the painful shoulder
TRANSCRIPT
OrthOpaedic ii: SOft tiSSue, MetabOliSM, Malignancy
The painful shoulderandrew frost
c Michael robinson
AbstractShoulder pain is usually caused by a small number of relatively common
conditions. clinical history and examination are essential in the dia
gnosis of shoulder pain, after which investigations often assist in con
firming the diagnosis.
One of the commonest causes of shoulder pain is rotator cuff dis
ease, which can be due to impingement syndrome (where the acromion
impinges on the supraspinatus tendon) or by tears to the rotator cuff
muscles. both conditions can be managed with physiotherapy, but sur
gery (subacromial decompression, arthroscopic cuff repair) may be indi
cated. frozen shoulder is a chronic condition often affecting middleaged
women. it can follow a period of immobility or minor trauma and is usu
ally managed with physiotherapy. calcific tendonitis is caused by calcium
deposition in the supraspinatus tendon and causes severe pain; calcium
deposits on plain radiographs are diagnostic. Symptoms gradually settle
over time in most cases, but surgical intervention may be indicated.
degenerative disease (e.g. osteoarthritis, rheumatoid arthritis) can also
cause shoulder pain and shoulder arthroplasty may be indicated. Shoul
der dislocations can lead to an unstable shoulder joint that is prone to
recurrent dislocation. Surgery may be required to stabilize the shoulder
and repair damage to the labrum or humeral head.
Other, less common, causes of shoulder pain (e.g. infection, neuralgic
amyotrophy, tumour) are also briefly considered in this review.
Keywords painful shoulder; rotator cuff disease; impingement syndrome;
frozen shoulder; calcific tendonitis; shoulder instability
The commonest shoulder disorders (Table 1) are relatively easy to diagnose with careful history-taking, structured clinical exam-ination and plain radiographs. The increasing availability of spe-cialist imaging and arthroscopy have enabled a more accurate assessment of shoulder disorders than was previously possible.
Clinical assessment of the painful shoulder
Symptoms of pain, stiffness, and loss of function must be elucidated. Most pain arising from the shoulder is poorly localized over the upper arm; pain from the acromioclavicular joint tends to be local-ized over the joint. Stiffness and loss of function may be continuous
Andrew Frost MRCS is a Senior House Officer in Orthopaedic Surgery at
New Royal Infirmary of Edinburgh, Edinburgh, UK.
C Michael Robinson FRCS(Orth) (Ed) is a Consultant Orthopaedic and
Trauma Surgeon at New Royal Infirmary of Edinburgh, Edinburgh, UK.
Surgery 24:11 36
or only when carrying out specific activities (e.g. reaching over-head, lying on the shoulder). Shoulder instability may present as frank episodes of shoulder dislocation or partial subluxation.
Clinical examination should look for: • skin changes • deformity • muscle wasting • scapular winging.The three bones and three joints of the shoulder girdle should be palpated to detect localized areas of tenderness. Referred pain from the neck or the chest may cause shoulder discomfort, and these areas should also be examined routinely.
The shoulder has three planes of movement which should be assessed: • abduction/adduction • flexion/extension • medial/lateral rotation.
Most shoulder movements represent a combination of gleno-humeral movement and scapulothoracic movement (gliding of the scapula on the chest wall). Examination from behind, with a hand placed over the blade of the scapula, helps to distinguish where a particular shoulder movement is occurring.
Imaging
Radiography – the standard plain radiographic views are the: • anterioposterior • axillary • scapula Y (outlet).Weightbearing anteroposterior views may help to diagnose sub-tle subluxation of the acromioclavicular joint.
Ultrasound can be used to view rotator cuff tears but is highly operator dependent.
CT provides superior imaging of bony abnormalities.MRI provides very good imaging of soft tissue. MRI should be
enhanced by contrast injection into the joint to assess the integrity of the capsule and labrum if shoulder instability is suspected.
Examination under anaesthesia and arthroscopy have increasing roles in diagnosis.
