the total right/left-volume-index: a new and simplified...
TRANSCRIPT

The Total Right/Left-Volume-Index: A New and Simplified Cardiac Magnetic
Resonance Measure to Evaluate the Severity of Ebstein’s Anomaly of the Tricuspid
Valve: A Comparison with Heart Failure Markers from Various Modalities
Hösch et al: New Total R-/L-Volume-Index for Ebstein’s Anomaly
Olga Hösch1; Jan Martin Sohns2,4, MD; Thuy-Trang Nguyen1, MD; Peter Lauerer1, MD;
Christina Rosenberg2; Johannes Tammo Kowallick2; Shelby Kutty5, MD;
Christina Unterberg3,4, MD; Andreas Schuster3,4, MD, PhD; Martin Faßhauer2,4, MD;
Wieland Staab2,4, MD; Thomas Paul1, MD; Joachim Lotz2,4, MD;
Michael Steinmetz1,4, MD
1Department of Pediatric Cardiology and Intensive Care Medicine, Georg-August University,
Göttingen, Germany
2Institute for Diagnostic and Interventional Radiology, Georg-August University, Göttingen,
Germany
3Department of Cardiology and Pneumology, Georg-August University, Göttingen, Germany
4DZHK (German Centre for Cardiovascular Research)
5University of Nebraska Medical Center/ Children’s Hospital and Medical Center, Omaha,
NE
Correspondence to Dr.med. Michael Steinmetz Clinic for Pediatric Cardiology and Intensive Care Medicine University Medical Center Göttingen, Georg-August-University Robert-Koch-Str. 40, D-37075 Göttingen, Germany Tel: +49-551-39-22550 Fax: +49-551-39-22551 Email: [email protected] DOI: 10.1161/CIRCIMAGING.113.001467
Subject Codes: Diagnostic testing:[30] CT and MRI, Heart failure:[11] Other heart failure,
Diagnostic testing:[125] Exercise testing
ne, GGGGGGGeoeoeoeoeoeoorgrgrgrgrggg-A-A-A-A-A-AAugugugugugugugusu
a
a t
Cardiology and Pneumology, Georg-August University, Göttin e
anynynynyny
agggggnononononostic andd Innnteeerveveveentnnnn iooonanannn lll RaRaadioolllogygygygygy, GGeororg-AuAuA gugugugugust UUUUUnnivversrssit
Cardiolooooogygygygygy aaaaandndndndnd PPPneneneneneumumumumumololololologogogogogy,y,y,y,y GGGGGeoeoeoeoeorgrgrgrgrg-AAAAAugugugugugususuusu t tt UnUnUnUnUnivivivivivererererersisisisisityytytyty,,,,, GöGGGG ttinge
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from
2
Abstract
Background—The classification of clinical severity of Ebstein’s Anomaly (EA) still remains
a challenge. The aim of this study was to focus on the interaction of the pathologically altered
right heart with the anatomically -supposedly- normal left heart and to derive from cardiac
magnetic resonance (CMR) a simple imaging measure for the clinical severity of EA.
Methods and Results—Twenty-five patients at a mean age of 26 14 years with unrepaired
EA were examined in a prospective study. Disease severity was classified using CMR
volumes and functional measurements in comparison with heart failure markers from clinical
data, Electrocardiography, laboratory and cardiopulmonary exercise testing and
echocardiography. All exams were completed within 24 hours. A Total Right/Left-Volume-
Index was defined from end diastolic volume measurements in CMR: Total R/L-Volume-
Index = (RA+aRV+fRV) (LA+LV). Mean Total R/L-Volume-Index was 2.6 1.7 [normal
values: 1.1 0.1]. This new Total R/L-Volume-Index correlated with almost all clinically
employed biomarkers of heart failure: BNP (r=0.691,p=0.0003), QRS (r=0.432,p=0.039),
peak VO2/kg (r=-0.479,p=0.024), VE/VCO2 (r=0.426,p=0.048), the severity of tricuspid
regurgitation (r=0.692,p=0.009), tricuspid valve offset (r=0.583,p=0.004) and TAPSE
(r=0.554,p=0.006). Previously described severity indices ((RA+aRV)/(fRV+LA+LV)) and
fRV/LV EDV corresponded only to some parameters.
Conclusions—In patients with EA, the easily acquired index of right sided to left sided heart
volumes from CMR correlated well with established heart failure markers. Our data suggest
that the Total R/L-Volume-Index should be used as a new and simplified CMR measure,
allowing more accurate assessment of disease severity than previously described scoring
systems.
Key Words: heart defect, congenital; magnetic resonance imaging; heart failure
nnararararararary y y y yy y exexexexexexexerererererererciciciciciccisesesesesesese
A ToToToToToToTotatatatatatatalllllll RiRiRiRiRiRiRighghghghghghght/t/ttt L
ed from end diastolic volume measurements in CMR: Total R
R
1]. This new Total R/L-Volume-Index correlated with almost
eeeeed d d dd from eeendndndndnd dddddiaiaiaiaiastststststolololololicicicicic vvvvvolooloo umumummmeee memeeasssssuuuruu emememememenenntststsss iiiiinnn CMCMCMCMCMR:RRRR TTTTTotototototalalalalal R
RV+++++fRfRfRfRfRV)V)V)V)V) (L(L(L(LA+A+A+AA LVLVLVLV).).).).) MMMMMeannn nn ToToToToT tatat lll R/R/R/R//LL-LLL VoVoVoVoVolululululumememem I-IInddddndexeexexe wasas 2222.666
111]]]. TTThihis nenenenen w w ww ToToToTT tatatatatal l l R/R/R/R/R/L-L-L-LL VoVoVoVoVolululululumememememe-I-I-IIIndndndnn exexexexex ccccorororrererererelalalalalateteteteted d d dd wiwiwiwwiththththth allmosttt
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

3
Ebstein’s anomaly (EA) of the tricuspid valve (TV) is a rare and complex congenital cardiac
malformation with a highly variable morphology1–3, fist described in 18664. It comprises
<1% of all congenital cardiac malformations and occurs in about 1 per 200.000 live births5.
The dysplastic TV is offset towards the apex to more than 8 mm/m2 body surface area and
thereby causes an “atrialization” of the right ventricle (aRV)5,6. Significant tricuspid
regurgitation (TR), right atrial (RA) and right ventricular (RV) volume overload, altered
cardiac morphology7 and altered electrical synchrony of the contraction cycle as well as
Wolff-Parkinson-White syndrome are associated with the disease5,8. Progressive right heart
failure and impaired physical exercise capacity afflict many patients with EA at a quite early
stage in their life9. However, to date, it is unknown which aspect of the altered anatomy,
morphology, function and electrophysiology cause deterioration of cardiac function. Some
studies have addressed TV replacement as a feasible therapy, but optimal timing and long-
term success are difficult to assess10.
To date, no single, simple and reliable classification of severity has been described which
allows correlation of heart failure parameters with functional parameters derived from cardiac
magnetic resonance (CMR) or echocardiography. Different approaches have been reported,
such as size or volume of RA or aRV and TV morphology or patency11,12. A retrospective
study by Tobler et al.12 described a correlation of the functional right ventricular (fRV) end
diastolic volume (EDV) and a CMR based ratio of fRV EDV / left ventricular (LV) EDV
from transversal steady state free precession (SSFP) cine images with a number of
cardiopulmonary exercise measures. Defining the fRV in SSFP cine images is tedious due to
strong inter-individual variations of TV morphology and TV offset. A reliable, yet, time-
consuming method to calculate individual volumes, especially of the anomalous right heart,
has been demonstrated previously13. However, no standard segmentation rules have been set
for fRV and aRV. Different groups use different definitions, either including or excluding
sssssspepepepepepepectctctctctctct ooooooof f ff f f f thththththththe e eeeee alalalalalalalteteteteteteterrrrrr
on ofofofofofofof cccccccararararararardididididididiacacacacacacac fffffffunuup y gy
d i
g s
p y gy
drrrerr ssss ed TV VVVV rrreplplplp acacacacacemememememennnnntt ttt asasas a fffeasiiiblelelelele ttttheheheheheraapyppy, bububuutttt t opopppptititititimamammm l l lll tititititimmmimm
diffffffifififificucucucucultltltltlt to asssess10.
gglle, isimpmpmpplelelele aaandndndndnd rreleleelliaiaiablbllle e e e clclclclclasasasssisisiififififif cacacac tititittionononon ooooof f ff sesesevevevevev ririririr tytytytyy hhhhasasasasas bbbbbeeeeeee nn ddess
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from
4
parts of the aRV11,12. This impairs accuracy and reproducibility of volume and function
measurements.
We sought to define a simple and reliable CMR measure that correlates well with clinical
heart failure markers, allows a classification of the severity of EA and might also be used as a
prognostic factor. To test this hypothesis, we generated in a pilot study, a new, easily
acquired, end diastolic Total Right/Left-Volume-Index (Total R/L-Volume-Index) derived
from CMR SSFP cine stacks. This divides the volume of the right sided by that of the left
sided cardiac chambers. We compared the Total R/L-Volume-Index to a multitude of well-
established heart failure markers.
Methods
Study population: Fifty-eight living patients with EA were identified in the patient database
of the Department of Pediatric and Adult Congenital Heart Disease, University Medical
Center Goettingen, Germany. Of these, 4 patients were < 10 years, 3 had implantable
cardioverter-defibrillator (ICD) or pacemakers, 12 patients had major corrective surgery (2
Glenn, 2 Fontan, 1 TV-replacement, 7 TV reconstruction), 2 had complex associated
congenital heart defects (corrected transposition of the great arteries, double aortic arch), 1
suffered from claustrophobia and aborted the CMR scan, 8 patients were lost in follow-up
and 8 refused to participate in the study. Some patients met multiple exclusion criteria.
Twenty-five patients remained who fulfilled the study criteria, gave written informed consent
to participate in the study and were examined prospectively within one day from January
2013 until July 2013 in our outpatient Clinic. Inclusion criteria were EA, no TV or major
cardiac corrective surgery (other than atrial septal defect closure), age > 10 years and
t
e r
MeMeMeMeeththhthoddsss
n: FiFiFiiifftfff y-eighhhhhttt livingngngngg pppppatients withttht EA A weww re identnnn ifiedd d in the pat
ent ffof PPPPededededediaiaiaiaatrtrtrtrtricicicicic aaaaandndndndnd AAAAAdududududultltltltlt CCCCCoooongngngngngeneneene itititttalalalalal HHHHHeaeaeaaartrtrtrtrt DDDDDisisisisiseaeaeaeaeasesesesee, , , Uniiiver
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

