the science of wound bed preparation · the science of wound bed preparation becky adkins, rn, msn,...
TRANSCRIPT

The Science ofThe Science ofWound Bed PreparationWound Bed Preparation
Becky Adkins, RN, MSN, CWSNurse Practitioner
April 28, 2004

Objectives
• Differentiate normal wound healing from chronic wound healing
• Discuss factors that contribute to impaired healing in the the chronic wound
• Identify the components of Wound Bed Preparation to include debridement, bacterial burden, moisture balance

Components of Normal Wound Healing
Cell types involved
PlateletsPlateletsCoagulation Process
PlateletsPlateletsMacrophagesMacrophagesNeutrophilsNeutrophilsInflammatory
ProcessMacrophagesMacrophagesLymphocytesLymphocytesFibroblastsFibroblastsEpithelial cellsEpithelial cellsEndothelial cellsEndothelial cells
Migratory/ ProliferativeProcess
FibroblastsFibroblastsRemodeling Process
Injury/Hours/Days Weeks23Kane DP, Krasner D. In: Chronic Wound Care. 2nd ed. Health Management Publications Inc; 1997:1-4.

Degrades ECMDegrades ECM•• impaired cell migrationimpaired cell migration•• impaired connective tissue depositionimpaired connective tissue depositionDegrades Growth Factors Degrades Growth Factors
Prolonged Inflammation Prolonged Inflammation Stimulation of macrophage and Stimulation of macrophage and
neutrophils to wound bedneutrophils to wound bed
Release of proRelease of pro--inflammatory inflammatory cytokinescytokines
↑↑ Production MMPs and Production MMPs and ↓↓ TIMPsTIMPs
Chronic WoundChronic WoundDelayed HealingDelayed HealingRepeated Trauma
Local Tissue IschemiaNecrotic Tissue
Heavy Bacterial BurdenTissue Breakdown
TNFTNFαα and ILand IL--11ββ

Biochemical Differences
Healing Wounds• cell mitosis• pro-inflammatory
cytokines• MMPs• Growth factors• Cells capable of
responding to healing signals
Chronic Wounds• mitogenic activity• pro-inflammatory
cytokines• MMPs• Varied # growth
factors• Senescent cells

Clinical Assessment
• Does this patient have the ability to heal?
• Consider overall goals of care• Address wound etiology• Consider factor that contribute to
impaired wound healing

Wound Etiology
MechanicalArterialVenousNeuropathicMalignancyVasculiticOther
Address the Address the etiologyetiology

Assessment
Systemic Factors
Medications
Tissue Oxygenation
Concomitant Disease
Age
Body Build
Stress
Nutrition
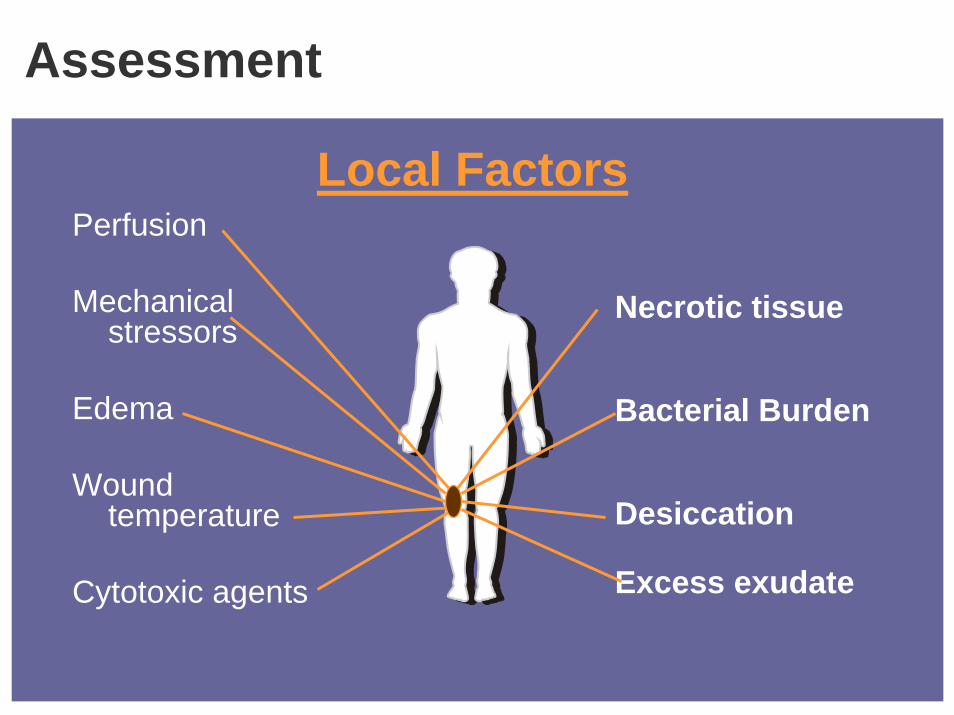
Assessment
Local FactorsPerfusion
Mechanical stressors
Edema
Wound temperature
Cytotoxic agents
Necrotic tissue
Bacterial Burden
Desiccation
Excess exudate

