the second stage of labour max brinsmead mb bs phd march 2013
TRANSCRIPT

The Second Stage The Second Stage of Labourof Labour
Max Brinsmead MB BS PhDMax Brinsmead MB BS PhD
March 2013March 2013

Subjects to be covered:Subjects to be covered: DefinitionsDefinitions What is the evidence that What is the evidence that
interventions are useful in the 2interventions are useful in the 2ndnd stage:stage:
Limitation on the lengthLimitation on the length Position to adoptPosition to adopt Coached pushing and or breath-holdingCoached pushing and or breath-holding
What is recommended for:What is recommended for: Observations in the 2Observations in the 2ndnd stage stage When to interveneWhen to intervene Maternal position for deliveryMaternal position for delivery Advice to mothers about pushingAdvice to mothers about pushing Reducing obstetric traumaReducing obstetric trauma Care for patients with previous 3Care for patients with previous 300 and 4 and 400
traumatrauma

Resources:Resources:
Cochrane databaseCochrane database
PubmedPubmed
NICE (UK) GuidelinesNICE (UK) Guidelines
My personal experienceMy personal experience

NICE recommends that the 2NICE recommends that the 2ndnd stage of stage of labour be divided and defined as...labour be divided and defined as... Passive Second StagePassive Second Stage
– From the time of full dilatation to From the time of full dilatation to the commencement of involuntary the commencement of involuntary expulsive effort by the womanexpulsive effort by the woman
Active Second StageActive Second Stage– From the commencement of From the commencement of
expulsive efforts by the woman expulsive efforts by the woman – PLUSPLUS– There are symptoms or signs of There are symptoms or signs of
full dilatationfull dilatation– OROR– The baby is visibleThe baby is visible
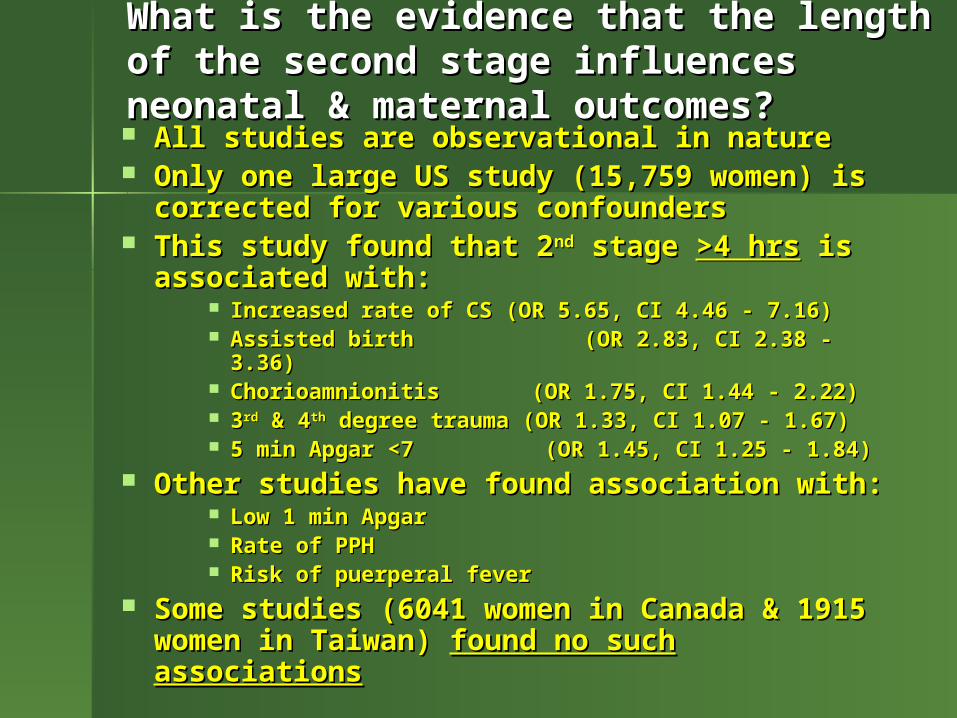
What is the evidence that the length of the second What is the evidence that the length of the second stage influences neonatal & maternal outcomes?stage influences neonatal & maternal outcomes? All studies are observational in natureAll studies are observational in nature Only one large US study (15,759 women) Only one large US study (15,759 women)
is corrected for various confoundersis corrected for various confounders This study found that 2This study found that 2ndnd stage stage >4 hrs>4 hrs is is
associated with:associated with: Increased rate of CS (OR 5.65, CI 4.46 - 7.16)Increased rate of CS (OR 5.65, CI 4.46 - 7.16) Assisted birth (OR 2.83, CI 2.38 - 3.36)Assisted birth (OR 2.83, CI 2.38 - 3.36) Chorioamnionitis (OR 1.75, CI 1.44 - 2.22)Chorioamnionitis (OR 1.75, CI 1.44 - 2.22) 33rdrd & 4 & 4thth degree trauma (OR 1.33, CI 1.07 - 1.67) degree trauma (OR 1.33, CI 1.07 - 1.67) 5 min Apgar <7 (OR 1.45, CI 1.25 - 1.84)5 min Apgar <7 (OR 1.45, CI 1.25 - 1.84)
Other studies have found association with:Other studies have found association with: Low 1 min ApgarLow 1 min Apgar Rate of PPHRate of PPH Risk of puerperal feverRisk of puerperal fever
Some studies (6041 women in Canada & Some studies (6041 women in Canada & 1915 women in Taiwan) 1915 women in Taiwan) found no such found no such associationsassociations

