the official journal of the academy of laser dentistry · the official journal of the academy of...
TRANSCRIPT

Vol. 23 No. 1 | 2015
T he O f f ic ia l Journal of the Academy of L aser D entis tr y
www.laserdentistry.org9900 W. Sample Rd. Suite 400 | Coral Springs FL 33065

ConvergentAD
EVERYTHING NEEDS LIGHT TO GROW.EVEN YOUR PRACTICE. Solea dentists report more than 95% of their hard and soft tissue procedures can be completed without anesthesia. The Solea laser ablates soft tissue with virtually no bleeding and allows multi-quadrant dentistry in a single visit. That means more procedures in one visit and happier patients. Solea fills your appointment book faster than the speed of light.
[email protected] | 844.GOSOLEA

The Academy of Laser Dentistry is a not-for-profit organization qualifying under Section 501(c)(3) of the Internal Revenue Code. The Academy of Laser Dentistry is an international professional membership association of dental practitioners and supporting organizations dedicated to improving the health and well-being of patients through the proper use of laser technology. The Academy is dedicated to the advancement of knowledge, research and education and to the exchange of information relative to the art and science of the use of lasers in dentistry. The Academy endorses the Curriculum Guidelines and Standards for Dental Laser Education.
© Copyright 2015 Academy of Laser Dentistry
Vol. 23 No. 1 | 2015
This paper meets the requirements of ANSI/NISO Z39.48-1992 (Permanence of Paper).
Efficacy of Laser Therapy in the Treatment of Peri-Implantitis: A Literature ReviewGeorgios E. Romanos, DDS, PhD, Prof. Dr. med. dent. and
Fawad Javed, BDS, PhD
How effective are lasers of different wavelengths in treating peri-implantitis? The authors examine the evidence from representative articles appearing in the literature
Laser Applications in Implantology: Scientific and Clinical PerspectivesStuart Coleton, DDS
5
6
TABLE ofCONTENTS
LITERATURE REVIEWEDITOR’S VIEW
ConvergentAD 11
GUIDELINES FOR AUTHORS
EVERYTHING NEEDS LIGHT TO GROW.EVEN YOUR PRACTICE. Solea dentists report more than 95% of their hard and soft tissue procedures can be completed without anesthesia. The Solea laser ablates soft tissue with virtually no bleeding and allows multi-quadrant dentistry in a single visit. That means more procedures in one visit and happier patients. Solea fills your appointment book faster than the speed of light.
[email protected] | 844.GOSOLEA

Editor-in-ChiefStuart Coleton, DDS | Chappaqua, NY [email protected]
Managing EditorGail S. Siminovsky, CAE, Executive DirectorCoral Springs, FL [email protected]
Consulting EditorJohn G. Sulewski, MA | Huntington Hills, MI [email protected]
PublisherMax G. Moses | Member MediaChicago, IL312-296-7864 • Fax: [email protected]
Editorial Advisory BoardSebastiano Andreana, DDS, Buffalo, NYPraveen B. Arany, BDS, MDS, MMSc, PhD, Cambridge, MAWilliam Gianni, DDS, Twain Harte, CADouglas A. Gilio, DMD, Visalia, CACharles Hoopingarner, DDS, Houston, TXArthur H. Jeske, DDS, Houston, TXGabi Kesler, DMD, Tel Aviv, IsraelMitchell A. Lomke, DDS, Olney, MDGloria E. Monzon, RDH, Milpitas, CAAngela S. Mott, RDH, Tulsa, OKShigeyuki Nagai, DDS, Tokyo, JapanGiovanni Olivi, DDS, MD, Rome, ItalyPeter Rechmann, DMD, PhD, San Francisco, CAJoel M. White, DDS, MS, San Francisco, CA
Mission StatementThe mission of the Journal of Laser Dentistry is to provide a professional journal that helps to fulfill the goal of information dissemination by the Academy of Laser Dentistry. The purpose of the Journal of Laser Dentistry is to present information about the use of lasers in dentistry. All articles are peer-reviewed. Issues include manuscripts on current indications for uses of lasers for dental applications, clinical case studies, reviews of topics relevant to laser dentistry, research articles, clinical studies, research abstracts detailing the scientific basis for the safety and efficacy of the devices, and articles about future and experimental procedures. In addition, featured columnists offer clinical insights, and editorials describe personal viewpoints.
Editorial Office9900 West Sample Road, Suite 400Coral Springs, FL 33065954-346-3776 | Fax 954-757-2598www.laserdentistry.org
AdvertisingIntegrity Media GroupKimberly [email protected]
Antimicrobial Effects of PhotosensitizersExperimental findings of the intraoral bactericidal effect of certain chemical substances, whether they are used alone or in photodynamic therapy
More on Laser-Assisted Orthodontic Tooth MovementFor facilitating tooth movement, is low-level laser stimulation or inhibition the underlying mechanism? How does emission mode affect the laser dose? A reader and the investigator share their dialogue.
RESEARCH ABSTRACTS
LETTERS
26
CLINICAL CASE
SCIENTIFIC RESEARCH
Er:YAG Laser-Assisted Bone and Gingival Augmentation Around ImplantsWalid Altayeb, DDS, MDS, PhDHow can an Er:YAG laser be used around ailing dental implants? The author demonstrates multiple applications of this laser for soft and hard tissue surgery and implant surface decontamination.
www.laserdentistry.org
37Antimicrobial Effects of the 810-nm Diode Laser in the Treatment of Peri-Implantitis: An Ex Vivo Pilot StudyErica Lavere, BS, DDS; Juliana Sagor, BA, DDS; Lynn Mikulski; Sebastiano Andreana, DDS, MSHow effective are different laser parameters in reducing a particular bacterial species, and how does adjunctive use of a photosensitizer affect the outcome? The authors demonstrate results using a novel tissue model.
47
44

SCIENTIFIC RESEARCHEDITOR’S VIEW
Laser Applications in Implantology: Scientific and Clinical PerspectivesStuart Coleton, DDS, New York Medical College, Valhalla, New York, and Westchester University Medical Center, Valhalla, New YorkJ Laser Dent 2015;23(1):5
For this and future issues of the Journal, we are expanding our regular scientific treatment of dental laser-related topics to include clinical cases. This complementary approach is designed to address the clinical needs of our readers while continuing to explore and relate the scientific foundations behind laser treatment of dental patients.
This issue concentrates on some of the applications of laser use in implantology. The American Academy of Implant Dentistry* estimates that 3 million Americans have dental implants, and that number is growing by one-half million yearly. Further, it is estimated that the U.S. and European market for dental implants is expected to reach $4.2 billion by 2022. From flap surgery to
removal of granulation tissues, from bone contouring to decontamination of implant surfaces, and from second-stage recovery to peri-implantitis treatment, lasers provide several means to support the placement and maintenance of dental implants.
Dr. Georgios Romanos and Dr. Fawad Javed furnish a literature review of the efficacy of laser therapy in treating peri-implantitis. For their analysis, they selected clinical and experimental studies cited in indexed databases. Their findings underscore the adjunctive role that laser therapy offers in treating this condition, providing clinicians adhere to safety and clinical application protocols.
Dr. Walid Altayeb presents a detailed case involving the use of an Er:YAG laser to assist in osseous and gingival augmentation surgery around ailing dental implants. The functional and aesthetic outcomes demonstrate how healthy and satisfactory results can be achieved by a cross-disciplinary dental team while considering relevant aspects of patient peri- and intraoral anatomy and respecting patient preferences for treatment.
Dr. Erica Lavere, one of the Academy of Laser Dentistry’s 2015 Dr. Eugene M. Seidner Student Scholarship Program honorees, and her colleagues present their research on “Antimicrobial Effects of the 810-nm Diode Laser in the Treatment of Peri-Implantitis: An Ex Vivo Pilot Study.” Their experimental model and approach examines the effects of 810-nm diode laser irradiation, with and without a photosensitizer, on a particular bacterial species.
Complementing Dr. Lavere’s study, the Research Abstracts explore the role that photosensitizers, whether or not they are used in conjunction with photodynamic therapy, could furnish in reducing the bacterial load of concern in peri-implantitis, periodontal disease, and other dental applications.
Finally, a letter to the editor and author response concerning laser irradiation doses in orthodontics continue the dialogue on “The Effect of Pulsed 810-nm Low-Level Laser Therapy on the Rate of Orthodontic Tooth Movement: A Randomized Clinical Trial,” as initially reported in the previous edition of the Journal.
Future issues will continue to provide scientific and clinical perspectives on the numerous applications of lasers in dentistry.
Yours for the future of lasers in dentistry,
Stuart Coleton, DDSEditor-in-Chief, Journal of Laser Dentistry
Stuart Coleton, DDS
AUTHOR BIOGRAPHY
Dr. Stuart Coleton is a
Diplomate of the American
Board of Periodontology
and the American Board of
Oral Medicine. He is chief
attending periodontist at
Westchester Medical Center
University Hospital, holds the
rank of assistant professor in
dental medicine at New York
Medical College, and is the
chief attending in periodontics
at the Metropolitan Medical
Center in New York City. He is a
past president of the Academy
of Laser Dentistry and is a
Recognized Course Provider.
He has been certified as having
Advanced Proficiency, Educator,
and Mastership status in lasers
by the Academy of Laser
Dentistry. His areas of special
expertise are periodontal
diagnosis and treatment as
well as oral medicine. He has
taught didactic and clinical
laser therapy to both dental
and medical general practice
residents. Dr. Coleton may
be contacted by e-mail at
Disclosure: Dr. Coleton has no laser-related commercial affiiations or personal conflicts of interest.
Coleton
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
5
*Dental Implants Facts and Figures. American Academy of Implant Dentistry Web site. http://www.aaid.com/about/Press_Room/Dental_Implants_FAQ.html. Accessed August 8, 2015.

Journal of Laser Dentistry: Guidelines for AuthorsThe Academy of Laser Dentistry Welcomes Your Articles for Submission
The Journal of Laser Dentistry publishes articles pertaining to the art, science, and practice of laser dentistry. Articles may be scientific and clinical in nature discussing new techniques, research, and programs, or may be applications-oriented describing specific problems and solutions. While lasers are our preferred orientation, other high-technology articles, as well as insights into marketing, practice management, regulation, and other aspects of dentistry that may be of interest to the dental profession, may be appropriate. All articles are peer-reviewed prior to acceptance, modification, or rejection.
These guidelines are designed to help potential authors in writing and submitting manuscripts to the Journal of Laser Dentistry, the official publication of the Academy of Laser Dentistry (ALD). Please follow these instructions carefully to expedite review and processing of your submission. Manuscripts that do not adhere to these instructions will not be accepted for consideration. The Academy of Laser Dentistry and the editors and publisher of the Journal of Laser Dentistry endorse the “Uniform Requirements of Manuscripts Submitted to Biomedical Journals” (www.icmje.org). The Journal reserves the right to revise or rescind these guidelines.
Authors are advised to read the more comprehensive Guidelines for Authors and required forms available by mail or online at www.laserdentistry.org.
Manuscript EligibilitySubmitted manuscripts must be written clearly and concisely in American English and appropriate for a scholarly journal. Write in active voice and use declarative sentences. Manuscripts will be considered for publication on the condition that they have been submitted exclusively to the Journal, and have not been published or submitted for publication in any part or form in another publication of any type, professional or lay, or in any language elsewhere, and with the understanding that they will not be reprinted without written consent from both the managing editor and the author(s).
PermissionsDirect quotations of 100 or more words, and illustrations, figures, tables, or other materials (or adaptations thereof) that have appeared in copyrighted material or are in press must be accompanied by written permission for their use in the Journal of Laser Dentistry from the copyright owner and original author along with complete information regarding source, including (as applicable) author(s), title of article, title of journal or book, year, volume number, issue number, pages. Photographs of identifiable persons must be accompanied by valid signed releases indicating informed consent. When informed consent has been obtained from any patient, identifiable or not, it should be noted in the manuscript. The appropriate Permission Letters must be submitted with the manuscript. Suggested template letters are available online.
CopyrightAll manuscript rights shall be transferred to the Journal of Laser Dentistry upon submission. Upon submission of the manuscript, authors agree to submit a completed Copyright Transfer Agreement form, available online. If the manuscript is rejected for publication, all copyrights will be retained by the author(s).
CommercialismALD members are interested in learning about new products and service offerings, however ALD stresses that submitted manuscripts should be educational in nature. The emphasis is on scientific research and sound clinical and practical advice, rather than promotion of a specific product or service.
Disclosure of Commercial RelationshipsAccording to the Academy’s Conflict of Interest and Disclosure policy, manuscript authors and their institutions are expected to disclose any economic or financial support, as well as any personal, commercial, technological, academic, intellectual, professional, philosophical, political, or religious interests or potential bias that may be perceived as creating a conflict related to the material being published. Such conditions may include employment, consultancies, stock ownership or other equity interests, honoraria, stipends, paid expert testimony, patent ownership, patent licensing arrangements, royalties, or serving as an officer, director, or owner of a company whose products, or products of a competitor, are identified. Sources of support in the form of contracts, grants, equipment, drugs, material
donations, clinical materials, special discounts or gifts, or other forms of support should be specified. The roles of the study or manuscript sponsor(s), if any, are to be described. Disclosure statements are printed at the end of the article following the author’s biography. This policy is intended to alert the audience to any potential bias or conflict so that readers may form their own judgments about the material being presented. Disclosure forms are to be signed by each author. Manuscripts will not be reviewed without the Journal having this form on file.
The Academy of Laser Dentistry also requires that authors disclose whether any product discussed in their manuscript is unlabeled for the use discussed or is investigational.
The Disclosure Statement form is available online and must be submitted with the manuscript.
Manuscript TypesSubmissions to the Journal should be limited to one of the types indicated below.• Scientific / Technology / Clinical Review• Case Reports and Clinical Case Studies• Scientific / Clinical Research• Randomized Clinical Trials• Advances in Dental Products• Trends• Practice Management• Guest Editorials and Essays• Letters to the Editor• Book Reviews
Manuscript Preparation and SubmissionFormatAll submitted manuscripts should be double-spaced, using 12 pt. font size with at least 6 mm between lines. Submit manuscripts in Microsoft Word (.doc), using either the Windows or Macintosh platform. Manuscripts must be submitted electronically in this format. Hard copy-only submissions will not be accepted.
Unacceptable FormatsThe following submission formats are unacceptable and will be returned:• Manuscripts submitted in desktop
publishing software• PowerPoint presentations• Any text files with embedded images• Images in lower than the minimum
prescribed resolution.
GUIDELINES FOR AUTHORS
6
Jour
nal o
f Las
er D
entis
try
|
2015
Vol
. 23,
No.
1

Upgrade to the ultra fast 1064XLASE™ Today!(888) [email protected]
On-board Video GuidanceWorld’s first laser with on board video navigation.
Touch Screen NavigationPresets with touch screen, ready to lead.
10W of 1064 SuperiorityPhoto Catalyze Protocols™ for dramatic results
Amazing SpeedFast, clean, beautiful surgery
Lightweight FormFold up stand for easy storage in a portable 3Lb package

