the neuro-infectious diseases - ulbmedecine.ulb.ac.be/ftpupload/dec13_syndic_neuro_ucl.pdf ·...
TRANSCRIPT
The Neuro -Infectious Diseases
C.J.M. SINDICLaboratory of Neurochemistry53-59 Avenue Mounier1200 Bruxelles

Haematogenous
- Coxsackie, echo, polio,mumps
- in monocytes : HIV
- in lymphocytes : JC virus
- in red blood cells : plasmodium
-Nesseiria meningitidis, Streptococcus pneumoniae, Listeria,Mycobacterium tub.,Nocardia
- Cryptococcus, Candida,Aspergillus
- Larvae
- Olfactory nerve(Herpes simplex)
- by proximity : nose,ears, sinusesBacteria, fungi,mucormycosis
- Trigeminal nerveherpes simplex,herpes zoster
-peripheral nervesrabiesBorreliaherpes zosterherpes simplex

Infectious muscle diseases
1) viral polymyositis with myalgiagroup B coxsackie, influenza, Epstein-Barr
2) Borrelia burgdorferi myositis
3) parasitic myositis� cysticercosis : calcifications in association with
neurocysticercosis� trichinosis : encysted larvae of Trichinella spiralis
weakness mainly in the cranial muscles(tongue, masseters, extra-ocular andpharyngeal muscles)
� eosinophilia, serum antibodies, muscle biopsy if requ ired


Peripheral nerves
� infectious mononeuropathy or multiple neuropathiesleprosy, HIV, hepatitis C virus, Borrelia burgdorferi� EMG, biopsy, CSF
� plexopathypara-infectious or post-vaccinal (Parsonage Turner syndrome)(Epstein-Barr Virus)� EMG, seldom CSF analysis, MRI
� polyneuropathiesacute idiopathic polyradiculoneuritis or Guillain-Barre syndromepost-infectious in 2 cases out 3 (mainly, CMV and Campylobacter jejuni)� EMG, CSF
Leprosy-related neuropathies
� “Mycobacterium leprae” is an obligatory intracellular organism
� no culture possible
� the nasal mucosa is the preferential site of entry an d exit of
the bacillus
� the oral mucosa is the secondary site of transmission
and infection
� worldwide, the detection of new cases is decreasing
from about 515,000 in 2003
to 245,000 in 2007

Leprosy-related neuropathies
Leprosy can be classified into three major clinical su btypes based
on the extent of host immune response :
� lepromatous (multibacillar) : predominant humoral resp onse
� tuberculoïd (paucibacillar) : predominant cell-mediat ed
immune response
� borderline (in- between)
Leprosy-related neuropathies
� about 4 – 10 % of patients with leprosy could have a pure
neural involvement
� nerve involvement may affect sensory, motor and auton omic
fibers
� granulomatous inflammation may cause palpable enlarge ment
� the posterior tibial nerve is the most commonly affect ed,
causing anesthesia on the soles of the feet, follow ed by the
ulnar, median, lateral popliteal and facial nerves (1 7 %)
� nerve biopsy is often required for the diagnosis

02

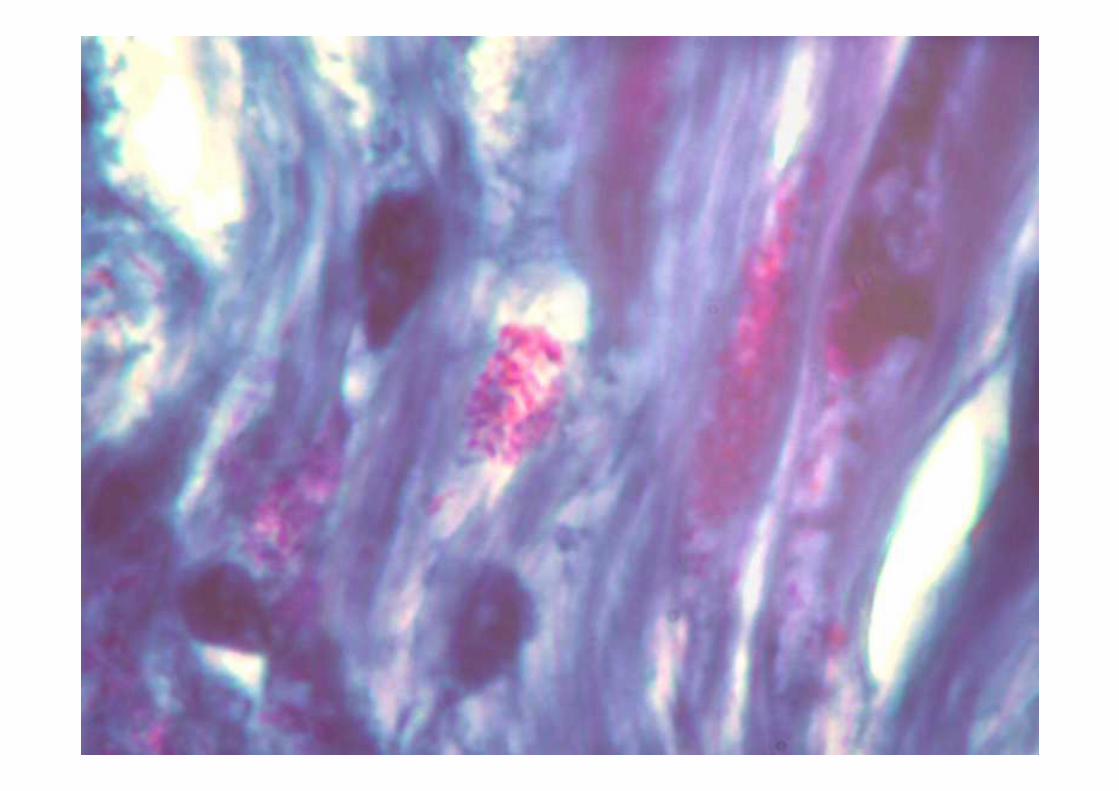
Case report : Leprosy in Belgium !
1993 - skin, brown lesion, right arm : « sarcoidosis » after biopsy
- glucocorticoids, good outcome
1998 - skin lesion in the left leg; fatigue, fever, weigh t loss (10 kgs)- glucocorticoids, good outcome
2001 - fatigue, fever, high CRP levels, recurrent skin le sions- glucocorticoids, good outcome
June 2001- nose involvement, epistaxis, oedema, ulcers, pares thesiae
in the legs, skin nodules, « dermitis »- muscle reflexes OK but pure sensory axonal
polyneuropathy- thermoanalgesia below the knees
� Nerve biopsy : typical globiZiehl/Auramine +PCR +
Trip in Tunisia, Greece, Thaïland ...


