the rationale for 2 drug art - acthiv
TRANSCRIPT

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
TheRationalefor2DrugART
Babafemi Taiwo,MBBSGeneStollerman ProfessorofMedicine,InfectiousDisease
Chief,DivisionofInfectiousDiseasesNorthwesternUniversityFeinbergSchoolofMedicine
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Disclosure• Dr.TaiwohasservedasapaidconsultanttoViiV Healthcare/GlaxoSmithKline,GileadandJanssen,andreceivedresearchfundingthroughNorthwesternUniversityfromViiV/GlaxoSmithKline.
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
EvolvingARTGoals
�SaveLives
�Immunerestoration�Durableviralsuppression�End-organoutcomes
�Long-termsuccess�Healthyaging�Qualityoflife

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
WHATISSUCCESFULART?S=sminusc
S=Successs=suppressionwithoutresistancec=costs(e.g.,toxicity/adverseevents,QOL,andfinancial)
Ø HIVisproneto“overtreatment”Ø AnyunnecessaryARVaddstothe“cost”
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Cantwo-drugdual-siteregimensprovidesimilarefficacybutbetterlong-termsafety,costand
druginteractionprofile?
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
DHHSGuidelinesforARTalreadyincludedualregimens
VIROLOGICALLYSUPPRESSEDINDIVIDUALS

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
2018DHHSGuidelines
“ThePanelalsonotesthat,traditionally,theGuidelineshaverecommendedstartingART-naivepatientsonaregimenconsistingofatleastthreeactivedrugs,severalstudieshavenownotedthatpersonswithHIVwhohavesustainedviralsuppressionwithnodrugresistancemaybemaintainedonregimensincludingonlytwoactivedrugs”
Panel on Antiretroviral Guidelines for Adults and Adolescents. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed March
2018
BT:Eventhisconservativescopecouldcover>50%ofPLWH
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
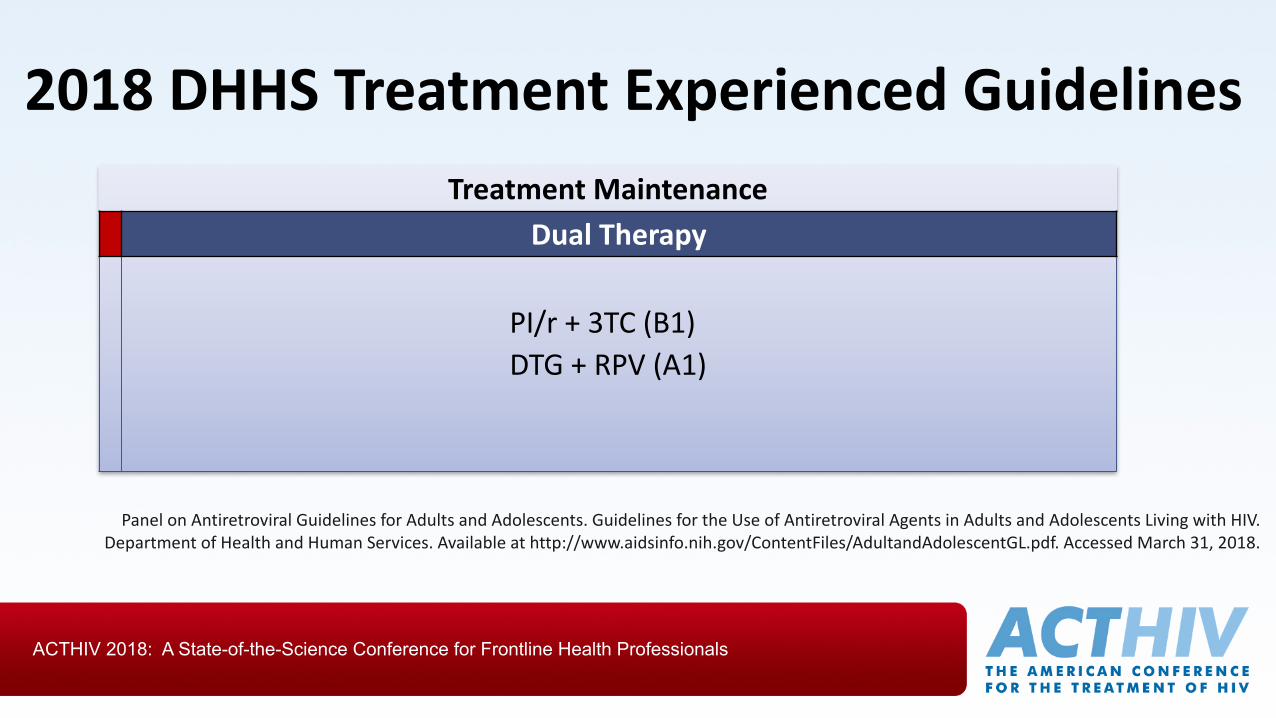
2018DHHSTreatmentExperiencedGuidelinesTreatmentMaintenance
DualTherapy
PI/r+3TC(B1)DTG+RPV(A1)
PanelonAntiretroviralGuidelinesforAdultsandAdolescents.GuidelinesfortheUseofAntiretroviralAgentsinAdultsandAdolescentsLivingwithHIV.DepartmentofHealthandHumanServices.Availableathttp://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.AccessedMarch31,2018.

