the prick will do the trick: protecting our healthcare workers from vaccine-preventable infections
TRANSCRIPT

Healthcare Workers Immunization Update
Rontgene M. Solante, MD., FPCP, FPSMID Phillipine Hospital Infection Control Society Annual Convention Crowne Plaza Hotel May 27, 2016

Rontgene M. Solante, MD
• Phil Society for Microbiology and Infectious Diseases (PSMID), Past President
• Global Steering Committee Member , MEDSCAPE for Pneumococcal Disease Prevention and Education thru vaccination
• Asian Advisory Board , Community Acquired Pneumonia Immunization Trial Adults (CAPiTA) 2015
• Chairman, Fellowship Program Adult Infectious Disease and Tropical Medicine- San Lazaro Hospital
• Medical Specialist III , National Reference Laboratory for HIV/AIDS San Lazaro Hospital
• Infection Control Chair: ManilaMed MCM, San Lazaro Hospital
• Assistant Professor , UERMMMC
• Fellow, Philippine College of Physicians and PSMID
Disclosure
• Pfizer vaccines , Asian and local advisory board member
• MSD vaccines Phil advisory board member
• Sanofi Pasteur Phil advisory board

Objectives
• Discuss the following:
• Why vaccinate healthcare workers?
• What are the currently recommended vaccines?

Definition: Healthcare personnel

Definition: Healthcare personnel
• all paid and unpaid persons working in health-care settings who have the potential for exposure to patients and/or to infectious materials, including body substances, contaminated medical supplies and equipment, contaminated environmental surfaces, or contaminated air.
• include (but are not limited to) the following
– physicians, nurses, nursing assistants, therapists, technicians, emergency medical service personnel, dental personnel, pharmacists, laboratory personnel, autopsy personnel, students and trainees, contractual staff
– clerical, dietary, housekeeping, laundry, security, maintenance, administrative, billing, and volunteers
“risk for exposure to (and possible transmission of) vaccine-preventable diseases”
1.US Department of Health and Human Services. Definition of health- care personnel (HCP). Available at http://www.hhs.gov/ash/programs/ initiatives/vacctoolkit/definition.html. Accessed October 5, 2011

2012 Recommended Immunization for Filipino Healthcare Workers PSMID-PHICS-PFV
Definition: Healthcare worker

Vaccines important for the HCW?
PUBLIC PRIVATE
Informal survey conducted during the HcW annual conventions (AMHOP, PHICS)

Why vaccinate healthcare personnel?
1. Protection against vaccine preventable diseases/infections including its complications
– protection for healthy HCP
– protection of at-risk HCPs (e.g. diabetes, immunocompromised, chronic conditions)
2. Prevent transmission of VPDs to patients and other HCPs
3. Minimize absenteeism and work flow disruption
4. Added cost for contact investigation, source of infection, diagnostics, and antibiotic treatment and prophylaxis

5 key recommended interventions preventing occupational acquisition of infection by HCP
(1) adherence to standard precautions
(2) rapid institution of appropriate isolation precautions
(3) proper use of personal protective equipment
(4) evaluation of personnel with exposure to communicable diseases for receipt of PEP
(5) appropriate immunizations
Vaccines 6th ed. 2013 Chap 66 pp 1290-1308

