologist,my father thought the momentous genetic discoveries ofthe 1950s would interest his three young children.
He was right, but it wasn’t for another thirty years thatthese facts were to take on a personal significance for myhusband Nigel and myself, when our second son Toby wasborn with a variety of medical problems. Sadly, Tobynever recovered from surgery the night after his birth torepair his diaphragmatic hernia. Before he died, bloodsamples were sent for analysis and within weeks welearned that the underlying cause of his multipleanomalies was a partial trisomy of chromosome 22.
Stepwise investigations then revealed that not only did Icarry an 11;22 balanced translocation but my brotherFabian and my sister Ann had exactly the samechromosomal re-arrangement. As my mother had normalchromosomes, the conclusion that the translocation was
Top: Dad(Professor JohnMills); middle:Fabian, Prisca,Ann; bottom:
Sophie.
11229:8876 17/6/13 15:12 Page 7

passed on by my father was inescapable. He was nolonger alive to discover this but would, I think, have beenintrigued and, given my parents’ apparently problem-freereproductive history, mildly surprised.
Amniocentesis in my next pregnancy showed the samebalanced 11;22 translocation, so since the birth of ourdaughter Sophie in 1983 it now spans three generations.
Professionally, I have worked in medical journalism formost of my life, starting out as editor of the then BritishDiabetic Association’s journal Balance, and latercontributing to a range of medical and consumerpublications, as well as writing three child healthhandbooks.
Working as Unique’s Senior Information Officer offers awonderful opportunity for the personal and professionalstrands of my life to intertwine. It is very exciting indeedto come on board for the launch of Unique’s innovativeproject to compile and publish information on the rareand, in some cases, very rare chromosome disorders thataffect each of us.�
Marion Mitchell– Family Support Officer
� I joined the group in May 1995, just after my son Robertwas diagnosed with an inverted duplication ofchromosome 15 at the age of one. In 1996 I becameInformation Officer for the group and in 1999Administrative Officer. In June 2003 I became FamilySupport Officer. I send out all of the new memberswelcome packs and I manage our social networkinggroups on facebook. I coordinate our local contacts’around the world and since 1996/7 I have organised/co-organised Unique’s past conference weekends. I alsoresearch and help write Unique’s parents’ guides onpractical matters. As area representative for West Sussex,I help to raise the profile of Unique in the county.
In 2012 Robert was re-diagnosed with two extra markerchromosomes 15 including partial octasomy (8 copies) ofthe segment 15q13q14. In 2012 Robert also became anadult and we have been undergoing transition from childto adult services for the past year. In 2013 he is about to
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
8
Marion, Robert and Steve.
11229:8876 17/6/13 15:12 Page 8
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
9
leave his school of 17 years and move into adult daycareservices.
Rob has profound learning difficulties, is non-verbal, hasepilepsy and eczema.
I am married to Steve and Rob is our only child together. Ialso have two step children and two step grandchildren.
My working background involved years of retailexperience including retail management and customerservices.�
Jenny Knight – Finance Officer
� I was appointed to the post of Finance Officer forUnique in July 2011 having been a member of Uniquefor many years. I have one son who will be 29 this yearand twin boys, George and Henry, who will be 18 thisyear. George possibly has a rare chromosome disorderalthough we don’t have a chromosome disorderdiagnosis as yet. He has been diagnosed with WorsterDrought Syndrome and has a very severe speech andlanguage disorder. We have recently joined the“Deciphering Developmental Disorders” study whichwill hopefully provide a further diagnosis forGeorge.�
Craig Mitchell– Chief Operating Officer
�My first contact with Unique was in late 2003 when mydaughter Ella was 9 months old and diagnosed with a 6p25 deletion. She was our first born and this was theculmination of a difficult period during which she hadsuffered infantile spasms (a severe form of epilepsy) andwe had spent some time with her in Guy’s Hospital inLondon. Very few of the doctors had seen infantile spasmsand after a number of fruitless consultations my wifeGemma and I resorted to videoing the spasms. This was adifficult thing to have to do but it helped in getting adiagnosis and appropriate treatment for her.
After it was diagnosed the doctors were great but knewvery little about Ella’s rare chromosome disorder and wewere referred to a geneticist who in turn told us aboutUnique. Having trawled the internet and read lots of hard
Jenny with sons Henry and George.
Craig, Ella and Holly.
11229:8876 17/6/13 15:12 Page 9

to understand and sometimes quite scary medicalliterature, we found the information from Unique to beboth accessible and straightforward. We realisedimmediately that we had a source of support andinformation and that there were lots of other families outthere struggling to come to terms with a diagnosis butdefinitely not alone.
Through our membership of Unique we have become verygood friends with a family who have a daughter with acompletely different chromosome disorder to Ella’s. Theyknow and understand only too well the challenges we faceand vice versa. I think that’s one of the keys with Unique:families who may be facing quite different challenges areable to come together and provide mutual help andsupport.
Ella now attends a special school near our home in Kentas she has learning difficulties with autism. She wearsglasses and has grommets fitted in her ears, hashypermobile joins and some mobility issues as she has apronated right ankle and very flat feet. She also sufferswith a skin condition on her legs called morphoea. Ellahas very little speech and is learning to communicate inher own way (using some Makaton signs) although shecan become very frustrated and quite angry. Despite thesechallenges she is an absolute joy, full of life and (usually)very happy.
On Christmas day 2007, Gemma gave birth to Ella’s sisterHolly (Holly has normal chromosomes) and though thismeant some upheaval for Ella, her initial indifference toher sister is now passing and she is learning to share herspace. In fact, she often listens to Holly more than to herparents!
I joined Unique in May 2008 as the charity’s firstOperations Manager and am currently Chief OperatingOfficer. My role involves supporting the specialist servicesteam, growing the organisation’s capacity to meet theneeds of an increasing membership and perhaps mostimportantly, overseeing our fundraising efforts. Sincejoining I’ve been amazed at how much is done by such asmall team and on a relative shoestring! I am veryfortunate to be able to work in an organisation which I
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
10
11229:8876 17/6/13 15:12 Page 10