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Somerecentcomparativetrialsof2versus3drugARTintreatmentnaïveandsuppressedPLWH
89% 88.3% 91.5%
84% 89.5% 89%
93%
83.7% 90.9%
78% 79.7%
93%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DRV/RTV+RAL LPV/RTV+3TC LPV/RTV+3TC ATV/RTV+3TC ATV/RTV+3TC DRV/RTV+3TC
NEAT GARDEL OLE SALT ATLAS DUAL-GESIDA
NAÏVE TREATMENTEXPERIENCED
2DR3DR
1 2
1
53 4 6
See slide notes for references

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
MaintenanceDolutegravir +Rilpivirine (SWORD)SnapshotoutcomesatWeek48(pooled)
• Dolutegravir+rilpivirine wasnon-inferiortostandardART
• NoINSTItreatment-emergentresistanceineitherarm
• Aparticipantondolutegravir +rilpivirinehadvirologic reboundwithK101K/E,andre-suppressedwithimprovedadherence
0
20
40
60
80
100
Virologicsuccess
Virologicnon-response
Novirologicdata
HIV
-1 R
NA
<50
c/m
L, %
DTG+RPV(n=513)CAR(n=511)
95 95
<1 15 4
Llibre JM, et al. 24th CROI. Seattle, 2017. Abstract 44LB.
Adjusted Treatment difference: -0.2% (95% CI:-3.0%-2.5%

