the national covid cohort collaborative (n3c): let’s get
TRANSCRIPT

The National COVID Cohort Collaborative (N3C): Let’s Get Involved !
Warren A. Kibbe, PhD, FACMIJune 15, 2021
Purdue Big Data in Cancer Workshop
@data2health@ncats_nih_gov
covid.cd2h.orgncats.nih.gov/n3c@wakibbe

Speaker Objectives
Warren KibbeDuke Biostatistics & BioinformaticsCTSA InformaticsDuke Cancer InstituteMember N3C
● Real World Data
● Open Science
● Overview of N3C
● N3C Data Enclave statistics
● How common data models and variables
are harmonized
● The scope of answerable questions
● Data access and security
● How common data models and variables
are harmonized
● Oncology research in N3C
A program of NIH’s National Center
for Advancing Translational Sciences

Special thanks to:
● Chris Chute, N3C, Johns Hopkins
● Melissa Haendel, N3C, Colorado University
● Umit Topaloglu, N3C, Wake Forest
● Frank Rockhold, Duke
● Noha Sharafeldin, N3C, UAB
4
Take homes
• N3C represents a unique resource to examine effects of COVID-19 on cancer
outcomes
• Largest COVID-19 and cancer cohort within the US
• Consistent with previous literature, older age, male gender, increasing comorbidities,
and hematological malignancies were associated with higher mortality in patients with
cancer and COVID-19
• The N3C dataset confirmed that cancer patients with COVID-19 who received recent
immuno-, or targeted therapies were not at higher risks of overall mortality

What is Real World Data?
Collected in the
context of patient
care. Real World
Data was called out
as part of the 21st
Century Cures Act
21st Century Cures Act: https://www.fda.gov/regulatory-information/selected-amendments-fdc-act/21st-century-cures-act
Graphic from HealthCatalyst: https://www.healthcatalyst.com/insights/real-world-data-chief-driver-drug-development

Our ability to generate biomedical data continues to grow in terms of
variety and volume
Current sources of data
molecular genome pathology imaging labs notes sensors
icons by the Noun Project

AI is changing our ability to go both deep and broad
Trustworthy AI
Provenance
Reusable
Reproducible

Having a health equity lens
● Digital Health, precision medicine, and real world data all have the power to transform healthcare. However, we must pay attention to structural racism and implicit bias if we want to achieve equity.

21st Century Cures Act
Last year I discussed the NCI Cancer
Moonshot and Precision Medicine
activities funded under the 21st Century
Cures Act
FDA was directed by congress to focus
on the use of RWD and RWE in drug
design, development and outcomes
assessment
https://www.fda.gov/regulatory-information/selected-
amendments-fdc-act/21st-century-cures-act

Is it just about Real World Data?
What about Open Science? Data transparency? Data Access?

The importance of Open Science
Calls for greater transparency and ‘open data access’ in clinical research
continue actively.
● “Open science is the movement to make scientific research, data and
dissemination accessible to all levels of an inquiring society”*
● Open Science Project**: “If we want open science to flourish, we should
raise our expectations to: Work. Finish. Publish. Release.”
● FAIR Principles: Findability, Accessibility, Interoperability, and Reusability***
● TRUST Principles: Transparency, Responsibility, User focus, Sustainability
and Technology
* https://www.fosteropenscience.eu/resources
** http://openscience.org/
*** https://www.nature.com/articles/sdata201618
****https://www.nature.com/articles/s41597-020-0486-7

Open Science and Patient Data Access
Some of the challenges are:
● Patient privacy
● Academic credit
● Commercial sensitivity and intellectual property
● Data standards
● Resources (money and people)
There should be room for researchers and patients alike to gain from this effort.
Informatics experts and data scientists are essential elements of this discussion.

One problem with Clinical Trials Data Sharing
● “The tendency for researchers to ‘‘sit’’ on their data for an unduly long period
of time is neither desirable from a scientific point of view nor acceptable from
an ethical perspective. ‘
● ‘After all, the data belong to the patients who agreed to participate in the
research, not to the investigators who coordinated it, as the new European
General Data Protection Regulation emphasizes.”*
*Rockhold, F, et al. Open science: The open clinical trials data journey, Clinical Trials, Vol 16 (5) 1-8, 2019

Access to patient-level data is important for research
There are certainly challenges, but question is not whether data should be
shared, but rather how and when access should be granted.
Responsible open access enables secondary analyses that:
● Enhance reproducibility of clinical research
● Honor the contributions of trial participants,
● Improve the design of future trials
● Generate new research findings
This journey of making patient data available is part of an evolution in
transparency and not a sudden awakening.

What about N3C?
It is an open science, controlled access environment

Clinical and Translational Science
Awards (CTSA) Program

● Algorithms (diagnosis, triage, predictive, etc.)● Drug discovery & pharmacogenetics● Multimodal analytics (EHR, imaging, genomics)● Interventions that reduce disease severity● Best practices for resource allocation● Coordinated research efforts to maximize efficiency and
reproducibility
These all require the creation of a comprehensive clinical data set
The pandemic highlights urgent needsA program of NIH’s National Center
for Advancing Translational Sciences

What Kinds of Questions Can N3C Address?
The scope and scale of the information in the platform
will support probing questions such as:
● What social determinants of health are risk factors for mortality?
● Do some therapies work better than others? By region? By demographics?
● Can we compare local rare clinical observations with national occurrences?
● Can we predict who might have severe outcomes if they have COVID-19?
● What factors will predict the effectiveness of vaccines?● Can we predict acute kidney injury in COVID-19 patients?
● Who might need a ventilator because of lung failure?
A program of NIH’s National Center
for Advancing Translational Sciences

Cohort characterization objectives
To clinically characterize the N3C cohort
● Largest U.S. COVID-19 cohort to date (+ representative controls)
● Racially, ethnically, and geographically diverse
To develop and share validated, versioned OMOP representations of
common variables (labs, vital signs, medications, treatments)
To generate hypotheses to be tested within N3C and elsewhere
● Clinical phenotypes and trajectories
● Treatment patterns and response
● … and many others
?
+
A program of NIH’s National Center
for Advancing Translational Sciences

Benefits for Participation
●Access to large scale COVID-19 data from across the nation
●Pilot data for grant proposals
●Opportunities for KL2 and TL1 and other scholars
●Team science opportunities for new questions and access to Teams, statistics, machine learning (ML), informatics expertise
●Learn ML analytics, NLP methods & access to tools, software, additional datasets
A program of NIH’s National Center
for Advancing Translational Sciences