Painful disorders of the shoulder
Rotator cuff diseaseImpingement syndromes are due to continuous abrasion of the rotator cuff muscles on the undersurface of the coraco-acromial arch. The anterolateral portion of supraspinatus is most vulnerable to this wear due to its position and poor supply of blood. Excessive downwards ‘hooking’ of the anterior acromion is usually present, although conditions that narrow the distance between the humeral head and the acromion predispose to impingement syndromes. Impingement is usually reversible, but may lead to rotator cuff tear or even degenerative change in the glenohumeral joint (‘rotator cuff arthropathy’) if untreated.
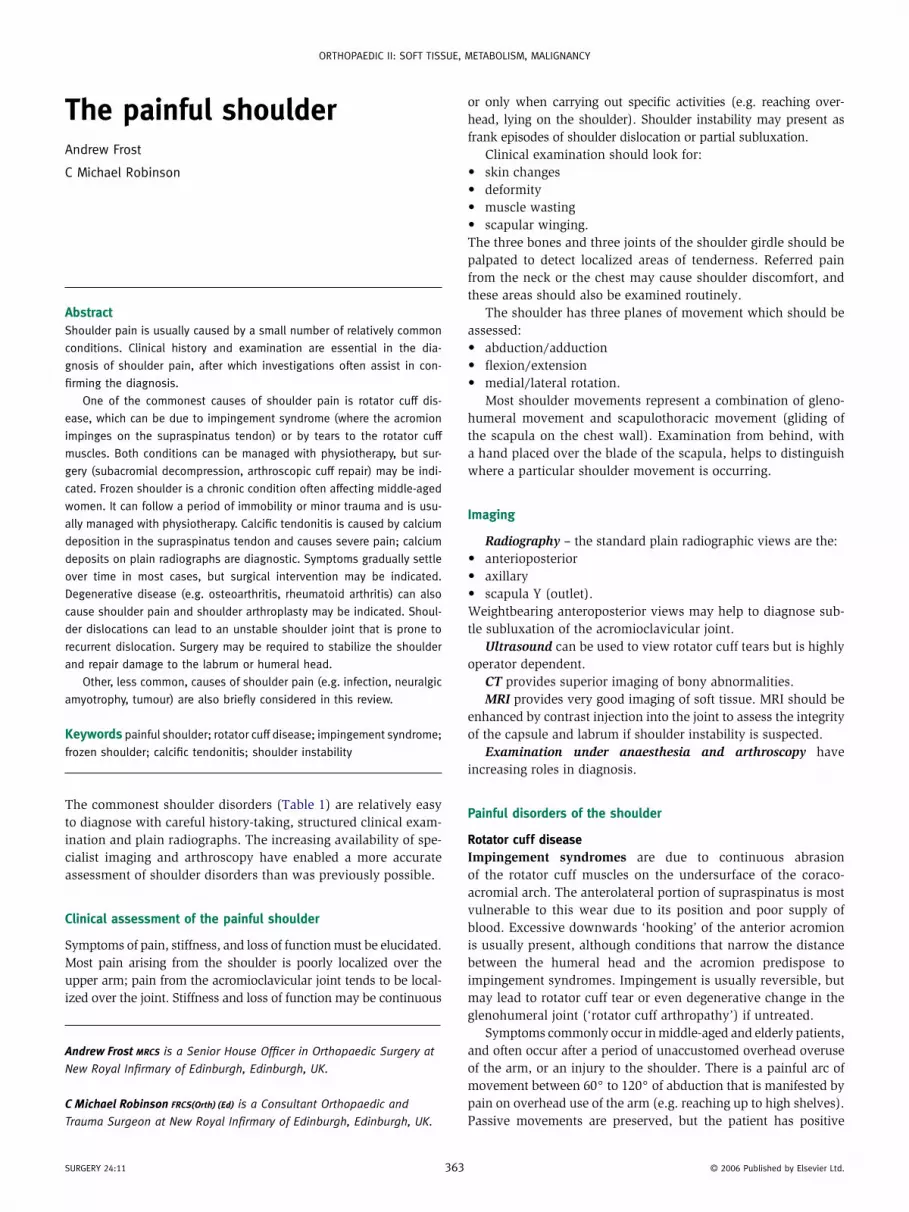
Symptoms commonly occur in middle-aged and elderly patients, and often occur after a period of unaccustomed overhead overuse of the arm, or an injury to the shoulder. There is a painful arc of movement between 60° to 120° of abduction that is manifested by pain on overhead use of the arm (e.g. reaching up to high shelves). Passive movements are preserved, but the patient has positive
3 © 2006 published by elsevier ltd.