5
sufficient compliance. The study protocol was approved by the local ethics committee and
was in accordance with the 1975 Declaration of Helsinki.
The study protocol comprised the following: detailed medical history, clinical examination,
laboratory testing, 12-channel standard Electrocardiography (ECG), 24h-Holter-ECG,
Cardiopulmonary exercise testing, echocardiography and CMR. Performance of CMR was
according to the guidelines in adults with congenital heart disease by the German Societies
for Cardiology and Pediatric Cardiology as well as the European Society for Cardiology14.
Clinical examination consisted of complete physical examination, including measurement of
transcutaneous oxygen saturation, blood pressure, heart rate (HR), bodyweight and height.
Laboratory testing was conducted with standard assays from clinical routine as used by and
officially certified for the Institute for Laboratory Medicine, University Medical Center
Goettingen. Measurements included full blood cell count, clinical chemistry and brain
natriuretic peptide (BNP).
12-channel resting ECG was recorded at 25 mm/s using Electrocardiograph ELI 250 and
VeritasTM –Software (Mortara Instruments, Inc., Milwaukee, WI, USA). ECG values of
interest were among others HR, PQ, QRS and QTc duration, delta wave, sings of heart block
and hypertrophy.
24h-Holter-ECG was performed using digital Holter-recorder H3+ and H-ScribeTM (Mortara
Instruments, Inc., Milwaukee, WI, USA). Measures of interest were HR range, origin and
frequency of any abnormal rhythm, bradycardia and HR variability.
Cardiopulmonary exercise testing was performed on a ZAN®600 (nSpire Health GmbH,
Oberthulba, Germany) using a ramp protocol with a total increase of 20 Watt/min.
Respiration gas flow was measured using a ZAN VIP (Variable Impedance
Pneumotachograph) flow sensor. Collected data was analyzed using ZAN-Tech Software.
Relevant values were maximal power, peak oxygen uptake (peak VO2), peak VO2 / heart beat
ccccclililililililininininininin cacacacacacacal l l ll ll rororororororoutututututututininininininine e ee ee e asasasasasasas
Unnnnnnnivivivivivivivererererererersisisisisisisitytytytytytyty MMMMMMMey , y
asurements included full blood cell count, clinical chemis r
d
i
y , y
asssuuru ementssss incncncclululululudededededed dd dd fufufufufulllllll bbblolololl odd celelelelellllll ccccoc ununntt, ccclinininininicalllll chchchhchemememememisisisisistr
de (BBBBBNPNPNPNPNP)).)))
iiingng EEECGCGCGGG wwwwasasass rrrecececcororordededeed d d atatataa 22225 5 5 55 mmmmmmmm/s/s/s/ uuuuusisisingngngn EEEEEleleleleectctctctrororoocacacaaardrdrdrddioioioiogrgrapaphh
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

6
(peak O2 pulse), expiratory volume per exhaled carbon dioxide (VE/VCO2), ECG changes in
repolarisation, minimal and maximal HR and minimal and maximal blood pressure.
Echocardiography comprised B- and M-Mode, pulsewave and continuous wave Doppler-,
Colour-Doppler as well as tissue-Doppler imaging in the standard views (short axis , long
axis, apical four chamber (4CV) and five chamber view (5CV), subcostal long and short axis,
suprajugular long and short axis) and was performed on an iE33 ultrasound system (Philips
Healthcare, Leiden, The Netherlands). Measurements and videos were electronically recorded
on MOD, using GE Carddas software (General Electrics, Fairfield, Connecticut, USA). Data
analysis comprised segmentation of epicardial and endocardial borders, calculation of volume
(according to Simpson’s method), ventricular mass, and fractional shortening as well as
ejection fraction (EF) and was performed using OsiriX© open source imaging software
V3.9.4 (Pixmeo Sarl, Bernex, Switzerland) as well as Image Arena (TomTec,
Unterschleißheim, Germany).
Measurements relevant for the study were fractional shortening (FS), EF, tricuspid annular
plane systolic excursion (TAPSE), TV offset compared to mitral valve insertion point in both
systole and diastole, RA, aRV, fRV, LV and left atrium (LA) areas in systole and diastole on
4CV, optically assessed TR (Nyquist Limit 61, gain 60%), and any abnormal morphological
features or additional malformations such as septal defects.
CMR: CMR scans were performed on a 1.5 Tesla MRI- “Symphony” scanner (Siemens
Medical, Erlangen, Germany). Phased-array-receiver coils were used to cover the thorax. All
patients were examined according to a standardized imaging protocol for EA. No sedation
was applied. The protocol included among others stacks of SSFP cine images in transversal
and ventricular short-axis orientation with a field of view (FOV) covering all cardiac
structures and great vessels, triplanar Half-Fourier Acquisition Single-Shot Turbo Spin-Echo
cccccctititititititionononononononalalalalalalal ssssssshohohohohohohortrtrtrtrtrr enenenenenenenininininininin
pen sososososososourururururururcecececececece iiiiiiimamamammamam g( ) p g p g
o Sarl, Bernex, Switzerland) as well as Image Aren
m
e u
( ) p g p g
o Sarl, BBBBBeeernenenenex,x,x,xx, SSSSSwiwiwiwiwitztztzeeerlallannnd) asasasasas wwwwwelell ll asasasaa IIIIImamamamaagegegegege AAAAArererereren
m, GeGeGeGeGermrmrmrmrmany))y)).
leleevananttt fofofofoor r r r ththththhe e e e stststudududuu y y y wewewew rerereree fffffrarararar ctctctctioioioioonananan l l l shshshorororo tetetenininniningngngngg (((((FSFSFSFSS),),),),, EEEEFFF, ttt iriccu
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

