the world health organization - criticalcarecanada.com
TRANSCRIPT
The World Health Organization: Does it have a Role in Critical Illness?
Rob Fowler, MDCM, MS(Epi), FRCP
Department of Medicine & Critical Care Medicine
Sunnybrook Hospital, University of Toronto
What is Critical Illness?



What is theWorld Health Organization?



Health Spending as a Percent of the GDP
Fowler RA, Adhikari N, et al Crit Care 2008

Life Expectancy and
per capita Health Spending
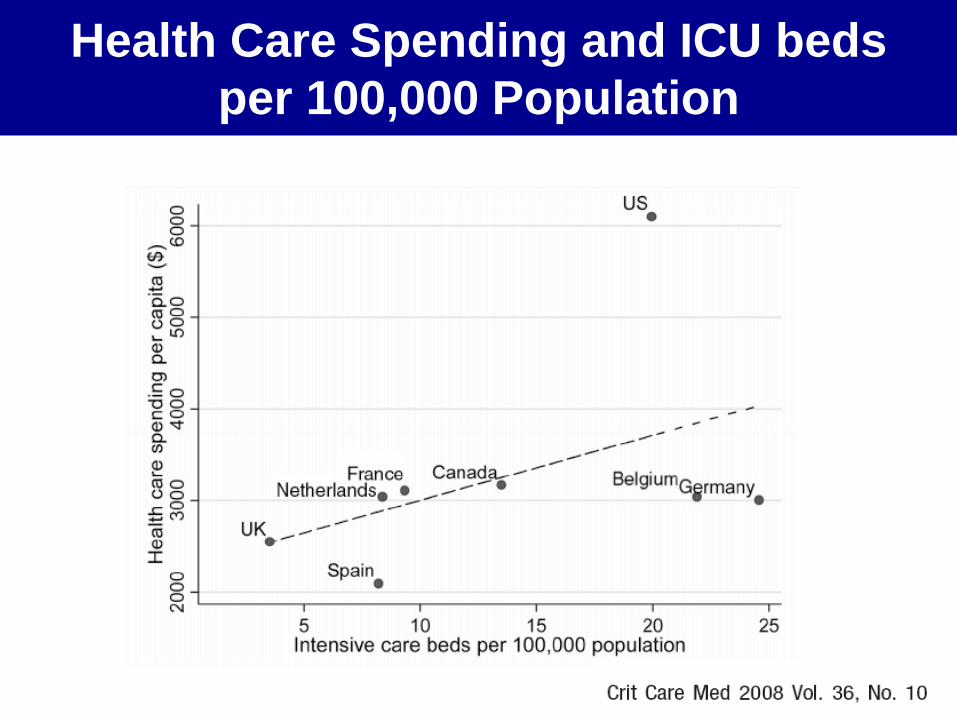
Health Care Spending and ICU beds
per 100,000 Population

Number of ICU Beds
by Country
Adhikari N, et al Lancet 2010
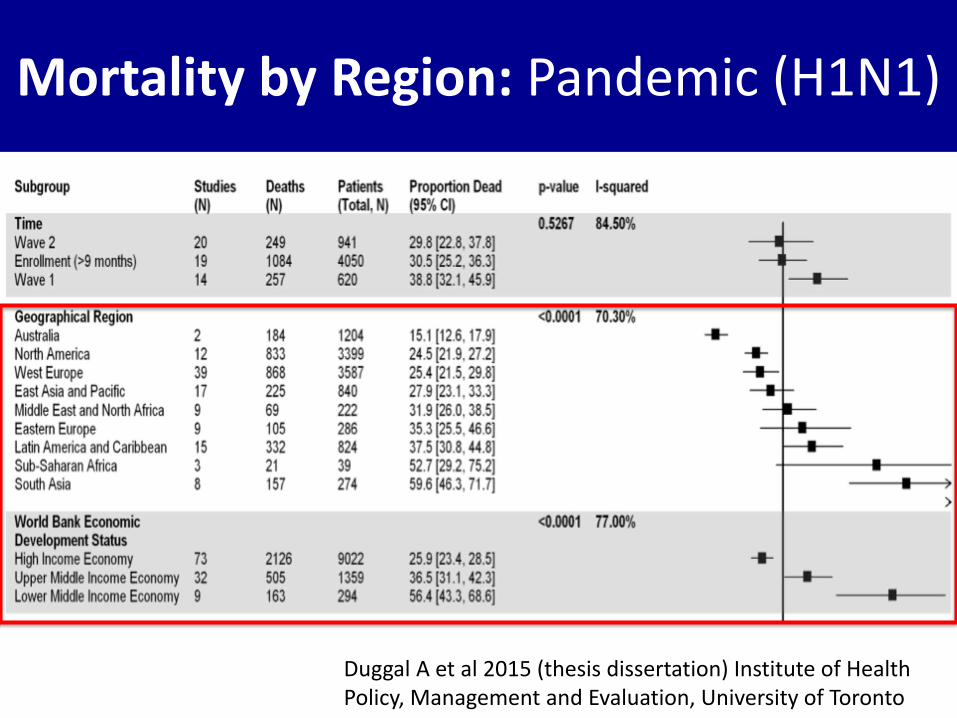
Mortality by Region: Pandemic (H1N1)
Duggal A et al 2015 (thesis dissertation) Institute of Health Policy, Management and Evaluation, University of Toronto

