the prodrome to delirium - ceconnection
TRANSCRIPT
The Prodrome to DeliriumA Grounded Theory Study
Kristie L. Szarpa, MSN, RN, ANP-BC, CHPN ƒ Christopher W. Kerr, MD, PhD ƒScott T. Wright, BA ƒ Debra L. Luczkiewicz, MD ƒ Pei C. Hang, PhD ƒLisa S. Ball, PhD, RN, FNP-BC
Delirium is a state of confusion that occurs in up to 90%of patients facing end-of-life. Despite its prevalence,there is a paucity of data that describes the prodrome todelirium. Family and caregivers are key observers of thephenomenology of delirium and often recall subtlesigns and symptoms that herald the delirious episode.The objective of this study was to describe caregiverobservations regarding the onset, characteristics, andprogression of the predelirium state in hospice patientsdiagnosed with delirium. A purposive sample of 10caregivers of hospice patients took part in private,semistructured, audiotaped interviews. The interviewswere transcribed verbatim and analyzed using theStraussian approach to grounded theory. Six categoriesof commonalities emerged: physically declining,cognitively/psychologically declining, withdrawing,end-of-life awareness, deteriorating sleep pattern, andsuffering. A process model was created that illustratesthe temporal progression of sleep deterioration in thepresence of overall decline, which leads to the diagnosisof delirium. In addition, the model illustrates theexperience of suffering, which is woven throughoutthis temporal decline, becoming increasingly magnifiedas delirium progresses. These findings provideinsight regarding early signs and symptoms ofemerging delirium.
KEY WORDScaregivers, delirium, end-of-life, prodrome to delirium,sleep disturbance
Delirium is a complex syndrome with multiple eti-ologies characterized by fluctuating disturbancesin consciousness, attention, memory, thought, and
perception.1-3 Delirium is nearly ubiquitous within medicalsettings and is themost common psychiatric disorder amongthe cancer patient population.4-6 It is present inmost patientsat the end of life, associated with poorer survival, and is anindependent predictor of mortality.7-12 Despite the prev-alence and significance of delirium, it remains under-diagnosed and undertreated.5,13-15 Delirium can acceleratethe end-of-life process, despite being potentially reversiblein as many as 50% of cases.16,17 In part, inconsistent as-sessment and diagnosis may limit the clinician’s ability torecognize the underlying pathogenesis of delirium.7 Unfor-tunately, delirium is often not diagnosed until in its ful-minate state, and there is a paucity of data that describes ordetect the prodromal phase of delirium.7,12,16,17 There is aneed for studies that clarify the risk factors and pathogenesisof delirium in order to provide earlier detection, prevent fur-ther worsening in reversible cases, and provide a strategythat reduces the risk of developing delirium.18 Although de-lirium in certain cases may be linked to specific etiologies,such as infection, sleep disturbance, medications, dehydra-tion, urinary retention, pain, or constipation,1,3 many deliri-ous patients have no clear toxic or metabolic abnormality.19
A more complete description may require acknowledge-ment of less definable causes or contributing factors.
Family and caregivers are key observers to the phenom-enology of delirium and often recall subtle signs and symp-toms that herald delirious episodes.14,20-22 They are oftenwitness to the earliest manifestations and challenges of de-lirium, such as nocturnal agitation and behavioral distur-bances, and may score even higher than their deliriousloved ones on measures of distress.2 Caregivers thereforeare in the best position to alert health care providers to earlysigns and symptoms of delirium. The caregiver perspectivealso highlights the fact that delirium has impact beyond thepatient and is a source of suffering for caregivers as well astheir loved ones.
Kristie L. Szarpa, MSN, RN, ANP-BC, CHPN, is nurse practitioner atthe Center for Hospice & Palliative Care, Cheektowaga, New York.
Christopher W. Kerr, MD, PhD, is chief medical officer at the Centerfor Hospice & Palliative Care, Cheektowaga, New York.
Scott T. Wright, BA, is research assistant at the Center for Hospice &Palliative Care, Cheektowaga, New York.