8
Jour
nal o
f Las
er D
entis
try
|
2015
Vol
. 23,
No.
1GUIDELINES FOR AUTHORS
Manuscript ComponentsTitle PageThe title page of the manuscript should include a concise and informative title of the article; the first name, middle initial(s), and last name of each author, along with the academic degree(s), professional title(s), and the name and location (city, state, zip code) of current institutional affiliation(s) and department(s). Authors who are private practitioners should identify their location (city, state, and country). Include all information in the title that will make electronic retrieval of the article sensitive and specific. Titles of case studies should include the laser wavelength(s) and type(s) utilized for treatment (for example, “810-nm GaAlAs diode”).
Identify the complete address, business and home telephone numbers, fax number, e-mail address, and Web site address (if any) for all authors. Identify one author as the corresponding author. Unless requested otherwise, the e-mail address is published in the Journal.
AbstractA self-standing summary of the text of up to 250 words should precede the introduction. It should provide an accurate summary of the most significant points and be representative of the entire article’s content. Provide the context or background for the article, basic procedures, main findings and conclusions. Emphasize new or important aspects. Do not use abbreviations (other than standard units of measurement) or references in the abstract.
Author(s) BiographyProvide a brief, current biographical sketch of each author that includes professional education and professional affiliations. For authors who hold teaching positions, include the title, department, and school. For authors who are in federal service, include rank or title and station.
ReferencesReferences are to be cited in the text by number in order of appearance, with the number appearing either as a superscript or in brackets. The reference list should appear at the end of the manuscript with references in order of first appearance in the text of the manuscript. The reference list must be typed double-spaced on a separate page and numbered in the same sequence as the reference citations appear in the text. Prior to submission, all references are to be properly prepared in the correct format, checked for completeness, carefully verified against their original documents, and checked for accurate correspondence between references cited in the text and listed in the References section.
• For journal citations, include surnames and all initials of all authors, complete title of article, name of journal (abbreviated according to the U.S. National Library of Medicine (www.nlm.nih.gov/services/lpabbrev.html), year of publication, volume, issue number, and complete inclusive page numbers. If abstracts are cited, add the abstract number after the page number.
• For book citations, specify surnames and initials of all authors, chapter number and title (if applicable), editors’ surnames and initials, book title, volume number (if applicable), edition number (if applicable), city and full name of publisher, year of publication, and inclusive page numbers of citation.
• For government publications or bulletins, identify the author(s) (if given); title; department, bureau, agency, or office; the publication series, report, or monograph number; location of publisher; publisher; year of publication; and inclusive page numbers.
• For articles published online but not yet in print, cite with the paper’s Digital Object Identifier (DOI) added to the end of the reference.
• For Web citations, list the authors and titles if known, then the URL and date it was accessed.
• For presentations, list the authors, title of presentation, indication that the reference is a lecture, name of conference or presentation venue, date, and location.
Illustration Captions and LegendsAll illustrations must be accompanied by individual explanatory captions which should be typed double-spaced on a separate page with Arabic numerals corresponding to their respective illustration.
TablesTables must be typewritten double-spaced, including column heads, data, and footnotes, and submitted on separate pages. The tables are to be cited in the text and numbered consecutively in Arabic numerals in the order of their appearance in the text. Provide a concise title for each table that highlights the key result.
IllustrationsIllustrations include photographs, radiographs, micrographs, charts, graphs, and maps. Each should be numbered and cited in the text in the order of appearance and be accompanied by explanatory captions. Do not embed figures within the manuscript text. Each figure and table should be no larger than 8-1/2 x 11 inches. Digital files must measure at least 5 inches (127 mm) in width. The image must be submitted in the size it will be printed, or larger. Illustrations are to augment, not repeat, material in the text. Graphs must not repeat data presented in tables. Clinical photographs must comply with ALD’s Guidelines for Clinical Photography, available online. Authors are to certify in a cover letter that digitized illustrations accurately represent the original data, condition, or image and are not electronically edited.
Summary of Illustration Types and Specifications
Illustration Type Definition and ExamplesPreferred
FormatRequired
Resolution
Line Art and Vector Graphics
Black and white graphic with no shading (e.g., graphs, charts, maps)
EPS or JPG 1200 DPI
Halftone Art
Photographs, drawings, or painting with fine shading (e.g., radiographs,
micrographs with scale bars, intraoral photographs)
TIFF or JPG300 DPI (black & white)
600 DPI (color)
Combination ArtCombination of halftone and line art
(e.g., halftones containing line drawing, extensive lettering, color diagrams)
EPS or JPG 1200 DPI
www.laserdentistry.org

9
Jour
nal o
f Las
er D
entis
try
|
2015
Vol
. 23,
No.
1
GUIDELINES FOR AUTHORS
Publisher and Copyright HolderThe Journal of Laser Dentistry is published by Max G. Moses, Member Media, 1844 N. Larrabee, Chicago, IL 60614, Telephone: (312) 296-7864; Fax: (312) 896-9119. The Journal of Laser Dentistry is copyrighted by The Academy of Laser Dentistry, 9900 W. Sample Road, Suite 400, Coral Springs, FL 33065, Telephone: (954) 346-3776; Fax: (954) 757-2598.
Articles, Questions, IdeasQuestions about clinical cases, scientific research, or ideas for other articles may be directed to Stuart Coleton, Editor-in-Chief, by e-mail: [email protected].
Submission of Filesby E-mail:Send your completed files by e-mail (files up to 10 MB are acceptable). If files are larger than 10 MB, they may be compressed or sent as more than one file, with appropriate labels. Files should be submitted to: Stuart Coleton, Editor-in-Chief, by e-mail: [email protected].
By Federal Express or Other Insured Courier:If using a courier, please send the files on a flash drive, include a hard copy of your manuscript and also send a verification by e-mail to Gail Siminovsky ([email protected]).
Gail SiminovskyAcademy of Laser Dentistry9900 W. Sample Road, Suite 400Coral Springs, FL 33065Phone: (954) 346-3776.
Editorial PolicyThe Journal of Laser Dentistry is devoted to providing the Academy and its members with comprehensive clinical, didactic, and research information about the safe and effective uses of lasers in dentistry. All statements of opinions and/or fact are published under the authority of the authors, including editorials and articles. The Academy is not responsible for the opinions expressed by the writers, editors or advertisers. The views are not to be accepted as the views of the Academy of Laser Dentistry unless such statements have been expressly adopted by the organization. Information on any research, clinical procedures or products may be obtained from the author. Comments concerning content may be directed to the Academy’s main office by e-mail to [email protected].
SubmissionsWe encourage prospective authors to follow JLD’s “Instructions to Authors” before submitting manuscripts. To obtain a copy, please go to our Web site www.laserdentistry.org/uploads/files/members/jld/JLD%20Author%20Guidelines.pdf. Please send manuscripts by e-mail to the Editor at [email protected].
Disclosure Policy of Contributing Authors’ Commercial RelationshipsAccording to the Academy’s Conflict of Interest and Disclosure policy, authors of manuscripts for the Journal of Laser Dentistry are expected to disclose any economic support, personal interests, or potential bias that may be perceived as creating a conflict related to the material being published. Disclosure statements are printed at the end of the article following the author’s biography. This policy is intended to alert the audience to any potential bias or conflict so that readers may form their own judgments about the material being presented.
Disclosure Statement for the Academy of Laser DentistryThe Academy of Laser Dentistry has no financial interest in any manufacturers or vendors of dental supplies.
Reprint Permission PolicyWritten permission must be obtained to duplicate and/or distribute any portion of the Journal of Laser Dentistry. Reprints may be obtained directly from the Academy of Laser Dentistry provided that any appropriate fee is paid.
The Journal of Laser Dentistry ISSN# 1935-2557.
The Journal of Laser Dentistry is published semi-annually and provided electronically to all ALD members. The Journal is mailed nonprofit standard mail to ALD members requesting a hard copy. Issues are also mailed to new member prospects and dentists requesting information on lasers in dentistry.
Copyright 2015 Academy of Laser Dentistry. All rights reserved unless other ownership is indicated. If any omission or infringement of copyright has occurred through oversight, upon notification amendment will be made in a future issue. No part of this publication may be reproduced or transmitted in any form or by any means, individually or by any means, without permission from the copyright holder.
Advertising Information and RatesDisplay rates are available at www.laserdentistry.org and/or supplied upon request. Insertion orders and materials should be sent to Integrity Media Group, Kimberly Price at [email protected]. Call 813-390-4003 with any questions.. Companies are encouraged to contact Integrity Media Group for information on display advertising specifications and rates. The Academy reserves the right to edit or refuse ads.
Editor’s Note on Advertising: The Journal of Laser Dentistry currently accepts advertisements for different dental laser educational programs. Not all dental laser educational courses are recognized by the Academy of Laser Dentistry. ALD as an independent professional dental organization is concerned that courses meet the stringent guidelines following professional standards of education. Readers are advised to verify with ALD whether or not specific courses are recognized by the Academy of Laser Dentistry in their use of the Curriculum Guidelines and Standards for Dental Laser Education.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed10
❝
Your patients will love
this
Discover how LLLT can help your patients and practice with THOR
LLLT is a non thermal laser treatment that increases ATP, reduces oxidative stress leading to reduced inflammation and with high irradiance treatments works as an analgesia. Clinical applications include:
• Dentinal Hypersensitivity• Burning mouth syndrome• Paresthesia / nerve damage• Post extraction pain / swelling• Gingivitis, periodontitis• Denture stomatitis• Osseointegration of implants• Improved tooth movement after
orthodontic treatment
• Orthodontic pain• Post op healing• Dentin-pulp repair• TMJD• Trauma• HSV• Mucositis• Xerostomia
To discover how LLLT can benefit your patients, as well as save your practice money, sign up for a THOR training course, available throughout the USA.
“The training with THOR Laser was thorough and made theunderstanding of the mode of action very clear. It taught me how the laser can be used in many situations. It is a real benefit to my patients!”Arthur B Levy DDM, Chester Dental Associates, United States
To find out more go to www.thorlaser.com/dental or phone USA 877 355 3151
Low Level Laser Therapy (LLLT) THOR Training Courses
Regulatory Approvals Include:
The THOR system is FDA-cleared for muscle and joint pain only, all other indications are off-label and for investigational use only.

Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
11
Efficacy of Laser Therapy in the Treatment of Peri-Implantitis: A Literature ReviewGeorgios E. Romanos, DDS, PhD, Prof. Dr. med. dent.Department of Periodontology, School of Dental Medicine, Stony Brook University, Stony Brook, New York, USA
Fawad Javed, BDS, PhDUniversity of Rochester, Eastman Institute for Oral Health, Department of General Dentistry, Rochester, New York
J Laser Dent 2015;23(1):11-24
ABSTRACTThe aim of the present study was to review indexed literature regarding the efficacy of laser therapy in the
treatment of peri-implantitis. Indexed databases were searched from using different combinations of the following key words: “peri-implantitis,” “bone loss,” “photodynamic therapy,” “laser,” and “light-activated disinfection.” Titles and abstracts of studies that fulfilled the eligibility criteria were screened by the authors and checked for agreement. Full texts of studies judged by title and abstract to be relevant were read and independently assessed against the eligibility criteria. The pattern of the present review was customized to summarize the relevant data. Laser therapy can effectively be used with conventional mechanical debridement protocols used for treating peri-implantitis. The erbium:yttrium-aluminum-garnet laser effectively strips off the contaminated oxide layer from implant surfaces without damaging implant surface characteristics. Likewise, the carbon dioxide laser application to implant surfaces is a potent strategy for implant surface disinfection and enhancing bone-to-implant contact around previously infected sites. The neodymium:yttrium aluminium garnet laser may melt the surface of failing implants and overheat the implant and surrounding tissues. Diode lasers (810-980 nm) can also be dangerous if they are used without following strict protocols. Photodynamic therapy exhibits high target specificity and destroys pathogens associated with the etiology of peri-implantitis. Laser therapy significantly reduces the clinical markers of peri-implant tissue inflammation (bleeding on probing and clinical attachment loss) without jeopardizing the integrity of the implant and alveolar bone. In conclusion, laser therapy, as an adjunct to conventional mechanical debridement therapy, is a modern therapeutic method that can effectively be used for the treatment of peri-implantitis when safety and clinical application protocols are cautiously followed.
Key words: Dental lasers, Peri-implantitis, Peri-implant bone loss, Photodynamic therapy
INTRODUCTIONPeri-implantitis is a disease of the tissues
surrounding dental implants. Roos-Jansåker et al.1 defined peri-implantitis as an inflammatory condition in which implants with varying degrees of bone loss are accompanied by a probing depth of at least 4 mm, bleeding on probing, and purulent discharge
on placid probing. It has been reported that peri-implantitis occurs on the order of 10% of implants and in 20% patients within 5 years to 10 years after implant placement.2 However, the individual reported figures are variable.2-4 Risk factors that have been associated with the etiology of peri-implantitis encompass poor
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed12
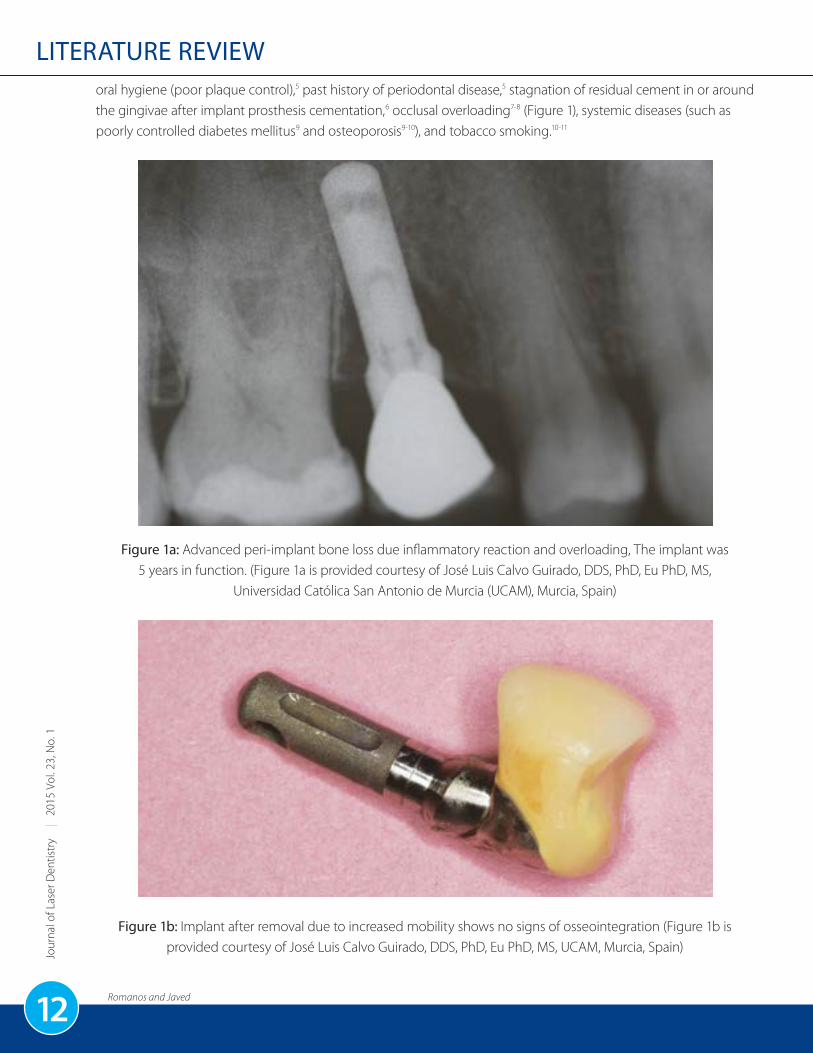
oral hygiene (poor plaque control),5 past history of periodontal disease,5 stagnation of residual cement in or around the gingivae after implant prosthesis cementation,6 occlusal overloading7-8 (Figure 1), systemic diseases (such as poorly controlled diabetes mellitus9 and osteoporosis9-10), and tobacco smoking.10-11
Figure 1a: Advanced peri-implant bone loss due inflammatory reaction and overloading, The implant was 5 years in function. (Figure 1a is provided courtesy of José Luis Calvo Guirado, DDS, PhD, Eu PhD, MS,
Universidad Católica San Antonio de Murcia (UCAM), Murcia, Spain)
Figure 1b: Implant after removal due to increased mobility shows no signs of osseointegration (Figure 1b is provided courtesy of José Luis Calvo Guirado, DDS, PhD, Eu PhD, MS, UCAM, Murcia, Spain)
Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
13
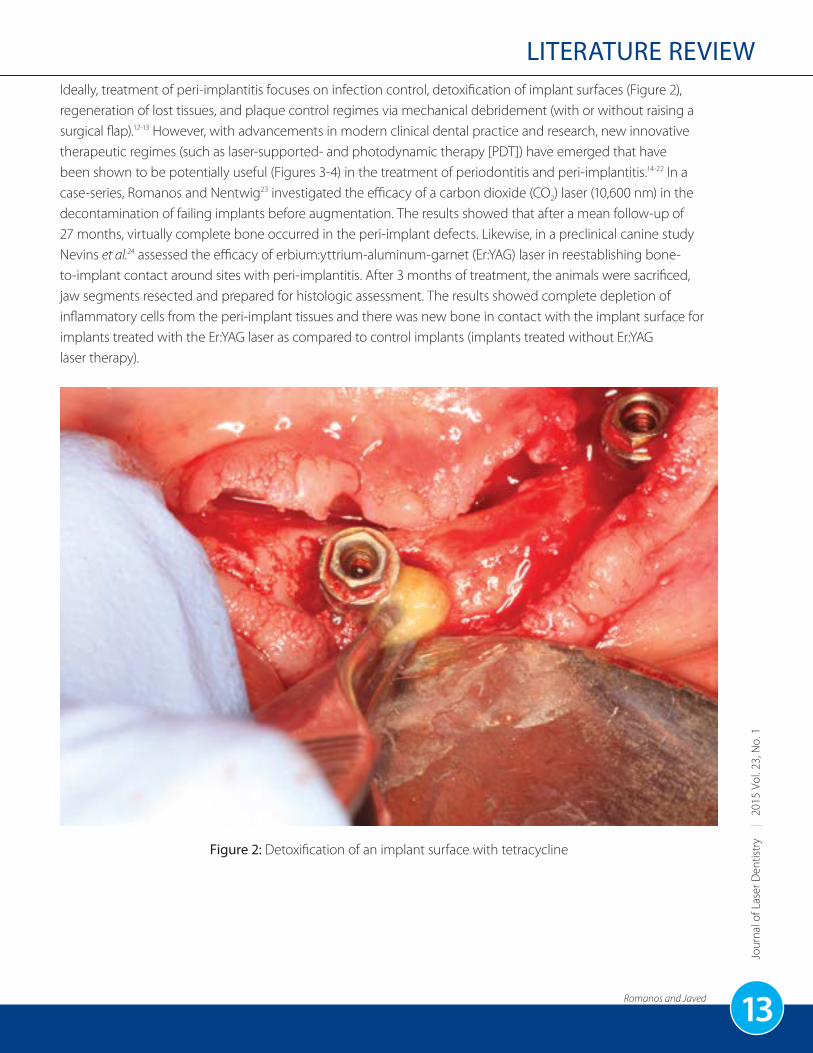
Ideally, treatment of peri-implantitis focuses on infection control, detoxification of implant surfaces (Figure 2), regeneration of lost tissues, and plaque control regimes via mechanical debridement (with or without raising a surgical flap).12-13 However, with advancements in modern clinical dental practice and research, new innovative therapeutic regimes (such as laser-supported- and photodynamic therapy [PDT]) have emerged that have been shown to be potentially useful (Figures 3-4) in the treatment of periodontitis and peri-implantitis.14-22 In a case-series, Romanos and Nentwig23 investigated the efficacy of a carbon dioxide (CO2) laser (10,600 nm) in the decontamination of failing implants before augmentation. The results showed that after a mean follow-up of 27 months, virtually complete bone occurred in the peri-implant defects. Likewise, in a preclinical canine study Nevins et al.24 assessed the efficacy of erbium:yttrium-aluminum-garnet (Er:YAG) laser in reestablishing bone-to-implant contact around sites with peri-implantitis. After 3 months of treatment, the animals were sacrificed, jaw segments resected and prepared for histologic assessment. The results showed complete depletion of inflammatory cells from the peri-implant tissues and there was new bone in contact with the implant surface for implants treated with the Er:YAG laser as compared to control implants (implants treated without Er:YAG laser therapy).
Figure 2: Detoxification of an implant surface with tetracycline

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed14
Figure 3: Decontamination of an implant surface with a noncontact CO2 laser (10,600 nm). The beam was defocused at a distance of 3-5 mm and with low power (2 Watts, pulsed mode).
Figure 4: Decontamination of implant surface with a low-power 810-nm noncontact diode laser (2 Watts average power with initiator using a defocused beam at a distance of 3-5 mm from the implant surface). (Figure 4 is
reproduced with permission and appears as Figure 7 in: Romanos GE, Javed F, Delgado-Ruiz R, Calvo-Guirado JL. Peri-implant diseases: A review of treatment interventions. Dental Clinics of North America 2015; 59: (1): 157-178).
The aim of the present study was to review the efficacy of laser therapy in the treatment of peri-implantitis.

Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
15
MATERIALS AND METHODSPubMed/MEDLINE (National Library of Medicine, Bethesda, Md., USA), Embase, Scopus, ISI-Web of Knowledge,
and Google Scholar databases were searched from 1991 up to and including August 2014 using different combinations of the following key words: “peri-implantitis,” “bone loss,” “photodynamic therapy,” “laser,” and “light-activated disinfection.” Clinical and experimental studies were included. Letters to the editor, case reports, historic reviews, and articles published in languages other than English were excluded. Titles and abstracts of studies that fulfilled the eligibility criteria were screened by the authors and checked for agreement. Full texts of studies judged by title and abstract to be relevant were read and independently assessed against the eligibility criteria. Following this, reference lists of original and review studies that were found to be pertinent in the previous step were hand-searched and checked for agreement via discussion between the authors. Since indexed literature has a dearth of studies assessing the role of lasers in the treatment of peri-implantitis, the pattern of this review was customized to primarily summarize the pertinent data.
DISINFECTION OF DENTAL IMPLANT SURFACESIt is known that implant surface characteristics
(surface roughness) play a significant role in osseointegration and long-term survival of dental implants.25 It has been reported that the Er:YAG laser has a high absorbability in water and removes the microbial-infiltrated oxide layer from the surface without jeopardizing the implant surface characteristics and surrounding alveolar bone.26-27 In their study on dogs, Nevins et al.24 investigated the ability of Er:YAG laser to treat peri-implantitis by removing the contaminated titanium oxide layer from implant surfaces. After 3 months of follow-up, the animals were clinically examined to assess the severity of peri-implant soft tissue inflammation following which the animals were sacrificed and jaw segments (containing the implants and surrounding tissues) were assessed histologically. Clinically, minimal gingival inflammation was seen and the histologic results showed bone formation and sufficiently enhanced bone-to-implant contact. Experimental results by Yamamoto and Tanabe26 also reported that the Er:YAG laser is potentially effective in stripping the contaminated titanium oxide layer from implant surfaces without damaging the implant surface and bone. However, controversial results have also been inked. In a 48-month follow-up clinical study, Schwarz et al.28 assessed the effect of two surface decontamination methods on the long-term outcomes following combined surgical resective and regenerative treatment of peri-implantitis. In Group
1, implant surfaces were treated with an Er:YAG laser, whereas those in Group 2 were treated with plastic curettes + cotton pellets + sterile saline. The 4-year follow-up results showed significantly greater reduction in bleeding on probing, plaque index, and attachment loss among implants in Group 2 as compared to implants in Group 1. An explanation in this regard is that use of laser equipment is technique-sensitive and operators’ experience with this technology plays a role in the overall effectiveness of laser therapy.21
It is pertinent to mention that alternations in implant surface characteristics have been reported with laser energies exceeding 140-180 mJ/pulse;29 however, Er:YAG laser when used at 100 mJ/pulse and 10 pulses/second for 60 seconds has been shown to be safe for use on implant surfaces.30 In this context, disinfection of implant surfaces using an Er:YAG laser system seems to be a promising therapeutic protocol for the treatment of peri-implantitis.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed16
SIGNIFICANCE OF CARBON DIOXIDE LASER IN THE TREATMENT OF PERI-IMPLANTITIS
The use of CO2 (10,600 nm) lasers in implant dentistry is increasing since this CO2 wavelength reduces the risk of temperature-induced tissue damage as this laser is minimally absorbed in the implant surface and it absorbs in water.20, 31-34 Romanos et al.35 assessed the osteoblast attachment on titanium disks after irradiation with and without CO2 and Er,Cr:YSGG lasers. The results showed that irradiation of titanium surfaces using CO2 laser or Er,Cr:YSGG laser does not influence negatively the osteoblast attachment to implant surfaces, thereby augmenting bone formation. This is in agreement with the experimental results by Stübinger et al.,31 where CO2
laser application (as an adjunct to mechanical debridement) augmented new bone formation in peri-implant defect sites (Figure 5). However, an understanding of the characteristics of the applied laser energy to optimize therapeutic implementation is crucial because heat production as a result of CO2 laser application may jeopardize osseointegration to an extent.36-37 In a clinical study on 32 patients, Deppe et al.38 assessed the efficacy of soft tissue resection with and without adjunct CO2 laser therapy in the treatment of peri-implantitis. The 5-year follow-up results showed that treatment of peri-implantitis is significantly accelerated by using a CO2 laser. However, the authors stated that with respect to long-term results in augmented defects, there seems to be no difference between laser and conventional decontamination.
Figure 5a: Intraoperative condition of peri-implant defects due to peri-implantitis

Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
17
Figure 5b: Decontamination of implant surface with a noncontact CO2 laser (10,600 nm) and 2 Watts power setting (pulsed mode)
Figure 5c: Augmentation with particulate bovine bone mineral immediately after implant surface decontamination. The blood clot was stable at the implant surface immediately before grafting.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed18
Figure 5d: Coverage with a cell-occlusive collagen membrane and fixation with titanium tags based on the principles of guided bone regeneration.
Figure 5e: Preoperative radiograph presenting the peri-implant bony defect before decontamination and bone augmentation. The implant had been 2 years in function under loading conditions.

Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
19
Figure 5f: Postoperative follow-up 5 months after surgery, presenting the bone fill. No signs of inflammation (such as bleeding on probing, exudation, and pain) were noticed.
ND:YAG LASER-ASSISTED PERI-IMPLANTITIS PROTOCOLThere is ongoing research on a relatively new technique termed “laser-assisted peri-implantitis protocol”
(LAPIP). LAPIP technique is an implant-specific modification of the laser-assisted new attachment protocol (LANAP). LAPIP and LANAP protocols use a laser ablation step to remove inflamed sulcular tissues (using an Nd:YAG laser) and decontaminate the implant/root surface followed by minimally invasive surgical periodontal therapy. The LAPIP protocol works on the concept of creation of blood clot stabilization that allows the defect area to heal apicocoronally by prevention the down-growth of gingival epithelium. However, to our knowledge from indexed literature, there are no randomized controlled trials, which have assessed the efficacy of LAPIP for the management of peri-implantitis. Therefore, studies are warranted in this regard.
However, previous studies using Nd:YAG laser irradiation in a noncontact mode on implant surfaces demonstrate the dramatic effects this laser wavelength can have on the implant surface due to the high absorption and overheating of the implant body.36 Therefore, there are concerns of the Nd:YAG laser use in vivo due to the possible high risks of complications.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed20
ROLE OF PHOTODYNAMIC THERAPY IN THE TREATMENT OF PERI-IMPLANTITIS
Photodynamic therapy (PDT) is a modern therapeutic strategy, which involves interactions between a light source of a particular wavelength (usually between 630 nm and 700 nm) and a photosensitizer (such as toluidine blue [TBO] or methylene blue [MB]) in the presence of oxygen.16, 39 This phototoxic and chemical reaction induces the production of reactive oxygen species (ROS) that cause oxidative damage to the target cells including microbial cells and tumor cells.40-41 In summary, some advantages of PDT encompass: (a) high target specificity;41 (b) biocompatibility with healthy human cells;42 (c) unlikely risk of chemical and/or thermal side-effects;43-44 and (d) improbable chances of microbes and fungi to develop resistance against PDT.45-46
In the study by Dörtbutak et al.,47 the pathogens existing in the peri-implant sulci of patients with peri-implantitis were significantly reduced following PDT. Likewise, experimental studies48-50 have also reported favorable outcomes of PDT in terms of minimizing bacterial counts. These results suggest that PDT may be considered as a useful treatment strategy in the management of peri-implantitis. Based on the experimental results,48-50 it is speculated that PDT when used as an adjunct to mechanical debridement is more effective in the treatment of peri-implantitis as compared to when conventional treatment is performed alone. However, clinical studies51-54 have reported contradictory results. For example, Esposito et al.52 compared the effect of mechanical and surgical debridement techniques with and without PDT in patients with peri-implantitis. In their study, peri-implant inflammatory parameters (probing pocket depth [PPD] and plaque and bleeding scores) were investigated at baseline and 52 weeks after the respective treatments. The results showed a comparable reduction in peri-implant inflammatory parameters when conventional treatments were performed either with or without PDT. Similar results
were reported by De Angelis et al.51 An explanation may be derived from the fact that severity of peri-implantitis most probably varied among all the clinical studies.47,
51-55 For example, in the studies by De Angelis et al.51 and Schär et al.,55 the mean PPD was 4.29 mm and 6.34 mm, respectively. Moreover, in the study by Deppe et
al.,54 there was no significant effect of PDT in patients with severe peri-implantitis (PPD 5-8 mm) as compared to those with moderate peri-implantitis (PPD 3-5 mm). Therefore, it is hypothesized that the efficacy of conventional debridement either with or without PDT is governed by the severity of peri-implantitis.
It is, however, pertinent to mention that the frequency and duration of PDT (1- 4 times and 10 s – 80 s, respectively) considerably varied among the clinical studies.47, 51-55 In addition, a standardized test- (mechanical debridement with adjunct PDT) and control-group (mechanical debridement alone) was also missing in most of the clinical studies.47, 53-55 Therefore, the clinical efficacy of PDT as an adjunct to conventional debridement techniques in the treatment of peri-implantitis remains debatable.
FUTURE PESPECTIVESTo our knowledge, there are no studies that have
assessed the efficacy of peri-implantitis using laser therapy in immunocompromised patients. Since the immunity is compromised in patients with systemic disorders (such as poorly controlled diabetes),56 it is hypothesized that the therapeutic outcomes of peri-implantitis therapy (either with or without adjunct laser therapy) are compromised in immunosuppressed patients as compared to controls. Further studies are warranted in this regard.
Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
21
CONCLUSIONWithin the limits of the present literature review, it is concluded that laser therapy as an adjunct to conventional
mechanical debridement therapy is a modern therapeutic protocol that can effectively be used for the treatment of peri-implantitis, provided that safety and clinical application protocols are cautiously followed. However, there is still a need to reach a consensus regarding the standardization of laser-related parameters that could yield the most favorable outcomes in terms of peri-implant infection therapy.
AUTHOR BIOGRAPHIES
Georgios E. Romanos is a Professor of Periodontology at the Stony Brook University School of Dental Medicine, Department of Periodontology, and a Professor in Oral Surgery and Implantology at the University of Frankfurt, Germany. He is fully trained in Periodontics, Prosthodontics, and Oral Surgery in Germany and has been Board Certified in Oral Surgery and Implant Dentistry in Germany. Dr. Romanos has a Certificate in Periodontology and Advanced Education in General Dentistry (AEGD) from the University of Rochester, New York, and is a Diplomate in the American Board of Periodontology and the International Congress of Oral Implantologists (ICOI). He is a former Professor and Director of Laser Sciences at the New York University College of Dentistry, and a former Professor of Clinical Dentistry at the University of Rochester. He maintains his Dental License in the State of New York and in Europe. Dr. Romanos is a Fellow of the Academy of Osseointegration (AO), International College of Dentists, International Congress of Oral Implantologists, International Team for Implantology Foundation, American Society for Laser Medicine and Surgery, the International Academy for Dental Facial Esthetics, and the Leadership Institute of the American Dental Education Association (ADEA). He is also an Editorial Board Member of the International Journal of Oral and
Maxillofacial Implants, Clinical Implant Dentistry and Related Research, Journal of Prosthodontics,
Odontology, Photomedicine and Laser Surgery, Quintessence International, Compendium, Journal
of Periodontology, International Journal of Dentistry, and others. He has published more than 300 articles, authored 5 books, and conducted over 700 presentations worldwide. Dr. Romanos may be contacted by e-mail at [email protected].
Fawad Javed completed his doctoral education and postdoctoral training from the Department of Dental Medicine, Karolinska Institutet, Stockholm, Sweden. He has published more than 90 articles in ISI-indexed medical and dental journals. Presently, he is a postdoctoral fellow and research associate at the Division of General Dentistry, Eastman Institute for Oral Health, University of Rochester, N.Y., USA. Dr. Javed’s research interests include oral oncology research, connection between oral inflammatory disorders and systemic conditions (particularly diabetes mellitus), impact of smoking and use of smokeless tobacco on oral health, cytokine profile in serum and oral fluids in patients with and without systemic conditions, implant dentistry, bone regeneration research, and saliva research. He is on the editorial board and member of peer-review panels of various indexed medical and dental journals.
Disclosures: The authors declare that they have no conflict of interest and there was no external source of funding for the present study.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed22
1. Roos-Jansåker A-M, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: Presence of peri-implant lesions. J Clin Periodontol 2006;33(4):290-295.
2. Mombelli A, Müller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res 2012;23(Suppl 6):67-76.
3. Schuldt Filho G, Dalago HR, Oliveira Souza JG, Stanley K, Jovanovic S, Bianchini MA. Prevalence of peri-implantitis in patients with implant-supported fixed prostheses. Quintessence Int 2014;45(10):861-868.
4. Costa FO, Takenaka-Martinez S, Cota LOM, Ferreira SD, Silva GLM, Costa JE. Peri-implant disease in subjects with and without preventive maintenance: A 5-year follow-up. J Clin Periodontol 2012;39(2):173-181.
5. Daubert DM, Weinstein BF, Bordin S, Leroux BG, Flemmig TF. Prevalence and predictive factors for peri-implant disease and implant failure: A cross-sectional analysis. J Periodontol 2015;86(3):337-347.
6. Pette GA, Ganeles J, Norkin FJ. Radiographic appearance of commonly used cements in implant dentistry. Int J Periodontics Restorative Dent 2013;33(1):61-68.
7. Naert I, Duyck J, Vandamme K. Occlusal overload and bone/implant loss. Clin Oral Implants Res 2012;23(Suppl 6):95-107.
8. Tawil G. Peri-implant bone loss caused by occlusal overload: Repair of the peri-implant defect following correction of the traumatic occlusion. A case report. Int J Oral Maxillofac Implants 2008;23(1):153-157.
9. Javed F, Romanos GE. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: A systematic literature review. J Periodontol 2009;80(11):1719-1730.
10. Chen H, Liu N, Xu X, Qu X, Lu E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS One 2013;8(8):e71955.
11. Galindo-Moreno P, León-Cano A, Ortega-Oller I, Monje A, O’Valle F, Catena A. Marginal bone loss as success criterion in implant dentistry: Beyond 2 mm. Clin Oral Implants Res 2015;26(4):e28-e34.
12. Bautista L, Huynh-Ba G. In patients with peri-implantitis, access flap surgery may be more effective than mechanical debridement in terms of clinical attachment gain although both treatments lead to improved clinical parameters (UT CAT #2432). Tex Dent J 2013;130(11):1112.
13. Schou S, Berglundh T, Lang NP. Surgical treatment of peri-implantitis. Int J Oral Maxillofac Implants 2004;19(Suppl):140-149.
14. Qadri T, Javed F, Poddani P, Tunér J, Gustafsson A. Long-term effects of a single application of a water-cooled pulsed Nd:YAG laser in supplement to scaling and root planing in patients with periodontal inflammation. Lasers Med Sci 2011;26(6):763-766.
15. Qadri T, Poddani P, Javed F, Tunér J, Gustafsson A. A short-term evaluation of Nd:YAG laser as an adjunct to scaling and root planing in the treatment of periodontal inflammation. J Periodontol 2010;81(8):1161-1166.
16. Vohra F, Al-Rifaiy MQ, Lillywhite G, Abu Hassan MI, Javed F. Efficacy of mechanical debridement with adjunct antimicrobial photodynamic therapy for the management of peri-implant diseases: A systematic review. Photochem Photobiol Sci 2014;13(8):1160-1168.
17. Javed F, Hussain HA, Romanos GE. Re-stability of dental implants following treatment of peri-implantitis. Interv Med Appl Sci 2013;5(3):116-121.
18. Javed F, Romanos GE. Does photodynamic therapy enhance standard antibacterial therapy in dentistry? Photomed Laser Surg 2013;31(11):512-518.
19. Leja C, Geminiani A, Caton J, Romanos GE. Thermodynamic effects of laser irradiation of implants placed in bone: An in vitro study. Lasers Med Sci 2013;28(6):1435-1440.
20. Romanos G, Ko H-H, Froum S, Tarnow D. The use of CO2 laser in the treatment of peri-implantitis. Photomed Laser Surg 2009;27(3):381-386.
REFERENCES