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
11
not only believe in strongly but one which was such a helpto my own family.�
Sarah Wynn – Information Officer
� For many years I have been working as a medicalresearch scientist. In 1999 I was awarded a PhD inGenetics from Imperial College, the subject of my thesisbeing Down’s syndrome. I then spent a number of yearsworking as a scientist at the University of Hong Kong. Itwas while living and working in Hong Kong that Isuffered three consecutive miscarriages. Subsequentinvestigations to try to determine the cause revealed thatmy husband, Marc, carries a 5;7 balanced translocation.
In my quest for more information I discovered Unique andwe became members in the summer of 2004. Meanwhile,we had returned to live in the UK and I took up a newresearch position at the National Institute of MedicalResearch. I became pregnant again. After the initialnervousness, the pregnancy progressed well and wedecided to undergo chorionic villus sampling (CVS) todetermine the baby’s chromosome make-up. The resultsrevealed that Daisy also carries the same balancedchromosomal re-arrangement. We have since had a seconddaughter, Martha, who has normal chromosomes, andafter three more miscarriages a son, Isaac who has alsoinherited his father’s translocation.
Since 2007 I have been one of Unique’s informationofficers which involves publishing information guides torare chromosome disorders, and getting involved withresearch projects and raising the profile of Unique withresearchers and healthcare professionals. I also helpBeverly with the many enquiries from new families andprofessionals.
Maj Hultén – Chief Medical Advisor
�When I was little I lived in a small town in southernSweden. Every Sunday I saw marches of unusual lookingchildren walking hand in hand in the street outside ourhouse. My mother told me that they lived all together,because their parents had found it difficult to look afterthem. She also said that sometimes it could happen that
Sarah and Daisy.
11229:8876 17/6/13 15:12 Page 11

there was more than one child in a family with similarproblems.
I was hooked and years later decided to study Psychologyand Education at the University of Stockholm to learnmore about what could cause such problems – and howthey could be overcome. I took my exams, but wasdisappointed not finding any real answers to myquestions. Genetics I thought then might be a better bet.This also turned out to be frustrating, not least becauseformalities at the time dictated that courses in Geneticswere only open to students who had spent several yearsstudying Zoology and Botany – and who had also passedan entrance exam. Luckily I managed to strike a dealwith the Professor to the effect that if against all odds, Iwould be ranking no 1 in the Genetics Entrance Exam, hewould accept me regardless. This was hard work, but itdid work.
I found the Genetics course fascinating, yet disappointing,primarily because the curriculum mostly concernedbacteria, fruitflies and plants – and statistics, hardlyanything that could explain learning disabilities inchildren.
In my final year I had to do a special project, taking acouple of months. I was offered a number of projects (17in total) pushing around and counting different types offruitflies under a dissecting microscope. I declined themall, and said I should like to look at human chromosomes.This turned out to be a decisive turning point. It wasarranged for me to be supervised by a Professor Levan,who had been looking at mouse chromosomes,particularly in tumours. (As it happened this was in thesame small town in southern Sweden, where I had grownup).
I was given a project, studying the effects of radiationtreatment on mouse tumours…
But, lo and behold, I later found out that work on humanchromosomes was actually going on in the sameDepartment! The night before Christmas Eve in 1955 Iwas offered to peer down the microscope to look atbeautiful spreads of human chromosomes. This was thefirst time human chromosomes could be correctly countedand proper photographs taken.
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
12
Maj Hultén.
11229:8876 17/6/13 15:12 Page 12

It is a truism to say that I can remember it as if it wasyesterday – the stinging smell of the chromosome stain(Acetic Orcein) blending together with that of Turkishcoffee made by the visiting scientist, Joe Hin Tjio, whohad produced the chromosome preparations, squashing thecells between two pieces of glass – making his thumbsbright red also. Sitting on a high laboratory stool I wasdrumming my legs against the bench in excitement, whilepointing out to Dr Tjio that it could now be possible tofind out if some people with learning disabilities mayhave chromosome abnormalities such as trisomies,monosomies, translocations, insertions, inversions, rings,duplications and deletions, previously only seen infruitflies and plants, as if he would not have realised thisby himself.
I decided on the spot to study medicine, hoping thatMedical Genetics would one day become a discipline,where the study of chromosomes would be very important.This was now more than 40 years ago. I have workedwith chromosomes and genetic counselling ever since. Oneof the challenges I faced was to convince Edna Knight totake me on board as Medical Advisor to the RareChromosome Disorder Support Group. I am glad sheeventually did – around 15 years ago. My vision is thatUnique is renowned not only for the help the groupprovides to families in the UK and many other countriesworldwide but also for the powerful stimulus it hasprovided for the formation of similar groups in many,many other countries.
I should add that my brother has had a child with aChromosome Disorder, a deletion of the long arm ofchromosome 8. He and my sister-in-law have not had thebenefit of a Support Group. My vision is that Unique oneday will be renowned not only for the help the Groupprovides to families in the UK (and some other countriesalready) but also for the powerful stimulus it has meantfor the creation of similar Groups in many, many othercountries. As far as I am aware Rare ChromosomeDisorders are equally common among all races and alldifferent parts of the world. So, in this respect we are notUnique! I also nourish a dream that never again should adoctor turn around to parents saying – ‘Your child has gota very rare Chromosome Disorder. I am afraid I know
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
13
11229:8876 17/6/13 15:12 Page 13

nothing about it!’ As I am sure many parents have, I havefound this very off putting. It should of course not havehappened in the past, and let us hope the mission ofUnique will imply this type of ignorance becomesincreasingly rare in the future.�
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
14
11229:8876 17/6/13 15:12 Page 14

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
15
The effects of rare chromosome disorders can bevery varied. The vast majority of carriers of balancedrearrangements will have no symptoms but mighthave problems in reproduction. Where there hasbeen a loss or gain of chromosome material, thesymptoms arising might include a combination ofphysical problems, health problems, learningdifficulties and/or challenging behaviour. Thecombination and severity of effects occurring verymuch depend upon which parts of whichchromosomes are involved. The outcome for theaffected children can be quite different. In general,loss of a segment of a chromosome is more seriousthan the presence of an extra copy of the samesegment. Defects of chromosomes 1 to 22 are usuallyfar more serious than those of the sex chromosomesX and Y. It is very important that a child’schromosome disorder is specified in as much detailas possible. The description of a person’schromosome make-up is called their GENOTYPE.
Sometimes children with the same genotype willshow similar problems. However, even children withthe same genotype can differ in some or even nearlyall of their problems. Why should this be? Thegenotype as seen under a light microscope is called aKARYOTYPE and only gives us the “big” picture.New technologies like array CGH analysis and nextgeneration sequencing (NGS) allow us to look atchromosome and DNA changes at a much greatermagnification and often show us that the actualbreakpoints in the chromosome might be manygenes apart. But even that does not explain all thedifferences. Even brothers and sisters with the samegenotype inherited as the result of a parent’s
consequences ofrare chromosome disorders
11229:8876 17/6/13 15:12 Page 15