Why would the WHO be interested in Critical Care?
SARS 2003

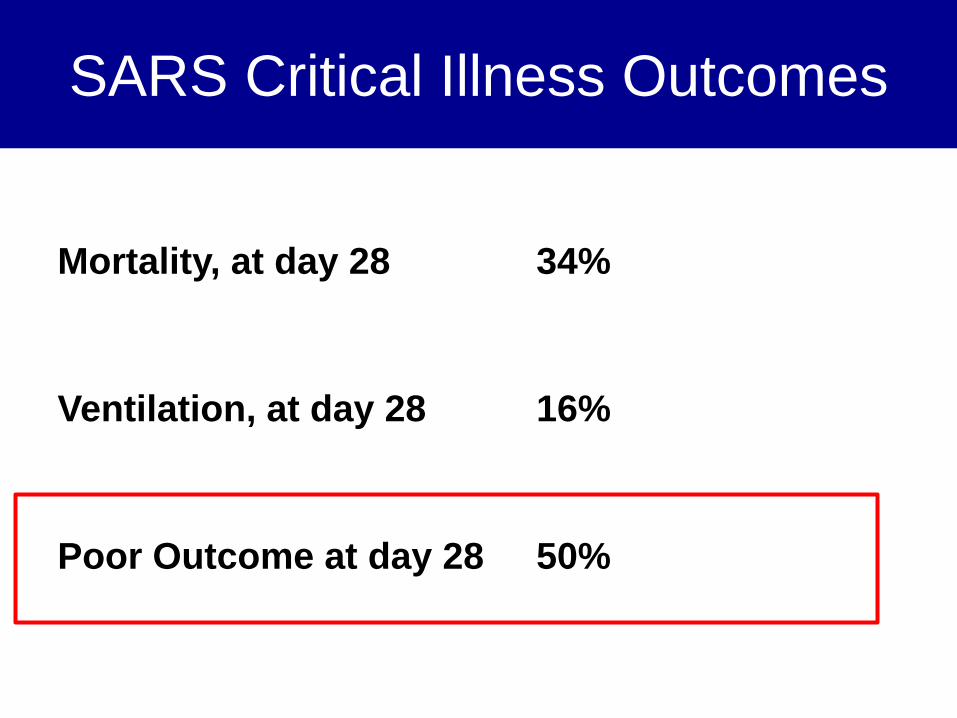
SARS Critical Illness Outcomes
Mortality, at day 28 34%
Ventilation, at day 28 16%
Poor Outcome at day 28 50%
H1N1 2009
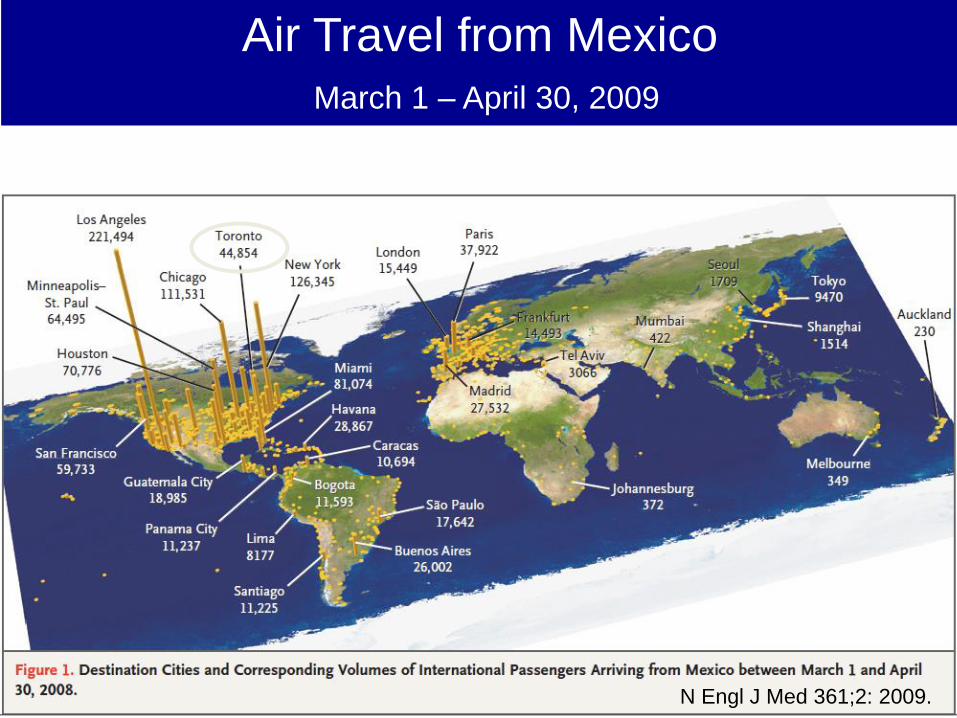
Air Travel from Mexico
March 1 – April 30, 2009
N Engl J Med 361;2: 2009.
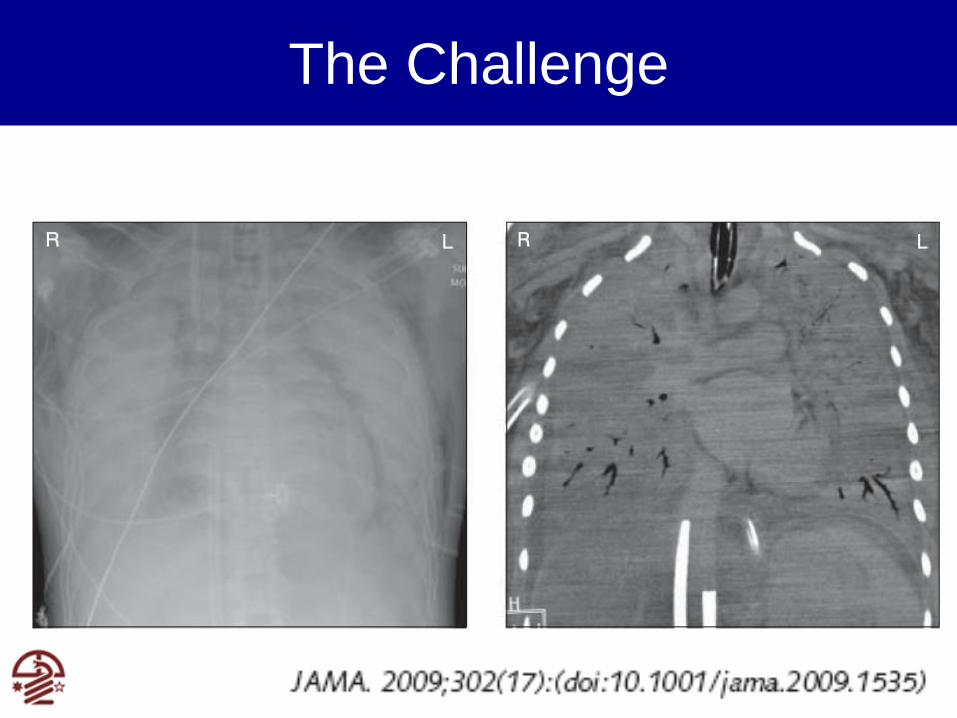
The Challenge