Hepatitis C virus-related neuropathies
� the most frequent extrahepatic manifestation of HCV infection
is cryoglobulinemia, present in up to 50 % of patien ts
� in patients with HCV-associated cryoglobulins, perip heral
neuropathy occurs in 26 to 86 % in function of the di agnostic
criteria used
� HCV-related neuropathies may occur in absence of
cryoglobulinemia
� physiopathology is quite heterogeneous: ischaemic in jury,
immune complexes, HCV-induced autoimmune mechanisms

HIV-related neuropathies
� peripheral neuropathy has become the major neurological
complication of HIV infection in the developed world
� distal sensory neuropathies are the most frequent and have two
different causes resulting in similar signs and symp toms:
-a primary HIV-induced neuropathy
-an anti-retroviral toxic neuropathy, especially seconda ry to the
use of reverse transcriptase inhibitors (didanosine, za lcitabine,
stavudine)

HIV-related neuropathies
� in both cases, the main symptom is a neuropathic pai n defined
as burning or aching sensations in the feet, paresthes ia, allodynia,
beginning in the toes and the soles of the feet
� neurological signs consist of absent or reduced ankle deep
tendon reflexes, and loss of pinprick, temperature or vibratory
sensations in the lower limbs
� in a prospective cohort of 2141 patients, the rate of
asymptomatic neuropathy was 32.1 % at 3 years, and of
symptomatic neuropathy, 8.6% (Evans et al, AIDS, 201 1,25:919-928)

Meningo -radiculitis
� usually, meningeal signs and symptoms are slight an dmay be overlooked
� heavy pain with nocturnal increase in a radicular distribution
� cranial nerves may be preferentially involved,especially the facial nerve,
herpes zoster, sometimes “sine herpete”herpes simplex type 2 (caudal neuritis; sciatalgia)HIVBorrelia burgdorferi
� CSF analysis is mandatory

Varicella zoster virus
� it causes chickenpox (varicella), becomes latent in the cranial
nerve and dorsal root ganglia, and may reactivate anywh ere on
the body several decades later
� the lifetime risk of herpes zoster (shingles) is estim ated
to be 10-20 %
� shingles is characterized by unilateral radicular pain and
a vesicular rash limited to one to three contiguous d ermatomes

Figure 1 Characteristic varicella-zoster virus and herpes simplex virus–1 rashVaricella-zoster virus reactivation is manifest by dermatomal skin l esions (left), while herpes simplex virus
reactivation is manifest by mucosal or patchy skin lesions (right).
Nagel M A , and Gilden D Neurol Clin Pract 2013;3:1 09-117
© 2013 American Academy of Neurology

Figure 2 With a decline in varicella-zoster virus–s pecific cell-mediated immunity, virus reactivates from ganglionic neurons and spreads per ipherally or centrally to cause
diseasePeripheral spread to the skin causes herpes zoster.
Nagel M A , and Gilden D Neurol Clin Pract 2013;3:1 09-117
© 2013 American Academy of Neurology

Neurological complications of shingles
� postherpetic neuralgia : a neuropathic pain syndrome th at
persists more than three months after the dermatomal r ash has
healed
� PNS complications :
• cranial neuropathies (ophthalmic zoster, Ramsay Hun t syndrome)
• motor neuropathies
• bladder and bowel dysfunction
� CNS complications :
• meningitis
• myelitis
• vasculitic encephalitis
THESE COMPLICATIONS MAY OCCUR IN ZOSTER SINE HERPETE

Herpes zoster oticus or Ramsay-Hunt syndrome
Features may include ipsilateral facial palsy, tinnit us, hearing loss,
hyperacusis, vertigo, dysgueusia, decreased tearing an d ear pain
Vesicles may appear before (60%), simultaneously (25 %) or after
(15 %) the facial nerve palsy

The CSF in Herpes zoster oticus
In a series of 9 consecutive cases of Ramsay Hunt
syndrome observed in our Department, the CSF showed
• a pleocytosis in 8 cases
• a positive PCR for VZV DNA in 6 cases
Grégoire et al, JNNP, 2006,77:938-942

Figure 3 Varicella-zoster virus vasculopathy and my elopathy on MRI(A) Varicella-zoster virus (VZV) vasculopathy is characterized by deep-seated lesions, typically at gray–white matter
junctions (arrows).
Nagel M A , and Gilden D Neurol Clin Pract 2013;3:1 09-117
© 2013 American Academy of Neurology
Zoster sine herpete
� in the absence of rash, disc herniation or other compres sive
causes, a painful sciatica, cruralgia or any other radi cular pain
requires an analysis of the CSF including VZV PCR an d detection
of intrathecal synthesis of anti-VZV antibodies
� in case of suspected CNS vasculitis, CSF analysis s hould also
include VZV PCR and anti-VZV antibodies

Neurosyphilis and Neuroborreliosis
Neurosyphilis and neuroborreliosis:
• Both are spirochetal infectious diseases
• Both induce an aseptic meningitis after the primary infection, which heals
spontaneously in most cases; a meningoradiculitis s yndrome with nocturnal
heavy pain predominates in neuroborreliosis
• Both may cause a meningovascular disease with acute stroke
• Both may be responsible for a chronic CNS infection with focal signs,
dementia, seizure…
• The CSF is always abnormal, with a predominant intr athecal IgM antibody
response, pleocytosis, and specific oligoclonal IgG bands

Neurosyphilis
Clinical presentations:
• Neuropsychiatric disorders: psychosis, delirium, de mentia (50%)
• Acute stroke with focal neurological deficit (15%)
• Ocular: uveitis, visual loss, optic nerve dysfuncti on (12%)
• Myelopathy (9%)
• Seizure (9%)
• Brain stem/cranial nerves (5%)

Neurosyphilis
Diagnosis:
• Positive CSF VDRL (Venereal Disease Research Labora tory) test
OR
• Positive anti-FTA antibody index and
•Abnormal CSF count
•Intrathecal IgM synthesis
•CSF specific oligoclonal IgG bands

Neuroborreliosis
Lyme neuroborreliosis:
• Sindic CJM et al, JNNP, 1987,50:1565-1571 (18 MR ca ses)
• Depré A et al, Rev Neurol,1988,144:416-420 (2 ME cas es)
• Montaigne P. et al, Rev Neurol,1994,150:75-77 (névr ite du grand dentelé)
• Van Snick S. et al, Acta neurol Belg, 2008,108:103- 106 (pontine stroke)
• Charles V. et al, JNNP, 2007 (polio-like)
• Sindic C. Infectious neuropathies Curr. Opin Neuro l, 2013,26:510-515


Neuroborreliosis
In Lyme neuroborreliosis with CNS involvement,
• a mononuclear pleocytosis is constant
• an impairment of the blood-CSF barrier is the rule
• an intrathecal immune response occurs after few day s (> 10 days),
characterized by :
�a predominant IgM response (in percentage of the in trathecal fraction)
�the presence of oligoclonal IgG bands with anti-Bo rrelia activity
�an associated, minor, polyspecific immune response
� the 41 kDa flagellar antigen is the most important epitope.
� this immune response may persist for years (up to 2 0) as an immune
scar, even in seronegative patients

Borrelia induced facial palsy (Lyme disease)
• Summer months (May - October)
• more frequently in children, with general signs (fe ver, pain)
• frequently bilateral
• CSF almost always abnormal in our hands (pleocytosis, local IgM synthesis, oligoclonal IgG bands)


