the treatment of hyperkalemia: the old and the new - … summer meeting/pierce color...the treatment...
TRANSCRIPT
The Treatment of Hyperkalemia: The Old and the New
Dwayne A. Pierce, PharmD, BCPSClinical Pharmacist-Nephrology/Internal MedicineAugusta University Medical CenterAugusta, Georgia

Disclosures• I, Dwayne Pierce, have nothing to disclose concerning
possible financial or personal relationships with commercial entities (or their competitors) mentioned in this presentation
• There will be discussion of off-label uses of certain pharmaceutical agents and the use of agents not yet approved by the FDA

Objectives• Define hyperkalemia• Be able to describe the pathophysiology and mechanisms
of the correction of hyperkalemia• Compare the different treatment modalities (both
pharmaceutical and non-pharmaceutical) for hyperkalemia• Contrast the current ‘old’ treatment options with the new
treatments that have been developed

Potassium• Intracellular (98%) > extracellular (2%)• Normal serum concentration 3.5-5 mEq/ml• Necessary for proper physiologic functions
ElectrophysiologyMyocardial contractility
• ExcretionRenal (~81 mEq/day)Gastrointestinal (colon) (~9 mEq/day)Sweat (minimal)
• Primarily dietary sources (~75-100 mEq/day)
https://i.ytimg.com/vi/s0wkm-8QfCA/maxresdefault.jpgRaebel, Card therapeutics Clinical Methods, 3rd Ed.
Agarwal R, Gasteroenterology 1994

www.nutrientsreview.com

comicvine.gamespot.com
comicvine.gamespot.com

Renal Potassium Handling
https://upload.wikimedia.org/wikipedia/commons/7/72/Renal_Diuretics.gif

Hyperkalemia
• Serum potassium of > 5 mEq/L• Signs and symptoms
WeaknessElectrocardiographic changes Ascending paralysis
• Asystolic cardiac arrest
ECG Changes
Circulation. 2005;112:IC-121-IV121-IC-125.httpsquizlet.com11006395nur-120-unit-4-test-4-electrolytes-and-electrolyte-imbalances-flash-card
ECG Changes

Epidemiology• Hyperkalemia occurred in 3.2% of
total study population – 66,259 events in 2,103,422 veteran
records
• Risk increased in CKD patients and patients on Renin Angiotensin Aldosterone System (RAAS) inhibitors
• Hyperkalemia occurred in inpatient setting 52.7% versus outpatient 47.3%
Einhorn, Arch Intern Med 2009Weir, CJASN 2010
• Incidence of hyperkalemia with no risk factors on RAAS inhibitors <2%
• Incidence with patients on 2 RAAS inhibitors ~5%
• Incidence on RAAS inhibitors and with HF or CKD 5-10%

Odds of Mortality at 1 day
Einhorn, Arch Intern Med 2009

Risk Factors• Usually due to more than one factor• Known risk factors
– Kidney disease– History of diabetes– Age– Medications

http://www.zuniv.net/physiology/book/images/24-5.jpg
Renin Angiotensin Aldosterone System (RAAS)

Treatment of hyperkalemia• Depends on acuity of hyperkalemia
– Cause– Symptoms and/or ECG changes– Potassium concentration; >6.5 mEq/L may require more
aggressive therapy
Treatment methods• Remove exogenous potassium sources
– Oral supplements– Intravenous sources (i.e. potassium-containing
maintenance fluids)• Minimize dietary sources• Hold medications that may contribute to
hyperkalemia– RAAS antagonists– Potassium-sparing diuretics

Treatment of acute hyperkalemia
Intracellular shift • Insulin regular IV / Dextrose IV
• Beta agonists – Albuterol INH
• Sodium bicarbonate IV
https://quizlet.com/18971944/chapter-10-notes-by-paula-flash-cards/

Removal therapies• Dialysis
• Loop diuretics
• Potassium binding therapies– Sodium Polystyrene Sulfonate– Patiromer– Sodium Zirconium Cyclosilicate (ZS-9)*
Treatment of acute hyperkalemia
* Currently not approved by the FDA

Intracellular shift• Insulin (Regular IV)
– Activates the sodium/hydrogen exchange pump • Improves sodium/potassium adenosine triphosphatase function• Promotes the movement of potassium from the extracellular to
intracellular space
• Dextrose (IV) – hypoglycemia associated with insulin administration
• Calcium (IV) - Stabilizes the cardiac membrane
Pierce, Ann Pharmacother 2015