Step 4. Federated Analytics with HPCWho is in the N3C? The N3C Computable Phenotype
● At a high level, our phenotype looks for patients:
○ With a positive COVID-19 test (PCR or antibody) OR
○ With an ICD-10-CM code of U07.1 OR
○ Two or more COVID-like diagnosis codes (ARDS, pneumonia, etc.) during the
same encounter, but only on or prior to 5/1/2020
● Each one of these patients is then demographically matched to two patients with
negative or equivocal COVID-19 tests.
● Each site securely sends this set of patients, along with their longitudinal EHR
data from 1/1/2018 to the present, to the N3C on a regular basis.
Age 47
Gender M
Race Black
Ethnicit
y
Unknow
n
COVID Positive
Matching algorithm
Age 49
Gender M
Race Black
Ethnicit
y
Hispanic/
Latino
COVID Negative
Age 46
Gender M
Race Black
Ethnicit
y
Not
Hispanic
COVID Negative
A program of NIH’s National Center
for Advancing Translational Sciences

N3C TimelineA program of NIH’s National Center
for Advancing Translational Sciences

N3C DashboardA program of NIH’s National Center
for Advancing Translational Sciences covid.cd2h.org/dashboard
55 sites with data released (purple) and 37 sites withdata pending (open circle). OCHIN is a national networkof 131 sites (diamond).
covid.cd2h.org/teams
31 Domain teams!
As of June 14, 2021

https://ncats.nih.gov/n3c/resources/data-contribution/data-transfer-agreement-signatories
Data Transfer Agreement Signatories
6/14/2021
88 DTA Signatories
Northwestern University at Chicago ᛫ Tufts Medical Center ᛫ Advocate Health Care Network ᛫ University of Alabama at Birmingham ᛫ Oregon Health & Science University ᛫
University of Washington ᛫ Stanford University ᛫ The University of Michigan at Ann Arbor ᛫ Children's Hospital Colorado ᛫ Duke University ᛫ Medical College of Wisconsin ᛫ The
Ohio State University ᛫ University of Nebraska Medical Center ᛫ University of Arkansas for Medical Sciences ᛫ George Washington University ᛫ Johns Hopkins University ᛫ West
Virginia University ᛫ Medical University of South Carolina ᛫ University of North Carolina at Chapel Hill ᛫ University of Virginia ᛫ The University of Texas Medical Branch at Galveston
᛫ University of Minnesota ᛫ University of Cincinnati ᛫ Columbia University Irving Medical Center ᛫ Cincinnati Children's Hospital Medical Center ᛫ Rush University Medical Center ᛫
Nemours ᛫ University of Wisconsin-Madison ᛫ The State University of New York at Buffalo ᛫ Washington University in St. Louis ᛫ University of Rochester ᛫ The University of
Chicago ᛫ University of Miami ᛫ The Scripps Research Institute ᛫ University of Texas Health Science Center at San Antonio ᛫ University of Kentucky ᛫ University of Illinois at
Chicago ᛫ Virginia Commonwealth University ᛫ Weill Medical College of Cornell University ᛫ Carilion Clinic ᛫ University Medical Center New Orleans ᛫ The University of Iowa ᛫
Emory University ᛫ Maine Medical Center ᛫ The University of Texas Health Science Center at Houston ᛫ Boston University Medical Campus ᛫ The University of Utah ᛫ University of
Southern California ᛫ George Washington Children's Research Institute ᛫ University of Colorado Denver I Anschutz Medical Campus ᛫ Mayo Clinic Rochester ᛫ The Rockefeller
University ᛫ Montefiore Medical Center ᛫ University of Mississippi Medical Center ᛫ University of Oklahoma Health Sciences Center, Board of Regents ᛫ University of
Massachusetts Medical School Worcester ᛫ Aurora Health Care ᛫ Penn State ᛫ University of New Mexico Health Sciences Center ᛫ NorthShore University HealthSystem ᛫ Wake
Forest University Health Sciences ᛫ Vanderbilt University Medical Center ᛫ Regenstrief Institute ᛫ Brown University ᛫ Stony Brook University ᛫ University of California, Davis ᛫ Yale
New Haven Hospital ᛫ Rutgers, The State University of New Jersey ᛫ MedStar Health Research Institute ᛫ Loyola University Chicago ᛫ Loyola University Medical Center ᛫
University of Delaware ᛫ Children's Hospital of Philadelphia

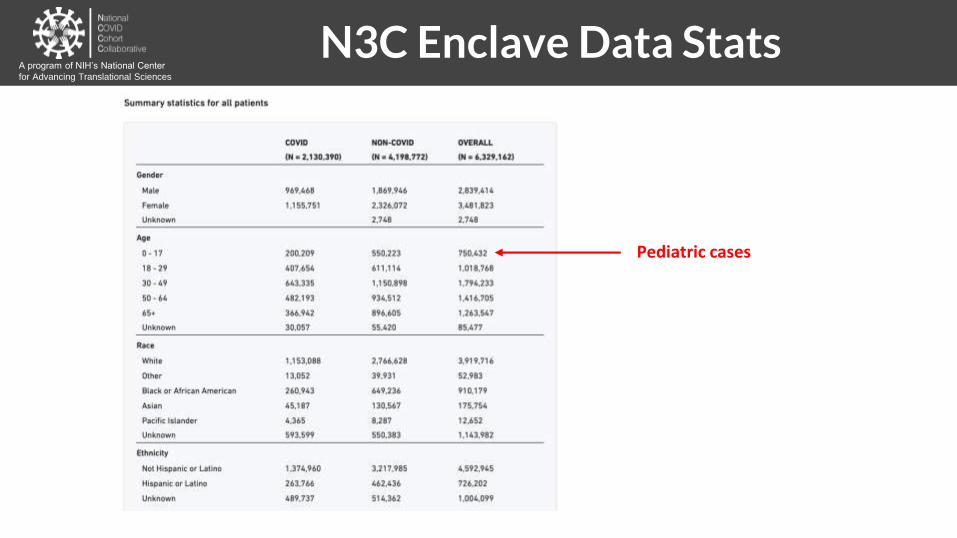
N3C Enclave Data Stats
Pediatric cases
A program of NIH’s National Center
for Advancing Translational Sciences
N3C Enclave Data Stats
Pediatric cases
A program of NIH’s National Center
for Advancing Translational Sciences

N3C Enclave Data StatsA program of NIH’s National Center
for Advancing Translational Sciences

