the rh blood group brian poirier, md ucdavis medical center 1
TRANSCRIPT

The Rh Blood Group
Brian Poirier, MD
UCDavis Medical Center
1

Topics
• Terminology systems
• Rh antibodies
• Consequences of Rh incompatibility
• Unusual phenotypes
2

Objectives
• Explain the derivation of the term Rh
• Differentiate Rh from LW
• Compare and convert the major genotypes among Fisher-Race, Wiener, and Rosenfield terminologies
• Define the basic biochemical structure of Rh
3
Objectives (Continued)
• Describe and differentiate three mechanisms that result in weak D expression on rbcs
• Describe 3 characteristics of Rh antibodies
• Describe how to prevent Rh D immunization
4

5

Rh Blood Group
• Second most important blood group (after ABO)
6

History of the Rh System
• 1939 Levine described a HTR in an OB patient:– After delivery of a still born infant, a woman
required transfusions. – After receiving her husband’s blood (ABO
compatible), she demonstrated the acute HTR.
– An antibody was isolated from mom’s serum that reacted both at 37 C and 20 C with father’s rbcs.
7

8
History of the Rh System (continued)

History of the Rh System (continued)
• 1940 Landsteiner and Wiener reported:– An antibody made by guinea pigs and rabbits
when they were transfused with rhesus monkey rbcs.
– The antibody agglutinated 85% of human rbcs, was named “Rh.”
– The antibody was renamed as anti-LW (Landsteiner and Wiener).
– The name Rh was retained for human-produced antibody.
9

Nomenclatures of the Rh system
• Fisher-Race: The DCE Terminology
• Wiener (Rh-Hr): The Rh-Hr Terminology
• Rosenfield: Alpha/Numeric Terminology
• ISBT (International Society of Blood Transfusion): Numeric Terminology
10

Fisher-Race (DCE or CDE)
• 5 major antigens: D, C, E, c, e– Rh positive really means D positive.– Absence of D designated “d” (later found not
to be a real antigen- an “amorph”).
• 8 potential haplotypes named based on presence of genes for above antigens (eg, Dce, dce).
11
Wiener (Rh-Hr)
• Different names for the 5 main antigens– Rho=D– rh’=C– rh”=E– hr’=c– hr”=e
12

Wiener (Rh-Hr) (continued)
• Gave shorthand names to the 8 potential combinations alluded to above; still in use
R1=DCe r’=dCe
R2=DcE r”=dcE
Ro=Dce r=dce
Rz=DCE ry=dCE
13

Converting Wiener (Rh-Hr) to Fisher-Race
Fisher-Race terminology is easier to use:
• R=D, r=d
• 1 or prime=C
• 2 or double prime=E
• 0 or blank=ce
• any superscript letter =CE
14

Rosenfield Terminology (alpha/numeric)
• Rosenfield system has no genetic basis, only demonstrates the presence or absence of the antigen on the red cells.
• A minus sign preceding a number designates absence of the antigen. The absence of the number indicates the antigen has not been typed.
15

Rosenfield Terminology (Continued)
• D is assigned Rh1; C is assigned Rh2; E is assigned Rh3; c is assigned Rh4; e is assigned Rh5
• Example 1: D+ C- E+ c+ e+ would be: Rh: 1, -2, 3, 4, 5
• Example 2: DCe/dcE would be: Rh: 1, 2, 3, 4, 5
16
ISBT Terminology
• ISBT adopted a six-digit number for each blood goup specificiy.
• First 3 numbers represent the system and the remaining 3 the antigen specificity.
• 004 was assigned to the Rh blood group system; each antigen assigned to the Rh system was given a unique number to complete the 6-digit computer number.
• Example: “D” antigen would be “004001”
17