Wound Bed Preparation - Defined
Wound bed preparation is the management of a wound in order to accelerate endogenous healing or to facilitate the effectiveness of other
therapeutic measures
1Falanga, 2003

International Advisory Panel on Wound Bed Preparation
Keith Harding, MD
Marco Romanelli, MD
Michael Stacey, DS
Luc Teot, MD, PhD
Wolfgang Vanscheidt, MD
Gregory Schultz, PhD
Vincent Falanga, MD
Gary Sibbald, MD
Elizabeth Ayello, PhD
Caroline Dowsett
Wound Bed Preparation:A Systematic Approach to Wound Management
Wound Repair and Regeneration, 2003; 11:1-28
20Schultz, Sibbald, Falanga, et al, 2003

TIME Principles of Wound Bed PreparationTissue non viable or deficient
Infection or inflammation
Edge of Wound non advancing or undermined
Moisture imbalance
High bacterial counts or prolonged inflammation
Defective matrix and cell debris
Desiccation or excess fluid
Non-migrating keratinocytesNon-responsive wound cells
Biological Agents Adjunct Therapies
Debridement
Restore wound base and ECM proteins
Low bacterial counts and controlled inflammation
Restore cell migration, maceration avoided
Stimulate keratinocytemigration
Dressings Compression
Debridement Antimicrobials

TTTissue:
Non-viable or Deficient

Debridement
Why debride?• Enhance wound assessment• Decrease potential for
infection• Necrotic tissue delays
formation of granulation and epithelial tissue

Debridement
What to debride?• Slough - moist yellow, tan or
gray non-viable tissue.• Eschar - dry, leathery

Debridement Methods
SurgicalMechanicalAutolytic
EnzymaticBiological
Select the most appropriate method for the patient’s condition and goals of care

Surgical Debridement
• Scalpel• Scissors• Curet• Laser
Recommended for removal of thick, adherent eschar and devitalized tissue in large wounds

Surgical DebridementConsiderations• The most aggressive debridement• Requires adequate perfusion• Tissue or bone cultures• Not recommended for severely compromised
patients• Analgesia/anesthesia required• Licensure/Skill• Associated with increased healing rates
among patients with diabetic foot ulcers5
5Steed et al, 1996

Surgical Debridement
Courtesy David Armstrong, MD

Mechanical Debridement
Definition - The removal of foreign material and dead or damaged tissue by the use of physical forces.
Methods– Irrigation– Wet-to-dry dressings– Hydrotherapy

Mechanical Debridement
Considerations• Aggressive debridement• Wet-to-dry dressing may be painful• Trauma to capillaries can cause bleeding• Skin maceration may occur• Dressing changes may be time-consuming

Mechanical Debridement
A B

Autolytic Debridement
Definition - The process by which the wound bed utilizes phagocytic cells and proteolytic enzymes to remove debris.
This process can be promoted and enhanced bymaintaining a moist woundenvironment.