Insulin and Dextrose– REGULAR Insulin 5-10 units intravenously
» Intravenous insulin faster onset than subcutaneous
– Dextrose 25-50 grams • Onset immediate• Duration ~30 minutes
Balentine, Acad Emerg Med 1998www.cvs.com
Results of insulin use in hyperkalemia• Decreases potassium by 0.65 + 0.09 mEq/L
• Maximum effect seen within 1-2 hours of administration
• May cause hypoglycemia
Allon, Kidney Int 1990Kim, Nephron 1996
Hypoglycemia
• Risk of hypoglycemia with insulin– Exogenous insulin metabolized by the kidneys
• Half-life of insulin increased in renal failure– Duration of effect 4-8 hours
– Cases of hypoglycemia in hyperkalemia up to 6-7.5 hours post dose
Pierce, Ann Pharmacother 2015Williams, Postgard Med J 1988

HypoglycemiaAuthor Rate of Hypoglycemia Units of insulin Population
Schafers 8.7% (BG <70)
2.3% (BG <40)
5-10 units with variable amounts Dextrose
All levels of renal function
Apel 13% (BG <60)
5.8% (BG <50)
10 units with 25gm Dextrose ESRD patients
Pierce 16.7% (BG <70)
8.9% (BG <50)
10 units with 25gm Dextrose Low eGFR
Schafers, J Hospital Med 2012Apel, Clin Kidney J 2014Pierce, Ann Pharmacother 2015

Design Single-center, cross over studyn=12 on hemodialysis with hyperkalemia (>5 mEq/L on 3 occasions during a 1 month period)Insulin 10 units/25gm D50%, Albuterol 20mg inhaled over 10 min, and a combination of both on one of three occasions
Outcomes Primary endpoint: Maximum decrease in serum potassium
Results Baseline serum potassium levels similar for all groups - 0.65 (+0.09) mEq/L for insulin/dextrose- 0.66 (+ 0.12) mEq/L for albuterol- 1.21 (+ 0.19) mEq/L for combination
Lepage CJASN 2015
Albuterol and Insulin for Treatment of Hyperkalemia in Hemodialysis Patients

Sodium Bicarbonate• Hyperkalemia seen in acute acidosis• Increased blood pH drives K+ into cells• Conflicting data
– Schwarz, 1959 (case series)• 5% Sodium Bicarbonate • 144-408 mEq over 2-4 hours
– Corrected acidosis– Decreased K+
– Blumberg, 1988 (n=10) • No change in K+ after 60 minute infusion of isotonic and hypertonic
sodium bicarbonate
Blumberg, Am J Med 1988Schwarz, Circulation 1959Fraley, Kidney Int 1977

Removal Therapies

Dialysis• Hemodialysis - most effective method to remove excess potassium• Dialysate potassium concentration
– Two potassium (2K+) bath– Zero potassium (0K+) bath
• Used for short period in order to avoid hypokalemia• Reserved for severe symptomatic cases
• >100 mEq of potassium can be removed over 4 hours– Plasma-to-dialysate K+ concentration gradient– Blood and dialysate flow rates– Total body potassium

Diuretics• Loop diuretics
– Furosemide IV– Inhibits inward transport of potassium via the Na-K-Cl Co-
transporter 2 channel in thick ascending limb• Requires residual renal function• Intermediate rapidity of action (15 min – 1 hr)• May give with fluids if volume depletion a concern
Leinhardt, Pediatr Nephrol 2011Hollander-Rodriquez J, Am Fam Physician 2006

Potassium Binding Therapies

Sodium Polystyrene Sulfonate (SPS)• Introduced in 1958• No clinical studies to support its
use when introduced• First clinical studies in 1961
– Poor methodology
cmppharma.comBatterink CJHP 2015

Sodium Polystyrene Sulfonate (SPS)• Cation exchange resin• Cross-linked polymer with sulfone groups preloaded
with sodium• Exchanges Na+ for K+ in the large intestine• Can cause constipation• Available
– Powder– Premixed solution 15gm/60ml with 33% sorbitol– Enema in sorbitol
Kamel, Nephrol Dial Transplant 2012Varriale, Am J Med 2014

Sodium Polystyrene Sulfonate (SPS)• Oral
– Dose: 15-60gm divided once to four times daily• Rectal
– Use for patients who cannot take by mouth– 30-60gm given once to twice daily– Retain for as long as possible, then irrigate with non-saline fluid
(2000ml)
Kayexylate Prescribing information, Sanofi-aventis

FDA warning (2009)– Cases of intestinal necrosis associated with SPS– Other serious GI adverse events
• Bleeding• Ischemic colitis• Perforation
– Do not use in patients with non-normal bowel function– Do not use in patients at risk for constipation or impaction– Concomitant sorbitol with SPS has been implicated in colonic
intestinal necrosis
http://www.fda.gov/Safety/MedWatch/SafetyInformation/ucm186845.htm