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
16
chromosome rearrangement can still developdifferently. There are many other factors besides aperson's chromosome disorder that affect how theydevelop, for example, the unique mixture of geneson their other normal chromosomes, theenvironment in which they are raised and so forth.Sometimes a particular chromosome disorder willgive a similar pattern of problems. If enoughchildren are born with this similar pattern, then thiscan be called a SYNDROME.
There are also some general characteristics of rarechromosomal disorders that occur in the majority ofaffected people to varying degrees. For instance,most people with any loss or gain of material fromchromosomes 1 to 22 will have some degree oflearning disability and developmental delay. This isbecause there are many genes located across all thesechromosomes that code for normal development ofthe brain. Defects in any one of them could have aharmful effect on normal development.
You might have been dismayed if the doctors andgeneticists that you have consulted about yourchild's chromosome disorder are not able to give youa definite idea of how your child will be affected inthe long term, especially if the disorder isparticularly rare. You might think that the doctorssimply do not want to help or can’t be bothered tofind out. Nothing could be further from the truth.The point is that, like any other child, your child isUNIQUE and while there might have been othersimilar chromosome disorders reported in themedical literature, it does not mean to say that yourchild will develop in the same way. Like any of us,doctors do not have a crystal ball to look into thefuture. They might only be able to give you an ideaof the possible problems that might arise.
You, or your family and friends, might have askedwhat can be done to “cure” a chromosome disorderin your baby or child. Nothing can be done about
11229:8876 17/6/13 15:13 Page 16

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
17
the actual chromosome defect because every singleone of the billions of affected cells would have tohave the missing chromosome material and all thegenes involved added or extra chromosome materialtaken away and this is not possible yet with today’stechnology. However, symptoms caused by thechromosome disorder can be treated as they ariseand the best environment given in order for thechild with the chromosome disorder to reach theirfull potential.
11229:8876 17/6/13 15:13 Page 17

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
18
Having a child with a rare chromosome disorder canbe a huge shock and can stir up a whole range ofemotions and a great desire to learn more about yourchild’s disorder. All of us who help run the grouphave been through these experiences and know howyou are feeling. Most parents’ first reaction, quiteunderstandably, is to “find” another, older child withthe same disorder as their child. Whilst this mightbe possible for some, it still does not mean that thetwo children will develop in the same way.However, just talking to other parents with a childwith a rare chromosomal disorder can be a greatrelief and can help to alleviate feelings of isolationand “why me?”.
As part of its services, Unique runs a helpline(+44 (0) 1883 330766) for new and existing familiesand professionals to find out more information aboutthe group and about specific rare chromosomaldisorders. A comprehensive computerised databasehas been developed detailing the effects of specificrare chromosomal disorders amongst members. Thedatabase can be used to link families on the basis ofa specific rare chromosomal disorder. Often of morepractical benefit, however, is to link families on thebasis of problems as they arise, whether these aremedical, developmental, behavioural, social,educational and so on. Unique also maintains closelinks with other similar groups around the world,thus increasing the “pool” of possible familycontacts. Information about a specific rarechromosomal disorder can be prepared from theUnique database whilst not revealing the identity ofthe families concerned. Unique has also developed a
what can unique doto help?
11229:8876 17/6/13 15:13 Page 18

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
19
website (www.rarechromo.org) and can be contactedby email ([email protected]).
Many local groups and contacts have been formedthroughout the UK (and even in a few othercountries). Families affected by any rarechromosomal disorder can come together locally forgeneral support and friendship and to pass oninformation about services available in theirneighbourhood. Unique publishes a regular magazinein which families can write about their experiencesand exchange useful information. The group alsoholds study days and a regular conference in variousvenues across the UK where families andprofessionals can meet and discuss latestdevelopments. Unique can also act as a go-betweento enable families to participate in any researchprojects relevant to their child’s condition.
Whatever your specific needs, Unique will try toprovide you with tailor-made information and helprelevant to your child’s disorder. Please make use ofthese services – Unique is YOUR group.
11229:8876 17/6/13 15:13 Page 19

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
20
When parents discover that their child has a rarechromosomal disorder, they often find themselvesconfronted with a very steep learning curve. Anyinformation learnt about genetics in biology classesat school may be a distant memory. Here we will tryto provide you with the basic facts aboutchromosomes and the different types of rarechromosome disorders. If you find the informationa bit complicated, please don’t be put off but doask if you aren’t sure what anything means.
Cells, Chromosomes,DNA and Genes
all aboutchromosomes and genes
FIG. 1 Increasingmagnification to showwhere chromosomes andgenes are found in thehuman body.
The human body is made up of billions of individualCELLS. With the exception of the red blood cells,each of these cells contains a structure called theNUCLEUS, which is held within a thick fluid calledthe CYTOPLASM. Inside the nucleus are found theCHROMOSOMES, which contain the GENES. Genes
Human Cellsgrouped together
Genes strung along theDNA of a Chromosome
IndividualHuman cell
A Chromosome
Cell Membrane
Cytoplasm
Nucleus
Chromosomes
11229:8876 17/6/13 15:13 Page 20

