the visitor's regard of their need for support, comfort, information proximity and assurance in...
TRANSCRIPT

Intensive and Critical Care Nursing (2012) 28, 263—268
Available online at www.sciencedirect.com
journa l h om epage: www.elsev ier .com/ iccn
ORIGINAL ARTICLE
The visitor’s regard of their need for support,comfort, information proximity and assurance in theintensive care unit
Grete Høghauga,∗, May Solveig Fagermoenb,c,1, Anners Lerdalb,d,1
a Division of Medicine, Center for Shared Decision Making and Collaborative Care Research, Oslo University Hospital, Oslo, Norwayb Division of Medicine, Section of Gastroenterology, Oslo University Hospital, Oslo, Norwayc Institute of Health and Society, Department of Nursing Science, University of Oslo, Oslo, Norwayd Lovisenberg Diakonale Hospital, Oslo, Norway
Accepted 28 November 2011
KEYWORDSCritical care;Family;Intensive care unit;Needs assessment
SummaryPurpose: To describe the relationships between demographic variables and the need for support,comfort, information, proximity and assurance amongst the visitors at the intensive care unit(ICU).Methods: In a cross-sectional correlational design, data were collected from March 2008 toJanuary 2009 at a university hospital in the city of Oslo, Norway. The Critical Care Family NeedsInventory was used to collect data on the participants’ perceived need for support, comfort,information, proximity and assurance. One hundred and forty-six questionnaires were given tothe visitors of 74 patients, and 62 (42.5%) responded.Results: The bivariate analyses showed that younger visitors regarded their need for comfort,information, proximity and assurance as more important than older visitors. Women reporteda need for more comfort than men. Visitors with a lower level of formal education regardedtheir need for more support and comfort as more important than those with a higher educa-tional level. After controlling for other socio-demographic variables, linear regression analysis
showed that low educational level was directly related to greater need for support, comfortand proximity.Conclusions: Professionals should pay special attention to the needs of younger visitors to theICU, females and those with a low level of education.© 2011 Elsevier Ltd. All rights re∗ Corresponding author at: Oslo University Hospital, P.O. Box 4940 NydE-mail addresses: [email protected] (G. Høg
[email protected] (A. Lerdal).1 Oslo University Hospital, P.O. Box 4940 Nydalen, N-0424 Oslo, Norwa
0964-3397/$ — see front matter © 2011 Elsevier Ltd. All rights reserved.doi:10.1016/j.iccn.2011.11.009
served.
alen, N-0424 Oslo, Norway. Tel.: +47 23075466; fax: +47 23075450.haug), [email protected] (M.S. Fagermoen),
y.

2
I
Cctocmefhtt4e2r2
(c1nTrcbp(WCveervn
M
T
S
Daiuiwt
M
Dt(yywmhhw
(4(ppsTC1o0oSf0ailrwscwm
P
Ttst
S
Dyltepa
64
ntroduction
ritically ill patients in the intensive care unit (ICU) haveomplex multisystem diseases and are treated in a highlyechnical environment. The hospitalisation of a patientften occurs acutely and without previous warning. The out-ome of the treatment is often uncertain, and the risk ofortality of the ICU patient can be as high as 20% (Harrison
t al., 2004). In this highly technical environment, stress-ul situations and distress might influence the psychologicalealth of visitors during and after the patient’s hospitalisa-ion in the ICU. Studies of the psychosocial health of visitorso patients in the ICU report prevalence rates of anxiety of2—73% and of depressive symptoms of 16—35% (Andersont al., 2008; Pochard et al., 2001, 2005; Azoulay et al.,004). Posttraumatic stress disorder occurs in 15—20% of theelatives of critically ill patients in the ICU (Rattray et al.,005; Cuthbertson et al., 2004).