Sodium retention• 4.1mEq (~100mg) sodium per 1gm SPS• 33% of sodium is exchanged and
retained• 30gm SPS x 100mg Sodium = 3000mg
Sodium• 3000mg Sodium x 0.33 = 1000mg • May be problematic in patients who are
sodium sensitive– Uncontrolled hypertension– Heart failure
Startupsarah.comVarriale, Am J Med 2014

Drug Interactions• Lithium• Thyroid products• Digoxin• Magnesium containing laxatives and antacids• Aluminum containing antacids
FDA Drug Safety Communication: FDA requires drug interaction studies with potassium-lowering drug sodium polystyrene sulfonate [10-22-15]
http://www.fda.gov/Drugs/DrugSafety/ucm468035.htmlKayexylate Prescribing information, Sanofi-aventis

Design Single center medical record review of patients from 2005-2010 n=14 with CKD and heart disease on RAAS inhibitors and daily SPS
Outcomes Hospitalizations, electrolyte levels and symptoms possibly attributable to SPS
Results Total of 289 days of follow-up with no colonic necrosis or life-threatening events attributed to SPSMild hypokalemia responding to dose reduction, no further hyperkalemia and no withdrawal or reduction of RAAS inhibitor therapy
Chernin, Clin Cardiol 2012
Secondary Prevention of Hyperkalemia With Sodium Polystyrene Sulfonate in Cardiac and Kidney Patients on Renin-Angiotensin-Aldosterone System Inhibition Therapy
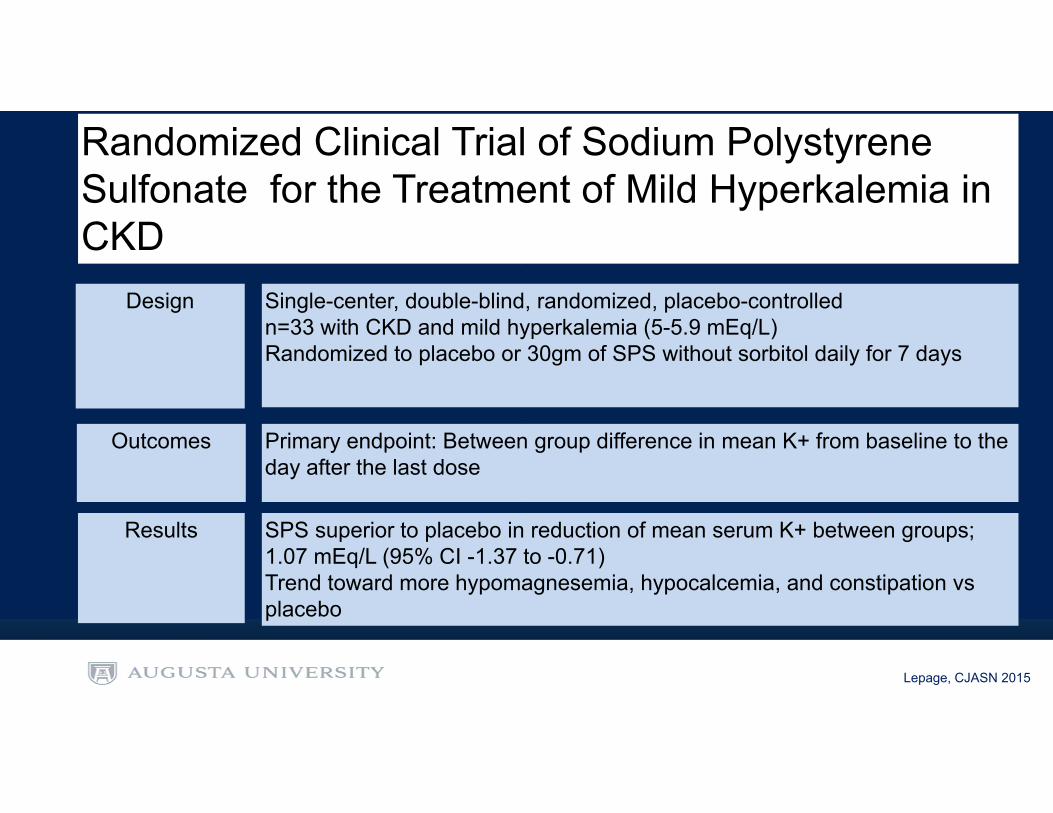
Design Single-center, double-blind, randomized, placebo-controlled n=33 with CKD and mild hyperkalemia (5-5.9 mEq/L)Randomized to placebo or 30gm of SPS without sorbitol daily for 7 days
Outcomes Primary endpoint: Between group difference in mean K+ from baseline to the day after the last dose
Results SPS superior to placebo in reduction of mean serum K+ between groups; 1.07 mEq/L (95% CI -1.37 to -0.71)Trend toward more hypomagnesemia, hypocalcemia, and constipation vs placebo
Lepage, CJASN 2015
Randomized Clinical Trial of Sodium Polystyrene Sulfonate for the Treatment of Mild Hyperkalemia in CKD