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
21
are “strung” along the chromosomes, a bit like beadsalong a necklace. Genes are the instructions that tellthe body how to develop and work properly.
Apart from the mother’s EGG cells or the father’sSPERM cells, every cell in the human body normallycontains 23 PAIRS of chromosomes, making 46chromosomes in total in each cell. This number ofchromosomes is known as the DIPLOID number.The Human Genome Project has shown there to beabout 30,000 genes in every cell. These genes arespread unevenly across the chromosomes, somechromosomes having many more genes than otherchromosomes and some parts of each chromosomeholding more genes than other parts. Of the 23 pairsof chromosomes in each of these cells, one memberof each pair is normally inherited from the fatherand the other member is normally inherited from themother. Members of each pair of chromosomes arecalled HOMOLOGOUS chromosomes. The first 22pairs of chromosomes are called the AUTOSOMESand are numbered from 1 to 22 according to theirlength, starting with number 1 as the longest. Thechromosomes in the 23rd pair are called the SEXCHROMOSOMES. Sex chromosomes are labelled Xor Y. Males normally have one copy of the Xchromosome and one copy of the Y chromosome ineach cell; it is the Y chromosome that determines“maleness”. Females, on the other hand, normallyhave two copies of the X chromosome but no Ychromosome.
The number of chromosomes in the egg or sperm isdifferent from that in other body cells. The mother’seggs each contain only 23 chromosomes (theHAPLOID number), made up of one copy of eachautosomal chromosome (1 to 22) along with onecopy of the X chromosome. The sperm from thefather also contain 23 chromosomes, again made upof one copy of each autosomal chromosome but alsoeither one copy of the X chromosome or one copy ofthe Y chromosome. So it is the father’s sperm that
11229:8876 17/6/13 15:13 Page 21
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
22
determines whether a child will be a boy (XY) or agirl (XX).
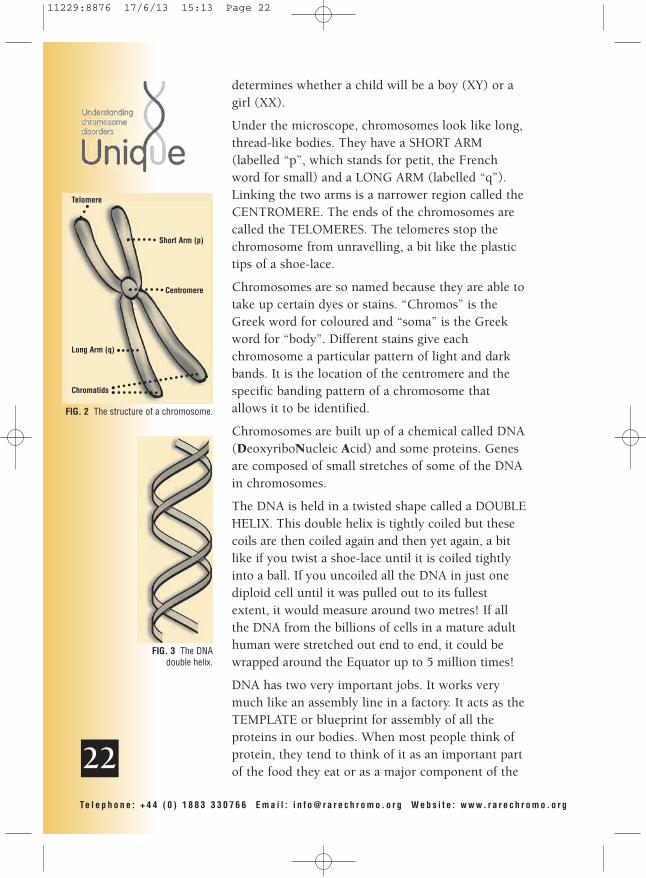
Under the microscope, chromosomes look like long,thread-like bodies. They have a SHORT ARM(labelled “p”, which stands for petit, the Frenchword for small) and a LONG ARM (labelled “q”).Linking the two arms is a narrower region called theCENTROMERE. The ends of the chromosomes arecalled the TELOMERES. The telomeres stop thechromosome from unravelling, a bit like the plastictips of a shoe-lace.
Chromosomes are so named because they are able totake up certain dyes or stains. “Chromos” is theGreek word for coloured and “soma” is the Greekword for “body”. Different stains give eachchromosome a particular pattern of light and darkbands. It is the location of the centromere and thespecific banding pattern of a chromosome thatallows it to be identified.
Chromosomes are built up of a chemical called DNA(DeoxyriboNucleic Acid) and some proteins. Genesare composed of small stretches of some of the DNAin chromosomes.
The DNA is held in a twisted shape called a DOUBLEHELIX. This double helix is tightly coiled but thesecoils are then coiled again and then yet again, a bitlike if you twist a shoe-lace until it is coiled tightlyinto a ball. If you uncoiled all the DNA in just onediploid cell until it was pulled out to its fullestextent, it would measure around two metres! If allthe DNA from the billions of cells in a mature adulthuman were stretched out end to end, it could bewrapped around the Equator up to 5 million times!
DNA has two very important jobs. It works verymuch like an assembly line in a factory. It acts as theTEMPLATE or blueprint for assembly of all theproteins in our bodies. When most people think ofprotein, they tend to think of it as an important partof the food they eat or as a major component of the
FIG. 2 The structure of a chromosome.
FIG. 3 The DNAdouble helix.
Telomere
Short Arm (p)
Centromere
Long Arm (q)
Chromatids
11229:8876 17/6/13 15:13 Page 22

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
23
structure of their muscles. While some proteins areindeed very important as part of the structure of ourbodies, others have essential parts to play incontrolling how our bodies work properly. Someproteins act as enzymes, which make the chemicalreactions in our bodies happen more easily andquickly, while others act as hormones, which helpcontrol our body’s proper functioning anddevelopment. Some proteins even help control theproduction of other proteins by different genes. Theprocess of protein production is a very complex oneand yet, most of the time, the correct proteins aremade to keep our bodies working properly andhealthily. With rare chromosomal disorders, though,many genes might be missing or extra and soessential proteins are either not made at all or aremade in too many copies or are made incorrectly orat the wrong time. The second important function ofDNA is to pass on the genetic blueprint from oldcells to new cells and from parent to child. Anaccurate copy of the DNA in each chromosome hasto be made every time a new cell is formed.
Chromosome and DNA AnalysisSpecialist scientists called cytogeneticists examine aperson’s chromosomes or DNA for defects. Usually,they will analyse the chromosomes or DNA in thewhite cells (lymphocytes) in a person’s blood. Theycan also analyse the chromosomes or DNA found inthe cells of other body tissues like bone marrow orskin or they might analyse the cells from chorionicvillus or amniotic fluid samples to see if a fetus iscarrying an abnormality. The cell samples have firstto be grown up under special laboratory conditionsand this can be very time-consuming, especially ifchorionic villus or amniocentesis samples are to beanalysed. This is one reason why it can take severalweeks for the results of a chromosome analysis to bereported.
Cytogeneticists will use special chemicals to stop the
11229:8876 17/6/13 15:13 Page 23