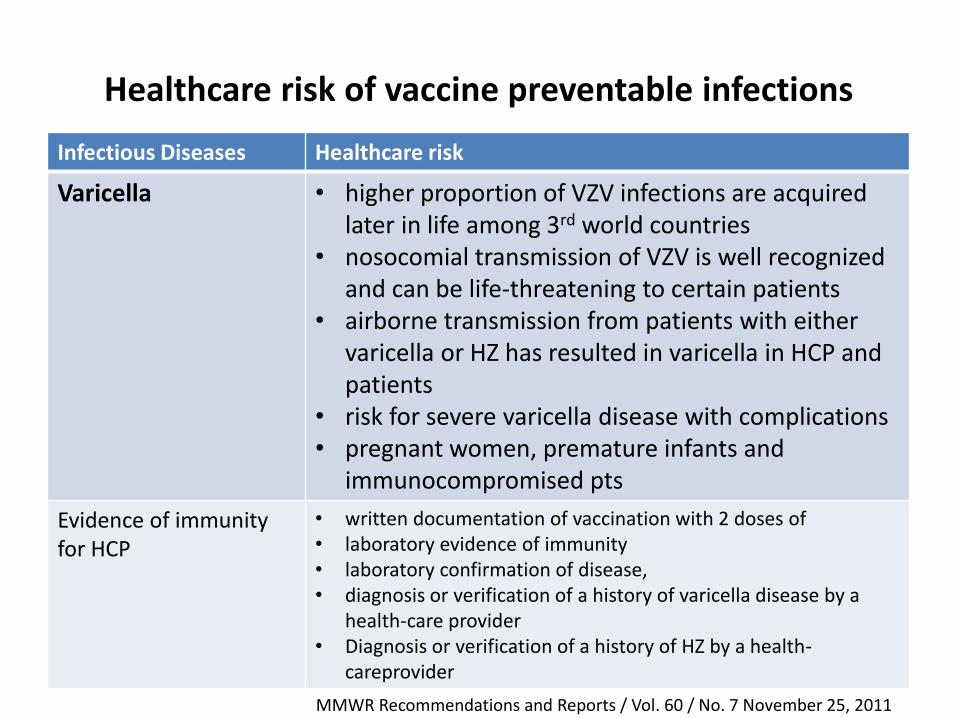
Healthcare risk of vaccine preventable infections
Infectious Diseases Healthcare risk
Hepatitis B • dependent on the frequency of percutaneous and mucosal exposures to blood or body fluids
• transmission from a needlestick exposure is up to 100 times more likely for exposure to HBeAg positive blood than to HIV-positive blood
• HBV can lead to chronic infection, which can result in cirrhosis of the liver, liver failure, liver cancer, and death
Influenza
• risk of occupationally acquired influenza • transmitting influenza to patients and other HCP • increased risk for severe outcomes from influenza • outbreaks in hospitals and long-term– care
facilities have been associated with low vaccination rates among HCP

SAGE recommendations for
influenza vaccination (2012)
• 5 recommended priority groups for countries using or considering introduction of seasonal influenza vaccination.
• Pregnant women highest priority group.
• Health-care workers
• Children under 5 (particularly 6-23 months)
• Elderly
• Underlying health conditions

Healthcare risk of vaccine preventable infections
Infectious Diseases Healthcare risk
Measles • highly contagious transmitted by respiratory droplets and airborne spread
• severe complications, which might result in death, include pneumonia and encephalitis
• WHO estimated 20 million measles cases occurring worldwide and approximately 164,000 related deaths
• Medical settings played a prominent role in perpetuating outbreaks of measles transmission
(1989-1991 outbreaks ; 2008 outbreaks)
Presumptive evidence of immunity to measles : •written documentation of vaccination with 2 doses of live measles or MMR •laboratory evidence of immunity •laboratory confirmation of disease, or •birth before 1957
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011

Healthcare risk of vaccine preventable infections
Infectious Diseases Healthcare risk
Mumps • health-care–associated transmission of mumps is infrequent, it might be underreported
• added economic costs because of furlough or reassignment of staff members from patient-care duties or closure of wards
Pertussis • transmission has occurred from hospital visitors to patients, from HCP to patients, and from patients to HCP
• documented outbreaks were costly and disruptive -diagnostic testing, prophylactic antibiotics, and exclusion from work
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011
Healthcare risk of vaccine preventable infections
Infectious Diseases Healthcare risk
Varicella • higher proportion of VZV infections are acquired later in life among 3rd world countries
• nosocomial transmission of VZV is well recognized and can be life-threatening to certain patients
• airborne transmission from patients with either varicella or HZ has resulted in varicella in HCP and patients
• risk for severe varicella disease with complications • pregnant women, premature infants and
immunocompromised pts
Evidence of immunity for HCP
• written documentation of vaccination with 2 doses of • laboratory evidence of immunity • laboratory confirmation of disease, • diagnosis or verification of a history of varicella disease by a
health-care provider • Diagnosis or verification of a history of HZ by a health-
careprovider
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011