7
(HASTE) sequences and 2D through-plane phase contrast (PC) in flow measurements in the
ascending aorta and pulmonary trunk.
Measurements of ventricular function and mass were performed using stacks of multislice-
multiphase SSFP in ventricular short-axis as well as transversal planes, each with full
coverage of both ventricles and both atria. The following features were applied: TR=14 ms,
TE=2.6 ms, flip angle=20°, slice thickness=5 mm, spatial resolution 1.3x2.5 mm max,
parallel imaging acceleration factor 2, 20-30 phases per heart cycle according to HR, with
retrospective gating. Total examination time for each patient was approx. 30-45 minutes.
Segmentation of individual slices was performed for both transversal and short-axis stacks
using QMass and Visia Software (Medis, Leiden, The Netherlands). The areas in 4CV were
derived using OsiriX© open source imaging software v3.9.4, (Pixmeo Sarl, Bernex,
Switzerland). Endocardial and epicardial borders were defined manually for all patients by an
experienced imager (OH). Contours were controlled and approved in a blinded and
randomized fashion by a senior imager (MS, 4 years’ experience in CMR). In case of need
for contour adjustment, expert consensus was reached among MS, OH and JL (>10 years of
experience in CMR).
Contours were drawn in end systole and end diastole for RA, aRV, fRV, LA and LV.
Volumes, mass and EF were calculated using QMass Software (Medis, Leiden, The
Netherlands).
RA, aRV and fRV were defined as shown in Figures 1 and 2 for transversal and short-axis
orientation, respectively. Segmentation followed the method described by Fratz et al.11.
Unlike the method described by Yalonetsky et al.13, this is more tedious but describes the
anatomy of EA more accurately. In the methods of Fratz et al. the malformed TV is traced in
detail, while Yalonetsky et al. used an arbitrary line to define RA, aRV and fRV. LV and LA
segmentation in short-axis followed the AHA standards set by Cerqueira et al.16. CMR flow
ananananannandsdsdsdsdsdsds).).).).).).). TTTTTTThehehehehehehe aaaaaaarerererererereasasasasasasas
9 4 (P(P(P(P(P(P(Pixixixixixixixmememememememeooooooo Sp g g , (
docardial and epicardial borders were defined manually for all p
a
ion b a senior ima r (MS, 4 ears’ ex rience in CMR). In
p g g , (
dodododd cardial ananananand epepeppepicicicicicararararardididididialalalalal bbbbbooordedededd rs wwwerrrrreeeee dededededefififififineneedd ddd mmmamm nununununualalallallylylylyly fffffororrrr aaaaallllllllll p
ager (((((OHOHOOHO ).)) CCCContours were contttrolllllllled dddd andd ddd approv dded iiiin a
iionon bby a a a a seseseseninininn orororor iimamamamaagegegeer r r r (M(MMMMS,S,S,S, 4444 yyyyyeaeaeaearsrsrs’’’ exexexexpepepepp riririririenenenencececec iiin n n nn CMCMCMCMR)R). IInIn
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

8
quantification was performed in the ascending aorta and pulmonary trunk using a cine PC
sequence during breath-hold. Scanner settings for these measurements were as follows:
spatial resolution 1.7x1.7x5.5 mm3, TE/TR 3.2/75.4, flip angle 30°, encoding velocity 130–
450 cm/s, 20 phases. The outflow tract blood flow was measured through plane in an imaging
plane perpendicular to the arterial jet 1 cm distal to the valves. Magnitude and PC maps were
analyzed using commercially available software (QFlow, Medis, Leiden, The Netherlands). If
PC CMR flow measurements were repeated, the record with the highest peak velocity was
included in the analysis.
Normal reference values for the Total R/L-Volume-Index were calculated from four CMR
studies in the literature for healthy volunteers of a similar age17–20.
Statistical analysis was performed using Microsoft Excel (Microsoft Corporation, Redmond,
Washington, USA) and Statistica (Stat Soft, North Melbourne, Australia) in cooperation with
the Institute for Medical Statistics, University Medical Center, Goettingen, Germany.
Statistical methods included descriptive measures, correlation coefficients using Pearson
method for continuous variables and Spearman rank order correlation for ordinal variables
(NYHA classification and TR° visual) with the corresponding 95 % confidence interval
(using Fisher transformation) and p-values of the test r=0. Bland-Altman plots were used to
display the variation between transversal and short-axis view measurements. In addition the
p-values of the Bland-Altman test of bias = 0 are given.
Results
Data from 25 patients (72% male) who met the inclusion criteria for the study were analyzed.
Mean patient age was 26 14 years, 40% were < 18 years. Patient characteristics and
severity of EA assessed clinically are summarized in Table 1.
20.......
rosofoffffoffttttttt CoCoCoCoCoCoCorprprprprprprporororororororatatatatatatatioip g ( p
A o
r Medical Statistics, University Medical Center, Goettin
o u
p g ( p
A)A)A)AA and Staaatttitt stststiciciciica a a aa (S(S(S(S(Statatatatat SoSoSoSoSoftftft, NoNoNoNN rth h MeMeMeMeMelblblbbbouooouo rnrnne, AAAususususustrtrtrtt alalalalaliaiaiaiaia) )))) innnnn cccccoooooo
r MeMeMeMeMedidididd calll StStSt ttatiisiii tics, Uniiiiiversitytytyy MMMMM ddedddiici alllll CCCCCenter, GGGGGoetttttttinii ge
dodss iin lclududududedededed dddddesesescrcrcripipipptitiiivevevev mmmmmeaeaeaeaasusususurrresesess,,,, cccccorororo rererer lalaaaatitititiionononon ccccoeoeoeeeffffffffficiciciciciie tntntss u
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from
9
Plasma BNP-levels (mean: 74 127 ng/l) were increased in 16% of patients markedly above
the heart failure level (100 ng/l). Oxygen saturation was normal (> 95%) in all but one
patient.
All patients were in sinus rhythm. The QRS duration was prolonged > 110 ms in 64%, QTc
prolonged > 440 ms in 20% of the patients. Eleven patients (44%) had a complete right
bundle branch block. Performed 24h-Holter-ECG analysis showed singular supraventricular
and ventricular extrasystoles, but no higher grade arrhythmias.
During cardiopulmonary exercise testing peak VO2/kg was decreased in 92% and VE/VCO2
was increased in 38% of the study population.
On echocardiography most patients (60%) exhibited a moderate to severe TR. TAPSE
margined from 1.7 – 5.2 cm and was reduced < 2 cm in 24% and supra-normal > 4 cm in
16% of the study population. Biplane LV EF was decreased < 60% in 15 cases (60%).
Cardiac magnetic resonance
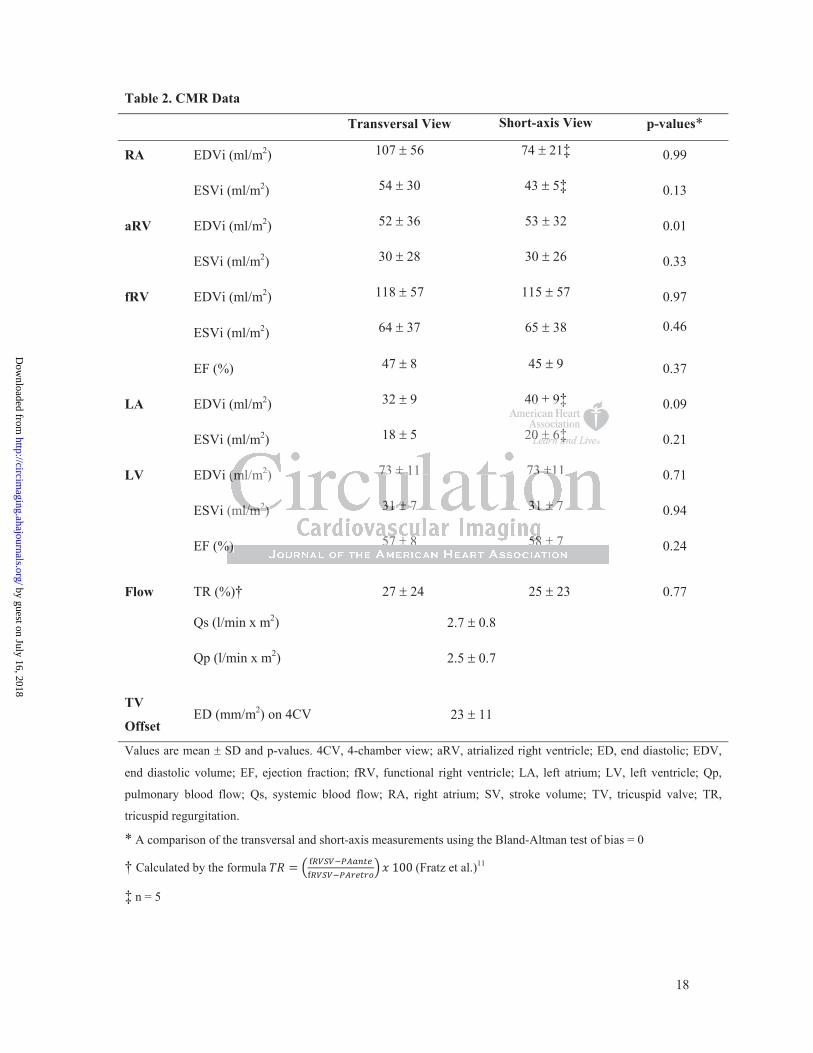
The CMR data of all 25 patients are summarized in Table 2. A comparison of transversal and
ventricular short-axis measurements using the Bland-Altman method showed significant
difference only in the aRV EDVi. In a comparison of TV offset (mm/m2) and the previously
described area derived severity index ((RA+aRV)/(fRV+LA+LV))15 from 4CV in
echocardiography and CMR, no relevant difference was found.
Severity Indices
Severity indices of EA in the study population as assessed from imaging modalities are
summarized in Table 3. Mean Total R/L-Volume-Index ((RA+aRV+fRV)/(LA+LV)) was 2.6
1.7 (limits: 1.2 – 7.7). Reference value for the Total R/L-Volume-Index calculated from
four studies with healthy volunteers in the literature17–20 was 1.1 0.1 (limits: 1.0-1.2) for
both children (8-18 years) and adults.
erererererereratatatatatatate e e e e ee totototototoo sssssssevevevevevevevererererererereeee eee
ddddddd.7 5.2 cm and was reduced 2 cm in 24% and supra norm
population. Biplane LV EF was decreased < 60% in 15 cases (6
i
f a
.7 5.2 cm and was reduced 2 cm in 24% and supra norm
ppppooopulationnn.n BBBipipipipiplalalalalanenenenene LLLLLVVV VV EFEE wwwas dddecccccrrrerr asasasasasedd << 666660%0%0%%% iiiiin 1515151515 cccaaasa esessss (6
ic resonanceeeee
ff lalll 2525 pppppatatatata ieieieieentntntntntssss ararararareeee sususuummmmmmmmmmarararararizizizizizededededed iiiiin n n n n TaTaTaaablblblblbleeee 2.2.2 AAAAA cccccomomomomompapapapapaririririisososososon fof tra
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

