the randomized controlled trial its uses and abuses 2006 hasan yazıcı university of istanbul
TRANSCRIPT

The Randomized Controlled Trial
its Uses and Abuses
2006Hasan Yazıcı
University of Istanbul

Plan● Why am I giving this talk?
● Why am I giving this talk?
● RCT as a scientific tool
- Historical aspects
- RCT and efficacy
- reallocation to a failing medicine
- extension studies
- RCT and adverse effects
- the time element
- FDA and the time element
● What next?

Randomized Controlled Trials in BS
The Cerrahpaşa Experience • Colchicine 1980, Haematologica
• Azathioprin 1990, N Engl J Med
• Alpha Interferon 1991, Br J Rheumatol
• Azapropazone 1995, Clin Exp Rheumatol
• Cyclosporine 1997, Int J Dermatol
• Thalidomide 1998, Ann Intern Med
• Colchicine 2001, Arthritis Rheum
• Etanercept 2005, J Rheumatol
• Steroids 2006, Rheumatology (Oxford)

“Forty percent of science news relates to health and medicine and we are seeing a gradual erosion of public trust.”
EA Zerhouni, Director NIH
PLoS Medicine 2006

Many people would simply say: “ We do this because we need to get FDA approval for the product.” Of course this is true but there is deeper societal reason for trying to determine medical products are useful. I am going to review briefly how we got where we are today, for pharmaceuticals in particular.
The efficacy requirement for pharmaceuticals dates back to the thalidomide tragedy in the late 1950s. Appalled by the concrete evidence of a drug’s truly devastating, undetected side effect, Congress decided that given the risks, drugs should not have been allowed on the market unless they had ben shown scientifically to have some benefit.
J Woodcock (FDA) Clinical Trials 2005

Confidence?• Complications of the COX-2 Inhibitors Parecoxib and Valdecoxib after
Cardiac Surgery. Nussmeier NA et al. NEJM 2005 352 1081 -1091.
• “The authors had complete access to the data after unblinding. All final analyses were conducted by an independent statistician at the Texas Heart Institute in Houston. The data reported here were those available to the authors as of February 14, 2005.”
• Cardiovascular Events Associated with Rofecoxib in a Colorectal Adenoma Chemoprevention Trial. Bresalier RS et al. NEJM 2005
352 1092 -1102. • “The data reported here are those available to the
authors as of February 14, 2005.”
The full texts of both articles appeared in the electronic version of NEJM on February 15, 2005.

Academic Medical Centers’ Standards for Clinical Trial Agreements with Industry
Mello et al N Engl J Med, 2005

Randomized Controlled Trial
Deductive
Tries to dis-prove (falficify) a hypothesis (Popperian)

The RCT and Efficacy
As a scientific tool the starting point of a RCT to study efficacy is to falcify the hypothesis that the new drug tested is superior to conventional, other new or no therapy.
If this hypothesis cannot be falcified only then the new treatment can be taken as superior to the other modalities.
K. Popper

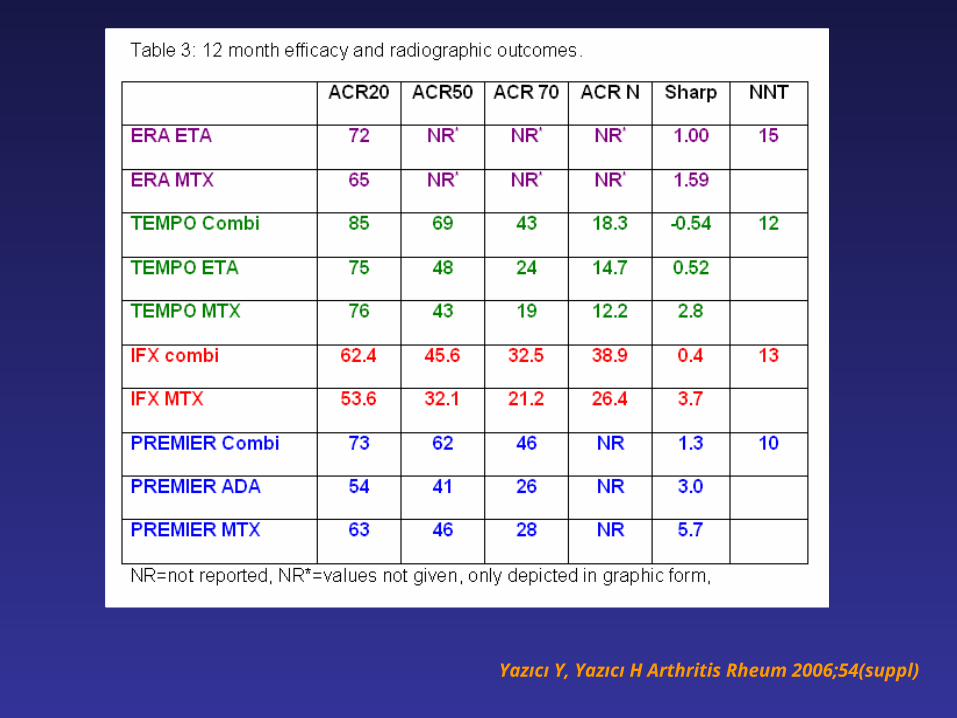
TNF Inhibitors: useful additional therapy to
Methotrexate in RA patients with severe disease
Only 3 (4?)/11 RCT’s with infliximab, etanercept and adalimumab were conducted among MTX naive patients.
Yazıcı Y, Yazıcı H Arthritis Rheum 2006;54(suppl)
Yazıcı Y, Yazıcı H Arthritis Rheum 2006;54(suppl)