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
24
cells they are examining at an appropriate stagewhen the chromosomes are at their most compact.At this stage, called METAPHASE, the chromosomescan be stained with different dyes. The stain usedmost often is called GIEMSA in a techniqueproducing G-BANDED chromosomes.
Different stains give the chromosomes acharacteristic pattern of light and dark bands whichhelps with their identification. Sometimes thechromosomes are analysed when they are a little lesscompact so that more bands can be seen and smallerextra or missing pieces of DNA can be identified.This is called High Resolution Analysis. Diagrams ofchromosomes showing these banding patterns arecalled IDEOGRAMS (see Fig 4). Other neweranalytical techniques have been developed which areused in addition or as an alternative to these stainingmethods. These newer techniques include, forexample, Fluorescence In Situ Hybridisation (FISH)and microarray comparative genomic hybridisation(array-CGH).
FISHWith FISH, known segments of DNA tagged withfluorescent dyes (so called DNA ‘probes’) are mixedwith specially pre-treated preparations from a tissuesample (most often chromosome preparations fromblood samples). These specific DNA probes bind to(“paint”) small parts of a chromosome in different
Fig. 5 FISH analysis using twoDNA probes for chromosome 22.
In green is the control probe and inred is the TUPLE probe which it
can be seen is present on one copyof chromosome 22 but missing
(deleted) from the secondchromosome 22.
Fig. 4 Ideogram ofG-Banded Chromosome 1.
36.3
36.2
36.1
35
34.334.234.1
33
32.332.232.1
31.3
31.2
31.1
22.3
22.2
22.1
21
13.3
13.213.1
121111
12
21.121.221.3
22
23
24
25
31
32.1
32.232.3
41
42.142.242.3
43
44
p
q
�Centromere
CourtesyoftheWestMidlandsRegionalGeneticsLaboratory
11229:8876 17/6/13 15:13 Page 24
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
25
fluorescent colours which can then be visualisedunder a special fluorescent microscope. In this way itis possible to determine the number of copies ofsmall sections of chromosomes. This technique isuseful if it is known or suspected which of the 23chromosomes might be involved. If, however, it isnot known (or suspected) which chromosome mightbe involved array-CGH might be used.
Microarray comparative genomichybridisation (array-CGH)With array-CGH analysis, DNA is usually extractedfrom a blood sample. This technique utilises amicroarray which is, in simple terms, a glass slide onwhich there are thousands of ‘spots’ of a reference(control) DNA sample. The control sample is from aperson who is known to have two complete copiesof each chromosome (as is usual). The person ofinterest’s DNA is compared with the reference DNA.An analysis of the ratio of the two sets of DNA candetermine whether there is the correct amount ofDNA, too much (a duplication) or too little (adeletion). This technique is extremely sensitive andtherefore much smaller gains or losses of DNA(called microdeletions or microduplications)throughout the entire human genome (ie across allthe chromosomes) can be detected than was possiblewith karyotyping. Unique has published moredetailed information guides on analytical techniquesand these are available from our websitewww.rarechromo.org.
As we have already mentioned, a person’schromosomal make-up is called their KARYOTYPE.Obviously, it would be impractical always to have toshow a photograph of someone’s chromosomes inorder to describe any chromosomal disorder theymight have. As a consequence, scientists havedevised a standardized code to describe a person’skaryotype. This system is called the InternationalSystem for Human Cytogenetic Nomenclature
11229:8876 17/6/13 15:13 Page 25

(ISCN). The mostrecent version waspublished in 2013and it now includesnomenclature formolecular cytogenetictechniques suchas FISH andmicroarrays. Thismeans that anyoneunderstanding thecode will have a fairlyprecise descriptionof a person’schromosomaldisorder.
In general, under theISCN convention,
karyotype codes are written so that the number ofchromosomes in a person’s cells come first, followedby their sex chromosome make-up and then by adescription of any chromosomal disorder. Usingthis method, a normal male karyotype would bedescribed as 46,XY and a normal female karyotypeas 46,XX.
Any breakpoints in chromosomes are describedby a standardised numbering system based onthe banding patterns produced in G-bandedchromosomes. The bands allow the chromosomes tobe mapped into REGIONS, which in turn are dividedinto BANDS and then into SUB-BANDS. This is a bitlike being able to identify a house along a road ifyou know the house number. With the ISCNnumbering system, the higher the number of thebreakpoint, the further away from the centromere itis located. To help you understand this system moreclearly, take a look at some examples of karyotypedescriptions.
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
26
Fig. 6 Normal Female Karyotype.
Fig. 7 Normal Male Karyotype.
11229:8876 17/6/13 15:13 Page 26
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
27
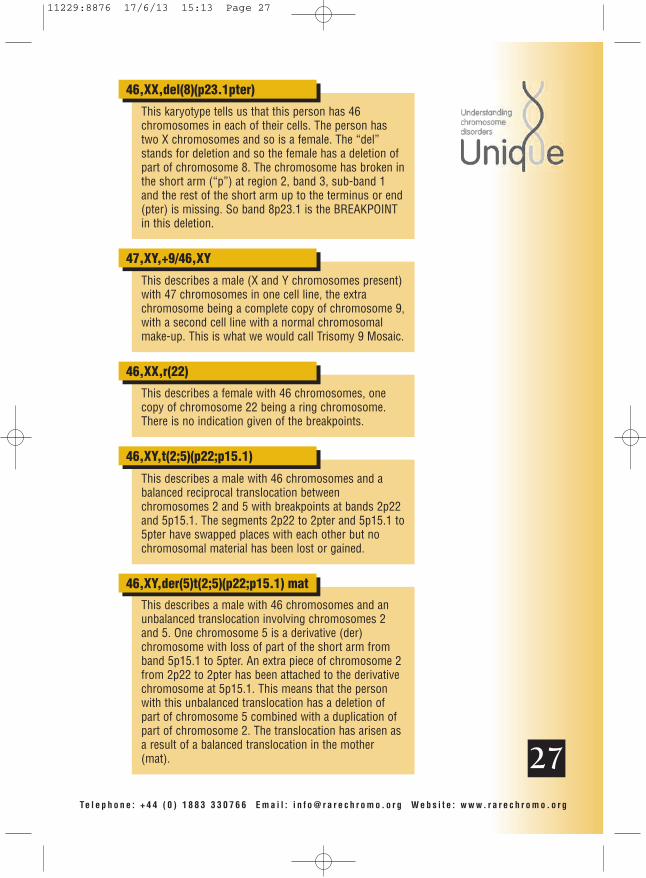
This karyotype tells us that this person has 46chromosomes in each of their cells. The person hastwo X chromosomes and so is a female. The “del”stands for deletion and so the female has a deletion ofpart of chromosome 8. The chromosome has broken inthe short arm (“p”) at region 2, band 3, sub-band 1and the rest of the short arm up to the terminus or end(pter) is missing. So band 8p23.1 is the BREAKPOINTin this deletion.
46,XX,del(8)(p23.1pter)
This describes a male (X and Y chromosomes present)with 47 chromosomes in one cell line, the extrachromosome being a complete copy of chromosome 9,with a second cell line with a normal chromosomalmake-up. This is what we would call Trisomy 9 Mosaic.
47,XY,+9/46,XY
This describes a female with 46 chromosomes, onecopy of chromosome 22 being a ring chromosome.There is no indication given of the breakpoints.
46,XX,r(22)
This describes a male with 46 chromosomes and abalanced reciprocal translocation betweenchromosomes 2 and 5 with breakpoints at bands 2p22and 5p15.1. The segments 2p22 to 2pter and 5p15.1 to5pter have swapped places with each other but nochromosomal material has been lost or gained.
46,XY,t(2;5)(p22;p15.1)
This describes a male with 46 chromosomes and anunbalanced translocation involving chromosomes 2and 5. One chromosome 5 is a derivative (der)chromosome with loss of part of the short arm fromband 5p15.1 to 5pter. An extra piece of chromosome 2from 2p22 to 2pter has been attached to the derivativechromosome at 5p15.1. This means that the personwith this unbalanced translocation has a deletion ofpart of chromosome 5 combined with a duplication ofpart of chromosome 2. The translocation has arisen asa result of a balanced translocation in the mother(mat).
46,XY,der(5)t(2;5)(p22;p15.1) mat
11229:8876 17/6/13 15:13 Page 27