The instrument Critical Care Family Needs InventoryCCFNI) has been used in studies of the need of the criti-al care patient’s relatives (Lorenz, 1995; Forrester et al.,990). It has been used to identify the most importanteeds of the relatives (Omari, 2009; Auerbach et al., 2005).hese studies have shown that the most important needs ofelatives include obtaining information about the patient’sondition and about changes in his or her condition, andeing assured that the best care is being given to theatient. Our review of the literature found few studiesLee and Lau, 2003; Delva et al., 2002; Chartier and Coutu-akulczyk, 1989; Rukholm et al., 1991) that have used theCFNI to study the relationships between socio-demographicariables and visitors’ preferences. Only one study (Delvat al., 2002) was from the past 20 years and from a West-rn country. The aim of our study was to investigate to theelationships between socio-demographic variables amongstisitors to patients in the ICU and how they regard theireeds.
The following research questions guided the analyses.
How do the visitors perceive their need for support, com-fort, information, proximity and assurance?
How are the visitors’ demographic variables (age, sex,level of formal education), length of hospitalisation in theICU and their relationship with the patient (being a part-ner or a daughter/son) related to their perceived need forsupport, comfort, information, proximity and assurance?
ethods
he study had a cross-sectional correlational design.
ampling
ata were collected between March 2008 and January 2009t the ICU of a university hospital in Norway. All persons vis-ting the patients at the ICU, 16 years or older and able to
nderstand Norwegian, were invited consecutively to partic-pate in the study. One hundred and forty-six questionnairesere given to visitors of 74 patients, and 62 (42.5%) ques-ionnaires were returned with valid data.
awWt
G. Høghaug et al.
easurements
ata were collected through the questionnaires. The ques-ionnaire was used to collect self-reported data on agegrouped into 16—30, 31—40, 41—50, 51—60, 61—70, ≥71ears); sex (women, men); level of formal education (≤13ears, >13 years); work status (in paid work, not in paidork); relationship with the patient (partner, daughter/son,other/father, sister/brother, friend, other); reason for
ospitalisation (acute, elective, unknown); and length ofospitalisation in the ICU (3 days, 4—7 days, 8—14 days, 3eeks, 4 weeks and more).
The CCFNI (Leske, 1991) was used to assess the visitors’study participants’) perceived needs. The CCFNI comprises5 statements grouped into five needs subscales: support15 items), comfort (six items), information (eight items),roximity (nine items) and assurance (seven items). Thearticipants rate how they regard their needs on a Likertcale ranging from not important (1) to very important (4).he validity and reliability of the five subscale scores ofCFNI USA-version has been reported as satisfactory (Leske,991). The internal consistency between the five subscalesf the CCFNI assessed with Cronbach’s alpha in Belgium is.62—0.80 (Bijttebier et al., 2000). The alpha coefficientf the CCFNI questionnaire in Sweden is 0.92 (Takman andeverinsson, 2004). In our study, Cronbach’s alpha valuesor the subscales were 0.88 for support, 0.88 for comfort,.78 for information, 0.74 for proximity and 0.78 for assur-nce. There is a validated Swedish translation of the CCFNInstruments (Takman, 2008). The Norwegian and Swedishanguages are very similar, and Swedes and Norwegiansead and understand both languages. A Swedish versionas chosen and adapted to Norwegian. The original item
ix, included in subscale proximity—–To have visiting hourshanged for special conditions—–was removed from the Nor-egian version because it was not relevant because visitorsay visit the patients at any time.
rocedures
he visitors were approached by office staff when they cameo the ICU and were given written information about thetudy, the questionnaire and a stamped return envelope withhe name and address of the project manager.
tatistical analysis
escriptive statistics were used in the univariate anal-sis and in the Pearson’s correlation analysis. Separateinear regression models were used to explore the rela-ionships between the visitors’ age, sex, level of formalducation, work status and their relationship with theatient for each of the subscales of the CCFNI. As notedbove, the internal consistency of the five subscales was
ssessed with Cronbach’s alpha. The level of significanceas set at p < 0.05. All tests were two-tailed. SPSS forindows version 15.0 software (SPSS, 2005) was used forhe statistical analysis.