10
Correlation of different indices for severity with clinically assessed heart failure parameters
are summarized in Table 4. The CMR derived Total R/L-Volume-Index showed relevant
correlations with almost all clinically employed measures of heart failure like BNP, QRS and
QTc duration, peak VO2/kg, peak O2 pulse, VE/VCO2, systemic and pulmonary blood flow
and also with the severity of TR from both echo and CMR as well as TV offset and TAPSE.
These correlations are shown in Figure 3. Measurements of TR from echocardiography
compared to CMR (calculated by the formula (Fratz et al.)11)
showed a good correlation for calculation in transversal (p=0.0051) and short-axis views
(p=0.0054).
The previously described CMR derived score of fRV EDV/ LV EDV12 corresponded only to
some of the heart failure parameters defined above. Only a few correlations to heart failure
parameters were found for the widely employed TV offset (from CMR 4CV) and for the
originally echo based severity Index ((RA+aRV)/(fRV+LA+LV))15. Moreover, we calculated
an index of all right sided to left sided cardiac areas in echocardiography on end diastolic
4CV, which correlated only modestly with heart failure markers, as did a modified volume
severity Index ((RA+aRV)/(fRV+LA+LV)) (from CMR) and the index of RA/LA volumes
from CMR.
Discussion
To the best of our knowledge, this is the first prospective study to define a simple index from
CMR data of patients with EA and relate it with heart failure markers from different
modalities such as clinical presentation, ECG, laboratory and cardiopulmonary exercise
testing and echocardiography. Currently the timing of therapeutic interventions for EA is
primarily driven by symptoms5,21. The results of the present study provide an imaging based
VV VVVVV EDEDEDEDEDEDEDVVVVVVV1212121212122 cccccccorororororororrererererererespspspspspspspooooooo
rt failure parameters defined above. Only a few correlations to
w
right sided to left sided cardiac areas in echocardi graphy on
rt fafafafafailililililururururureeeee paaaaararrrr meters defined abobobobobovevvvv . Only a fewewewewew correlations to
fofofofofound for tttheee widededded ly empmm loyooyedd TVVVVV ofoofoo fsseeet (frfrrommm CMRMMRMM 4CVCVV
ased severitytytytyty IIIIIndndndndndexexexexex (((((R(R(R(R(RA+A+A+A+A+aRaRaRaRaRV)V)V)VV)/(/(/(/ fRfRfRfRfRV+V+V+VV LALALALALA+L+L+L+L+LV)V)V)V)V))))))15..... MoMM reover, w
righg t sidededededed dddd tototototo lllllefefefefeft tttt sisss dededeeded dddd cacacacacardrdrdrdrdiaiaiaiaiaccccc arararara eaeeas ssss ininininin eeechchchchchocococococararararardididididiogogogoo rararararaphphppp y yy on
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

11
classification of the severity of EA, which may serve as a predictive factor for the appropriate
timing of therapeutic interventions in this group of patients.
We defined a Total R/L-Volume-Index that presents a simplified CMR based correlation of
cardiac function and clinical severity of EA. It takes into account the overall mechanical
interaction of right and left side (transversal) as well as of the atrium with the ventricle
(longitudinal) of the malformed Ebstein’s heart. Instead of tediously tracing every individual
cardiac chamber - especially on the right side of the heart we propose to trace the right sided
cardiac chambers (i.e. RA, aRV, fRV) as a whole, ignoring the malformed TV and ill defined
atrial or ventricular borders, as well as the left sided cardiac chambers (i.e. LA, LV) as a
whole in order to obtain total volumes.
The Total R/L-Volume-Index appears to be a reliable and easy approach to assess clinical
severity of EA for the following reasons: The Total R/L-Volume-Index correlates very well
with most heart failure markers employed in clinical routine. This includes clinical
presentation (NYHA classification)22, laboratory tests (BNP)23, ECG (QRS duration)24,25,
cardiopulmonary exercise testing (peak VO2, VE/VCO2)12,23, echocardiography (TAPSE)26
and CMR (Cardiac Index)13,27,28.
The Total R/L-Volume-Index simplifies CMR segmentation and takes both atrio-ventricular
(longitudinal) and left-right (transversal) interactions into account. Tobler et al. were the first
to look at CMR functional data and a number of cardiopulmonary exercise measures in a
retrospective study. They proposed that a score of fRV/LV EDV from CMR could help to
classify the severity of EA12. However, the presented method to define fRV is challenging
with regard to reproducibility, since tracing of the TV can be difficult11,13. Unlike Tobler et
al., our study demonstrates a correlation of CMR data to peak VO2 and VE/VCO2, which in
adults with congenital heart disease is regarded as a predictor of poor outcomes as
hospitalization or death29.
sy apppppppppppppprororororororoacacacacacacachhhhhhh tototototototo app y pp
or the following reasons: The Total R/L-Volume-Index correla
t failure markers employed in clinical routine. This inc u
Y
pp y pp
oororoor tthe follooooowiwwww ngngngng rrrrreaeaeaeaeasssoss nsnsnsnsns: TTThehehehh Totottalllll RRRRR/L/L/L/L/L-V-V-Vololumumumuu e---e--InInInInIndededededex x xxx cococoocorrrrrrrrrreeelee a
t faffff ilililii uuuruu e maarkkkers employ dedddd iiiin cllllliiiniciiii lalll routititine. ThThThTT isiiii iiinclull
YYYHAHAHA cclalaaassssssssifififficiciiccatatata ioiooon)n)n)n))2222, ,,, lalabobobobborarararaatotototoryryryryy ttttesesestststststs ((((BNBNBNBNNP)P)P)P)P)2323,,,,, ECECECECCG G G G (Q(QRSRSRS
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