Instead of, or in addition, to a karyotype, you maybe given the results of molecular analysis such asFISH or a microarray.
Results of a FISH analysis might look something likethis:
46,XY.ish del(9)(q34.3)(D9S2168-)dn
This means:
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
28
46 The total number ofchromosomes in your child’scells
XY The two sex chromosomes,XY for males; XX for females
.ish The analysis was by FISH
del A deletion, or material ismissing
(9) The deletion is fromchromosome 9
(q34.3) The chromosome has brokenat band 9q34.3, indicating asmall deletion of the end ofthe chromosome just shortof the ‘telomere’
(D9S2168-) A marker or probe whoseposition on the humangenome is known, in thiscase marker D9S2168, ismissing
dn dn stands for de novo
The parents’ chromosomeshave been checked and norearrangement foundinvolving 9q34.3
11229:8876 17/6/13 15:13 Page 28

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
29
With microarray analysis breakpoints at either end ofa deletion or duplication are denoted either by thename of a DNA “clone” or by a base pair coordinate.A base pair is simply one of the “rungs” on theladder of the double helix of DNA (Fig. 8). Theresults are likely to read something like this:
arr [hg19] 16p11.2(29673954-30198600)x1
This means:
arr The analysis was byarray-CGH
[hg19] Human Genome build 19.This is the reference DNAsequence that the base pairnumbers refer to. As moreinformation about the humangenome is found, new“builds” of the genome aremade and the base pairnumbers may be adjusted
16p11.2 A change was found in band16p11.2
(29673954-30198600)x1 The first base pair shown tobe missing is number29673954
The last base pair shown tobe missing is 30198600
The microdeletion is 524,646base pairs in size
x1 means is only one copy ofthese base pairs, not two –one on each chromosome 16– as you would normallyexpect
bp 1 base pair
1kb 1,000 base pairs
1Mb 1,000,000 base pairs
Fig. 8 Two strands of DNA are heldtogether in the shape of a doublehelix by the bonds between basepairs.
Basepairs
11229:8876 17/6/13 15:13 Page 29

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
30
You might already have been your child’s karyotypeor the results of molecular analysis such as FISH ormicroarray and would like to work out exactly whatthe code means. If you do not know your child’sresults, ask your doctor or geneticist for them,preferably with a copy of the original laboratoryreport(s), so that you have a correct description ofyour child’s chromosomal disorder. Here is a list ofthe more common symbols used in karyotypedescriptions and molecular analysis results.
Symbols used in karyotypes andmolecular analysis results
Symbol Description
add Additional material ofunknown origin
arr Microarray
arrow (->) From - to
Brackets, square ([ ]) Surround number of cells
cen Centromere
cgh Comparative genomichybridisation
single colon (:) Chromosomal break
double colon (::) Chromosomal break andreunion
comma (,) Separates chromosomenumbers, sex chromosomesand chromosomeabnormalities
decimal point (.) Denotes sub-bands
del Deletion
de novo Designates a chromosomalabnormality which has notbeen inherited
der Derivative chromosome
dic Dicentric
dup Duplication
h Heterochromatin
hg Human genome build
11229:8876 17/6/13 15:13 Page 30

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
31
i Isochromosome
idic Isodicentric chromosome
ins Insertion
inv Inversion
ish In situ hybridisation
mar Marker chromosome (extrachromosome of unknownorigin)
mat Maternal origin
minus sign (-) Loss
MLPA Multiple ligation-dependentprobe amplification
mos Mosaic
multiplication sign (x) Multiple copies of rearrangedchromosomes or number ofcopies of a chromosomalregion
p Short arm of chromosome
parentheses ( () ) Surround structurally alteredchromosomes andbreakpoints
pat Paternal origin
period (.) Separates various analyticaltechniques
plus sign (+) Gain
psu Pseudo
q Long arm of chromosome
question mark (?) Questionable identification ofa chromosome orchromosome structure
r Ring chromosome
rcp Reciprocal
rea Rearrangement
rec Recombinant chromosome
rob Robertsonian translocation
s Satellite
11229:8876 17/6/13 15:13 Page 31

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
32
semicolon (;) Separates alteredchromosomes andbreakpoints in structuralrearrangements involvingmore than one chromosome
slant line (/) Separates cell lines (used inmosaic karyotypes)
subtel Subtelomeric region
t Translocation
tel Telomere
ter Terminal (end ofchromosome)
trp Triplication
upd Uniparental disomy
var Variant or variable region
wcp Whole chromosome paint
11229:8876 17/6/13 15:13 Page 32
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
33
Some changes or mutations in chromosomes are sosmall they only affect the composition of the DNAwithin a single gene and these are known as pointmutations. However, when changes in chromosomesaffect whole copies of one or more genes, they arecalled chromosome aberrations or disorders. Suchchromosome disorders can be classified into twomain types, NUMERICAL DISORDERS andSTRUCTURAL DISORDERS. If these disorders ariseduring the formation of the egg or the sperm cells,then the disorder would be passed on to every cell inthe body of a child produced. If the disorder arisesin one of the new cells produced soon after the egghas been fertilized by the sperm, then only aproportion of the child’s cells will be affected andthis is called MOSAICISM.
Unique publishes information guides on manydifferent individual chromosome disorders and theseare freely available from our website or on request.For rarer chromosome disorders not covered by theguides, Unique might hold information in the offlinedatabase. Please contact us with your informationrequests.
NUMERICAL DISORDERSIf cells carry complete extra sets of chromosomes,this is known as POLYPLOIDY. When there is oneextra set, to give 69 chromosomes in total, this iscalled TRIPLOIDY.
If only some of the body’s cells carry the extra setof chromosomes, then this is known as TriploidMosaicism, or Diploid Triploid Mosaicism or evenMixoploidy.
rare chromosomedisorders
11229:8876 17/6/13 15:13 Page 33

