theoretical and methodological issues in research related ...6... · theoretical and methodological...
TRANSCRIPT
402
For more information about the concepts in this article please contact Dr Mkanta at williammkantawkuedu
Theoretical and Methodological Issues in Research Related to Value-Based Approaches in Healthcare William N Mkanta PhD associate professor Department of Public Health Western Kentucky University Bowling Green Madhuri Katta BDS research assistant Department of Public Health Western Kentucky University Karthika Basireddy BDS research assistant Department of Public Health Western Kentucky University Gary English PhD associate professor Department of Public Health Western Kentucky University and Maria C Mejia de Grubb MD assistant professor Department of Family and Community Medicine Baylor College of Medicine Houston Texas
E X E C U T I V E S U M M A R YThe US healthcare system is undergoing a transformation from traditional fee-for-service models to value-based purchasing in an attempt to build a culture of account-ability and address escalating costs and other major concerns Research related to the new environment of care is imperative in light of the growing body of data that informs the healthcare system about the impact of value-based purchasing This study reviews theoretical and methodological issues related to research in value-based care The concept of value is reviewed on the basis of its definition measure-ment and application in healthcare settings Stakeholder roles in relation to creation management and improvement of value are also explored The authors also conduct a review of theoretical frameworks that can be applied to the assessment of value and offer suggestions about what might constitute an ideal framework Recommenda-tions for future research are presented with a focus on areas in which health systems and providers have the potential to generate value and achieve professional benefits and fiscal integrity in this new environment of care
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
403
value-baseD aPProacHes In HealtHcare
I N T R O D U C T I O NThe US healthcare system is undergo-ing changes in care delivery and pay-ment mechanisms that reflect a shift from volume- to value-based healthcare The shift aims to replace the traditional fee-for-service (FFS) reimbursement model driven by volume and costly services to value-based purchasing (VBP) a model driven by accountability through integration of cost and quality (Conway 2009) Under this approach healthcare is moving toward a value-based system of reimbursement whereby performance or quality of care is the basis of reimbursement for providers and systems Since passage of the Affordable Care Act (ACA) in 2010 evidence has been growing that value-based approaches are being adopted by healthcare organizations Payers and consumers have gradually become more aware of the financial and health benefits of value-based care while providers are gaining familiarity with accountable care models (Werner amp Dudley 2009)
Unfortunately with all the delibera-tions and to some extent implementa-tion of the transformations related to value in healthcare the concepts of value and value-based care have been defined differently by researchers providers and healthcare organizations Because the main premise of value-based approaches is to generate a data-driven system of care reimburse-ment monitoring and service improve-ment a working definition of value must be determined and adopted for successful generation of comparable data Although there is strong agreement that value in healthcare is judged as
outcomes in relation to costs (Halm Lee amp Chassin 2002 Lohr 1988) cost savings alone should not gauge the success of value-based approaches Instead value analysis should be developed on the basis of carefully collected and measured data this analysis should be capable of producing projections in cost and other important healthcare metrics Discussions of measurements of value should incorpo-rate ideas on how to evaluate the effect of intangibles such as those influencing patient-centered care that might be important complements to value
Failure to develop an acceptable definition of value will hinder progress in achieving the intended benefits of value-based practices For example delays by healthcare professionals and organizations in adopting VBP might occur and health services may fail to achieve the desired standards and as a result create new cost threats Moreover value measurements will vary because of mixed or indistinct definitions Research and evaluation efforts that depend on the accuracy of data could be adversely affected by these inconsistencies Although increasing numbers of health-care professionals and organizations have begun using value-based approaches definitional issues mea-surements and the relationship between cost and outcomes have yet to be understood by all stakeholders
The aim of this study is to review theoretical and methodological issues related to conducting research on value-based healthcare Our intent is to help health policy researchers identify and address concerns related to research in the emerging field of VBP in healthcare
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
404
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Because cost and quality are major concerns in the US healthcare system value-based data should be readily available so that researchers can deter-mine whether VBP has led to new and favorable patterns of care
C O N C E P T U A L I S S U E S A N D T H E O R E T I C A L F R A M E W O R KHealth policy researchers need concep-tual frameworks to study understand and analyze value-based care Key conceptual issues are related to diverse sources of information and how access to these sources varies among stakeholders such as providers managers and con-sumers A classification of these sources is needed based on how they generate and make use of value-based data Various conceptual models such as that discussed by Miller (2009) have been postulated to illustrate the transition to
value-based care and the data that could be generated The conceptual issues around this transition are manifested in four aspects of healthcare provider practices clinical systems payment models and managerial systems This transition is expected to be gradual and multidimensional starting with changes in organizational structure coordination processes and internal operations
Miller (2009) depicted the transi-tion to VBP (Figure 1) The model focuses on the delivery systemrsquos transfor-mation and how it leads to transforma-tions in payment systems This framework illustrates how the definition of value may be reached when the healthcare system completes different phases of the journey to value-based care Therefore all stakeholders involved in the various stages of this transforma-tion must arrive at a common definition
F I G U R E 1 Phases of Transition From Volume-Based Care to Value-Based Care
Source Reprinted with permission from Miller (2009)
Transition in Both the Payment and the Delivery Systems
Value-driven coordinated care
Interimvirtual coordination
arrangements
Volume-driven fragmented care
Delivery system
Ideal
Transition
Today
Fee-for-service Virtual episode-of-care and comprehensive care payment
Episode-of-care or comprehensive care payment
Payment system
Failure due to lack of organizational capacity to manage value-driven payment
Co-evolution of
organization and payment
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
405
value-baseD aPProacHes In HealtHcare
when VBP becomes the dominant model of reimbursement
Several generic and disease-specific frameworks have been developed to support assessment of information at different levels and initiatives in the VBP environment
Care Delivery Value ChainThe care delivery value chain framework can help stakeholders understand the organization and structure of care delivery and thus provides a means to evaluate services delivered for a particu-lar condition (Reid Compton Gross-man amp Fanjiang 2005) This framework can be used to conceptualize how value-based data can be generated while emphasizing its application for
conditions associated with high expen-ditures The key takeaway is that this model allows value-based care to be examined and adopted for specific conditions that traditionally have been associated with high costs of care