Predicting Clinical Severity using machine
learning (64 input variables)
The most powerful predictors are patient age and widely available
vital sign and laboratory values.
The National COVID Cohort Collaborative: Clinical Characterization and Early Severity Prediction
https://pubmed.ncbi.nlm.nih.gov/33469592/

Step 4. Federated Analytics with HPCHow does data get into N3C?
● We have gone through the high-level purpose – EHR data about COVID-19
patients
● Identified the contributing sites
● Know what the inclusion criteria for N3C is – documented COVID-19 testing
● Seen the dashboard overview of N3C and the overall cohort characteristics
● What are the data ingestion, harmonization, query, and publication processes?
● Data governance and security?
● And finally, what about cancer and COVID-19?
A program of NIH’s National Center
for Advancing Translational Sciences

Leveraging Common Data ModelsA program of NIH’s National Center
for Advancing Translational Sciences
● These four data models are commonly used by academic medical centers throughout the US.
● CDMs are used to store EHR data in a consistent way.
● Sites participating in N3C may send data in one of these four formats—the idea is to make it as convenient as possible for sites to submit.
● Common data models also allow us to write a consistent computable phenotype that can be run with few local changes at sites with one or more of these data models.

Harmonization of N3C Data
A program of NIH’s National Center
for Advancing Translational Sciences

Data Availability vs UtilityA program of NIH’s National Center
for Advancing Translational Sciences
● Collections of data are not always useful
● Even if they are available
● Consistently classified data is
alway more useful

FAIR: Findable, Accessible,
Interoperable, ReusableA program of NIH’s National Center
for Advancing Translational Sciences
What does Interoperable mean with respect to data? Harmonized!
Syntactic Interoperability (harmonization)
● One can make sense of the structure
● Metaphor: sentence has good grammar
● Domain of the data standards and data model communities
Semantic interoperability (harmonization)
● One can make sense of the meaning
● Metaphor: the words are understandable
● Domain of the vocabulary, ontology, classification communities

N3C Data Ingestion & Harmonization PipelineA program of NIH’s National Center
for Advancing Translational Sciences
(future)
Span manual
curation of mapping
resources to
industrial scale
production
transformation

Harmonized, not HomogenousA program of NIH’s National Center
for Advancing Translational Sciences
CDMs are built for purpose. Different CDMs emphasize and prioritize different things.

Secure, reproducible, transparent, versioned, provenanced, attributed, and shareable analytics on patient-level EHR data
Collaborative Analytics -
N3C Secure Data Enclave

Federated versus Centralized DQA program of NIH’s National Center
for Advancing Translational Sciences
Many clinical data research networks are federated; N3C is centralized. Centralized datasets
have some advantages where data quality assessment is concerned.
Federated Network Centralized Data
Questions asked
directly against
all sites’ data
combined
Federated versus Centralized DQA program of NIH’s National Center
for Advancing Translational Sciences
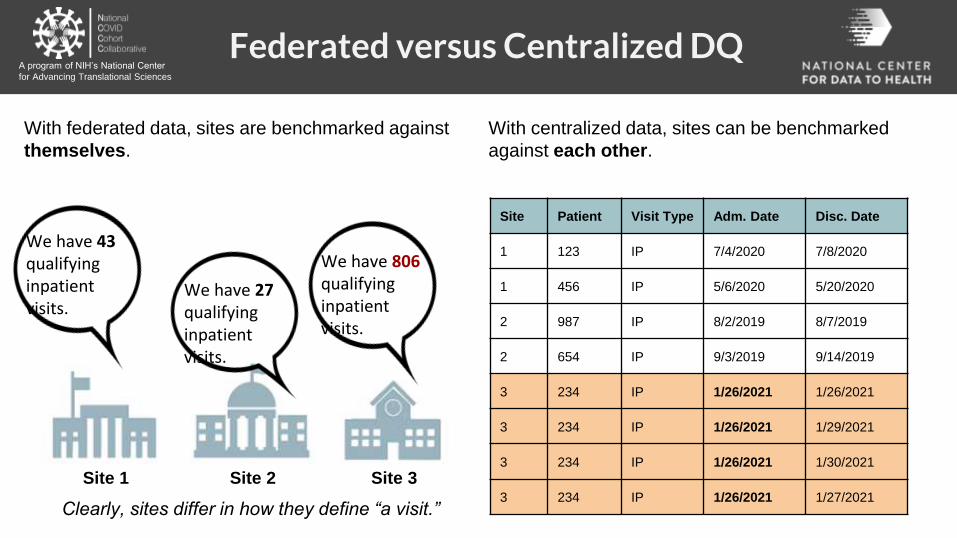
With federated data, sites are benchmarked against
themselves.
With centralized data, sites can be benchmarked
against each other.
We have 43 qualifying inpatient visits.
We have 27 qualifying inpatient visits.
We have 806 qualifying inpatient visits.
Site 1 Site 2 Site 3
Site Patient Visit Type Adm. Date Disc. Date
1 123 IP 7/4/2020 7/8/2020
1 456 IP 5/6/2020 5/20/2020
2 987 IP 8/2/2019 8/7/2019
2 654 IP 9/3/2019 9/14/2019
3 234 IP 1/26/2021 1/26/2021
3 234 IP 1/26/2021 1/29/2021
3 234 IP 1/26/2021 1/30/2021
3 234 IP 1/26/2021 1/27/2021Clearly, sites differ in how they define “a visit.”
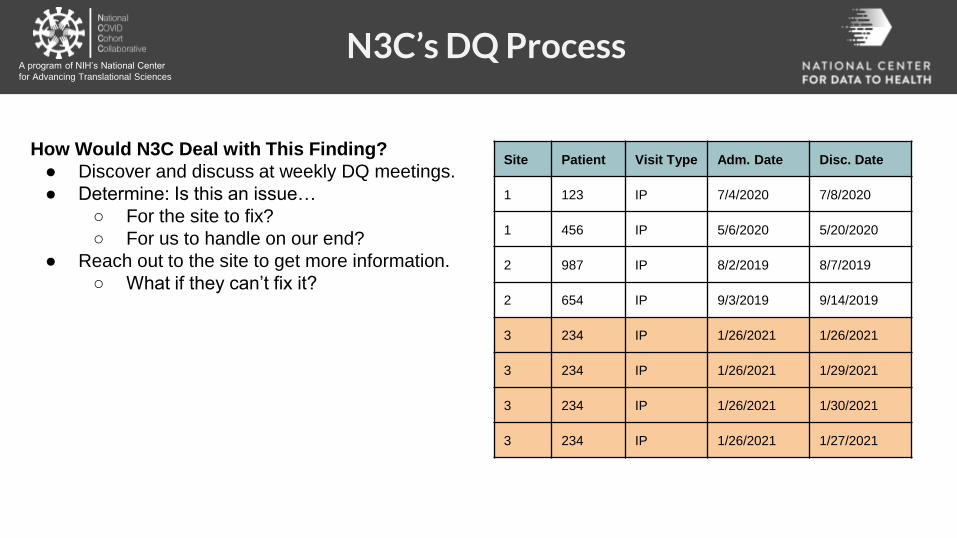
N3C’s DQ ProcessA program of NIH’s National Center
for Advancing Translational Sciences
How Would N3C Deal with This Finding?
● Discover and discuss at weekly DQ meetings.
● Determine: Is this an issue…
○ For the site to fix?
○ For us to handle on our end?
● Reach out to the site to get more information.
○ What if they can’t fix it?
Site Patient Visit Type Adm. Date Disc. Date
1 123 IP 7/4/2020 7/8/2020
1 456 IP 5/6/2020 5/20/2020
2 987 IP 8/2/2019 8/7/2019
2 654 IP 9/3/2019 9/14/2019
3 234 IP 1/26/2021 1/26/2021
3 234 IP 1/26/2021 1/29/2021
3 234 IP 1/26/2021 1/30/2021
3 234 IP 1/26/2021 1/27/2021