Healthcare risk of vaccine preventable infections
Infectious Diseases Healthcare risk
Meningococcal Disease • Nosocomial transmission of Neisseria meningitidis is rare
• HCP increased risk after direct contact with respiratory secretions of infected persons (e.g., managing of an airway during resuscitation) and in a laboratory setting
• HCP with known HIV infection are at increased risk for meningococcal disease
Typhoid Fever • transmitted nosocomially via the hands of infected persons
Hepatitis A • HCP not at increased risk for hepatitis A virus infection because of occupational exposure
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011

Guidelines and recommendations
• 2011 Advisory Committee Immunization Practices (ACIP) Immunization of Health-Care Personnel
• 2012 PSMID – PHICS – PFV Recommended immunization for healthcare workers
• 2016 ACIP Updated Recommendations

Diseases for Which Vaccination Is Recommended
Hepatitis B
Influenza
Measles Mumps Rubella (MMR)
Pertussis
Varicella
Diseases for Which Vaccination Might Be Indicated in Certain Circumstances
Meningococcal
Typhoid Fever
Pneumococcal
Tetanus and Diphtheria
Human papilloma virus
Zoster
2011 Immunization of Health-Care Personnel Advisory Committee on Immunization Practices (ACIP)
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011


Strongly recommended
Hepatitis B
Influenza
Measles Mumps Rubella (MMR)
Tetanus, Diphtheria, acellular Pertussis (Tdap)
Varicella
Recommended
Pneumococcal
Recommended for selected HCW
Hepatitis A
Meningococcal vaccine
Rabies
Typhoid vaccine
2012 Healthcare Workers Vaccination Guide
2012 Recommended immunization for healthcare workers PSMID PHICS and PFV

2012 Healthcare Workers Vaccination Guide
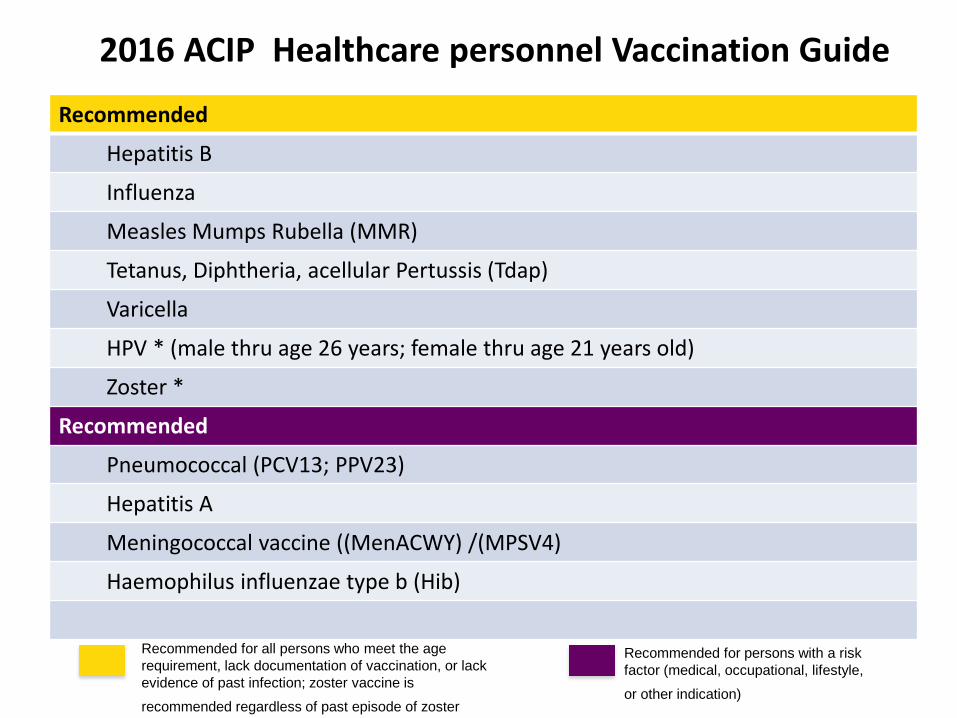
Recommended
Hepatitis B
Influenza
Measles Mumps Rubella (MMR)
Tetanus, Diphtheria, acellular Pertussis (Tdap)
Varicella
HPV * (male thru age 26 years; female thru age 21 years old)
Zoster *
Recommended
Pneumococcal (PCV13; PPV23)
Hepatitis A
Meningococcal vaccine ((MenACWY) /(MPSV4)
Haemophilus influenzae type b (Hib)
2016 ACIP Healthcare personnel Vaccination Guide
Recommended for all persons who meet the age
requirement, lack documentation of vaccination, or lack
evidence of past infection; zoster vaccine is
recommended regardless of past episode of zoster
Recommended for persons with a risk
factor (medical, occupational, lifestyle,
or other indication)