Four-Level Healthcare System ModelFerlie and Shortell (2001) developed a model to describe a systems approach to healthcare delivery We propose a modification of this model to make it applicable to value-based care The four-level healthcare system model (Figure 2) is a potentially useful tool for studying VBP in different care settings
To achieve integrated team-based and patient-centered care researchers and providers should assess value at
F I G U R E 2 The Four-Level Healthcare System Model
Source Ferlie and Shortell (2001)
ENVIRONMENTRegulatory market and policy framework
(public and private regulators insurers healthcare purchasers research
funders et al)
ORGANIZATIONInfrastructureresources
(hospitals clinics nursing homes etc)
CARE TEAMFrontline care providers
(healthcare professionals family members and others)
PATIENT
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
406
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
each of the four levels Accordingly the primary focal point is the patient and providers and systems should identify the concept of patient-centeredness as the core component of care in the VBP environment Care facilitators at all levels should shift their focus to respond to the needs of the patient and provide optimal care options Since the early 2000s patient-centeredness has been increasingly recognized and accepted by providers as being essential to success in healthcare Epstein and Street (2011) reported that patients who perceive themselves to be active participants in their care are more likely to comply with treatment and are likely to achieve better outcomes (Bell 2014) In the new VBP environment researchers should develop tools capable of capturing the contribution of patient-centeredness to value-based care Previous studies have reported that patient involvement at different levels of healthcare design and infrastructure has the potential to ensure optimal and efficient care delivery (Caixeta Bross Fabricio amp Tzortzopou-los 2013) For example investigators can compare information about service availability and care decisions from patients who interacted with patient navigators or community health workers with that from patients without such interactions to assess any differences in outcomes Therefore under a VBP environment patients should be regarded as co-creators of value whereby their input is solicited at the design stage when planning for health services product development and new technology
To correctly judge the value of care received by the patient researchers
should use the four-level model to conceptualize how information related to patient care can be effectively coordi-nated across all levels The second level in the model is the care team consist-ing of providers who have direct contact with the patient Value at this level can be achieved only when providers engage the patient in a way that utilizes evidence-based treatment guidelines and support systems to generate treat-ment plans that best suit the patientrsquos needs Some potential challenges to achieving success at this level include lack of teamwork training inadequate focus on the customerrsquos needs and providersrsquo or healthcare systemsrsquo reluc-tance to adapt to team-based care because they are accustomed to FFS practices
Organization the third level of the model establishes the infrastructure and resources necessary for the optimal delivery of health services Efficient utilization of administrative logistical and technical support adds to the value of care at this level Although value is measured from patientndashprovider encounters the organization is impor-tant with respect to guiding providers on how to use innovative processes and available resources to create value
The outer level in this model is the political and financial environment that governs healthcare through legislation and policies meant to produce effective VBP practices For instance the ACA contains provisions for establishing a VBP environment as a way to provide accountable care with favorable cost implications Promotion of integrated care under payment models such as accountable care organizations (ACOs)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

403
value-baseD aPProacHes In HealtHcare
I N T R O D U C T I O NThe US healthcare system is undergo-ing changes in care delivery and pay-ment mechanisms that reflect a shift from volume- to value-based healthcare The shift aims to replace the traditional fee-for-service (FFS) reimbursement model driven by volume and costly services to value-based purchasing (VBP) a model driven by accountability through integration of cost and quality (Conway 2009) Under this approach healthcare is moving toward a value-based system of reimbursement whereby performance or quality of care is the basis of reimbursement for providers and systems Since passage of the Affordable Care Act (ACA) in 2010 evidence has been growing that value-based approaches are being adopted by healthcare organizations Payers and consumers have gradually become more aware of the financial and health benefits of value-based care while providers are gaining familiarity with accountable care models (Werner amp Dudley 2009)
Unfortunately with all the delibera-tions and to some extent implementa-tion of the transformations related to value in healthcare the concepts of value and value-based care have been defined differently by researchers providers and healthcare organizations Because the main premise of value-based approaches is to generate a data-driven system of care reimburse-ment monitoring and service improve-ment a working definition of value must be determined and adopted for successful generation of comparable data Although there is strong agreement that value in healthcare is judged as
outcomes in relation to costs (Halm Lee amp Chassin 2002 Lohr 1988) cost savings alone should not gauge the success of value-based approaches Instead value analysis should be developed on the basis of carefully collected and measured data this analysis should be capable of producing projections in cost and other important healthcare metrics Discussions of measurements of value should incorpo-rate ideas on how to evaluate the effect of intangibles such as those influencing patient-centered care that might be important complements to value
Failure to develop an acceptable definition of value will hinder progress in achieving the intended benefits of value-based practices For example delays by healthcare professionals and organizations in adopting VBP might occur and health services may fail to achieve the desired standards and as a result create new cost threats Moreover value measurements will vary because of mixed or indistinct definitions Research and evaluation efforts that depend on the accuracy of data could be adversely affected by these inconsistencies Although increasing numbers of health-care professionals and organizations have begun using value-based approaches definitional issues mea-surements and the relationship between cost and outcomes have yet to be understood by all stakeholders
The aim of this study is to review theoretical and methodological issues related to conducting research on value-based healthcare Our intent is to help health policy researchers identify and address concerns related to research in the emerging field of VBP in healthcare
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
404
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Because cost and quality are major concerns in the US healthcare system value-based data should be readily available so that researchers can deter-mine whether VBP has led to new and favorable patterns of care
C O N C E P T U A L I S S U E S A N D T H E O R E T I C A L F R A M E W O R KHealth policy researchers need concep-tual frameworks to study understand and analyze value-based care Key conceptual issues are related to diverse sources of information and how access to these sources varies among stakeholders such as providers managers and con-sumers A classification of these sources is needed based on how they generate and make use of value-based data Various conceptual models such as that discussed by Miller (2009) have been postulated to illustrate the transition to
value-based care and the data that could be generated The conceptual issues around this transition are manifested in four aspects of healthcare provider practices clinical systems payment models and managerial systems This transition is expected to be gradual and multidimensional starting with changes in organizational structure coordination processes and internal operations