“The Big Four Rh Phenotypes
• R1, R2, R0, and r are most frequently encountered phenotypes.
• R0 most common in blacks, least common in whites.
• R1> R2
• r is always second in frequency
• Whites: R1 > r > R2 > R0
• Blacks: R0 > r > R1 > R2
18
Gene Frequency of Rh Antigens
Gene Frequency %
D 85
d 15
C 70
E 30
c 80
e 9819
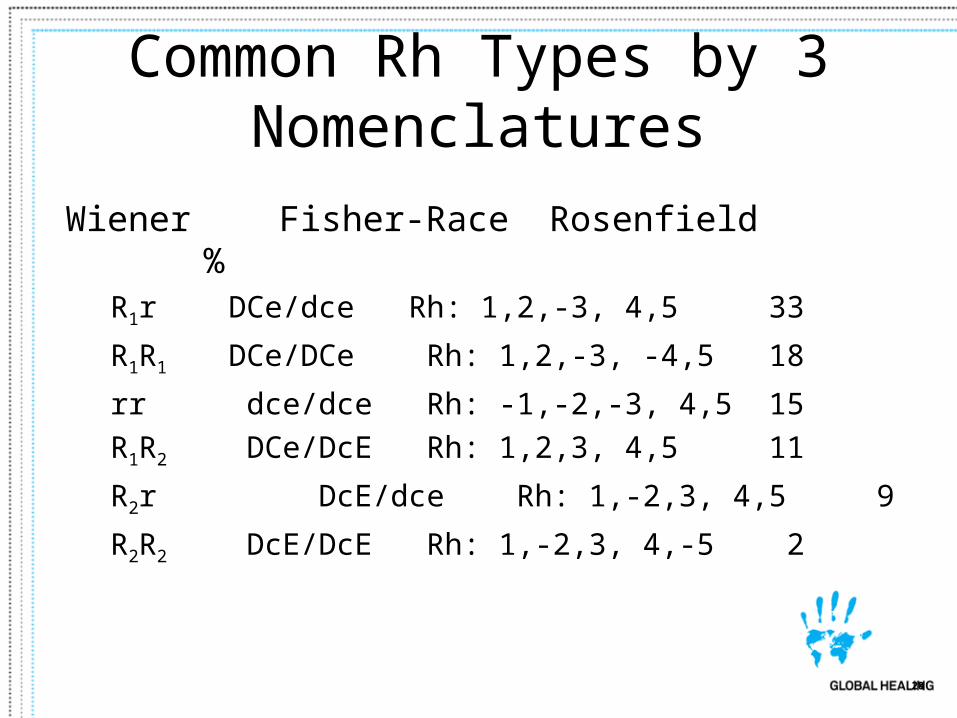
Common Rh Types by 3 Nomenclatures
Wiener Fisher-Race Rosenfield %R1r DCe/dce Rh: 1,2,-3, 4,5
33
R1R1 DCe/DCe Rh: 1,2,-3, -4,5 18
rr dce/dce Rh: -1,-2,-3, 4,5 15
R1R2 DCe/DcE Rh: 1,2,3, 4,5 11
R2r DcE/dce Rh: 1,-2,3, 4,5 9
R2R2 DcE/DcE Rh: 1,-2,3, 4,-5 2
20
Rh Antigens
• Non-glycosylated proteins in the red cell membrane.
• Inherited as codominant alleles.• Are transmembrane polypeptides and are an
integral part of the red cell membrane.• All Rh antigens (D,C,E) are very similar; differ
by only 44 base pair.• C and c differ in 4 a.a.• E and e differ in 1 a.a.
21

22
Rh Antigens
Hillyer et al 2009

Rh Antigens (continued)
• Rh antigens are highly immunogenic:D > c > E > C > e
• The D antigen is the most immunogenic antigen outside the ABO system.
• As little as 0.5 ml will elicit anti-D allo-immunization in healthy volunteers (Gunson et al 1970).
23
Rh Antibodies
• Do not bind complement
• Extravascular
• IgG
• Can cross placenta and cause HDFN
• HTR
• Exposure required (pregnancy or transfusion)
24
Consequences of Rh Incompatibility
• Unexposed: 80% of healthy D negative individuals make anti-D with one unit transfused. Approximately 22% of hospitalized (non-oncology) patients (Yazer et al 2007).
• Exposed: HTRs with extravascular hemolysis
• Most severe HDFN
25

Prevention of D Immunization:RhIgG
• Macro dose (300 g): protect against 30 mL of WB or 15 mL of packed RBCs
• Micro dose (50 g): protect against 5 mL of WB; sufficient for abortion, amniocentesis, and ectopic rupture at up to 12 weeks gestation
26

27

Unusual Rh Phenotypes
• Weak D phenotype Du
• Rhnull phenotype
• Compound Rh antigens
28
Weak D phenotype (Du)• Some D positive individuals require AHG
phase to demonstrate D antigen• Reasons:
– C opposite chromosome to D (C in trans position): eg, Dce/dCe
– Genetic weak D (weakened D expression)– Partial D (“Mosaic”)
• (most prone to making anti-D)
29
Determination of D Status
• Donors: D neg donors must be confirmed by AHG test
• Recipients: D neg recipients do not need to be confirmed by AHG (though most are)
30