So does a review of what is “normal” help?So does a review of what is “normal” help?
The mean plus or minus 2 SD for The mean plus or minus 2 SD for “normal” women with a “normal” “normal” women with a “normal” outcome is:outcome is:
54 ± 142 minutes for Nullips54 ± 142 minutes for Nullips
20 ± 60 minutes for Multips20 ± 60 minutes for Multips
Note the very wide SDNote the very wide SD And the variable is not normally And the variable is not normally
distributeddistributed So the answer is “NO”So the answer is “NO”

NICE conclusions for the length of the NICE conclusions for the length of the second stagesecond stage For nulliparaFor nullipara
– 2.5 hours without an epidural2.5 hours without an epidural– 3 hours with an epidural3 hours with an epidural
For the parous patientFor the parous patient– 60 minutes without an epidural60 minutes without an epidural– 120 minutes with an epidural120 minutes with an epidural
NICE recommends:NICE recommends: Consultation with the obstetrician for a Consultation with the obstetrician for a
Nullipara whose delivery is not Nullipara whose delivery is not imminent after 2 hoursimminent after 2 hours
And 1 hour in a previously parous And 1 hour in a previously parous patientpatient
Reassess all patients with an epidural Reassess all patients with an epidural who do not push within 1 hour after who do not push within 1 hour after fully dilatedfully dilated