OrthOpaedic ii: SOft tiSSue, MetabOliSM, Malignancy
Clinical presentations of the commonest shoulder conditions
Condition Patients usually affected Key diagnostic features Treatment
rotator cuff impingement Middleaged painful arc. full range of passive
movement. relief of impingement by
subacromial injection.
Subacromial corticosteroid
injection. Subacromial
decompression for recurrent
symptoms.
rotator cuff tear Middleaged and elderly Selective weakness of supraspinatus/
infraspinatus. positive ultrasound/Mri.
individualized treatment.
frozen shoulder Middleaged restriction of passive shoulder
movement (particularly loss of external
rotation).
physiotherapy. distension
arthrogram/manipulation if
refractory.
calcific tendonitis Middleaged Severe pain. full range of passive
movement. calcific deposit on
radiograph.
Subacromial steroid injection.
Subacromial decompression and
deposit removal for recurrent
symptoms.
acromioclavicular osteoarthosis Middleaged and elderly pain over joint. radiographic changes. analgesia. excision of joint for
refractory symptoms.
glenohumeral osteoarthosis Middleaged and elderly loss of passive shoulder movement.
radiographic changes.
analgesia. arthroplasty for
refractory symptoms.
Shoulder instability age < 40 years recurrent dislocation or subluxation
symptoms. clinical signs of instability.
Stabilization for traumatic
instability. physiotherapy for
atraumatic instability. nonsurgical
treatment for voluntary instability.
Table 1
tests for impingement (Figure 1). Plain radiographs may be normal or may show sclerosis of subacromial bone.
Relief of symptoms by subacromial injection of corticosteroid and local anaesthetic is diagnostic and therapeutic. Impingement symptoms may resolve completely in the early stages although, more often, the relief is temporary (4–6 weeks). Activity modi-fication, NSAIDs (p.o.) and physiotherapy are useful adjuvant treatments. Open or arthroscopic subacromial decompression should be done if recurrence occurs despite two injections of corticosteroid. This consists of excision of the subacromial bursa (bursectomy) and removal of the anterior acromial spur (acromioplasty). Other causes of dynamic impingement (e.g. osteoarthrosis of the acromioclavicular joint, malunited greater tuberosity fractures) should also be treated surgically.
Rotator cuff tears: cuff tears are commonest in the middle-aged and elderly (‘grey hair equals cuff tear’). They may result from chronic impingement or acutely after a shoulder injury. Patients aged >50 years who sustain a glenohumeral dislocation are par-ticularly at risk. Presentation is with pain and weakness when attempting to reach to the side or overhead. The main rotator cuff muscles can be selectively screened for weakness. • Supraspinatus—assess the strength of initiation of abduction with the arm at the side. • Infraspinatus—assess the strength of resisted external rotation with the elbow at the side and flexed at 90°. • Subscapularis—assess the strength of resisted internal rota-tion with the elbow at the side and flexed at 90°.The supraspinatus and infraspinatus are usually involved, and inability to initiate abduction with selective weakness on resisted
Surgery 24:11 36
external rotation is usually pathognomonic. Plain radiographs may show superior migration of the humeral head and degen-erative joint disease of the shoulder or acromioclavicular joint. Ultrasound or MRI should be obtained to: • confirm the clinical diagnosis • assess the tear size • assess the extent of its retraction.
The treatment of a cuff tear should be individualized depen-dent upon: • its size • its chronicity • the patient’s physiological status.