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
34
When individual whole chromosomes are missing orextra, this is called ANEUPLOIDY. This can happenwith any of the autosomal chromosomes (1 to 22) orthe sex chromosomes (X and Y).
If one extra complete chromosome is present, this isknown as TRISOMY and the number ofchromosomes in each affected cell would be 47.Probably the most well-known example of Trisomyis Down Syndrome (Trisomy 21).
Two extra complete chromosomes would be calledTETRASOMY and the number of chromosomeswould be 48. If a complete chromosome is missing,this is known as MONOSOMY and the number ofchromosomes in each cell would be 45.
STRUCTURAL DISORDERSStructural disorders occur because of breakages in achromosome. They can occur spontaneously (this iscalled DE NOVO) or they can be inherited from aparent. Structural disorders include various types oftranslocation, deletions, ring chromosomes,duplications, inversions and isochromosomes.
TranslocationsA translocation happens when DNA is transferredfrom one non-homologous chromosome to another.They include reciprocal translocations, Robertsoniantranslocations and insertional translocations.Translocations can be balanced or unbalanced.
Fig.10 Karyotype showing a singleextra chromosome (T21).
Fig. 9 Ideogram and Triploid Karyotype.
11229:8876 17/6/13 15:13 Page 34
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
35
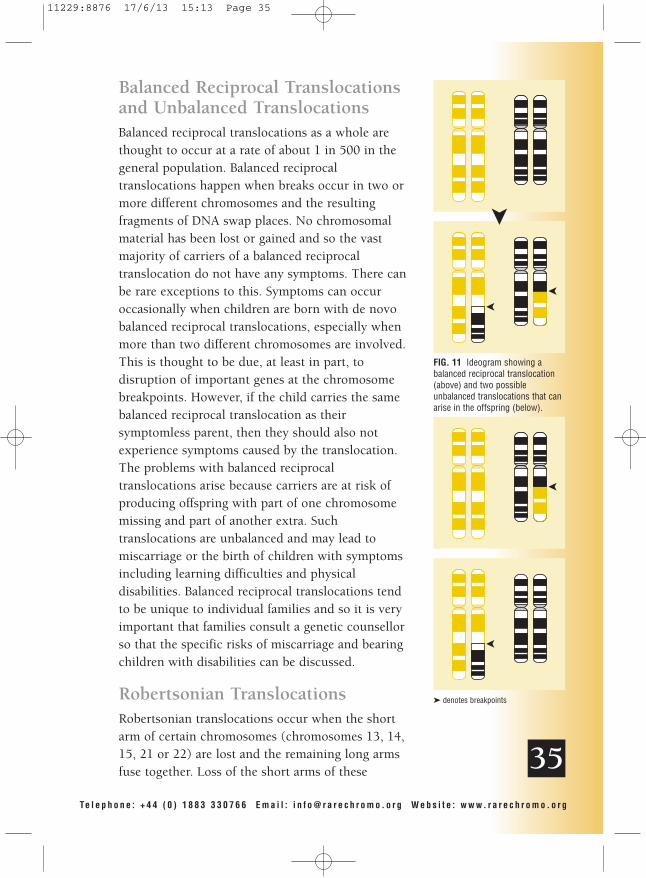
Balanced Reciprocal Translocationsand Unbalanced TranslocationsBalanced reciprocal translocations as a whole arethought to occur at a rate of about 1 in 500 in thegeneral population. Balanced reciprocaltranslocations happen when breaks occur in two ormore different chromosomes and the resultingfragments of DNA swap places. No chromosomalmaterial has been lost or gained and so the vastmajority of carriers of a balanced reciprocaltranslocation do not have any symptoms. There canbe rare exceptions to this. Symptoms can occuroccasionally when children are born with de novobalanced reciprocal translocations, especially whenmore than two different chromosomes are involved.This is thought to be due, at least in part, todisruption of important genes at the chromosomebreakpoints. However, if the child carries the samebalanced reciprocal translocation as theirsymptomless parent, then they should also notexperience symptoms caused by the translocation.The problems with balanced reciprocaltranslocations arise because carriers are at risk ofproducing offspring with part of one chromosomemissing and part of another extra. Suchtranslocations are unbalanced and may lead tomiscarriage or the birth of children with symptomsincluding learning difficulties and physicaldisabilities. Balanced reciprocal translocations tendto be unique to individual families and so it is veryimportant that families consult a genetic counsellorso that the specific risks of miscarriage and bearingchildren with disabilities can be discussed.
Robertsonian TranslocationsRobertsonian translocations occur when the shortarm of certain chromosomes (chromosomes 13, 14,15, 21 or 22) are lost and the remaining long armsfuse together. Loss of the short arms of these
FIG. 11 Ideogram showing abalanced reciprocal translocation(above) and two possibleunbalanced translocations that canarise in the offspring (below).
� denotes breakpoints
11229:8876 17/6/13 15:13 Page 35

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
36
FIG 12 The Knight family with ideograms of their chromosomes 9 and 20.Edna (left) has a balanced insertion of part of chromosome 9 in chromosome20, as has daughter Claire (not shown). Julie and Wendy (centre) have partialduplications of the short arm of chromosome 9, while Linda (right) has normalchromosomes.
DeletionsA DELETION involves loss of a part (a segment) of achromosome and is sometimes known as a PARTIALMONOSOMY. Deletions can occur in any part of anychromosome. If the segment is lost from near to the
chromosomes should not cause any symptoms. Aperson with a Robertsonian translocation has a totalchromosome number of 45. Robertsoniantranslocations are relatively common in the generalpopulation (about 1 in 1000), the most frequentbeing fusion of the long arms of chromosomes 13and 14. The significance of a RobertsonianTranslocation is the risk of miscarriage or ofproducing children with an unbalanced chromosomemake-up.
InsertionsInsertions occur when a segment of onechromosome is inserted into a gap in anotherchromosome. If someone carries a balancedinsertional rearrangement, they should not have anysymptoms (unless a critical gene is disrupted at thebreakpoints) but they are at risk of producing a childwith either a deletion or a duplication ofchromosomal material but not both disorders.
11229:8876 17/6/13 15:13 Page 36

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
FIG 13 Ideogram showing a partialdeletion of the short arm ofchromosome 9 (right) along withits normal homologouschromosome (left).
� denotes breakpoint
�p
p22
q
37
FIG 14 Ring Chromosome.
�
centromere, this is called a PROXIMAL DELETION.If the segment is lost from nearer to the end of thechromosome (the telomere), then the deletion iscalled a DISTAL DELETION. If there is just onebreak in the chromosome, then the deletion is calleda TERMINAL DELETION. (Terminal just refers tothe end of the chromosome and does not infer thatthe deletion will be lethal to the child.) If there aretwo breaks in the arm of the chromosome with theintervening segment being lost and the remainingparts of the chromosome joining up, then this iscalled an INTERSTITIAL DELETION. Somedeletions are so small they cannot be seen down alight microscope and are called MICRODELETIONS.
RingsA RING chromosome usually forms when the endsof both arms of the same chromosome are deleted.The remaining broken ends of the chromosome are“sticky” and join together to make a ring shape.Usually, it is the missing DNA that is significant. Ineffect, the person with a ring chromosome has aterminal deletion of both the short and the longarms of the chromosome. However, if the ringchromosome is present as an extra (orSUPERNUMERARY) chromosome, then it is thechromosomal material that has NOT been deletedthat is significant. The material in the extra ringchromosome has effectively been duplicated. Somegeneticists believe that there can also be a generaleffect caused by any ring chromosome, poor growthand developmental delay being the outcome.
DuplicationsA DUPLICATION occurs when an extra copy of asegment of a chromosome is present. A duplicationis sometimes known as a PARTIAL TRISOMY. If aperson has two extra copies of a chromosomalsegment, then this is known as a TRIPLICATION ora PARTIAL TETRASOMY. Some duplications are so
11229:8876 17/6/13 15:13 Page 37