Scalp pH in LabourScalp pH in Labour

My observations:My observations:
It is obvious that there is fetal deterioration It is obvious that there is fetal deterioration with increasing length of the second stagewith increasing length of the second stage
Because the ultimate outcome is fetal deathBecause the ultimate outcome is fetal death Few women can actively push in a normal Few women can actively push in a normal
second stage with 2-3:10 contractions for second stage with 2-3:10 contractions for more than 60 minutesmore than 60 minutes
So most will accept or even welcome So most will accept or even welcome intervention when they have become intervention when they have become exhaustedexhausted
Provided there is no suspicion of fetal Provided there is no suspicion of fetal compromisecompromise the second stage can continue the second stage can continue for as long as there is evidence of progressfor as long as there is evidence of progress
But convincing a patient of the need for But convincing a patient of the need for intervention on the grounds of possible fetal intervention on the grounds of possible fetal compromise is our greatest challengecompromise is our greatest challenge
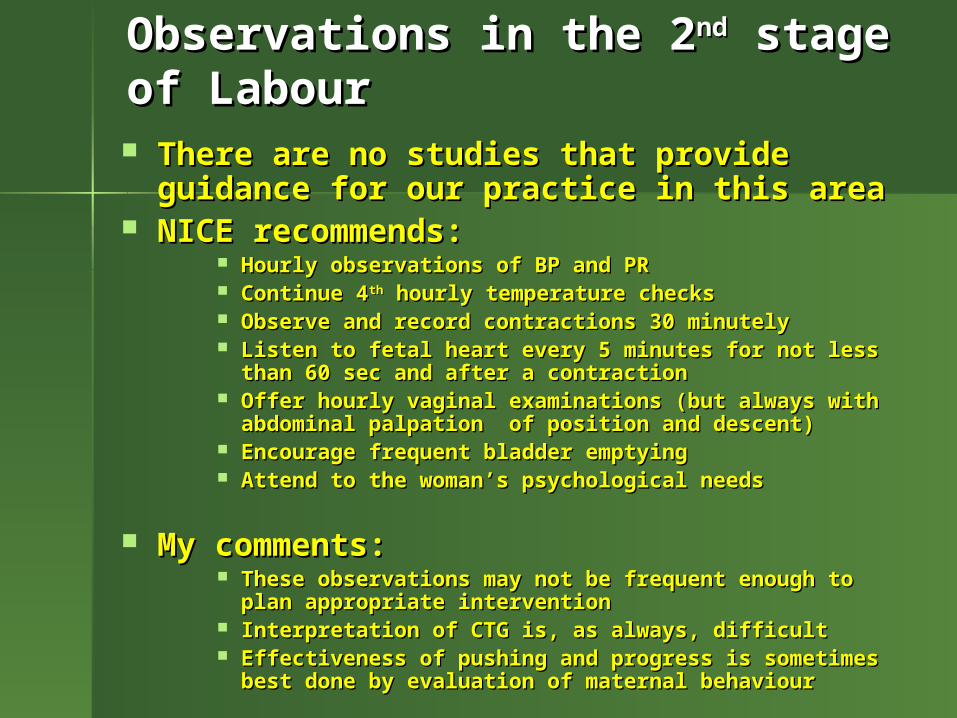
Observations in the 2Observations in the 2ndnd stage of Labour stage of Labour
There are no studies that provide There are no studies that provide guidance for our practice in this areaguidance for our practice in this area
NICE recommends:NICE recommends: Hourly observations of BP and PRHourly observations of BP and PR Continue 4Continue 4thth hourly temperature checks hourly temperature checks Observe and record contractions 30 minutelyObserve and record contractions 30 minutely Listen to fetal heart every 5 minutes for not less than Listen to fetal heart every 5 minutes for not less than
60 sec and after a contraction60 sec and after a contraction Offer hourly vaginal examinations (but always with Offer hourly vaginal examinations (but always with
abdominal palpation of position and descent)abdominal palpation of position and descent) Encourage frequent bladder emptyingEncourage frequent bladder emptying Attend to the woman’s psychological needsAttend to the woman’s psychological needs
My comments:My comments: These observations may not be frequent enough to These observations may not be frequent enough to
plan appropriate interventionplan appropriate intervention Interpretation of CTG is, as always, difficultInterpretation of CTG is, as always, difficult Effectiveness of pushing and progress is sometimes Effectiveness of pushing and progress is sometimes
best done by evaluation of maternal behaviourbest done by evaluation of maternal behaviour

What is the evidence that there is an optimal What is the evidence that there is an optimal maternal position for the second stage of labour?maternal position for the second stage of labour? A systematic review of 19 trials (but not A systematic review of 19 trials (but not
all good RCT’s) involving 5764 women all good RCT’s) involving 5764 women compared:compared:
Sitting, semi recumbent , squatting and lateral Sitting, semi recumbent , squatting and lateral positionspositions
Compared to…Compared to… Supine or lithotomy positionsSupine or lithotomy positions
Findings:Findings: Reduced length of 2Reduced length of 2ndnd stage (weighted mean reduction stage (weighted mean reduction
4.5 minutes, CI 2.94 - 5.65 minutes)4.5 minutes, CI 2.94 - 5.65 minutes) Fewer assisted births (RR 0.84, CI 0.73 - 0.98)Fewer assisted births (RR 0.84, CI 0.73 - 0.98) Fewer episiotomies (RR 0.84, CI 0.79 - 0.91)Fewer episiotomies (RR 0.84, CI 0.79 - 0.91) Reduced pain (RR 0.73, CI 0.60 - 0.90)Reduced pain (RR 0.73, CI 0.60 - 0.90) Fewer abnormal CTG’s (RR 0.31, CI 0.08 - 0.98)Fewer abnormal CTG’s (RR 0.31, CI 0.08 - 0.98) *More frequent 2*More frequent 200 tears (RR 1.23, CI 1.09 - 1.39) tears (RR 1.23, CI 1.09 - 1.39) *More PPH’s (RR 1.68, CI 1.32 - 2.15)*More PPH’s (RR 1.68, CI 1.32 - 2.15)*Seems to relate to the use of rigid birth stools rather *Seems to relate to the use of rigid birth stools rather
than upright positionthan upright position No difference in analgesia required, 3No difference in analgesia required, 300 & 4 & 400 tears, need tears, need
for transfusion, patient satisfaction, NICU admission or for transfusion, patient satisfaction, NICU admission or any neonatal outcomeany neonatal outcome