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
LATTE2(LACABOTEGRAVIR+RPV)Wk 96
Ø ATLAS, FLAIR, ATLAS 2M
94
4 2
87
0
13
84
2
14
0
20
40
60
80
100
Virologicsuccess
Virologicnonresponse
No virologicdata
HIV
-1 R
NA
<50
c/m
L, %
CAB+RPVLAQ8W(n=115)
CAB+RPVLAQ4W(n=115)
CAB+NRTIsPO(n=56)
Margolis DA, et al. Lancet.2017;390(10101):1499-1510
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
CD4 BINDING
CO-RECEPTOR BINDING
FUSIONBUDDING
HIVViron
gp120
CD4
Assembly
Translation
Viral RNAs
Transcription
Proviral DNA
Reverse transcriptionof viral RNA genome
Integration
ChemokineCo-receptor(CCR5 orCXCR4)
ssRN
MATURATION
NEW HIV VIRON
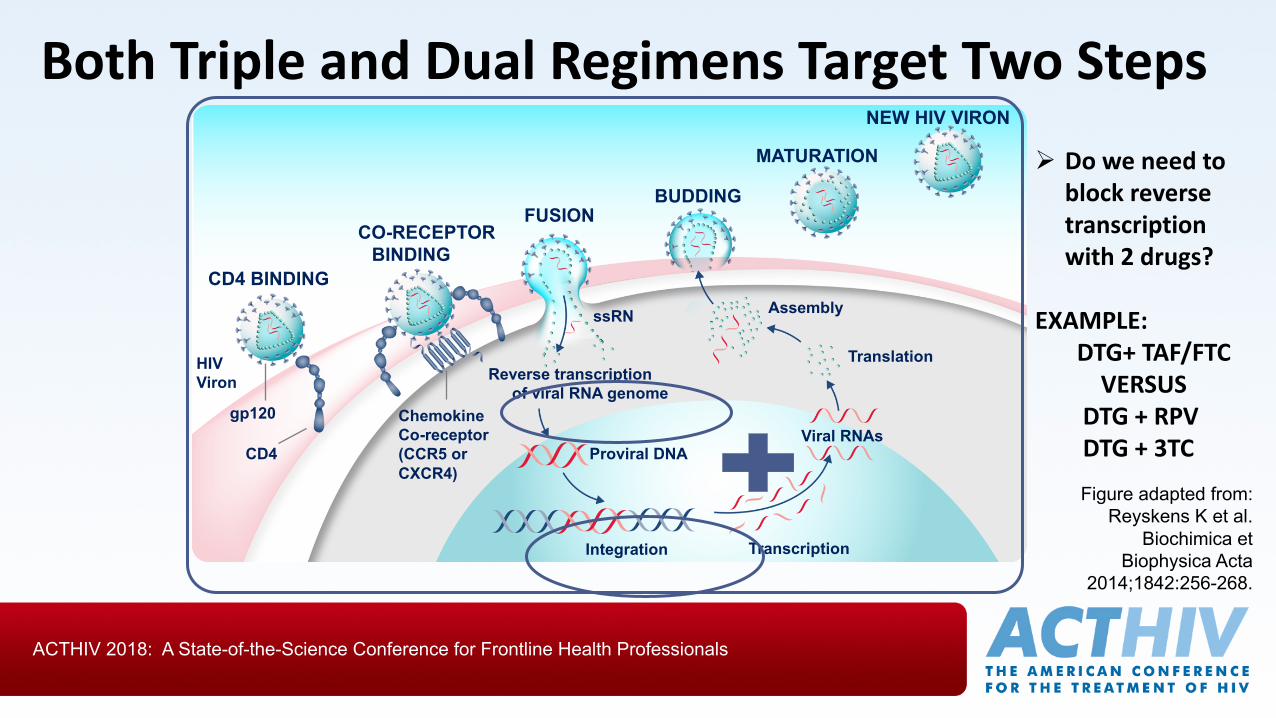
BothTripleandDualRegimensTargetTwoSteps
Figure adapted from: Reyskens K et al.
Biochimica et Biophysica Acta
2014;1842:256-268.
Ø Doweneedtoblockreversetranscriptionwith2drugs?
EXAMPLE:DTG+TAF/FTCVERSUS
DTG+RPVDTG+3TC
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
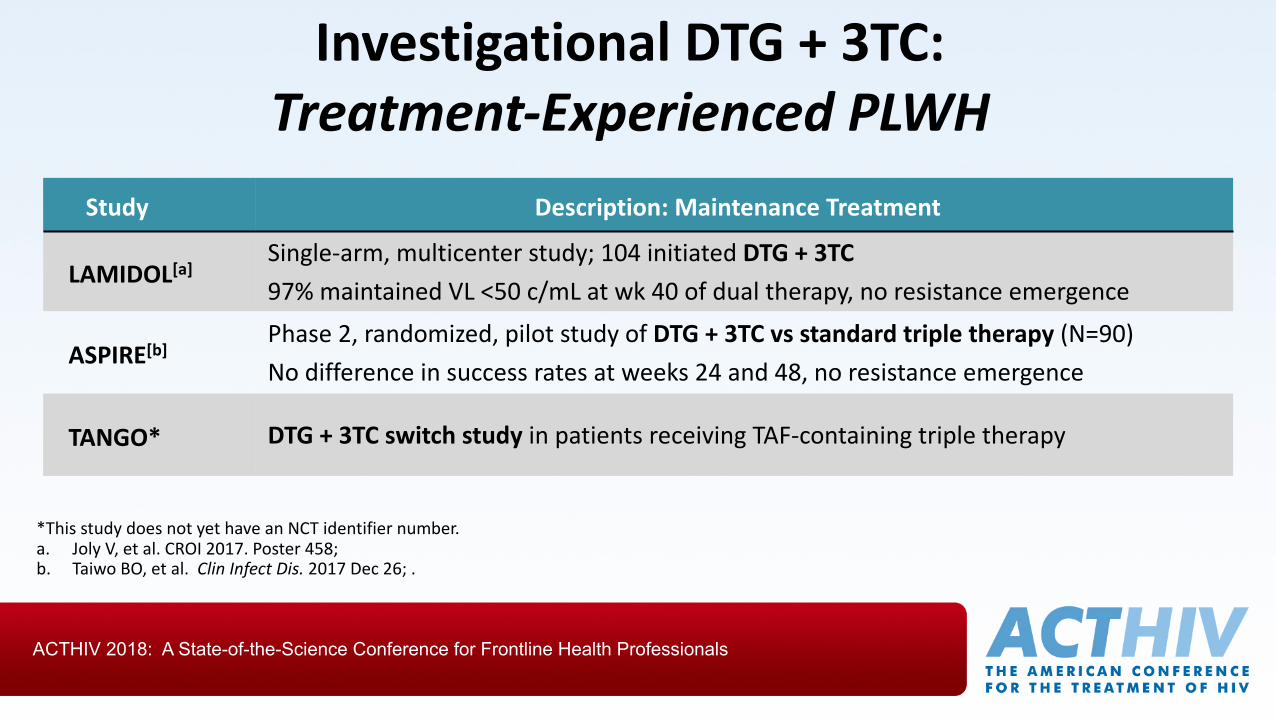
*ThisstudydoesnotyethaveanNCTidentifiernumber.a. JolyV,etal.CROI2017.Poster458;b. Taiwo BO,etal. ClinInfectDis.2017Dec26;.