Debra L. Luczkiewicz, MD, is physician at the Center for Hospice &Palliative Care, Cheektowaga, New York.
Pei C. Hang, PhD, is director of Research at the Center for Hospice &Palliative Care, Cheektowaga, New York.
Lisa S. Ball, PhD, RN, FNP-BC, is assistant professor in the NursingDepartment at Daemen College, Amherst, New York.
Address correspondence to Christopher W. Kerr, MD, PhD, Center forHospice & Palliative Care, 225 Como Park Blvd, Cheektowaga, NY14227 ([email protected]).
The authors have no conflicts of interest to disclose.
DOI: 10.1097/NJH.0b013e31828fdf56
332 www.jhpn.com Volume 15 & Number 6 & August 2013
2.3 ANCC Contact HoursSymptom Management Series
The purposes of this studywere to explore the develop-ment and progression of delirium experienced by hospicepatients and to generate a theoretical model that describesthe prodrome to delirium as observed by caregivers.Grounded theory analysis was used to establish cate-gories and characterize the progression of observed pa-tient changes leading to the development of deliriumin an effort to more clearly define the prodromal phaseof delirium.
METHODS
Study DesignThe current study was based on grounded theory method-ology, which provides insight into complex processes andsignificant life events such as delirium in the dying patientusing inductive methods to analyze qualitative data.23
Corbin and Strauss24 noted that grounded theory develop-ment involves the discovery of concepts and recognition ofthemes within data and identifying relationships betweenthemes and categories derived directly from the data andnot frompreconceived hypotheses. The Straussianmethodincorporates a current literature search as well as the re-searchers’ previous experiences with the topic in questionand offers a transparent and structured method for explor-ing otherwise elusive details and processes.25,26
The studywas reviewed and approved by the Center forHospice & Palliative Care’s Proposal Review Committee aswell as the Daemen College Human Subjects Research Re-view Committee. Written consent was obtained from eachparticipant who voluntarily took part in the study. Partici-pant interviews were conducted over a 3-month period in2012. The data used in this study were a subset of data col-lected for a larger study,which looked at the progression ofdelirium in advanced illness from both the caregiver andclinician perspective.27
ParticipantsStudy participants included a purposive sample of care-givers of hospice patients admitted into the Hospice BuffaloInpatient Unit with a diagnosis of delirium according toDi-agnostic and Statistical Manual of Mental Disorders,Fourth Edition criteria. To be included in this study, care-giver participants had to be 18 years or older, English-speaking, and willing to talk with the researcher in aninterview format about their observations regarding the on-set, features, and course of witnessed clinical progressiontoward delirium. Patients with a history of psychosis orthought disorder, diagnosis of dementia, encephalopathy,brainmetastasis, or signs of significant renal or hepatic dys-functionwere excluded from this study as these factorsmayproduce many of the same symptoms seen in deliriouspatients.
ProceduresConsenting caregivers participated in a semistructured in-terview with open-ended questions regarding observa-tions of their loved ones in the period prior to admissionto the Hospice Buffalo Inpatient Unit. Each interview wasbetween 20 and 45 minutes in length, audiotaped, andtranscribed verbatim without identifying information in or-der to maintain confidentiality in preparation for analysis.The data analysis process included open, axial, and selec-tive coding, which entails identifying and assigning labelsto what is happening in the data, relating and categorizingthose labels, and then selecting which categories and rela-tionships are the central processes to the developing theory,thus ensuring that the theory is grounded in the data.24 Toensure a high level of validity and rigor, two independentresearchers manually coded all data. In addition, to deter-mine fit of findings after theoretical saturation of the majorcategorieswas reached, the emerging theory findingswerebrought back to participants to determine that they accu-rately reflected their experience of the prodrome to delir-ium. Theoretical saturation, the point at which no newsignificant relationships or characteristics regarding theemerging theory are identified, was reached after inter-viewing 10 participants.