N3C’s DQ ProcessA program of NIH’s National Center
for Advancing Translational Sciences
How Would N3C Deal with This Finding?
● Discover and discuss at weekly DQ meetings.
● Determine: Is this an issue…
○ For the site to fix?
○ For us to handle on our end?
● Reach out to the site to get more information.
○ What if they can’t fix it?
We can write an algorithm to make this
site’s visits look more like the other sites:
if:
● the visit type is inpatient
● and there are > 1 per patient
per day
then:
● merge into a single “macro”
visit
Site Patient Visit Type Adm. Date Disc. Date
1 123 IP 7/4/2020 7/8/2020
1 456 IP 5/6/2020 5/20/2020
2 987 IP 8/2/2019 8/7/2019
2 654 IP 9/3/2019 9/14/2019
3 234 IP 1/26/2021 1/26/2021
3 234 IP 1/26/2021 1/29/2021
3 234 IP 1/26/2021 1/30/2021
3 234 IP 1/26/2021 1/27/2021

N3C’s DQ ProcessA program of NIH’s National Center
for Advancing Translational Sciences
Site Patient Visit Type Adm. Date Disc. Date
1 123 IP 7/4/2020 7/8/2020
1 456 IP 5/6/2020 5/20/2020
2 987 IP 8/2/2019 8/7/2019
2 654 IP 9/3/2019 9/14/2019
3 234 IP 1/26/2021 1/26/2021
3 234 IP 1/26/2021 1/29/2021
3 234 IP 1/26/2021 1/30/2021
3 234 IP 1/26/2021 1/27/2021
Site Patient Visit Type Adm. Date Disc. Date
1 123 IP 7/4/2020 7/8/2020
1 456 IP 5/6/2020 5/20/2020
2 987 IP 8/2/2019 8/7/2019
2 654 IP 9/3/2019 9/14/2019
3 234 IP 1/26/2021 1/30/2021
DQ fix
Takeaways
● Centralized DQ processes allow us to fully
realize the potential of N3C’s large sample size.
● All transformations are fully logged and always
completely reversible if needed.
Original Table Ready for Analysis

N3C Data Ingestion & Harmonization PipelineA program of NIH’s National Center
for Advancing Translational Sciences
(future)

Harmonizing numeric dataA program of NIH’s National Center
for Advancing Translational Sciences
● Problem: Different sites provide their
data in different units
● Solution: Harmonize each to a standard
unit
Kilograms = Pounds / 2.20462
Kilograms = Ounces / 35.274
Kilograms = Grams / 1000

Harmonizing numeric dataA program of NIH’s National Center
for Advancing Translational Sciences
● Problem: Some units are missing
● Solution 1: Contact the source
● Solution 2: N3C inference engine
Kilograms = x / 2.20462 ?
Kilograms = x / 35.274 ?
Kilograms = x / 1000 ?

Harmonization progressA program of NIH’s National Center
for Advancing Translational Sciences
● Harmonized measurements
○ By original unit
○ Across many sites
Homogeneity
after
harmonization
Humans measured in grams do not
look the same as humans measured
in kilograms!

Unit harmonization progressA program of NIH’s National Center
for Advancing Translational Sciences
Canonical unit
Uses a known conversion
Unit not plausible
Missing unit inferred
Unit still missing
● ~2x increase in usable data from our
harmonization procedures
We can rescue
a lot of data!

N3C Data Ingestion & Harmonization PipelineA program of NIH’s National Center
for Advancing Translational Sciences
(future)

714140
Pharyngalgia = Sore throatPlain-language medical vocabulary for precision diagnosis. Nat Genet. 2018 50:474-476.
Long-COVID phenotypes are myriad patient-reported and researcher-measured phenotypes are starkly different
Map literature and patient-reported terms to HPO

N3C Harmonization TakeawaysA program of NIH’s National Center
for Advancing Translational Sciences
What N3C has revealed most in terms of needs:
● Interoperability - we need syntactic and semantic!
○ FHIR ⇒ OMOP (syntactic)
○ Common vocabulary/codeset mapping provenance
and management (semantic)
● Approach data harmonization from an end-to-end data
life cycle perspective
● Leverage USCDI, but build for
interoperable semantic modeling
and extensions

Governing N3C Data
A program of NIH’s National Center
for Advancing Translational Sciences

Goal of the Data Use Agreement is Privacy Protection to Promote broad access:
● COVID-Related research only● NIH housed secure repository● No re-identification of individuals or data source● No download or capture of raw data● Open platform to all researchers● Investigator activities are recorded and can be
audited for security and reproducibility
N3C: Unique Data Use and PrivacyA program of NIH’s National Center
for Advancing Translational Sciences

N3C: Governance and Access

Data Levels to Access

Goal of the Data Use Agreement is Privacy Protection to Promote broad access:● COVID-Related research only● No re-identification of individuals or data source● No download or capture of raw data● Open platform to all researchers● Security: Activities in the N3C Data Enclave are recorded and can be audited● Disclosure of research results to the N3C Data Enclave for the public good● Analytics provenance● Contributor Attribution tracking
Data Use and Privacy

