the role of tranexamic acid in patient blood management ... · acid in patient blood management...
TRANSCRIPT

The Role of Tranexamic
Acid in Patient Blood
Management
Undergoing Cardiac
Surgery
Dr Sarah Armarego
FANZCA FANZCP
Senior Staff Specialist
John Hunter Hospital
Newcastle

Declaration
Former member of a medical advisory
committee for Pfizer for Tranexamic acid

Disclaimer
This presentation discusses pharmaceutical
products and/or use of products that may
have not been approved by the TGA.
Please consult the approved Product
Information before prescribing.

Tranexamic Acid
• Patient Blood Management in Cardiac Sx
• Role of Antifibrinolytics (TxA)
– Risks/Benefits
• How should we be giving TxA ?
– Pharmacokinetics
– Dose
– Timing

PBM
• The timely application of evidence based
medical and surgical concepts designed to
– Maintain Hb concentration
– Optimise haemostasis and
– Minimise blood loss
• In an effort to improve patient outcome • Society for the Advancement of Blood
Management

Importance
• Blood usage in cardiac surgery
– Blood bank data
– Audits
– ANZCTS database
• High
– > 50% to 90%
– Depending on operation
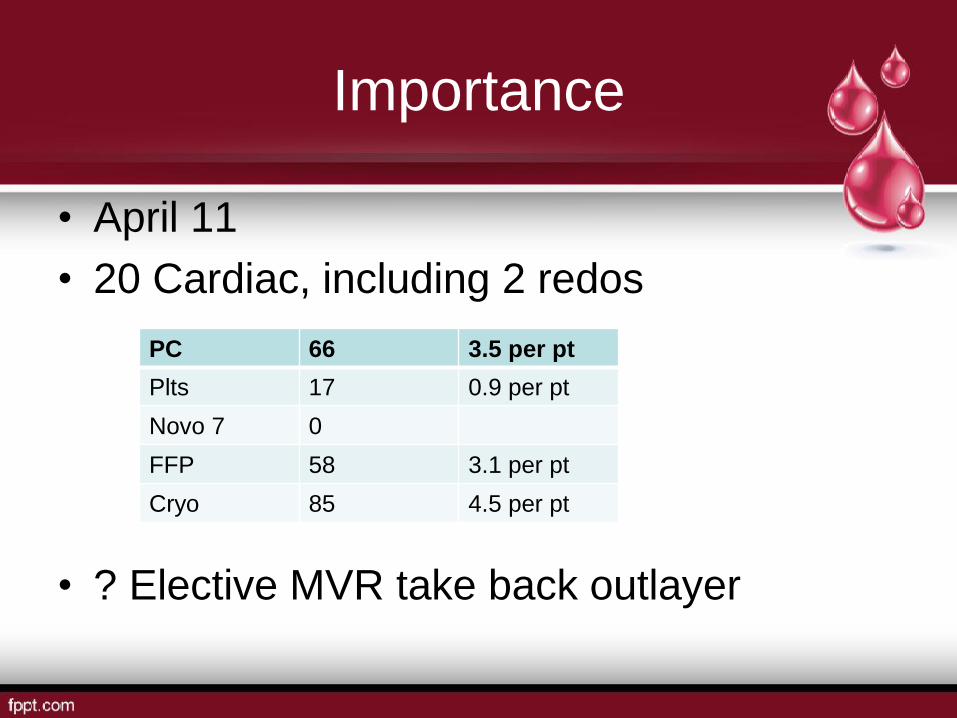
Importance
• April 11
• 20 Cardiac, including 2 redos
• ? Elective MVR take back outlayer
PC 66 3.5 per pt
Plts 17 0.9 per pt
Novo 7 0
FFP 58 3.1 per pt
Cryo 85 4.5 per pt

Importance
• NOT IN MY UNIT
– Transfusion rate low
intraoperative
– Transfusions occurring
ICU/postop