RESULTS
Ten caregiver participants were interviewed regardingchanges observed in their loved ones during the time pe-riod leading up to the diagnosis of delirium. This time pe-riod varied greatly among participants. Some reflectedback over a period of months, whereas others offered theirobservations of change and decline over a period of daysto weeks. Despite variations in preceding timeframe, par-ticipants overwhelmingly described suffering, the corecategory that emerged in this study, as the process that en-capsulated all other processes. Those other processes in-cluded physically declining, cognitively/psychologicallydeclining,withdrawing, end-of-life awareness, and deteri-orating sleep pattern. A theoretical model depicting thisprocess is presented in the Figure. This model shows theoverall patterning of the processes that occurs in the timepreceding outright delirium; whether the processes oc-curredgradually, stepwise, or suddenlywas variablebetweenpatients and may be due to factors such as differences inunderlying etiologies. This model depicts a V-shaped framerepresenting the decreasing fullness of life, which ultimatelyends in delirium, depicted in bold letters at the bottom pointof the V-frame. Centralized, interwoven, downward spiral-ing arrows represent 4 of the 6 processes leading to delirium(physically declining, cognitively/psychologically declining,withdrawing, and end-of-life awareness) that are experi-enced by most patients, although there was wide variationin degree and no pattern noted other than an overall decline
Journal of Hospice & Palliative Nursing www.jhpn.com 333
Symptom Management Series
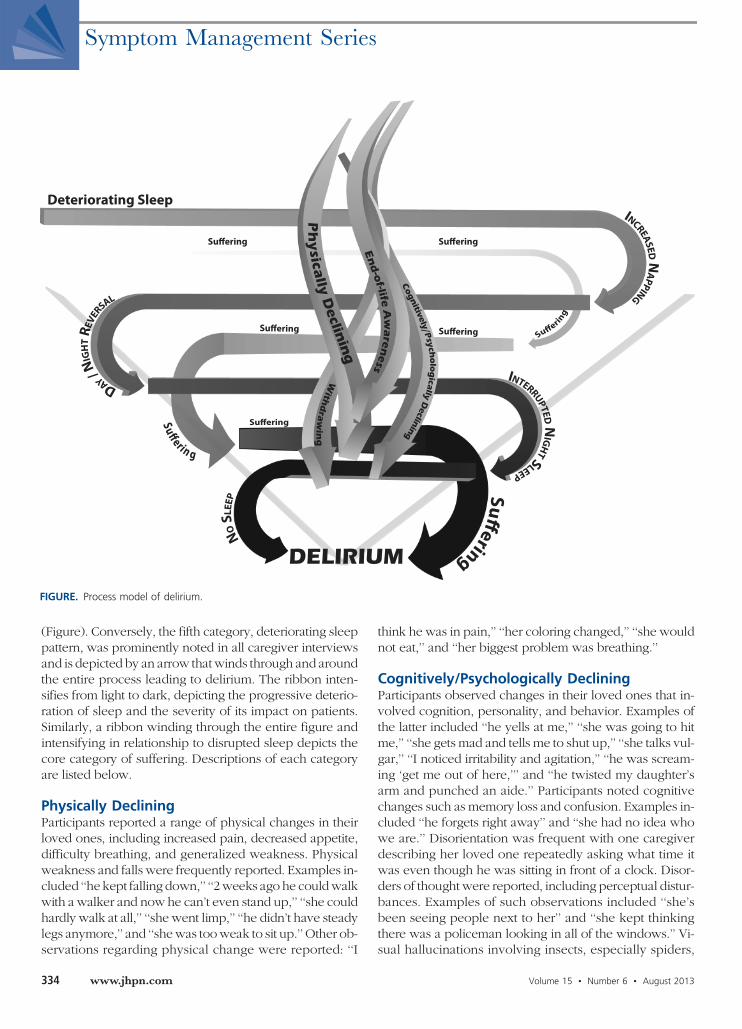
(Figure). Conversely, the fifth category, deteriorating sleeppattern, was prominently noted in all caregiver interviewsand is depicted by an arrow thatwinds through and aroundthe entire process leading to delirium. The ribbon inten-sifies from light to dark, depicting the progressive deterio-ration of sleep and the severity of its impact on patients.Similarly, a ribbon winding through the entire figure andintensifying in relationship to disrupted sleep depicts thecore category of suffering. Descriptions of each categoryare listed below.