InvestigationalDTG+3TC:Treatment-ExperiencedPLWH
Study Description: MaintenanceTreatment
LAMIDOL[a]Single-arm,multicenterstudy;104initiatedDTG+3TC97%maintainedVL<50c/mLatwk 40ofdualtherapy,noresistanceemergence
ASPIRE[b]Phase2,randomized,pilotstudyofDTG+3TCvsstandard tripletherapy(N=90)No differenceinsuccessratesatweeks24and48,noresistanceemergence
TANGO* DTG+3TCswitchstudyinpatientsreceivingTAF-containingtripletherapy
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
DHHSGuidelinesforARTalreadyincludedualregimens
TREATMENTNAÏVEINDIVIDUALS
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
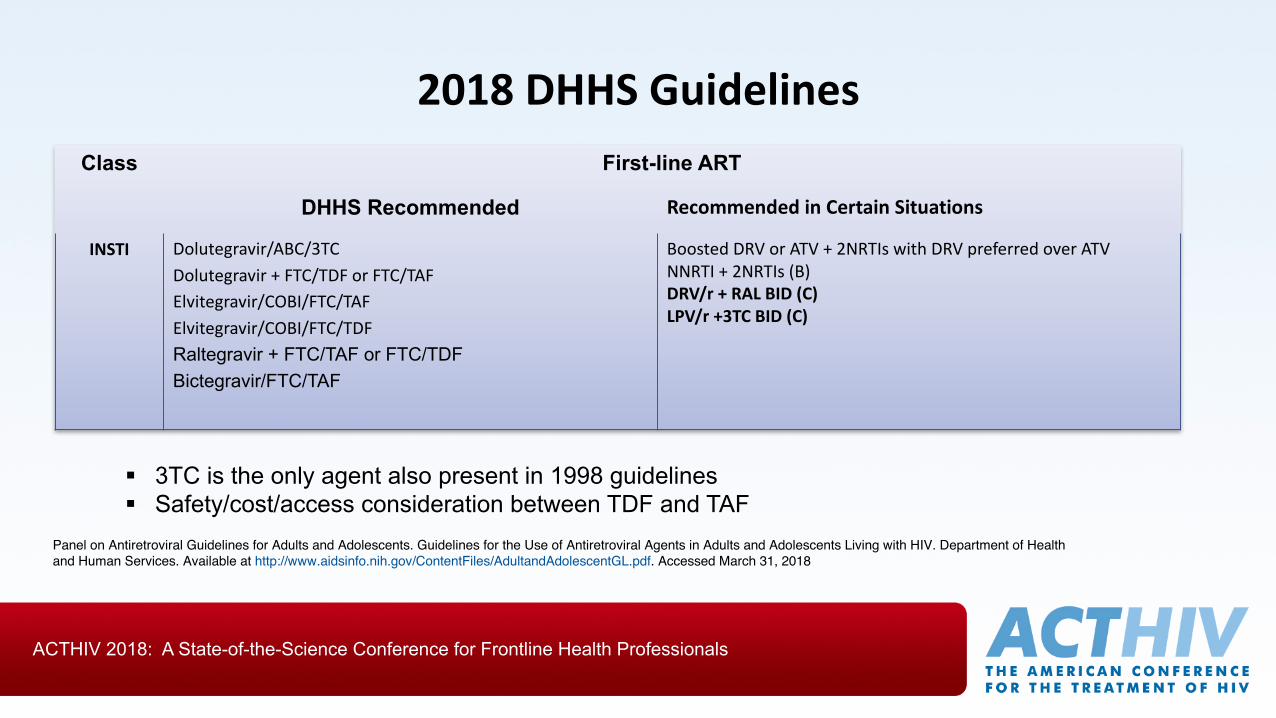
2018DHHSGuidelinesClass First-line ART
DHHS Recommended RecommendedinCertainSituations
INSTI Dolutegravir/ABC/3TCDolutegravir+FTC/TDForFTC/TAFElvitegravir/COBI/FTC/TAFElvitegravir/COBI/FTC/TDFRaltegravir + FTC/TAF or FTC/TDFBictegravir/FTC/TAF
BoostedDRV orATV +2NRTIs withDRVpreferredoverATVNNRTI +2NRTIs(B)DRV/r+RAL BID(C)LPV/r+3TCBID(C)
