the science of patient safety: longitudinal studies in an environment of change. wagar ea, hilborne...
TRANSCRIPT

The Science of Patient Safety: Longitudinal Studies in an Environment of Change.
Wagar EA, Hilborne LH, Yasin B, Tamashiro L, and Bruckner DA. UCLA Healthcare and Department of Pathology & Laboratory
Medicine, David Geffen School of Medicine at UCLA

Patient Identification Safety Initiative
• November, 2002, reviewed all types of specimen errors and created categories
• Consulted with nursing, physicians, laboratory professionals
• Began collecting continuous data

Specimen Error Information: Categories
• Clotted specimen• Container leaking• Duplicate order• Hemolyzed specimen• Improperly collected• Improperly handled• Mislabeled specimen
• Quantity not sufficient• Requisition mismatch• Specimen not suitable
for test• Tube overfilled• Tube underfilled• Unlabeled specimen
Methods
• Baseline data collect 11-02 through 3-03
• Critical patient identification categories targeted
• Three patient safety initiatives implemented at 4, 10, and 14 months
• Statistical analyses by paired student’st-test and linear trend analysis
Three Critical Patient Identification Errors
• Specimen/requisition mismatch
• Unlabeled specimens
• Mislabeled specimens (“wrong blood in tube”)
Three Patient Safety Initiatives
• Phlebotomy service reorganization and education: 4 months
• Electronic event reporting system: 10 months
• Automated processing system: 14 months
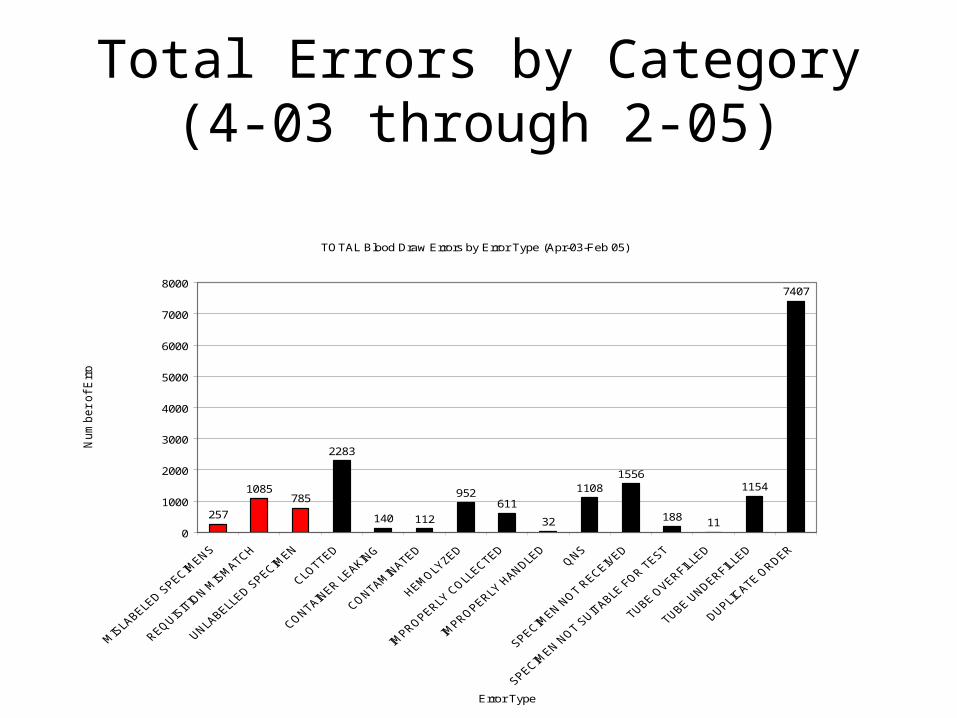
Total Errors by Category(4-03 through 2-05)
TOTAL Blood Draw Errors by Error Type (Apr-03-Feb 05)
257
1085785
2283
140 112
952611
32
11081556
188 11
1154
7407
0
1000
2000
3000
4000
5000
6000
7000
8000
Error Type
Num
ber
of
Err
ors

Patient Identification ErrorsTotal Blood Draw Errors-Selected Error Types (Apr-03-Feb-05)
257
1085
785
0
200
400
600
800
1000
1200
MISLABELED SPECIMENS REQUISITION MISMATCH UNLABELLED SPECIMEN
Error Type
Num
ber
of E
rror
s
MISLABELED SPECIMENS
REQUISITION MISMATCH
UNLABELLED SPECIMEN

Patient Identification Errors: ICUs
ICU Blood Draw Errors-Selected Error Types (Jan-04 to Feb-05)
52
302
207
0
50
100
150
200
250
300
350
MISLABELLED SPECIMENS REQUISITION MISMATCH UNLABELLED SPECIMEN
Specimen Error Category
Tot
al IC
U E
rror
s

Patient Identification Errors
• Critical identification errors were 12.0% of all specimen errors
• Over 4.29 million specimens and 2.31 million phlebotomy requests
• Critical identification errors are <0.1% of all procedures or all specimens
• Patient identification errors occurred frequently in ICUs

Longitudinal Data: Patient Identification Errors
CRITICAL ERRORS by TYPE/MONTHPeriod: Apr 2003 thru Jan 2005
1517
10
2426
11
16 17
33
17
25
1
16
0
3 2
11
7
2 1 20
76
55 56
63
47 48
52
47 48
29
40
45
48 47
37 37
45
42
39
42
53
50
56
49
39
3638
29
46
30 3133 33 32
39
21
25
28
25
42
36
39
29
32
0
10
20
30
40
50
60
70
80
Apr-03
May-03
Jun-03
Jul-03 Aug-03
Sep-03
Oct-03
Nov-03
Dec-03
Jan-04
Feb-04
Mar-04
Apr-04
May-04
Jun-04
Jul-04 Aug-04
Sep-04
Oct-04
4-Nov 4-Dec 4-Jan
MISLABELED SPECIMENS REQUISITION MISMATCH UNLABELLED SPECIMEN
Linear (MISLABELED SPECIMENS) Linear (REQUISITION MISMATCH) Linear (UNLABELLED SPECIMEN)
Centralized Phlebotomy/Education
Electronic Error Reporting Initiated
Installation of Automated Processor

Longitudinal Data: Patient Identification Errors
Error Specimen Category
P-Value
Mislabeled Specimens 0.014
Requisition Mismatches 0.001
Unlabeled Specimens 0.002

Other Things that Happed Along the Way……….
• Outside consultant, November 2002
• JCAHO, April, 2004
• Departure of the outside consultant, June, 2004
• New CEO appointment, July, 2004
• No significant changes in trends over the period March, 2003, through February, 2005

Conclusions
• Critical patient identification errors can be decreased in an environment of change: Leadership commitment!
• Expensive IT solutions are helpful but not essential as change factors
• Awareness is a key factor for change
• Changes were sustainable (April, 2003, to February, 2005)

Patient Safety Paradigm for Change
AWARENESS
NOISE
SUSTAINABILITY

THANK YOU
THE UCLA PATIENT SAFETY TEAM