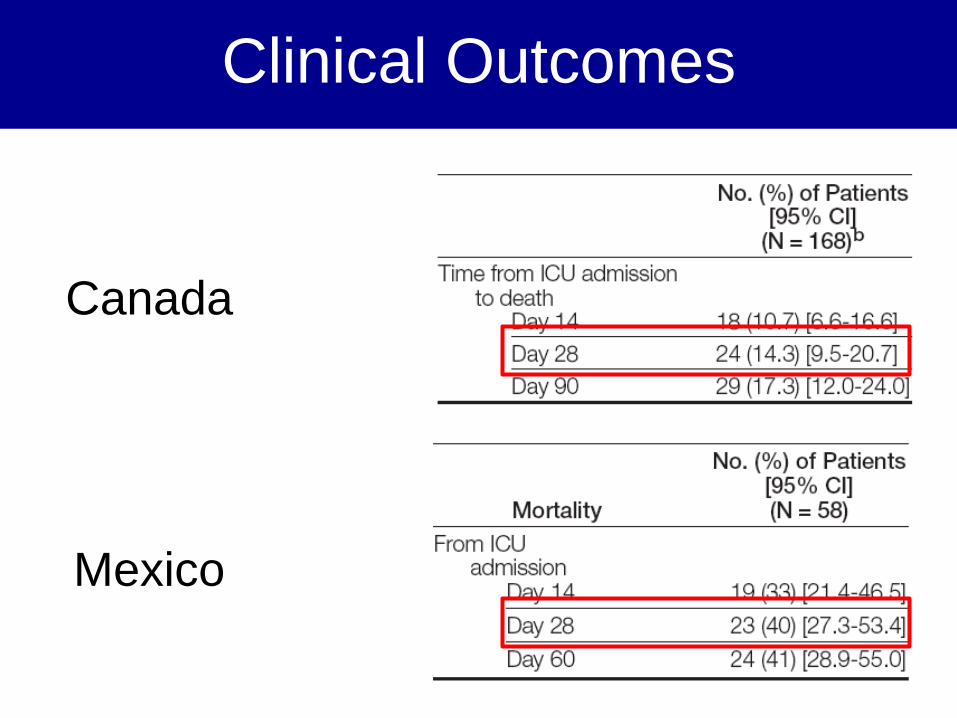
Clinical Outcomes
Canada
Mexico
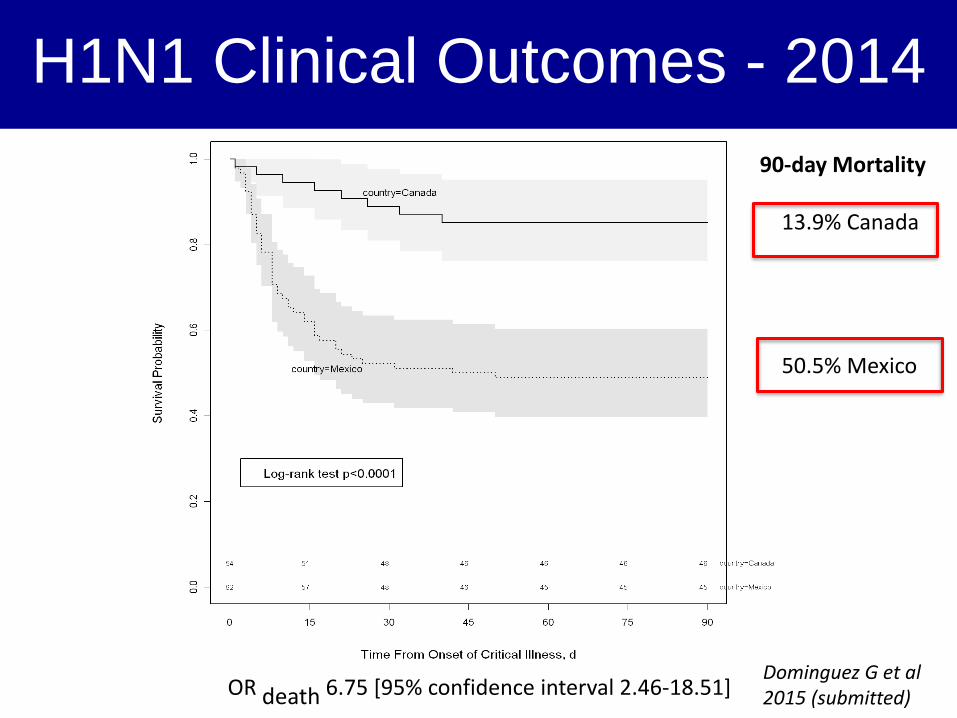
H1N1 Clinical Outcomes - 2014
OR death 6.75 [95% confidence interval 2.46-18.51]
90-day Mortality
13.9% Canada
50.5% Mexico
Dominguez G et al 2015 (submitted)
When will the next outbreak or
pandemic occur?
•
published on April 24, 2013, at NEJM.org
Mortality ~ 30%