New Alternatives
Patiromer

Patiromer• Non-absorbed polymer • Binds K+ in exchange for Ca++• Does not swell and does not require cathartic • Acts in distal colon• Powder for suspension to be taken orally• Single-use packets of 8.4gm, 16.8gm, 25.2gm
Valtessa prescribing information, Relypsa

Design Phase III, multicenter, open-label, dose ranging trial,n=306 outpatients with K+>5 with type 2 DM and Stage 3-4 CKD on RAAS inhibitorsStratified to mild (5-5.5 mEq/L) or moderate (5.6-5.9) hyperkalemiaRandomized to 4.2, 8.4gm 12.6gm (mild) and 8.4gm, 12.6gm, 16.8gm (mod) PO BID
Outcomes Primary endpoint: Mean change in K+ from baseline to week 4 or until dose titrationSecondary endpoint: mean change in K+ from baseline to 52 weeks
Results Primary: Mean reduction of 0.35, 0.51, 0.55 (mild) 0.87, 0.97, 0.92 (moderate) p<0.001 for all vs baseline
Secondary: Significant reduction in K+ from baseline to 52 weeks
Bakris, JAMA 2015
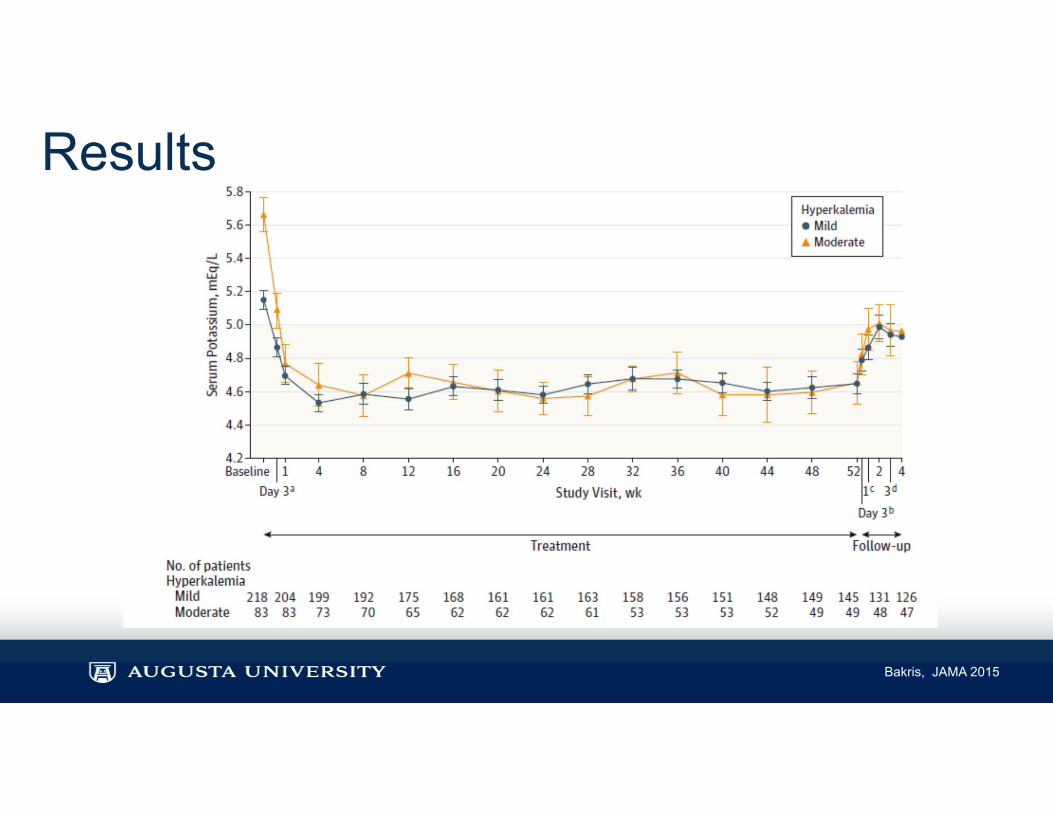
Results
Bakris, JAMA 2015

Adverse Drug Events• 20% of patients experienced adverse drug events
– Hypomagnesemia 8.6%– Hypokalemia 5.6%– Constipation 4.6%– Diarrhea 2.7%
Bakris, JAMA 2015