Borrelia burgdorferi myelitis


Gadolinium +



Meningitis
� severe headache, stiff neck, nausea and vomiting,photophobia, phonophobia, feverdrowsiness and confusion make difficult to distingui sha pure meningitis from meningoencephalitis
� viral infections : enteroviruses (echo, coxsackie, pol io), mumps,herpes simplex type 2, Epstein-Barr, herpes zoster, aden ovirus,HIV, lymphocytic choriomeningitis
� bacterial infections : streptococcus pneumoniae, Nes seriameningitidis, Haemophilus influenzae, Listeria mono cytogenes,other Gram -bacilli, Streptococcus suis (Hantson et al, ANB, 1 991)…Mycobacterium tuberculosis
� spirochetal infections : syphilitic meningitis, neuro borreliosis,leptospirosis
� fungal infections : Cryptococcus, Candida, Aspergil lus, Mucor
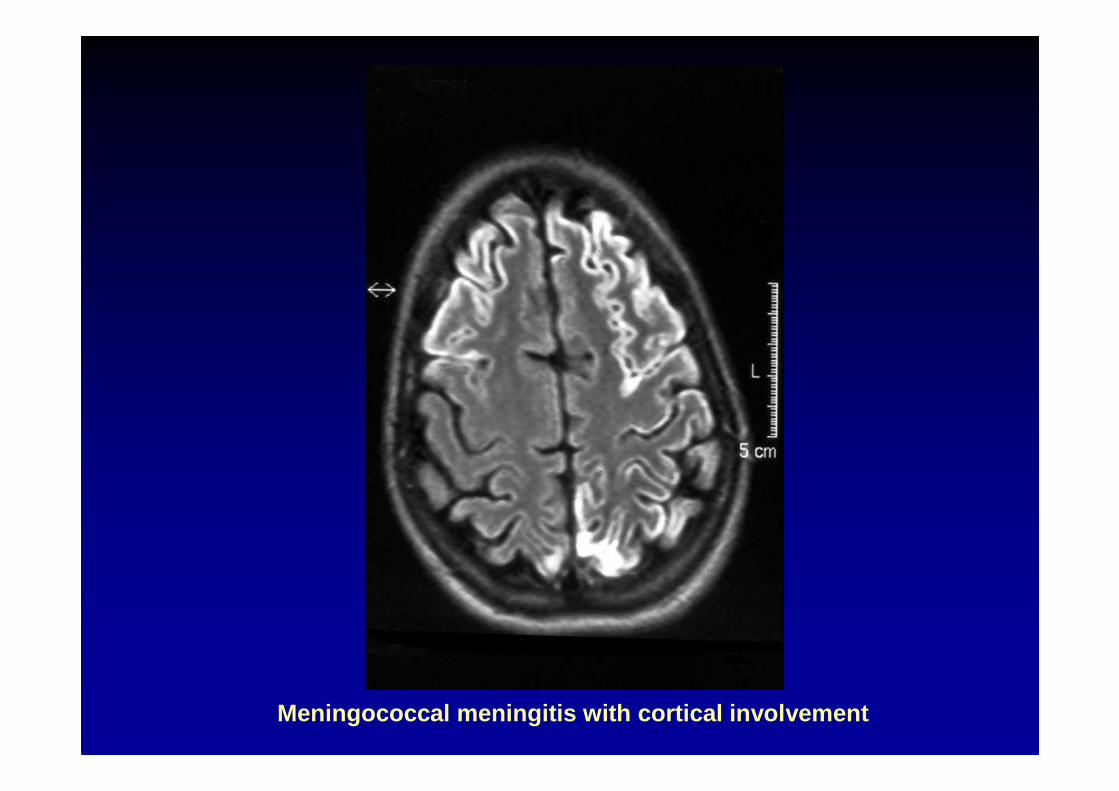
Meningococcal meningitis with cortical involvement

PCR of infectious DNA in CSF is a very
important tool for diagnosis of many,
but not all, CNS infections

Sensitivity and specificity of PCRfor selected CNS infections
Pathogen Sensi tivity (%) Pathogen Sensi tivity (%) Specificity (%)Specificity (%)
HSV type 1HSV type 1 > 95> 95 100100CMVCMV 80 80 -- 100100 75 75 -- 100100VZVVZV unknownunknown 100100EBVEBV 9797 100100JC virusJC virus 74 74 -- 9292 92 92 -- 9696EnterovirusEnterovirus 9797 100100
Borrelia burgdorferiBorrelia burgdorferi 40 40 -- 5050 95 95 -- 100100(Ab : > 95%)(Ab : > 95%)
Mycobacterium tuberculosisMycobacterium tuberculosis 60 60 -- 9090 94 94 -- 100100

THE QUANTIFICATION OF AN INTRATHECAL SYNTHESISOF ANTIBODIES IS BASED ON :
� the calculation of a CSF/serum antibody quotient (Qab) after ELISA determination on a continuousscale (arbitrary units)
� the use of an antibody index : Q ab/QIgG
� the use of a correction factor , Q Limit ,if Q IgG > QLimit (Reiber and Lange, Clin. Chem., 1991, 37 : 1153-1160)

Méningite à Herp ès simplex type 2
� tout patient qui présente des signes et des symptôm esméningés dans le décours d’un herpès génital estsuspect de m éningite à herpes simplex type 2
� à l’inverse, tout patient présentant une m éningite viraledoit être examiné pour la présence d’un herpès génit al
� cependant, une m éningite à herpes simplex type 2 peutsurvenir en l ’absence d’une anamnèse d’herpèsgénital, et sans lésion herpétique concomitante

Méningites lymphocytaires récidivantes
� Herpes simplex type 2 est la cause la plus fréquent edu syndrome de m éningite lymphocytaire bénignerécidivante, appelée aussi m éningite de Mollaret
� la PCR pour l’ADN de herpes simplex type 2 estpositive dans le LCR, dans 75 à 85 % des cas
� une synthèse intra-thécale d’anticorps anti-herpèssimplex est quasi constante.
Le diagnostic des m éningites tuberculeuses
1. Suspicion clinique
Signes m éningés, fièvre et altération du niveau de conscience(confusion, somnolence)
AVEC un CT scan ou une IRM anormaux
- prise de contrastes méningé dans les scissures de Sy lvius et les
citernes de la base
- une hydrocéphalie
ET/OU des radiographies du thorax suggestives de tubercul ose
ET/OU un LCR avec pléocytose lymphocytaire, hyperprotéino rachie,hypoglycorachie

Le diagnostic des m éningites tuberculeuses
2. Confirmation microbiologique
� culture positive du LCR
� examen direct positif (Ziehl)
� détection par PCR du génome de Mycobacteriumtuberculosis dans le LCR
� synthèse intrathécale d ’anticorps anti-mycobactéries


Monteyne and Sindic, Acta Neurol. belg. 1995, 95 : 80-87

Tuberculomas in cerebellum and brainstem

lanes 1,2,3 : same patient; samples before, 2 weeks and 3 months after treatment
lane 4 : another case of TB meningitis
lanes 5,6 : controls
Fungal infections of the CNS
1. Cryptococcus neoformans
meningitis, encephalitis
2. Candida albicans
meningitis, encephalitis
3. Aspergillus fumigatus
meningitis (biopsy !) (van de Wyngaert et al, J.Neu rol, 1986)
4. Mucormycosis
meningitis, vasculitis (biopsy !) Dusart et al, ANB, 2013)
lymphocytic or neutrophilic chronic meningitis !
CSF-specific oligoclonal bands are frequently observ ed!