The 3 Pillars

Antifibrinolytics
• Maintain Hb concentration
– By reducing blood loss
• Optimise Haemostasis
– Preventing secondary fibrinolysis

Evidence
• Overwhelming number of
– Observational studies
– Prospective studies
– Meta-analyses – Cochrane and otherwise
• TxA v EACA v Aprotinin v Placebo

Evidence
• Decreased blood loss
• Decreased RBC transfusion
• Decreased other blood products (?)
• Decreased take-backs

Evidence
• ? Decreased Mortality
• ? Decreased Morbidity
• ? Decreased ventilator time
• ? Decreased LOS – ICU
• ? Decreased LOS - Hospital

Evidence
• BENEFITS
– Aprotinin > TXA ~ EACA
– MOA – antifibrinolytic and anti-inflammatory
• RISKS
– Aprotinin > TXA ~ EACA
– Non-cardiac mortality
– ? Why

BALL PARK FIGURES
• Cochrane Analysis
2011
– 252 RCT
– 25 000 participants
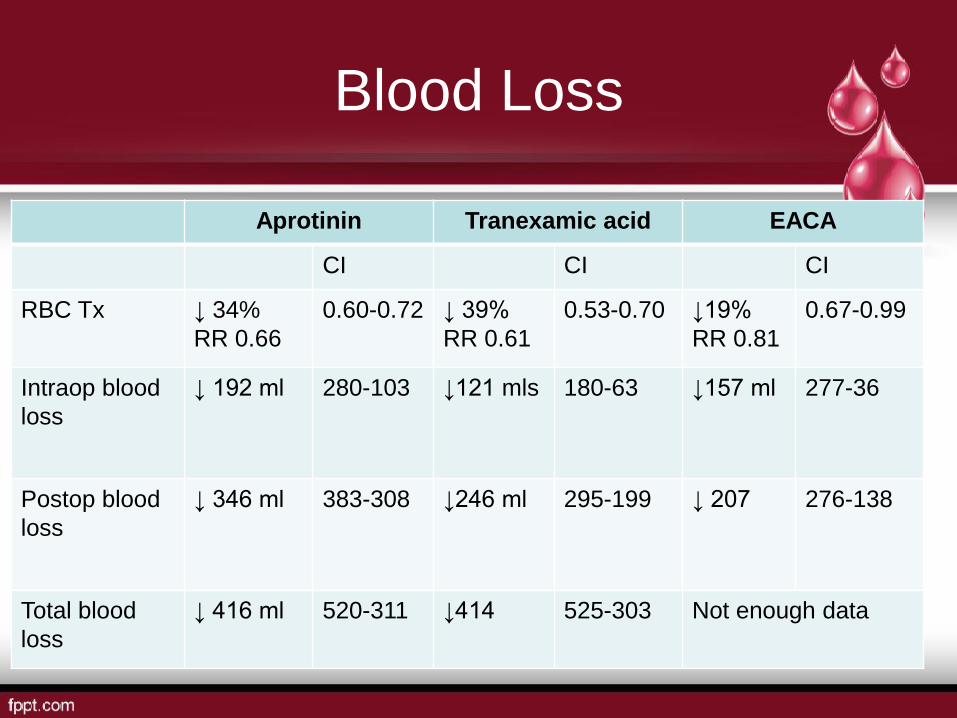
Blood Loss
Aprotinin Tranexamic acid EACA
CI CI CI
RBC Tx ↓ 34%
RR 0.66
0.60-0.72 ↓ 39%
RR 0.61
0.53-0.70 ↓19%
RR 0.81
0.67-0.99
Intraop blood
loss
↓ 192 ml 280-103 ↓121 mls
180-63 ↓157 ml 277-36
Postop blood
loss
↓ 346 ml 383-308 ↓246 ml
295-199 ↓ 207 276-138
Total blood
loss
↓ 416 ml 520-311 ↓414
525-303 Not enough data