● Transparent and collaborative environment where all contributions are acknowledged
● Provenance and reproducibility
● Promptly sharing research results with N3C users
● Publish in high-impact journals
● Attribution for all N3C artifacts
N3C Attribution and Publication Principles
Researchers, projects, and
artifacts are all linked
together in the enclave
using the Contributor
Attribution Model (CAM).
N3C Provenance, Transparency, Attribution & Rapid SharingA program of NIH’s National Center
for Advancing Translational Sciences

N3C Data Access: Process
Data Use Request
HSP / Security Training
Data Use Agreement
https://ncats.nih.gov/n3c/about/applying-for-access
A program of NIH’s National Center
for Advancing Translational Sciences

Realizing Team Science
A program of NIH’s National Center
for Advancing Translational Sciences

Key functions can nucleate projects:
● Education & training
● Biostatistics
● Study design
● Evaluation
● Informatics
● Clinical expertise
● Innovation & commercialization
● Community & partnerships
N3C Domain Team Expertise:
● Enclave technology
● Data model (OMOP)
● Terminologies
● Data quality
● Codesets, variables, phenotype
● Using/parsing N3C data
● Workflows, methods, algorithms
RolesIngredients (Methods, datasets, instruments)Scientific questions
N3C team Science within & across institutions
https://covid.cd2h.org/domain-teams
CTSAs

OUTCOMES OF COVID-19 IN
CANCER PATIENTS: REPORT
FROM THE NATIONAL COVID
COHORT COLLABORATIVE
(N3C)
Noha Sharafeldin, Benjamin Bates, Qianqian Song, Vithal Madhira, Yao Yan, Sharlene Dong, Eileen Lee, Nathaniel Kuhrt, Yu Raymond Shao, Feifan Liu, Timothy Bergquist, Justin Guinney, Jing Su, Umit Topalogluon behalf of the N3C Consortium
Given on June 4, 2021
https://covid.cd2h.org/ cd2h.slack.com @data2health

N3C Oncology Domain Team (ODT)
60
Noha Sharafeldin, MBBCh, PhD
Benjamin Bates, MD
Rutgers University
Umit Topaloglu, PhD
Wake Forest
University
Noha Sharafeldin, MD, PhD
The University of Alabama at
Birmingham
Leadership
https://covid.cd2h.org/oncologySlack channel: #n3c-tt-oncology

N3C ODT Expertise
61
Noha Sharafeldin, MBBCh, PhD
Noha Sharafeldin
Informatics Biostatistics Clinical Epidemiology N3C data and Logic
Umit Topaloglu Jing Su Benjamin Bates Justin Guinney Vithal Madhira Tim Bergquist
Feifan Liu Qianqian Song Yu Raymond Shao Nate Kuhrt Sharlene Dong Eileen LeeYao Yan

N3C OncologyA program of NIH’s National Center
for Advancing Translational Sciences
http://ascopubs.org/doi/full/10.1200/JCO.21.01074

N3C Cancer Cohort
Primary Diagnosis
63
Noha Sharafeldin, MBBCh, PhD
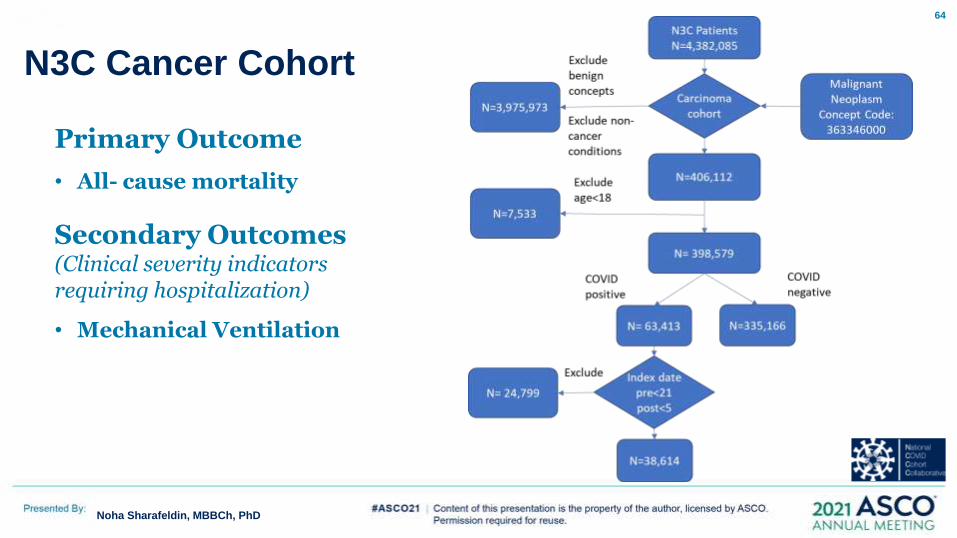
N3C Cancer Cohort
64
Noha Sharafeldin, MBBCh, PhD
Primary Outcome
• All- cause mortality
Secondary Outcomes (Clinical severity indicators requiring hospitalization)
• Mechanical Ventilation