What about hands and knees?What about hands and knees?
One RCT in USA (147 women) of all One RCT in USA (147 women) of all fours for POP found:fours for POP found:
No effect on the rate of head rotationNo effect on the rate of head rotation But less back painBut less back pain No effect on maternal or neonatal outcomesNo effect on maternal or neonatal outcomes
Confirmed by a Swedish RCT of 271 Confirmed by a Swedish RCT of 271 womenwomen
Also found less perineal pain in the puerperiumAlso found less perineal pain in the puerperium But no effect on the length of the second stageBut no effect on the length of the second stage
My observation:My observation: Once you get used to the back to front mechanism of Once you get used to the back to front mechanism of
birth, then all fours, kneeling or standing with the birth, then all fours, kneeling or standing with the accoucheur posterior has much to recommend itaccoucheur posterior has much to recommend it
And I still put a woman on her side with the back And I still put a woman on her side with the back uppermost when there is malposition and slow uppermost when there is malposition and slow progress in the second stage of labourprogress in the second stage of labour
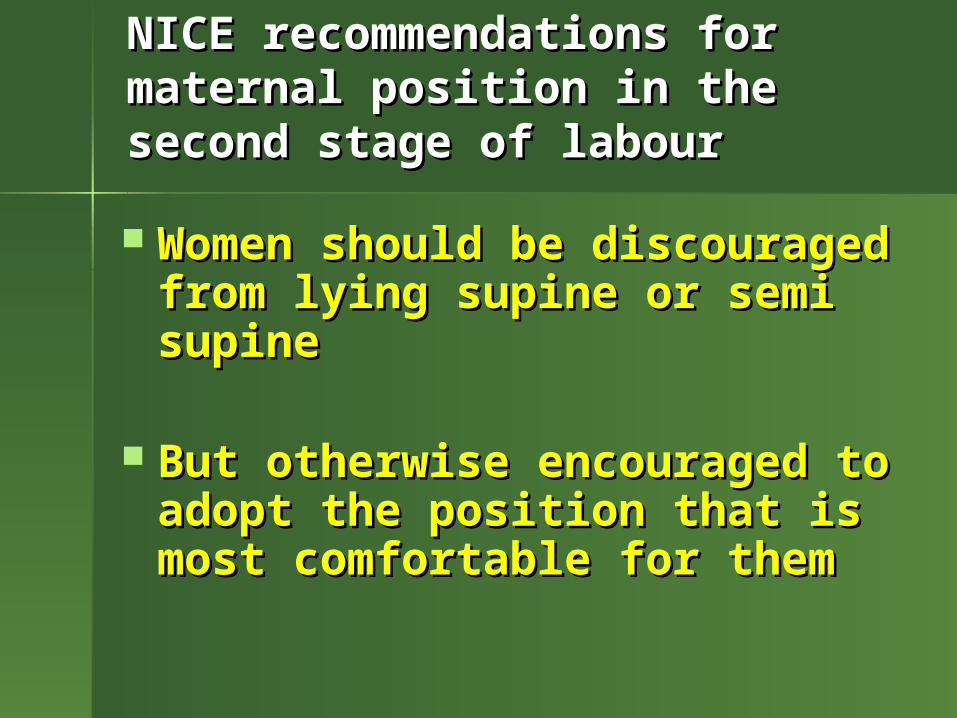
NICE recommendations for maternal NICE recommendations for maternal position in the second stage of labourposition in the second stage of labour
Women should be Women should be discouraged from lying discouraged from lying supine or semi supinesupine or semi supine
But otherwise encouraged But otherwise encouraged to adopt the position that is to adopt the position that is most comfortable for themmost comfortable for them