2012 PSMID-PFV-PHICS 2016 ACIP
Routinely Recommended
Hepatitis B Hepatitis B
Influenza Influenza
Measles Mumps Rubella (MMR) Measles Mumps Rubella (MMR)
Tetanus, Diphtheria, acellular Pertussis (Tdap) Tetanus, Diphtheria, acellular Pertussis (Tdap)
Varicella Varicella
Human Papilloma virus
Zoster
Not Routine Recommended but based on Risk
Pneumococcal (PPV23) Pneumococcal (PCV13; PPV23)
Hepatitis A Hepatitis A
Meningococcal Meningococcal
Rabies Hemophilic influenzae type b (Hib)
Typhoid

Recommendations on Immunization of Health Care Personnel with Special Conditions
Pregnancy
HIV infection CD4 <200
Immunocompromising conditions
Chronic liver ,heart and lung dses and alcoholism
Asplenia and complement component deficiencies
Kidney failure, end- stage renal disease, receipt of hemodialysis
Diabetes Men sex with men MSM)
Influenza
Tdap
Varicella
HPV
Rabies
Zoster
MMR
Pneumococcal (PCV13
Pneumococcal (PPV23)
Hepatitis A
Hepatitis B
Meningococcal
R- recommended; UI-use if indicated; C-contraindicated Vaccines 6th ed. 2013 Chap 66 pp 1290-1308

Vaccine with specific indications on selected healthcare personnel
Vaccine Specific indications
Typhoid vaccine • Food handlers, dieticians, cooks, nutritionist • microbiologist
Meningococcal • Clinical and research microbiologists who may be routinely exposed to isolates of Neisseria meningitides
Rabies • Laboratory personnel or researchers who work with rabies virus of potentially infected animals;
• PEP may be required for potential exposure despite primary immunization
• veterinarians and veterinary students, • health care workers directly involved in care of
rabies patients • individuals directly involved in rabies control, field
workers)
Vaccines 6th ed. 2013 Chap 66 pp 1290-1308

Vaccine schedule

HEPATITIS B ROUTINE ADULT VACCINATION
Vaccine type: Target individuals
• Inactivated vaccine • intramuscularly (IM) 3 doses :0,1,6-12 months • Accelerated schedule Days 0, 7, 21-30, and at 12 months • Booster is not routinely recommended
Vaccine efficacy: • >90% after the 3rd dose • 40 y.o., <90% • 60 y.o, 75%
•Those without documented evidence of immunity to
Hepatitis B
•All healthcare workers
•Sexually active persons, MSMs, IV drug users,
•Clients and staff members of institutions for persons
with disabilities
•Travelers to countries with high or intermediate
prevalence of chronic Hepatitis B infection
•Diabetics, Persons with HIV/AIDS
•Chronic liver disease, Hemodialysis patients
•Household contacts of HBV carrier •Recipients of blood products • Immigrants from areas of high HBsAg endemicity
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