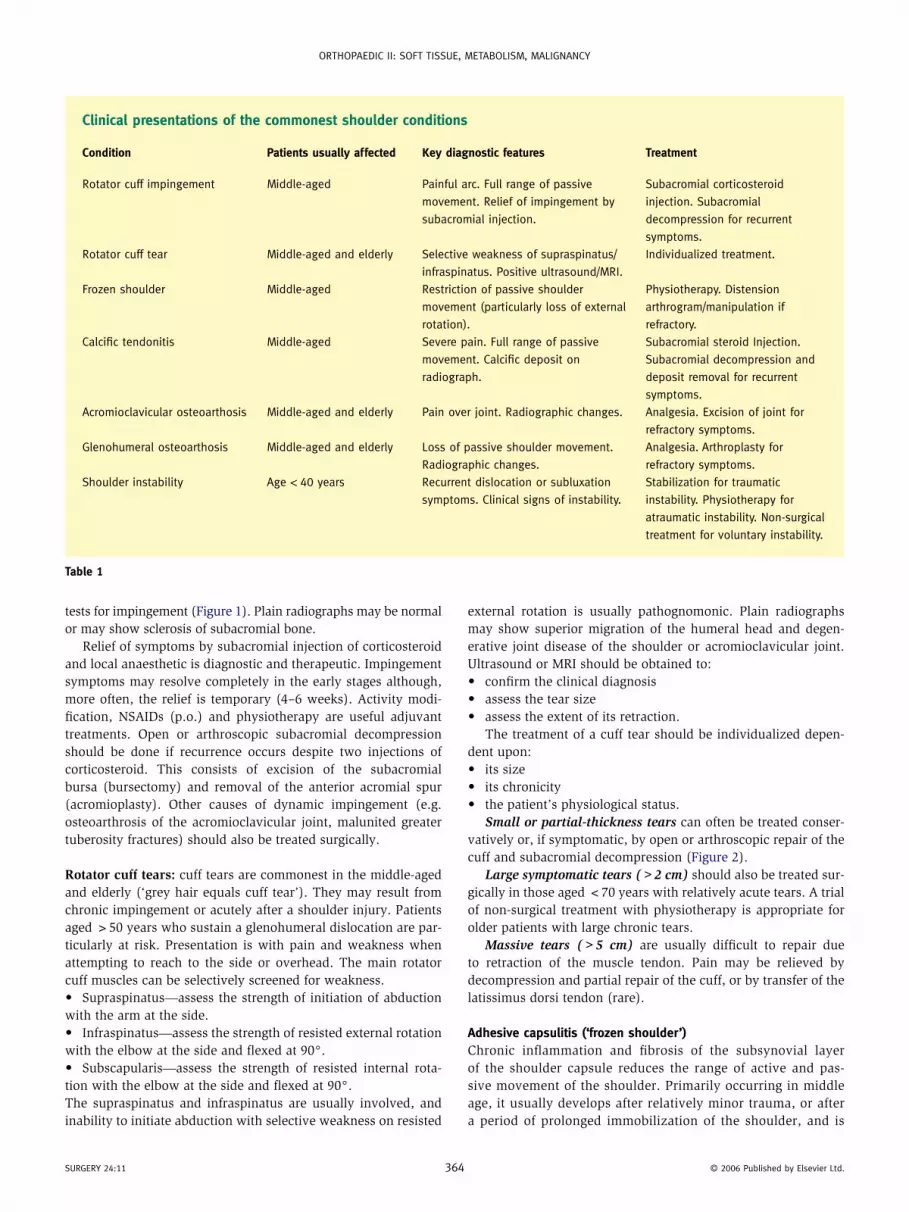
Small or partial-thickness tears can often be treated conser-vatively or, if symptomatic, by open or arthroscopic repair of the cuff and subacromial decompression (Figure 2).
Large symptomatic tears (>2 cm) should also be treated sur-gically in those aged <70 years with relatively acute tears. A trial of non-surgical treatment with physiotherapy is appropriate for older patients with large chronic tears.
Massive tears (>5 cm) are usually difficult to repair due to retraction of the muscle tendon. Pain may be relieved by decompression and partial repair of the cuff, or by transfer of the latissimus dorsi tendon (rare).
Adhesive capsulitis (‘frozen shoulder’)Chronic inflammation and fibrosis of the subsynovial layer of the shoulder capsule reduces the range of active and pas-sive movement of the shoulder. Primarily occurring in middle age, it usually develops after relatively minor trauma, or after a period of prolonged immobilization of the shoulder, and is
4 © 2006 published by elsevier ltd.
OrthOpaedic ii: SOft tiSSue, MetabOliSM, Malignancy
more common in women and patients with heart disease or diabetes.
Severe debilitating pain that disrupts sleep and marked limita-tion of shoulder movement is typical. Selective loss of passive external rotation movement is diagnostic. The clinical course characteristically passes through an initial painful stage, followed
Figure 1 Symptoms of rotator cuff impingement are reproduced by
internally rotating the shoulder while it is abducted or flexed at 90°.