The visitor’s regard of their need for support, comfort, information proximity and assurance in the ICU 265
Table 1 Demographic characteristics, hospitalisation andlength of hospitalisation in the ICU of the sample.
Variable N (%)
Age group (years)16—20 1 (14.5)21—30 8 (1.6)31—40 13 (21.0)41—50 15 (24.2)51—60 14 (22.6)61—70 6 (9.7)≥71 5 (8.1)
SexWomen 36 (58.1)Men 26 (41.9)
Level of formal educationEducation ≤13 years 28 (45.2)Education >13 years 34 (54.8)
Work statusIn paid work 46 (74.2)Not in paid work 15 (24.2)
Relationship to the patientsPartner 16 (25.8)Daughter or son 24 (38.7)Mother or father 6 (9.7)Sister or brother 7 (11.3)Friend 5 (8.1)Other 3 (4.8)
HospitalisationAcute 51 (82.3)Elective 9 (14.5)Unknown 2 (3.2)
Length of hospitalisation in ICU3 days 7 (11.3)4—7 days 28 (45.2)8—14 days 18 (29.0)3 weeks 6 (9.7)
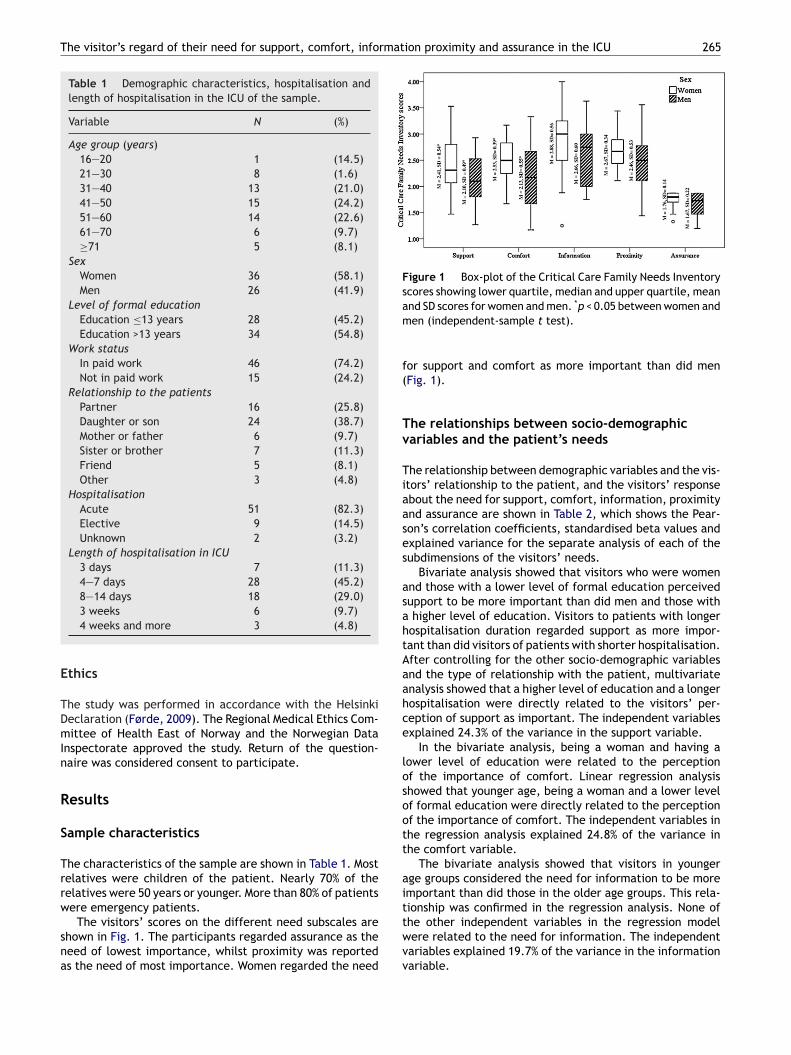
Figure 1 Box-plot of the Critical Care Family Needs Inventoryscores showing lower quartile, median and upper quartile, meana *
m
f(
Tv
Tiaases
asahtAaahce
losoott
ait
4 weeks and more 3 (4.8)
Ethics
The study was performed in accordance with the HelsinkiDeclaration (Førde, 2009). The Regional Medical Ethics Com-mittee of Health East of Norway and the Norwegian DataInspectorate approved the study. Return of the question-naire was considered consent to participate.