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV. Department of Health and Human Services. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed March 31, 2018
§ 3TC is the only agent also present in 1998 guidelines§ Safety/cost/access consideration between TDF and TAF
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
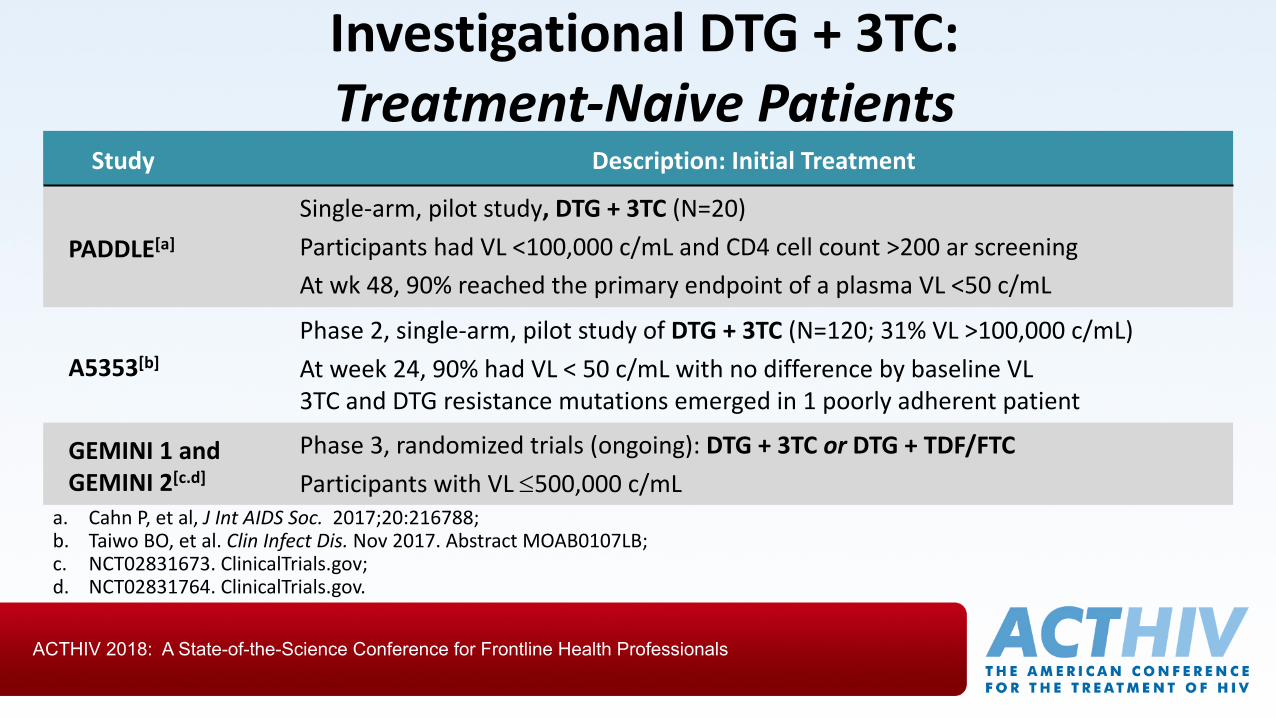
a. CahnP,etal,JIntAIDSSoc. 2017;20:216788;b. Taiwo BO,etal.Clin InfectDis.Nov2017.AbstractMOAB0107LB;c. NCT02831673.ClinicalTrials.gov;d. NCT02831764.ClinicalTrials.gov.
InvestigationalDTG+3TC:Treatment-NaivePatients
Study Description: InitialTreatment
PADDLE[a]Single-arm,pilotstudy,DTG+3TC(N=20)ParticipantshadVL<100,000c/mLandCD4cellcount>200ar screeningAtwk48,90%reachedtheprimaryendpointofaplasmaVL<50c/mL
A5353[b]Phase2,single-arm,pilotstudyofDTG+3TC(N=120;31%VL>100,000c/mL)Atweek24,90%hadVL<50c/mLwithnodifferencebybaselineVL3TCandDTGresistancemutationsemergedin1poorlyadherentpatient
GEMINI1andGEMINI2[c.d]
Phase3,randomized trials (ongoing):DTG+3TCor DTG+TDF/FTCParticipantswithVL£500,000c/mL