Autolytic Debridement
Considerations• Less aggressive debridement• Slower than other methods• Easy to perform• Little or no discomfort• Performed in any setting• Contraindicated in the presence of infection

Autolytic Debridement

Enzymatic Debridement
Definition - The use of topically applied chemical agents to stimulate the breakdown of necrotic tissue.
Common Topical Agents– Papain-Urea– Papain-Urea - Chlorophyllin– Collagenase

Enzymatic Debridement
Collagenase• Derived from Clostridium Hystoliticum• Highly specific for peptide sequence found in
collagen• Less aggressive debridement• Site of action – collagen fibers anchoring
necrotic tissue to the wound bed
10Harper (1972) 11Boxer (1969) 12Varma (1973)

Enzymatic Debridement
Papain-Urea• Proteolytic enzyme derived papaya6
• Urea is added as a denaturant6
• Site of action – cysteine residues on protein8
• Inactive against collagen6
• Aggressive debridement
6Falabella (1998) 8 Sherry and Fletcher (1962

Papain-Urea Mode of Action

Enzymatic Debridement
Papain-Urea Chlorophyllin• Contains Papain, Urea and Sodium Copper
Chlorophyllin • Sodium copper chlorophyllin is a chlorophyll
derivative– Anti-agglutinin
• Results in anti-Inflammatory action– Reduces odor
7Morrison J, Casali J (1957)

Enzymatic DebridementConsiderations• Should be painless• Less traumatic than surgical or mechanical
debridement• Easy dressing change• Observe caution with infected wounds• Consider the use of enzymatic debridement
for individuals who:– Cannot tolerate surgery– Reside in a long-term-care facility– Receive care at home*
*Agency for Healthcare Research and Quality (1994)

Enzymatic Debridement
Eschar Preparation• Cross Hatching• Hydrating agents

Debridement Methods
More Aggressive• Surgical• Mechanical• Papain-Urea
Less Aggressive• Autolytic• Collagenase• Papain-Urea
Chlorophyllin

Debridement Decisions:Clinical Indications
Aggressive Methods• Majority of wound
covered with necrotic tissue
• Goal of therapy is quick removal of necrotic tissue
• Wound continues to improve with current therapy

Debridement Decisions:Clinical Indications
• Majority of wound is clean and granulating
• No threat to patient’s health
Less Aggressive Methods

Debridement Decisions
Selecting the Appropriate Method• Wound characteristics• Degree of desired aggressiveness• Time available for debridement• Skill/licensure of clinician• Care setting
Clinicians may choose more than one method of debridement – e.g., surgical, followed by enzymatic

Most Aggressive - Surgical

Aggressive

Less Aggressive
The right method is a clinical decision that requires judgment

IIInfection or
Inflammation

Risk Factors that Increase the Risk for Infection
Systemic• Vascular disease• Edema• Malnutrition• Diabetes mellitus• Alcoholism• Prior surgery or radiation• Drugs e.g.
corticosteroids• Inherited immune
defects
Local• Large wound area• Increased wound depth• Degree of chronicity• Anatomic location (distal
extremity, perineal)• Presence of foreign bodies• Necrotic tissue• Mechanism of injury
Degree of post-wounding contamination
• Reduced perfusion