Results
Sample characteristics
The characteristics of the sample are shown in Table 1. Mostrelatives were children of the patient. Nearly 70% of therelatives were 50 years or younger. More than 80% of patientswere emergency patients.
The visitors’ scores on the different need subscales areshown in Fig. 1. The participants regarded assurance as theneed of lowest importance, whilst proximity was reportedas the need of most importance. Women regarded the need
twvv
nd SD scores for women and men. p < 0.05 between women anden (independent-sample t test).
or support and comfort as more important than did menFig. 1).
he relationships between socio-demographicariables and the patient’s needs
he relationship between demographic variables and the vis-tors’ relationship to the patient, and the visitors’ responsebout the need for support, comfort, information, proximitynd assurance are shown in Table 2, which shows the Pear-on’s correlation coefficients, standardised beta values andxplained variance for the separate analysis of each of theubdimensions of the visitors’ needs.
Bivariate analysis showed that visitors who were womennd those with a lower level of formal education perceivedupport to be more important than did men and those with
higher level of education. Visitors to patients with longerospitalisation duration regarded support as more impor-ant than did visitors of patients with shorter hospitalisation.fter controlling for the other socio-demographic variablesnd the type of relationship with the patient, multivariatenalysis showed that a higher level of education and a longerospitalisation were directly related to the visitors’ per-eption of support as important. The independent variablesxplained 24.3% of the variance in the support variable.
In the bivariate analysis, being a woman and having aower level of education were related to the perceptionf the importance of comfort. Linear regression analysishowed that younger age, being a woman and a lower levelf formal education were directly related to the perceptionf the importance of comfort. The independent variables inhe regression analysis explained 24.8% of the variance inhe comfort variable.