Figure 2 arthroscopic view of a rotator cuff tear (retracted edge of tear
indicated by arrows). Source: david potter, northern general hospital,
Sheffield, uK.
Surgery 24:11 36
by a stiff, and then a resolving ‘thawing’ phase. Recovery of function may take more than two years, particularly in diabetic patients, who often have a more protracted clinical course.
Treatment is initially aimed at pain control using NSAIDs, and maintenance of the range of movement by physiotherapy. Disten-sion arthrography (injecting fluid to stretch the joint capsule) or early manipulation under anaesthesia is often used to produce an earlier improvement in the range of motion. Rarely, arthroscopic surgical release may be indicated in refractory forms of adhesive capsuilitis. After these invasive treatments, physiotherapy should be started immediately to retain the extra movement achieved.
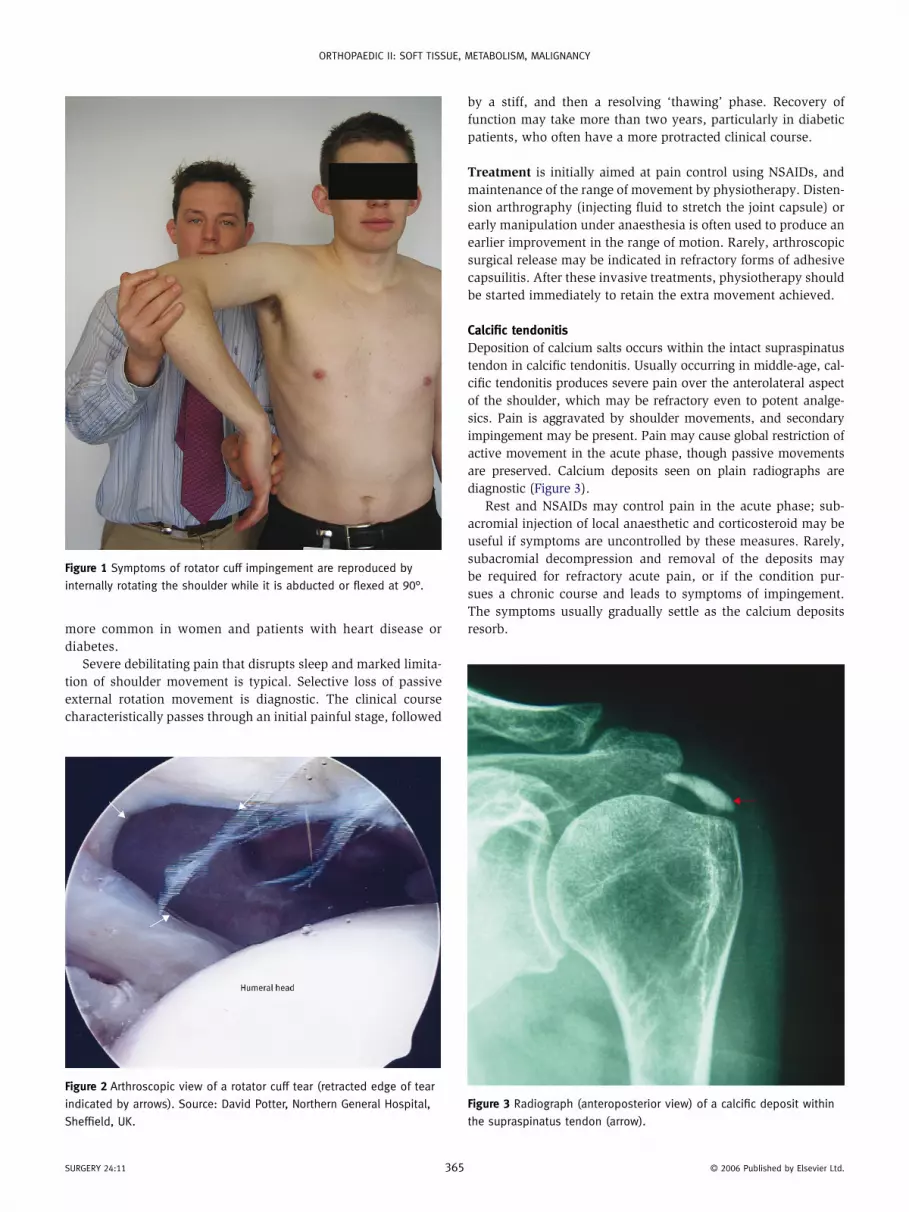
Calcific tendonitisDeposition of calcium salts occurs within the intact supraspinatus tendon in calcific tendonitis. Usually occurring in middle-age, cal-cific tendonitis produces severe pain over the anterolateral aspect of the shoulder, which may be refractory even to potent analge-sics. Pain is aggravated by shoulder movements, and secondary impingement may be present. Pain may cause global restriction of active movement in the acute phase, though passive movements are preserved. Calcium deposits seen on plain radiographs are diagnostic (Figure 3).