Design Multicenter, single-blind, randomized, placebo-controlled, two phasen=243, Stage 3-4 CKD on > 1 RAAS inhibitor with chronic hyperkalemia (5.1-6.4) Stratified to mild (5.1-<5.5) = 4.2gm or moderate (5.5-<6.5) = 8.4gm in initial phase, then randomized to same dose or placebo for 8 weeks (withdrawal phase)
Outcomes Primary endpoint (initial phase): mean change in K+ from baseline - week 4Primary endpoint (withdrawal phase): Difference between patiromer and placebo in median change in serum K+ from baseline - week 4 of withdrawal phase
Results Primary (initial): Mean serum K+ change; -1.01 + 0.03 mEq/L (95%CI -1.07 to -0.95), p<0.001) Primary (withdrawal): Difference in median change in serum K+ from baseline -week; 0.72 (95% CI 0.46 to 0.99) (p<0.001)
Weir, NEJM 2015

Adverse Drug Events• 47% of subjects with at least one ADE• Most common ADE were gastrointestinal
– Constipation 11%– Diarrhea 3-4%– Nausea 3%– Hypokalemia 3%
Weir, NEJM 2015

Patiromer Black Box Warning
Veltassa Prescribing Information, Relypsa Pharmceuticals 2015

Drug Interactions• Twenty-eight drugs tested• 50% of drugs tested demonstrated interaction (>30%
binding)• Cationic, anionic, and neutral drugs affected
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/205739Orig1s000ClinPharmR.pdf

Percent of Drug Bound>50% 30-50% <30%
Amlodipine Clopidogrel Allopurinol DigoxinCinacalcet Lithium Amoxacillin Glipizide
Ciprofloxacin Metoprolol Apixaban PhenytoinLevothyroxine Verapamil Aspirin Rivaroxaban
Quinidine Warfarin Atorvastatin SpironolactoneTrimethoprim Cephalexin Valsartan
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/205739Orig1s000ClinPharmR.pdf

Drug interactions, in vivo• Current labeling based on in vitro studies• Company conducting in vivo studies on previously listed
medications– 12 of 14 drugs interacting in vitro were tested in vivo
• 3 drugs demonstrated “clinically meaningful” reduced absorption when co-administered– Ciprofloxacin– Metformin– Levothyroxine
• When separated by 3 hours, no interactions present
Data on File, Relypsa, INC October 2015

Distribution• Obtained by individual outpatients through two national
specialty pharmacies only• Hospitals can obtain through authorized specialty
distributors

Sodium Zirconium Cyclosilicate (ZS-9)
http://www.zspharma.com/clinical-development/zs9/
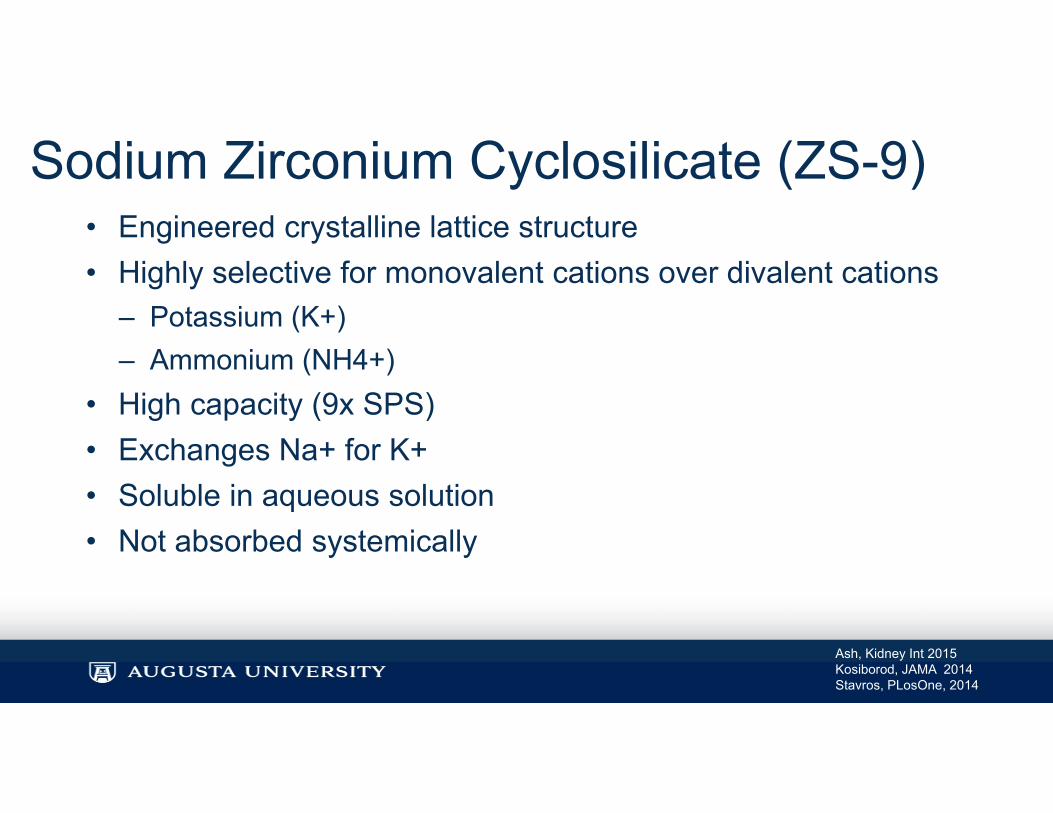
Sodium Zirconium Cyclosilicate (ZS-9)• Engineered crystalline lattice structure• Highly selective for monovalent cations over divalent cations
– Potassium (K+)– Ammonium (NH4+)
• High capacity (9x SPS)• Exchanges Na+ for K+• Soluble in aqueous solution• Not absorbed systemically
Ash, Kidney Int 2015Kosiborod, JAMA 2014Stavros, PLosOne, 2014