12
Previous studies have explored imaging data to reliably assess the severity of EA. However,
no easy and accurate measurement has been presented so far. Currently two classification
schemes for EA are used in echocardiography: The Severity Index by Celermajer et al.
measures the area of the RA and aRV divided by the area of the fRV, LA and LV
((RA+aRV)/(fRV+LA+LV)) from 4CV15. It is graded from I to IV (grade I: index <0.5, grade
II: 0.5-0.99, grade III: 1.0-1.49, grade IV >1.5). A more morphologic classification by
Carpentier et al.30 divides EA into groups A-D by analyzing the morphology of the TV and
the right sided heart chambers. Both classifications have not been shown to correlate with
peak VO2 or other heart failure markers12,23. Moreover, the Severity Index by Celermajer et
al. calculated from our data in echocardiography and CMR 4CV correlated with only a few
heart failure parameters.
We hypothesize, that an important clue to understanding the altered mechano-kinetics in EA
is an understanding of the longitudinal (i.e. base to apex or atrium to ventricle) and
transversal (i.e. right to left) mechanical and electrical interactions of the heart chambers. Our
Total R/L-Volume-Index appears to be a suitable imaging surrogate for these longitudinal
and transversal functional interactions.
In contrast, the severity index proposed by Celermajer et al. ((RA+aRV)/(fRV+LA+LV))
combines right and left sided cardiac areas that interact with each other on a longitudinal axis
(aRV and RA) while an important component of the longitudinal function of the right heart
(i.e. the fRV) is combined with left sided areas and function. Thereby, the score by
Celermajer et al. combines longitudinal and transversal interactions of the cardiac chambers,
possibly resulting in a less accurate description of the hemodynamic substrate in EA. In
previous studies, the Celermajer Severity Index did not correlate well with heart failure
parameters such as BNP or peak VO212,23.
CVCVVVVVV cccccccorororororororrererererererelalalalalalalateteteteteteted d d d d d d wiwiwiwiwiwiwittttttt
k
ding of the longitudinal (i.e. base to apex or atrium to v
ight to left) mechanical and electrical interactions of the heart ch
thththht at an immmmmpppopp rtrtrtrtanananananttttt clclclclclueeeee ttttooo uuunddeded rsstaaandndndndndinininininggggg ththt eee alalalalalteeereeeeed dd dd mememememechchchhchananananano-o-o-o-o-k
ding ofofofofof thehhh lllongigigitudidididiinal (i(i(i(i(i.e. babbb se tttto apex or atttriiiiium tttto v
ii hghttt ttoto llefefefefe t)t)t)t) mmmmececece hahaaaaninin cacacaallll ananannnd d d d elelelelecececectrtrtriciciciicalalall iintntntntn ererere acacaccctitititiiononononsss ofofofof ttttthehehehehe hheaea trtrt cchh
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

13
Within our cohort the Total R/L-Volume-Index correlated well with the different degrees and
levels of heart failure parameters described above. In addition, a comparison of the Total
R/L-Volume-Index from our study with an age matched healthy reference group derived from
the literature (Table 3)17–20 showed low i.e. normal values in healthy volunteers. Contrarily,
patients with EA had a higher i.e. abnormal Total R/L-Volume-Index, in parallel with an
increasing degree of heart failure.
Limitations
The study has inherent limitations of a cross sectional study with relatively small sample size.
The study cohort consisted of patients with heterogeneous age. Due to the low incidence of
EA, the statistical power was limited. A prospective longitudinal multi-center study would be
ideal to reach a more profound statistical power and to determine the impact of the Total R/L-
Volume-Index on operative timing and outcome. However, the size of our patient cohort is
comparable to patient numbers in previously published studies. Furthermore, only 20% of the
patients in our study cohort had a severe form of EA with overt symptoms of heart failure. PC
imaging of the TV for assessment of TR was not performed in this study. PC mapping of the
atrioventricular valve is generally more cumbersome and prone for errors because of the
movement of the valve annulus during ventricular systole, and this issue is likely exaggerated
in the Ebstein’s TV. Finally, we did not look at the prospective value of the proposed Total
R/L-Volume-Index. Since all patients were included in a registry we are optimistic that we
could obtain the prospective data in the future.
Conclusion
In patients with EA, the CMR derived Total R/L-Volume-Index correlated best with
established heart failure parameters as well as with the clinical status of the patient.
Moreover, this Total R/L-Volume-Index is very easy to obtain from either transversal or short
axis CMR stacks. We suggest that the Total R/L-Volume-Index may be used as a new and
alalallalll mmmmmmmululululululultititititititi-c-c-c-c-c-c-cenenenenenenenteteteteteteterrrrrr r stststststststuuuuuuu
e theeeeeee imimimimimimimpapapapapapapactctctctctctct ooooooofffffff thp p p
n operative timing and outcome. However, the size of our p i
atient numbers in previously published studies. Furthermore, onl
ud cohort had a severe form of EA with overt toms of hea
p p p
nnn nn oopo erative eeee tttimimimimimingngngngng aaaaandndndndnd outututcoommme.. Hooooowewewewewevevvvev r,r,, tthhehehh sizizizizize ofofofofof oooourururuur pppppataaaa i
atienttt nnununn mbbbberrs s iini pre iiviiiousllllly publblbllb iiishehhh dddd d sttttt duddddiiiei s. FFFurthththththermore, onl
dudy cocohohoooortrtrtt hhhhadadadadad aaa ssssevevevvverererre e e e fofoooormrmrmm oooof f f f EAEAEAA wwwwwititth h hh ovovovo erererere t t t t sysysysyympmpmpmpmptototooomsmsmsms ooff hheaa
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

14
simplified CMR measure, by which the severity of EA can be assessed more reliably than by
previously described severity scores. Further studies to validate the prognostic value of the
Total R/L-Volume-Index are planned.
Disclosures
None.
References
1. Dearani JA, Danielson GK. Congenital Heart Surgery Nomenclature and Database Project: Ebstein's anomaly and tricuspid valve disease. Ann Thorac Surg. 2000;69:S106-17. 2. Brown ML, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, Li Z, Hodge DO, Driscoll DJ. The outcomes of operations for 539 patients with Ebstein anomaly. JThorac Cardiovasc Surg. 2008;135:1120-36, 1136.e1-7. 3. Negoi RI, Ispas AT, Ghiorghiu I, Filipoiu F, Negoi I, Hostiuc M, Hostiuc S, Ginghina C. Complex Ebstein's malformation: defining preoperative cardiac anatomy and function. JCard Surg. 2013;28:70–81. 4. Ebstein W. Ueber einen sehr seltenen Fall von Insufficienz der Valvula tricuspidalis, bedingt durch eine angeborene hochgradige Missbildung derselben. Archiv für Anatomie, Physiologie und. 1866:238–254. 5. Attenhofer Jost CH, Connolly HM, Dearani JA, Edwards WD, Danielson GK. Ebstein's anomaly. Circulation. 2007;115:277–285. 6. Anderson KR, Lie JT. Pathologic anatomy of Ebstein's anomaly of the heart revisited. AmJ Cardiol. 1978;41:739–745. 7. Postma AV, van Engelen K, van de Meerakker J, Rahman T, Probst S, Baars MJH, Bauer U, Pickardt T, Sperling SR, Berger F, Moorman AFM, Mulder BJM, Thierfelder L, Keavney B, Goodship J, Klaassen S. Mutations in the sarcomere gene MYH7 in Ebstein anomaly. CircCardiovasc Genet. 2011;4:43–50. 8. Celermajer DS, Bull C, Till JA, Cullen S, Vassillikos VP, Sullivan ID, Allan L, Nihoyannopoulos P, Somerville J, Deanfield JE. Ebstein's anomaly: presentation and outcome from fetus to adult. J Am Coll Cardiol. 1994;23:170–176. 9. Kipps AK, Graham DA, Lewis E, Marx GR, Banka P, Rhodes J. Natural history of exercise function in patients with Ebstein anomaly: A serial study. Am Heart J. 2012;163:486–491. 10. Oxenius A, Attenhofer Jost CH, Prêtre R, Dave H, Bauersfeld U, Kretschmar O, Seifert B, Balmer C, Valsangiacomo Buechel ER. Management and outcome of Ebstein's anomaly in children. Cardiol Young. 2013;23:27–34. 11. Fratz S, Janello C, Müller D, Seligmann M, Meierhofer C, Schuster T, Schreiber C, Martinoff S, Hess J, Kühn A, Vogt M, Stern H. The functional right ventricle and tricuspid regurgitation in Ebstein's anomaly. Int J Cardiol. 2013;167:258–261. 12. Tobler D, Yalonetsky S, Crean AM, Granton JT, Burchill L, Silversides CK, Wald RM. Right heart characteristics and exercise parameters in adults with Ebstein anomaly: New
HHHM,M,M,M,M,M, WWWWWWWararrrrrrnenennnnn s s s CACACACACACACA,,,,,,,ntst wwwwwwwititititititith h h h h h h EbEbEbEbEbEbEbstststststststeieieieieieieinnnnnnn
as AT, Ghiorghiu I, Filipoiu F, Negoi I, Hostiuc M, Hostiuc ,n's malformation: defining preoperative cardiac anatomy and;
Ui fü
st C , Co o y , ea a J , dwa ds W , a e so G
as AAAAAT,TTTT GGGGGhihihihihioorororo ghiu I, Filipoiu F, NeNeNeNeN goi I, Hosoooo tiiiiiuucuuu M, Hostiuc S,n'n'n'n'n'ssss malfforororrrmammmm tititititiononononon::: dededededefififififinininininingngngngn ppppprrer opopperrrrratatataativivivivive ee cacacardrdrdrddiaiaiiaiac anananananatatatatatomomomomomy y yyy anaanana d;22222888:88 70–81.
Uebebebebeberr rrr eieieieieinenenen n nnn seseseeehrhrhrhrh seleleleleltetetetetennenn n nnnn FaFaFaFaFallllllllll vvvvvononononon IIIIInsnsnsnsnsufufufufuffifififif cicicicic enenene z zz dededededer rrrr VaVaVaVaalvlvlvlvl ulululuu aa aaaine angeborrrrreneneneene ee ee hohohohohochchchhchgrgrgrgrgradadadadadigigigigige e e e e MiMiMMM sssssssssbibibibibildldldl unununnggggg dededededersrsrrsr elelelelelbebebebebennnn.n Archiv fü18186666:2:23838–225454. ststst CCCHH,H, CCCCConononnononollllllllllyyy HMHMHMHMH ,, DeDeDeDD arararanananiii JAJAJAJAJA,, EdEdEdEdEdwawawardrdrdddsss WDWDWDWDWD,, DaDaDaDD nininiielelelsososonnn GGG
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

