the use of mri and psma pet ct to guide salvage therapy · psma pet ct to guide salvage therapy...
TRANSCRIPT

The use of MRI and
PSMA PET CT to
guide salvage
therapy
Peter Black
Vancouver Prostate Centre
University of British Columbia

Financial and Other
Disclosures
I have the following financial interests or
relationships to disclose: Disclosure code
Astellas, Janssen, Merck, Roche, Bayer, Sanofi,
Lilly, Spectrum, Sitka, Cubist, BioCancell,
AbbVie, Ferring
C
New B Innovation, iProgen, GenomeDx S
Treatment of localized prostate ca
Ablative therapy
Radical
prostatectomy
External beam
radiation
Brachytherapy
Salvage
therapy

The nihilistic view of salvage
those who are likely to die of their disease will not be
rescued by salvage therapy
we don’t know where to treat because we are
treating PSA only and cannot visualize recurrence
ADT is as good as anything else we have to offer
local salvage therapy causes unacceptably high
rate of complications
major impact on quality of life

But the tides are shifting…..
More aggressive
intervention for high
risk/advanced
prostate cancer
Better imaging:
• mpMRI
• PSMA-PET
More precise
salvage therapy:
• SBRT
• ablation

Salvage after prostatectomy
1. Is PCa confined to the pelvis so that patient has
potential to respond to salvage RT?
2. Is there PCa in lymph nodes that can be surgically removed or targeted by SBRT?
3. What to do about oligometastatic recurrent PCa?

Local salvage after
radiotherapy or ablation
Some of same issues, but also:
Is the cancer localized to the prostate?
Multiparametric MRI for
identification of local recurrence
currently: local recurrence = absence of
distant recurrence based on bone scan,
CT scan and clinical risk stratification
in addition, disease in prostate post-RT determined
by systematic biopsy
can mpMRI be used to identify local
recurrence in prostatic fossa after RP
or in prostate after RT/ablation?

Multiparametric MRI post RP
88 patients with BCR after RP
median PSA 0.30 ng/mL (IQR 0.19-0.72 ng/mL)
24% had visible lesion on mpMRI
Liauw et al, Int J Radiat Oncol Biol Phys. 2013

Multiparametric MRI post RT
or ablation therapy
diffusely low T2 DCE color map ADC

UCL Experience
Kanthabalan et al Clin Oncol 2016 in press

UCL Experience
Kanthabalan et al Clin Oncol 2016 in press

UCL Trial – “FORECAST”
FOcal RECurrent Assessment and Salvage Treatment
(NCT01883128)
prior RT ± ADT; BCR according to Phoenix
plan n=177 (prospective, multicentre)
incorporates:
1. whole body MRI (compared to bone and choline PET/CT)
2. MRI-fusion biopsy
3. transperineal mapping biopsy
4. focal salvage HIFU/cryo
Study Chair: Hashim Ahmed, University College London

What about PET-CT for target
identification after BCR?
11C-choline has been superseded by 68Ga-PSMA
only ≈1300 men with PSMA PET-CT published in
the literature
suggests PPV >90%
but NPV remains unknown
need pathology or at least follow-up imaging!
information about local, nodal and distant sites