Closed glottis or breath-holding in the 2Closed glottis or breath-holding in the 2ndnd stage labour? stage labour?
Breath-holding Breath-holding → ↓maternal pO→ ↓maternal pO22 & oxygen & oxygen saturationsaturation
Does this have adverse fetal effects?Does this have adverse fetal effects? A study by Simpson & James Nurs. Res. 2005A study by Simpson & James Nurs. Res. 2005 Randomised 45 nullipara at 10 cm to either Randomised 45 nullipara at 10 cm to either
immediate pushing or delayed until the immediate pushing or delayed until the mother had the urge to pushmother had the urge to push
Monitored fetal OMonitored fetal O22 saturation continuously, saturation continuously, fetal & maternal outcomesfetal & maternal outcomes
The early pushing group experienced:The early pushing group experienced: Lower mean fetal OLower mean fetal O22 (12.5 vs 4.6, p<0.001) (12.5 vs 4.6, p<0.001) More frequent OMore frequent O22 <30% for >2 min <30% for >2 min More variable heart rate decelsMore variable heart rate decels More perineal lacerationsMore perineal lacerations
No difference in length 2No difference in length 2ndnd stage, Apgars or stage, Apgars or cord pHcord pH
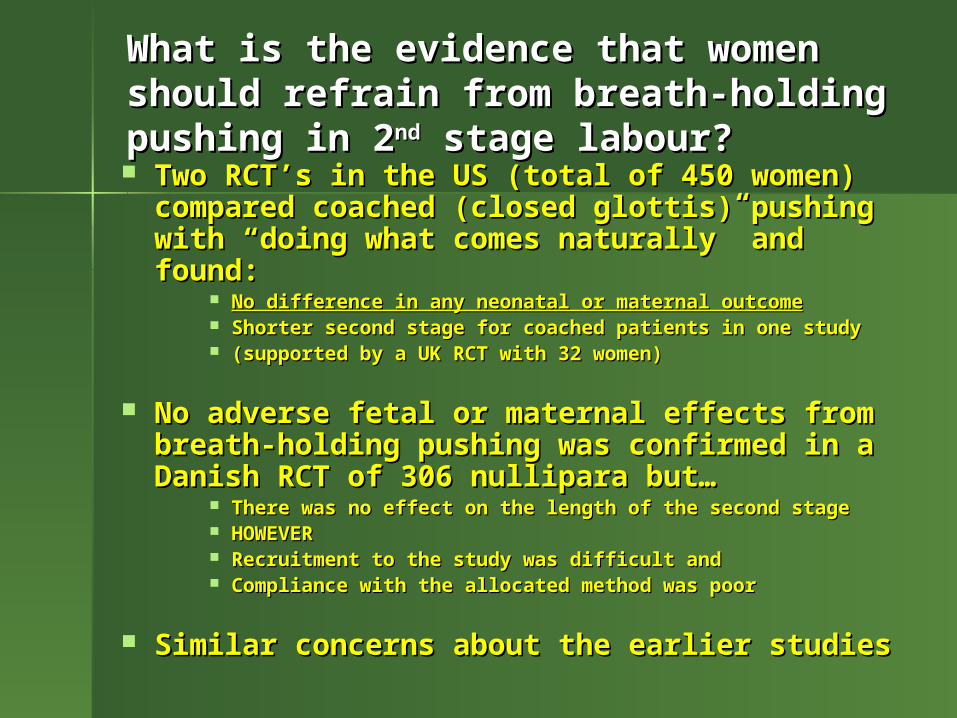
What is the evidence that women should refrain What is the evidence that women should refrain from breath-holding pushing in 2from breath-holding pushing in 2ndnd stage labour? stage labour? Two RCT’s in the US (total of 450 women) Two RCT’s in the US (total of 450 women)
compared coached (closed glottis) compared coached (closed glottis) pushing with “doing what comes pushing with “doing what comes naturally” and found:naturally” and found:
No difference in any neonatal or maternal outcomeNo difference in any neonatal or maternal outcome Shorter second stage for coached patients in one studyShorter second stage for coached patients in one study (supported by a UK RCT with 32 women)(supported by a UK RCT with 32 women)
No adverse fetal or maternal effects from No adverse fetal or maternal effects from breath-holding pushing was confirmed in breath-holding pushing was confirmed in a Danish RCT of 306 nullipara but…a Danish RCT of 306 nullipara but…
There was no effect on the length of the second stageThere was no effect on the length of the second stage HOWEVERHOWEVER Recruitment to the study was difficult andRecruitment to the study was difficult and Compliance with the allocated method was poorCompliance with the allocated method was poor
Similar concerns about the earlier studiesSimilar concerns about the earlier studies
NICE recommendations about pushing in NICE recommendations about pushing in the second stage of labourthe second stage of labour
Women should be guided by their Women should be guided by their own urge to pushown urge to push
If their pushing is ineffectual then…If their pushing is ineffectual then… Provide support & encouragementProvide support & encouragement Change positionChange position Empty the bladderEmpty the bladder
My observation:My observation: I find this advice to be unhelpfulI find this advice to be unhelpful Some women obviously require advice about how Some women obviously require advice about how
to pushto push But the physiological evidence suggests that they But the physiological evidence suggests that they
should avoid really prolonged breath-holdingshould avoid really prolonged breath-holding