The bivariate analysis showed that visitors in youngerge groups considered the need for information to be moremportant than did those in the older age groups. This rela-ionship was confirmed in the regression analysis. None ofhe other independent variables in the regression model
ere related to the need for information. The independentariables explained 19.7% of the variance in the informationariable.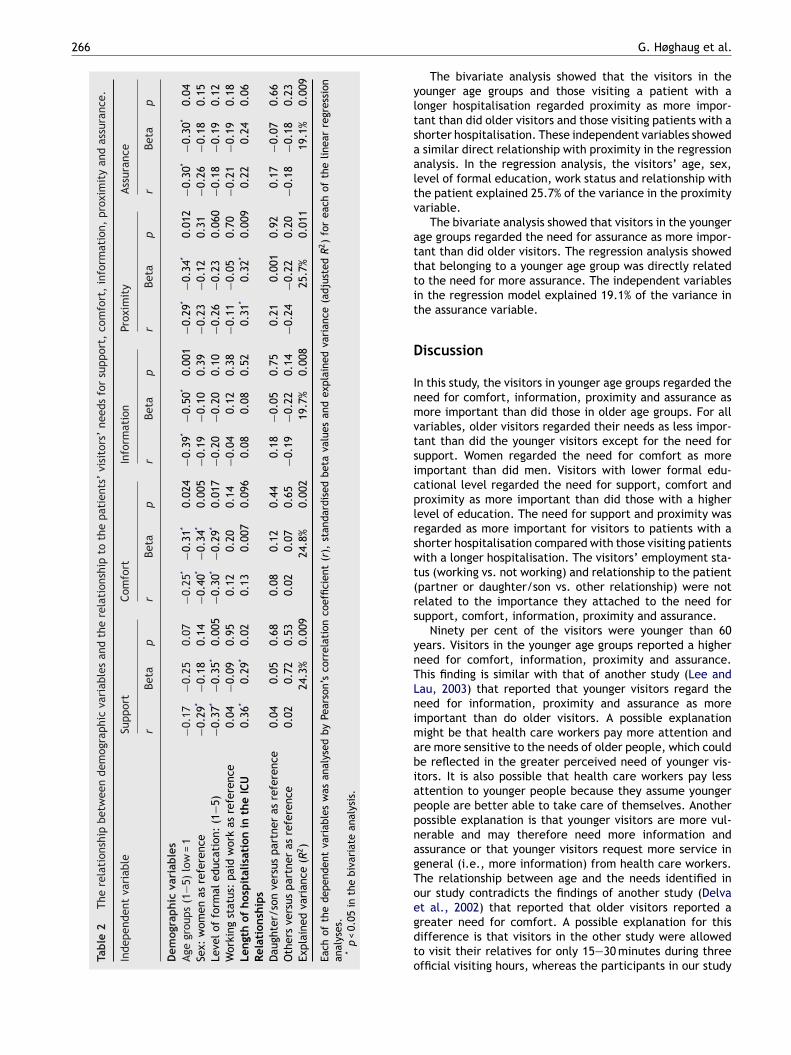
266
Tabl
e
2
The
rela
tion
ship
betw
een
dem
ogra
phic
vari
able
s
and
the
rela
tion
ship
to
the
pati
ents
’
visi
tors
’
need
s
for
supp
ort,
com
fort
,
info
rmat
ion,
prox
imit
y
and
assu
ranc
e.
Inde
pend
ent
vari
able
Supp
ort
Com
fort
Info
rmat
ion
Prox
imit
y
Assu
ranc
e
r
Beta
p
r
Beta
p
r
Beta
p
r
Beta
p
r
Beta
p
Dem
ogra
phic
vari
able
sAg
e
grou
ps
(1—
5)
low
=
1
−0.1
7
−0.2
5
0.07
−0.2
5*−0
.31*
0.02
4
−0.3
9*−0
.50*
0.00
1
−0.2
9*−0
.34*
0.01
2
−0.3
0*−0
.30*
0.04
Sex:
wom
en
as
refe
renc
e
−0.2
9*−0
.18
0.14
−0.4
0*−0
.34*
0.00
5
−0.1
9
−0.1
0
0.39
−0.2
3
−0.1
2
0.31
−0.2
6
−0.1
8
0.15
Leve
l of
form
al
educ
atio
n:
(1—
5)
−0.3
7*−0
.35*
0.00
5
−0.3
0*−0
.29*
0.01
7
−0.2
0
−0.2
0
0.10
−0.2
6
−0.2
3
0.06
0 −0
.18
−0.1
9
0.12
Wor
king
stat
us:
paid
wor
k
as
refe
renc
e
0.04
−0.0
9
0.95
0.12
0.20
0.14
−0.0
4
0.12
0.38
−0.1
1
−0.0
5
0.70
−0.2
1
−0.1
9
0.18
Leng
th
of
hosp
ital
isat
ion
in
the
ICU
0.36
*0.
29*
0.02
0.13
0.00
7
0.09
6
0.08
0.08
0.52
0.31
*0.
32*
0.00
9
0.22
0.24
0.06
Rela
tion
ship
sD
augh
ter/
son
vers
us
part
ner
as
refe
renc
e
0.04
0.05
0.68
0.08
0.12
0.44
0.18
−0.0
5
0.75
0.21
0.00
1
0.92
0.17
−0.0
7
0.66
Oth
ers
vers
us
part
ner
as
refe
renc
e
0.02
0.72
0.53
0.02
0.07
0.65
−0.1
9
−0.2
2
0.14
−0.2
4 −0
.22
0.20
−0.1
8
−0.1
8
0.23
Expl
aine
d
vari
ance
(R2)
24.3
%
0.00
9
24.8
%
0.00
2
19.7
%
0.00
8
25.7
%
0.01
1
19.1
%
0.00
9
Each
of
the
depe
nden
t
vari
able
s
was
anal
ysed
by
Pear
son’
s
corr
elat
ion
coef
ficie
nt
(r),
stan
dard
ised
beta
valu
es
and
expl
aine
d
vari
ance
(adj
uste
d
R2)
for
each
of
the
linea
r
regr
essi
onan
alys
es.