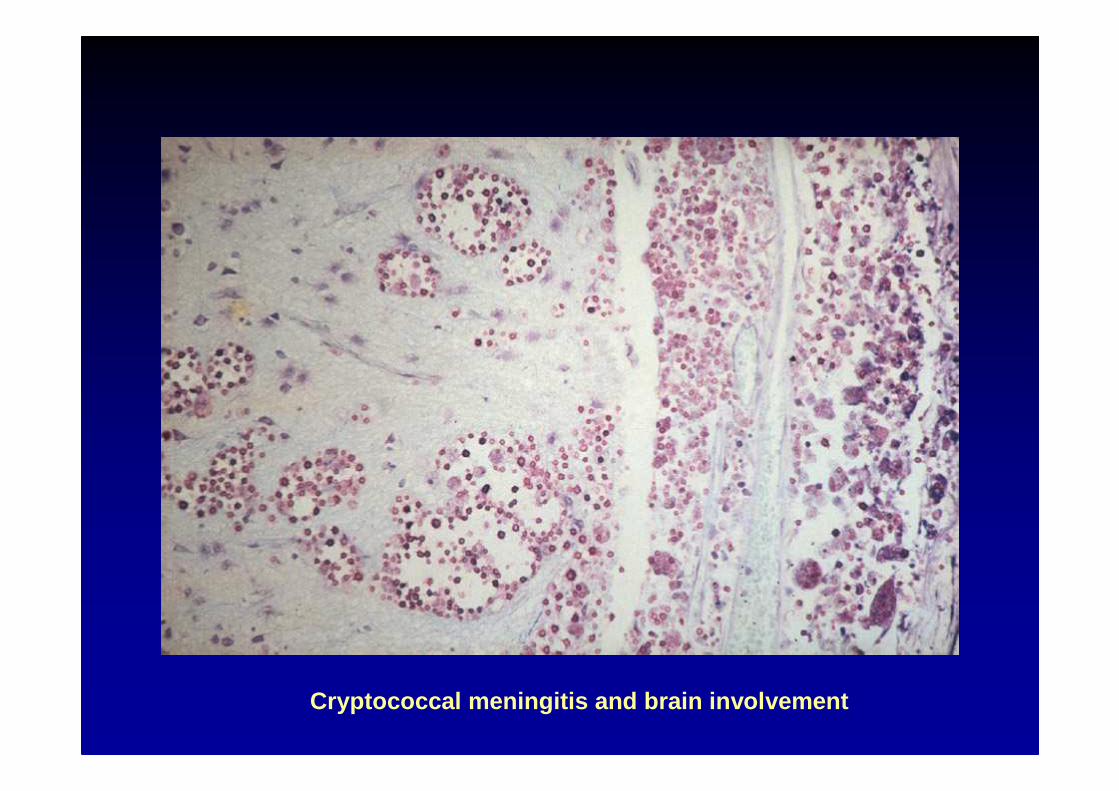
Cryptococcal meningitis and brain involvement

Cryptococcal meningitis and brain involvement

Candida albicans encephalitis

Clinical history
• G.N. , 64 year-old, retired, civil engineer
• Medical past history :
– 1985 : somatotropic pituitary macroadenoma
treated by transsphenoidal surgery and
radiotherapy � anterior pituitary deficiency.
– Pulmonary tuberculosis (recurrence in 2001,
during a travel in Congo)
Dusart A. et al, ANB, 2013, 113:179-184

Timeline
Right hemifacial pain
Right nasal
obstruction
Right hemifacial pain
Right nasal
obstruction
Diplopia
Right VIth nerve
partial palsy
Diplopia
Right VIth nerve
partial palsy
11.2006 01.2007 05.200703.2007 06.2007 08.2007
Appearance of
archaïc reflexes
Appearance of
archaïc reflexes
Cognitive
decline
Cognitive
decline
Meningeal signsMeningeal signs
Fluctuating
consciousness
Fluctuating
consciousness
Bradypsychia
Incontinence
Bradypsychia
Incontinence
Sphenoïd
sinusitis
Sphenoïd
sinusitisCarotid
Pseudoaneurysm
Carotid
Pseudoaneurysm Carotid and
aneurysmal
thrombosis
Carotid and
aneurysmal
thrombosis
Radiologic
statu quo
Radiologic
statu quoHydrocephalus
Pachymeningitis
Thalamic ischemia
Pansinusopathy
Hydrocephalus
Pachymeningitis
Thalamic ischemia
Pansinusopathy
CSF : 16c/µl, (ly),
P : 76mg/dl,
G : 44mg/dl, BO (-)
CSF : 16c/µl, (ly),
P : 76mg/dl,
G : 44mg/dl, BO (-)
CSF : 62c/µl (ne),
P : 131mg/dl
BO (+)
CSF : 62c/µl (ne),
P : 131mg/dl
BO (+)
CSF: 22c/µl (ne),
P : 186mg/dl,
BO (++)
CSF: 22c/µl (ne),
P : 186mg/dl,
BO (++)
VIth nerve
complete palsy
VIth nerve
complete palsyRight trigeminal
hypoesthesia
Right trigeminal
hypoesthesia

Evolutive sphenoid sinusitis
T2-weighted images (coronal sections) : evolution of the sphenoid sinusopathy between December 2006 and
February 2007. Hyperintense mucous thickening evolving to a submucous oedema of sphenoid sinus. Ethmoid
and frontal sinuses seem initially normal but are only partially seen. Hemifacial pain can be explained by the
sphenoid sinusopathy as well as by a trigeminal nerve invasion/inflammation or compression in the cavernous
sinus.

T1-weighted images (coronal
sections) : occurrence of a
large and irregular
pseudoaneurysmal dilatation
of the right intracavernous
internal carotid.

Right internal carotid pseudoaneurysm
Brain CT angiography (transversal and coronal sections) : voluminous right internal carotid pseudoaneurysm

MRI angiography and FLAIR-weighted images : mucormycotic thrombosis of the right internal carotid
pseudoaneurysm. Preservation of middle cerebral artery flow via the posterior communicant cerebral
artery. No acute ischemic lesion was seen in diffusion-weighted images..
May 2007May 2007

Spontaneous occlusion of the carotid
pseudoaneurysm
T1 and T2-weighted images (coronal sections) : enhancing of the pituitary mass
involving cavernous sinus. Thrombosis of the large carotid aneurysm
May 2007May 2007