15
perspectives from cardiac magnetic resonance imaging studies. Int J Cardiol. 2013;165:146–150. 13. Yalonetsky S, Tobler D, Greutmann M, Crean AM, Wintersperger BJ, Nguyen ET, Oechslin EN, Silversides CK, Wald RM. Cardiac magnetic resonance imaging and the assessment of ebstein anomaly in adults. Am J Cardiol. 2011;107:767–773. 14. Kilner PJ, Geva T, Kaemmerer H, Trindade PT, Schwitter J, Webb GD. Recommendations for cardiovascular magnetic resonance in adults with congenital heart disease from the respective working groups of the European Society of Cardiology. Eur. Heart J. 2010;31:794–805. 15. Celermajer DS, Cullen S, Sullivan ID, Spiegelhalter DJ, Wyse RK, Deanfield JE. Outcome in neonates with Ebstein's anomaly. J Am Coll Cardiol. 1992;19:1041–1046. 16. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, Pennell DJ, Rumberger JA, Ryan T, Verani MS. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539–542. 17. Hudsmith LE, Petersen SE, Francis JM, Robson MD, Neubauer S. Normal human left and right ventricular and left atrial dimensions using steady state free precession magnetic resonance imaging. J Cardiovasc Magn Reson. 2005;7:775–782. 18. Sievers B, Addo M, Breuckmann F, Barkhausen J, Erbel R. Reference right atrial function determined by steady-state free precession cardiovascular magnetic resonance. JCardiovasc Magn Reson. 2007;9:807–814. 19. Sarikouch S, Peters B, Gutberlet M, Leismann, B., Kelter-Kloepping A, Koerperich H, Kuehne T, Beerbaum P. Sex-specific pediatric percentiles for ventricular size and mass as reference values for cardiac MRI: assessment by steady-state free-precession and phase-contrast MRI flow. Circ Cardiovasc Imaging. 2010;3:65–76. 20. Sarikouch S, Körperich H, Böthig D, Peters B, Lotz J, Gutberlet M, Beerbaum P, Kühne T. Reference values for atrial size and function in children and young adults by cardiac MR: a study of the German competence network congenital heart defects. J Magn Reson Imaging. 2011;33:1028–1039. 21. Bonow RO, Carabello BA, Chatterjee K, Leon AC de, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118:e523-661. 22. Paranon S, Acar P. Ebstein's anomaly of the tricuspid valve: from fetus to adult: congenital heart disease. Heart. 2008;94:237–243. 23. Trojnarska O, Szyszka A, Gwizda a A, Siniawski A, Oko-Sarnowska Z, Chmara E, Straburzy ska-Migaj E, Katarzy ski S, Cie li ski A. Adults with Ebstein's anomaly—Cardiopulmonary exercise testing and BNP levels. Int J Cardiol. 2006;111:92–97. 24. Hou Y, Fang P, Li H, Lei S, Bao J, Hu J, Yu J, Zhang S. Clinical analysis of arrhythmia in 297 Ebstein's anomaly patients. Chin Med J (Engl). 2012;125:3587–3588. 25. Assenza G, Valente AM, Geva T, Graham D, Romana Pluchinotta F, Sanders SP, Autore C, Volpe M, Landzberg MJ, Cecchin F. QRS duration and QRS fractionation on surface electrocardiogram are markers of right ventricular dysfunction and atrialization in patients with Ebstein anomaly. Eur Heart J. 2013;34:191–200.
......bel RRRRRRR.. ReReReReReReRefefefefefefeferererereererencncncncncncnceesculararararararar mmmmmmmagagagagagagagnenenenenenenetititititititicccccy y p g
nK
baum P. Sex-specific pediatric percentiles for ventricular size n
wKör rich H, Böthig D, Peters B, Lotz J, Gutberlet M, Beerba
ues for atrial size and function in children and young adults by c
y y p gn ReReReReResonnnn..... 200000000700 ;9:807–814.
PPPPeters B, GGGututututbebebebeberlrlrlrlrletetetetet MMMMM, LLeLeisisi mammannnn, B.B.B.B.B.,,, KKeKeKK ltlterererrr-KKKlololololoepeppppipipipipingngngng AAAAA, Kbaaaaauumumuu P. Seexxx-spspspecififififificiiii pppppededeee iiiatrriccc ppeeercececececentntntilless forr venenenenentriccccuuluuu arar sizizze
for cccccardiiiac MRMRMRMRMRI: assessment bybybyby stttteadddddy- ttsttattte free-precessiiionw. Circ Carrrrdididididiovovovovovasasasasasc cccc ImImImImImagagagagaginininininggggg. .. 202020202010100010;3;3;3;3;3:65–5–5–7676767676....KKKöörörpepeririiichchchcch HHH, ,, BöBöBöthththt igigg DDDD, PePePePeP teteteteersrsrsrs BBB, , ,,, LoLoLoootztztztzz JJJJ,,, GuGuGuGuG tbtbtbtbtbererere lelelleet t t t M,M,M,M,M, BBBBeeee brbaa
ueueuesss fofoforrr atatatriririalalal sssizizizeee anananddd fufufuncncnctititiononon iiinnn chchchililildrdrdrenenen aaandndnd yyyouououngngng aaadududultltltsss bybyby ccc
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

16
26. Nihoyannopoulos P, McKenna WJ, Smith G, Foale R. Echocardiographic assessment of the right ventricle in Ebstein's anomaly: relation to clinical outcome. J Am Coll Cardiol. 1986;8:627–635. 27. Steinmetz M, Preuss HC, Lotz J. Non-Invasive Imaging for Congenital Heart Disease – Recent Progress in Cardiac MRI. J Clin Exp Cardiolog. 2012;S8:008. 28. Lee CM, Sheehan FH, Bouzas B, Chen SSM, Gatzoulis MA, Kilner PJ. The shape and function of the right ventricle in Ebstein's anomaly. Int. J. Cardiol. 2012;167:704-710. 29. Diller G, Dimopoulos K, Okonko D, Li W, Babu-Narayan SV, Broberg CS, Johansson B, Bouzas B, Mullen MJ, Poole-Wilson PA, Francis DP, Gatzoulis MA. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation. 2005;112:828–835. 30. Carpentier A, Chauvaud S, Macé L, Relland J, Mihaileanu S, Marino JP, Abry B, Guibourt P. A new reconstructive operation for Ebstein's anomaly of the tricuspid valve. JThorac Cardiovasc Surg. 1988;96:92–101.
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