Blood Loss
• Aprotinin Vs TxA
– Cardiac Sx
• ↓ Blood Tx RR 0.87 CI 0.76-0.99
– Combined Sx
• NS RR 0.9 CI 0.81-1.01
– Post op bleeding (cardiac)
• More effective MD -145.81 mls CI -209.99 to –
81.62

Re-op for Bleeding
RR CI 95%
Aprotinin ↓54% 0.46 0.34 – 0.62
Absolute risk reduction of 2% or NNT of 50
TxA No ↓ 0.80 0.55 – 1.17
EACA Trend to ↓ 0.32 0.11 – 0.99
Aprotinin V
TxA
↓ 0.69 0.51 – 0.93
Heavily weighted by BART (63%)

Risks - Aprotinin
Risk RR CI 95%
MI Nil 0.87 0.69-1.11
Renal Dysf Nil 1.10 0.79-1.54
Renal Dysf
Cardiac Sx
Trend but NS 1.07 0.76-1.15
Stroke Nil 0.82 0.44 – 1.52
LOS Nil reduction -0.25 days – 0.71 to 0.2 days
Mortality Nil 0.81 0.63 – 1.06

Risks - TxA
Risk RR CI 95%
MI Nil 0.79 0.41-1.52
Renal Dysf Nil 0.89 0.33-2.37
Stroke Nil 1.23 0.49-3.07
LOS Nil reduction -0.34 days – 0.82 to 0.13 days
Mortality Nil 0.6 0.33 – 1.10

Risks - EACA
Risk RR CI 95%
MI Nil 0.88 0.48 -1.63
Renal Dysf Nil 0.41 0.14-1.22
Stroke Nil 0.62 0.16-2.36
LOS Nil reduction 0.58 days – 3.17 to 4.33 d
Mortality Nil 0.6 0.33 – 1.10

Risks
• Aprotinin vs TxA and EACA
– MI - ↑NS
• RR 1.11, CI 0.82-1.50
– Mortality – ↑
• RR 0.1.39, CI 1.02-1.89
• Most data comes from BART

STUDY PROBLEMS
• Different dosing regimes
– Bolus +/- Infusion
– Pump prime +/-
– Adjustment for eGFR
– Length of infusion (up to
12h)

STUDY PROBLEMS
• PBM
– Cell savers
– Pleural drainage
reinfusion
– Transfusion triggers
– Pump volume
especially paeds
– Re-sternotomy def
– Change in PBM