Mortality ~ 30%

Ebola

Aug 26 2015 (+ 36 cases in Nigeria, Senegal, Mali, USA, Spain, UK = 28,041)
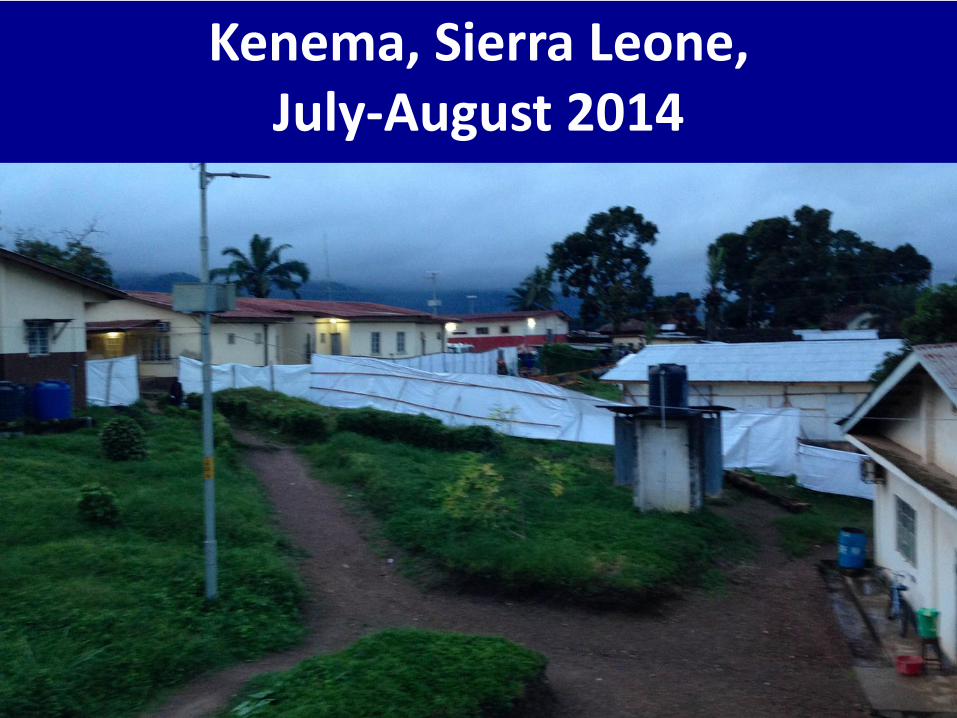
Kenema, Sierra Leone, July-August 2014


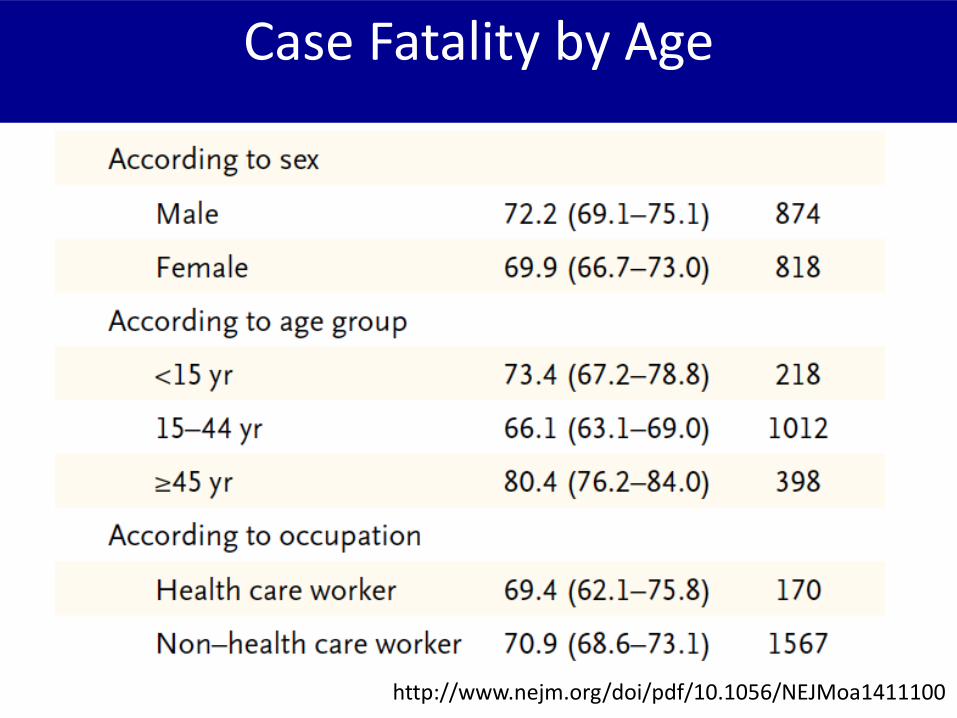
Case Fatality by Age
http://www.nejm.org/doi/pdf/10.1056/NEJMoa1411100