Design Phase II, multicenter, double-blind, placebo-controlled trial,n=90 in-patients with stage III CKD and K+ 5-6 mEq/Lrandomized 2:1 to 3 doses (0.3, 3, 10gm) of ZS-9 or placebo PO TID x 48 hrs
Outcomes Primary endpoint: Rate of decline in K+ from baseline at 48 hours,
Secondary endpoint: Significant decrease from baseline in K+ at 1 hour
Results Primary: 10gm vs placebo (-0.92 (+ 0.52) mEq/L at 38 hours) (p<0.0001)
Secondary: 10gm (-0.11 + 0.46 mEq/L) vs placebo (0.12 + 0.36 mEq/L), p=0.02
Ash, Kidney Int 2015

Results
Ash, Kidney Int 2015

Adverse Drug Events• No serious adverse drug events• No change in Mg++, Ca+, or Na+• No hypokalemia• Gastrointestinal ADE in ZS-9
– Vomiting 13%– Nausea 8%– Diarrhea 4%
Ash, Kidney Int 2015

Design Phase III, multicenter, double-blind, placebo-controlled trial, n=753 ambulatory outpatients with K+ 5-6.5 (63-71% on RAAS inhibitors)Randomized to 4 doses of ZS-9 or placebo PO TID x 48 hours, thennormokalemic subjects randomized 1:1 to same dose daily or placebo for days 3-14
Outcomes Primary endpoint: Exponential rate of change in serum K+ at 48 hrsSecondary endpoint: Between group difference in mean absolute change in K+
Results Primary: Mean exponential reduction of 0.3% with 10gm ZS-9 vs 0.09% for placebo(<0.001)Secondary: Mean absolute change in K+ of -0.73 for 10gm vs placebo
Packham, NEJM 2015
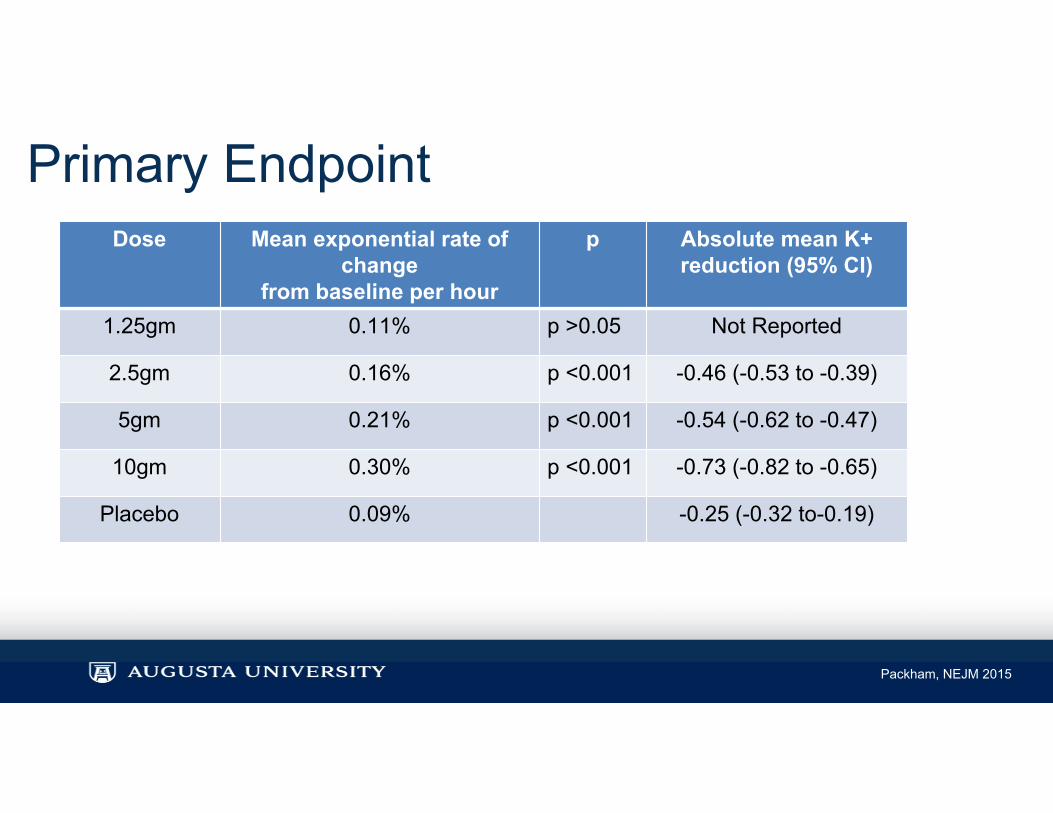
Primary EndpointDose Mean exponential rate of
changefrom baseline per hour
p Absolute mean K+ reduction (95% CI)
1.25gm 0.11% p >0.05 Not Reported
2.5gm 0.16% p <0.001 -0.46 (-0.53 to -0.39)
5gm 0.21% p <0.001 -0.54 (-0.62 to -0.47)
10gm 0.30% p <0.001 -0.73 (-0.82 to -0.65)
Placebo 0.09% -0.25 (-0.32 to-0.19)
Packham, NEJM 2015