*p
<
0.05
in
the
biva
riat
e
anal
ysis
.
yltsaaltv
atttit
D
Inmvtsicplrswt(rs
ynTLnimabiappnagToegdto
G. Høghaug et al.
The bivariate analysis showed that the visitors in theounger age groups and those visiting a patient with aonger hospitalisation regarded proximity as more impor-ant than did older visitors and those visiting patients with ahorter hospitalisation. These independent variables showed
similar direct relationship with proximity in the regressionnalysis. In the regression analysis, the visitors’ age, sex,evel of formal education, work status and relationship withhe patient explained 25.7% of the variance in the proximityariable.
The bivariate analysis showed that visitors in the youngerge groups regarded the need for assurance as more impor-ant than did older visitors. The regression analysis showedhat belonging to a younger age group was directly relatedo the need for more assurance. The independent variablesn the regression model explained 19.1% of the variance inhe assurance variable.
iscussion
n this study, the visitors in younger age groups regarded theeed for comfort, information, proximity and assurance asore important than did those in older age groups. For all
ariables, older visitors regarded their needs as less impor-ant than did the younger visitors except for the need forupport. Women regarded the need for comfort as moremportant than did men. Visitors with lower formal edu-ational level regarded the need for support, comfort androximity as more important than did those with a higherevel of education. The need for support and proximity wasegarded as more important for visitors to patients with ahorter hospitalisation compared with those visiting patientsith a longer hospitalisation. The visitors’ employment sta-
us (working vs. not working) and relationship to the patientpartner or daughter/son vs. other relationship) were notelated to the importance they attached to the need forupport, comfort, information, proximity and assurance.
Ninety per cent of the visitors were younger than 60ears. Visitors in the younger age groups reported a highereed for comfort, information, proximity and assurance.his finding is similar with that of another study (Lee andau, 2003) that reported that younger visitors regard theeed for information, proximity and assurance as moremportant than do older visitors. A possible explanationight be that health care workers pay more attention and
re more sensitive to the needs of older people, which coulde reflected in the greater perceived need of younger vis-tors. It is also possible that health care workers pay lessttention to younger people because they assume youngereople are better able to take care of themselves. Anotherossible explanation is that younger visitors are more vul-erable and may therefore need more information andssurance or that younger visitors request more service ineneral (i.e., more information) from health care workers.he relationship between age and the needs identified inur study contradicts the findings of another study (Delvat al., 2002) that reported that older visitors reported a
reater need for comfort. A possible explanation for thisifference is that visitors in the other study were allowedo visit their relatives for only 15—30 minutes during threefficial visiting hours, whereas the participants in our study
rmat
apfshtcossp
S
Osafmaibns
C
OstatiHsineanno
R
A
A
A
The visitor’s regard of their need for support, comfort, info
had free access to their relatives. It is also possible that thehealth care professionals in the other study gave less atten-tion to older visitors and thus the older participants reportedgreater perceived need. Allowing visitors access to patientsfor only 15—30 minutes provides little flexibility, especiallyfor older visitors who may live far from the hospital. Thecontradictory findings between studies may be explained bydifferences in the sample characteristics, i.e., younger sub-jects (mean age 48 years) in our study compared with theprevious study (Delva et al., 2002).
Except for women perceiving comfort to be more impor-tant than men, we found no sex-related differences in thevisitors’ needs. This is a similar finding to that of a Belgianstudy (Delva et al., 2002). A study from Hong Kong (Lee andLau, 2003) found no differences between women and menin relation to any of the five subscales in the CCFNI. How-ever, because in this study (Lee and Lau, 2003) each of theitems in the CCFNI was analysed separately, we cannot com-pare the mean scores of the subscales directly. In the studyfrom Hong Kong (Lee and Lau, 2003), woman rated the need‘‘to see the patient frequently’’ and ‘‘to visit at any time,’’which is within the proximity subscale, as more importantthan did men. Men reported the need ‘‘to have someoneconcerned with your health,’’ which is within the supportsubscale, to be more important than did women.