Physically DecliningParticipants reported a range of physical changes in theirloved ones, including increased pain, decreased appetite,difficulty breathing, and generalized weakness. Physicalweakness and falls were frequently reported. Examples in-cluded ‘‘he kept falling down,’’ ‘‘2 weeks ago he couldwalkwith a walker and now he can’t even stand up,’’ ‘‘she couldhardly walk at all,’’ ‘‘she went limp,’’ ‘‘he didn’t have steadylegs anymore,’’ and ‘‘shewas tooweak to sit up.’’ Other ob-servations regarding physical change were reported: ‘‘I
think he was in pain,’’ ‘‘her coloring changed,’’ ‘‘she wouldnot eat,’’ and ‘‘her biggest problem was breathing.’’
Cognitively/Psychologically DecliningParticipants observed changes in their loved ones that in-volved cognition, personality, and behavior. Examples ofthe latter included ‘‘he yells at me,’’ ‘‘she was going to hitme,’’ ‘‘she gets mad and tells me to shut up,’’ ‘‘she talks vul-gar,’’ ‘‘I noticed irritability and agitation,’’ ‘‘he was scream-ing ‘get me out of here,’’’ and ‘‘he twisted my daughter’sarm and punched an aide.’’ Participants noted cognitivechanges such as memory loss and confusion. Examples in-cluded ‘‘he forgets right away’’ and ‘‘she had no idea whowe are.’’ Disorientation was frequent with one caregiverdescribing her loved one repeatedly asking what time itwas even though he was sitting in front of a clock. Disor-ders of thought were reported, including perceptual distur-bances. Examples of such observations included ‘‘she’sbeen seeing people next to her’’ and ‘‘she kept thinkingthere was a policeman looking in all of the windows.’’ Vi-sual hallucinations involving insects, especially spiders,
FIGURE. Process model of delirium.
334 www.jhpn.com Volume 15 & Number 6 & August 2013
Symptom Management Series

were prevalent. Others described emotional distress suchas ‘‘fear’’ or restlessness such as pacing.
WithdrawingParticipants described patient withdrawal in statementssuch as ‘‘nothing interested him anymore’’ and ‘‘I noticedshe is not interested in things.’’ One caregiver explainedthat her loved one used to live for visits from her grand-children but now would not speak to them when theycame to visit. Another participant explained that her lovedone would no longer look at her favorite magazine. Inabil-ity to focus was commonly described: ‘‘she’d just stareahead,’’ ‘‘he’d just stare right through things,’’ ‘‘he never re-ally focused anymore,’’ ‘‘she is not there in the moment,’’and ‘‘she’d just stare ahead when you are talking to her.’’One participant summed up her loved one’s withdrawingby saying, ‘‘his eyes didn’t shine anymore.’’
End-of-Life AwarenessIssues surrounding end-of-life awareness evoked thegreatest emotion from caregivers. Nearly all caregiversreported that their loved one expressed awareness of thedying process or impending death. One caregiver recalledthat her loved onemade comments such as ‘‘I wonderwhatit’s like in the end’’ and ‘‘I wonder if I’ll know when it’stime.’’ Another caregiver said her loved one stated ‘‘I’mdyingI I feel itI there is a veil coming down over me.’’Others reported themesof life reviewand ‘‘going backoverlife events.’’ One caregiver recounted her loved one’s vividfuneral dream and noted that her loved one began to saygoodbye, asking if the caregiver was going to be okay. An-other of the caregivers described a ‘‘breakthroughmoment’’in which his previously confused loved one suddenlygained clarity, recognized everyone around him, huggedthem, and expressed his love.