Adverse Drug Events• Initial Phase
– ZS-9 12.9% vs placebo 10.8% • Maintenance Phase
– ZS-9 25.1% vs placebo 24.5%• Diarrhea (ZS-9 vs placebo)
– Initial phase: 1.8% vs 2.5% – Maintenance phase: 1.7% vs 2.2%
• Hypokalemia– 2 cases with ZS-9
• No edema
Packham, NEJM 2015

Design Phase III, multicenter, randomized, double-blind, placebo-controlledn=258 adult ambulatory patients with K+ > 5.1 mEq/LOpen label treatment phase 10gm TID for 48 hours If normokalemic, then randomized to 5,10,15 gm or placebo daily for 28 d
Outcomes Primary endpoint: Comparison of mean serum K+ levels between placebo and each treatment group during days 8-29 of randomized phase
Secondary: proportion of patients who were normokalemic at 29 days
Results Maintenance: Mean between group differences in mean K+ for ZS-9 vs placebo = -0.3 mEq/L, -0.6 mEq/L, and -0.7 mEq/L Secondary: 71%, 76% and 85% vs 48% for placebo (p=.01, 0.002, and <0.001)
Kosiborod, JAMA 2014

Adverse Drug Events• Comparable between ZS-9 and placebo• Edema (maintenance phase)
– 6% of 10gm– 14.3% of 15gm– 2.5% with placebo
• Gastrointestinal adverse events– 9% in 15gm group vs 14% with placebo
• Hypokalemia (maintenance phase) – 10.7% of 15gm– 9.8% of 10gm– none with placebo
Kosiborod, JAMA 2014
FDA approval• May 2016
– FDA approval denied due to manufacturing issues– No additional clinical trials requested– Manufacturer states it is addressing the issues– Will appeal ruling with new anticipated approval 2017

New Agents• Onset
– Patiromer 7 hours (-0.2 mEq/L)– ZS-9 1 hour (-0.11 mEq/L)
• Majority of studies were in the ambulatory setting• Most dealt with chronic hyperkalemia• 60-70% of subjects were on RAAS inhibitors• Most studies excluded stage 5 CKD (ESRD)