Recurrence in bone
Maurer et al Nat Rev Urology 2016

Recurrence in pelvic lymph node
Maurer et al Nat Rev Urology 2016
Heidelberg Experience
319 patients (292 with recurrence; 226 post-RP)
median serum PSA 4.6 ng/ml
≥1 suspicious lesion found in ~83% of patients
histological confirmation 42 patients:
all lesions with positive 68Ga-PSMA–PET signal had histologically
confirmed metastatic prostate cancer (n = 98)
lesion based 77% sensitivity, 100% specificity, 91% NPV and 100% PPV
29 lymph nodes missed in 3 patients (all had disease elsewhere)
one local relapse with follow-up
Afshar-Oromieh et al Eur J Nucl Med Mol Imaging 2015
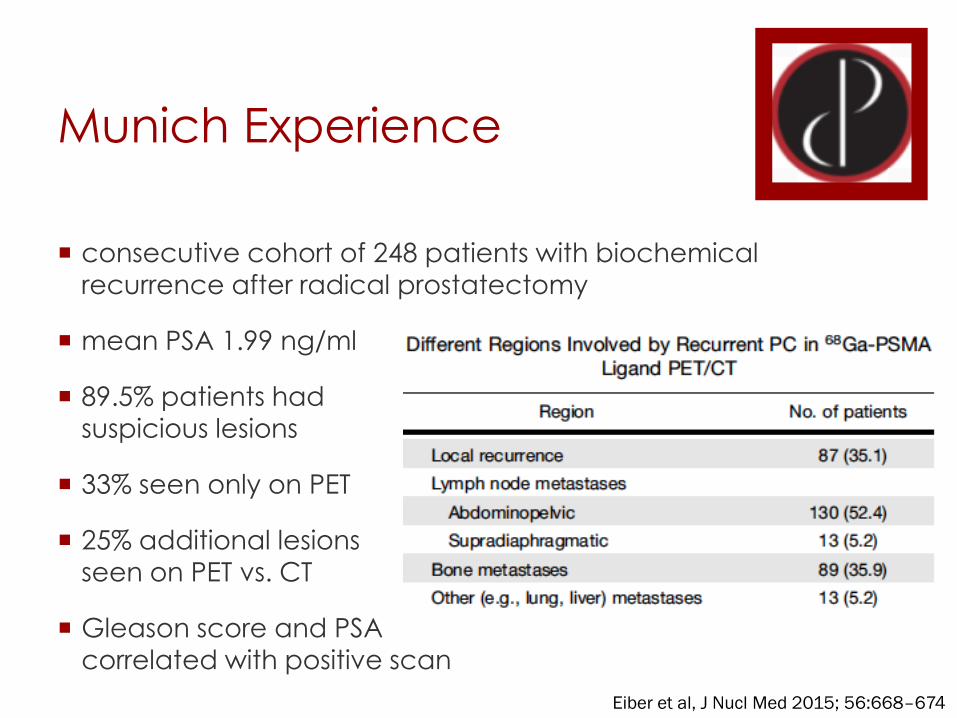
Munich Experience
consecutive cohort of 248 patients with biochemical
recurrence after radical prostatectomy
mean PSA 1.99 ng/ml
89.5% patients had
suspicious lesions
33% seen only on PET
25% additional lesions
seen on PET vs. CT
Gleason score and PSA
correlated with positive scan
Eiber et al, J Nucl Med 2015; 56:668–674

Histopathologic Confirmation
Munich Experience
48 men with median PSA 1.3 underwent PLND after PET/CT or PET/MRI
performance by lymph node “fields”:
97% specificity
78% sensitivity (27% sensitivity of CT/MRI alone)
Rauscher et al, J Nucl Med 2016 in press

What is best PSA cut-off for
obtaining PSMA-PET/CT?
clinical dilemma:
salvage RT best administered at PSA < 0.5 ng/dl
but PSMA-PET/CT most sensitive at higher
Eiber et al, J Nucl Med 2015; 56:668–674