Rh antigen typing reagents
• Saline anti-D (IgM, can’t be used for Du)
• High protein anti-D (requiring Rh control)
• Chemically modified anti-D (low protein)
• Monoclonal anti-D
• Blend of Monoclonals (anti-IgM and anti-IgG anti-D)
31

Rhnull Phenotype
• Lacks all Rh antigens
• Rhnull syndrome demonstrates a mild compensated hemolytic anemia with stomatocytosis, spherocytosis and reticulocytosis
• Transfuse with Rhnull blood
• The clinical symptoms of Rhmod phenotype are less severe and rarely clinically remarkable.
32
Compound Rh Antigens
• f = antigen present when c and e are on the same chromosome
• G: G is present on most D pos and all C pos RBCs. Anti-G originally appeared to be anti-D+C; further investigation showed that anti-G was directed toward D+G.
33

The LW System
• LW antigens
• Anti- LW
34
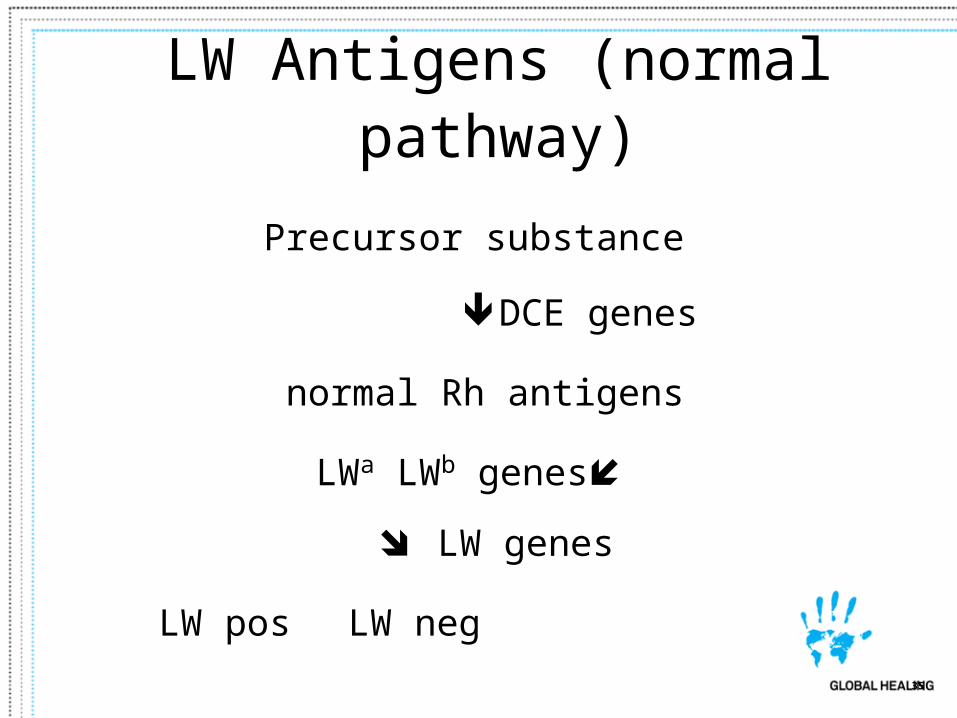
LW Antigens (normal pathway)
Precursor substance
DCE genes
normal Rh antigens
LWa LWb genes LW genes
LW pos LW neg
35

Anti- LW:
– Reacts strongly with most D pos rbcs.– Reacts weakly with D neg rbcs.
– No reaction with Rhnull rbcs.
– Reacts equally well with cord cells regardless of D typing.
– Rarely clinically significant.
36
Objectives
• Explain the derivation of the term Rh
• Differentiate Rh from LW
• Compare and convert the major genotypes among Fisher-Race, Wiener, and Rosenfield terminologies
• Define the basic biochemical structure of Rh
37

Objectives (Continued)
• Describe and differentiate three mechanisms that result in weak D expression on rbcs
• Describe 3 characteristics of Rh antibodies
• Describe how to prevent Rh D immunization
38

39

THANKS TO
• Rosemary Howard, CLS
• Dr Chris Gresens
40

References
• Transfusion Medicine and Hemostasis, Hillyer et al, 2009, Elsevier Pub.
• Yazer et al, (2007), Detection of anti-D in D- recipients transfused with D + red cells, Transfusion 47 2197-2201
• Avent ND, Reid (2000) The Rh blood group system: a review Blood 95 375-387.
• Gunson et al (1970) The Anti-Rh0(D) Responses of Immunized Volunteers following Repeated Antigenic Stimuli, BJH
41