Others have also reported a relationship between the visi-tor’s level of formal education and the perceived importanceof needs (Lee and Lau, 2003; Delva et al., 2002; Chartierand Coutu-Wakulczyk, 1989). One explanation may be thatnurses and doctors adjust their care unconsciously to thevisitor’s social status; i.e., health care professionals conveymore support, comfort, information, proximity and assur-ance to those visitors with a higher educational level. Onemay question whether visitors with less formal educationreceive adequate help and support. Further research on thisissue is needed.
Our study showed that the visitor’s relationship with thepatient (i.e., a partner, son or daughter) had no effect onthe visitor’s perceived different needs. A similar result wasreported in another study (Lee and Lau, 2003). However,a study from the UK (Harrison et al., 2004) reported thatthe relationship between the visitor and patient was sig-nificantly related to how the visitor regarded his or herneed for information and assurance; i.e., partners regardedthe need for information and assurance as more importantthan visitors who were not partners. A possible explana-tion for this inconsistency between studies may be thedifferent categorization of the variables in the differentstudies.
In our study, more than 50% of the patients had been inthe ICU for seven days or less when their families respondedto the questionnaire. Visitors to patients with a shorter hos-pital stay regarded the need for support and proximity tobe more important than visitors to patients with longer hos-pital stays. This finding raises the question whether healthcare personnel provide less support and empathy to visitorsto patients who stay for a short time in the ICU. We have notbeen able to identify any studies exploring this issue. How-
ever, two studies reported that family members and nurseshave different perceptions of the needs of family membersof critically ill patients (Hinkle et al., 2009; Maxwell et al.,2007).B
ion proximity and assurance in the ICU 267
Our study shows that socio-demographic variablesre related to how the visitors regard their needs. Aossible interpretation of this finding is that health pro-essionals treat patients differently according to theirocio-demographic background. For example, visitors with aigher level of education may receive more attention, andhose with a lower level of education regard the need foromfort as more important than do those with a higher levelf education. Studies are needed to explore these relation-hips further and to include possible confounding variablesuch as the visitor’s level of stress, health status and otherersonal factors.
trengths and limitations of the study
ur study has several limitations. First, it is a cross-sectionaltudy, which does not allow us to assess the relationship from
cause-and-effect perspective. Second, we did not controlor the patients’ medical conditions and outcomes, whichight be related to the visitors’ judgement of which needs
re important to relatives in the ICU. Third, we have lim-ted empirical data available to interpret the relationshipsetween the visitors’ perceptions of their needs and exter-al or internal factors. These should be explored in futuretudies.
onclusions
ur study showed that differences in the visitors’ age andex were related to how they regarded the importance ofhe need for support, comfort, information, proximity andssurance. Visitors with a lower educational level reportedhat the need for support, comfort and proximity was moremportant than did those with a higher educational level.ealth care personnel should pay attention to the visitors’ocio-demographic background because these factors maynfluence the visitors’ perceptions of care and their owneeds. We do not know how these potential differences arexpressed in the actual clinical situation or whether needsre unmet or satisfied. However, our findings suggest thaturses and physician should pay special attention to theeeds of younger visitors, females and those with a low levelf education.
eferences
nderson WG, Arnold RM, Angus DC, Bryce CL. Posttraumatic stressand complicated grief in family members of patients in the inten-sive care unit. J Gen Intern Med 2008;23:1871—6.
uerbach SM, Kiesler DJ, Wartella J, Rausch S, Ward KR, Ivatury R.Optimism, satisfaction with needs met, interpersonal percep-tions of the healthcare team, and emotional distress in patients’family members during critical care hospitalization. Am J CritCare 2005;14:202—10.
zoulay E, Pochard F, Chevret S, Adrie C, Annane D, Bleichner G,et al. Half the family members of intensive care unit patients donot want to share in the decision-making process: a study in 78French intensive care units. Crit Care Med 2004;32:1832—8.
ijttebier P, Delva D, Vanoost S, Hobbaers H, Lauwers P, Ver-tommen H. Reliability and validity of the Critical Care FamilyNeeds Inventory in a Dutch-speaking Belgian sample. Heart Lung2000;29:278—86.