HEPATITIS B and HCPs Pre-exposure Post-exposure
• Pre-vaccination serologic testing is indicated for HCP and is cost-effective in certain high-risk populations regardless of vaccination status
• Post-vaccination serologic testing should be performed for all HCP at high risk for occupational percutaneous or mucosal exposure to blood or body fluids
• Post-vaccination serologic testing is performed 1–2 months after administration of the vaccine series
• Persons determined to have anti-HBs concentrations of ≥10 mIU/mL are considered immune
• If anti-HBs concentrations <10 ,administration a second 3-dose series on an appropriate schedule, followed by anti-HBs testing 1–2 months
• If no response, test for HBsAg and anti-HBc
• Vaccinated HCP with documented immunity
(anti-HBs concentrations of ≥10 mIU/mL)
require no postexposure prophylaxis,
serologic testing, or additional vaccination
• Vaccinated HCP with documented
nonresponse to a 3-dose vaccine series
should receive 1 dose of HBIG and a second
3-dose vaccine series if the source is HBsAg-
positive or known to be at high risk for
carrying hepatitis
• Vaccinated HCP with documented
nonresponse to two 3-dose vaccine series
should receive 2 doses of HBIG, 1 month
apart if the source is HBsAg-positive or
known to be at high risk for carrying
hepatitis
•
MMWR Recommendations and Reports / Vol. 60 / No. 7 November 25, 2011

Pre-exposure Management for
Healthcare Personnel with a Documented Hepatitis B Vaccine
Series Who Have Not Had Post- vaccination
Serologic Testing

INFLUENZA Vaccine type and schedule WHO 2016 Recommendation
2 types:
•trivalent inactivated
•quadrivalent inactivated
• IM route
• Southern Hemisphere strain
• February to June, but maybe given throughout the year.
Vaccine efficacy: •varies from year to year •age and health status of the person •similarity “match” between the viruses or virus in the vaccine and those in circulation
It is recommended that trivalent vaccines for use in the 2016 influenza season (southern hemisphere ) contain the following:
•an A/California/7/2009 (H1N1)pdm09-like virus;
•an A/Hong Kong/4801/2014 (H3N2)-like virus;
•a B/Brisbane/60/2008-like virus. •It is recommended that quadrivalent vaccines containing two influenza B viruses contain the above three viruses and a B/Brisbane/60/2008-
like virus.

The Rationale For Quadrivalent Influenza Vaccines (QIV)
Why is it important that an
additional B strain be added to
trivalent influenza vaccines?

Circulating Influenza B lineages Philippines 2003-2013 and Vaccine mismatch
Source: Flunet, http://apps.who.int/globalatlas/dataQuery/default.asp, accessed January 2014

Vaccine type/route Schedule
MEASLES, MUMPS, RUBELLA (MMR) •live attenuated, SQ
•2-dose vaccine effectiveness of 99% (Measles) 75-95% (Mumps), 95% (rubella)
2 doses
• 0, 1 month interval
Tetanus, Diphtheria, acellular Pertussis (Tdap) - inactived, IM route
•vaccine effectiveness at 66%- 78%
3 doses (1 Tdap + 2 Td): • 0,1,6-12 months Booster every 10 years with Td
VARICELLA • live attenuated, SQ
• vaccine effectiveness 80%– 85%
2 doses
• 0, 1-2 months
Post-exposure Prophylaxis
• Given within 72 hours of exposure;
Single dose
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

HUMAN PAPILLOMAVIRUS (HPV)
Vaccine type Target individuals
• Inactivated
1. Bivalent (Types 16,18) • Females only
2. Quadrivalent (Types (6,11,16,18)
• Females and males
Recommended for: • Females: 9-55 years old • Males: 10-26 years old
•May be given as catch up vaccination to 13-21 years old who have not been previously vaccinated or who have not completed the 3-dose series
Schedules
Bivalent – for females only •2 doses: 9 to 13 years old, (0, 6 or 12 months)
•3 doses: >13 years old, (0, 1, 6 months)
Quadrivalent - for males and females •3 doses 0,2,6 months
• Females: 14 to 45 years old • Males: 14 to 26 years old
•2 doses: Female 9-13 years old. 0, 6 or 12 months
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