STUDY PROBLEMS
• Look at benefits but not risks
– Prothrombotic risks
• MI
• Stroke
• DVT/PE
– Renal function
– Seizures
• Small numbers
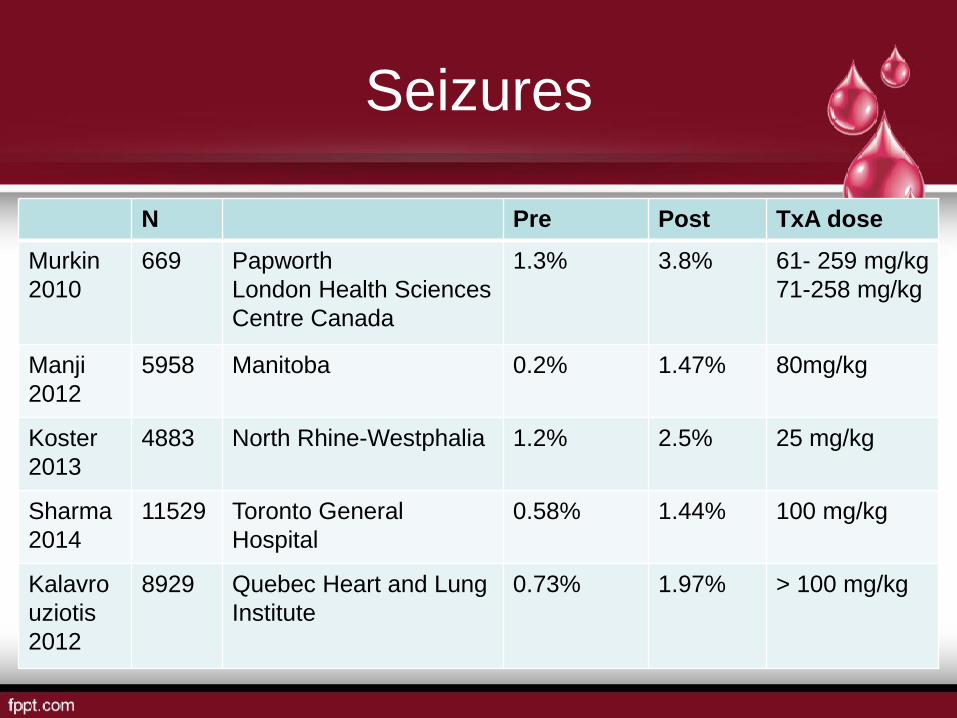
Seizures
N Pre Post TxA dose
Murkin
2010
669 Papworth
London Health Sciences
Centre Canada
1.3% 3.8% 61- 259 mg/kg
71-258 mg/kg
Manji
2012
5958 Manitoba 0.2% 1.47% 80mg/kg
Koster
2013
4883 North Rhine-Westphalia 1.2% 2.5% 25 mg/kg
Sharma
2014
11529
Toronto General
Hospital
0.58% 1.44% 100 mg/kg
Kalavro
uziotis
2012
8929 Quebec Heart and Lung
Institute
0.73% 1.97% > 100 mg/kg

Seizures
N OR 95% CI
Manji
2012
5958 7.4 2.8-19.3 P<0.001
Koster
2013
4883 2.10 1.29-3.41 P=0.003
Sharma
2014
11529
14.3 5.5-36.7 P<0.001
Kalavrouziotis
2012
8929 2.6 1.7-3.8 P < 0.0001

Seizure Characteristics
• Patient characteristics
– High and moderate dose TxA
– Most open heart
• (CPB)(more complicated ops)
– Older pts
– Renal dysf (dose adjustment/HF)
– More atheroma – Ao, PVD

Seizure Characteristics
• Seizures
– Grand Mal
– Occurring in ICU (observation effect)
– Coincident with sedation weaning
– No ass with new or old infarcts on CT/MRI

Seizure outcome
• ↑ Ventilation time
• ↑ICU stay
• ↑ Hospital stay
• ↑ Mort
– Koster 19% in open heart
– Sharma 2.5 x in hospital

Dose Effect
• Manji
– Post op seizure
• 0.3% having 50mg/kg
bolus only
• 2.6% when receiving
infusion (16 mg/kg/h)
– Cumulative effect
• Kalavrouziotis
– DRC

SEIZURE - Mechanism
• Structural analogue of
glycine
– A major inhibitory NTM
in brain and SC
• Competitively inhibit
glycine R
Pro-convulsant effect
• Topical application to
neural tissue and high
iv doses

Lecker Studies
• TxA inhibits glycine currents when both
pre and co-applied with glycine
• TxA applied alone does not cause currents
and is therefore not a glycine R agonist
• TxA does not modulate glycine R
• TxA moves the glycine response curve to
the right without changing max response

Lecker Studies
• Onset of TxA inhibition was not channel
use dependent
• Recovery from blockade was reversed
immediately after TxA washout
• TxA inhibits GABAA R in brain and SC
• Propofol and isoflurane but not midazolam
attenuated TxA inhibition
• Propofol dose required is 3 x normal