Bacterial Burden
Contamination - Infection Continuum
INFE
CTION
CRITICALL
Y
COLONIZE
D
CONTAMIN
ATION
COLONIZE
DLocal Systemic
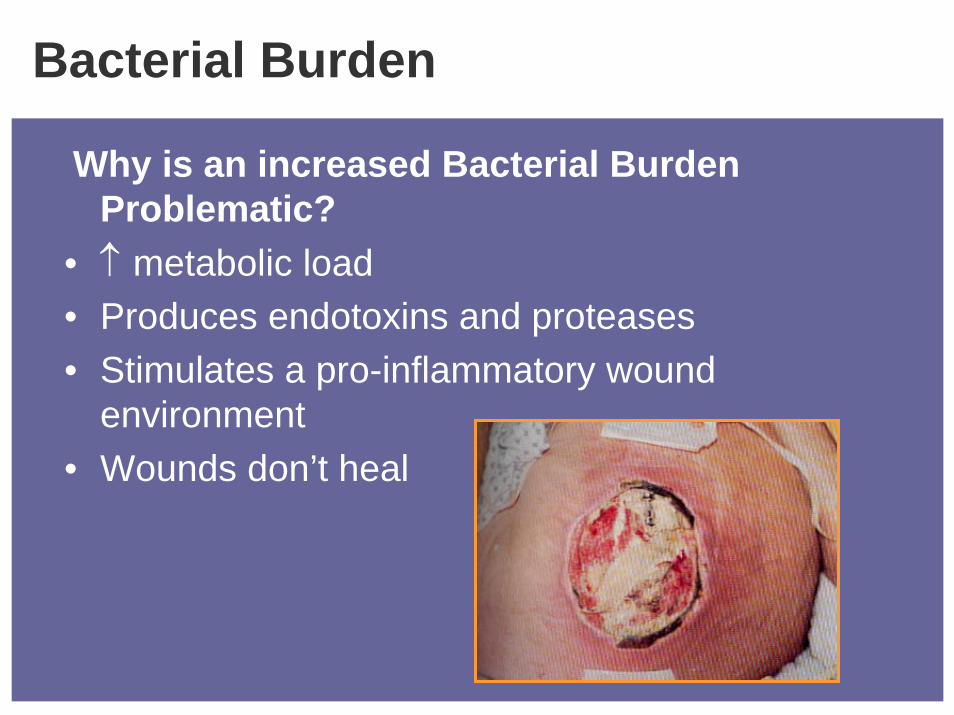
Bacterial Burden
Why is an increased Bacterial Burden Problematic?
• ↑ metabolic load• Produces endotoxins and proteases• Stimulates a pro-inflammatory wound
environment• Wounds don’t heal

BacterialBalance
HostResistance
Bacterial quantityand
virulence
AdhesinsCell Capsules
BiofilmsAntibiotic Resistance
Local perfusionImmunosuppression
DiabetesMedications
3Sibbald et al (2000) 14Dow (2001)

Clinical Presentation
“Classic” Signs & Symptoms of Infection
Acute Wound Infectionor
SevereChronic Wound
Infection
Advancing erythemaFeverWarmthEdema / swellingPainPurulence
Clinical Presentation
Critically Colonized-
↑ Bacterial Burden-
Local Wound Infection
Delayed healingChange in color of wound bedFriable granulation tissueAbsent or abnormal granulation tissue↑ or abnormal odor↑ serous drainage↑ pain at wound site
15Cutting & Harding (1994)16Gardner, Frantz & Doebbeling (2001)
Secondary Signs & Symptoms of Infection

Reducing Bacterial Burden
Interventions• Debridement• Wound cleansing• Avoid routine use of antiseptics
– Betadine– Hydrogen Peroxide– Acetic Acid– Dakin’s Solution

Recommendations for Wound Bed PrepCONTA
MINATIO
N
COLONIZ
EDWound progressingWound progressing
•Routine wound cleansing•Exudate management•No indication for cultures