Deteriorating Sleep PatternDisrupted sleep was the most commonly reported changeobserved by participants. Sleep fragmentation was de-scribed as frequent awakenings, alterations in the day/night cycle, and increased daytime somnolence. Partici-pant reports included ‘‘he was always sleepy,’’ ‘‘he wassleeping more,’’ ‘‘she did sleep a lot more during the daythan a normal person did,’’ and ‘‘she would sleep 16 hoursa day.’’ The next reported change involved day/night re-versal in which loved ones slept during the day, awokein late evening, and often stayed awake all night. One par-ticipant recounted: ‘‘She would get up and have breakfast,and it wasn’t even an hour later, and she would not sayanything, and she would go back to bed and sleep for3 to 4 hours and even past meal time, and I would go inand say ‘do youwant lunch,’ and she would sleep past thatand that would go on for 2 to 3 days most times. Then shewould be up all night.’’
The next category of observations involved progres-sively deteriorating sleep quality defined by frequentlyinterrupted, often cyclic, nighttime sleep. Multiple care-givers commented that their loved one awoke as often asevery 20minutes.Oneparticipant explained, ‘‘the episodesof waking up at night were more frequent, every night.’’Poor sleep quality, including vivid dreaming, was well de-scribed. Examples included ‘‘she’s not in a sound sleep,’’‘‘I could tell his sleep wasn’t sound anymore,’’ and ‘‘shemay have looked like she was sleeping, but her eyes neverreally closed.’’ Disrupted sleep correlated with accelerateddecline in all other categories of observed change resultingin agitation, restlessness, and vivid and frightening dreamsas well as hallucinations. The severity of restlessness wasincompatible with sleep and in many cases extended intodays of sleep deprivation. In one case, a participant calledfor help after she and her loved one were awake for 6 con-secutive days. Per the participant, the patient stated that ‘‘Ijust can’t sleep, my mind starts racing.’’
SufferingSuffering clearly emerged as the overarching process thatdefined the prodromal phase of delirium and was experi-enced by both participants and their loved ones. Statementsincluded ‘‘I knew he was suffering, whether it was mentallyor physically,’’ ‘‘there is no question he is sufferingVhe isin a state of suffering,’’ and ‘‘he was suffering, absolutely.’’Psychogenic suffering was inferred by participants who re-ported that their loved one was experiencing sadness, de-pression, frustration, and feeling as if they were ‘‘trapped.’’One participant recounted her loved one screaming‘‘GodIwhy are you doing this tome?’’ Throughout the in-terviews, participants struggled with their emotions, oftencrying as they reflected back upon these events.
DISCUSSION
The current study examined the onset, features, and pro-gression of delirium in hospice patients as described bytheir caregivers. Given their special role, caregivers are of-ten witness to the subtle signs and symptoms that precededelirious episodes.14,20-22 Caregiver observations wereanalyzed using grounded theorymethodology, which re-vealed six categories of clinical changes leading to the di-agnosis of delirium: physically declining, cognitively/psychologically declining, withdrawing, end-of-life aware-ness, deteriorating sleep pattern, and suffering. Althoughthe categories identified within this study have previouslybeenassociatedwitheitherdeliriumor theend-of-lifeprocess,there is an absence of data exploring the progression of signsand symptoms leading to the diagnosis of delirium.7,16,17
Prior studies have established a connection between ill-ness progression and delirium. Morita et al21 surveyedbereaved family members whose loved ones developed
Journal of Hospice & Palliative Nursing www.jhpn.com 335
Symptom Management Series

delirium. Family members associated factors such as pain,medications, and physical discomfort with the emergenceand progression of delirium.21 Caregivers interviewed inthis study also noted pain and generalized decline in thetimeframe leading up to delirium. Physical weakness, tothe point of falling down, was described in multiple inter-views. This finding has not been previously explored in re-lationship todeliriumandmaywarrant further consideration,as it is not clear whether falls may serve as an indicator ofpotential emergence of delirium and related symptomssuch as agitation, or may be due to progression of illness.Cognitive decline, behavioral changes, and withdrawalhave also been correlated with the pathogenesis of the de-lirious state. Duppils and Wikblad28 noted several behav-ioral andpsychological changes, suchas anxiety, experiencedin postoperative, elderly patients who subsequently devel-oped delirium. Bush and Bruera,13 in their exploration ofdelirium, noted lack of focus and inattention, as well asother cognitive changes including altered perceptions. Thecognitive decline andwithdrawal revealed by caregivers inthe current study add to these findings and suggest thatsubtle and nonspecific signs and symptoms that character-ize the progression of deliriummay be clinically significant.