Miller (2009) depicted the transi-tion to VBP (Figure 1) The model focuses on the delivery systemrsquos transfor-mation and how it leads to transforma-tions in payment systems This framework illustrates how the definition of value may be reached when the healthcare system completes different phases of the journey to value-based care Therefore all stakeholders involved in the various stages of this transforma-tion must arrive at a common definition
F I G U R E 1 Phases of Transition From Volume-Based Care to Value-Based Care
Source Reprinted with permission from Miller (2009)
Transition in Both the Payment and the Delivery Systems
Value-driven coordinated care
Interimvirtual coordination
arrangements
Volume-driven fragmented care
Delivery system
Ideal
Transition
Today
Fee-for-service Virtual episode-of-care and comprehensive care payment
Episode-of-care or comprehensive care payment
Payment system
Failure due to lack of organizational capacity to manage value-driven payment
Co-evolution of
organization and payment
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
405
value-baseD aPProacHes In HealtHcare
when VBP becomes the dominant model of reimbursement
Several generic and disease-specific frameworks have been developed to support assessment of information at different levels and initiatives in the VBP environment
Care Delivery Value ChainThe care delivery value chain framework can help stakeholders understand the organization and structure of care delivery and thus provides a means to evaluate services delivered for a particu-lar condition (Reid Compton Gross-man amp Fanjiang 2005) This framework can be used to conceptualize how value-based data can be generated while emphasizing its application for
conditions associated with high expen-ditures The key takeaway is that this model allows value-based care to be examined and adopted for specific conditions that traditionally have been associated with high costs of care
Four-Level Healthcare System ModelFerlie and Shortell (2001) developed a model to describe a systems approach to healthcare delivery We propose a modification of this model to make it applicable to value-based care The four-level healthcare system model (Figure 2) is a potentially useful tool for studying VBP in different care settings
To achieve integrated team-based and patient-centered care researchers and providers should assess value at
F I G U R E 2 The Four-Level Healthcare System Model
Source Ferlie and Shortell (2001)
ENVIRONMENTRegulatory market and policy framework
(public and private regulators insurers healthcare purchasers research
funders et al)
ORGANIZATIONInfrastructureresources
(hospitals clinics nursing homes etc)
CARE TEAMFrontline care providers
(healthcare professionals family members and others)
PATIENT
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
406
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
each of the four levels Accordingly the primary focal point is the patient and providers and systems should identify the concept of patient-centeredness as the core component of care in the VBP environment Care facilitators at all levels should shift their focus to respond to the needs of the patient and provide optimal care options Since the early 2000s patient-centeredness has been increasingly recognized and accepted by providers as being essential to success in healthcare Epstein and Street (2011) reported that patients who perceive themselves to be active participants in their care are more likely to comply with treatment and are likely to achieve better outcomes (Bell 2014) In the new VBP environment researchers should develop tools capable of capturing the contribution of patient-centeredness to value-based care Previous studies have reported that patient involvement at different levels of healthcare design and infrastructure has the potential to ensure optimal and efficient care delivery (Caixeta Bross Fabricio amp Tzortzopou-los 2013) For example investigators can compare information about service availability and care decisions from patients who interacted with patient navigators or community health workers with that from patients without such interactions to assess any differences in outcomes Therefore under a VBP environment patients should be regarded as co-creators of value whereby their input is solicited at the design stage when planning for health services product development and new technology
To correctly judge the value of care received by the patient researchers
should use the four-level model to conceptualize how information related to patient care can be effectively coordi-nated across all levels The second level in the model is the care team consist-ing of providers who have direct contact with the patient Value at this level can be achieved only when providers engage the patient in a way that utilizes evidence-based treatment guidelines and support systems to generate treat-ment plans that best suit the patientrsquos needs Some potential challenges to achieving success at this level include lack of teamwork training inadequate focus on the customerrsquos needs and providersrsquo or healthcare systemsrsquo reluc-tance to adapt to team-based care because they are accustomed to FFS practices
Organization the third level of the model establishes the infrastructure and resources necessary for the optimal delivery of health services Efficient utilization of administrative logistical and technical support adds to the value of care at this level Although value is measured from patientndashprovider encounters the organization is impor-tant with respect to guiding providers on how to use innovative processes and available resources to create value
The outer level in this model is the political and financial environment that governs healthcare through legislation and policies meant to produce effective VBP practices For instance the ACA contains provisions for establishing a VBP environment as a way to provide accountable care with favorable cost implications Promotion of integrated care under payment models such as accountable care organizations (ACOs)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
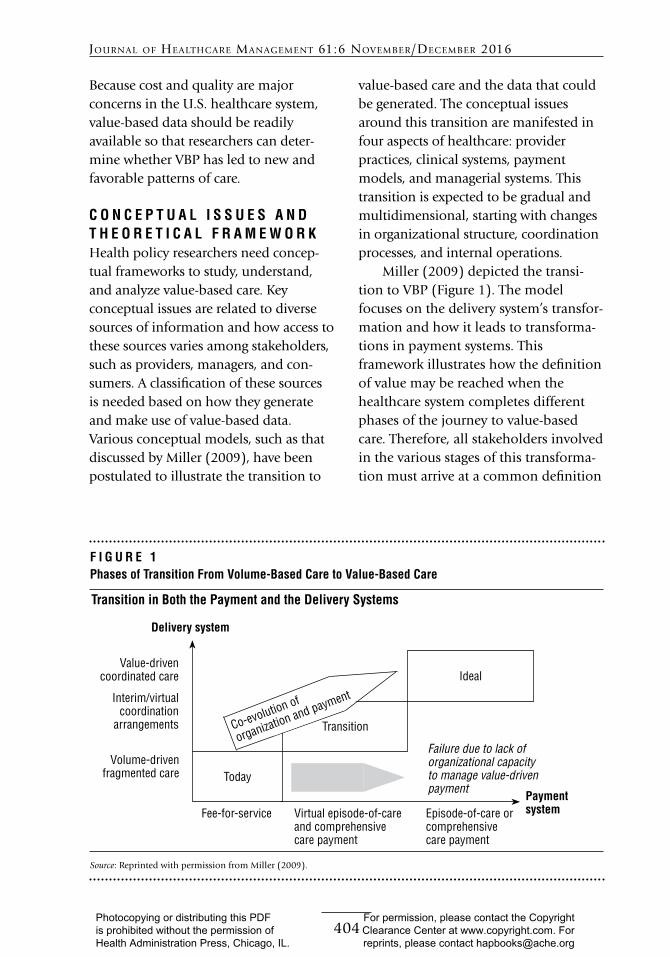
404
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Because cost and quality are major concerns in the US healthcare system value-based data should be readily available so that researchers can deter-mine whether VBP has led to new and favorable patterns of care
C O N C E P T U A L I S S U E S A N D T H E O R E T I C A L F R A M E W O R KHealth policy researchers need concep-tual frameworks to study understand and analyze value-based care Key conceptual issues are related to diverse sources of information and how access to these sources varies among stakeholders such as providers managers and con-sumers A classification of these sources is needed based on how they generate and make use of value-based data Various conceptual models such as that discussed by Miller (2009) have been postulated to illustrate the transition to
value-based care and the data that could be generated The conceptual issues around this transition are manifested in four aspects of healthcare provider practices clinical systems payment models and managerial systems This transition is expected to be gradual and multidimensional starting with changes in organizational structure coordination processes and internal operations
Miller (2009) depicted the transi-tion to VBP (Figure 1) The model focuses on the delivery systemrsquos transfor-mation and how it leads to transforma-tions in payment systems This framework illustrates how the definition of value may be reached when the healthcare system completes different phases of the journey to value-based care Therefore all stakeholders involved in the various stages of this transforma-tion must arrive at a common definition
F I G U R E 1 Phases of Transition From Volume-Based Care to Value-Based Care
Source Reprinted with permission from Miller (2009)
Transition in Both the Payment and the Delivery Systems
Value-driven coordinated care
Interimvirtual coordination
arrangements
Volume-driven fragmented care
Delivery system
Ideal
Transition
Today
Fee-for-service Virtual episode-of-care and comprehensive care payment
Episode-of-care or comprehensive care payment
Payment system
Failure due to lack of organizational capacity to manage value-driven payment
Co-evolution of
organization and payment
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
405
value-baseD aPProacHes In HealtHcare