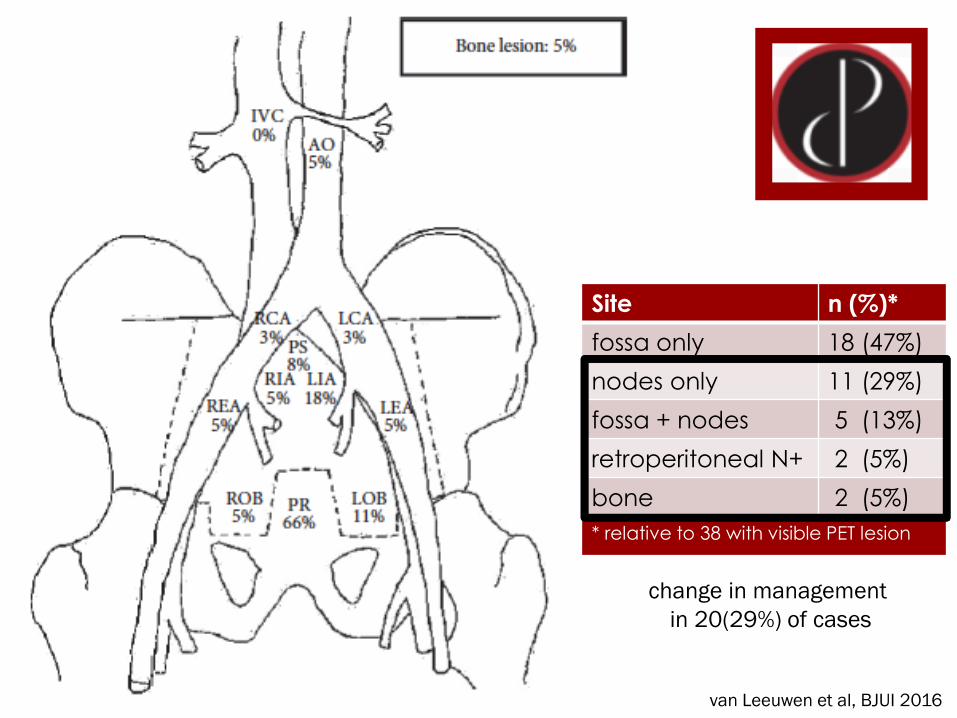
Sydney Experience PSA<1.0
n=300 PSMA-PET in
6 months in 2015!
n=70 in men with BCR post RP considering
salvage RT
PSA>0.05 but <1.0
53 lesions in 38
patients (54%)
van Leeuwen et al, BJUI 2016
van Leeuwen et al, BJUI 2016
Site n (%)*
fossa only 18 (47%)
nodes only 11 (29%)
fossa + nodes 5 (13%)
retroperitoneal N+ 2 (5%)
bone 2 (5%)
* relative to 38 with visible PET lesion
change in management
in 20(29%) of cases
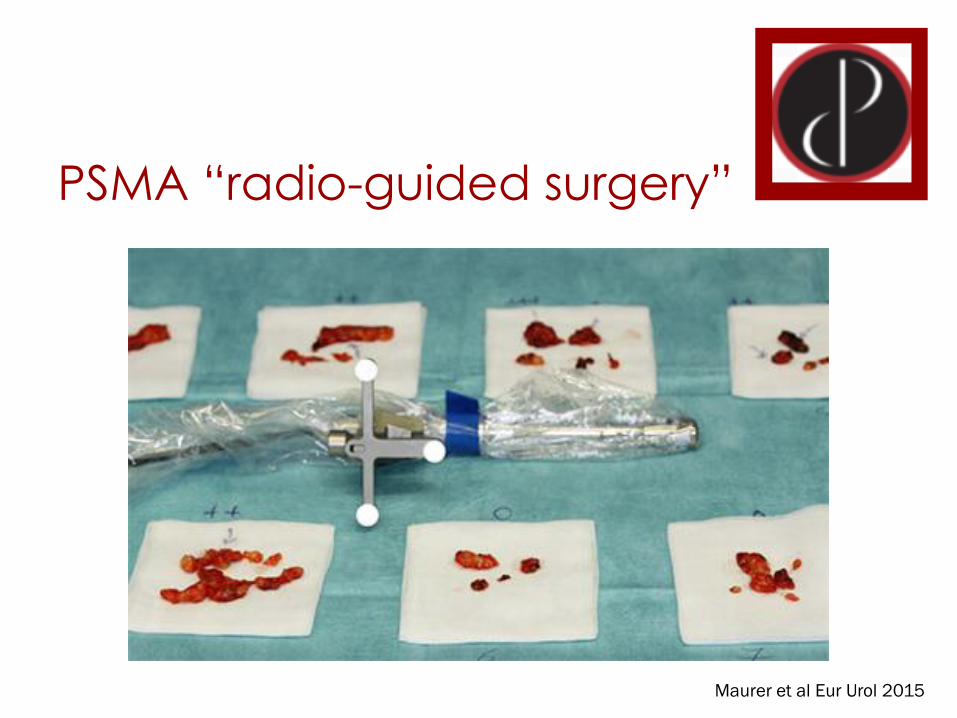
PSMA “radio-guided surgery”
Maurer et al Eur Urol 2015