65
Insert Name
(Insert > Header & Footer > Apply to All)
Demographic, clinical, and tumor characteristics9
Noha Sharafeldin, MBBCh, PhD
2%13%
31%
54%
Age
18-29
30-49
50-64
65+
COVID-19 Positive
4%13%
61%
22%
Race
Hispanic
Non-Hispanic Black
Non-Hispanic White
Other or Unknown
51%49%
Sex
Female
Male
11%
34%
28%
5%
22%
Geographical Location
US-Northeast
US-Midwest
US-South
US-West
Unknown
66
Insert Name
(Insert > Header & Footer > Apply to All)
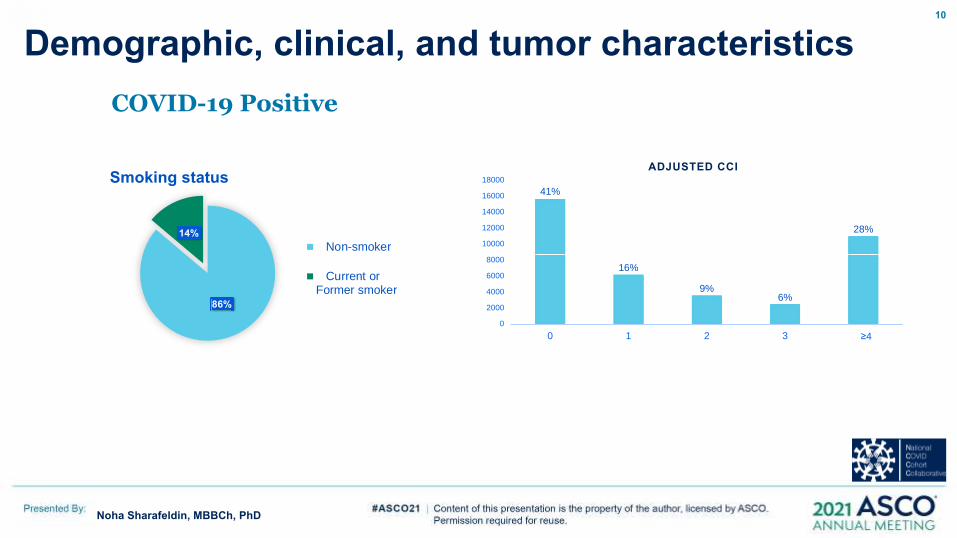
Demographic, clinical, and tumor characteristics10
Noha Sharafeldin, MBBCh, PhD
COVID-19 Positive
86%
14%
Smoking status
Non-smoker
Current orFormer smoker
41%
16%
9%6%
28%
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
0 1 2 3 ≥4
ADJUSTED CCI
67
Insert Name
(Insert > Header & Footer > Apply to All)
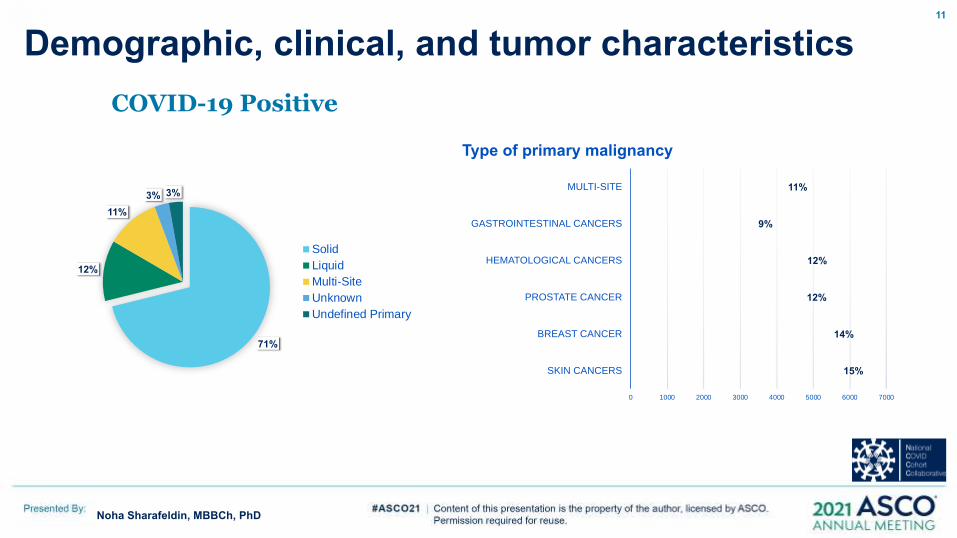
Demographic, clinical, and tumor characteristics11
Noha Sharafeldin, MBBCh, PhD
COVID-19 Positive
15%
14%
12%
12%
9%
11%
0 1000 2000 3000 4000 5000 6000 7000
SKIN CANCERS
BREAST CANCER
PROSTATE CANCER
HEMATOLOGICAL CANCERS
GASTROINTESTINAL CANCERS
MULTI-SITE
Type of primary malignancy
71%
12%
11%
3% 3%
Solid
Liquid
Multi-Site
Unknown
Undefined Primary

COVID-19 Treatment68
Noha Sharafeldin, MBBCh, PhD
COVID-19 Treatment (Yes) COVID positive (n=38,614)
Systemic antibiotics
Systemic steroids
Azithromycin
Remdesivir
Dexamethasone
Hydroxychloroquine (HCQ)
4032(15.75%)
3514(13.73%)
1197(4.68%)
1047(4.09%)
1029(4.02%)
364(1.42%)

Death and invasive ventilation in hospitalized patients
69
Noha Sharafeldin, MBBCh, PhD
Outcome COVID positive
(n=19,515)
COVID negative
(n=184,988)
Death
Invasive Ventilation
2,894 (14.8%)
1,606 (8.2%)
23,207 (12.5%)
9,576 (5.2%)

Survival Probability –by COVID status
70
Noha Sharafeldin, MBBCh, PhD
HR = 1.20 (95%CI: 1.15 – 1.24, p<0.001)

Survival Probability by cancer type among COVID positive patients
71
Noha Sharafeldin, MBBCh, PhD

Hazard ratios associated with 1-year all-cause mortality among COVID-positive patients
72
Noha Sharafeldin, MBBCh, PhD

Hazard ratios associated with 1-year all-cause mortality among COVID-positive patients
73
Noha Sharafeldin, MBBCh, PhD

Hazard ratios associated with 1-year all-cause mortality among COVID-positive patients
74
Noha Sharafeldin, MBBCh, PhD

Hazard ratios associated with 1-year all-cause mortality among COVID-positive patients
75
Noha Sharafeldin, MBBCh, PhD

76
Noha Sharafeldin, MBBCh, PhD
Limitations
• RWD Challenges (e.g. data missingness)
• Limited capture of recent cancer therapy
• Potential misclassification of cancer patients
• Challenges in primary cancer diagnosis mapping and limited historical data
• Method for construction of COVID-19 negative control

77
Noha Sharafeldin, MBBCh, PhD
Conclusions
• N3C represents a unique resource to examine effects of COVID-19 on cancer outcomes
• Largest COVID-19 and cancer cohort within the US
• Consistent with previous literature, older age, male gender, increasing comorbidities, and hematological malignancies were associated with higher mortality in patients with cancer and COVID-19
• The N3C dataset confirmed that cancer patients with COVID-19 who received recent immuno-, or targeted therapies were not at higher risks of overall mortality

78
Noha Sharafeldin, MBBCh, PhD
Acknowledgements
The Patients
US Data Partners
N3C Consortial Authors
Christopher Chute
Melissa Haendel
Amit Mitra
Ramakanth Kavuluru
NCATS U24 TR002306
NIGMS 5U54GM104942-04
NCI P30CA012197 [UT, QS]
LLS 3386-19 [NS]
Indiana University Precision Health
Initiative [JS]
N3C Core Teams