when VBP becomes the dominant model of reimbursement
Several generic and disease-specific frameworks have been developed to support assessment of information at different levels and initiatives in the VBP environment
Care Delivery Value ChainThe care delivery value chain framework can help stakeholders understand the organization and structure of care delivery and thus provides a means to evaluate services delivered for a particu-lar condition (Reid Compton Gross-man amp Fanjiang 2005) This framework can be used to conceptualize how value-based data can be generated while emphasizing its application for
conditions associated with high expen-ditures The key takeaway is that this model allows value-based care to be examined and adopted for specific conditions that traditionally have been associated with high costs of care
Four-Level Healthcare System ModelFerlie and Shortell (2001) developed a model to describe a systems approach to healthcare delivery We propose a modification of this model to make it applicable to value-based care The four-level healthcare system model (Figure 2) is a potentially useful tool for studying VBP in different care settings
To achieve integrated team-based and patient-centered care researchers and providers should assess value at
F I G U R E 2 The Four-Level Healthcare System Model
Source Ferlie and Shortell (2001)
ENVIRONMENTRegulatory market and policy framework
(public and private regulators insurers healthcare purchasers research
funders et al)
ORGANIZATIONInfrastructureresources
(hospitals clinics nursing homes etc)
CARE TEAMFrontline care providers
(healthcare professionals family members and others)
PATIENT
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
406
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
each of the four levels Accordingly the primary focal point is the patient and providers and systems should identify the concept of patient-centeredness as the core component of care in the VBP environment Care facilitators at all levels should shift their focus to respond to the needs of the patient and provide optimal care options Since the early 2000s patient-centeredness has been increasingly recognized and accepted by providers as being essential to success in healthcare Epstein and Street (2011) reported that patients who perceive themselves to be active participants in their care are more likely to comply with treatment and are likely to achieve better outcomes (Bell 2014) In the new VBP environment researchers should develop tools capable of capturing the contribution of patient-centeredness to value-based care Previous studies have reported that patient involvement at different levels of healthcare design and infrastructure has the potential to ensure optimal and efficient care delivery (Caixeta Bross Fabricio amp Tzortzopou-los 2013) For example investigators can compare information about service availability and care decisions from patients who interacted with patient navigators or community health workers with that from patients without such interactions to assess any differences in outcomes Therefore under a VBP environment patients should be regarded as co-creators of value whereby their input is solicited at the design stage when planning for health services product development and new technology
To correctly judge the value of care received by the patient researchers
should use the four-level model to conceptualize how information related to patient care can be effectively coordi-nated across all levels The second level in the model is the care team consist-ing of providers who have direct contact with the patient Value at this level can be achieved only when providers engage the patient in a way that utilizes evidence-based treatment guidelines and support systems to generate treat-ment plans that best suit the patientrsquos needs Some potential challenges to achieving success at this level include lack of teamwork training inadequate focus on the customerrsquos needs and providersrsquo or healthcare systemsrsquo reluc-tance to adapt to team-based care because they are accustomed to FFS practices
Organization the third level of the model establishes the infrastructure and resources necessary for the optimal delivery of health services Efficient utilization of administrative logistical and technical support adds to the value of care at this level Although value is measured from patientndashprovider encounters the organization is impor-tant with respect to guiding providers on how to use innovative processes and available resources to create value
The outer level in this model is the political and financial environment that governs healthcare through legislation and policies meant to produce effective VBP practices For instance the ACA contains provisions for establishing a VBP environment as a way to provide accountable care with favorable cost implications Promotion of integrated care under payment models such as accountable care organizations (ACOs)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
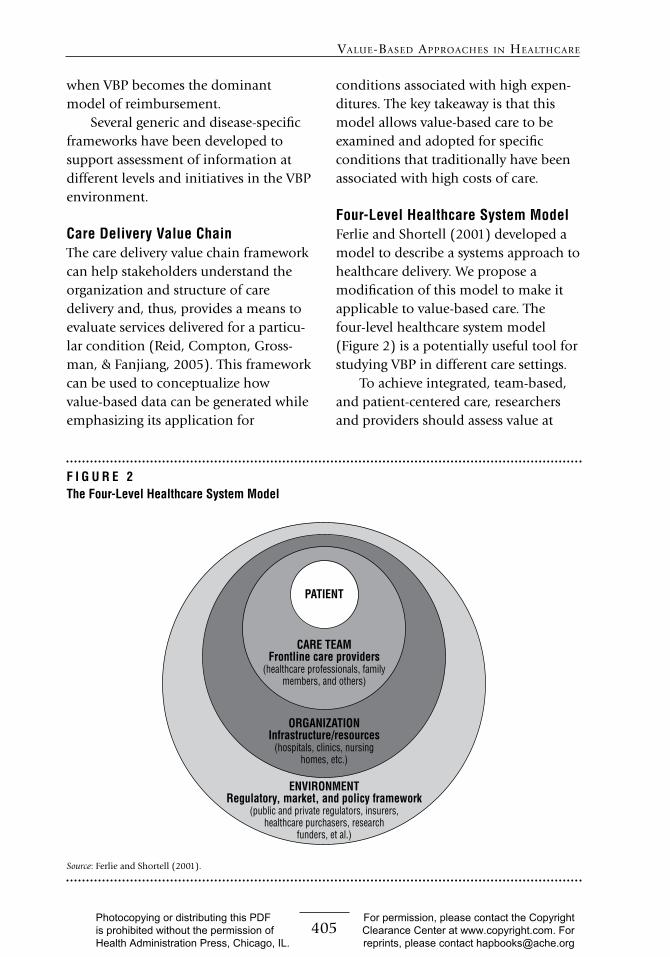
405
value-baseD aPProacHes In HealtHcare
when VBP becomes the dominant model of reimbursement
Several generic and disease-specific frameworks have been developed to support assessment of information at different levels and initiatives in the VBP environment
Care Delivery Value ChainThe care delivery value chain framework can help stakeholders understand the organization and structure of care delivery and thus provides a means to evaluate services delivered for a particu-lar condition (Reid Compton Gross-man amp Fanjiang 2005) This framework can be used to conceptualize how value-based data can be generated while emphasizing its application for
conditions associated with high expen-ditures The key takeaway is that this model allows value-based care to be examined and adopted for specific conditions that traditionally have been associated with high costs of care
Four-Level Healthcare System ModelFerlie and Shortell (2001) developed a model to describe a systems approach to healthcare delivery We propose a modification of this model to make it applicable to value-based care The four-level healthcare system model (Figure 2) is a potentially useful tool for studying VBP in different care settings
To achieve integrated team-based and patient-centered care researchers and providers should assess value at
F I G U R E 2 The Four-Level Healthcare System Model
Source Ferlie and Shortell (2001)
ENVIRONMENTRegulatory market and policy framework
(public and private regulators insurers healthcare purchasers research
funders et al)
ORGANIZATIONInfrastructureresources
(hospitals clinics nursing homes etc)
CARE TEAMFrontline care providers
(healthcare professionals family members and others)
PATIENT
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
406
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
each of the four levels Accordingly the primary focal point is the patient and providers and systems should identify the concept of patient-centeredness as the core component of care in the VBP environment Care facilitators at all levels should shift their focus to respond to the needs of the patient and provide optimal care options Since the early 2000s patient-centeredness has been increasingly recognized and accepted by providers as being essential to success in healthcare Epstein and Street (2011) reported that patients who perceive themselves to be active participants in their care are more likely to comply with treatment and are likely to achieve better outcomes (Bell 2014) In the new VBP environment researchers should develop tools capable of capturing the contribution of patient-centeredness to value-based care Previous studies have reported that patient involvement at different levels of healthcare design and infrastructure has the potential to ensure optimal and efficient care delivery (Caixeta Bross Fabricio amp Tzortzopou-los 2013) For example investigators can compare information about service availability and care decisions from patients who interacted with patient navigators or community health workers with that from patients without such interactions to assess any differences in outcomes Therefore under a VBP environment patients should be regarded as co-creators of value whereby their input is solicited at the design stage when planning for health services product development and new technology
To correctly judge the value of care received by the patient researchers