Rest and NSAIDs may control pain in the acute phase; sub-acromial injection of local anaesthetic and corticosteroid may be useful if symptoms are uncontrolled by these measures. Rarely, subacromial decompression and removal of the deposits may be required for refractory acute pain, or if the condition pur-sues a chronic course and leads to symptoms of impingement. The symptoms usually gradually settle as the calcium deposits resorb.
Figure 3 radiograph (anteroposterior view) of a calcific deposit within
the supraspinatus tendon (arrow).
5 © 2006 published by elsevier ltd.
OrthOpaedic ii: SOft tiSSue, MetabOliSM, Malignancy
Degenerative disease of the jointGlenohumeral joint: osteoarthrosis in older patients is often sec-ondary to overuse injury, untreated rotator cuff tears and proxi-mal humeral fractures. Massive collapse of the humeral head in younger patients is often attributable to avascular necrosis of the humeral head, and may be secondary to: • alcohol abuse • sickle cell disease • corticosteroid • proximal humeral fracture.The joint is also commonly affected by rheumatoid arthritis. Symp-toms of pain, stiffness and loss of function are common, and night pain may be particularly troublesome. The characteristic features of osteoarthrosis on plain radiographs confirm the diagnosis.
Treatment is initially NSAIDs (p.o.) and physiotherapy to retain shoulder movement; non-responders can undergo humeral head arthroplasty (using a traditional cemented or uncemented stem) or surface replacement. Total joint replacement is done only if there is severe involvement of the glenoid with osteoarthrosis or rheumatoid arthritis.
Acromioclavicular joint: osteoarthrosis is common in middle-aged men, often as a sequel to an injury to the joint, and leads to pain, which is often well localized over the joint. Impingement of the underlying rotator cuff can occur from the resultant osteo-phytes. The patient complains of pain on flexing and adducting the arm (‘scarf sign’). Plain radiographs may show the gross fea-tures of osteoarthrosis, although MRI may be required to detect earlier forms of the disease.
Treatment – relief by injection of local anaesthetic and corti-costeroid is diagnostic and therapeutic. If symptoms recur, open or arthroscopic excision of the joint should be done, combined with a subacromial decompression if concomitant impingement symptoms are present.
Dislocation or instabilityAcute anterior dislocation occurs typically in two groups of patients: • the elderly (who often sustain concomitant rotator cuff tears) • young adults (who often develop recurrent shoulder
instability).Clinical assessment should ensure the neurovascular integrity
of the arm (particularly assessing the axillary nerve by testing deltoid function and sensation in the ‘badge’ area of the shoul-der) before closed relocation under sedation using the Hippo-cratic or Milch technique.
Acute posterior dislocation is less common but must be suspected if there is shoulder pain after a period of altered consciousness (particularly epileptics and diabetics, alcoholics and drug abusers who suffer hypoglycaemic or withdrawal fits). A modified axial view or CT must always be obtained because the radiological features of posterior dislocation are subtle on the anteroposterior view. Confirmed posterior dislocations should be referred for specialist orthopaedic advice because relocation may be difficult and assessment of the stability of the reduction is required.
Recurrent instability: three major categories of patients develop recurrent shoulder instability.