Lecker Studies
• TxA applied to cortical slices evoke
epilepiform activity due to both glycine
inhibition and GABAA inhibition
• Serum and CSF TxA levels from pts
undergoing thoracoabdominal Ao repairs are
within range of causing seizures
• CSF peak levels occur after infusion
cessation
• Subunit variability
Seizures
Why some more than others
• Increased incidence in open heart =
breakdown of BBB
• Microemboli
• Increased permeability for TXA and toxic
cerebral TXA concentrations

GUIDELINES - ABA
RECOMMENDATIONS – medications (tranexamic acid)
• R17
• In adult patients undergoing cardiac surgery, the use
of intravenous tranexamic acid is recommended
(Grade A)
• Body of evidence can be trusted to guide practice
GUIDELINES Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists
• Drugs used for intraoperative blood Mx
– Lysine analogues – epsilon aminocaproic acid
(Amicar) and tranexamic acid (Cyklokapron) –
reduce total blood loss and decrease the
number of patients who require blood
transfusion during cardiac procedures and are
indicated for blood conservation
– Level I (A)

GUIDELINES European Society of Anesthesiology
• We recommend that Tranexamic acid or EACA
should be considered before CABG surgery 1A
• We recommend that intraoperative Tranexamic
acid or EACA administration should be
considered to reduce perioperative bleeding in
high-, medium – and low risk cardiovascular
surgery 1A
• We recommend the consideration of Tranexamic
acid (20-25 mg/kg) 1A

THE QUESTION IS NOT WHETHER TO GIVE
TxA BUT HOW MUCH?
BACKGROUND
Australia
• Synthesised by Okamoto in late 50’s
• First regulatory approval Jan 1966 Austria
• TGA approved oral formulation (72,84,87) • Hereditary angioneurotic odema
• Short term use for hyphaema
• Pts with established coagulopathies undergoing
minor Sx
• Menorrhagia

BACKGROUND
Australia
• Aprotinin removed from market by Bayer
in Nov 2007
• SAS use of IV Tranexamic acid increased
• TGA approached Pfizer for approval of IV
form Sept 2010

Background
• Adults
– For the reduction of peri- and post-operative
blood loss and the need for blood transfusion
in patients undergoing cardiac surgery or total
knee arthroplasty or total hip arthroplasty
• Children
– For the reduction of peri- and post-operative
blood loss and the need for blood transfusion
in patients undergoing cardiac surgery

BACKGROUND
• Problems
– A lot changes 50 years (bureaucracy)
– Animal data
– In vitro data
– Minimal PK studies in humans
– No after market surveillance

Dose - PI
• Adults
– 15 mg/kg bolus followed by 4.5mg/kg/h +/- 0.6
mg/kg of the infusion dose added to prime
• Paeds
• 10 mg/kg bolus followed by a rpt bolus of 10
mg/kg during surgery or as an infusion

BART TRAIL DOSE
• Dowd 2002
– 30 adults (CABG, Valve and ASD) divided into
50 mg/kg bolus, 100 mg/kg bolus and 10
mg/kg bolus followed by infusion of 1 mg/kg/h
for 10 hours
• Plasma concentration Vs time curves
• 2 compartmental model

Dowd
• Dosing regimes were
then calculated using
the PK data obtained
and assumptions
about required
plasma concentration
for inhibition of
fibrinolysis (in vitro)

Dowd
• In vitro tissue extracts (Andersson)
– Cp 100 mcg/ml (636 μM) reduce fibrinolytic
activity in tissue extracts by 98 – 100%
– Cp 10 mcg/ml (64 μM) reduce fibrinolytic
activity by 80%
– Cp 16 μg/ml suppresses plasmin-induced plt
activation
– Suggested target 20 - 150 μg/ml

Dowd
Load
Over 30 min
Infusion Prime Cp Inhibition
12 mg/kg 6.5 mg/kg/h 1 mg/kg > 345 μM > 80%
30 mg/kg 16 mg/kg/h 2 mg/kg > 800 μM > 90%