should use the four-level model to conceptualize how information related to patient care can be effectively coordi-nated across all levels The second level in the model is the care team consist-ing of providers who have direct contact with the patient Value at this level can be achieved only when providers engage the patient in a way that utilizes evidence-based treatment guidelines and support systems to generate treat-ment plans that best suit the patientrsquos needs Some potential challenges to achieving success at this level include lack of teamwork training inadequate focus on the customerrsquos needs and providersrsquo or healthcare systemsrsquo reluc-tance to adapt to team-based care because they are accustomed to FFS practices
Organization the third level of the model establishes the infrastructure and resources necessary for the optimal delivery of health services Efficient utilization of administrative logistical and technical support adds to the value of care at this level Although value is measured from patientndashprovider encounters the organization is impor-tant with respect to guiding providers on how to use innovative processes and available resources to create value
The outer level in this model is the political and financial environment that governs healthcare through legislation and policies meant to produce effective VBP practices For instance the ACA contains provisions for establishing a VBP environment as a way to provide accountable care with favorable cost implications Promotion of integrated care under payment models such as accountable care organizations (ACOs)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

406
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
each of the four levels Accordingly the primary focal point is the patient and providers and systems should identify the concept of patient-centeredness as the core component of care in the VBP environment Care facilitators at all levels should shift their focus to respond to the needs of the patient and provide optimal care options Since the early 2000s patient-centeredness has been increasingly recognized and accepted by providers as being essential to success in healthcare Epstein and Street (2011) reported that patients who perceive themselves to be active participants in their care are more likely to comply with treatment and are likely to achieve better outcomes (Bell 2014) In the new VBP environment researchers should develop tools capable of capturing the contribution of patient-centeredness to value-based care Previous studies have reported that patient involvement at different levels of healthcare design and infrastructure has the potential to ensure optimal and efficient care delivery (Caixeta Bross Fabricio amp Tzortzopou-los 2013) For example investigators can compare information about service availability and care decisions from patients who interacted with patient navigators or community health workers with that from patients without such interactions to assess any differences in outcomes Therefore under a VBP environment patients should be regarded as co-creators of value whereby their input is solicited at the design stage when planning for health services product development and new technology
To correctly judge the value of care received by the patient researchers
should use the four-level model to conceptualize how information related to patient care can be effectively coordi-nated across all levels The second level in the model is the care team consist-ing of providers who have direct contact with the patient Value at this level can be achieved only when providers engage the patient in a way that utilizes evidence-based treatment guidelines and support systems to generate treat-ment plans that best suit the patientrsquos needs Some potential challenges to achieving success at this level include lack of teamwork training inadequate focus on the customerrsquos needs and providersrsquo or healthcare systemsrsquo reluc-tance to adapt to team-based care because they are accustomed to FFS practices
Organization the third level of the model establishes the infrastructure and resources necessary for the optimal delivery of health services Efficient utilization of administrative logistical and technical support adds to the value of care at this level Although value is measured from patientndashprovider encounters the organization is impor-tant with respect to guiding providers on how to use innovative processes and available resources to create value
The outer level in this model is the political and financial environment that governs healthcare through legislation and policies meant to produce effective VBP practices For instance the ACA contains provisions for establishing a VBP environment as a way to provide accountable care with favorable cost implications Promotion of integrated care under payment models such as accountable care organizations (ACOs)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

407
value-baseD aPProacHes In HealtHcare
and bundled payment is one of the provisions of the ACA aimed at improv-ing quality and reducing the cost of care (Aroh Colella Douglas amp Eddings 2015) The key takeaway from the four-level model is its placement of the patient at the center amid all other aspects of care that contribute to enhanced value-based health services
Donabedian ModelTechniques for evaluating health services based on value need to be established at various care levels so that quality can be measured accurately For instance the Donabedian Model identifies meaning-ful classifications of measurements that can be used to assess value (Teckie McCloskey amp Steinberg 2014) Accord-ing to this model investigators can measure quality on the basis of three categories structure process and outcome This framework has been applied widely in quality and outcomes assessment For example researchers used the Donabedian model of patient safety to examine risks and hazards in the structure of care that can lead to negative patient outcomes (Gustafson Beaubien Salas amp Barach 2005) The key takeaway from this model is its ability to guide researchers and care providers in assessing value in different dimensions of care that might provide additive or multiplicative benefit
Porterrsquos FrameworkA conceptual framework that can help to clarify definitional and measurement issues regarding the concept of value has been proposed It takes into account the patientrsquos initial diseases diagnoses reported health outcomes patient
satisfaction and other clinical and administrative factors (Porter 2010) According to this model a measure of value can be established for a specific disease or patient population However Porter acknowledged that value is a complex concept involving various interdependent factors and indicators The model proposes that value should be expressed as a function of the patientrsquos initial conditions that affect the treatment processes which in turn have an effect on disease indicators that eventually are reflected in health out-comes The key takeaway from this model is the opportunity to create and apply risk adjustments when assessing value-based care
Measurement Issues in Conducting Research Related to Value-Based HealthcareAssessing the impact of value-based care depends on the achievements made in measuring value From the mid-1990s to the mid-2000s value measurements targeted specific health conditions and were done for the most part on an experimental basis to cover select populations (Rosenthal Landon Normand Frank amp Epstein 2006) More recently Medicarersquos pay-for- performance initiatives have been in the forefront of value-based reimbursement approaches with applications in conditions such as diabetes (Leichter 2006) heart failure and pneumonia (Kahn Ault Isenstein Potetz amp Van Gelder 2006) however even when the same health condition was compared between populations or over time varied measurements of quality were used Eventually investigators suggested
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

408
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
that selection of appropriate and consistent high-impact measures along with proper program design would be key to developing successful VBP plans (Shelton amp Saigal 2011)