Vaccine type Indications and schedule
Pneumococcal vaccine
(inactivated)
•Polysaccharide (PPSV23)
IM or SQ
• Conjugate (PCV13) IM route
•Sequential pneumococcal
vaccination (PCV13-PPV23)
For elderly (>50 yo), immunocompetent
•PCV13 then PPSV23 in 6-12 months
For immunocompromised
•PCV13 then PPSV23 at least 8 weeks
For those previously received 1 or 2 doses PPV23
• Give PCV13 12 months after the most recent dose
of 23vPPV
Revaccination
•Single dose PPV23 after 5 months
Meningococcal Vaccine • Polysaccharide (MPSV): SQ/IM • Conjugate (MCV4) : IM
• For immunocompetent, single dose 0.5 ml’ no revaccination
• For immunocompromised, single dose 0.5 ml, revaccination after 5 years
Hepatitis A
• IM; Single antigen or in
combination with Hepatitis B
For monovalent: 2 doses at 0, 6-12 months In combination with hepatitis B: 0,1,6 months
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

HERPES ZOSTER
Vaccine type: Target individuals
• Live, attenuated VZV
vaccine • single-dose 0.65 ml SQ
•Prevention of herpes zoster (HZ) •Prevention of postherpetic neuralgia (PHN) •Reduction of acute and chronic HZ-associated pain
•Adults ≥ 60 years old with or without a prior episode of herpes zoster • Persons with history of zoster • Men sex with men (MSMs) •Persons with chronic medical conditions
•chronic renal failure •diabetes mellitus •rheumatoid arthritis •Heart disease, chronic lung and chronic liver disease •healthcare workers •Asplenia
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

Vaccine type/route Schedule
TYPHOID •IM, •VI capsular polysaccharide
For primary and booster single 0.5 ml M dose on the deltoid
RABIES •IM/Intradermal (HDCV , PVRV, PCECV)
Pre-exposure: 3 injections on days 0, 7 & 21 or 28 Post-exposure :
2015 Schedule of Adult Immunization
Philippine Society for Microbiology and Infectious Disease (PSMID) and Philippine Foundation for Vaccination (PFV)

IMPACT OF VACCINES
Johnson DR, et al. Am J Med 2008;121:S28-S35 JAMA. 2007;298(18):2155-2163
CDC. MMWR January 7, 2011;59(52);1704-1716.
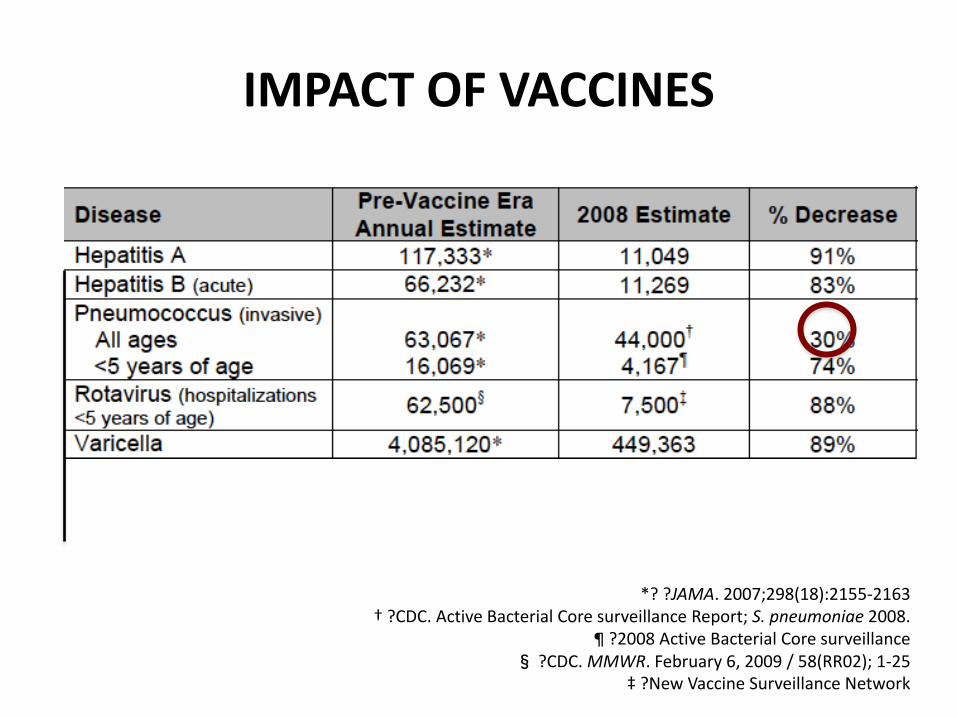
IMPACT OF VACCINES
*? ?JAMA. 2007;298(18):2155-2163 † ?CDC. Active Bacterial Core surveillance Report; S. pneumoniae 2008.
¶ ?2008 Active Bacterial Core surveillance § ?CDC. MMWR. February 6, 2009 / 58(RR02); 1-25
‡ ?New Vaccine Surveillance Network