WHO: Challenges Faced

The “Goldilocks” Curse of EpidemicsThere is no response that is Just Right

The “Goldilocks” Curse of EpidemicsThere is no response that is Just Right
It is easy to over-react
The “Goldilocks” Curse of EpidemicsThere is no response that is Just Right

The “Goldilocks” Curse of EpidemicsThere is no response that is Just Right
It is easy to under-react
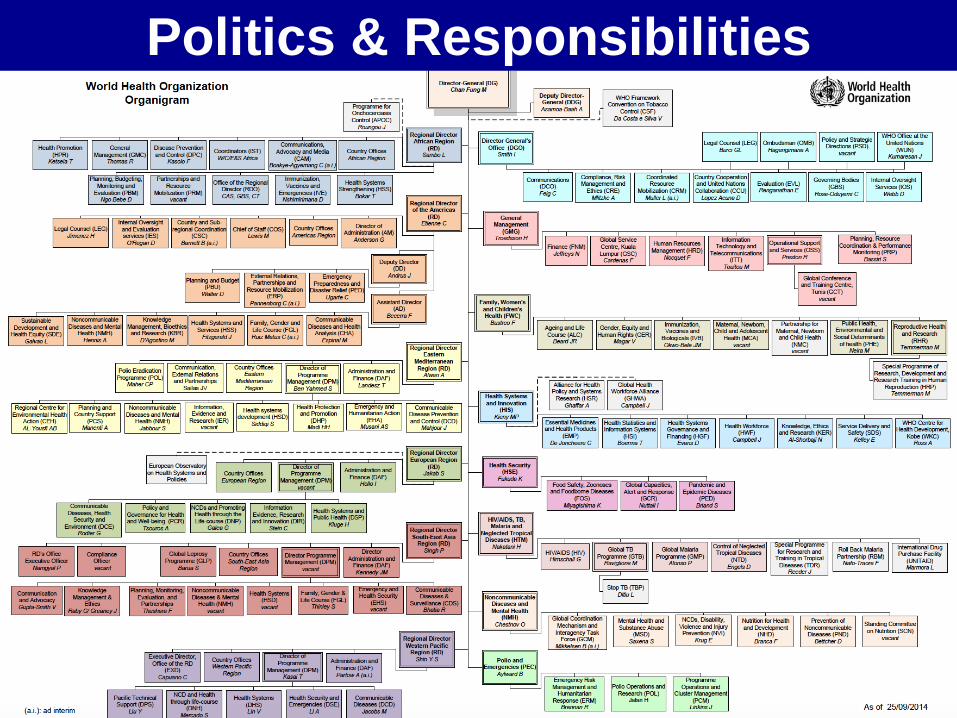
Politics & Responsibilities

Budget* (and Personnel)

WHO: Opportunities

• There is no one else who can do (a portion of) this work– Inherent focus is on developing world
– Neutrality
– Intimately connected at global (UN), regional (AFRO, EMRO, PAHO, WPRO, EURO, SEARO), country (MOH) and district levels
– Ability to convening partners who would not work together (MSF, medical branches of military, etc.)
– Ability to produce guidance that is generally viewed as the authoritative
– Its agenda influences other bodies
WHO: Opportunities
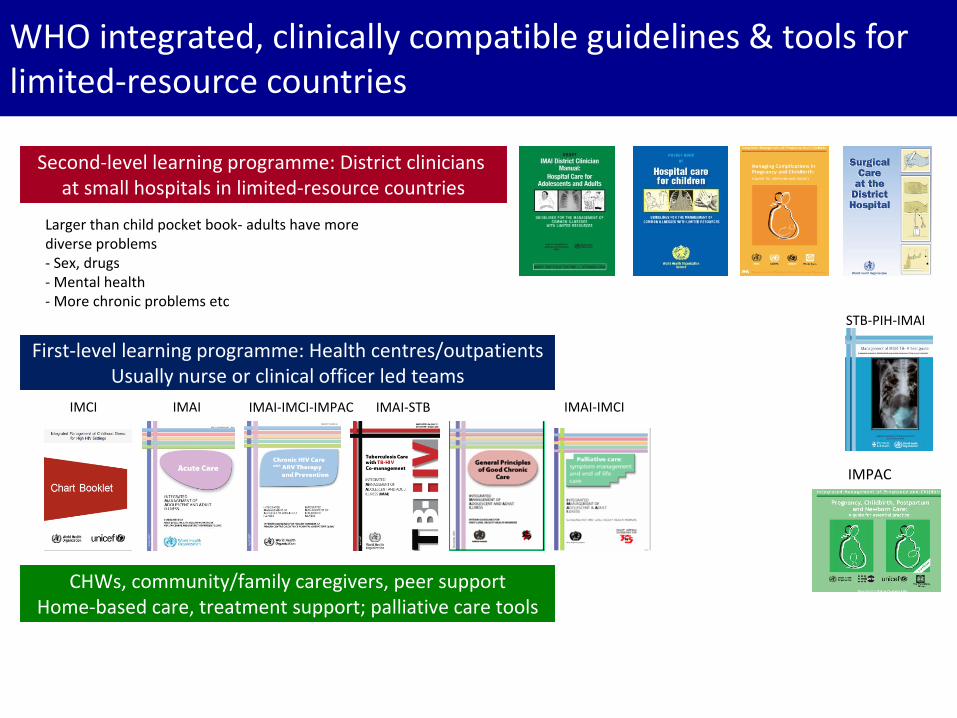
WHO integrated, clinically compatible guidelines & tools for limited-resource countries
Second-level learning programme: District clinicians at small hospitals in limited-resource countries
First-level learning programme: Health centres/outpatientsUsually nurse or clinical officer led teams
CHWs, community/family caregivers, peer supportHome-based care, treatment support; palliative care tools
IMAI-IMCI-IMPAC IMAI-IMCIIMAI-STBIMCI
IMPAC
IMAI
STB-PIH-IMAI
Larger than child pocket book- adults have more diverse problems- Sex, drugs- Mental health- More chronic problems etc