small they cannot be seen down a light microscopeand are called MICRODUPLICATIONS.
InversionsInversions occur when there are two breaks in asingle chromosome. The segment between thebreakpoints turns through 180 degrees and reinsertsitself into the “gap” left in the chromosome. If bothbreaks occur in the same arm of the chromosome,this is called a PARACENTRIC INVERSION. If onebreak occurs in the short arm and the other in thelong arm of the chromosome, then this is called aPERICENTRIC INVERSION. Usually, inversions donot cause problems in the carrier (unless importantgenes are disrupted) but there is a risk of producingsperm or eggs with unbalanced chromosomes.Carriers of paracentric inversions very rarely givebirth to children with abnormalities. On the otherhand, carriers of pericentric inversions morefrequently give birth to children with abnormalities.These children will have a partial duplication of onearm of the affected chromosome along with a partialdeletion of the end of the other arm of thatchromosome or vice versa. The closer thebreakpoints are to the ends (telomeres) of thechromosomes, the greater the chance of the childsurviving to birth. This is because the chromosomesegments deleted and duplicated will be smaller.
Isochromosomes and sSMCsSometimes people carry an extra or supernumerarychromosome made up of parts of one or morechromosomes. They will effectively carry aduplication or triplication of the material formingthis extra chromosome. If the origin of the extrachromosome is unknown, it is sometimes referred toas a small supernumerary marker chromosome(sSMC) or a marker chromosome. If the extrachromosome is made up of two copies of the samesegment of a chromosome, this is called an
Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
38
FIG 16 Ideogram of a pericentricinversion of chromosome 10 (B)
with its normal homologouschromosome (A) and of aparacentric inversion of
chromosome 16 (D) and its normalhomologous chromosome (C).
The inverted segments lie betweenthe black arrows.
p
q
A B C D
�
�
�
�
FIG 15 Ideogram showing partialduplication of the long arm of
chromosome 1 (right) along withits normal homologous
chromosome (left).
� denotes breakpoint
�
�
p
q
11229:8876 17/6/13 15:13 Page 38

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
39
FIG. 17 Ideogram of Isodicentric(idic) 15 (right) with two copies ofpart of a chromosome and twonormal chromosomes 15 (left).
� denotes breakpoint
p
q
q13 �
isochromosome. When these extra chromosomescarry two copies of the same centromere, they arecalled isodicentric chromosomes.
Uniparental disomy (UPD)In uniparental disomy (UPD) both chromosomes inone of the 23 pairs have come from the same parentinstead of one coming from the father and the otherfrom the mother. The result of UPD is a doublepresence of genes from one parent and no inputfrom the other parent. When all the genes comefrom the mother, this is termed maternal UPD,sometimes shortened to mUPD or UPDmat. Whenall the genes come from the father, this is termedpaternal UPD, sometimes shortened to pUPD orUPDpat. For most chromosomes having all the genesfrom one parent does not matter, but for certainchromosomes (e.g. chromosome 14) or parts ofthem it does make a difference.
11229:8876 17/6/13 15:13 Page 39

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
40
If you would like to read more detailed booksabout medical genetics (aimed at the medical orcytogenetics student or qualified doctor), findout what those incomprehensible medical andcytogenetic terms mean, keep up to date with paperspublished about specific rare chromosomal disordersor consult cytogenetic databases, the following maybe helpful.
• “Essential Medical Genetics”, 6th Edition,by Edward S Tobias, Michael Connor &Malcolm FergusonSmith, John Wiley and Sons LtdWiley-Blackwell, ISBN10: 1405169745ISBN13: 9781405169745
• “Emery’s Elements of Medical Genetics”,14th Edition, by Peter Turnpenny & Sian Ellard,Churchill Livingstone, ISBN 9780702040436
• “Oxford Desk Reference: Clinical Genetics” byHelen Firth and Jane Hurst with Judith Hall (Ed),Oxford University Press, ISBN 0-19-262896-1
• “ISCN 2013: An International System for HumanCytogenetic Nomenclature (2013)”, Ed. Lisa G.Shaffer, Jean McGowan-Jordan & Michael Schmid,Karger, Basel, ISBN 978-3-318-02253-7
• “Dorland’s Illustrated Medical Dictionary”,Edition 32, Saunders, ISBN 9781416062578
• The Online Mendelian Inheritance in Man (OMIM)website www.ncbi.nlm.nih.gov/Omim
• The Medline website www.ncbi.nlm.nih.gov/PubMed(lists abstracts of papers published about medicalconditions, including specific rare chromosomaldisorders – updated regularly)
• Decipher database https://decipher.sanger.ac.uk
• Ecaruca database www.ecaruca.net
further reading andinformation
11229:8876 17/6/13 15:13 Page 40

Te l e p h o n e : + 4 4 ( 0 ) 1 8 8 3 3 3 0 7 6 6 Ema i l : i n f o@ r a r e c h r omo . o r g Web s i t e : www. r a r e c h r omo . o r g
41
Unique receives no government funding. Theservices we offer are paid for by voluntary donations,grants, fundraising and Gift Aid. To help us toexpand our services and to keep them free tomembers, please give generously if you can. You candonate by sending a cheque, made payable toUnique, in GB pounds, Euros, US dollars orAustralian dollars, or, preferably, by any of the majorcredit cards using the secure payment system on ourwebsite (www.rarechromo.org). Please send anydonations to:
Jenny Knight, Unique Finance Officer122 Copse Avenue, West WickhamKent BR4 9NP, EnglandTelephone: +44 (0) 20 8777 3717Email: [email protected]
For more information about donating or, for UKmembers only, about how to subscribe to the GiftAid Scheme, please get in touch with Jenny.
For more information about fundraising, please getin touch with:
Craig Mitchell, Unique COOPO Box 2189, CaterhamSurrey CR3 5GN, EnglandTelephone: +44(0)1883 330766Email: [email protected]
This book usually costs £5.00. If you have foundit useful, please would you consider making adonation to Unique to help cover our costs?Simply follow the instructions above.
donations, fundraisingand gift aid
Thank you
11229:8876 17/6/13 15:13 Page 41

PO Box 2189Caterham
Surrey CR3 5GNEngland
Telephone: +44 (0) 1883 330766Email: [email protected]: www.rarechromo.org
Rare Chromosome Disorder Support GroupRegistered Charity Number 1110661
Registered in England and Wales Company Number 5460413Registered Office: Valiant House, 3 Grange Mills, Weir Road, London SW12 0NE Issue 7
11229:8876 17/6/13 15:13 Page i