Alterations in the sleep/wake cycle have long been as-sociated with delirium. The delirious state is known to in-clude symptoms of daytime somnolence and reversal ofthe sleep/wake cycle as well as sleep interrupted by agita-tion and restlessness.29,30 It remains uncertain whether adisrupted sleep cycle is a cause or consequence of delir-ium. A recent prospective, longitudinal study of 105 hospicepatients found that poor sleep quality precedes deliriumonset, adding support to a causal relationship betweensleep disturbance and delirium.31 Others have proposeda link between severe rapid eye movement deficiency andthe development of delirium in neurodegenerative disease31,32
aswell as in intensive care unit patients.33,34 The current find-ings describe a prodromal pattern of poor sleep quality prog-ressing to fragmentation of the sleep/wake cycle, agitation,and cognitive disturbances. Although an orderly progres-sion is suggested, the time period of sleep disturbance de-scribed in this study varied. However, recognition of thecore deficit of sleep dysfunction may help alert cliniciansand other members of the interdisciplinary team caring forthepatient to the early signs of deliriumor predelirious states.
The overarching theme reported by caregivers of delir-ious patients in this study was suffering. Clinicians share anunderstanding that delirium involves sufferable states, in-cluding pain, which are challenging to define.33 In the cur-rent study, participants stated both indirectly and directlythat they also experienced suffering as they witnessedthe loss of personhood, which characterizes delirium. Suf-feringwas also associatedwith each of the other categoriesof delirium-associated changes aswell. There is an elementof suffering associatedwith physical and cognitive decline,
as well as patient withdrawal from loved ones, activities,and interests. Given complications such as nocturnal agita-tion and sleeplessness, it is not surprising that the inter-views conducted in this study suggested that deterioratingsleep plays a key role in contributing to overall sufferingfor both patients and their caregivers. Previous researchhas also shown that caregivers may score even higher thantheir delirious loved ones on measures of distress leadingto challenges in coping with consequences of delirium.2
Processing impending death is intrinsic to end-of-lifeclosure and acceptance. However, this process also con-tributes to the spiritual and psychological suffering experi-enced by dying patients and their loved ones. Participantsin this study consistently reported distressing commentsmade by their loved ones, which were categorized in thisstudy as ‘‘end-of-life awareness.’’ It is unclear to what ex-tent the degree of distress associated with end-of-lifeawareness in this study was affected by developing delir-ium. The overall prevalence of suffering in the current studyleads to questions regarding the relationship between con-fusional states and the psychological processing inherentto the dying process. Is it possible, for example, that theprocess of dying is associated with psychological discom-fort that may also lower the threshold for delirium? Dostates of severe psychological suffering contribute to thedevelopment of cognitive disorganization? Further re-search is needed to explore the association between end-of-life awareness, associated psychogenic distress, and thedevelopment of delirium.