79
Noha Sharafeldin, MBBCh, PhD
AcknowledgementsWe gratefully acknowledge contributions from the following N3C core teams:• Principal Investigators: Melissa A. Haendel*, Christopher G. Chute*, Kenneth R. Gersing, Anita Walden• Workstream, subgroup and administrative leaders: Melissa A. Haendel*, Tellen D. Bennett, Christopher G. Chute, David A. Eichmann, Justin Guinney, Warren A. Kibbe, Hongfang Liu, Philip R.O. Payne, Emily R. Pfaff, Peter N. Robinson, Joel H. Saltz, Heidi Spratt, Justin Starren, Christine Suver, Adam B. Wilcox, Andrew E. Williams, Chunlei Wu• Key liaisons at data partner sites• Regulatory staff at data partner sites• Individuals at the sites who are responsible for creating the datasets and submitting data to N3C• Data Ingest and Harmonization Team: Christopher G. Chute*, Emily R. Pfaff*, Davera Gabriel, Stephanie S. Hong, Kristin Kostka, Harold P. Lehmann, Richard A. Moffitt, Michele Morris, Matvey B. Palchuk, Xiaohan Tanner Zhang, Richard L. Zhu• Phenotype Team (Individuals who create the scripts that the sites use to submit their data, based on the COVID and Long COVID definitions): Emily R. Pfaff*, Benjamin Amor, Mark M. Bissell, Marshall Clark, Andrew T. Girvin, Stephanie S. Hong, Kristin Kostka, Adam M. Lee, Robert T. Miller, Michele Morris, Matvey B. Palchuk, Kellie M. Walters• Project Management and Operations Team: Anita Walden*, Yooree Chae, Connor Cook, Alexandra Dest, Racquel R. Dietz, Thomas Dillon, Patricia A. Francis, Rafael Fuentes, Alexis Graves, Julie A. McMurry, Andrew J. Neumann, Shawn T. O'Neil, Andréa M. Volz, Elizabeth Zampino• Partners from NIH and other federal agencies: Christopher P. Austin*, Kenneth R. Gersing*, Samuel Bozzette, Mariam Deacy, Nicole Garbarini, Michael G. Kurilla, Sam G. Michael, Joni L. Rutter, Meredith Temple-O'Connor• Analytics Team (Individuals who build the Enclave infrastructure, help create codesets, variables, and help Domain Teams and project teams with their datasets): Benjamin Amor*, Mark M. Bissell, Katie Rebecca Bradwell, Andrew T. Girvin, Amin Manna, Nabeel Qureshi• Publication Committee Management Team: Mary Morrison Saltz*, Christine Suver*, Christopher G. Chute, Melissa A. Haendel, Julie A. McMurry, Andréa M. Volz, Anita Walden• Publication Committee Review Team: Carolyn Bramante, Jeremy Richard Harper, Wenndy Hernandez, Farrukh M Koraishy, Federico Mariona, Saidulu Mattapally, Amit Saha, Satyanarayana Vedula

N3C Registration/Traininghttps://covid.cd2h.org/tutorials
Training Office Hours: Tuesdays & Thursdays at 10-11 am PT/1-2 pm ET Registration Required at this link
Orientation Video Coming Soon
Additional Training Tutorials available in the Enclave
Registration for Documents, Meetings & the N3C Data Enclave
Requires Authentication
Enclave Checklist
A program of NIH’s National Center
for Advancing Translational Sciences

● N3C comprises the largest, most representative patient-level COVID-19 cohort in the US and continues to grow
● We CAN do transparent, reproducible, innovative science (including ML) on sensitive observational data at scale, together!
● N3C is an innovative partnership between clinical sites, CDM communities, NIH ICs, CD2H, and commercial partners
● Automation of data extraction and minimum requirements reduces burden and increases site participation
● Robust attribution of all contributors; also provides great venue for trainees
● N3C data is complicated, but there are many people and resources to help users do good science
Step 4. Federated Analytics with HPCTakeawaysA program of NIH’s National Center
for Advancing Translational Sciences

Register with N3C: https://labs.cd2h.org/registration/
Joining Workstreams:
N3C Data Ingestion & Harmonization Workstream
Slack Channel Harmonization
Google Group Harmonization
N3C Phenotype & Data Acquisition Workstream
Slack Channel Phenotype
Google Group Phenotype
N3C Collaborative Analytics Workstream
Slack Channel Analytics
Google Group Analytics
N3C Data Partnership & Governance Workstream
Slack Channel Governance
Google Group Governance
N3C Synthetic Clinical Data Workstream
Slack Channel Synthetic
Google Group Synthetic
N3C Implementation Workstream- Coming soon
Additional Information:
Onboarding N3C, Slack, Google | Finding and Joining a Google Group
NCATS N3C Webpage N3C Website
How to Get Involved with N3CA program of NIH’s National Center
for Advancing Translational Sciences