Barriers for Vaccination
• Both Private and Public HcW views vaccines as expensive increasing barriers for vaccination despite the need.
PUBLIC PRIVATE

BARRIERS
PATIENT AWARENESS/B
ELIEFS
PHYSICIAN RESOURCES / KNOWLEDGE
INFRASTRUCTURE
National Foundation for Infectious Diseases. Call To Action: Adult Vaccination Saves Lives. Bethesda, MD, 2012.
MYTHS

Steps in the process of implementing a vaccination policy for HCWs
H.C. Maltezou, G.A. Poland / Vaccine 32 (2014) 4876–4880

Measures should be taken to ensure healthcare workers are provided convenient access to vaccine.
Employers of healthcare workers need to commit resources toward institutionalizing immunization in the workplace
They need to demonstrate that immunization is an employee and patient safety PRIORITY.
45

KEY CHALLENGE
“THE BIGGEST CHALLENGE IS THE CHALLENGE OF CHANGING SOMEONE’S MIND”
-- Paul Sax, MD

http://www.vaccines.gov/basics/protection/
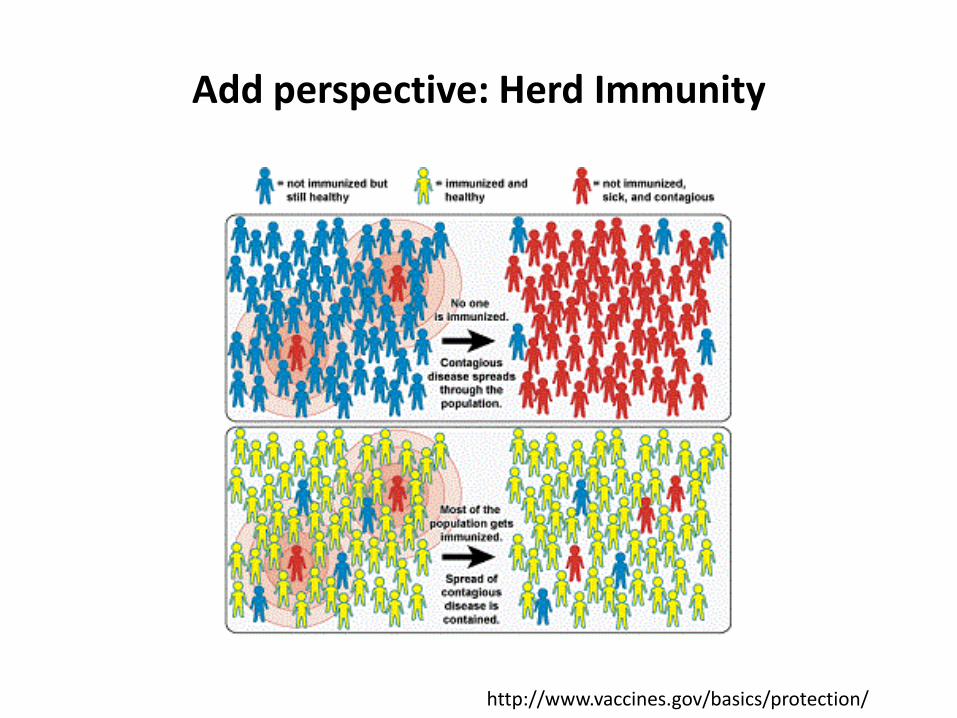
Add perspective: Herd Immunity
http://www.vaccines.gov/basics/protection/

Before you vaccinate adults, consider their “H-A-L-O”!
H-A-L-O checklist of factors that indicate a possible need for adult vaccination
Technical content reviewed by the Centers for Disease Control and Prevention www.immunize.org/catg.d/p3070.pdf


51
Thank you