Recommendations for Wound Bed Prep
Delayed healingDelayed healing
Critica
lly
Colonized
Local
Infection
• Thorough cleansing• Exudate management
• Debridement if needed• Consider topical antimicrobials
-Silver dressing-Cadexomer idodine gel
Topical Antimicrobials - Silver
• Centuries of proven antimicrobial activity
• Cytotoxicity concerns associated with carriers not silver - ex. Silver nitrate, Silver sulfadiazine
• Traditional delivery required repeated applications due to binding with chlorine and proteins
• New silver dressings allow for continued silver release - up to 7 days
17Demling and DeSanti (2001)
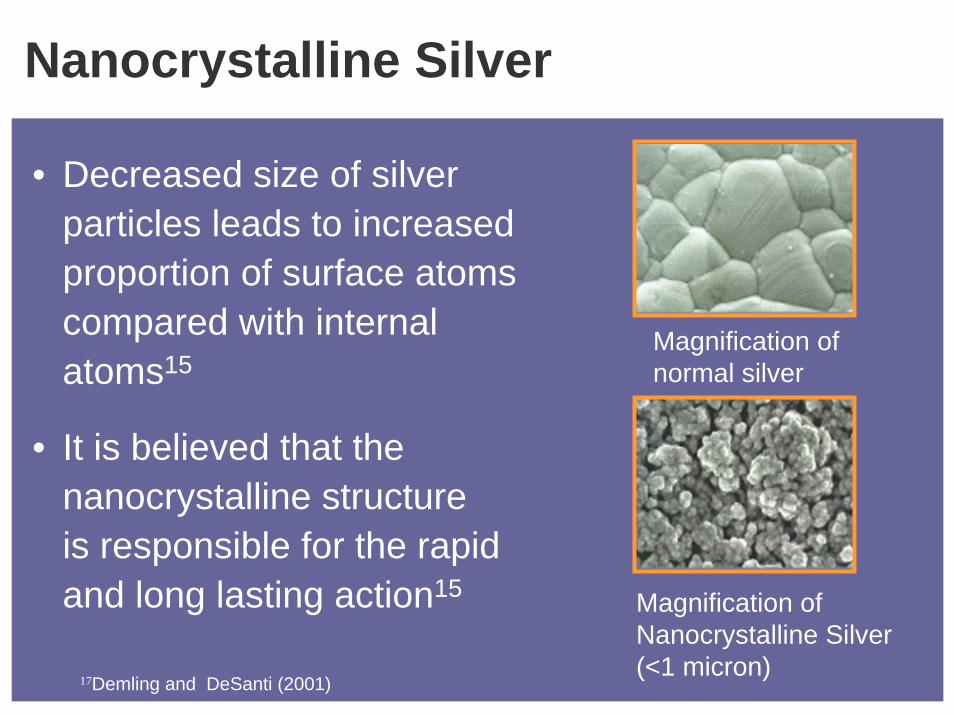
Nanocrystalline Silver
• Decreased size of silver particles leads to increased proportion of surface atoms compared with internal atoms15
• It is believed that the nanocrystalline structure is responsible for the rapid and long lasting action15
Magnification of normal silver
Magnification of Nanocrystalline Silver (<1 micron)
17Demling and DeSanti (2001)

Case Study
Day 0
10 year old venous leg ulcers previously treated with compression and SSD
Day 20
After treatment with nanocrystalline silver
18Data on file

Topical Antimicrobials Cadexomer Iodine
• Iodine is a well known antimicrobial agent• 0.9% iodine is carried in polysaccharide
beads• Provides a slow sustained release of
iodine in non-cytotoxic concentrations• High rate of absorption from exudating
ulcers.• No documented cases of bacterial
resistance.

Recommendations for Wound Bed Prep
Impaired healingImpaired healing
Contam
inated
INFE
CTION
Coloniz
ed
Critica
lly
Coloniz
ed
Courtesy AAWC• Thorough cleansing• Debridement if needed • Exudate management• Consider topical antimicrobials
•Silver dressing•Cadexomer iodine gel
• Systemic antibiotics

Moisture Imbalance - Dry
• Desiccation slows epithelial migration• Painful and uncomfortable for the
patient• Delays normal healing process• Acts as a source of infection• Longer treatment time • Increased cost

Moisture Imbalance - Wet
• Maceration of peri-wound skin
• Chronic wound fluid issues