T1, post-gadolinium
T1 and FLAIR
weighted images
(transversal
sections) :
progression of
hyperintense lesions
of the skull base
with meningeal
enhancing
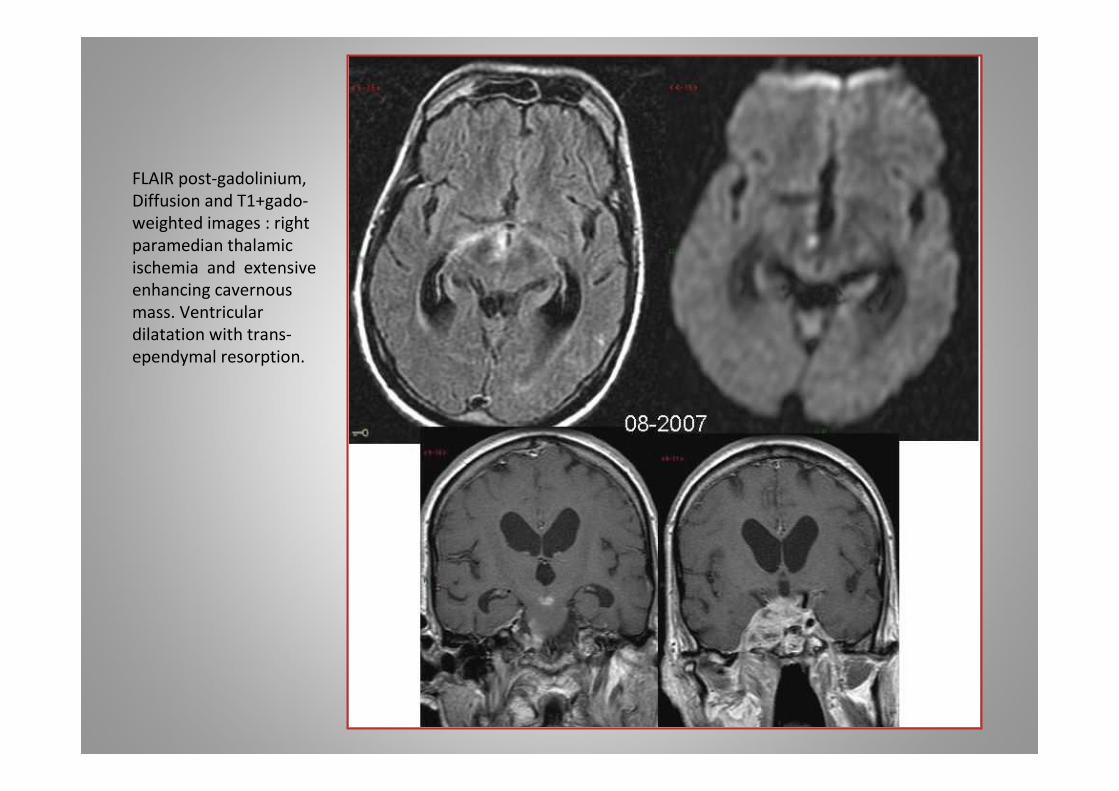
FLAIR post-gadolinium,
Diffusion and T1+gado-
weighted images : right
paramedian thalamic
ischemia and extensive
enhancing cavernous
mass. Ventricular
dilatation with trans-
ependymal resorption.
Autopsy
• Microscopic findings :
– Purulent invasion of pituitary area:
• Cellular debris
• Polymorphonuclear neutrophilic infiltrate
• Inflammatory infiltrate of vessel wall
– Presence of wide and irregular hyphae with some right-angle branchings
– Hyphae are found in vessel wall and in intravascular thrombi
– Meningeal inflammation

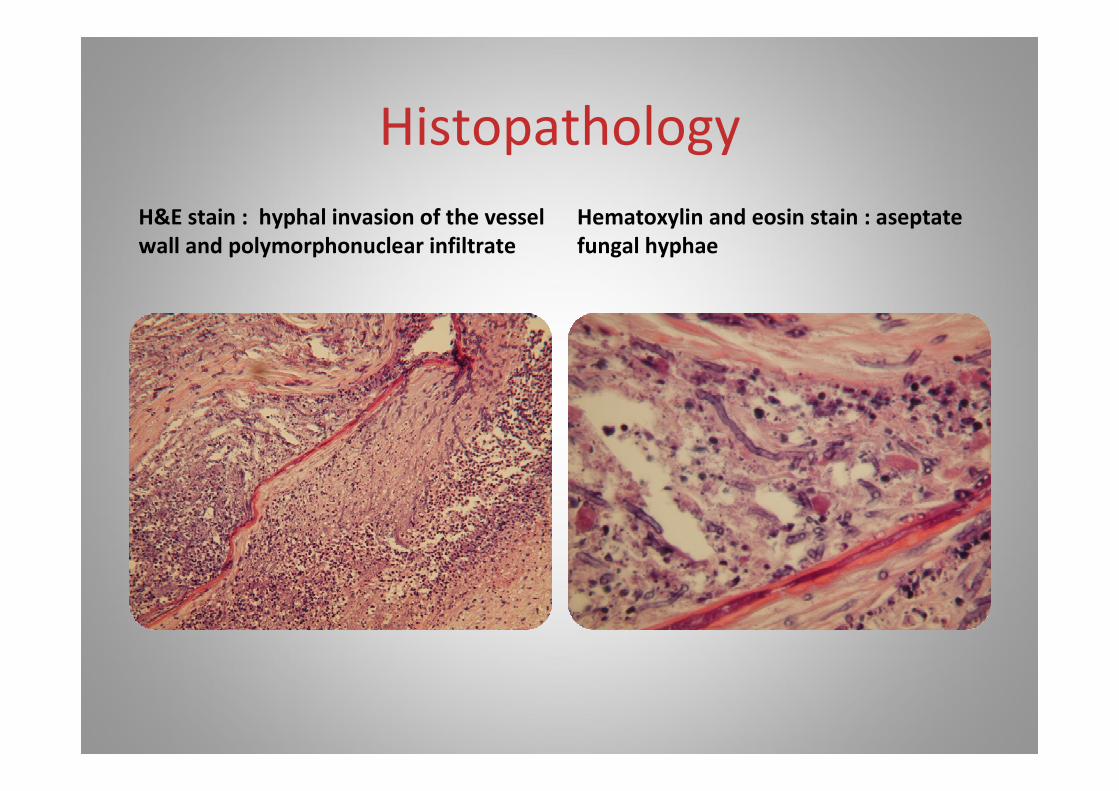
Histopathology
PAS : intravascular mucorthrombus and
necrotic debris in the vessel wall
Periodic acid schiff stain : right-
branching, irregular, thin-walled hyphae
Histopathology
H&E stain : hyphal invasion of the vessel
wall and polymorphonuclear infiltrate
Hematoxylin and eosin stain : aseptate
fungal hyphae
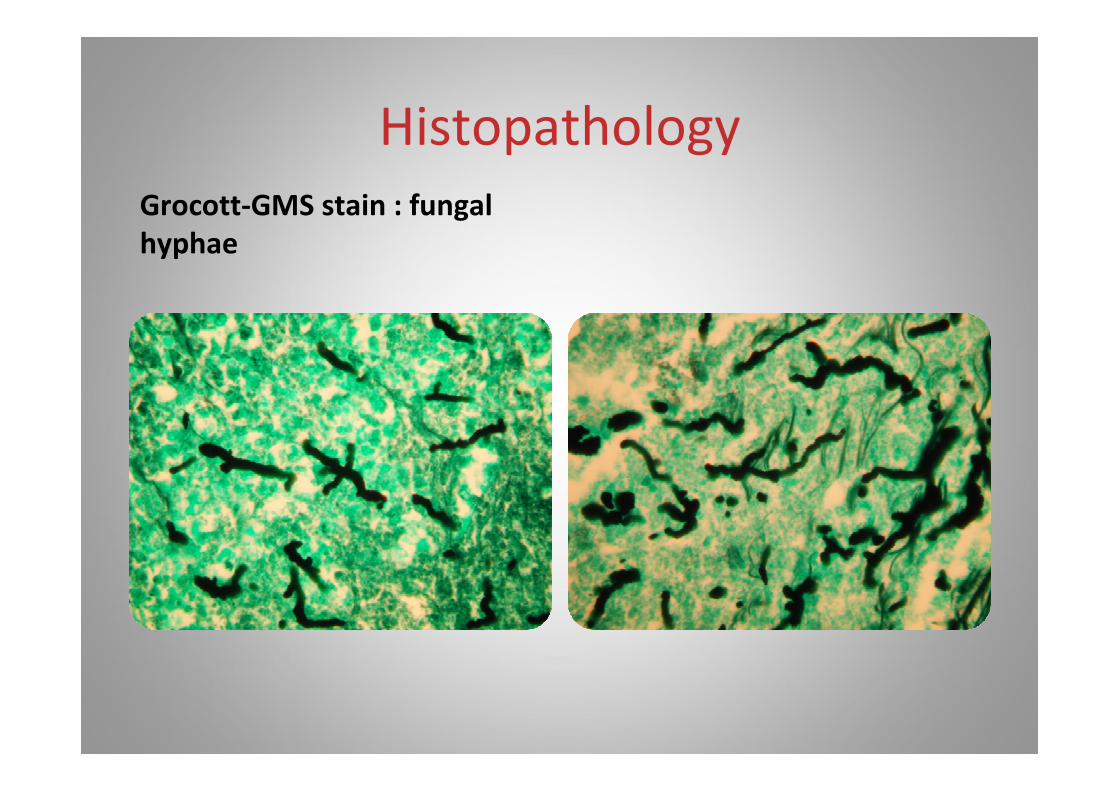
Histopathology
Grocott-GMS stain : fungal
hyphae