ComparisonDrug Advantages DisadvantagesSodium Polystyrene Sulfonate (SPS)
• Established use in acute treatment
• Variable onset• Risk of severe gastrointestinal
adverse events• Risk of Na+ retention• Possible revised drug interaction
profile• Non-selective for K+
Patiromer • Exchanges Ca++ for K+• Daily dosing for chronic use• Effective at reducing K+• Mild GI adverse drug events
• Onset 7 hours• Drug interactions and inflexibility
of dosing• Potential non-selectivity for K+
Sodium Zirconium Cyclosilicate (ZS-9)
• Shorter onset than Patiromer• More selective for K+• Mild adverse drug events
• Possible problems with Na+ retention
• Unknown drug interaction profile
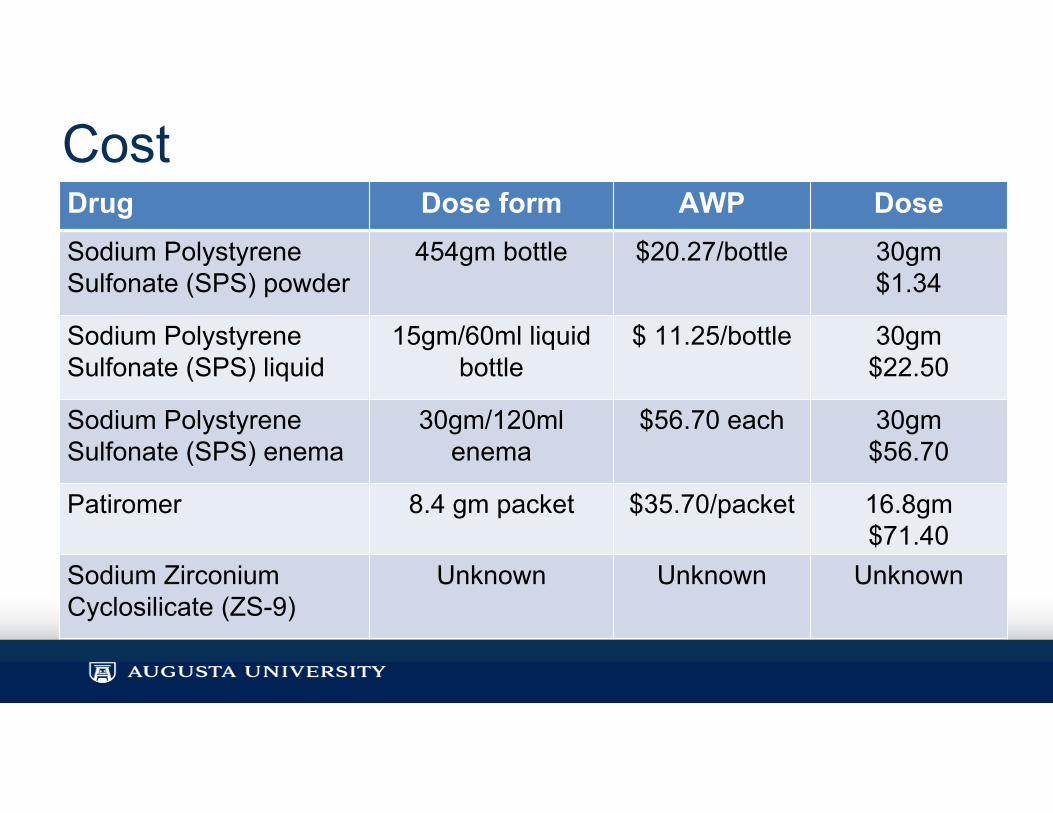
CostDrug Dose form AWP DoseSodium Polystyrene Sulfonate (SPS) powder
454gm bottle $20.27/bottle 30gm$1.34
Sodium Polystyrene Sulfonate (SPS) liquid
15gm/60ml liquid bottle
$ 11.25/bottle 30gm$22.50
Sodium Polystyrene Sulfonate (SPS) enema
30gm/120ml enema
$56.70 each 30gm$56.70
Patiromer 8.4 gm packet $35.70/packet 16.8gm$71.40
Sodium Zirconium Cyclosilicate (ZS-9)
Unknown Unknown Unknown

Summary• Newer binding therapies primarily studied for outpatient chronic use
• Newer agents may provide advantages over SPS in chronic patients– Lower rates of adverse effects– More selectivity for potassium– More rigorous efficacy data
• Based on onset of action, Patiromer likely unsuitable for acute treatment of hyperkalemia
• Use of ZS-9 for acute hyperkalemia needs to be investigated further
• The incidence of sodium retention and edema with ZS-9 requires further investigation

Conclusions• Niche drugs
– Outpatient for chronic hyperkalemia from RAAS antagonists
• Use for acute treatment of inpatient mild-moderate hyperkalemia unclear and unstudied– Patiromer unlikely effective due to 7 hour onset– ZS-9 shorter onset

Questions?
en.hdvo.org
The Treatment of Hyperkalemia: The Old and the New
Dwayne A. Pierce, PharmD, BCPSClinical Pharmacist-Nephrology/Internal MedicineAugusta University Medical CenterAugusta, Georgia

Question 1The treatment of hyperkalemia consists of two basic methods: drive the potassium intracellularly and remove potassium from the body.
A) TrueB) False

Question 2Which FDA approved potassium binding agent has a black box warning concerning the binding of other medications necessitating a separation of 6 hours from the agent?
A) Sodium Polystyrene SulfonateB) PatiromerC) Sodium Zirconium CyclosilicateD) Sorbitol

Question 3What adverse effect is most associated with the combination of calcium/insulin/ and dextrose for the treatment of hyperkalemia?
A) Athlete’s footB) SneezingC) HypoglycemiaD) Headache