Value is defined predominantly in terms of outcomes relative to cost or outcomes per cost expended (Beattie amp Nelson 2008) However this definition needs to be considered carefully because outcomes and cost are not rigidly defined constructs in healthcare For example outcomes can take different forms and might be affected by both patient factors such as the degree of illness and nonpatient factors such as geographic region while the magnitude of cost depends on the point at which the assessment is made in the episode of care In addition focusing on outcomes and cost without adequately considering the process of care might result in underrepresentation or exclusion of patient needs which might create new concerns in service delivery For example in a study of VBP programs Damberg et al (2014) found that only 17 of the programs included goals related to the patientrsquos experience of care or their perspectives on the process of care In other words the programs focused mainly on the outcomes of care rather than on the patients themselves Ulti-mately the value measure should include all services that address patientsrsquo needs and the relevant costs for a full set of interventions leading to attainment of a full set of outcomes while adjusting for patient and environmental factors (Porter amp Lee 2013) In other words the definition of value that can be applied in research should capture the total cost of care and optimal outcomes
Methodological Issues in Conducting Research Related to Value-Based HealthcareA lack of clarity in the definition of value is the leading methodological issue facing researchers in the VBP environment Without a working definition research in this field will produce only narrowly applicable results In addition other important methodological challenges such as those pertaining to data data collection and study designs might affect the quality of studies and need to be care-fully examined to inform policy researchers and providers
Availability of Data Related to Value-Based PracticesThe ability to assess different aspects of care under value-based practices depends on the amount and type of information generated from health services in which resources and providers are dedicated to VBP Relevant data need to be available in a format that allows investigators to evaluate various components of care and assign specific costs to them The pro-viderrsquos time and expertise are usually the main cost factors Other system resources such as the time needed to process patient data office space materi-als and equipment (Scanlon Chernew amp Doty 2002) also need to be included in the cost computation
Investigators have tried to evaluate VBP on the basis of expenditure data This approach might elicit clear-cut data pertaining to specific clinical conditions although the information gathered might not capture potential savings because expenses do not always equate to the actual costs (Tompkins Altman
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
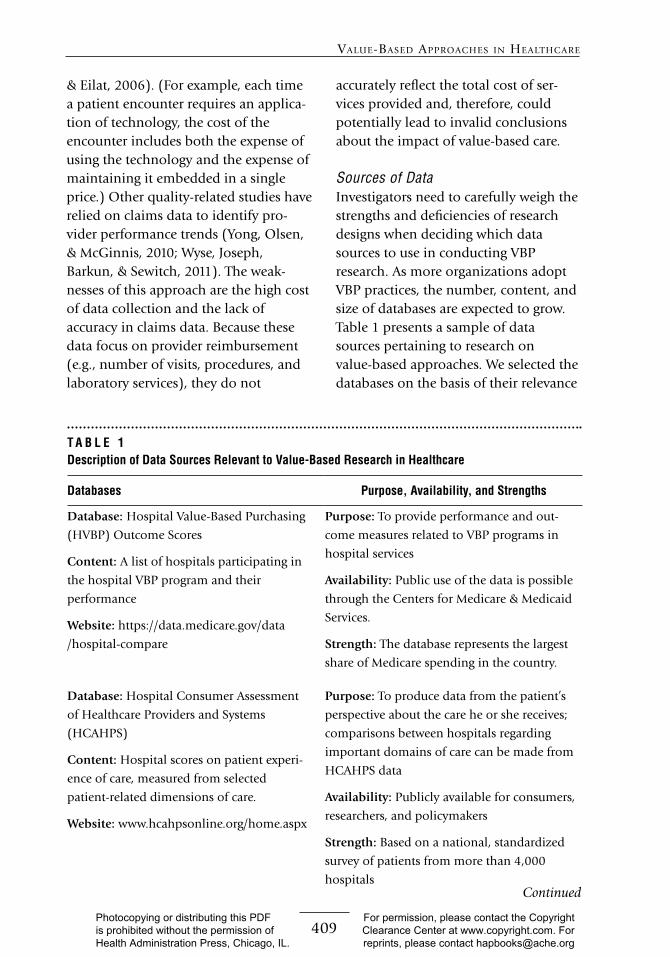
409
value-baseD aPProacHes In HealtHcare
amp Eilat 2006) (For example each time a patient encounter requires an applica-tion of technology the cost of the encounter includes both the expense of using the technology and the expense of maintaining it embedded in a single price) Other quality-related studies have relied on claims data to identify pro-vider performance trends (Yong Olsen amp McGinnis 2010 Wyse Joseph Barkun amp Sewitch 2011) The weak-nesses of this approach are the high cost of data collection and the lack of accuracy in claims data Because these data focus on provider reimbursement (eg number of visits procedures and laboratory services) they do not
accurately reflect the total cost of ser-vices provided and therefore could potentially lead to invalid conclusions about the impact of value-based care
Sources of DataInvestigators need to carefully weigh the strengths and deficiencies of research designs when deciding which data sources to use in conducting VBP research As more organizations adopt VBP practices the number content and size of databases are expected to grow Table 1 presents a sample of data sources pertaining to research on value-based approaches We selected the databases on the basis of their relevance
T A B L E 1Description of Data Sources Relevant to Value-Based Research in Healthcare
Databases Purpose Availability and Strengths
Database Hospital Value-Based Purchasing
(HVBP) Outcome Scores
Content A list of hospitals participating in
the hospital VBP program and their
performance
Website httpsdatamedicaregovdata
hospital-compare
Purpose To provide performance and out-
come measures related to VBP programs in
hospital services
Availability Public use of the data is possible
through the Centers for Medicare amp Medicaid
Services
Strength The database represents the largest
share of Medicare spending in the country
Database Hospital Consumer Assessment
of Healthcare Providers and Systems
(HCAHPS)
Content Hospital scores on patient experi-
ence of care measured from selected
patient-related dimensions of care
Website wwwhcahpsonlineorghomeaspx
Purpose To produce data from the patientrsquos
perspective about the care he or she receives
comparisons between hospitals regarding
important domains of care can be made from
HCAHPS data
Availability Publicly available for consumers
researchers and policymakers
Strength Based on a national standardized
survey of patients from more than 4000
hospitals Continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

410
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Databases Purpose Availability and Strengths
Database Colorado All Payer Claims
Database
Content Claims data featuring transparent
price quality cost of care and utilization
information across Colorado
Website httpwwwcohealthdataorg
Purpose A statewide repository of health
insurance claims information from all health-
care payers including health insurers govern-
ment programs and self-insured employer plans
Availability Publicly available to consumers
providers researchers and policymakers
Strength Availability of comprehensive prices
for hospital-based services at different admin-
istrative levels in the state
Database National Database of Nursing
Quality Indicators (NDNQI)
Data The NDNQI database contains
information relevant for measuring nursing
quality including indicators that can be
linked to important outcomes such as
hospital-acquired conditions and adverse
events The unit-level data contained in the
NDNQI make it possible for specific unit
requirements to be identified and addressed
Website httppressganeycomsolutions
clinical-qualitynursing-quality
Purpose To examine the relationship between
nursing and patient outcomes The database
includes elements of pay-for-performance
reimbursement approaches
Availability Contact NDNQI for availability
E-mail NDNQISupportpressganeycom
Strength The only national nursing database
that provides reporting of structure process
and outcome indicators for evaluation of
nursing care at the unit level
Database American College of Surgeons
National Surgical Quality Improvement
Program (NSQIP)
Data Risk-adjusted case-mixndashadjusted data
that enable surgeons and hospitals to better
assess their quality of care compared with
similar hospitals with similar types of
patients Information from patientsrsquo health
records is used for completeness and
consistency in reporting and making
comparisons More than 600000 cases are
included in the database
Website httpswwwfacsorgquality
-programsacs-nsqip
Purpose To improve the quality of surgical
care with better outcomes fewer complica-
tions and greater patient satisfaction
Availability Data are available to surgeons
clinical reviewers and researchers All requests
must be processed by NSQIP staff E-mail
techsupportacsnsqiporg
Strength Designed to benefit hospitals and
surgeons (individuals and teams) in producing
positive surgical outcomes
T A B L E 1 continued
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

411
value-baseD aPProacHes In HealtHcare
in terms of outcomes patient experi-ence and expenditures Information about the purpose availability and strength of the databases also is provided
The main purpose of the Hospital Value-Based Purchasing (HVBP) Outcome Scores Database is to list participating hospitals according to their performance and outcomes scores in relation to the hospitalrsquos VBP practices (Ryan Burgess Pesko Borden amp Dimick 2015) The Centers for Medicare amp Medicaid Services (CMS) collects and examines data from each hospital to evaluate their usefulness in value-based approaches Since it is a national-level database HVBP offers scholars a way of obtaining information about the types of care delivered and allows easy follow-up within and across facilities The Colorado All Payer Claims Database is a state-level database that includes data from commercial health plans as well as Medicare and Medicaid This compre-hensive claims dataset also contains information about important state trends since passage of the ACA in 2010