Melissa A. Haendel,1,4,7,8,10,13,14,52,78,101 Christopher G. Chute,1,4,8,10,13,14,52,78,100,101 Tellen D. Bennett,9,10,13,14,52,100,101 David A. Eichmann,4,9,10,13,78,101 Justin Guinney,4,9,10,14,78,101 Warren A. Kibbe,9,10,52,78,101 Philip R.O. Payne,4,9,10,78,101 Emily R. Pfaff,9,10,13,15,52,78 Peter N. Robinson,4,9,10,15,52,78,100 Joel H. Saltz,10,13,14,15,52,78,101 Heidi Spratt,9,10,100 Christine Suver,10,78,101 John Wilbanks,10,78,101 Adam B. Wilcox,10,101 Andrew E. Williams,10,13,78 Chunlei Wu,9,13,14,78
Clair Blacketer,15,52 Robert L. Bradford,9,52 James J. Cimino,10,14,101 Marshall Clark,9,15,52 Evan W. Colmenares,9,15,52 Patricia A. Francis,78 Davera Gabriel,9,10,13,14,15,52 Alexis Graves,7,9,78 Raju Hemadri,9,15,52 Stephanie S. Hong,9,15,52 George Hripscak,10,52 Dazhi Jiao,9,15,52 Jeffrey G. Klann,14,52,101 Kristin Kostka,9,15,52 Adam M. Lee,9,15,52 Harold P. Lehmann,9,15,52 Lora Lingrey,9,15,52 Robert T. Miller,9,15,52 Michele Morris,9,15,52 Shawn N. Murphy,9,15,52 Karthik Natarajan,9,15,52 Matvey B. Palchuk,9,15,52 Usman Sheikh,9,78 Harold Solbrig,9,15,52 Shyam Visweswaran,10,15,52,101 Anita Walden,7,10,13,14,52,101 Kellie M. Walters,10,14,101 Griffin M. Weber,10,101 Xiaohan Tanner Zhang,9,15,52 Richard L. Zhu,9,15,52 Benjamin Amor,78 Andrew T. Girvin,15,78 Amin Manna,78 Nabeel Qureshi,15,78 Michael G. Kurilla,10,78 Sam G. Michael,10,78 Lili M. Portilla,101 Joni L. Rutter,1,101 Christopher P. Austin,101 Ken R. Gersing,78,101
Shaymaa Al-Shukri,4,15 Adil Alaoui,101 Ahmad Baghal,15 Pamela D. Banning,15,100 Edward M. Barbour,8,15 Michael J. Becich,15,52,101 Afshin Beheshti,14 Gordon R. Bernard,8,15 Sharmodeep Bhattacharyya,100 Mark M. Bissell,9,15 L. Ebony Boulware,14,100 Samuel Bozzette,100,101 Donald E. Brown,101 John B. Buse,14 Brian J. Bush,8,101 Tiffany J. Callahan,14,52 Thomas R. Campion,8,15 Elena Casiraghi,9,15 Ammar A. Chaudhry,13,14 Guanhua Chen,9 Anjun Chen,13 Gari D. Clifford,8,15 Megan P. Coffee,14,100 Tom Conlin,14 Connor Cook,7,78 Keith A. Crandall,9,14,101 Mariam Deacy,78 Racquel R. Dietz,78 Nicholas J. Dobbins,8,9
Peter L. Elkin,15,52,100 Peter J. Embi,52,101 Julio C. Facelli,8,15 Karamarie Fecho,13 Xue Feng,9 Randi E. Foraker,8,13,15 Tamas S. Gal,8,15 Linqiang Ge,14 George Golovko,15,101 Ramkiran Gouripeddi,14,15 Casey S. Greene,13,14 Sangeeta Gupta,52,101 Ashish Gupta,13,101 Janos G. Hajagos,9,15 David A. Hanauer,15,52 Jeremy Richard Harper,9,14,52 Nomi L. Harris,14 Paul A. Harris,101 Mehadi R. Hassan,9 Yongqun He,15,52,100
Elaine L. Hill,9,14 Maureen E. Hoatlin,14 Kristi L. Holmes,4,101 LaRon Hughes,14 Randeep S. Jawa,14 Guoqian Jiang,14 Xia Jing,7,14 Marcin P. Joachimiak,8,15 Steven G. Johnson,9,14,101 Rishikesan Kamaleswaran,9,15,78 Thomas George Kannampallil,15,101 Andrew S. Kanter,15,52 Ramakanth Kavuluru,9,13,14 Kamil Khanipov,8,14 Hadi Kharrazi,9,14 Dongkyu Kim,15,52 Boyd M. Knosp,8,15 Arunkumar Krishnan,9
Tahsin Kurc,9,15 Albert M. Lai,101 Christophe G. Lambert,52,101 Michael Larionov,14 Stephen B. Lee,1,14 Michael D. Lesh,9 Olivier Lichtarge,14 John Liu,9 Sijia Liu,8,9,101 Hongfang Liu,9,15 Johanna J. Loomba,1,15,78,101
Sandeep K. Mallipattu,9,14,15 Chaitanya K. Mamillapalli,14 Christopher E. Mason,15 Jomol P. Mathew,8,15,52 James C. McClay,101 Julie A. McMurry,1,4,7,9,13,14,78 Paras P. Mehta,14 Ofer Mendelevitch,9 Stephane Meystre,8,14,15 Richard A. Moffitt,9,13,15 Jason H. Moore,8,9 Hiroki Morizono,13,14,15,52 Christopher J. Mungall,15,52 Monica C. Munoz-Torres,7,10,78 Andrew J. Neumann,78 Xia Ning,14 Jennifer E. Nyland,13,14 Lisa O'Keefe,78 Anna O'Malley,78 Shawn T. O'Neil,78 Jihad S. Obeid,10,14,15 Elizabeth L. Ogburn,13 Jimmy Phuong,9,15,52,100,101 Jose D Posada,8,15 Prateek Prasanna,14,52 Fred Prior,9,14,15 Justin Prosser,9,78 Amanda Lienau Purnell,101 Ali Rahnavard,9,52 Harish Ramadas,9,52,78 Justin T. Reese,9,10 Jennifer L. Robinson,14,100 Daniel L. Rubin,101 Cody D. Rutherford,9,101 Eugene M. Sadhu,8,15 Amit Saha,9 Mary Morrison Saltz,15,52,101 Thomas Schaffter,78 Titus KL Schleyer,14 Soko Setoguchi,8,14,15 Nigam H. Shah,8,14 Noha Sharafeldin,14 Evan Sholle,15,52 Jonathan C. Silverstein,15,52,101 Anthony Solomonides,101 Julian Solway,14,101
Jing Su,101 Vignesh Subbian,9,52,101 Hyo Jung Tak,15 Bradley W. Taylor,9,14 Anne E. Thessen,14,101 Jason A. Thomas,15 Umit Topaloglu,15,52 Deepak R. Unni,8,9,15,52 Joshua T. Vogelstein,14 Andréa M. Volz,7 David A. Williams,14,15 Kelli M. Wilson,9,78 Clark B. Xu,8,9,15 Hua Xu,9,10,14 Yao Yan,9,15,52 Elizabeth Zak,8,15 Lanjing Zhang,101 Chengda Zhang,14 Jingyi Zheng,14
1CREDIT_00000001 (Conceptualization) 4CREDIT_00000004 (Funding acquisition) 7CRO_0000007 (Marketing and Communications) 8CREDIT_00000008 (Resources) 9CREDIT_00000009 (Software role) 10CREDIT_00000010 (Supervision role) 13CREDIT_00000013 (Original draft) 14CREDIT_00000014 (Review and editing) 15CRO_0000015 (Data role) 52CRO_0000052 (Standards role) 78CRO_0000078 (Infrastructure role) 100Clinical Use Cases 101Governance
https://academic.oup.com/jamia/advance-
article/doi/10.1093/jamia/ocaa196/5893482

Questions or Comments?

Thank you! Thank you!
A program of NIH’s National Center
for Advancing Translational Sciences