Implications for Practice and Future ResearchThe current study highlights the importance of caregiversas witnesses to the signs and symptoms associatedwith theprogression of delirium. Although delirium is common anddistressing for end-of-life patients, the pathogenesis of de-lirium is poorly understood, and there is a clear need forcaregiver education. Interviews of families whose lovedones experienced delirium at the end of life have demon-strated a desire for improved delirium screening and man-agement.21 Others have reported that families can assist inthe prevention of delirium given their bedside presenceand advocacy.35 The current study suggests the existenceof a set of signs and symptoms that may precede deliriumand that may progress in a more or less predictable fashionto full-blown delirium. Findings from this research studyare important for clinical practice, education, and research.An understanding of this progression may help lead to im-proved screening methods to identify delirium in its early,more easily treated stages, resulting in greater quality of lifeand a decrease in suffering for patients and their caregivers.A greater awareness of the prodromal symptoms of delir-ium may also help other members of the hospice interdis-ciplinary team, such as chaplains, social workers, aides,therapists, and even volunteers, identify patients at risk
336 www.jhpn.com Volume 15 & Number 6 & August 2013
Symptom Management Series

for development of delirium so that the patient’s nurse andphysician can intervene to provide education and interven-tion at earlier stages.
Limitations of this study include the retrospective natureof the interviews, which may have affected participants’ability to recall the episodes reported in the interviews.The emotional content of the interviewsmay also have col-ored recollections of the severity of symptoms and relativeprominence of events. Given the nature of delirium, whichby definition causes confusion, the actual personexperiencing delirium is not a reliable source of informa-tion, and thus data had to be collected from the next bestsource, the caregivers. This may have resulted in a degreeof bias due to second-person assessment of the deliriumexperience as lived by the patient. Limitations inherent tothe use of grounded theory analysis include the potentialfor researcher-induced bias in the categorization of dataand the qualitative nature of the results, but the rigorousmethods used in this study, including purposive sampling,bracketing, member checking, and researcher triangula-tion, help increase the degree of credibility, transferability,dependability, and confirmability of the findings. In addi-tion, there may be some confound between delineatingwhat may be due to prodrome of delirium and what is re-lated to general disease-related decline. Despite these lim-itations, the results of this study provide a starting point forfuture studies of the signs and symptoms of the prodrometo delirium and may help lead to earlier identification ofand screening for delirium.
References1. Marcantonio ER. Delirium.Ann InternMed. 2011;154(11):ITC6-1.2. Breitbart W, Gibson C, Tremblay A. The delirium experience:
delirium recall and delirium-related distress in hospitalizedpatients with cancer, their spouses/caregivers, and their nurses.Psychosomatics. 2002;43(3):183-194.
3. Gofton TE. Delirium: a review.Can J Neurol Sci. 2011;38(5):673-680.4. Caraceni A, Simonetti F. Palliating delirium in patients with
cancer. Lancet Oncol. 2009;10(2):164-172.5. Cole MG. Delirium in elderly patients. Am J Geriatr Psychiatry.
2004;12(1):7-21.6. Pisani MA, McNicoll L, Inouye SK. Cognitive impairment in the
intensive care unit. Clin Chest Med. 2003;24(4):727-737.7. Boyle DA. Delirium in older adults with cancer: implications for
practice and research. Oncol Nurs Forum. 2006;33(1):61-78.8. Bruera E, Miller MJ, Kuehn N, MacEachern T, Hanson J.
Estimate of survival of patients admitted to a palliative care unit:a prospective study. J Pain Symptom Manage. 1992;7(2):82-86.
9. Caraceni A, Nanni O, Maltoni M, et al. Impact of delirium on theshort term prognosis of advanced cancer patients. Italian Multi-center StudyGrouponPalliativeCare.Cancer. 2000;89(5):1145-1149.
10. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor ofmortality in mechanically ventilated patients in the intensivecare unit. JAMA. 2004;291(14):1753-1762.
11. Francis J, Martin D, Kapoor WN. A prospective study ofdelirium in hospitalized elderly. JAMA. 1990;263(8):1097-1101.
12. Moyer DD. Terminal delirium in geriatric patients with cancerat end of life. Am J Hosp Palliat Care. 2011;28(1):44-51.
13. Bush SH, Bruera E. The assessment and management of deliriumin cancer patients. Oncologist. 2009;14(10):1039-1049.
14. Caraceni A, Grassi L. DeliriumVAcute Confusional States inPalliative Medicine. New York: Oxford University Press, USA; 2003.