Surgery 24:11 36
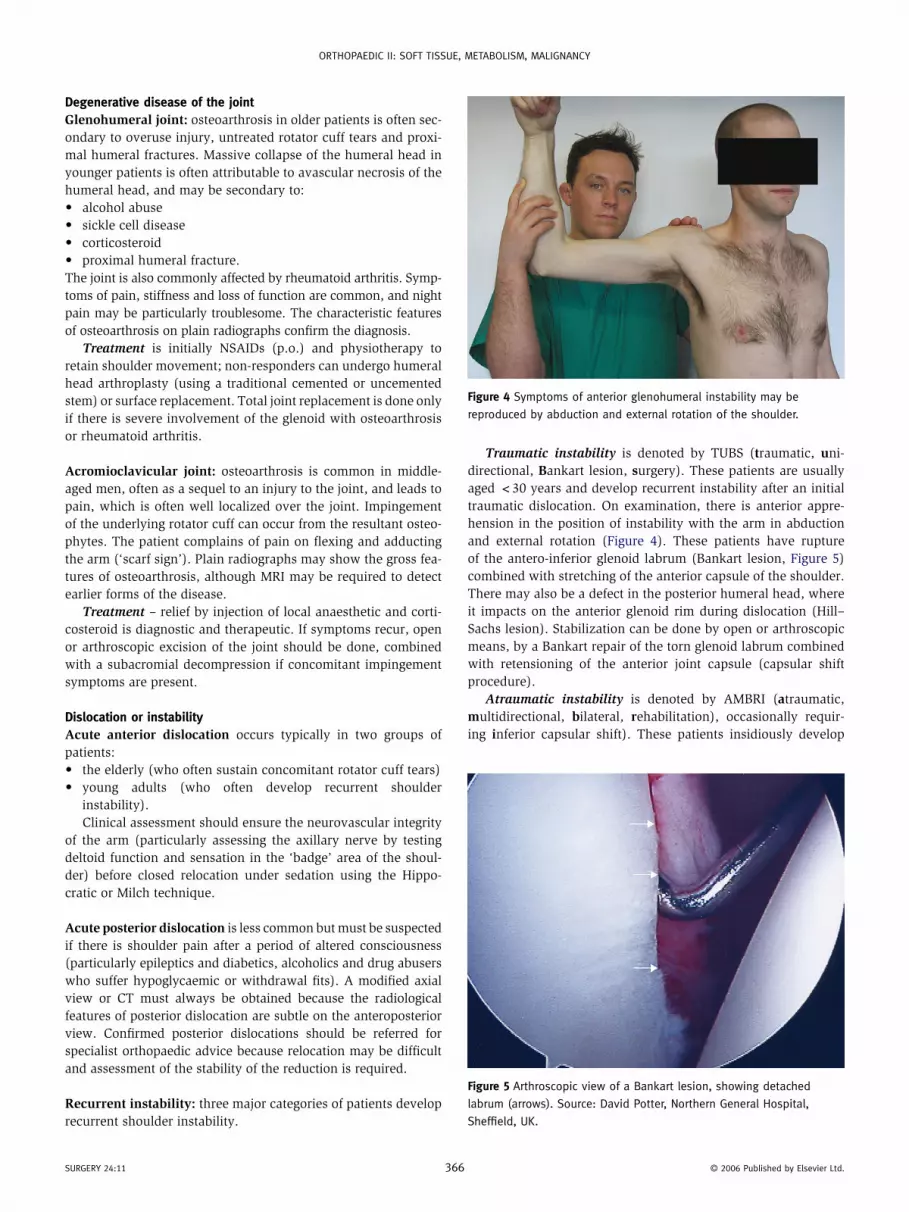
Traumatic instability is denoted by TUBS (traumatic, uni-directional, Bankart lesion, surgery). These patients are usually aged <30 years and develop recurrent instability after an initial traumatic dislocation. On examination, there is anterior appre-hension in the position of instability with the arm in abduction and external rotation (Figure 4). These patients have rupture of the antero-inferior glenoid labrum (Bankart lesion, Figure 5) combined with stretching of the anterior capsule of the shoulder. There may also be a defect in the posterior humeral head, where it impacts on the anterior glenoid rim during dislocation (Hill–Sachs lesion). Stabilization can be done by open or arthroscopic means, by a Bankart repair of the torn glenoid labrum combined with retensioning of the anterior joint capsule (capsular shift procedure).