WHO integrated, clinically compatible guidelines & tools for limited-resource countries
Second-level learning programme: District clinicians at small hospitals in limited-resource countries
First-level learning programme: Health centres/outpatientsUsually nurse or clinical officer led teams
CHWs, community/family caregivers, peer supportHome-based care, treatment support; palliative care tools
IMAI-IMCI-IMPAC IMAI-IMCIIMAI-STBIMCI
IMPAC
IMAI
STB-PIH-IMAI
Larger than child pocket book- adults have more diverse problems- Sex, drugs- Mental health- More chronic problems etc
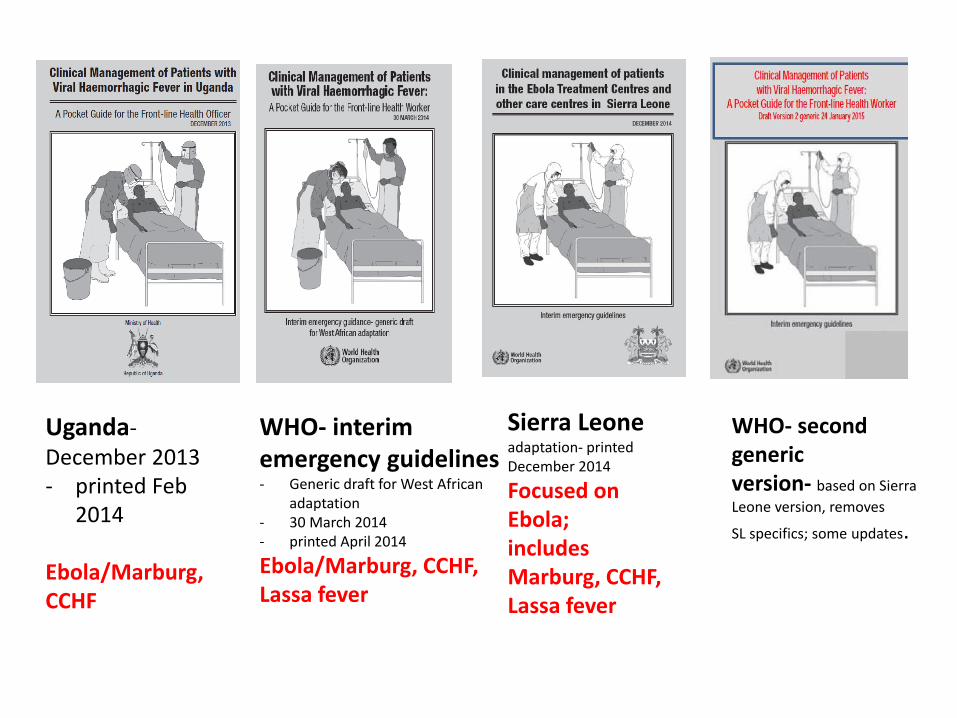
Uganda-December 2013- printed Feb
2014
Ebola/Marburg, CCHF
WHO- interim emergency guidelines - Generic draft for West African
adaptation- 30 March 2014- printed April 2014
Ebola/Marburg, CCHF, Lassa fever
Sierra Leone adaptation- printed December 2014
Focused on Ebola; includes Marburg, CCHF, Lassa fever
WHO- second genericversion- based on Sierra
Leone version, removes
SL specifics; some updates.