1 1.59 -0.54 0.52 2.8 0.4 3.7 1.3 3 5.70
50
100
150
200
250
300
350
400
450
ERA ETA ERA MTX TEMPOCombi
TEMPO ETA TEMPO MTX IFX Combi IFX MTX PREMIERCombi
PREMIERADA
PREMIERMTX
Yazıcı Y, Yazıcı H Arthritis Rheum 2006;54(suppl)


• Equipose
• Informed consent
• Power calculations
• Intent to treat
• Delaying useful treatment
• Changing of authors
• No new information
Sins of Extension Studies

Equipose
In real hypothesis testing the likelihood of proving or disproving your hypothesis is approximately 50%.
Nihilistic view (JF Fries): RCT has probably became obsolete

Randomized Controlled Trials in BS
The Cerrahpaşa Experience • Colchicine 1980, Haematologica
• Azathioprin 1990, N Engl J Med
• Alpha Interferon 1991, Br J Rheumatol
• Azapropazone 1995, Clin Exp Rheumatol
• Cyclosporine 1997, Int J Dermatol
• Thalidomide 1998, Ann Intern Med
• Colchicine 2001, Arthritis Rheum
• Etanercept 2005, J Rheumatol
• Steroids 2006, Rheumatology (Oxford)

• Equipose
• Informed consent
• Power calculations
• Intent to treat
• Delaying useful treatment
• Changing of authors
• No new information
Sins of Extension Studies

Why can RCT be problemetic when looking for both
Safety & Efficacy • Short duration
• Limited number of patients enrolled
• Big differences (including other
medications used) between the
patients enrolled in a trial and
seen in real practice!

RA Patients in Real Lifefulfilling the entrance criteria to a major RCT (ATTRACT, Lancet
1999)
Sokka et al: 42/229 (18.3%)
Gogus et al: 9/155 (6.0%)
Sokka T et al: J Rheumatol 2003Göğüş F et al Clin Exp Rheumatol 2005


Merck Co., press releaseSeptember 4, 2004
“Merck has always believed that prospective, randomized, controlled clinical trials are the best way to evaluate the safety of medicines. APPROVe is precisely this type of study—and it has provided us with new data on the cardiovascular profile of VIOXX.”
Peter S. Kim, Ph.D.
President of Merck Research Laboratories.

The RCT and Adverse Events
As a scientific tool the starting point of a RCT to study adverse events should be to falcify the hypothesis that the new drug tested does have more/serious adverse events when tested against conventional, “other” new or no therapy.
• When this hypothesis cannot be falcified only then the new treatment can be said not to have more adverse effects compared to other modalities.
• Such undertaking would clearly be undesirable for “deeper socieatal” concerns.
K. Popper
Adverse Events
The Time Element


....I think this is rather misleading. Of the 26 lymphomas they refer to in the main text, 14 occurred within 2 months of TNF antagonist use. Thus, a more realistic comparator would be a deduced (from the annual rates) 2-month incidence of lymphoma in the general population....
H Yazici Arthritis Rheum 2003

Time to Adverse Effects A survey of inclusion of the time element when reporting adverse effects in randomized controlled trials of cyclooxygease-2 and tumor necrosis factor alpha inhibitors
Arthritis and Rheum
Ann Rheum Dis
Rheumatology
J Rheumatol
Clin Exp Rheumatol
N Engl J Med
JAMA
Lancet
Ann Intern Med
Am J Med
Arch Intern Med
Y Yazici and H Yazici Ann Rheum Dis, in print