Romanos and Javed
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LITERATURE REVIEW
23
21. Romanos GE, Gupta B, Yunker M, Romanos EB, Malmstrom H. Lasers use in dental implantology. Implant Dent 2013;22(3):282-288.
22. Romanos GE, Weitz D. Therapy of peri-implant diseases. Where is the evidence? J Evid Based Dent Pract 2012;12(3 Suppl):204-208.
23. Romanos GE, Nentwig GH. Regenerative therapy of deep peri-implant infrabony defects after CO2 laser implant surface decontamination. Int J Periodontics Restorative Dent 2008;28(3):245-255.
24. Nevins M, Nevins ML, Yamamoto A, Yoshino T, Ono Y, Wang C-W(J), Kim DM. Use of Er:YAG laser to decontaminate infected dental implant surface in preparation for reestablishment of bone-to-implant contact. Int J Periodontics Restorative Dent 2014;34(4):461-466.
25. Javed F, Almas K, Crespi R, Romanos GE. Implant surface morphology and primary stability: Is there a connection? Implant Dent 2011;20(1):40-46.
26. Yamamoto A, Tanabe T. Treatment of peri-implantitis around TiUnite-surface implants using Er:YAG laser microexplosions. Int J Periodontics Restorative Dent 2013;33(1):21-29.
27. Takasaki AA, Aoki A, Mizutani K, Kikuchi S, Oda S, Ishikawa I. Er:YAG laser therapy for peri-implant infection: A histological study. Lasers Med Sci 2007;22(3):143-157.
28. Schwarz F, Hegewald A, John G, Sahm N, Becker J. Four-year follow-up of combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination. J Clin Periodontol 2013;40(10):962-967.
29. Kim J-H, Herr Y, Chung J-H, Shin S-I, Kwon Y-H. The effect of erbium-doped:yttrium, aluminium and garnet laser irradiation on the surface microstructure and roughness of double acid-etched implants. J Periodontal Implant Sci 2011;41(5):234-241.
30. Monzavi A, Shahabi S, Fekrazad R, Behruzi R, Chiniforush N. Implant surface temperature changes during Er:YAG laser irradiation with different cooling systems. J Dent (Tehran) 2014;11(2):210-215.
31. Stübinger S, Henke J, Donath K, Deppe H. Bone regeneration after peri-implant care with the CO2 laser: A fluorescence microscopy study. Int J Oral Maxillofac Implants 2005;20(2):203-210.
32. Deppe H, Greim H, Brill T, Wagenpfeil S. Titanium deposition after peri-implant care with the carbon dioxide laser. Int J Oral Maxillofac Implants 2002;17(5):707-714.
33. Deppe H, Horch H-H, Henke J, Donath K. Per-implant care of ailing implants with the carbon dioxide laser. Int J Oral Maxillofac Implants 2001;16(5):659-667.
34. Walsh LJ. The use of lasers in implantology: An overview. J Oral Implantol 1992;18(4):335-340.
35. Romanos G, Crespi R, Barone A, Covani U. Osteoblast attachment on titanium disks after laser irradiation. Int J Oral Maxillofac Implants 2006;21(2):232-236.
36. Romanos GE, Everts H, Nentwig GH. Effects of diode and Nd:YAG laser irradiation on titanium discs: A scanning electron microscope examination. J Periodontol 2000;71(5):810-815.
37. Geminiani A, Caton JG, Romanos GE. Temperature increase during CO2 and Er:YAG irradiation on implant surfaces. Implant Dent 2011;20(5):379-382.
38. Deppe H, Horch H-H, Neff A. Conventional versus CO2 laser-assisted treatment of peri-implant defects with the concomitant use of pure-phase β-tricalcium phosphate: A 5-year clinical report. Int J Oral Maxillofac Implants 2007;22(1):79-86.
39. Javed F, Samaranayake LP, Romanos GE. Treatment of oral fungal infections using antimicrobial photodynamic therapy: A systematic review of currently available evidence. Photochem Photobiol Sci 2014;13(5):726-734.
40. Sperandio FF, Huang Y-Y, Hamblin MR. Antimicrobial photodynamic therapy to kill gram-negative bacteria. Recent Pat Antiinfect Drug Discov 2013;8(2):108-120.
41. Hamblin MR, Hasan T. Photodynamic therapy: A new antimicrobial approach to infectious disease? Photochem Photobiol Sci 2004;3(5):436-450.
42. Soukos NS, Goodson JM. Photodynamic therapy in the control of oral biofilms. Periodontol 2000 2011;55(1):143-166.
43. Tremblay J-F, Dussault S, Viau G, Gad F, Boushira M, Bissonnette R. Photodynamic therapy with toluidine blue in Jurkat cells: Cytotoxicity, subcellular localization and apoptosis induction. Photochem Photobiol Sci 2002;1(11):852-856.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LITERATURE REVIEW
Romanos and Javed24
44. Sibata CH, Colussi VC, Oleinick NL, Kinsella TJ. Photodynamic therapy: A new concept in medical treatment. Braz J Med Biol Res 2000;33(8):869-880.
45. Kömerik N, Nakanishi H, MacRobert AJ, Henderson B, Speight P, Wilson M. In vivo killing of Porphyromonas gingivalis by toluidine blue-mediated photosensitization in an animal model. Antimicrob Agents Chemother 2003;47(3):932-940.
46. Donnelly RF, McCarron PA, Tunney MM. Antifungal photodynamic therapy. Microbiol Res 2008;163(1):1-12.
47. Dörtbudak O, Haas R, Bernhart T, Mailath-Pokorny G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri-implantitis. Clin Oral Implants Res 2001;12(2):104-108.
48. Eick S, Markauskaite G, Nietzsche S, Laugisch O, Salvi GE, Sculean A. Effect of photoactivated disinfection with a light-emitting diode on bacterial species and biofilms associated with periodontitis and peri-implantitis. Photodiagnosis Photodyn Ther 2013;10(2):156-167.
49. Hayek RRA, Araújo NS, Gioso MA, Ferreira J, Baptista-Sobrinho CA, Yamada AM Jr, Ribeiro MS. Comparative study between the effects of photodynamic therapy and conventional therapy on microbial reduction in ligature-induced peri-implantitis in dogs. J Periodontol 2005;76(8):1275-1281.
50. Marotti J, Tortamano P, Cai S, Ribeiro MS, Franco JEM, de Campos TT. Decontamination of dental implant surfaces by means of photodynamic therapy. Lasers Med Sci 2013;28(1):303-309.
51. De Angelis N, Felice P, Grusovin MG, Camurati A, Esposito M. The effectiveness of adjunctive light-activated disinfection (LAD) in the treatment of peri-implantitis: 4-month results from a multicentre pragmatic randomised controlled trial. Eur J Oral Implantol 2012;5(4):321-331.
52. Esposito M, Grusovin MG, De Angelis N, Camurati A, Campailla M, Felice P. The adjunctive use of light-activated disinfection (LAD) with FotoSan is ineffective in the treatment of peri-implantitis: 1-year results from a multicentre pragmatic randomised controlled trial. Eur J Oral Implantol 2013;6(2):109-119.
53. Bassetti M, Schär D, Wicki B, Eick S, Ramseier CA, Arweiler NB, Sculean A, Salvi GE. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin Oral Implants Res 2014;25(3):279-287.
54. Deppe H, Mücke T, Wagenpfeil S, Kesting M, Sculean A. Nonsurgical antimicrobial photodynamic therapy in moderate vs severe peri-implant defects: A clinical pilot study. Quintessence Int 2013;44(8):609-618.
55. Schär D, Ramseier CA, Eick S, Arweiler NB, Sculean A, Salvi GE. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: Six-month outcomes of a prospective randomized clinical trial. Clin Oral Implants Res 2013;24(1):104-110.
56. Javed F, Qadri T, Ahmed HB, Al-Hezaimi K, Corbet FE, Romanos GE. Is photodynamic therapy with adjunctive non-surgical periodontal therapy effective in the treatment of periodontal disease under immunocompromised conditions? J Coll Physicians Surg Pak 2013;23(10):731-736.

Register now at ADA.org/meeting.
Come for the Education. Stay for the Experience. #ADADC
EducationInnovative education begins at the ADA annual meeting.
Exhibit HallTouch, feel and compare an endless array of new dental products.
ConnectionsMingle with colleagues from across the nation and the world.

Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE CLINICAL CASE
Altayeb26 27
LITERATURE REVIEW
Er:YAG Laser-Assisted Bone and Gingival Augmentation Around ImplantsWalid Altayeb, DDS, MDS, PhDDoha, Qatar
J Laser Dent 2015;23(1):26-36
PRETREATMENT
A. Outline of Case
1. Clinical DescriptionA 35-year-old female patient presented with minimal attached tissue on the buccal aspect of endosseous implants at the #7 and #8 sites that had been placed more than six months earlier. The patient was undergoing prosthetic treatment and wore a tooth-supported maxillary provisional bridge (Figure 1). The referring implantologist’s report indicated that these implants were inserted at the same time of extraction of teeth #7 and #8 (immediate implantation) (Figure 2). The referring doctor noted inflammation and suppuration at the 3-month follow-up visit. He performed a nonsurgical treatment option for peri-implantitis by using antibiotics and antiseptics. He succeeded in arresting the infection process but was left with a compromised result, caused by the loss of bone and attached gingiva around the neck of the implant.
Figure 1: Photo of the patient taken by prosthodontist before treatment (7 months before referral)
Figure 2: Photo of the patient taken by the implantologist during implant insertion (6 months
before referral)
The prosthodontist was uncertain about the success of the implants and the final esthetic result, so he referred the patient to our clinic to give final recommendations about removing the implants or performing bone augmentation around them.
The options of a treatment plan were discussed with both the prosthodontist and the patient, detailing the nature and potential risks of the proposed procedures. The patient was informed that the final treatment plan would be selected after uncovering the implants and checking their stability, since the implants were still submerged and their stability was uncertain.

Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE CLINICAL CASE
Altayeb26 27
2. Medical HistoryThe patient was in excellent medical health with no medical concerns or history. She had no known allergies to any medications and was not taking any medication at the time. She had no history of bleeding or clotting disorders.
3. Dental HistoryThe patient was undergoing comprehensive dental treatment including:
· Extraction of hopeless teeth· Root canal treatment· Endosseous implant insertion· Replacement of old bridges and crowns in the
maxilla.
4. OcclusionThe occlusion was not stable since the patient was involved in full-mouth rehabilitation for the maxillary and mandibular teeth.
5. TMJExamination of both temporomandibular joints, through palpation, revealed normal movements.
6. Radiographic ExaminationThe height of the alveolar bone and the outline of the bone crest around the implants were examined radiographically (Figure 3). Most of the mesiodistal peri-implant bone support appeared to be adequate. No periapical pathology was detected on the radiographs.
Figure 3: Preoperative panoramic X-ray
7. Soft Tissue ExaminationFull-mouth periodontal probing was performed; there was no gingivitis or periodontitis. The attached gingiva was very thin on the buccal aspect of implant #7 and #8 (Figure 4). Decreasing inflammation around implants #7 and #8 was completed by the referring dentist.
There were no furcation or mobility involvements. Oral hygiene instructions were reviewed with the patient, emphasizing the importance of effective brushing twice daily and flossing once daily.
Figure 4: Preoperative anterior view showing loss of buccal bone and attached gingiva at
implant #7 and #8
8. Hard Tissue ExaminationClinical examination revealed that teeth #2, 5, 6, 7, 8, 10, 14, 18, 19, 29, 30, and 31 were missing. All remaining maxillary teeth were under endodontic treatment with provisional crowns and bridges. Endosseous dental implants were inserted during the last six months at sites #5, 7, 8, 14, 18, 19, 29, and 30.
9. Preoperative PhotographyA series of intra- and extraoral photos were taken.
10. Other TestsNo other tests were done.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1CLINICAL CASE
Altayeb28
B. Diagnosis and Treatment Plan
1. Provisional DiagnosisSurgical complications including bone resorption and insufficient attached tissue in the buccal aspect of endosseous implants #7 and #8.
2. Final DiagnosisPeri-implantitis around implants #7 and #8 caused by inadequate crestal ridge width at the time of implant placement, resulting in a knife-edge ridge of bone around the implants which was lost during the healing phase of treatment.
3. Treatment PlanOsseous and gingival regenerative surgery around dental implants #7 and #8 was planned in two-stage surgery:
a. The first stage included bone regeneration using a bone xenograft and a resorbable membrane. Use of an Er:YAG laser (2,940 nm) was to be applied at different settings to open the flap, remove the granulation tissues, contour the bone, and decontaminate the implant surfaces.
b. The second stage surgery would be performed four months after the first stage, and included uncovering implants #7 and #8 with an Er:YAG laser, the placement of a connective tissue graft, accompanied by a vestibuloplasty and the deepithelization of the gingival margins of the implants.
4. Treatment Plan Outlinea. General
Regenerative osseous and gingival surgery would be employed to promote reosseointegration, increasing the attached gingiva on the buccal aspect of the implants, and a vestibuloplasty would be performed to remove the mobile mucosa and release the frenal attachments extending into the area of the implants.
b. SpecificEr:YAG laser-assisted regenerative osseous surgery around implants presents several advantages compared to conventional treatment methods:
· The laser is capable of effectively removing plaque, biofilm, and granulation tissues on the implant surface without damaging their surfaces.
· The laser is able to recontour both hard and soft tissues with minimal necrosis of surrounding tissues caused by collateral thermal damage.
· Vestibuloplasty with the laser achieves a more sustainable result, causes minimal pain, and allows for faster and uneventful wound healing.
· Deepithelization is easily achieved with the laser without bleeding and postoperative discomfort.
5. Indications and Contraindicationsa. IndicationsTreatment: In cases of bone loss around an implant related to peri-implantitis, biomechanical stresses, and overheating of the bone where the implant is still stable and the bone loss is not too severe, the implant can often be treated and saved.
· Debridement and regenerative osseous surgery is the treatment of choice, accompanied by attempted mechanical removal of all diseased tissue from around the implant, removal of as many bacteria as possible, administration of antibiotics, and application of bone-grafting material in an attempt to regenerate the peri-implant hard tissues.

Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE
29
· A free connective tissue graft is used to increase the width and thickness of the attached gingiva to improve esthetics, and make the gingival margin bind better around the implants.
· A vestibuloplasty is indicated to ensure the presence of adequate vestibular depth around the implants which is important for oral hygiene and to prevent mechanical tension on the neck of the implant.
· Deepithelization of the gingival margins of the implant with a laser may enhance connective attachment around the implant neck by slowing epithelium growth.
Laser: The pulsed Er:YAG laser can cut and ablate tissues with excellent surgical precision and minimal collateral effects resulting in decreased tissue damage and thus faster healing. Implant surface debridement and decontamination are obtained effectively and safely with the Er:YAG laser compared to plastic curettes. With its wavelength of 2,940 nm and associated maximum water absorption, the Er:YAG laser effectively removes biofilm from the implant surface without damage.
b. ContraindicationsTreatment: Absolute contraindication would be present if the patient were suffering from serious illnesses of the hematogenic system. Implant mobility is another contraindication for this treatment.
Laser: Lasers are safe to use if the user adheres to protocols, so there was no known contraindication for the chosen wavelength in this case.
6. Precautions· The clinician must be careful to avoid
possible damage to adjacent root surfaces.· It is appropriate to use minimal power
and proper technique, minimizing the risk of collateral tissue and implant surface damage.
· Laser energy vaporizes biological tissue
and amalgam restorations; therefore the clinician must be aware of this potential danger.
· Perpendicular aiming of laser beam is to be avoided to minimize laser reflection from implant surfaces to the operator and adjacent tissues.
· Direct laser irradiation of the implant over an extended period is to be avoided so as not to impair the implant/bone surface through overheating.
· During a vestibuloplasty it is important to make sure that the laser is guided parallel to the bone in order to avoid unwanted side effects such as thermal collateral damage or unintentional bone ablation.
7. Treatment AlternativesTreatment planning in a complex implant case can be confusing because of the many different surgical and restorative approaches to solve the same problem. The possible alternative treatment for this patient could be:
a. Removal of old implants #7 and #8, with a bone augmentation procedure by the conventional approach of augmenting the ridge first and placing the implant(s) after six months of healing.
b. Removal of old implants #7 and #8, with simultaneous implant placement with a bone augmentation approach in which bone grafting is done at same time as implant placement.
c. Use of plastic therapeutic instruments for implant surface debridement and topical citric acid or tetracycline after debridement as substitute for the laser.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1CLINICAL CASE
Altayeb30
Depending on the situation, the removal of infected implants and a two-stage bone augmentation technique of the alveolar ridge are more advantageous than other approaches in achieving esthetic results with better predictability. This is due to the fact that gingival morphology follows the shape of the underlying bone, and it is difficult to build esthetically acceptable gingiva in areas with vertically deficient supporting bone. For financial reasons and the number of treatments, the patient chose to keep the affected implants after the proposed treatment. The prosthodontist supported the patient preference especially since the patient had a low smile line which hid the vertical tissue loss around the implant and expected asymmetry of gingival contour with adjacent teeth.
8. Informed ConsentFollowing discussion of the relative risks/benefits and treatment alternatives with the patient and prosthodontist, the Er:YAG laser-assisted regenerative tissue surgery in a two-stage procedure was decided. Written consent was signed by the patient and prosthodontist.
TREATMENT
A. Treatment ObjectivesImprove the functional and esthetic longevity of dental implants through:
· Regeneration of subsequent bone in the buccal aspect of dental implants #7 and #8.
· Establishing a healthy gingival contour around implants. This can be done through the widening of attached gingiva to enhance plaque removal around the gingival margin, reduce inflammation, and improve esthetics.
B. Laser Operating ParametersThe instrument of choice was an Er:YAG laser (K.E.Y. Laser, KaVo Dental GmbH, Biberach, Germany) with the following operating features:
· Wavelength: 2940 nm· Pulse energy: 80 to 600 mJ· Pulse frequency: 2 to 30 Hz· Pulse Width: 250 µs· Average Power: 0.16 to 7.8 W· Emission mode: Free-running pulse· Delivery system: Flexible quartz-silica optical
fiber with an additional rigid quartz or sapphire tip
· Tip diameter: Disposable 400-micron width, lengths either 6 mm or 18 mm
Specific laser operating parameters for this treatment were:
1. The flap incision: 100 mJ/pulse, 25 Hz, with air, no water. Laser handpiece 2062 with fiber insert size 50/10 (0.47 mm diameter and 10 mm length) in contact mode. Total estimated exposure duration was 2 minutes.
2. Vaporization of granulation tissue and bone recontouring: 120 mJ/pulse, 20 Hz, with maximum water and air. Laser handpiece P2061 with cylindrical fiber (1.1 mm diameter, circular flat exit surface) in near-contact mode, as close as possible to the target without direct contact. Total estimated exposure duration was 2 minutes.

Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE
31
3. Implant debridement and decontamination: 100 mJ/pulse, 10 Hz, with maximum water and air. Laser handpiece 2061 and cylindrical fiber (1.1 mm diameter, circular round exit surface) in noncontact (defocused) mode, at least 5 mm from the target tissue. Total estimated exposure duration was 1 minute.
4. Vestibuloplasty: 300 mJ/pulse, 15 Hz, with air, no water. Laser handpiece 2062 with fiber insert size 50/10 in contact mode. Total estimated exposure duration was 2 minutes.
5. Deepithelization: 140 mJ/pulse, 6 Hz, with air, no water. Laser handpiece 2060 in noncontact mode, at least 5 mm from the target tissue. Total estimated exposure duration was 1 minute.
C. Preliminary to Patient TreatmentPrior to the treatment, the following safety precautions were implemented:
· Infection control guidelines were respected for the environment, patient, and dental staff.
· A safe environment was maintained by restricting operating room access to persons not involved in the treatment, posting warning signs, and minimizing highly reflective surfaces.
· All instruments were pre-dispensed prior to treatment commencing. High-volume evacuation was used.
· The patient and all staff members working in the above-mentioned safety controlled area wore protective glasses specific for the laser.
· The laser was first test-fired outside of the patient’s mouth. The patient was then seated and appropriate safety equipment was utilized.
D. Treatment Delivery SequenceFirst Stage Surgery
1. After cleansing the preparation site and disinfection with chlorhexidine, a topical anesthetic (benzocaine) was placed from tooth areas #6 to #9, followed by local anesthesia (articaine HCl 4% and adrenaline 1:200,000,
Ubistesin™, 3M™ ESPE™, Seefeld, Germany).2. The implants were accessed with an appropriate
laser incision. The procedure was started with a vertical incision for release with handpiece E 2062 and fiber (50/10). The incision was performed on the mesial aspect of tooth #9, followed by a crestal incision on the alveolar ridge, to the mesial of tooth #4. Down-pressure on the tissue was avoided so as to protect the tissue and prevent the fiber from adhering to it. The energy used for the incision was 100 mJ per pulse at 25 Hz. Average power: 2.5 W, in contact mode without water irrigation. It was noted that at site #8 there was bone loss to the sixth thread on the buccal aspect, and at site #7 the implant body was transparent through thin buccal bone (Figure 5).
Figure 5: View after raising the flap shows bone loss to the sixth thread of implant #8 and very thin buccal
bone of implant #7

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1CLINICAL CASE
Altayeb32
3. Once the implant and the surrounding bone were exposed, the diseased tissue was vaporized by the laser using the 1.1 mm cylindrical tip, 2.4 W average power with air and water irrigation. The tip of the laser was in contact with the bony crest and maximum water spray cooling was applied to avoid thermal damage. By ablating a thin layer of bone, a new, healthy bone surface was achieved and necrotic bone was removed.
4. After the treated site was cleaned by ablating tissue and blood on the threads, the implant surface was decontaminated using a cylinder tip (1.1 mm) with the tip almost parallel to the implant surface, 1 W average power with air and water irrigation (Figure 6).
Figure 6: Removal of plaque biofilm and granulation tissue using a cylindrical fiber tip of an Er:YAG laser
5. The bone defects around the implant #7 and #8 were filled with anorganic bovine-derived bone mineral matrix (NuOss™, Collagen Matrix, Inc., Franklin Lakes, N.J., USA) and resorbable collagen membrane (RCM6™, Collagen Matrix, Inc., Franklin Lakes, N.J., USA) which was fixed in place with titanium pins (Figures 7 and 8).
Figure 7: Filling the defect with bone substitute
Figure 8: Buccal view of resorbable collagen membrane secured over the graft with titanium pins
6. Sutures were applied using 4-0 silk, and primary closure was achieved. A provisional fixed bridge was placed during the healing period (Figure 9).
Figure 9: Post-first surgery view shows wound closure and provisional fixed bridge
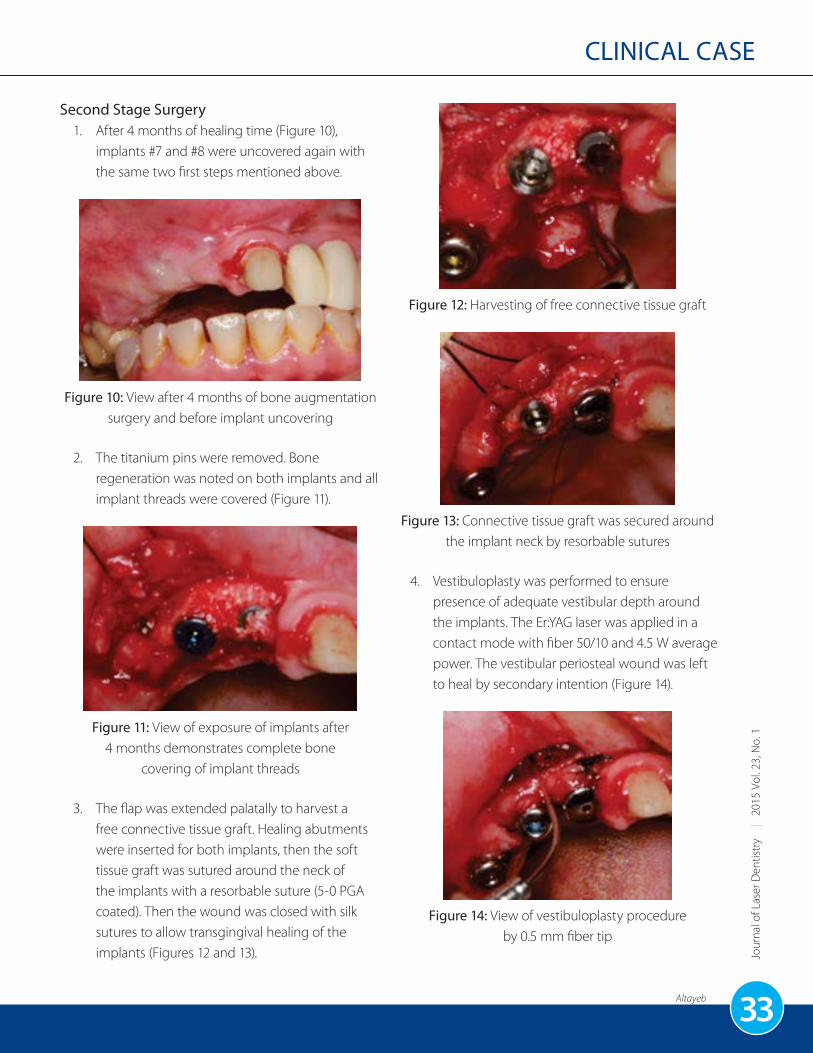
Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE
33
Second Stage Surgery1. After 4 months of healing time (Figure 10),
implants #7 and #8 were uncovered again with the same two first steps mentioned above.
Figure 10: View after 4 months of bone augmentation surgery and before implant uncovering
2. The titanium pins were removed. Bone regeneration was noted on both implants and all implant threads were covered (Figure 11).
Figure 11: View of exposure of implants after 4 months demonstrates complete bone
covering of implant threads
3. The flap was extended palatally to harvest a free connective tissue graft. Healing abutments were inserted for both implants, then the soft tissue graft was sutured around the neck of the implants with a resorbable suture (5-0 PGA coated). Then the wound was closed with silk sutures to allow transgingival healing of the implants (Figures 12 and 13).
Figure 12: Harvesting of free connective tissue graft
Figure 13: Connective tissue graft was secured around the implant neck by resorbable sutures
4. Vestibuloplasty was performed to ensure presence of adequate vestibular depth around the implants. The Er:YAG laser was applied in a contact mode with fiber 50/10 and 4.5 W average power. The vestibular periosteal wound was left to heal by secondary intention (Figure 14).
Figure 14: View of vestibuloplasty procedure by 0.5 mm fiber tip

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1CLINICAL CASE
Altayeb34
5. Deepithelization of gingival margins was achieved by a 2060 laser handpiece, 0.84 W average power in defocused mode (10 mm away from gingival tissue) (Figures 15 and 16).
Figure 15: View of laser deepithelization procedure by defocused mode
Figure 16: View immediately following second stage surgery
E. Postoperative InstructionsAfter both surgical phases, verbal and written postoperative instructions were given to the patient. No gingival pack was applied in either stage. The patient was placed on clavulanic acid (Augmentin 1 g) one tab every 12 hours for 7 days; ibuprofen (600 mg) one tab every eight hours for three days, and chlorhexidine rinse twice a day for 10 days. The patient was evaluated postoperatively at 3 and 10 days.
F. ComplicationsThe patient had no complications during either surgical phase.
G. PrognosisThe prognosis was very good during the postoperative period.
H. Treatment RecordsAll procedural details were entered in the patient’s treatment notes, along with the consent forms, radiographs, and chartings.
FOLLOW-UP CARE
A. Assessment of TreatmentThe patient was first assessed at one week, and then at one month after each stage of surgery. This case was followed for 16 months. All through the follow-up care, there was no sign of any complications related to the laser treatments. The recovery was relatively uneventful.
During the first three days following each surgical session, the patient reported moderate pain and moderate swelling. There was no tissue bleeding and the site remained closed, and the flap showed signs of attachment and was healing nicely. At 1 week postoperative, the patient returned for inspection and removal of sutures; the swelling had resolved and the patient no longer had complaints of pain (Figure 17).
Figure 17: One week postoperative view

Altayeb
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
CLINICAL CASE
35
One month after second-stage surgery (implant exposure), the soft tissue was completely healed (Figure 18), and there were no reported complications, no recession, no bleeding, and no implant mobility. Six months after the start of treatment, the full-mouth rehabilitation was completed by the prosthodontist with ceramic crowns on the teeth and implants. The radiographs confirmed improved bone levels surrounding the implants with no evidence of bony defects (Figure 19).
Figure 18: One-month postoperative view demonstrating tissue healing. Note increasing width
and thickness of attached gingiva with adequate vestibular depth
Figure 19: Radiograph taken at 6-month postoperative interval showing improvement in bone level
Healing assessment at the 9- and 16-month appointments showed that the patient had excellent healing and improved tissue color, contour, and consistency. Gingival tissue was well attached and gingival margins were stable (Figures 20 and 21).
Figure 20: View after 9 months of uneventful healing. Note the healthy gingival contour around implants
Figure 21: Postoperative photograph at 16 months shows excellent healing around implants
#7 and #8. Note the improved vestibule depth and stability of attached gingiva
B. ComplicationsThere were no significant postoperative complications. As expected, severe ridge deficiency resulted in a long implant-supported fixed restoration. The prosthodontist used pink porcelain to mask the increased length of the crowns. As anticipated, the patient’s low lip smile line hid this compromised esthetic result.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1CLINICAL CASE
Altayeb36
C. Long-Term ResultsThe long-term results were felt to be good at the 16-month recall visit, the soft tissue remained healthy, and no gingival or bone recession was observed. The tissue healing remained relatively the same through the postoperative period. The final reconstruction demonstrated a functional and esthetic outcome. The results were satisfactory to the patient and the clinician.
D. Long-Term PrognosisThe use of an Er:YAG laser in regenerative osseous surgery around implants presents several advantages over conventional treatment, with no complications and with high patient and clinician satisfaction and confidence.
AUTHOR BIOGRAPHY
Walid Altayeb received his dental degree from the Faculty of Dentistry, Damascus University in 1998, and completed his Master of Science in Periodontics in 2004 and Doctorate of Philosophy in Periodontics in 2007. He is a Fellow and Master of the Academy of Laser Dentistry. He has served as lecturer in the Department of Periodontics, Damascus University. He has participated in many conferences in the Middle East, Spain, and USA as speaker in the fields of periodontal medicine and laser dentistry. Dr. Altayeb has achieved an advanced level of knowledge about the application of lasers in dental science and patient treatment (Advanced Proficiency certificates from the Academy of Laser Dentistry in 980-nm diode and 2940-nm Er:YAG lasers). He is currently Chair of the ALD affiliate study club in Qatar and is working in private as a periodontist and implantologist in Madina Dental Center, Doha. Dr. Altayeb may be contacted by e-mail at [email protected].
Disclosure: Dr. Walid Altayeb has no financial arrangements with any corporate organization related to this article.