Myelitis
� poliomyelitis : injury of anterior horn cellspolio, some arboviruses
�myelitis with long tracts involvement
Viral : herpes simplex, herpes zoster, HIV, HTLV-I
Spirochetal : Borrelia, Treponema pallidum
Parasitic : schistosomiasisToxocara
Para-infectious : EBV, Mycoplasma pneumoniae
� spinal MRI, CSF

Duprez et al, Neuroradiology, 1996, 38 : 792-795

Goffette et al, Eur. J. Neurology, 2000, 7 : 703-70 6

Schistosomiasis

GADO +
FLAIR
CEREBRAL SCHISTOSOMIASIS
Rommel et al, Acta Neurol. Belg.
2005, 105, 89-93

GADO +

GADO +
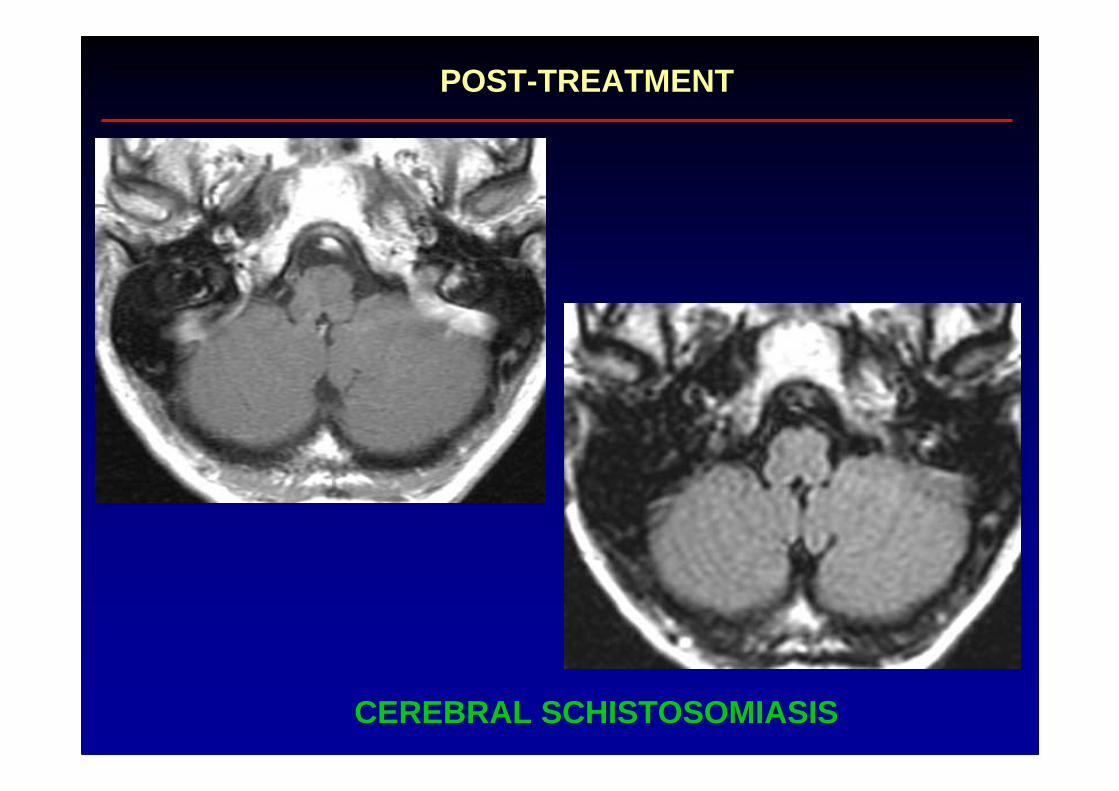
CEREBRAL SCHISTOSOMIASIS
POST-TREATMENT
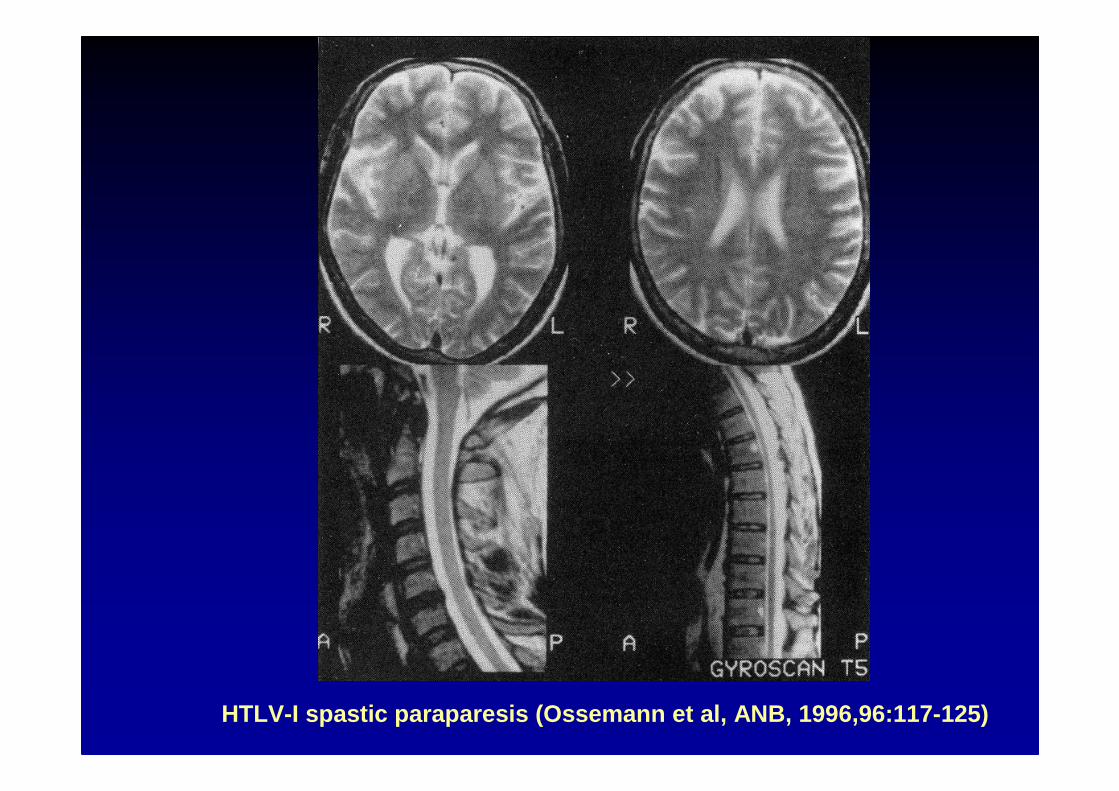
HTLV-I spastic paraparesis (Ossemann et al, ANB, 19 96,96:117-125)