Atraumatic instability is denoted by AMBRI (atraumatic, multidirectional, bilateral, rehabilitation), occasionally requir-ing inferior capsular shift). These patients insidiously develop
Figure 4 Symptoms of anterior glenohumeral instability may be
reproduced by abduction and external rotation of the shoulder.
Figure 5 arthroscopic view of a bankart lesion, showing detached
labrum (arrows). Source: david potter, northern general hospital,
Sheffield, uK.
6 © 2006 published by elsevier ltd.

OrthOpaedic ii: SOft tiSSue, MetabOliSM, Malignancy
shoulder instability without injuring their shoulder. Features of generalized ligamentous laxity are usually present, and other stigmata of Marfan’s syndrome or Ehlers–Danlos syndrome may be present. There is no structural damage of the shoulder and the instability is due to increased shoulder volume from capsu-lar hyperlaxity. Stability can usually be restored by rotator cuff strengthening exercises, although rarely surgical stabilization may be required to retension the capsule by the inferior capsular shift procedure.
Voluntary instability – these patients voluntarily dislocate their shoulder for secondary gain. Often there is a history of pre-vious psychological disturbance and the patient may be able to show painless instability on prompting. Treatment is conserva-tive, including psychological counselling.
Labral tearsThe glenoid labrum is prone to tear at the insertion of the long head of biceps tendon in ‘overhead athletes’ (e.g. tennis players, basketball players). The resulting superior labral tear from ante-rior to posterior tear (SLAP lesion) often causes pain on perform-ing overhead activities. Patients who are symptomatic despite conservative measures can usually be treated by an arthroscopic repair of the lesion.
Rupture of the biceps tendonAcute rupture of the long head of the biceps tendon may occur in older patients. This causes a characteristic visible lump over the mid biceps (‘Popeye sign’, Figure 6). The rupture is usually man-aged conservatively in elderly patients, although early surgical repair should be considered in younger athletes.
Figure 6 rupture of the long head of biceps (‘popeye sign’). Source:
david potter, northern general hospital, Sheffield, uK.
Surgery 24:11 3
InfectionSeptic arthritis can occur at the shoulder as a result of infec-tion with pyogenic organisms (see Bennet, CROSS REFERENCE). Elderly, diabetic or immunosuppressed patients are particularly at risk, and the shoulder is usually hot and exquisitely painful to movement. Systemic signs of infection may be absent if the patient is immunosupressed. Urgent sterile aspiration of the joint (usually under ultrasound guidance) is indicated. Antibiotics should be started as soon as the aspirate has been taken, and urgent surgical joint washout is necessary if infection is con-firmed from the joint aspirate.
Neuralgic amyotrophy (Parsonage–Turner syndrome)Neuralgic amyotrophy is an uncommon peripheral neuro-pathy that typically affects young males after a viral illness. It is characterized by an insidious onset of pain and weakness in the shoulder girdle, usually associated with winging of the scapula. Recovery occurs spontaneously and usually starts within six weeks of the onset of symptoms. Full recovery may take several months.
TumoursPrimary tumours of bone (see page 392) cause constant, deep-seated pain, unrelated to use of the arm, which may be worse at night. If malignant, they are usually associated with systemic symptoms such as weight loss and night sweats. Radiological features of bone destruction, new bone formation and perios-teal elevation are typical, and further specialist imaging and biopsy are required to stage the lesion before definitive treat-ment in a specialist centre. Secondary metastases may also occur in the shoulder girdle, and the proximal humerus is a relatively common site. ◆
CRoss ReFeReNCe
bennet gc, bennet SJ. infection of bone and joint. Surgery 2006; 24(6):
211–4.
FuRTheR ReADINg
apley ga, Warwick d, nayagam S, Solomon l, eds. apley’s system of
orthopaedics and fractures, 8th edn. london: arnold, 2001.
copeland S. Operative shoulder surgery (orthopedic surgical skills).
london: churchill livingstone, 1995.
iannotti Jp, Williams gr, eds. disorders of the shoulder: diagnosis and
management. philadelphia: lippincott, Williams and Wilkins, 1999.
rockwood ca, Matsen fa, Wirth Ma, harryman dJ, Matsen lr.
the shoulder, 2nd edn. philadelphia: Wb Saunders, 1998.
67 © 2006 published by elsevier ltd.