Perineal MassagePerineal Massage
One large RCT in Australia (1340 women One large RCT in Australia (1340 women in 3 sites) of midwife massage between in 3 sites) of midwife massage between contractions in the second stage:contractions in the second stage:
No effect on any measure of obstetric trauma, pain, No effect on any measure of obstetric trauma, pain, return to coitus or urinary and bowel functionreturn to coitus or urinary and bowel function
There was no apparent measure of There was no apparent measure of compliancecompliance
But the study is confirmed by a US RCT But the study is confirmed by a US RCT of 1211 women in which compliance was of 1211 women in which compliance was highhigh
I am impressed by the RCT’s of the Epi-I am impressed by the RCT’s of the Epi-No device (a self-performed progressive No device (a self-performed progressive dilation of the perineum from 36 weeks)dilation of the perineum from 36 weeks)
Hot Compresses for the Perineum?Hot Compresses for the Perineum?
One large US observational study One large US observational study (2595 women) found that:(2595 women) found that:
Warm compresses reduced the need for Warm compresses reduced the need for episiotomy in nulliparas and was episiotomy in nulliparas and was borderline for multiparasborderline for multiparas
Also reduced the rate of spontaneous 2Also reduced the rate of spontaneous 20 0
tears in bothtears in both
But this was not confirmed by another US But this was not confirmed by another US RCT of 1211 womenRCT of 1211 women
““Hands on” or “Hands poised” during Hands on” or “Hands poised” during delivery of the fetal head?delivery of the fetal head? One large UK RCT of 5316 One large UK RCT of 5316 ♀ ♀ found:found:
A small reduction in perineal pain at 10 A small reduction in perineal pain at 10 days from “hands on” days from “hands on”
No difference in any measure of obstetric No difference in any measure of obstetric traumatrauma
Inexplicably fewer manual removals in the Inexplicably fewer manual removals in the “hands poised” group (2.6% vs 1.5%)“hands poised” group (2.6% vs 1.5%)
Broadly similar findings in an Broadly similar findings in an Austrian study of 1076 women Austrian study of 1076 women
But episiotomy was more common in the But episiotomy was more common in the “hands on” group“hands on” group
NICE concludes that either NICE concludes that either technique is appropriate technique is appropriate
And noted evidence that there is less And noted evidence that there is less trauma when the head delivers trauma when the head delivers betweenbetween contractionscontractions
Lignocaine spray for the perineum?Lignocaine spray for the perineum?
One RCT of 185 women found that:One RCT of 185 women found that:
No effect on perineal painNo effect on perineal pain But less dyspareunia when coitus was But less dyspareunia when coitus was
resumedresumed And fewer second degree tears in the And fewer second degree tears in the
treated group (RR 0.63, CI 0.42 – 0.93)treated group (RR 0.63, CI 0.42 – 0.93)
But NICE concludes that But NICE concludes that Lignocaine spray should not be Lignocaine spray should not be usedused
Routine or restricted use of episiotomy?Routine or restricted use of episiotomy? Seven RCT’s with 5001 women and 8 Seven RCT’s with 5001 women and 8
cohort studies with 6463 women. cohort studies with 6463 women. Meta analysis confirms that restricted Meta analysis confirms that restricted episiotomy will result in:episiotomy will result in:
Less posteriorLess posterior trauma (RR 0.87, CI 0.83 - 0.91) trauma (RR 0.87, CI 0.83 - 0.91) More anteriorMore anterior trauma (RR 1.75, CI 1.52 - 2.01) trauma (RR 1.75, CI 1.52 - 2.01) Fewer 3Fewer 300 and 4 and 400 tears (RR 0.74, CI 0.42 - 1.28) tears (RR 0.74, CI 0.42 - 1.28)
Some studies also point to:Some studies also point to: Overall more intact perineums Overall more intact perineums Less perineal painLess perineal pain Quicker return to coitus with restricted use of Quicker return to coitus with restricted use of
episiotomy andepisiotomy and More anal sphincter damage with liberal More anal sphincter damage with liberal
episiotomyepisiotomy
But no difference in…But no difference in… Sexual function at 3m & 3 yrs or bladder Sexual function at 3m & 3 yrs or bladder
functionfunction
NICE recommendations for the use of NICE recommendations for the use of episiotomyepisiotomy
Routine episiotomy is not recommended Routine episiotomy is not recommended for spontaneous birthfor spontaneous birth
Episiotomy Episiotomy should be performedshould be performed when when clinically indicated clinically indicated – e.g. fetal compromise suspected or e.g. fetal compromise suspected or
instruments requiredinstruments required
Mediolateral episiotomy is best Mediolateral episiotomy is best – i.e. start at the posterior fouchette and i.e. start at the posterior fouchette and
proceed at an angle of 45 - 60 degreesproceed at an angle of 45 - 60 degrees
Tested anaesthesia is requiredTested anaesthesia is required– Except in an extreme emergencyExcept in an extreme emergency
Birth after Previous 3Birth after Previous 300 and 4 and 400 Trauma Trauma
There are no prospective trials and There are no prospective trials and only a few retrospective studiesonly a few retrospective studies
The risk of repeat 3The risk of repeat 300 and 4 and 400 trauma trauma is similar to the original incidenceis similar to the original incidence
There is some evidence that if the There is some evidence that if the woman is asymptomatic then woman is asymptomatic then vaginal birth vaginal birth does notdoes not further further increase the risk of those symptomsincrease the risk of those symptoms
There is some evidence that for There is some evidence that for symptomatic women then vaginal symptomatic women then vaginal birth birth doesdoes increase the severity of increase the severity of those symptoms those symptoms

NICE recommendations for the care of NICE recommendations for the care of patients with previous 3patients with previous 300 and 4 and 400 trauma trauma
Routine episiotomy is not recommendedRoutine episiotomy is not recommended
Discussion about intrapartum care Discussion about intrapartum care should cover…should cover…
Current symptoms of dysfunction of the anal Current symptoms of dysfunction of the anal sphinctersphincter
The previous traumaThe previous trauma The risk of recurrenceThe risk of recurrence Success of previous repairSuccess of previous repair Psychological aspects of the traumaPsychological aspects of the trauma
Then a combined decision concerning Then a combined decision concerning subsequent mode of birth and subsequent mode of birth and intrapartum care can be madeintrapartum care can be made

Any Questions or Any Questions or Comments?Comments?
Please leave a note on the Please leave a note on the Welcome Page to this websiteWelcome Page to this website