Time to Adverse Effects
Drug COX-2
(n=26)
TNF-α
(n=44)
Total
(n=70)
Number of patients
mean; median; range
1541
601; 67-8076
216
42; 20-1049
Number of publications giving time to AE (%) 6 (23) 17 (39) 23(33) Number of publications giving time to serious AE (%)
3 (12) 9 (20) 12 (17)
Annual incidence used as a comparator (%) 0 8 (18) 8 (11)
Use of patient – years (%) 2 (8) 4 (9) 6 (9)
Y Yazici and H Yazici Ann Rheum Dis, in e. print

www.fda.gov/cder/guidance/3580fnl.pdf

Most applicants will construct adverse event tables by compiling and presenting the numbers and/or percentages of patients experiencing an adverse event in a study (or the absolute number of adverse events experienced in a group), without regard to the duration of treatment received. This is often satisfactory for relatively short-term studies. If studies of significantly different durations are pooled, however, or if there is a different discontinuation rate in the treatment arms and the risk of the adverse reaction persists over time, one must consider these durations to understand the real occurrence rate that patients will experience. One way to deal with the problem of different durations is to use the total person-time exposure for each treatment group and calculate the rate of the adverse event per period of exposure (# of patients with adverse event total person-time exposure), rather than the risk (# of patients with adverse event total number of patients).

This is particularly useful for the more important adverse reactions and reactions that occur at a fairly constant rate over time, but the person-time approach can also be used when the hazard rate changes over time. In this case, however, the observation period must be broken into component periods (e.g., evaluating person-time rates for each treatment for month 1, month 2, ....).
If concurrently controlled data are unavailable, overall rates from well-monitored, single-arm databases can be used to provide some indication of rates that were observed in treated patients, but there is little ability to establish causality except insofar as reactions are predicted by the known pharmacology of the drug.
For the most part, attributions of causality by the investigators should be discounted, and adverse events should be assessed without regard to attribution.

Explorations for dose dependency. These are important. The reviewer should ordinarily rely on fixed dose studies, as titration studies tend to show that those who tolerate higher doses have lower adverse reaction rates, but in some cases titration studies may show a clearly increased rate of adverse reactions with dose. It may also be useful to evaluate safety as a function of weight-adjusted dose, body surface-adjusted dose, or cumulative dose. Dose increases may be associated with adverse reactions or the severity of adverse reactions.
For events that occur commonly, explorations of time to onset for common, troublesome events (e.g., somnolence, nausea) explorations of adaptation to develop information on the time course of, and tolerance for, such events …..

7.1.6 Less Common Adverse Events
• In general, a fairly large database is needed to evaluate less common adverse events. To identify relatively rare events of significant concern, the reviewer has to examine the occurrence of adverse events over the entire phase 2 to 3 database, including data for which there is no useful concurrent control. The overall database is typically heterogeneous, including uncontrolled exposure for varying durations and at varying doses, and is unlikely to lend itself to meaningful estimates of rates or assessment of causality (except where there has been rechallenge). Thus, it may be sufficient for the reviewer to group these data in gross categories of incidence and by body system. For example, it may be useful to categorize less common events in order of decreasing frequency within the following incidence ranges:
• Adverse events occurring at rates less than or equal to 1/100
• Adverse events estimated to occur at rates between 1/100 and 1/1000
• Adverse events estimated to occur at rates less than 1/1000

The review should also provide overall conclusions about the safety of the drug, including:
• Overall assessment of the available safety information, referring both to what it has shown and its adequacy
• The limitations of the available data • Additional information needed, including both
further analyses and additional studies. • Comparison, to the extent possible, of the safety
of the drug under review to the safety of other available products, and the basis for that comparison (direct comparative data vs. clinical opinion)
• Whether a risk management program (beyond labeling) is needed and why
• Analysis of likely uses beyond labeling, (e.g., in more severe patients, in other diseases, in children)
• Whether there is a need for postmarketing safety studies

For the most part, attributions of causality by the investigators should be discounted, and adverse events should be assessed without regard to attribution. Also, in general, tables should give rates for all severities of a given effect, although in some cases (notably cytotoxic drugs), it is important to distinguish more and less severe reactions, as the former may be therapy-limiting or may affect the overall benefit-risk conclusion for the drug. For events with high background rates (e.g., headache, fatigue, and other events that occur frequently independent of drug therapy), however, display of all reported events can result in a high event rate that obscures drug-relatedness. This can be a particular problem when time on drug is prolonged. For example, it is common for studies of 4 to 6 weeks duration to report headache at a high (20 to 25 percent) rate. In that case, considering the severity or causality assessment of such events may allow a better assessment (e.g., if severe headaches are found only in the drug-treated group). Events that are more severe and for which subjects have multiple occurrences while on drug therapy are more likely drug-related. In determining incidence, however, both single occurrence and multiple occurrence events should be counted as one event.