2
C
C
D
F
F
H
H
L
L
L
M
O
P
P
R
R
ST
68
hartier L, Coutu-Wakulczyk G. Families in ICU: their needs andanxiety level. Intensive Care Nurs 1989;5:11—8.
uthbertson BH, Hull A, Strachan M, Scott J. Post-traumatic stressdisorder after critical illness requiring general intensive care.Intensive Care Med 2004;30:450—5.
elva D, Vanoost S, Bijttebier P, Lauwers P, Wilmer A. Needs andfeelings of anxiety of relatives of patients hospitalized in inten-sive care units: implications for social work. Soc Work HealthCare 2002;35:21—40.
orrester DA, Murphy PA, Price DM, Monaghan JF. Critical care fam-ily needs: nurse-family member confederate pairs. Heart Lung1990;19:655—61.
ørde R. Helsinkideklarasjonen: http://www.etikkom.no/no/FBIB/Praktisk/Lover-og retningslinjer/Helsinkideklarasjonen[accessed 10.02.09].
arrison DA, Brady AR, Rowan K. Case mix, outcome and length ofstay for admissions to adult, general critical car units in Eng-land, Wales and Northern Ireland: the intensive Care NationalAudit & Research Centre Case Mix Programme Database. CritCare 2004;8:99—111.
inkle JL, Fitzpatrick E, Oskrochi GR. Identifying the per-ception of needs of family members visiting and nursesworking in the intensive care unit. J Neurosci Nurs 2009;41:85—9.
ee LYK, Lau YL. Immediate needs of adult family members
of adult intensive care patients in Hong Kong. J Clin Nurs2003;12:490—500.eske JS. Internal psychometric properties of the Critical Care Fam-ily Needs Inventory. Heart Lung 1991;20:236—44.
T
G. Høghaug et al.
orenz B. Needs of family members of critically ill adults. Nursing(Lond) 1995;4:445—51.
axwell KE, Stuenkel D, Saylor C. Needs of family members of criti-cally ill patients: a comparison of nurse and family perceptions.Heart Lung 2007;36:367—76.
mari FH. Perceived and unmet needs of adult jordanian fam-ily members of patients in ICUs. J Nurs Scholarsh 2009;41:28—34.
ochard F, Darmon M, Fassier T, Bollaert PE, Cheval C, ColoignerM, et al. Symptoms of anxiety and depression in familymembers of intensive care unit patients before discharge ordeath. A prospective multicenter study. J Crit Care 2005;20:90—6.
ochard F, Azoulay E, Chevret S, Lemaire F, Hubert P, Canoui P,et al. Symptoms of anxiety and depression in family membersof intensive care unit patients: Ethical hypothesis regardingdecision-making capacity. Crit Care Med 2001;29:1893—7.
attray JE, Johnson M, Wildsmith JAW. Predictors of emo-tional outcomes of intensive care. Anaesthesia 2005;60:1085—92.
ukholm E, Barley P, Coutu-Wakulczyk G, Barley B. Needs and anx-iety level in relatives of intensive care unit patients. J Adv Nurs1991;16:920—8.
PSS. Base version 15.0 for Windows, USA; 2005.akman C. Vårdpersonals antaganden om närståendes behov. Uni-
versitetet i Oslo: Doktorgrad Det medisinske fakultet; 2008.akman C, Severinsson E. Comparing Norwegian nurses’ and physi-
cians’ perceptions of the needs of significant others in IntensiveCare Units. J Clin Nurs 2004;14:621—31.