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
DRV/r/3TCFDCforHIV-1Treatment-NaivePatients:Week48ResultsoftheANDESStudy
• 145randomized• 1patientVFatw48onTT• NodifferenceinCD4count(~200cells
increase)• LDLandTriglyceridesnon-significanttrendin
favorofTT• AEdiscontinuationsimilarbetweenarms
Endpoint DualTherapy
TripleTherapy
ITT 93% 94%ITTifVL>100K(24%)
91% 92%
Per Protocol 100% 99%Grade2-4AE(28pts)
11 17
María I.Figueroa etal.CROI2018

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Whatisthefutureofdualtherapyinguidelinesandinreality?

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
PLWHAreOlder
Centers for Disease Control and Prevention. HIV Surveillance Report, 2015; vol. 27. http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Published November 2016. Accessed [21Dec2017].
17% ≥50 years
≈50% ≥50 years

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
ARVDrugsMayIncreasetheRiskofComorbiditiesARVAgent Potentialrisk
Tenofovir Disoproxil Fumarate Renal/bone
Tenofovir Alafenamide ?Exemplifies “overtreatment”
Boosted Pis Possible dyslipidemia/cardiovascularrisk/BOOSTER
Atazanavir Treatment-limitingjaundice
Dolutegravir ?Insomnia
Efavirenz CNS adverseeffects
Abacavir Cardiovascularrisk
Ritonavir orCobicistat Drug-drug interactions
NounnecessaryARVmedicationissafe
FinancialandothercostsaccumulateoverdecadesofART
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
ClinicalInfectiousDiseases®2016;62(6):784–91
• With50%uptakeof2-drugsforART-naïvepatients,costsavingstotaled$800million,within5years
• Savingsreached>$3billionif25%ofcurrentlysuppressedpatientswereswitchedtoDTG+3TCmaintenance.

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
TopReasonsCitedinSupportofTripleTherapy
1. Hep Bco-infection–contraindicationUNLESSENTECAVIRisadded2. TAFissosafe,it’sanobrainer3. Compartmentsconcerns4. Failure/resistancefear5. Experiencewithtripletherapy Experience:Repeatingthe
samemistakewithincreasedconfidence

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
FirstDHHSGuidelines(1998)
Recommended Antiretroviral Agents for Treatment of Established HIV Infection
Preferred Strong evidence of clinical benefit and/or sustained suppression of plasma viral load. Once choice each from column A and column B. Drugs are listed in random, not priority, order:
Column AIndinavir (AI)Nelfinavir (AII)Ritonavir (AI)Saquinavir – SGC* (AII)Ritonavir + Saquinavir SGC or HGC** (BII)Efavirenz (AII)
Column BZDV +ddI (AI)d4T + ddI (AII)ZDV + ddC (AI)ZDV + 3TC† (AI)d4T + 3TC† (AII)
DHHS https://aidsinfo.nih.gov/contentfiles/adultandadolescentgl12011998012.pdf Accessed December 21, 2017,
†optional use is in 3-drug antiretroviral combinations that reduce viral load to undetectable levels.
THE HIV FIELD HAS A TRADITION OF EVIDENCE-DRIVEN PROGRESS

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Isitpossiblethatthemajorityof patients donotneed3drugsforover95%oftheir
treatmentlife?

ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
Acknowledgments
• ChicagoAIDSClinicalTrialsUnit• VolunteerPLWH• JudithAberg