Exudate Management
EdemaBacterialBurden
Breakdown of Necrotic tissue(Debridement)
MicrobialManagement
Compression
Dressing Selection
Chronic Wound Fluid

Chronic Wound Fluid - Edema
Ankle-Brachial Index & Compression< 0.5 --- 0.6 ------------- 0.8 ---------------1.0
NoneNoneReduced Reduced
HighHigh

Dressing Selection Factors
• Amount of exudate • Anatomical location• Presence of dead space (Depth,
undermining, tunneling)• Condition of surrounding skin• Caregiver ability• Healable vs. non-healable wound• Cost

Managing Moisture Imbalance
None Small Moderate LargeNone Small Moderate LargeNone Small Moderate LargeExudate Amount
FilmsHydrogel
HydrocolloidAlginate
Foams
Specialty Absorbent

Small Amount of Exudate
A B
CD
Courtesy AAWC

Moderate Amount of Exudate
A B
C D
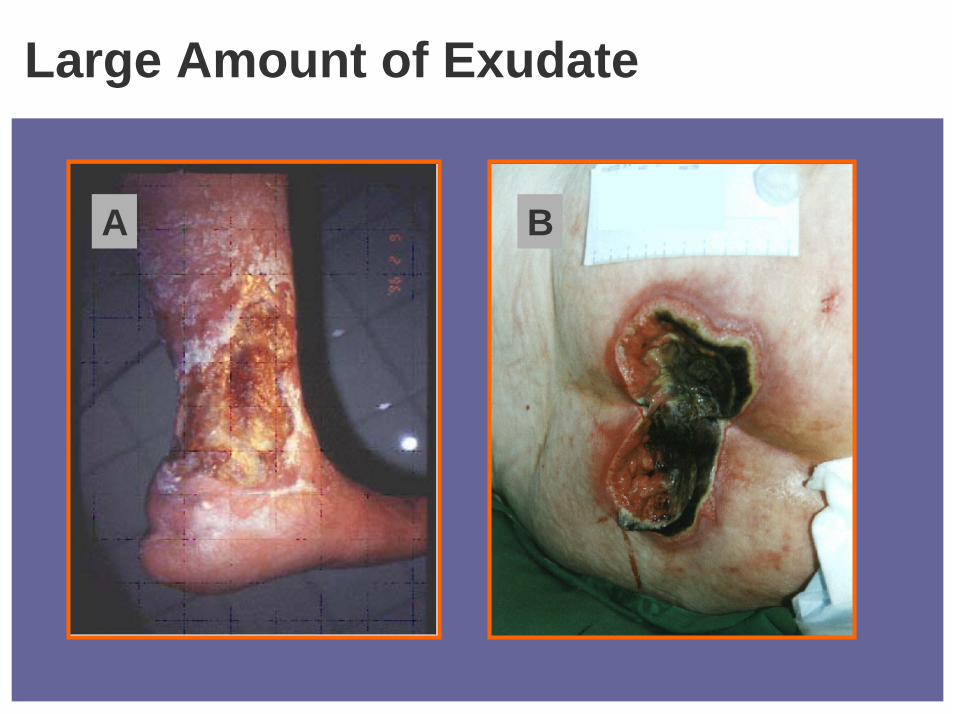
Large Amount of Exudate
A B

Edge of Wound Non-advancing or
Undermined
EE

Edge of Wound Non-advancing or UnderminedProblem • Cells not capable of responding to healing
signals• Hyper-proliferation of epidermal cells
occurs at the wound margins• Epidermis fails to migrate across the
wound

Edge of WoundNon-advancing or undermined
Interventions• Debridement• Biological Agents• Skin Grafts• Adjunctive Therapies
20Adapted from Schultz, Sibbald, Falanga, et al, 2003

Continuous Assessment
SystemicFactorsPatientEtiology
Local Factors
Time Principles