Harrow
• 1995 Pennsylvania
Load
mg/kg
Infusion
Mg/kg/h
N
RBC
5 d
Mean
Blood loss g
0 0 27 26% 552
2.5 0.25 24 38% 504
5 0.50 22 36% 386
10 1.0 21 29% 365
20 2.0 27 26% 344
40 4.0 27 26% 369

Harrow
• Placebo gp showed significant increase in
D dimers
• Dose-response wrt blood lost but not with
blood transfused
• Recommend 10 mg/kg bolus followed by 1
mg/kg/h

ADULTS
• Grassin-Delyle 2013 France
N Cp
Low dose 30 10 mg/kg bolus
1 mg/kg/h infusion
1 mg/kg CPB
(Harrow)
28-55 μg /ml
High dose 31 30 mg/kg
16 mg/kg/h
2 mg/kg CPB
(Dowd)
114-209 μg/ml Increasing
levels
(90%)

ADULTS
• Based on maintaining a plasma conc of
150 to 190 μg/ml
– 46 mg/kg given in one hour followed by an
infusion of
– 11 mg/kg/h in pts 50-75 kg
– 10 mg/kg/h in pts 75-100 kg
– 9 mg/kg/h in pts 100-125 kg

Adults
• Sigaut 2013
N Tx up
to 7 d
FFP Plt Blood loss Rpt
sternotomy
Low
dose
2
8
4
10 mg/kg bolus
1 mg/kg/h
infusion
1 mg/kg CPB
63% 26% 23% 820 +/-
50.7
6%
High
dose
2
8
5
30 mg/kg
16 mg/kg/h
2 mg/kg CPB
60% 18% 15% 590 +/-
50.4
2.5%
P=0.3 P=0.03 P=0.02 P=0.01 P=0.01

Children
• Grassin-Delyle 2013
• 12 M – 12 Y
• Stratified into 3 gps according to weight
– 10-15 kg
– 15-20 kg
– 20-30 kg
• No UF

Children
N Cp
Continuous 10 mg/kg bolus
1 mg/kg/h infusion
10 mg/kg in pump
9 8.1-91.1 μg/ml
16.1% < 20 μg/ml
Dis-
Continuous
10 mg/kg bolus
10 mg/kg in pump
10 mg/kg after CPB
12 7.7 – 106.7 μg/ml
16.2% < 20 μg/ml

Children
• Larger portion pump prime cf blood vol
• CPB had a large impact on PK
• Using PK data for Cp 20-30 μg/ml
– Loading dose of 6.5 mg/kg
– Followed by a weight adjusted infusion
– 3.1 mg/kg/h for 5 kg
– 2.0 mg/kg/h for 40 kg

Children
• TxA clearance is approx 3 x lower in
children
• 2 x increase in Central volume
• 4 x increase in peripheral volume
• Increased Vd
• Affect of MUF and hypothermia not
explored