Conclusions
salvage therapy after failed primary treatment has
been relatively neglected up to now
advanced imaging enhances our ability to define the extent and location of recurrent disease
mpMRI enables salvage ablative therapy to the
prostate after RT
PSMA-PET facilitates salvage PLND or SBRT, although
true impact of interventions requires more study
delay systemic therapy, but improved outcomes?
clinical trials need to catch up with technology
PET-MRI and other advances (e.g. new radiotracers)
are likely to continue to improve resolution of imaging and precision of salvage therapy

Emerging frontrunner: 18F-DCFPyL-PSMA
18F has potential advantages over 68Ga:
more favorable dosimetry – can inject higher dose
lower energy of emitted protons – higher spatial
resolution
mass production (vs. local production on-site)
head-to-head comparison in BCR patients:
better tumor-to-background ratio; higher SUV values
higher rate of detection
Dietlein et al, Mol Imaging Biol 2015
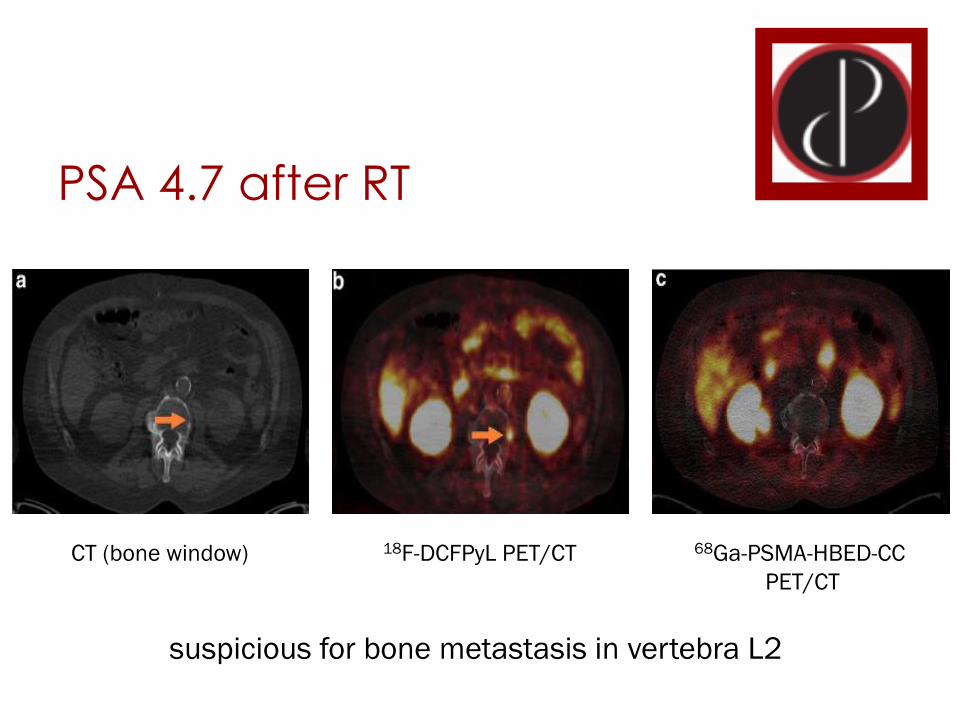
PSA 4.7 after RT
CT (bone window) 18F-DCFPyL PET/CT 68Ga-PSMA-HBED-CC
PET/CT
suspicious for bone metastasis in vertebra L2

PSMA-PET/MRI
Eiber et al Eur Urol 2016 in press

Evolving paradigm
RP
Biochemical
recurrence PET-MRI EBRT/BT
Ablation
Salvage
PLND
SBRT for
oligo-
metastatic
Systemic
therapy for
widely
metastatic
Local
salvage
(prostate)