Lavere et al.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
SCIENTIFIC RESEARCH
37
Antimicrobial Effects of the 810-nm Diode Laser in the Treatment of Peri-Implantitis: An Ex Vivo Pilot StudyErica Lavere, BS, DDSUniversity at Buffalo School of Dental Medicine, Buffalo, New York, USA
Juliana Sagor, BA, DDSDental Resident, St. Barnabas Hospital, New York, New York, USA
Lynn MikulskiResearch Support Specialist, University at Buffalo School of Dental Medicine, Buffalo, New York, USA
Sebastiano Andreana, DDS, MSAssociate Professor and Director of Implant Dentistry, University at Buffalo School of Dental Medicine, Department of Restorative Dentistry, Buffalo, New York, USA
J Laser Dent 2015;23(1):37-43
ABSTRACT
Background: Peri-implantitis is a condition associated with the presence of bacteria along the surfaces of implants, creating deleterious effects to the peri-implant hard and soft tissues.
Objective: This ex vivo pilot study compared three settings on an 810-nm diode laser to determine optimal laser power levels to suppress bacteria growing in a bony defect adjacent to an implant.
Materials and Methods: The study was conducted in two phases. Fourteen sterile titanium implants were placed into sterilized porcine ribs. A 2 mm x 2 mm wide, 3 mm deep defect adjacent to the implant was created. Three microliters of S. sanguinis ATCC® 10556™ in ½ brain heart infusion were inoculated into the defect and left for 24 hours in 5% CO2 at 37°C. For Study 1, four defects were not treated with the laser, and 3 were treated with an 810-nm diode laser at 0.6 Watt, 4 at 0.8 W, and 3 at 1.0 W. The laser tip was noninitiated and laser energy
was delivered in continuous mode. Defects were rinsed with ½ brain heart infusion transport media and bacteria were plated on tryptic soy agar (TSA) media and left for 48 hours to grow. The colony-forming units (CFUs) were counted. The experiment was repeated three times. Following results from Study 1, a second study was performed. Study 2 involved the use of 3 microliters of indocyanine green as chromophore, delivered into the peri-implant bony defect. The same power settings and techniques were followed as in Study 1.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1SCIENTIFIC RESEARCH
Lavere et al.38
Results: The amount of post-treatment growth varied within the 0.6 W and 0.8 W groups, with an average count of CFUs of 56 and 30 respectively, whereas the 1.0 W group showed a barely detectable growth, 0.33 CFUs. The untreated defects (control group) showed an average CFU count of 207 (P < 0.5), with the differences in the 1.0 W group being statistically significant. Study 2 revealed an additional antimicrobial effect when indocyanine green was added in the 0.8 W and 1.0 W, but not in the 0.6 W groups.
Conclusions: The 810-nm diode laser at 1.0 W was successful in minimizing bacteria growth in ex vivo peri-implantitis defects, whereas even lower laser power levels were able to remarkably diminish the amount of bacteria. One Watt diode laser treatment could be an effective setting to use when treating peri-implantitis cases. The addition of a chromophore increased the antimicrobial activity at 1.0 W, indicating a possible clinical advantage of the photodynamic-enhanced antimicrobial therapy.
Key words: Dental lasers, Peri-implantitis, Indocyanine green, Antimicrobial effect
INTRODUCTION
Peri-implantitis is an emerging and growing problem in the dental field due to the increased placement of implants to restore edentulous spaces. This condition is associated with the presence of bacteria along the surfaces of implants creating deleterious effects to the peri-implant hard and soft tissue. Peri-implantitis is detrimental to the health of the tissue around the implant and to the function of the implant due to the way that peri-implantitis causes a loss of supporting bone.1 A recent review demonstrated that the prevalence of peri-implantitis is 21.7%. This statistic was generated through a meta-analysis of numerous different case studies.2 It is difficult to generate a true statistic because of the way in which different studies use different thresholds of disease. But from this percentage it may be concluded that the occurrence is high and it is crucial to be able to predictably eliminate disease around implants and to decrease failure rates. There are many different ways to treat this condition but there is no consensus on which treatment is most effective. Mechanical debridement with chlorhexidine and the use of amino acid glycine powder are among the alternative treatments.3 Other topical treatments have been reported such as the use of tetracycline slurry,4 and minocycline in a microsphere slow-release system.5
The diode laser has been used in various in vitro studies to decontaminate titanium surfaces. In most investigations of the decontamination of titanium surfaces a flat titanium disc has been used. Titanium discs do not represent the true clinical surface properties of implants, therefore using actual dental implants is important in evaluating the effectiveness of laser treatment in decontaminating peri-implant defects and implant surfaces. The main difference between the titanium disc and the implant is that the implant has a curvy surface.6 The diode laser is one of the most utilized lasers by dental professionals. A study that surveyed five different lasers commonly used in dentistry demonstrated that 63% of dentists who use a laser use a diode laser.7 The aim of this study was to determine the lowest laser wattage that could be used with the 810-nm diode laser that would still be effective in eliminating bacteria from a peri-implant defect and implant surface.

Lavere et al.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
SCIENTIFIC RESEARCH
39
MATERIALS AND METHODS
Fresh porcine ribs were obtained from a local butcher. All skin and meat were removed from the ribs until just bone remained. The ribs were then cut into 14 bone blocks. Next, the bone blocks were sterilized in a steam autoclave. Under a clean surgical environment, incorporating sterile drapes, gloves, and instrumentation, a sterile number two round bur was then used to create a pilot hole prior to placing implants. The implant space was then prepared using an implant kit (Nobel Biocare, Zurich, Switzerland). Fourteen sterile titanium implants were placed into the bone blocks (Brånemark MKIII, Nobelpharma, Yorba Linda, Calif., USA). Each implant was treated with glow discharge for 60 seconds before placement to maintain surface properties. Previous studies including the ones from Youngblood and Ong8 and Baier et al.9 have clearly demonstrated that glow-discharge surface treatment could be used as alternative treatment to sterilize the implant surface, without negatively affecting the biological properties of the titanium surfaces. A 2 mm x 2 mm wide, 3 mm deep circumferential defect was created adjacent to the implant. Three microliters of S. sanguinis ATCC 10556 in ½ brain heart infusion (BHI) were inoculated into the defects. The bone blocks were then placed into separate sterile containers and left for 24 hours in an atmosphere of 5% CO2 at 37°C.
After 24 hours the containers were opened and the bone blocks were exposed for decontamination with the laser. Three laser power levels were used in this study. Three bony defects were treated with the laser (Odyssey® 2.4G, Ivoclar Vivadent, Amherst, N.Y., USA) at 0.6 W, four at 0.8 W, and three at 1.0 W. The laser was not initiated and was used in continuous mode for 30 seconds in each defect. Four defects were not treated with the laser to serve as a control group. Defects were rinsed with ½ brain heart infusion (BHI) transport media; 1:1000 dilutions were made of the transport media and bacteria were plated on tryptic soy agar (TSA) plates
and left for 48 hours to grow. The colony-forming units (CFUs) were counted. The experiment was repeated three times. The study was then repeated with one added parameter. Indocyanine green (IG), which is a medical diagnostic dye, was used as a chromophore. Three microliters of this dye was pipetted into each defect before laser treatment. The groups in this trial were the control groups, which consisted of no laser treatment and no IG, and no laser treatment with IG. The 0.6, 0.8, and 1.0 W test groups were divided into laser treatment only and laser with IG. Refer to Figure 1 for the model.
Figure 1: Experimental model showing implant inserted into bone block with laser fiber inserted into
the defect adjacent to the implant.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1SCIENTIFIC RESEARCH
Lavere et al.40
RESULTS
The initial experiments showed that bacteria growth on the agar plates decreased from the control group (no laser treatment) to the group that was treated with 1.0 W. After this experiment was repeated three times for the control group, the average number of colony-forming units was 590.5. The average number for the group that was treated with 0.6 W was 56 CFUs, and the group treated with 0.8 W averaged 30 CFUs. The 1.0 W group showed minimal to no detectable growth with an average of 0.33 CFUs (Figure 2). The control group’s average CFU count of 590.5 was statistically significantly different from the group treated with 1.0 W (P < 0.5).
0
100
200
300
400
500
600
700
CFU
Laser Power Levels in WattsCONTROL 0.6 W 0.8 W 1.0 W
"
Figure 2: Colony-forming unit averages for specific laser power levels in first phase of the study
Results from the trials using IG as a chromophore were similar to the initial study, however the 0.6 W group did not follow the same trend of the 0.8 W and 1.0 W groups. The control group that received no laser treatment and had no green dye present had an average CFU count of 192 (SD 35.0). The control group that contained indocyanine green but no laser treatment had a count of 129.25 CFUs (SD 5). The 0.6 W laser-treated group without indocyanine green averaged 39.5 CFUs (SD 4.3), and the 0.6 W group with IG averaged 103.5 (SD 10.6). The 0.8 W laser treated group without indocyanine green averaged 58.5 CFUs (SD 7.7) and the group with IG averaged 0 CFUs. The 1.0 W laser treated group without IG averaged 18.5 CFUs (SD 24.1) and the group with IG averaged 0 CFUs (Figure 3).

Lavere et al.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
SCIENTIFIC RESEARCH
41
CG = Cardio green (indocyanine green)
0
50
100
150
200
250
No Laser No CG No Laser CG 0.6 W No CG 0.6 W CG 0.8 W No CG 0.8 W CG 1.0 W No CG 1.0 W CG
CFU
Laser Power Levels in Watts
Figure 3: Colony-forming unit averages for specific laser power levels for defects with and without indocyanine green in second phase of the study
DISCUSSIONThis study reports the effect of suppressing S. sanguinis growth on implant surfaces. The results indicate that the 810-nm diode laser at the parameters used in the present study was successful in suppressing bacterial growth in ex vivo peri-implant defects.
Several comments, however, have to be reported. The use of this model is of foremost relevance. In vitro laboratory studies have been conducted primarily on titanium discs. This allows for the direct access to the implant surface, not representing the true clinical scenario for the dentist. Our study mimics closely the real clinical setting, with real bone facing the contaminated implant surface. It is worthwhile to mention some of the differences with the real-life situation. In our model, there is a lack of body fluids, such as saliva and blood. In addition, the second study involved the use of a specific chromophore. In real life, the blood due to the peri-implant inflammation serves as a chromophore for the diode laser.
In our study we used indocyanine green as a chromophore. This particular dye, while safe, was also tested by Boehm and Ciancio10 in combination with the 810-nm diode laser on periodontal pathogens. The results of their in vitro study indicated that this combination has a successful bactericidal effect, at very minimal wattages ranging between 0.1 and 0.5 W in continuous mode. However their study aimed at investigating the killing effect in bacterial pellets. Our study adopted similar techniques, but the killing effect was evaluated on implant surfaces inserted into real bone. From the results of the present study, when the chromophore was used with 0.8 W, the level of bacteria suppression was similar to the results obtained when the chromophore was not used in the 1.0 W group. It is important to report, however, that the IG had some antimicrobial effect on its own as shown in the nonlaser treated group. This aspect leads to two points of discussion: (1) IG may have some antimicrobial effect, and (2) IG is safe on mammalian cells. These points possibly strongly suggest its clinical use, being safe on the human body and having a killing effect on bacteria.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1SCIENTIFIC RESEARCH
Lavere et al.42
Our model used S. sanguinis as the tested microorganism. S. sanguinis is one of the pioneer bacteria colonizing oral surfaces.11 Pioneers are the first colonizers on surfaces. With development of the early biofilm, additional bacterial species may colonize, including the pathogenic species. Future studies involving use of a mixed biofilm may provide additional and more clinically relevant data.
It has been reported that the diode laser may overheat the implant surfaces, therefore transmitting high temperatures to the peri-implant bone. An ex vivo study conducted by and Beneduce et al.12 has indicated that the temperature rise from 36.5°C is negligible and still within physiological parameters. The above-mentioned study was performed having the specimens at 36.5°C in a water bath, to mimic as much as possible the clinical conditions.
CONCLUSIONS
Overall, this ex vivo study has indicated an antimicrobial effect of the 810-nm laser on dental implants laced in real bone. Furthermore, it may be concluded that indocyanine green in combination with low-wattage 810-nm diode laser irradiation could be used to decontaminate implant surfaces colonized by S. sanguinis. Further studies are needed to confirm preliminary reports presented by Kutkut et al. on humans.13 In their case report, the investigators used an 810-nm diode laser to further decontaminate infected dental surfaces in conjunction with topical antibiotic therapy, prior to successful bone regeneration treatment. The laser was used at 1 W in continuous mode, without the use of IG.
CORRESPONDING AUTHOR BIOGRAPHY
Dr. Lavere is a pediatric dentistry resident at the University at Buffalo School of Dental Medicine and Women and Children’s Hospital of Buffalo, New York. She may be contacted by e-mail at [email protected].
Disclosure: Dr. Lavere has reported no commercial affiliations or personal conflicts of interest relative to this article.
Editor’s Note: This research was performed while Ms. Lavere was a 4th-year dental student at the University of Buffalo School of Dental Medicine, Buffalo, New York, USA.

Lavere et al.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
SCIENTIFIC RESEARCH
43
REFERENCES
1. Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontol 2000 1998;17(1):63-76.
2. Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 2015;42(Suppl 16):S158-S171.
3. Sahm N, Becker J, Santel T, Schwarz F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: A prospective, randomized, controlled clinical study. J Clin Periodontol 2011;38(9):872-878.
4. Muller E, González YM, Andreana S. Treatment of peri-implantitis: Longitudinal clinical and microbiological findings – A case report. Implant Dent 1999;8(3); 247-254.
5. Renvert S, Lessem J, Dahlén G, Renvert H, Lindahl C. Mechanical and repeated antimicrobial therapy using a local drug delivery system in the treatment of peri-implantitis: A randomized clinical trial. J Periodontol 2008;79(5):836-844.
6. Barfeie A, Wilson J, Rees J. Implant surface characteristics and their effect on osseointegration. Br Dent J 2015;218(5):E9. doi: 10.1038/sj.bdj.2015.171.
7. Knight R. See the light. Dent Prod Rep 2009;43(3):30-32, 35-37.
8. Youngblood T, Ong JL. Effect of plasma-glow discharge as a sterilization of titanium surfaces. Implant Dent 2003;12(1):54-60.
9. Baier RE, Meyer AE, Natiella JR, Natiella RR, Carter JM. Surface properties determine bioadhesive outcomes: Methods and results. J Biomed Mater Res 1984;18(4):337-355.
10. Boehm TK, Ciancio SG. Diode laser activated indocyanine green selectively kills bacteria. J Int Acad Periodontol 2011;13(2):58-63.
11. Hauser-Gerspach I, Kulik EM, Weiger R, Decker E-M, Von Ohle C, Meyer J. Adhesion of Streptococcus sanguinis to dental implant and restorative materials in vitro. Dent Mater J 2007;26(3):361-366.
12. Beneduce C, Angelova D, Angelov N, Andreana S. Thermal propagation of 810nm diode laser in porcine dermal tissues. J Dent Res 2008;87(Spec. Issue A): Abstract 0950.
13. Kutkut A, Andreana S, Al-Sabbagh M. Treatment of periimplant infection in the posterior maxilla, with 810-nm diode laser decontamination of the implant surfaces: A case report. J Laser Dent 2011;19(3):270-275.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LETTERS
44
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LETTERS
44
Letters to the EditorThe Journal of Laser Dentistry welcomes letters from readers on topics of current interest to Academy of Laser Dentistry members. The Journal reserves the right to edit all correspondence and requires that all letters be signed. The views expressed are those of the letter writer and do not necessarily represent the opinion or official policy of the Academy or the editors of the Journal.
MORE ON LASER-ASSISTED ORTHODONTIC TOOTH MOVEMENT
Dose windows in laser orthodontics – a comment on: “The Effect of Pulsed 810-nm Low-Level Laser Therapy on the Rate of Orthodontic Tooth Movement: A Randomized Clinical Trial” by Dr. Monica K. Gawlik et al. (J Laser Dent 2014;22(2):70-78).
Dear Editor,
A desire to increase the velocity of tooth move-ment in orthodontics has produced several suggestions for therapeutic approaches, low-level laser (LLL) being one of them. The literature is still unambiguous.1
LLL can produce two biological effects: stimula-tion and inhibition, depending on the applied dose and energy. As for inhibition, several studies have confirmed that the application of LLL can reduce postoperative pain. The mechanism is still not quite clear, but the investigation by Chow2 suggests the formation of transient axonal vari-cosities, lowering the rate of neural flow. Reduc-tion of pain requires fairly high energies.
On the other hand, lower energies and doses are required for stimulation. The possible influ-ence on tooth velocity should presumably be based upon stimulation, not upon inhibition. This leads to the assumption that there are two separate dose windows for laser orthodontics – low energies for increase of the velocity of tooth movement and high energies for pain reduction. If there is an overlapping area, the two effects would both still be in a suboptimal part of both
windows. But indeed, Youseff3 reports consider-able pain reduction and increased tooth velocity using 8 J per tooth.
In the present study, the dose is claimed to be 16 J/cm2, based upon 200 mW and 80 seconds of irradiation. This is actually 16 joules (J) and not 16 joules per cm2.
16 J over one tooth is, according to the available literature, rather in the pain-relieving window than in the stimulatory window. However, the effect on pain reduction was not studied in the present paper.
The dose (J/cm2) is calculated as the applied energy (J) divided by the irradiated area. Apply-ing 1 J over an area of 1 cm2 results in a dose (fluence) of 1 J/cm2. If the irradiated area is 0.5 cm2, the same applied energy results in a dose of 2 J/cm2. In the present study, the size of the irradiated area was 0.4 mm (400 microns) and the dose becomes extremely high in each spot. This further contributes to the conclusion that the laser parameters were outside of the stimu-latory window. The misunderstanding of what is energy and dose is too common, and the 8 J ap-plied in the study by Youseff is also called “dose.”

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
LETTERS
45
A complicating factor in the evaluation of optimal parameters is that stimulation is best achieved with low output and long time.4
The use of traditional Class IV dental lasers for biostimulation has pros and cons. The advan-tage of course is that with a reduced handpiece, the dentist can perform biostimulation without investing much money. The downside is that the
control over the parameters is difficult, if at all possible. Using the thin fiber in a scanning mode from a slight distance is a possibility, but the control is still uncertain. It is recommended that a biostimulation handpiece should preferably have a “laser eye” of 0.25 or 0.5 cm2. That would make the calculation easy: 1 joule with the 0.25 cm2 laser eye produces a dose of 4 J/cm2.
Sincerely,
Jan Tunér, DDSPrivate Dental Clinic, Grängesberg, SwedenEditor of Laser Annals
REFERENCES
1. Abdallah M-N, Flores-Mir C. Are interventions for accelerating orthodontic tooth movement effective? Evid Based Dent 2014;15(4):116-117.
2. Chow RT, David MA, Armati PJ. 830 nm laser irradiation induces varicosity formation, reduces mitochondrial membrane potential and blocks fast axonal flow in small and medium diameter rat dorsal root ganglion neurons: Implications for the analgesic effects of 830 nm laser. J Peripher Nerv Syst 2007;12(1):28-39.
3. Youssef M, Ashkar S, Hamade E, Gutknecht N, Lampert F, Mir M. The effect of low level-laser therapy during orthodontic movement: A preliminary study. Lasers Med Sci 2008;23(1):27-33.
4. Castano AP, Dai T, Yaroslavsky I, Cohen R, Apruzzese WA, Smotrich MH, Hamblin MR. Low-level laser therapy for zymosan-induced arthritis in rats: Importance of illumination time. Lasers Surg Med 2007;39(6):543-550.
Dr. Tunér may be contacted by e-mail at [email protected].
Disclosure: The author has no commercial bond to any laser manufacturer.
THE AUTHOR RESPONDS
Dear Editor,
The comments by Dr. Tunér are appreciated. However, the statement that the laser parameters used were outside of the stimulatory window based on previous studies cannot be made, as all previous studies employed a continuous laser setting.

Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1LETTERS
46
If the laser light had been delivered in a continuous mode, the dose used in this study would likely have been too high for stimulation of tooth movement. However, as described in the paper, it is very difficult to quantify the level of energy emitted from lasers operating in pulsed modes. There are two distinct power measurements for a pulsed laser: peak power and average power. Peak power is a measure of the rate at which energy is emitted during the pulse, whereas average power measures the average rate at which energy flows from the laser during an entire cycle. As this was the first study to determine the effect of low-level laser therapy (LLLT) on tooth movement using a pulsed mode, an estimate of dose prescription was necessary.
In another arm of this study (not reported in the paper), the same laser parameters were used to exam-ine the effect of the pulsed laser on pain during canine retraction. It was concluded that pain in ortho-dontic patients can be significantly reduced with the administration of pulsed LLLT.
It would be most advantageous to the clinician if the same laser could be used for both biostimulation of tooth movement and pain reduction. Controlling the size of the irradiated area by varying the hand-piece would undoubtedly increase the adoptability of this technology by orthodontists.
Sincerely,
Monica Gawlik, DDS, MSc, FRCD(C)Private Orthodontic Practice, Toronto, Ontario, Canada

Editor’s Note: The following 4 abstracts are offered as topics of current interest. Readers are invited to submit to the
editor inquiries concerning laser-related scientific topics for possible inclusion in future issues. We’ll scan the literature
and present relevant abstracts.
Antimicrobial Effects of PhotosensitizersIn their report on “Antimicrobial Effects of the 810-nm Diode Laser in the Treatment of Peri-Implantitis: An Ex Vivo Pilot Study” (pages 37-43), Dr. Erica Lavere and colleagues observe that the tested chromophore indocyanine green enhanced the antimicrobial activity of laser irradiation. They also found that the chromophore exhibited some antimicrobial effect of its own, without the application of laser light.
How effective are such chromophores – by themselves – in promoting bacterial reduction? How do they work? And what are some of the factors that influence their effectiveness?
Indocyanine green is most commonly used as an intravenous diagnostic dye to determine blood flow in organs such as the eyes, kidneys and lungs; to measure cardiac output; and in liver function tests.1
Two other chromophores, methylene blue and the related chemical compound toluidine blue, are customarily used as biologic stains. Methylene blue is also used to treat cyanide poisoning and other conditions; as a surgical marker; and as a potent, reversible monoamine oxidase inhibitor.1-2 When used pharmaceutically, toluidine blue has been utilized to treat menstrual disorders and to detect oral and gastric carcinomas.1
All three substances have also been tested experimentally as photosensitizers to determine their relative bactericidal effects in a technique called antimicrobial photodynamic therapy, alternately termed photoactivated disinfection, photodynamic inactivation, and lethal photosensitization, among other names.
A photosensitizer is an agent that increases a material’s sensitivity to electromagnetic radiation.3 In medicine, the term photodynamic therapy (PDT) generally refers to the process whereby a photosensitizing agent is administered intravenously and selectively concentrates in metabolically active tumor tissue. Following exposure to specific wavelengths of light, cytotoxic free radicals are produced that selectively destroy the photosensitized tissue.1
The principal is similar in experimental dental applications of antimicrobial photodynamic therapy. In such uses, the generation of highly reactive singlet oxygen during excitation of a photosensitizer is considered the main antimicrobial agent. The singlet oxygen oxidizes cellular targets such as membrane, enzymes, and lipids that lead to destruction of bacteria.4
Wilson, Gibson, and colleagues5-6 posited that raising the redox potential of the periodontal pocket should create an environment unsuitable for the growth of anaerobic periodontal pathogens. They applied the redox dye methylene blue to test sites in human patients; no light activation was used. They then collected samples from the periodontal pockets via sterile endodontic paper points for bacteriological analysis. The investigators noted reductions in proportions of black-pigmented anaerobes, spirochetes, and motile bacteria.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
47

Table 1 summarizes the findings of selected studies that have examined the antimicrobial effects of a number of photosensitizers on a variety of microorganisms relevant to dentistry. Featured are indocyanine green, methylene blue, and toluidine blue.
Generally, while not shown in the table, antimicrobial properties of photosensitizers are most pronounced when the agent has been “photoexcited” by subablative levels of irradiation from various laser devices, light-emitting diodes (LEDs), or curing lights. Pertinent to the focus of this survey, the last column of the table highlights the effects of the agent itself, when used without the accompanying irradiation, on specified microbes. Results vary from mild or significant reductions in bacteria to no significant effect.
Table 1: Antibacterial Effects of Selected PhotosensitizersWhen Used Without Light Activation
Study Design Investigators Microbe(s) Photosensitizer(s)Light Source(s) for Photoactivation
Effect of Photosensitizer(s) Alone
In vitro suspensions
7Omar et al., 2008
Staphylococcus
aureus (S.a.),
Streptococcus
pyogenes (S.p.)
Indocyanine Green 808 nm GaAlAs laser
Small reduction in S.a. viable count;No significant reduction in viability of S.p.
In vitro
suspension
8Nagahara et al., 2013
Porphyromonas
gingivalis (P.g.)
Indocyanine Green 805 nm diode laser No effect on P.g. viability
In vitro
suspensions
9Topaloglu et al., 2013
S.a.,
Pseudomonas
aerunginosa (P.a.)
Indocyanine Green 809 nm diode laser No lethal effect on any strain
In vitro
suspensions
10Kranz et al., 2015
Aggregatibacter
actinomycetem-
comitans
(Ag.a.), P.g.,
Fusobacterium
nucleatum (F.n.)
Indocyanine Green in presence of Trolox™, a vitamin E analogue
808 nm GaAs diode laser
No remarkable antibacterial effect
In vitro
suspension
11Fekrazad et al., 2015
Candida albicans
(C.a.)
Methylene Blue (MB), Indocyanine Green (IG)
630 nm InGaAlP laser for MB;810 nm diode laser for IG
Reduced colony counts
In vitro
suspension
12Fekrazad et al., 2013
Streptococcus
mutans (S.m.)
Toluidine Blue, Indocyanine Green
620-640 nm (peak 630 nm) LED,662 nm diode laser,810 nm diode laser
No significant reduction of colonies
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1RESEARCH ABSTRACTS
48

Study Design Investigators Microbe(s) Photosensitizer(s)Light Source(s) for Photoactivation
Effect of Photosensitizer(s) Alone
In vitro biofilm-coated discs
13Müller et al., 2007
Biofilm: Actinomyces
naeslundii,
Veillonella dispar,
F.n., Streptococcus
sobrinus,
Streptococcus
oralis, C.a.
Methylene Blue 665 nm laser Reduced microbiota of the biofilm by less than 1 order of magnitude, not significantly different from PDT
In vitro
suspension
14George et al., 2008
Enterococcus
faecalis (E.f.)
Methylene Blue 664 nm diode laser Viability of bacteria was not significantly affected by MB in deionized water without irradiation. However, viability of E.f. cells was considerably lowered when cells were subjected to MB dissolved in a mixture of glycerol-ethanol-water without irradiation
In vitro
suspension
15Miyabe et al., 2011
Staphylococcus
sppMethylene Blue 660 nm GaAlAs
laserSmall reduction in bacterial counts
In vitro biofilm in acrylic discs
16Pereira et al., 2011
C.a., S.a., S.m. Methylene Blue 660 nm InGaAlP laser
No cytotoxic effect for the microorganisms tested
In vitro biofilm on acrylic resin
17De Freitas-Pontes et al., 2014
S.m., S.a.,
Escherichia coli
(E.c.), P.a., C.a.
Methylene Blue 630 nm LED Decreased S.m. scores;No effect on S.a.;No effect on E.c.;Decreased P.a. scores;Decreased C.a. CFU count
In vitro biofilms 18Vilela et al.,
2012S.a., E.c. Methylene Blue,
Toluidine Blue, Malachite Green
660 nm InGaAlP diode laser
No toxic effects on S.a. and E.c.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
49

Study Design Investigators Microbe(s) Photosensitizer(s)Light Source(s) for Photoactivation
Effect of Photosensitizer(s) Alone
In vitro suspension
19Rolim et al., 2012
S.m. Methylene Blue (MB),Toluidine Blue Ortho (TB),Malachite Green (MG);Eosin (EOS),Erythrosine (ERI),Rose Bengal (RB)
636 nm LED for MB, TB, MG;570 nm curing light for EOS, ERI, RB
For MB, TB, EOS, and MG, no significant effect on the viability of S.m.
For RB and ERI, complete bacterial kill and a decrease in cell viability, respectively, were observed, possibly due to high concentration of these photosensitizers
In vitro implant surfaces
20Haas et al., 1997
Actinobacillus
actinomycetem-
comitans (A.a.),
P.g., Prevotella
intermedia (P.i.)
Toluidine Blue 905 nm diode laser Bacterial lawns were present in all cultures
15 humans, implants, in
vivo
21Dörtbudak et
al., 2001P.g., P.i., A.a. Toluidine Blue 690 nm diode laser Lowered mean
values of bacterial counts
In vitro suspension
22Matevski et al., 2003
P.g., A.a.,
Bacteroides
forsythus, F.n., P.i.
Toluidine Blue Red-filtered xenon lamp,635 nm diode laser
No statistically significant decline in bacterial survival
In vitro suspensions
23Schlafer et al., 2010
E.c., C.a., E.f., F.n. Toluidine Blue 628 nm LED Mild reductions in the viable counts of all 5 organisms, none of which was statistically significant
In vitro suspensions
24Mattiello et al., 2011
Ag.a.,
Streptococcus
sanguinis (S.s.)
Toluidine Blue 660 nm AlGaInP diode laser
No statistically significant bacteria reduction
In vitro tooth specimens
25Poggio et al., 2011
E.f., S.m., S.s. Toluidine Blue 628 nm LED Showed the lowest bacterial reduction percentages for all tested strains
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1RESEARCH ABSTRACTS
50

Study Design Investigators Microbe(s) Photosensitizer(s)Light Source(s) for Photoactivation
Effect of Photosensitizer(s) Alone
33 patients with chronic periodontitis
26Theodoro et al., 2012
A.a., P.g., P.i.,
Tannerella
forsythia,
Prevotella
nigrescens (P.n.)
Toluidine Blue (TB) 660 nm GaAlAs laser
At 180 days there were greater reductions in positivity for P.i. and P.n. in the TB group than in the scaling and root planing (SRP) group. At all other time intervals and in all other species, TB showed fewer reductions than other groups
Biofilms: In vitro hydroxyapatite discs and in situ enamel slab specimens in 21 humans
27Teixeira et al., 2012
S.m. Toluidine Blue 620-660 nm (predominant 638.8 nm) red LED
No significant effect on the viability of S.m.
In vitro titanium discs and artificial periodontal pockets
28Eick et al., 2013 16 species including P.g.,
A.g.
Toluidine Blue 625-635 nm LED Reduced CFU counts
In vitro suspension
29Hakimiha et al., 2014
S.m. Toluidine Blue (TB),Radachlorin
®630 nm LED for TB662 nm laser for Radachlorin
No significant reductions of S.m. colonies were observed
In vitro suspension and in vivo on tibial bone defects in rats
30Dos Reis Junior et al., 2014
S.a. Toluidine Blue 660 nm diode laser Significant reduction of bacterial counts
In vitro suspension
31Paschoal et al., 2014
S.m. Toluidine Blue, Curcumin
400 to 799 nm noncoherent light source
Did not reduce the log10 CFU when compared with control groups
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
51

What might account for the variance in findings? Dörtbudak et al.21 suggested that a variable bonding behavior of the photosensitizer to different bacterial membranes may occur. The Rolim group19 mentioned differing partition coefficients among photosensitizers that affect their ability to permeate and accumulate in the hydrophobic region of the cellular membrane, thus influencing their bactericidal activities. They also stated that the photodynamic efficacy of each photosensitizer varies according to the characteristics of different target microorganisms.
Theodoro and colleagues26 identified a number of conditions that may affect biological response to photodynamic therapy: drug ion concentration (a consideration also discussed by the Rolim cohort19), period of retention of the drug within the tissue, time for biological response, pH of the environment, presence of exudates and gingival fluid, and mode of drug application (irrigation, slow release gel).
George et al.4 considered the uptake pathways of photosensitizers into bacteria. They suggested that the uptake of anionic photosensitizers (such as indocyanine green) by bacterial cells may be mediated through a combination of electrostatic charge interaction and by protein transporters, while the uptake of cationic photosensitizers (such as methylene blue) may be mediated by electrostatic interactions and by so-called self-promoted uptake pathways which involve the binding of cationic molecules to lipopolysaccharide that results in the progressive weakening of the cell’s outer membrane.
Of course, these and other factors come into play when the photosensitizer is actually “photoexcited” by a light source. Irradiation wavelength, duration of exposure, fluence, and absorption characteristics of the target area are among the additional considerations that must be optimized to achieve the most beneficial bactericidal effect.
To these factors must be added yet another consideration, applicable to those instances in which certain organisms display elevated resistance to photodynamic treatment. As Kossakowska et al.32 note below, the use of multicomponent sensitizing agents (such as the combination of protoporphyrin diarginate, toluidine blue, and 5-aminolevulinic acid) could eradicate virulent strains of the target species.
Continuing research is required to clearly define the mechanisms, means, and protocols required to achieve desired outcomes of photosensitizers and antimicrobial photodynamic therapy.
REFERENCES
1. Dorland’s illustrated medical dictionary. 31st edition. Philadelphia, Pa.: Saunders Elsevier, 2007.
2. FDA Drug Safety Communication: Serious CNS reactions possible when methylene blue is given to patients taking certain psychiatric medications. Facts about Methylene Blue. U.S. Department of Health & Human Services, U.S. Food and Drug Administration Web site. http://www.fda.gov/drugs/drugsafety/ucm263190.htm. Updated October 20, 2011. Accessed August 7, 2015.
3. The Photonics Dictionary. 48th edition. Pittsfield, Mass.: Laurin Publishing, 2002.
4. George S, Hamblin MR, Kishen A. Uptake pathways of anionic and cationic photosensitizers into bacteria. Photochem Photobiol Sci 2009;8(6):788-795.Jo
urna
l of L
aser
Den
tistr
y
| 2
015
Vol.
23, N
o. 1
RESEARCH ABSTRACTS
52