15. Inouye SK, Foreman MD, Mion LC, Katz KH, Cooney LM Jr.Nurses’ recognition of delirium and its symptoms: comparisonof nurse and researcher ratings. Arch Intern Med. 2001;161(20):2467-2473.
16. Leonard M, Agar M, Mason C, Lawlor P. Delirium issues in pal-liative care settings. J Psychosom Res. 2008;65(3):289-298.
17. Nicholson TR, Henderson M. Management of delirium. Br JHosp Med (Lond). 2009;70(4):217-221.
18. Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multi-component intervention to prevent delirium in hospitalizedolder patients. N Engl J Med. 1999;340(9):669-676.
19. Bruera E, Miller L, McCallion J, Macmillan K, Krefting L, Hanson J.Cognitive failure in patients with terminal cancer: a prospectivestudy. J Pain Symptom Manage. 1992;7(4):192-195.
20. Matsushima E, Nakajima K, Moriya H, Matsuura M, Motomiya T,Kojima T. A psychophysiological study of the development ofdelirium in coronary care units. Biol Psychiatry. 1997;41(12):1211-1217.
21. Morita T, Akechi T, Ikenaga M, et al. Terminal delirium:recommendations from bereaved families’ experiences. J PainSymptom Manage. 2007;34(6):579-589.
22. Namba M, Morita T, Imura C, Kiyohara E, Ishikawa S, Hirai K.Terminal delirium: families’ experience. Palliat Med. 2007;21(7):587-594.
23. Streubert HJ, Carpenter DR. Qualitative Research in Nursing:Advancing the Humanistic Imperative. Philadelphia, PA:Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011.
24. Corbin J, Strauss A. Basics of Qualitative Research: Techniquesand Procedures for Developing Grounded Theory. ThousandOaks, CA: SAGE Publications; 2008.
25. Hunter A, Murphy K, Grealish A, Casey D, Keady J. Navigatingthe grounded theory terrain. Part 2. Nurse Res. 2011;19(1):6-11.
26. Hunter A, Murphy K, Grealish A, Casey D, Keady J. Navigatingthe grounded theory terrain. Part 1. Nurse Res. 2011;18(4):6-10.
27. Kerr CW, Donnelly JP, Wright ST, et al. Progression of deliriumin advanced illness: a multivariate model of caregiver and clinicianperspectives. J Palliat Med. 2013. In press.
28. Duppils GS, Wikblad K. Delirium: behavioural changes beforeand during the prodromal phase. J Clin Nurs. 2004;13(5):609-616.
29. Kushida CA. Sleep Deprivation: Clinical Issues, Pharmacology,and Sleep Loss Effects. New York: Marcel Dekker; 2005.
30. Macleod AD. Delirium: the clinical concept. Palliat Support Care.2006;4(3):305-312.
31. Slatore CG, Goy ER, O’Hearn DJ, et al. Sleep quality and itsassociation with delirium among veterans enrolled in hospice.Am J Geriatr Psychiatry. 2012;20(4):317-326.
32. Arnulf I, Bonnet AM, Damier P, et al. Hallucinations, REM sleep,and Parkinson’s disease: a medical hypothesis. Neurology.2000;55(2):281-288.
33. Ganzini L. Care of patients with delirium at the end of life. AnnLong Term Care. 2007;15:35-40.
34. Weinhouse GL, Schwab RJ, Watson PL, et al. Bench-to-bedsidereview: delirium in ICUpatients - importanceof sleepdeprivation.Crit Care. 2009;13(6):234.
35. Rosenbloom-Brunton DA, Henneman EA, Inouye SK. Feasibilityof family participation in a delirium prevention program forhospitalized older adults. J Gerontol Nurs. 2010;36(9):22-33;quiz 25-34.
For more than 43 additional continuing education articles related to hospice and palliative care,go to NursingCenter.com/CE.
Journal of Hospice & Palliative Nursing www.jhpn.com 337
Symptom Management Series