Time to onset of Adverse Events Strom BL ed. Pharmacoepidemiology,2000

Criteria for the casual nature of an
association 1. Plausibility
2. Consistency
3. Time sequence
4. Specificity
5. Strength a. Quantitative b. Dose-response c. Study design
Strom BL ed. Pharmacoepidemiology,2000
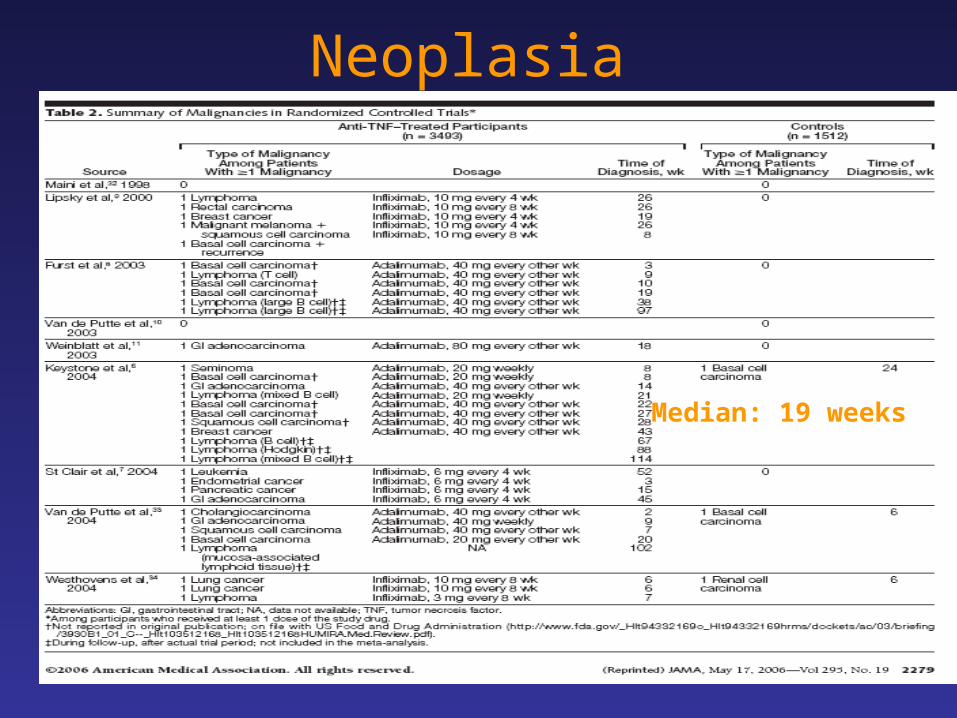
Neoplasia
Median: 19 weeks

0
2
4
6
8
10
12
14
0-12 13-24 25-36 37-48 49-60 61-72 72+Weeks
Num
ber
wit
h n
eopla
sia
nTime to Neoplasia
Based on T Bongartz et al JAMA 2006

Tumor necrosis factor-α antagonist use and cancer in patients with rheumatoid arthritis
Arhritis Rheum 2006
The tumor necrosis factor (TNF ) antagonists, a type of biologic DMARD with profound immunoregulatory effects, have had a significant impact on the treatment of RA. However, safety concerns regarding these drugs arose after the Food and Drug Administration's postmarketing spontaneous adverse event reporting system (MedWatch) received reports of lymphoma. Brown et al reviewed MedWatch reports of 26 cases of lymphoproliferative disorders that occurred following treatment with either of 2 TNF antagonists, etanercept or infliximab. The extrapolated crude incidence of lymphoproliferative disorders was 19.9 per 100,000 person-years for etanercept and 6.6 per 100,000 person-years for infliximab (16). Although these rates were smaller than that in the general population, features of the cases were of concern: in 54% of the patients who developed lymphoma, it was detected within 8 weeks after initiation of TNF antagonist treatment, and in 2 of these patients, it remitted after cessation of TNF antagonist treatment.
Tumor necrosis factor-α antagonist use and cancer in patients with rheumatoid arthritis
Arhritis Rheum 2006
DMARD exposure and potential confounders.
All patients included in the study had been prescribed a biologic DMARD (etanercept, infliximab, adalimumab, or anakinra) or MTX. Cohort followup started at the time of the first prescription of a biologic DMARD or MTX during the study period. Some patients contributed person-time to multiple exposure categories. Patients who were receiving both a biologic DMARD and MTX at the same time were categorized as biologic DMARD users. We assumed that the effect of the biologic DMARDs persists from the initiation of its use until the end of followup, testing the hypothesis that the effect of these agents on cancer is both profound and long term (16). In a secondary analysis, we assumed a 180-day induction period and excluded that period from the followup time.

Drug DevelopmentNew Approaches
●Personalized medicines
●Bayesian approach
●Extrapolation of efficacy
J Woodcock Clinical Trials 2005

“It is timely and healthy to question the real value of the controlled clinical trial as the ultimate guide for evidence based practice of medicine. Sometimes, however, it is not the “controlled clinical trial”, but its interpretation that needs to be put on trial.”
H Yazici J Rheumatol 2004