17
Table 1. Patients characteristics and severity of EA assessed clinically
Study cohort (n=25) n (%) or mean
SDmedian (limits)
Age (years) 26 14 23 (10-60)
< 18 years 10 (40)
Gender (male) 18 (72)
Height (cm) 170 14 172 (145-188)
Weight (kg) 72 25 77 (31-133)
BSA (m2) 1.8 0.4 1.9 (1.1-2.6)
BMI (kg/m2) 24 6 25 (15-39)
NYHA Classification
I
II
III
IV
20 (80)
3 (12)
1 (4)
1 (4)
BNP (ng/l) 74 127 28 (10-547)
QRS duration (ms) 115 30 110 (50-160)
QTc duration (ms) 412 29 413 (356-460)
Cardiopulmonary Exercise testing
Peak VO2 (% predicted) 67 22 72 (15-113)
VE/VCO2 (% predicted) 118 36 111 (88-245)
Peak O2 Puls (% predicted) 79 21 83 (26-114)
Echocardiography data
Tricuspid Regurgitation moderate 15 (60)
Apical TV Offset ED (mm/m2) 21 11 18 (8-49)
TAPSE (cm) 2.8 1.0 2.5 (1.7-5.2)
LV EF (biplane, Simpson) (%) 58 9 58 (29-71)
BMI, body mass index; BNP, brain natriuretic peptide; BSA, body surface area; ED, end diastolic;
EF, ejection fraction; LV, left ventricle; NYHA, New York Heart association; O2, oxygen;
TAPSE, tricuspid annular plane systolic excursion; TV, tricuspid valve; VE/VCO2, ventilatory
response to carbon dioxide production at anaerobic threshold; VO2, oxygen consumption.
1 (4)
s
y
1 (4)
7474747 11127222 282222 (((((1010101010-5-5-555474744747) ))) )
s))))) 115555 3330 110 0000 (5(5(5(5(50---1616166160)0))
s) 414141414122222 222229 9999 414141414 3 33 3 3 (3(3(3(3(356-460)
y EExer icisesesesese tttteseesestititititingnnnn
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from
18
Table 2. CMR Data
Transversal View Short-axis View p-values*
RA EDVi (ml/m2) 107 56 74 21‡ 0.99
ESVi (ml/m2) 54 30 43 5‡ 0.13
aRV EDVi (ml/m2) 52 36 53 32 0.01
ESVi (ml/m2) 30 28 30 26 0.33
fRV EDVi (ml/m2) 118 57 115 57 0.97
ESVi (ml/m2) 64 37 65 38 0.46
EF (%) 47 8 45 9 0.37
LA EDVi (ml/m2) 32 9 40 9‡ 0.09
ESVi (ml/m2) 18 5 20 6‡ 0.21
LV EDVi (ml/m2) 73 11 73 11 0.71
ESVi (ml/m2) 31 7 31 7 0.94
EF (%) 57 8 58 7 0.24
Flow TR (%)† 27 24 25 23 0.77
Qs (l/min x m2) 2.7 0.8
Qp (l/min x m2) 2.5 0.7
TV
Offset ED (mm/m2) on 4CV 23 11
Values are mean SD and p-values. 4CV, 4-chamber view; aRV, atrialized right ventricle; ED, end diastolic; EDV,
end diastolic volume; EF, ejection fraction; fRV, functional right ventricle; LA, left atrium; LV, left ventricle; Qp,
pulmonary blood flow; Qs, systemic blood flow; RA, right atrium; SV, stroke volume; TV, tricuspid valve; TR,
tricuspid regurgitation.
* A comparison of the transversal and short-axis measurements using the Bland-Altman test of bias = 0
† Calculated by the formula (Fratz et al.)11
‡ n = 5
40 9‡
202000000 66666‡‡‡‡‡‡‡
%
(((((mmlmm /m2) 7377 11 737337373 111111
(ml/l/l/l/l/mmmmm22))) 3131313131 77777 3333311111 77777
%%)) 575757 888 5555588888 777
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

19
Table 3. Severity indices of EA in the present study population assessed from imaging
modalities
Severity Index
4CV
Severity Index
4CV
fRV/LV –
Index
Severity Index
Volume
Total Right/Left -
Volume - Index
Study by Celermajer et al. (1992)
Yalonetsky et al. (2011)
Tobler et al. (2013)
Hösch et al.
Hösch et al.
Modality TTE CMR CMR CMR CMR
Measure Area Area Volume Volume Volume
Calculation (RA+aRV)/ (fRV+LA+LV)
(RA+aRV)/ (fRV+LA+LV)
fRV EDV / LV EDV
(RA+aRV)/ (fRV+LA+LV)
(RA+aRV+fRV)/ (LA+LV)
Results n
10-18 years 10 0.7 0.6 0.6 0.4 1.5 0.6 0.6 0.6 2.6 1.8
> 18 years 15 0.7 0.4 0.6 0.2 1.7 1.4 0.5 0.1 2.6 1.6
all 25 0.7 0.5 0.6 0.3 1.7 1.1 0.5 0.4 2.6 1.7
Reference* 1.1 0.1 1.1 0.1
Values are mean SD. 4CV, 4-chamber view; aRV, atrialized right ventricle; CMR, cardiac magnetic resonance imaging;
EDV, end diastolic volume; fRV, functional right ventricle; LA, left atrium; LV, left ventricle; RA, right atrium; TTE,
transthoracic echocardiography.
* Reference values from the literature, calculated in healthy subjects17–20. Reference results for children and adults are equal.
0.5 0.1
0000000.5.5.5.5.5.5.5 0000000.4.4.4.4.4.4.4
e
R
C
h17 20
CV,VVVV 44444-c-c-c-- hahahaaambmbmbmm eereee vvviieieii www;ww aaaaaRVRVRVRVRV,,,,, aatriririririalalalalalizizizizizeddddd rrrrrigigiggghththttt vvvvvenenenenentrrrrriciciciciclelelelele; ; ; ;; CMCMCMCMCMR,R,R,RR cccccarararrardididididiacaccacc mmmmmagagagaa nnnenn
fRV, functionononononalalalalal rrrigigigigighthththh vvvvvenenenenentrtrtrtrtriciciciciclelelelele; ; ; ; ; LALALALAL , leleleleleftftftftft aaatrtrtriuiuiuiuium;m;m;m;m; LLLLLV,VVVV llllefefefefeft t ttt ventricle; R
hhhy. 17 20
1.11111 0000.11111
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