5. Wilson M, Gibson M, Strahan D, Harvey W. A preliminary evaluation of the use of a redox agent in the treatment of chronic periodontitis. J Periodontal Res 1992;27(5):522-527.
6. Gibson MT, Mangat D, Gagliano G, Wilson M, Fletcher J, Bulman J, Newman HN. Evaluation of the efficacy of a redox agent in the treatment of chronic periodontitis. J Clin Periodontol 1994;21(10):690-700.
7. Omar GS, Wilson M, Nair SP. Lethal photosensitization of wound-associated microbes using indocyanine green and near-infrared light. BMC Microbiol 2008 Jul 1;8:111. doi: 10.1186/1471-2180-8-111.
8. Nagahara A, Mitani A, Fukuda M, Yamamoto H, Tahara K, Morita I, Ting C-C, Watanabe T, Fujimura T, Osawa K, Sato S, Takahashi S, Iwamura Y, Kuroyanagi T, Kawashima Y, Noguchi T. Antimicrobial photodynamic therapy using a diode laser with a potential new photosensitizer, indocyanine green-loaded nanospheres, may be effective for the clearance of Porphyromonas gingivalis. J Periodontal Res 2013;48(5):591-599.
9. Topaloglu N, Gulsoy M, Yuksel S. Antimicrobial photodynamic therapy of resistant bacterial strains by indocyanine green and 809-nm diode laser. Photomed Laser Surg 2013;31(4):155-162.
10. Kranz S, Huebsch M, Guellmar A, Voelpel A, Tonndorf-Martini S, Sigusch BW. Antibacterial photodynamic treatment of periodontopathogenic bacteria with indocyanine green and near-infrared laser light enhanced by Trolox™. Lasers Surg Med 2015;47(4):350-360.
11. Fekrazad R, Ghasemi Barghi V, Poorsattar Bejeh Mir A, Shams-Ghahfarokhi M. In vitro photodynamic inactivation of Candida albicans by phenothiazine dye (new methylene blue) and Indocyanine green (EmunDo®). Photodiagnosis Photodyn Ther 2015 Mar;12(1):52-57.
12. Fekrazad R, Khoei F, Hakimiha N, Bahador A. Photoelimination of Streptococcus mutans with two methods of photodynamic and photothermal therapy. Photodiagnosis Photodyn Ther 2013;10(4):626-631.
13. Müller P, Guggenheim B, Schmidlin PR. Efficacy of gasiform ozone and photodynamic therapy on a multispecies oral biofilm in vitro. Eur J Oral Sci 2007;115(1):77-80.
14. George S, Kishen A. Influence of photosensitizer solvent on the mechanisms of photoactivated killing of Enterococcus faecalis. Photochem Photobiol 2008;84(3):734-740.
15. Miyabe M, Junqueira JC, Pereira da Costa ACB, Jorge AOC, Ribeiro MS, Feist IS. Effect of photodynamic therapy on clinical isolates of Staphylococcus spp. Braz Oral Res 2011;25(3):230-234.
16. Pereira CA, Romeiro RL, Costa ACBP, Machado AKS, Junqueira JC, Jorge AOC. Susceptibility of Candida albicans, Staphylococcus aureus, and Streptococcus mutans biofilms to photodynamic inactivation: An in vitro study. Lasers Med Sci 2011;26(3):341-348.
17. de Freitas-Pontes KM, Gomes CEde P, de Carvalho BMDF, Sabóia Rde SC, Garcia BA. Photosensitization of in vitro biofilms formed on denture base resin. J Prosthet Dent 2014;112(3):632-637.
18. Vilela SFG, Junqueira JC, Barbosa JO, Majewski M, Munin E, Jorge AOC. Photodynamic inactivation of Staphylococcus aureus and Escherichia coli biofilms by malachite green and phenothiazine dyes: An in vitro study. Arch Oral Biol 2012;57(6):704-710.
19. Rolim JPML, de-Melo MAS, Guedes SF, Albuquerque-Filho FB, de Souza JR, Nogueira NAP, Zanin ICJ, Rodrigues LKA. The antimicrobial activity of photodynamic therapy against Streptococcus mutans using different photosensitizers. J Photochem Photobiol B 2012;106:40-46.
20. Haas R, Dörtbudak O, Mensdorff-Pouilly N, Mailath G. Elimination of bacteria on different implant surfaces through photosensitization and soft laser. An in vitro study. Clin Oral Implants Res 1997;8(4):249-254.
21. Dörtbudak O, Haas R, Bernhart T, Mailath-Pokorny G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri-implantitis. Clin Oral Implants Res 2001;12(2):104-108.
22. Matevski D, Weersink R, Tenenbaum HC, Wilson B, Ellen RP, Lépine G. Lethal photosensitization of periodontal pathogens by a red-filtered Xenon lamp in vitro. J Periodontal Res 2003;38(4):428-435.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
53

23. Schlafer S, Vaeth M, Hørsted-Bindslev P, Frandsen EVG. Endodontic photoactivated disinfection using a conventional light source: an in vitro and ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109(4):634-641.
24. Mattiello FDL, Coelho AAK, Martins OP, Mattiello RDL, Ferrão Júnior JP. In vitro effect of photodynamic therapy on Aggregatibacter actinomycetemcomitans and Streptococcus sanguinis. Braz Dent J 2011;22(5):398-403.
25. Poggio C, Arciola CR, Dagna A, Florindi F, Chiesa M, Saino E, Imbriani M, Visai L. Photoactivated disinfection (PAD) in endodontics: An in vitro microbiological evaluation. Int J Artif Organs 2011;34(9):889-897.
26. Theodoro LH, Silva SP, Pires JR, Soares GHG, Pontes AEF, Zuza EP, Spolidório DMP, de Toledo BEC, Garcia VG. Clinical and microbiological effects of photodynamic therapy associated with nonsurgical periodontal treatment. A 6-month follow-up. Lasers Med Sci 2012;27(4):687-693.
27. Teixeira AH, Pereira ES, Rodrigues LKA, Saxena D, Duarte S, Zanin ICJ. Effect of photodynamic antimicrobial chemotherapy on in vitro and in situ biofilms. Caries Res 2012;46(6):549-554.
28. Eick S, Markauskaite G, Nietzsche S, Laugisch O, Salvi GE, Sculean A. Effect of photoactivated disinfection with a light-emitting diode on bacterial species and biofilms associated with periodontitis and peri-implantitis. Photodiagnosis Photodyn Ther 2013;10(2):156-167.
29. Hakimiha N, Khoei F, Bahador A, Fekrazad R. The susceptibility of Streptococcus mutans to antibacterial photodynamic therapy: A comparison of two different photosensitizers and light sources. J Appl Oral Sci 2014;22(2):80-84.
30. dos Reis Junior JA, de Carvalho FB, Trindade RF, de Assis PN, de Almeida PF, Pinheiro ALB. A new preclinical approach for treating chronic osteomyelitis induced by Staphylococcus aureus: In vitro and in vivo study on photodynamic antimicrobial therapy (PAmT). Lasers Med Sci 2014;29(2):789-795.
31. Paschoal MA, Santos-Pinto L, Lin M, Duarte S. Streptococcus mutans photoinactivation by combination of short exposure of a broad-spectrum visible light and low concentrations of photosensitizers. Photomed Laser Surg 2014;32(3):175-180.
32. Kossakowska M, Nakonieczna J, Kawiak A, Kurlenda J, Bielawski KP, Grinholc M. Discovering the mechanisms of strain-dependent response of Staphylococcus aureus to photoinactivation: Oxidative stress toleration, endogenous porphyrin level and strain’s virulence. Photodiagnosis Photodyn Ther 2013;10(4):348-355.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1RESEARCH ABSTRACTS
54

Antibacterial Photodynamic Treatment of Periodontopathogenic Bacteria with Indocyanine Green
and Near-Infrared Laser Light Enhanced by Trolox™Stefan Kranz,1 Marie Huebsch,2 Andre Guellmar,1 Andrea Voelpel,1
Silke Tonndorf-Martini,1 Bernd W. Sigusch1
1Polyclinic for Conservative Dentistry and Periodontology, University Hospital Jena, Jena, Germany
2Polyclinic for Prosthetic Dentistry and Material Science, University Hospital Jena, Jena, Germany
Lasers Surg Med 2015;47(4):350-360
Background and Objectives: It has been shown that certain vitamins can significantly enhance the effect of photodynamic anti-tumor therapy. Unfortunately, there is no sufficient information available about the impact of those antioxidants on antimicrobial Photodynamic Therapy (aPDT). The present study is aimed at investigating the antimicrobial effect of the dye indocyanine green (ICG) in the presence of Trolox™, a vitamin E analogue, upon irradiation with near-infrared (NIR) laser light (808 nm) on the gram-negative periodontopathogenic bacteria Aggregatibacter actinomycetemcomitans (A.a.), Porphyromonas gingivalis (P.g.) and Fusobacterium
nucleatum (F.n.).
Methods: Bacteria solved in PBS were incubated with ICG (50-500 mg/ml) in the presence and absence of Trolox™ (2 mM). Irradiation was performed after 10 minutes of dark-incubation with NIR-laser-light (25-100 J/cm2, 810 nm). During treatment, temperature was also recorded inside the bacterial solutions. The treated suspensions were serial diluted and plated onto blood agar plates. After anaerobe cultivation for 5 days the colony-forming units (CFU/ml) were determined.
Results: The antibacterial effect was ICG-concentration and exposure dependent. It was found that high ICG-concentrations and light fluence rates caused bacterial reduction due to hyperthermia. Where low ICG-concentrations (< 250 mg/ml) and fluence rates only induced minor regression, additional Trolox™-administration significantly enhanced the photodynamic effect. While treatment of A.a. (250 mg/ml ICG, 100 J/cm2) without Trolox™ caused no bacterial reduction, additional administration led to total eradication. In the presence of Trolox™ reduction to one-fifth of the original ICG-concentration (50 mg/ml) still induced total suppression of P.g. and F.n. at identical fluence (100 J/cm2). Treatment with ICG, NIR-light or Trolox™ alone showed no remarkable bactericidal effect. Application of high ICG-concentrations (500 mg/ml) and exposure values (100 J/cm2) caused peak temperatures of 64.53°C.
Conclusions: The results clearly show that Trolox™ significantly enhanced the antibacterial effect of ICG upon irradiation with NIR-laser-light. Additional administration of Trolox™ may also increase the efficiency of other aPDT systems.
© 2015 Wiley Periodicals, Inc. Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
55

In Vitro Photodynamic Inactivation of Candida albicans by Phenothiazine Dye (New Methylene
Blue) and Indocyanine Green (EmunDo®)Reza Fekrazada,1-2 Vadood Ghasemi Barghia,1 , 3
Arash Poorsattar Bejeh Mird,4 Masoumeh Shams-Ghahfarokhie 5
1Laser Research Center in Medical Sciences, AJA University of Medical Sciences, Tehran, Iran
2Department of Periodontics, Dental Faculty, AJA University of Medical Sciences, Tehran, Iran
3Department of Periodontics, Ardabil University of Medical Sciences, Ardabil, Iran
4Dental Materials Research Center, Dentistry School, Babol University of Medical Sciences, Babol, Iran
5Department of Mycology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
Photodiagnosis Photodyn Ther 2015;12(1):52-57
Background: The application of a new generation of photosensitizers to increase the efficacy of antifungal photodynamic therapy (aPDT) is an important aspect of PDT. Thus, this in vitro study is aimed to evaluate the antifungal efficacy of the photo-elimination of Candida albicans with photothermal and antifungal photodynamic therapy.
Method and Material: aPDT with new methylene blue and photothermal therapy with EmunDo® were applied to a fungal suspension, which was then subcultured in Sabouraud dextrose agar (SDA). The C. albicans colonies were counted and are expressed as colony-forming unit per milliliter (CFU/ml).
Results: aPDT with either EmunDo® or new methylene blue (NMB) considerably diminished the viability of inoculated C. albicans (P < 0.001) by log reduction of 1.9 and 3.37, respectively, compared with the control group. The antifungal potency or dark toxicity of the two photosensitizers alone did not significantly differ (P = 0.70). The same trend was observed for the light sources (λ: 810 nm vs. λ: 630 nm), which also did not significantly differ (P = 0.78).
Conclusion: The photo-elimination of C. albicans with either new methylene blue or EmunDo® as a photosensitizer can reduce the viability of fungal cells. Although the result of this study is encouraging, further investigations are warranted to determine clear protocols for the reliable and safe application of this method in clinical practice.
© 2015 Elsevier B.V. All rights reserved.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1RESEARCH ABSTRACTS
56
Streptococcus mutans Photoinactivation by Combination of Short Exposure of a Broad-Spectrum Visible
Light and Low Concentrations of Photosensitizers
Marco Aurelio Paschoal, DDS, PhD,1 Lourdes Santos-Pinto, DDS, PhD,1 Meng Lin, MSc,2 Simone Duarte, DDS, PhD2
1Department of Pediatric Dentistry, Araraquara Dental School, UNESP-Univ Estadual Paulista, Araraquara, SP, Brazil
2Department of Basic Science and Craniofacial Biology, College of Dentistry, New York University, New York, New York, USA
Photomed Laser Surg 2014;32(3):175-180
Objective: Investigate the photodynamic antimicrobial effect by the combination of a novel noncoherent broad spectrum visible light and low concentrations of curcumin and toluidine blue over suspensions of Streptococcus mutans.
Background Data: Long illumination times to activate photosensitizers (PS) and the use of high concentrations of these drugs in photodynamic antimicrobial chemotherapy (PACT) are limitations of its application as an antimicrobial technology in dental practice.
Materials and Methods: Planktonic suspensions of S. mutans were standardized and submitted to PACT treatment at low concentrations of curcumin (C) (0.075; 0.75 and 7.5 µM) and toluidine blue (T) (0.25; 2.5 and 25 µM) exposed to 42 J/cm2 (12.2 sec; set power: 3.930 mW) of a white light (WL) (output wavelength range: 400-700 nm; beam diameter: 12 mm) (C + WL + and T + WL +, PACT groups; incubation time, C: 60 sec; T: 5 min); isolated effect of both C (C + WL –) and T concentrations (T + WL –); effect of light source (C – WL + and T – WL + ) and suspensions neither submitted to PS nor to light-emitting diode (LED) illumination (control groups, C – WL – and T – WL –). Aliquots of each group were diluted and cultured on blood agar plates and the number of colony-forming units (CFU)/mL was recorded, transformed into log10 and analyzed by ANOVA and Tukey’s test at a cutoff value at 0.05.
Results: The groups submitted to PACT presented a bacterial reduction value of > 5-log10 to both tested PS in comparison with control groups (P < 0.05). PS or light source used alone demonstrated no antimicrobial effect on the number of viable bacterial counts.
Conclusions: The combination of a novel noncoherent light at short illumination exposure time with low concentrations of studied PS achieved a lethal photoinactivation of S. mutans, and can be considered an effective antimicrobial in vitro approach for reducing the number of microorganisms involved with the dental caries process.
© Mary Ann Liebert, Inc.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1
RESEARCH ABSTRACTS
57

Discovering the Mechanisms of Strain-Dependent Response of Staphylococcus aureus to Photoinactivation:
Oxidative Stress Toleration, Endogenous Porphyrin Level and Strain’s Virulence
Monika Kossakowska,1 Joanna Nakonieczna,1 Anna Kawiak,2-3 Julianna Kurlenda,4 Krzysztof P. Bielawski,1 Mariusz Grinholc, PhD1
1Laboratory of Molecular Diagnostics, Department of Biotechnology, Intercollegiate Faculty of Biotechnology, University of Gdansk and Medical University of Gdansk, Gdansk, Poland
2Department of Biotechnology, Division of Plant Protection and Biotechnology, Intercollegiate Faculty of Biotechnology, University of Gdansk and Medical University of Gdansk, Gdansk, Poland
3Laboratory of Human Physiology, Medical University of Gdansk, Gdansk, Poland
4Department of Clinical Bacteriology at the Provincial Hospital, Koszalin, Poland
Photodiagnosis Photodyn Ther 2013;10(4):348-355
Background: Staphylococcus aureus is generally known to be susceptible to photoinactivation. However, the phenomenon of its strain-dependent response to photodynamic treatment has been reported. Moreover, the factors determining the emerging variation among strains according to photoinactivation remain unclear.
Methods: This work aimed to investigate any relevant correlation between bacterial toleration of oxidative stress, porphyrin level, photosensitizer uptake and strain’s virulence of studied methicillin-susceptible and methicillin-resistant S. aureus strains and their response to photodynamic inactivation (using protoporphyrin diarginate, toluidine blue O and 5-aminolevulinic acid).
Results: Obtained data demonstrated that studied factors have limited impact on strain response to PDI. However, we have shown that a multicomponent sensitizing agent, i.e., consisting of PPArg2, ALA, and TBO, would eliminate the S. aureus elevated resistance to photoinactivation and that both highly virulent and low virulent S. aureus strains could be easily eradicated with the use of PDI. Moreover, we have shown that photodynamic inactivation could decrease the virulence of S. aureus extracellular fraction.
Conclusion: The mechanism underlying strain-dependent response to photoinactivation is complex and multifactorial, nevertheless with the use of several sensitizing agents the elevated resistance to photodynamic treatment can be omitted.
Copyright © 2013 Elsevier B.V. All rights reserved.
Jour
nal o
f Las
er D
entis
try
|
201
5 Vo
l. 23
, No.
1RESEARCH ABSTRACTS
58

91st ANNUL SESSION
The argest Dental Meeting/Congress/xposition in the nited tates
Greater ew York Dental Meeti ng™570 eventh Avenue - uite 800
ew York, Y 10018 ATel: (212) 398-6922 / Fax: (212) 398-6934
-mail: [email protected] Website: www.gnydm.com
2 0 1 5
Exhibit DatesNovember 29 - December 2
Jacob K. Javits Conventi on Center, ew York City
WWW.GYDM.CM
Meeting DatesNovember 27 - December 2
* RG TRAT F*
6 Hours of Free C very Day
ver 700 xhibitors
GYDM ffers More Than 350 cientific Programs
ncluding 2nd Annual World mplant xpo
1st Global rthodonti c ConferenceDental aboratory Meeti ng
nternati onal ral Cancer ymposium
Sponsored by the Second District and New York County Dental Societi es

ATS™
See more atfotona.com
Expand your practice with Lightwalker™ (888) 550-4113
WPT™ Laser Perio Advanced Dual Wavelength
PHAST PIPS™ Laser Endo Effective & Exclusive
Nightlase™ Procedure Laser Snoring Reduction
Ultra Fast, No Shot Cavity Preps
Precise Fast Osseous Cutting/Shaping Procedures
Bloodless, Suture Free Soft Tissue Procedures
New Digital Scanner, Faster and More Precise
1508
12-0
1
The prestigious “red dot”
Design Award
Awarded Best of ClassBy the Pride Institute at the
American Dental Association
Dentistry Today’sTop 100 Products
Nd:YAG & Erbium Laser: The Endo, Perio, Hard & Soft Tissue Laser