References1 Falanga V. (Ed.). New Concepts in Wound Bed Preparation. Springer-Verlag GmbH & Co. KG, Science
Communication Corporate Publishing, Berlin Heidelberg, 2003.
2 Falanga V. Classifications for wound bed preparation and stimulation of chronic wounds. Wound Repair and Regeneration 2000;8:347-352.
3 Sibbald RG, Williamson D, Orsted HL, Campbell K, Keast D, Krasner D, Sibbald D. Preparing the Wound Bed -Debridement, Bacterial Balance and Moisture Balance. O/WM 2000;46(11)14-35.
4 Mast BA, Schultz GS. Interactions of cytokines, growth factors, and proteases in acute and chronic wounds. Wound Repair and Regeneration 1996;4:411-420.
5 Steed DL, Donohoe D, Webster MW, Lindsley l, and the Diabetic Ulcer study Group. Effect of Extensive Debridement and Treatment on the Healing Diabetic Foot Ulcer. Journal of the American College of Surgeons 1996;183:61-64.
6 Falabella A. Debridement of Wounds. Wounds 1998:10;1C-9C.7 Morrison J, Casali J. Continuous Proteoplytic Therapy for Decubitus Ulcers. Am Journal of Surgery 1957; 93: 446-448.8 Sherry S. and Fletcher AP. Proteolytic enzymes: a Therapeutic evaluation. Clinical Pharmacology and Therapeutics
196X;1:202-226.
9 Lutterman A, Curtis R, Blache C, Johnston K & Frye K. Accuzyme Papain/Urea Ointment vs. Collagenase Santyl Ointment in the Treatment of Partial Thickness Burn Wounds, presented at SAWC, 2001
10 Harper E. Studies on the Mechanism of Action of Bacterial Collagenase. in Collagenase. Mandl, I., ed., Gordon& Breach, Science Publishers, Inc. New York, 1972.
11 Boxer AM, Gottesman N, Bernstein H, Mandl I. Debridement of Dermal Ulcers and decubiti with collagenase. Geriatrics 1969;24(7):75-86.

12 Varma AO, Bugatch E, German FM. Debridement of Dermal Ulcers with Collagenase. Gynecology & Obstetrics 1973;136:281-281.
13 Robson, MC. Wound Infection: A Failure of Wound Healing Caused by an Imbalance of Bacteria. Surgical Clinics of North America 1997;77(3)637-651.
14 Dow G. Infection in chronic wounds. In: Krasner DL, Rodheaver GT, Sibbald RG (eds). Chronic Wound Care: A Clinical Source Book for Healthcare Professsionals, Third Edition. Wayne, PA: HMP Comunications, 2001:343-356.
15 Cutting KF, Harding KG. Criteria for Identifying wound infection. Journal of Wound Care 1994;3(4):198-201.
16 Gardner SE, Frantz RA, Doebbeling BN. The validity of the clinical signs and symptoms used to identify localized wound infection. Wound Repair and Regeneration 2001;9(3):178-186.
17 Demling R. DeSanti L. Effects of Silver on wound Management. Wounds 2001;13(1) Supplement A:4-15.
18 Data on file
19 Schultz G, Mast B. Molecular Analysis of the Environment of Healing and Chronic Wounds: Cytokines, Proteases and Growth Factors. Wounds 1998;10:1F-9F20 Schultz G. sibbald RG, Falanga V, Ayello A, Dowsett C, Harding K, Romanelli M, Stacey M, Teot L, Vanscheidt W. (2003) Woud bed preparation: a systematic approach to wound management. Wound Repair & Regeneration 11(1): 1-28.21 Enoch S, Harding K. (2003). Wound bed preparation: the science behind the removal of barriers to healing. Wounds, 15(7): 213-229.22 Sibbald RG. Topical Antimicrobials. Ostomy/Wound Management 2003;49(5A-suppl): 3-33.23. Kane DP, Krasner D. In: Chronic Wound Care. 2nd ed. Health Management Publications Inc; 1997:1-4.
References