20
Table 4. Comparison of Correlation of different indices for severity evaluation in the present study population with heart failure and functional parameters
Severity Index 4CV
fRV/LV – Index
Severity IndexVolume
Total Right/Left - Volume - Index
Study by Celermajer et al. (1992)
Tobler et al. (2013) Hösch et al.
Hösch et al.
Modality TTE CMR CMR CMR Measure Area Volume Volume Volume Calculation (RA+aRV)/
(fRV+LA+LV) fRV EDV / LV EDV
(RA+aRV)/ (fRV+LA+LV)
(RA+aRV+fRV)/ (LA+LV)
Clinical examination NYHA – Classification
r=0.499, p=0.011 CI=0.127-0.738
r=0.201, p=0.347 CI=-0.215-0.549
r=0.507, p=0.012 CI=0.128-0.747
r=0.401, p=0.052 CI=-0.002-0.683
Laboratory testing
BNP r=0.110, p=0.62 CI=-0.309-0.490
r=0.877, p<0.0001 CI=0.721-0.944
r=0.151, p=0.49 CI=-0.272-0.520
r=0.691, p=0.0003 CI=0.383-0.852
ECG
QRS duration r=0.581, p=0.004 CI=0.217-0.793
r=0.167, p=0.45 CI=-0.257-0.532
r= 0.530, p=0.009 CI=0.148-0.764
r=0.432, p=0.039 CI=0.024-0.707
QTc duration r=0.319, p=0.14 CI=-0.105-0.636
r=0.295, p=0.17 CI=-0.130-0.620
r=0.468, p=0.024 CI=0.068-0.728
r=0.465, p=0.029 CI=0.064-0.727
Cardiopulmonary exercise testing
Peak VO2 (% predicted) r=-0.257, p=0.25 CI=-0.601-0.180
r=-0.462, p=0.030 CI=-0.730-(-0.049)
r=-0.250, p=0.26 CI=-0.597-0.187
r=-0.479, p=0.024 CI=-0.740-(-0.070)
VE/VCO2 (% predicted) r=0.101, p=0.66 CI=-0.327-0.491
r=0.486, p=0.022 CI=0.079-0.744
r=0.182, p=0.42 CI=-0.253-0.550
r=0.426, p=0.048 CI=0.005-0.708
Peak O2 Puls (% predicted) r=-0.301, p=0.17 CI=-0.630-0.135
r=-0.436, p=0.042 CI=-0.714-(-0.017)
r=-0.410, p=0.058 CI=-0.699-0.014
r=-0.532, p=0.011 CI=-0.770-(-0.139)
Echocardiography
TR° visual r=0.108, p=0.608 CI=-0.294-0.474
r=0.660, p=0.001 CI=0.343-0.833
r=0.284, p=0.180 CI=-0.132-0.607
r=0.557, p=0.005 CI=0.194-0.776
TAPSE r=0.035, p=0.88 CI=-0.374-0.432
r=0.615, p=0.002 CI=0.266-0.812
r=0.222, p=0.31 CI=-0.204-0.571
r=0.554, p=0.006 CI=0.180-0.778
CMR
TV Offset r=0.655, p=0.001 CI=0.326-0.833
r=0.266, p=0.22 CI=-0.160-0.601
r=0.689, p=0.0003 CI=0.380-0.851
r=0.583, p=0.004 CI=0.220-0.794
TR (%)* r=-0.021, p=0.95 CI=-0.544-0.516
r=0.922, p<0.0001 CI=0.743-0.974
r=0.027, p=0.93 CI=-0.511-0.549
r=0.692, p=0.009 CI=0.220-0.889
Qp r=-0.260, p=0.39 CI=-0.689-0.324
r=-0.737, p=0.004 CI=-0.907-(-0.303)
r=-0.259, p=0.39 CI=-0.689-0.325
r=-0.683, p=0.010 CI=-0.886-(-0.204)
Qs r=-0.285, p=0.35 CI=-0.703-0.301
r=-0.643, p=0.018 CI=-0.869-(-0.138)
r=-0.217, p=0.48 CI=-0.665-0.362
r=-0.620, p=0.024 CI=-0.860-(-0.101)
Values are correaltion coefficients (r), corresponding p-values and 95% confidence intervals (CI). 4CV, 4-chamber view; aRV, atrialized right ventricle; BNP, brain natriuretic peptide; CMR, cardiac magnetic resonance imaging; EDV, end diastolic volume; fRV, functional right ventricle; LA, left atrium; LV, left ventricle; NYHA, New York Heart association; O2, oxygen; Qp, pulmonary blood flow; Qs, systemic blood flow; RA, right atrium; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspidal regurgitation; TTE, transthoracic echocardiography; TV, tricuspid valve; VE/VCO2, ventilatory response to carbon dioxide production at
r= 0.555555530303030303030, , , , , , p=p=p=p=p=p=p=0.0.0.0.0.0.0 000000000000009 9 9 99 99CI 0 217 0 793 CI 0 257 0 532 CI 0 148 0 764
t
r 0 101 p 0 66 r=0 486 p=0 022 r 0 182 p 0 42
CICCICIC =0=0==0=0.2.2. 1717171717-0--- .793 CI=-0.255557-7-7-7-7-0.532 CICCCC =0.148-0.764 r=0.311119,9,9,9,9, ppppp=0=0000.1.1.1.114 4 4 44CI=-0.10055-0.63336
r=r==r=0.0000 29292922 5, pp=0=0=0.11.1.1.177777CICI=-0.0..130-0--0.62626262620 0000
r=rr=rr 0.46464646468,8,8,8,8, ppppp=0=0=0=0=0.0.0.0.002424242424 CICICI==0.068686868-0-0- .77288
tinggggg
r=-0.257, p=p=p=p=p=0.0.0.00.2525252525 CICICI=-0.0.0.0 606060111-000.181818000
r=r=r=r=r=-0-0-0-0-0.4.4.4.4.46262626262,, p=p=p=p=p=0.0.0.0.0.03000CICICI=-000.737373000-(-(-(-( 0.00.040404449)9)9))
r=r==-0-0-0-0-0.2.2.2.2. 50, p=0.26 CICICI=-000.595959777-000.181818777
r=r=r=000 101010111 ppp=0=0=0 666666 r=r=r=00 484866 ppp=0=0 002222 r=r=r=000 181818222 ppp=0=0=0 444222
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

21
anaerobic threshold; VO2, oxygen consumption. * Calculated by the formula by Fratz et al. (see Tab. 2)11.
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

22
Figure Legends
Figure 1. Measurements of areas and volumes to define severity indices in Echocardiography
(A) and CMR (B-F). Definition of echo based Severity Index15 and apical offset of the septal
TV leaflet in end diastolic 4CV (A,B). Systolic and diastolic contours in transversal (C,D)
and short-axis view (E,F) to define functional values and volume severity indices in end
diastole.
Figure 2. Illustration of Total R/L-Volume-Index calculation in transversal view. The index
is defined as volumes of [right atrium (RA) + atrialized right ventricle (aRV) + functional
right ventricle (fRV)] [left atrium (LA) + left ventricle (LV)] in end diastole.
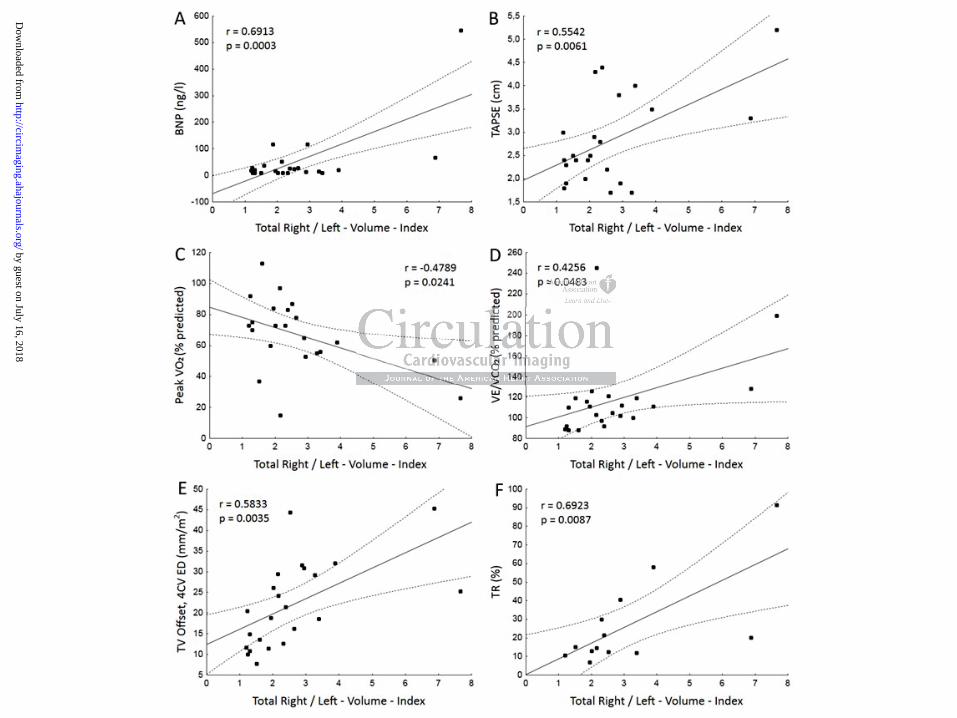
Figure 3. Correlations of Total R/L-Volume-Index and (A) BNP, (B) TAPSE, (C,D)
Cardiopulmonary exercise data and (E,F) CMR data. Depicted lines represent regression
straight with 95% confidence band. Spearman rank correlation estimates corresponding with
panels A-F were as follows: 0.27, 0.35, -0.44, 0.48, 0.71 and 0.62.
in end diastoleleleleeee.......
A) BBBBBBBNPNPNPNPNPNPNP (B(B(B(B(B(B(B))))))) TTATTTelations of Total R/L Volume Index and (A) BNP, (B) TA
y exercise data and ,F CMR data. De cted lines r re e
% p
elationons ofofof Total R/L Volume Indnnn ex and (A)A)A)A)A) BNP, (B) TA
y eeexercise dddataaa annnnnd d ddd (EEEEE,F,F) CMCMMRR daaaaatatatatata..... DeDepppicttttteeed lllllineeesee rreppppreeeeessess
% confffidenceeeee bbbbband. SSSSSpepppp arman rannnnk corrrrelation eseee timates corresp
as folloooowswswswws:::: 0.0.0.0.0.272727227, 0.0.0.0.0.353535355,,, -0-0- .4.4.4.4.44,4,4,44 00000.44.4.448,8,8,8,8, 0000.7.777711111 ananananand dd 0.0.0.0.0.6262626262.....
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Staab, Thomas Paul, Joachim Lotz and Michael SteinmetzTammo Kowallick, Shelby Kutty, Christina Unterberg, Andreas Schuster, Martin Faßhauer, Wieland Olga Hösch, Jan Martin Sohns, Thuy-Trang Nguyen, Peter Lauerer, Christina Rosenberg, Johannes
with Heart Failure Markers from Various ModalitiesMeasure to Evaluate the Severity of Ebstein's Anomaly of the Tricuspid Valve: A Comparison
The Total Right/Left-Volume-Index: A New and Simplified Cardiac Magnetic Resonance
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2014 American Heart Association, Inc. All rights reserved.
TX 75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas,Circulation: Cardiovascular Imaging
published online May 7, 2014;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/early/2014/05/07/CIRCIMAGING.113.001467World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information aboutnot the Editorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center,Circulation: Cardiovascular Imaging Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 16, 2018http://circim
aging.ahajournals.org/D
ownloaded from