HTLV-I infection
A-B : September 89 C-D : September 93

Acute Viral Encephalitis
a febrile illness expressed by meningitis, to which areadded in various combinations :
confusion, stupor, comaseizuresmutism, aphasia, hemiparesis, ataxiacranial nerve palsies
except for herpes simplex encephalitis, viral encep halitis are seasonal and occur in epidemic form (arboviruse s, such as Eastern, Western, and Venezuelan equine, St Louis, West Nile…)
� MRI, CSF, serology

Virus responsables d ’enc éphalites primaires
� Rage : • mortalité > 99 %� Herpes simplex : • mortalité > 70 % en absence de
virus traitement� Arbovirus : • mortalité de 1 à 50 % (dépend du virus et
de l ’âge de l ’hôte)� Oreillons : • encéphalites peu sévères� EBV, CMV, : • encéphalites rares et peu sévères,
HHV-6 lors de la primo-infection� Adénovirus : • encéphalites très rares; sévères chez
l ’enfant et l ’immunodéprim é� Coxsackie : • encéphalites rares, parfois fatales che z le
nouveau-né
Subacute or chronic encephalitis
� Viral : HIVencephalitis related to immunodeficiency states : CM V,
Herpes zoster, papovavirus (PML)
�Tuberculoma, brain abscesses
� Parasitic : neurocysticercosistrypanosomiasiscerebral malariatoxoplasmosisechinococcosis
� Fungal : cryptococcosis, candidiasis
� Spirochetal : tertiary Lyme disease, late neurosyphilis

NEURO-AIDS
� Primary infection: stade A
� Headache (50%) and aseptic meningitis (20-25%)
� Meningo-radiculitis (with facial palsy)
� Acute polyradiculoneuritis (Guillain-Barrésyndrome)
� Acute encephalitis with psychosis (rare)
NEURO-AIDS
� Latent infection: stade B
� Recurrent shingles
� Chronic aseptic meningitis
� Intrathecal synthesis of anti-HIV antibodies (Bukasa et al, ANB, 1988,51:1063-1068)
NEURO-AIDS
� Stade C
� C1: opportunistic CNS infections: toxoplasmosis, PML, cryptococcal meningitis, tuberculous meningitis, CMV encephalitis
� C2: CNS lymphoma
� C3: HIV-related chronic encephalitis, HIV-related neuropathies, vacuolar myelopathy


CMV encephalitis in a AIDS patient

Toxoplasma gondii abscess

Putative Toxoplasma abscesses in a HIV-positive pat ient


Progressive multifocal leukoencephalopathy (PML)
or
JC virus encephalitis

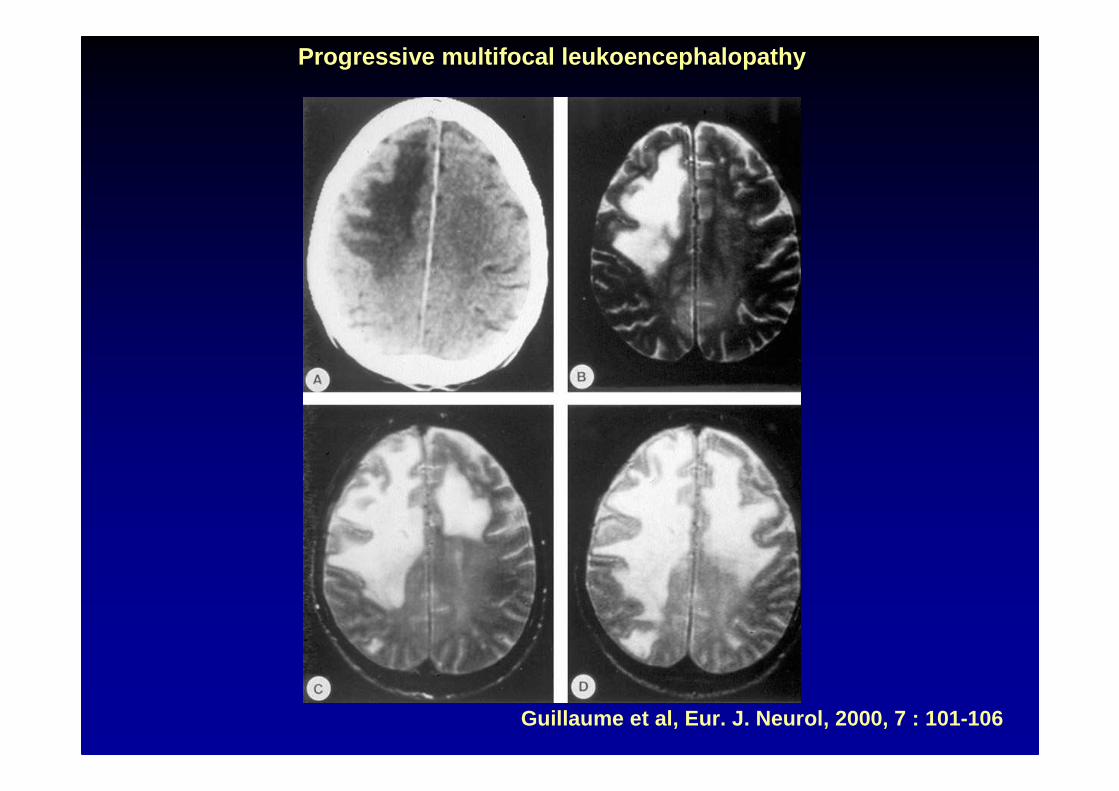
Guillaume et al, Eur. J. Neurol, 2000, 7 : 101-106
Progressive multifocal leukoencephalopathy

Progressive Multifocal Leukoencephalopathy (1)(PML)
�described in 1958 by Astrom, Mancall andRichardson in 2 CLL and 1 Hodgkin ’s diseasepatients
� papova virus-like particles in oligodendrocytesnuclei
� isolation of the virus in 1971 from the brain of a patient with Hodgkin’s disease (JC)

�The brain biopsy : the gold standard for diagnosis ofPML challenged by JCV DNA detection in the CSF(PCR)1°) JCV-infected oligodendrocytes with enlarged nucl ei
confirmed by immunochemistry for polyomavirus proteins or in situ by hibridization for JCV DNA
2°) reactive gliosis with enlarged astrocytes, some harboringa non-lytic JCV infection
3°) lipid-laden macrophages phagocyting myelin
Progressive Multifocal Leukoencephalopathy (3) (PML)

Associated diseases :N = 61 between 1996 to 2003 :
80 % with AIDS and highly active antiretroviraltherapy (HAART)
13 % with haematological malignancies
5 % with transplantation
2 % with chronic inflammatory diseases
Koralnick et al, NEJM, 2004,350:1882-1893
Before HAART : AIDS was the underlying disease in 87 % of PML cases
Progressive Multifocal Leukoencephalopathy (4) (PML)
Associated diseases in HIV-negative patients:N = 58 between 1957 and 2005 (Mayo Clinics) :
55 % with haematological malignancies15 % with chronic inflammatory diseases9 % with sarcoidosis
7 % with transplantation
7 % with other conditions (cirrhosis, pulmonaryfibrosis)
7 % without predisposing illness except for agebetween 66-80 y.
Aksamit, The Neurologist, 2006
Progressive Multifocal Leukoencephalopathy (5) (PML)