Although the list of resources presented in Table 1 is encouraging more consolidated effort is needed to create centralized sources of information that can be used to assess value Accord-ingly future research strategies need to support scholars in developing or adopting common frameworks for VBP research Organizations or systems with the potential to create databases should emphasize accessibility and interpret-ability of the information because patients and other consumers are key stakeholders in the VBP environmentmdashthey need to be aware of provider
practices and know what to expect in the processes of care under VBP
Publicly available data sources typically do not include privately owned databases because such databases are confined to proprietary use and strategic planning purposes By providing data sources in Table 1 we hope that policy researchers will be motivated to explore other state- and national-level sources of information regarding VBP initiatives Medicarersquos ACOs and other organiza-tions that follow the ACO model are examples of good sources of data According to Casalino (2014) however investigators should realize that infor-mation from the ACO models was generated during the experimental phases of the schemes and must be treated as such during different stages of research
In addition to having access to the right data policy researchers need to be familiar with the appropriate methods of handling qualitative and quantitative data generated from value-based prac-tices We review the types and strengths of these methods to guide scholars in choosing analytical methods pertaining to VBP research
Qualitative MethodsNumerous qualitative research designs have been developed that could be useful in analyzing VBP performance Three designs that have great applicabil-ity potential are grounded theory (Hysong Teal Khan amp Haidet 2012) ethnography (Kaplan et al 2014) and case studies (Kirkpatrick Smith Zapas amp Thomas 2013) (Table 2) A review of studies based on these designs revealed that information about performance
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

412
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
measures could be obtained from both clinical and nonclinical professionals demonstrating the wide applicability of qualitative analysis in investigations related to value-based care For instance as organizations and systems adopt VBP a single-case design or multicase design (Yin 2013) can be used to explore evidence of the effectiveness of VBP in and between systems A recent case study involving the state of Oregon examined the societal impact of VBP in terms of cost and other related factors (Koenig Dall Ruiz Saavoss amp Tongue 2014) The study findings showed that the value of a medical service should be based on both costs and benefits and high-expenditure services should not be discouraged solely on the basis of cost (Koenig et al 2014)
Though there are advantages to these types of approaches because they help investigators develop hypotheses regarding relationships between value-based practices and predetermined outcomes (based on experience or the patientrsquos goals for care) interviews and multiple-site visits are likely to be costly and time consuming Moreover the results of case studies are limited to the specific groups of people or organiza-tions being studied An exploratory qualitative study based on the experi-ence of 24 health plans in four states obtained in-depth information about the use of performance measures for quality improvement (Scanlon Darby Rolph amp Doty 2001) As we will discuss quantitative designs are equally useful and can be used to identify trends associated with value-based care establish associations and develop forecast models
Quantitative DesignsTable 2 presents five quantitative research designs that are useful in evaluating value-based care and corre-sponding outcomes They include cross-sectional (Chien Eastman Li amp Rosenthal 2012) casendashcontrol (Kim et al 2011) pretestposttest (Heikkinen Salanterauml Suomi Lindblom amp Leino-Kilpi 2011) longitudinal (Blu stein Borden amp Valentine 2010) and time series (Campbell Reeves Kontopantelis Sibbald amp Roland 2009) The table includes design attributes considered to be applicable to VBP research moreover examples of published studies using these designs are presented When choosing research designs for VBP studies investigators should carefully consider a number of design-related factors Researchers can design studies that either elicit findings regarding the current state of VBP approaches or create projections of the interrelationships between factors and possible causative factors in VBP practices Several quanti-tative studies have reported findings on value-based outcomes (Borah et al 2012 Gilman et al 2015 McHugh Neimeyer Powell Khare amp Adams 2013 Spaulding Zhao amp Haley 2014) These studies represent early adoption of or progressive improvements in VBP research in which varied definitions of value might have been used for different VBP strategies based on specific popula-tions or health conditions
C O N C L U S I O N S A N D R E C O M M E N D A T I O N S Although the US healthcare system has been through several reforms since the enactment of Medicare and Medicaid in
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
413
value-baseD aPProacHes In HealtHcare
the 1960s none of the reforms has affected service delivery to the extent that VBP is poised to revolutionize the field With its focus on the patient in planning and service delivery the VBP concept leads stakeholders to make major revisions to their traditional roles Stakeholders in key categories of con-sumers providers and purchasers have to shift their attention to assessing the value of healthcare services To foster research and produce improvements in care associated with higher-quality and less-costly care in the VBP environment it is imperative that the concept of value be unambiguous in its meaning defini-tion measurement and context of use
As research related to value-based approaches grows the healthcare system should be consistent in generating pertinent data that can be examined for variations and trends in key aspects of service delivery Meaningful research will be conducted by understanding and overcoming conceptual and method-ological challenges in assessing value and VBP approaches Findings from such research will help inform policy changes relevant to the new environ-ment of care because it will be based on carefully defined concepts of value and value-based care
As we have discussed sources of value-based data exist and continue to emerge as VBP gains ground in health-care Although this is promising many of the emerging databases may not provide generalizable information because they are developed by organiza-tions defining value in the context of their individual strategic plans Before conducting VBP investigations research-ers should carefully consider the sources
and types of available data With its vast base of patients and power to influence delivery CMS should take a leading role in encouraging healthcare organizations to continue developing their value capabilities and build national-level data sources Medicare ACOs whose design is based on a VBP scheme provide the best opportunity for genera-tion of rich data related to value
As we have shown value can be assessed at the patient provider organi-zation or population level in different processes of care We hope researchers will consider developing new frame-works or use existing theoretical frame-works including those discussed earlier to delineate these assessment levels in relation to VBP Such frameworks can be used to better understand the concept of value and allow for systematic analysis of value-based data and incorporation of different levels of care together with their possible interactions In the long run these models should be used to determine how providers and systems respond to VBP strategies and serve as a guide to find ways to improve value We hope that stakeholder collaborations and contributions will be better under-stood and effectively managed as the frameworks inform these groups about their specific roles in the new environ-ment of service delivery