CCM 2013:41(2)

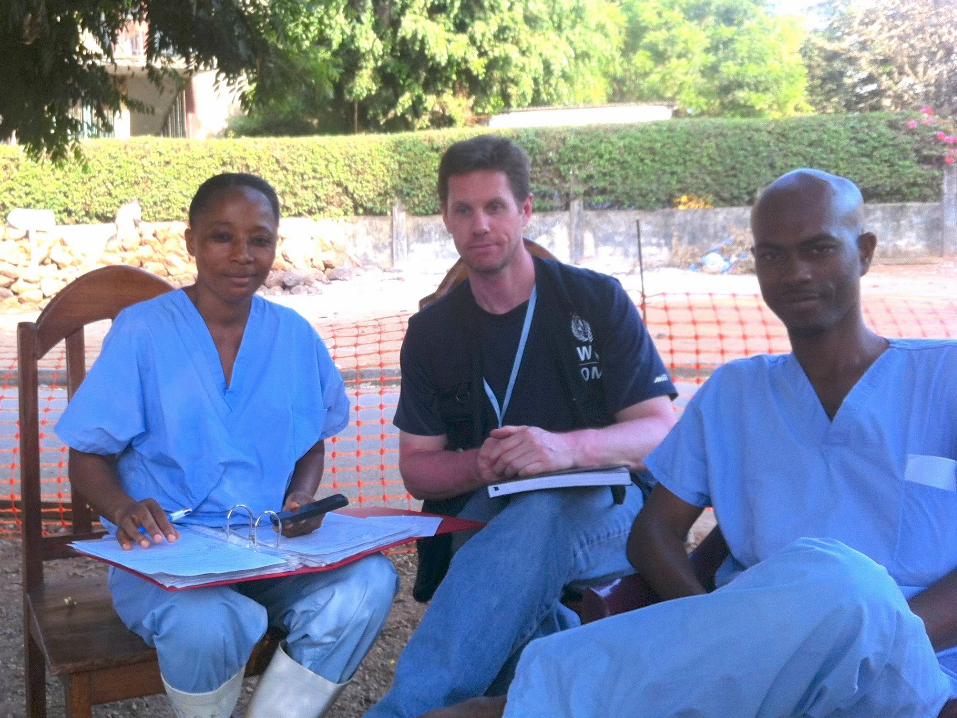
Goderich, SIERRA LEONEItalian Emergency NGO

Courtesy of Prof Antonio Pesenti & Dr. Gino Strada

[email protected]@who.int


Emerging Disease Clinical Assessment and Response Network
Clinical & Infection Control
Pandemic & Epidemic Diseases
WHO-HQ, Geneva
WHO Emerging Disease Clinical Assessment and Response Network (EDCARN)
Vision
The mortality due to emerging pathogens is reduced through
improved clinical management, even in absence of
vaccine or specific treatment. Enhance/empower the role
of clinical care / clinicians
Mission
In the Global Health Security context,
To strengthen global collaboration between clinicians, researchers,
WHO, medical NGO's, national health authorities and other
stakeholders in order to improve clinical management of patients
during outbreaks of emerging diseases.
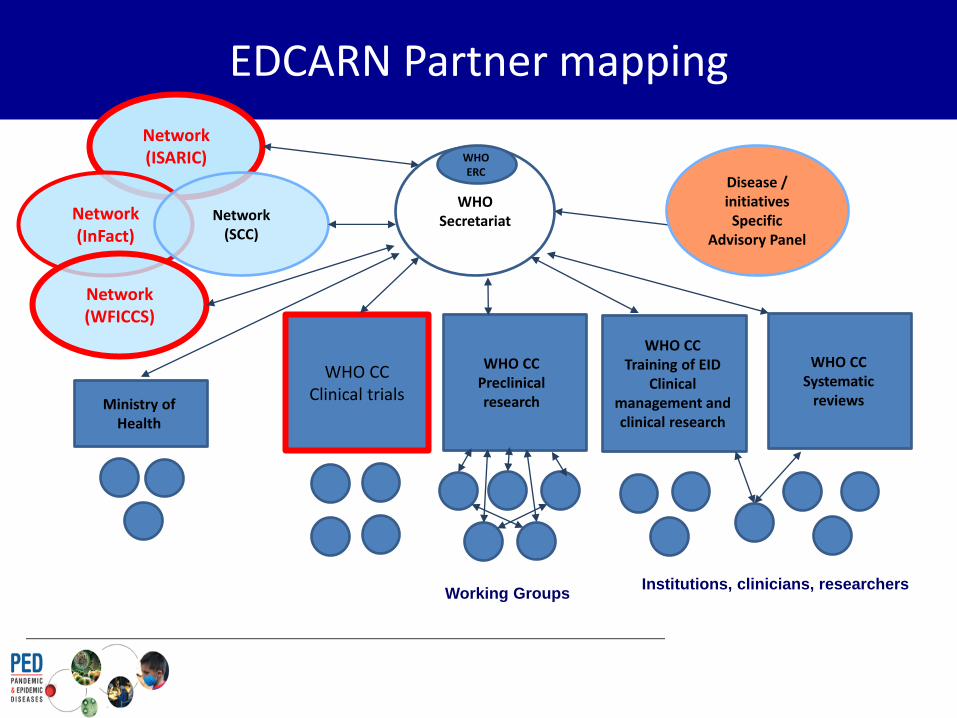
EDCARN Partner mapping
WHO Secretariat
WHO CCSystematic
reviews
WHO CCTraining of EID
Clinical management and clinical research
WHO CCPreclinical research
WHO CCClinical trials
WHO ERC
Network(ISARIC)
Network(InFact)
Network(SCC)
Network(WFICCS)
Ministry of Health
Working GroupsInstitutions, clinicians, researchers
Disease / initiatives Specific
Advisory Panel