Classical signs and symptoms :subacute neurological deficits� hemiparesis or monoparesis� altered mental status� appendicular or gait ataxia� hemianopsia� diplopia� other symptoms mimicking a cortical disorder
aphasiacortical blindness
seizures (18%)
sparing of the optic nerves and the spinal cord
Progressive Multifocal Leukoencephalopathy (6) (PML)

Classical disease course :
� progressive and death within a few months� few patients experience disease stabilization and
prolonged survival� before HAART, only 10 % of HIV-positive patients wit h
PML lived for more than a year� with HAART, 1-year survival has increased to 50 %
but in case of survival, there is no remyelination neurological sequelae are severe
Progressive Multifocal Leukoencephalopathy (7) (PML)

Classical MRI lesions :� hypodense areas on CT scans� hypointense on T1-weighted images� hyperintense on T2 and FLAIR images� well demarcated, not contrast-enhancing, not
surrounded by oedema, without substantial masseffect
Lesions are usually bilateral, asymmetric, localized i n the subcortical hemispheric white matter
The posterior fossa and the deep gray structures (basa l ganglia and thalamus) are affected in up to 55% of cases
PML can also rarely present initially as a single les ion
Progressive Multifocal Leukoencephalopathy (8) (PML)

Diagnosis
�brain biopsy : sensitivity of 64 to 96 %specificity of 100 %
�CSF PCR : sensitivity close to 100 %specificity of 100 %
Progressive Multifocal Leukoencephalopathy (11) (PML)

About the JC virus
� a small DNA virus (5100 bp), in a capsid constituted by 3 proteins (VP1, VP2, VP3)
� asymptomatic seroconversion of JCV occurs usually inchildhood, but seroprevalence continues to increase untilthe seventh decade of life
� JCV can be found in the urine samples of approximatel y30 % of people, regardless of their immune status
� the primary infection could occur through urine-oralcontamination
Progressive Multifocal Leukoencephalopathy (12) (PML)

About the JC virus
� after primary infection, the virus remains latent in th ekidneys and in lymphoid organs (tonsils, bone marrow)latency in the brain ? In normal digestive system ?
� profound cellular immunosuppression leads toreactivation with JC viremia :
- rare in healthy individuals
- in 20-40 % of HIV-positive patients
- in 60-80 % of PML patients
B cells are the main blood cells carrying JCV
Progressive Multifocal Leukoencephalopathy (13) (PML)
Treatment� there is no specific treatment
� optimization of HAART in AIDS-related PML
� removal or decrease of any potential sources ofimmunosuppression, steroids included
� cytosine arabinoside :
- active on JCV replication in vitro
- positive in some case reports
- negative in a multicenter prospective study with a combinedIV and intrathecal administration
(Hall et al, NEJM, 1998, 338 : 1345-1351)
Progressive Multifocal Leukoencephalopathy (14) (PML)

� 54 year-old left-handed female� Admitted 07.1998� 1983 polyarthritis
– Prednisolone 7.5 mg/d since 1983– Methotrexate 15mg/w 1990-1995– Cladribine 36mg/2w 06.95-05.97– Azathioprine 100 mg since 1997
Case report : history 1

Case report : current disease
� Admitted July 1998� Complains for two months about
– Problems to dress– Problems to use left hand– « visual problems », expecially for distances,
with unability to read,to drive� Neurological examination

Neuropsychological examination

Magnetic Resonance Imaging
Hypo T1, cortex spared, Gado (-), hyper T2, hyper F LAIR, no mass effect

Pathology
Macrophages
Astrocytes
Multifocal demyelination, withmacrophages and giant astrocytes (Trichrome de Masson)

Pathology
Enlarged Oligodendrocyte nucleuswith viral inclusion
Enlarged bizarre atrocytes

Magnetic Resonance Imaging
3 months : slight gado(+)1 year : gado(-), necrosis2 - 5 years : regression, dilatation

Natalizumab -related PML
• About 400 cases worldwide
• 20 % died
• Increased prevalence in long duration (>2 years) treat ment and in case of previous immunosuppressive treatments
• Virtually never observed in JC-seronegative patients

Estimates of PML Incidence Overall and By Duration*
2,80
0,55
0,981,18
1,91
2,68
3,21
0,20 0,230,41
0,70 0,70
0,11
1,00
0,37
0,65 0,75
1,19
1,46
0,89
0,44
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
Clinic
al T
rial s
Post M
arketin
g>=1
2 Inf
u sions
>= 18
Infus
ions
>=24
Infu sio
ns>=3
0 Inf
u sions
>=36
Infu
sions
Estimated PML Incidence by Treatment Duration
Inci
denc
e pe
r 10
00pa
tient
s
*In Europe, we assume one infusion per month

Neuro -cysticercosis
�The most frequent parasitic disease of the CNS in the world
�Seizure as the main neurological symptom
�Subacute encephalitis, focal deficits, hydrocephalus…t

Neurocysticercosis

Neurocysticercosis

Neurocysticercosis

PINS : general characteristics
� arise within 4-6 weeks of a systemic infection/vacci nation
� 8 % are postvaccination syndromes and may present all the
syndromic phenotypes
� mean age : 60 years (18-80)
� excluding PNS involvement only, PINS are :
• central in 64% (E, EM, M) and
• mixed (EMRN, MRN) in 36 % (Marchioni et al, Neurology, 2013, 80 :
882-889)
Postinfectious neurologic syndromes (PINS) : syndromic phenotypes
� involving the peripheral nervous system only
• Guillain-Barré syndrome (2/3)
• brachial plexitis (Parsonage-Turner)
� involving the central nervous system only (“ADEM ” : acute
disseminated encephalomyelitis)
• encephalitis
• myelitis
• cerebellitis
• rhombencephalitis

Postinfectious neurologic syndromes (PINS) : syndromic phenotypes
� involving both peripheral and central nervous system s
• encephalomyeloradiculoneuritis
• myeloradiculoneuritis

PINS : clinical characteristics
In the series of 179 patients in Marchioni et al :
� maximum clinical dysfunction 6 days after onset (med ian)
� polysymptomatic in 94 % : paraparesis, urinary dysfunc tion,
consciousness impairment are the most frequent sympto ms
PINS : CSF abnormalities
� 12 % had normal CSF profile
� blood-CSF barrier damage (albumin quotient > 8) in 83 %
� pleocytosis, except in 6 cases with albumin-cytolog ical
dissociation
� CSF IgG pattern:
• polyclonal : 58.5 %
• mirror : 13.6 %
• mixed (mirror + specific bands) : 2 %
• specific bands : only 1 = 19 %
> 1 = 6 %
in 7 out 11 cases, IgG bands were transient

PINS : relapses
� in 24.6 % of patients with central PINS, in 41.6 % w ith mixed
syndromes
� the relapse consisted in isolated myelitis in 98 % ( 51 of 52
patients), even when the first episode had involved the brain
alone
� relapses occurred more frequently within the 12 months of onset,
never after 24 months
� relapses are located at the same spinal level in 71% of cases
at a different spinal level in 29 % of cases
� in all cases, lesions observed during the first episod e had
disappeared
� the only independent predictor of relapse was PNS in volvement



Myélite post-Mycoplasma pneumoniae

CONCLUSIONS
� An anatomic diagnosis is required to focus imagingtechniques on the relevant areas
� Imaging techniques are rarely specific enough foretiologic diagnosis especially at the spinal cord l evel
� Blood and CSF analysis are important tools foretiologic diagnosis but must be correlated with eac hother
� « Tropical diseases » may be encountered worldwide