Neonates
• Wesley 2015 Boston Children’s Hospital
• 55 pts aged 2 d to 4 y
• Stratified into 3 gps
– < 2 M
– 2 M-1 y
– >1y and weighing up to 20 kg
• 100 mg/kg bolus followed by 10 mg/kg/h
plus 100 mg/kg in prime
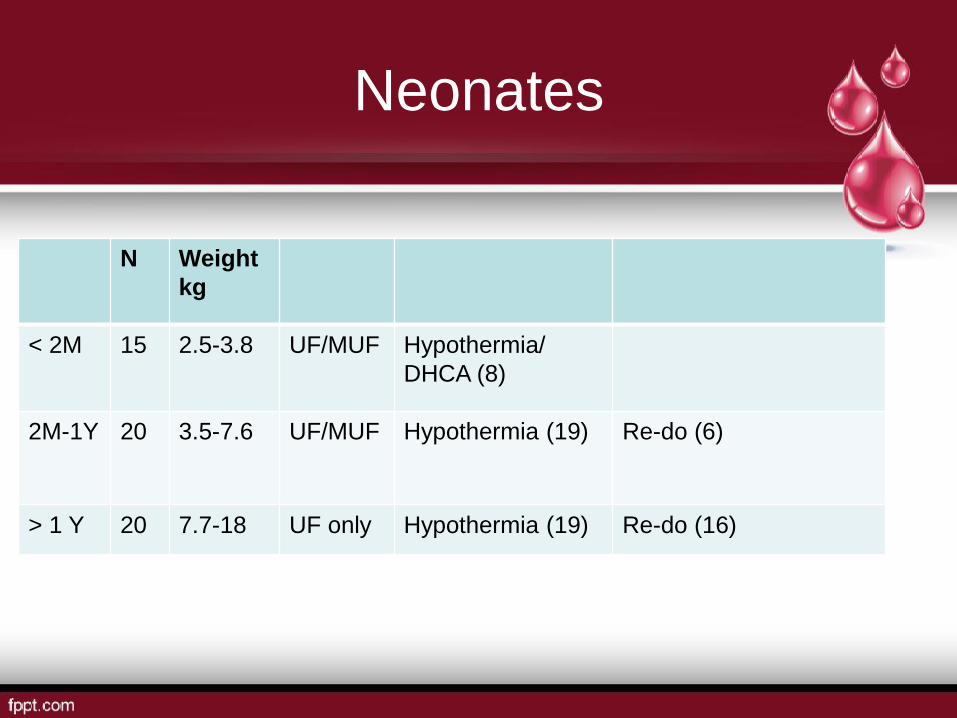
Neonates
N Weight
kg
< 2M 15 2.5-3.8 UF/MUF Hypothermia/
DHCA (8)
2M-1Y 20 3.5-7.6 UF/MUF Hypothermia (19) Re-do (6)
> 1 Y 20 7.7-18 UF only Hypothermia (19) Re-do (16)

Neonates
Age Dose 20 μg/ml 60 μg/ml 150 μg/ml
0-2 M Load mg/kg 15 50 120
Infusion mg/kg/h 2.5 7 17
Prime μg/ml 20 60 150
2-12 M Load mg/kg 9 26 65
Infusion mg/kg/h 2 6 14
Prime μg/ml 20 60 150
> 12 M Load mg/kg 4 13 31
Infusion mg/kg/h 2 5.5 14
Prime μg/ml 20 60 150

Neonates
• NN dosing different to > 1 year
• 2 monthers require higher loading dose
than 12 monthers
• Developmental changes better captured
by age (rather than weight)
• MUF dose not impact significantly on dose
• Dose prime on volume not patient weight

Neonates
• Neonatal cord blood require lower TxA
concentrations to completely prevent
hyperfibrinolysis (Yee 2013)
• 6.54 μg/ml (95% CI 5.19-7.91)
cf 17.5 μg/ml (95% CI 14.59-20.41)

Dose-Effect
• Faraoni 2014
• TxA dose on TEG
N R min Angle MA mm LY30 %
Placebo 12 10.0 +/- 2.8 52.6 +/- 15.5 58.4 +/- 8.1 0.9 +/- 1.1
30 mg/kg bolus
16 mg/kg/h
infusion
40 9.2 +/- 2.2 46.4 +/- 13.2 58.7 +/- 6.2 0.2 +/- 0.5
5 mg/kg bolus
5 mg/kg/h
infusion
12 10.1 +/- 3.5 53.7 +/- 11.6 58.6 +/- 5.1 0.1 +/- 0.2

Where from here?
• Confirmation of PK in
different pt populations
esp paediatrics
• Dose adjustment
requirement for eGFR
• Obesity PK
(hypothermia/UF)

Timing?
• Cumulative dose
effects (infusions in
long cases)
• Total dose limits
• Timing (?12 hours)
– Max secondary
fibrinolysis
• In Vivo dose-effect

THE END