Research
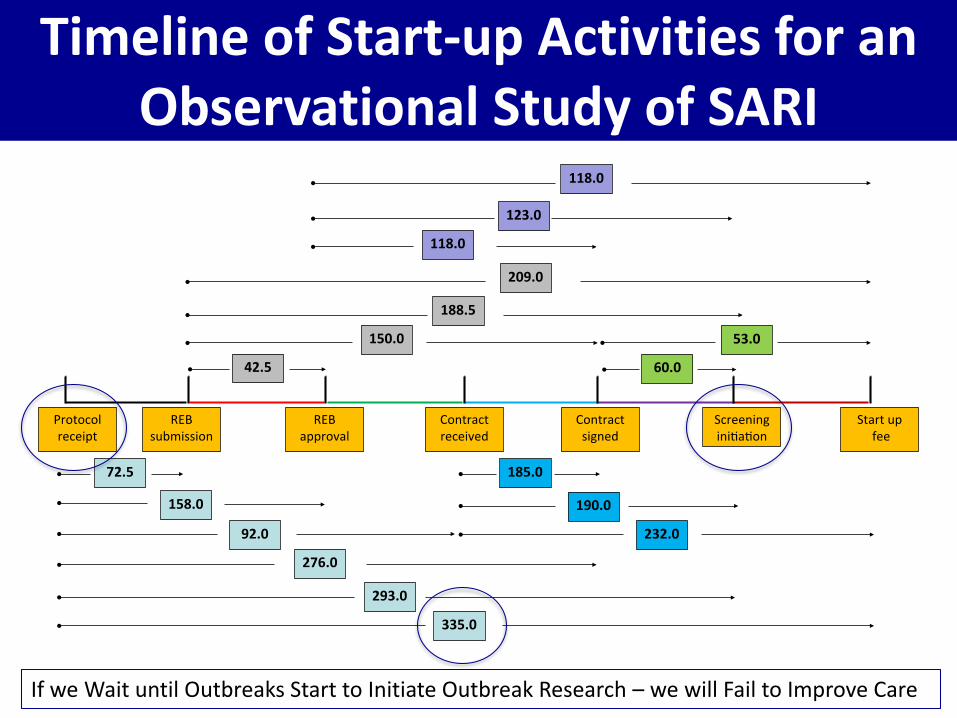
Timeline of Start-up Activities for an Observational Study of SARI
If we Wait until Outbreaks Start to Initiate Outbreak Research – we will Fail to Improve Care
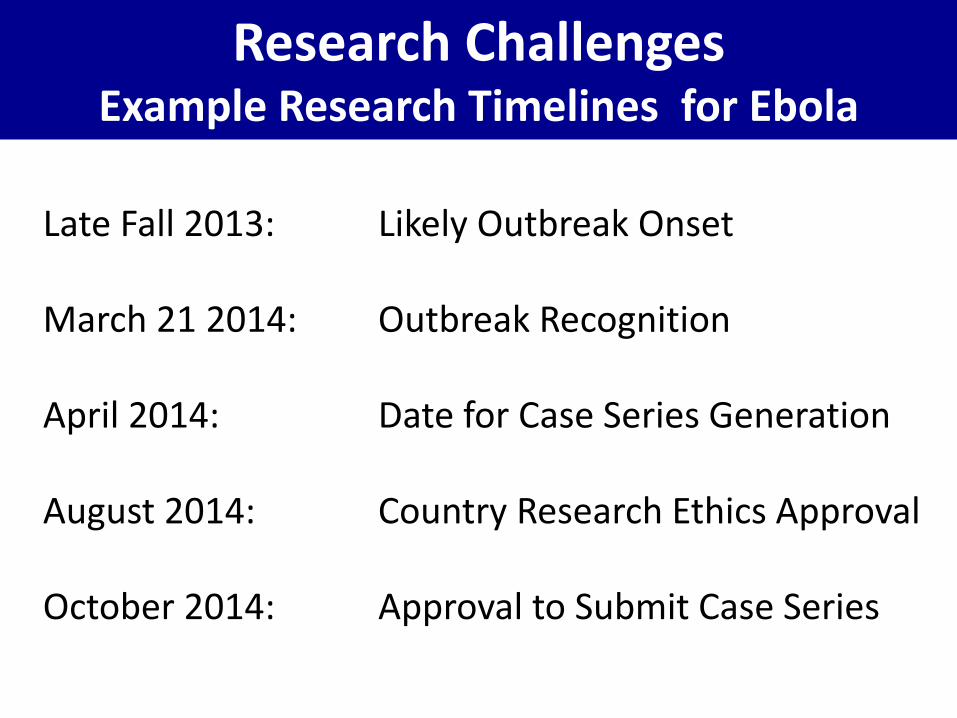
Late Fall 2013: Likely Outbreak Onset
March 21 2014: Outbreak Recognition
April 2014: Date for Case Series Generation
August 2014: Country Research Ethics Approval
October 2014: Approval to Submit Case Series
Research ChallengesExample Research Timelines for Ebola

WHO – Research Potential Ways Forward
If we wait for an outbreak or epidemic to start planning, initiating research, we will almost always fail to improve care during the outbreak and for the future
We must have somewhat generalizable, flexible observational studies, with paper and electronic case report forms, ready and ethics approved BEFORE
These CRFs should be “tiered” and be the platform upon which biological sampling and interventions are tested
• Tier 0: 1-page minimal CRF with descriptors and outcomes• Tier 1: Traditional observational study with characteristics, severity of
illness, course of care, treatments, available labs, outcomes• Tier 2: Biological sampling studies• Tier 3: Intervention Evaluation, open or randomized
There must be funds / a virtual fund-in-waiting to get this work done

WHO-ISARIC Research Collaboration Potential Ways Forward


[email protected]@who.int
Ebola Virus Disease