VBP has the potential to signifi-cantly change the way care is delivered in the United States Careful planning of service delivery strategies and incorpora-tion of multistakeholder approaches will help researchers and policymakers overcome conceptual and practical challenges associated with conducting research in this era of transformation
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
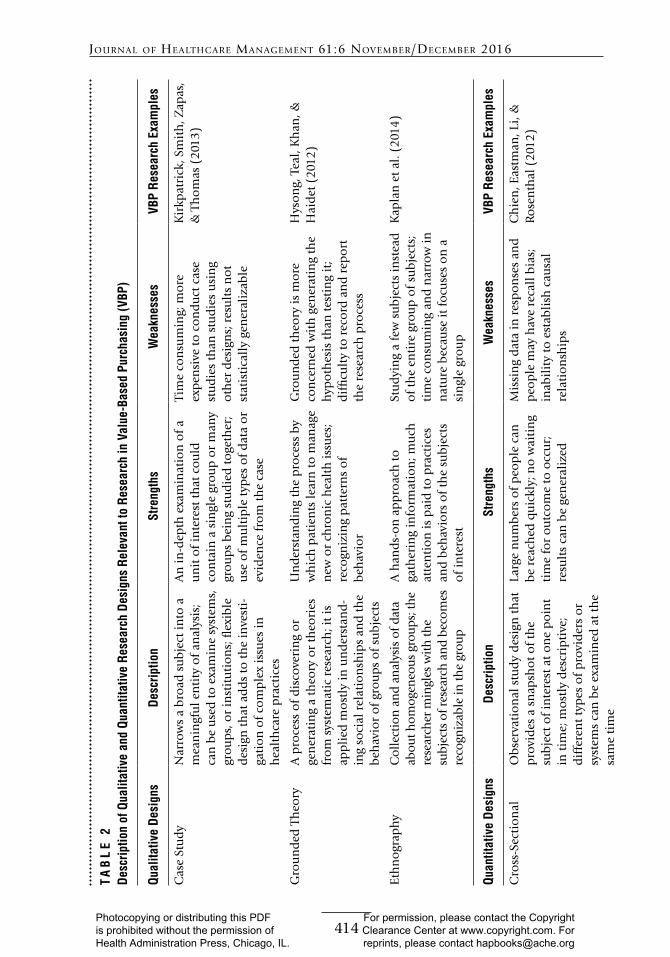
414
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
TA
BL
E 2
Desc
riptio
n of
Qua
litat
ive
and
Quan
titat
ive
Rese
arch
Des
igns
Rel
evan
t to
Rese
arch
in V
alue
-Bas
ed P
urch
asin
g (V
BP)
Qual
itativ
e De
sign
sDe
scrip
tion
Stre
ngth
sW
eakn
esse
sVB
P Re
sear
ch E
xam
ples
Cas
e St
ud
yN
arro
ws
a b
road
su
bje
ct in
to a
m
ean
ingf
ul e
nti
ty o
f an
alys
is
can
be
use
d to
exa
min
e sy
stem
s
gro
up
s o
r in
stit
uti
on
s fl
exib
le
des
ign
th
at a
dd
s to
th
e in
vest
i-ga
tio
n o
f co
mp
lex
issu
es in
h
ealt
hca
re p
ract
ices
An
in-d
epth
exa
min
atio
n o
f a
un
it o
f in
tere
st t
hat
co
uld
co
nta
in a
sin
gle
gro
up
or
man
y gr
ou
ps
bei
ng
stu
die
d t
oge
ther
u
se o
f m
ult
iple
typ
es o
f d
ata
or
evid
ence
fro
m t
he
case
Tim
e co
nsu
min
g m
ore
ex
pen
sive
to
co
nd
uct
cas
e st
ud
ies
than
stu
die
s u
sin
g o
ther
des
ign
s r
esu
lts
no
t st
atis
tica
lly
gen
eral
izab
le
Kir
kpat
rick
Sm
ith
Zap
as
amp T
ho
mas
(20
13)
Gro
un
ded
Th
eory
A p
roce
ss o
f d
isco
veri
ng
or
gen
erat
ing
a th
eory
or
theo
ries
fr
om
sys
tem
atic
res
earc
h i
t is
ap
pli
ed m
ost
ly in
un
der
stan
d-
ing
soci
al r
elat
ion
ship
s an
d t
he
beh
avio
r o
f gr
ou
ps
of
sub
ject
s
Un
der
stan
din
g th
e p
roce
ss b
y w
hic
h p
atie
nts
lear
n t
o m
anag
e n
ew o
r ch
ron
ic h
ealt
h is
sues
re
cogn
izin
g p
atte
rns
of
beh
avio
r
Gro
un
ded
th
eory
is m
ore
co
nce
rned
wit
h g
ener
atin
g th
e h
ypo
thes
is t
han
tes
tin
g it
d
iffi
cult
y to
rec
ord
an
d r
epo
rt
the
rese
arch
pro
cess
Hys
on
g T
eal
Kh
an amp
H
aid
et (
2012
)
Eth
no
grap
hy
Col
lect
ion
an
d an
alys
is o
f dat
a ab
out h
omog
eneo
us g
roup
s th
e re
sear
cher
min
gles
wit
h th
e su
bjec
ts o
f res
earc
h a
nd
beco
mes
re
cogn
izab
le in
the
grou
p
A h
and
s-o
n a
pp
roac
h t
o
gath
erin
g in
form
atio
n m
uch
at
ten
tio
n is
pai
d t
o p
ract
ices
an
d b
ehav
iors
of
the
sub
ject
s o
f in
tere
st
Stu
dyi
ng
a fe
w s
ub
ject
s in
stea
d
of
the
enti
re g
rou
p o
f su
bje
cts
ti
me
con
sum
ing
and
nar
row
in
nat
ure
bec
ause
it f
ocu
ses
on
a
sin
gle
gro
up
Kap
lan
et
al (
2014
)
Quan
titat
ive
Desi
gns
Desc
riptio
nSt
reng
ths
Wea
knes
ses
VBP
Rese
arch
Exa
mpl
es
Cro
ss-S
ecti
on
al
Ob
serv
atio
nal
stu
dy
des
ign
th
at
pro
vid
es a
sn
apsh
ot
of
the
sub
ject
of
inte
rest
at
on
e p
oin
t in
tim
e m
ost
ly d
escr
ipti
ve
dif
fere
nt
typ
es o
f p
rovi
der
s o
r sy
stem
s ca
n b
e ex
amin
ed a
t th
e sa
me
tim
e
Larg
e n
um
ber
s o
f p
eop
le c
an
be
reac
hed
qu
ickl
y n
o w
aiti
ng
tim
e fo
r o
utc
om
e to
occ
ur
re
sult
s ca
n b
e ge
ner
aliz
ed
Mis
sin
g d
ata
in r
esp
on
ses
and
p
eop
le m
ay h
ave
reca
ll b
ias
in
abil
ity
to e
stab
lish
cau
sal
rela
tio
nsh
ips
Ch
ien
Eas
tman
Li
amp
Ro
sen
thal
(20
12)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
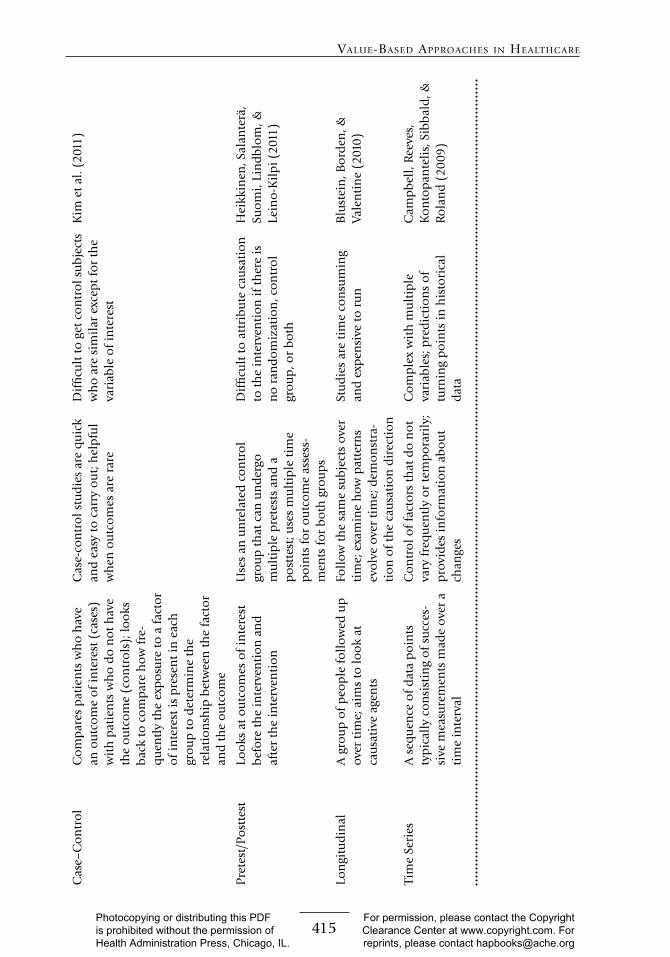
415
value-baseD aPProacHes In HealtHcare
Cas
endashC
on
tro
lC
om
par
es p
atie
nts
wh
o h
ave
an o
utc
om
e o
f in
tere
st (
case
s)
wit
h p
atie
nts
wh
o d
o n
ot
hav
e th
e o
utc
om
e (c
on
tro
ls)
loo
ks
bac
k to
co
mp
are
how
fre
-q
uen
tly
the
exp
osu
re t
o a
fac
tor
of
inte
rest
is p
rese
nt
in e
ach
gr
ou
p t
o d
eter
min
e th
e re
lati
on
ship
bet
wee
n t
he
fact
or
and
th
e o
utc
om
e
Cas
e-co
ntr
ol s
tud
ies
are
qu
ick
and
eas
y to
car
ry o
ut
hel
pfu
l w
hen
ou
tco
mes
are
rar
e
Dif
ficu
lt t
o g
et c
on
tro
l su
bje
cts
wh
o a
re s
imil
ar e
xcep
t fo
r th
e va
riab
le o
f in
tere
st
Kim
et
al (
2011
)
Pre
test
Po
stte
stLo
oks
at
ou
tco
mes
of
inte
rest
b
efo
re t
he
inte
rven
tio
n a
nd
af
ter
the
inte
rven
tio
n
Use
s an
un
rela
ted
co
ntr
ol
gro
up
th
at c
an u
nd
ergo
m
ult
iple
pre
test
s an
d a
p
ost
test
use
s m
ult
iple
tim
e p
oin
ts f
or
ou
tco
me
asse
ss-
men
ts f
or
bo
th g
rou
ps
Dif
ficu
lt t
o a
ttri
bu
te c
ausa
tio
n
to t
he
inte
rven
tio
n if
th
ere
is
no
ran
do
miz
atio
n c
on
tro
l gr
ou
p o
r b
oth
Hei
kkin
en S
alan
terauml
Su
om
i Li
nd
blo
m amp
Le
ino
-Kil
pi (
2011
)
Lon
gitu
din
al
A g
rou
p o
f p
eop
le f
oll
owed
up
ov
er t
ime
aim
s to
loo
k at
ca
usa
tive
age
nts
Foll
ow t
he
sam
e su
bje
cts
over
ti
me
exa
min
e h
ow p
atte
rns
evo
lve
over
tim
e d
emo
nst
ra-
tio
n o
f th
e ca
usa
tio
n d
irec
tio
n
Stu
die
s ar
e ti
me
con
sum
ing
and
exp
ensi
ve t
o r
un
Blu
stei
n B
ord
en amp
Va
len
tin
e (2
010)
Tim
e Se
ries
A s
equ
ence
of
dat
a p
oin
ts
typ
ical
ly c
on
sist
ing
of
succ
es-
sive
mea
sure
men
ts m
ade
over
a
tim
e in
terv
al
Co
ntr
ol o
f fa
cto
rs t
hat
do
no
t va
ry f
req
uen
tly
or
tem
po
rari
ly
pro
vid
es in
form
atio
n a
bo
ut
chan
ges
Co
mp
lex
wit
h m
ult
iple
va
riab
les
pre
dic
tio
ns
of
turn
ing
po
ints
in h
isto
rica
l d
ata
Cam
pb
ell
Ree
ves
K
on
top
ante
lis
Sib
bal
d amp
R
ola
nd
(20
09)
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

416
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Several healthcare plans and networks that have adopted some degree of VBP have reported that these approaches have benefited their organizations (Berwick 2011 Bunkers Koch McDonough amp Whited 2014 CMS 2011) This suggests a well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemes (Damberg et al 2014) Eventually policymakers and researchers will be able to assess the effectiveness of VBP objectives includ-ing cost control quality improvement and better outcomes of care
R E F E R E N C E SAroh D Colella J Douglas C amp Eddings A
(2015) An example of translating value-based purchasing into value-based care Urologic Nursing 35(2) 61ndash75
Beattie P F amp Nelson R M (2008) Preserv-ing the quality of the patient-therapist relationship An important consideration for value-centered physical therapy care Journal of Orthopaedic amp Sports Physical Therapy 38(2) 34ndash35
Bell L (2014) Patient-centered care American Journal of Critical Care 23(4) 325ndash335
Berwick D M (2011) Launching account-able care organizations The proposed rule for the Medicare Shared Savings Program New England Journal of Medi-cine 364(16) e32
Blustein J Borden W B amp Valentine M (2010) Hospital performance the local economy and the local workforce Findings from a US national longitudinal study PLoS Medicine 7(6) e1000297
Borah B J Rock M G Wood D L Roel-linger D L Johnson M G amp Naessens J M (2012) Association between value-based purchasing score and hospital characteristics BMC Health Services Research Retrieved from httpsbmc healthservresbiomedcentralcomarticles1011861472-6963-12-464
Bunkers B Koch M McDonough B amp Whited B (2014) Aligning physician
compensation with strategic goals hfm 68(7) 38ndash45
Caixeta M C B F Bross J C Fabricio M M amp Tzortzopoulos P (2013) Value genera-tion through user involvement in healthcare design In Proceedings IGLC-21 21st Annual Conference of the International Group for Lean Construction Fortaleza Brazil 299ndash308
Campbell S M Reeves D Kontopantelis E Sibbald B amp Roland M (2009) Effects of pay for performance on the quality of primary care in England New England Journal of Medicine 361(4) 368ndash378
Casalino L P (2014) Accountable care organizations The risk of failure and the risks of success New England Journal of Medicine 371(18) 1750ndash1751
Centers for Medicare amp Medicaid Services (CMS) (2011) Medicare program Hospital inpatient value-based purchasing program Final rule Federal Register 76(88) 26490ndash26547
Chien A T Eastman D Li Z amp Rosenthal M B (2012) Impact of a pay for perfor-mance program to improve diabetes care in the safety net Preventive Medicine 55(Suppl) S80ndashS85
Conway P H (2009) Value-driven health care Implications for hospitals and hospitalists Journal of Hospital Medicine 4(8) 507ndash511
Damberg C L Sorbero M E Lovejoy S L Martsolf G R Raaen L amp Mandel D (2014) Measuring success in health care value-based purchasing programs Summary and recommendations Santa Monica CA RAND Corporation Retrieved from httpwwwrandorgpubsresearch_reports RR306z1html
Epstein R M amp Street R L (2011) The values and value of patient-centered care Annals of Family Medicine 9(2) 100ndash103
Ferlie E amp Shortell S (2001) Improving the quality of health care in the United Kingdom and the United States A framework for change Milbank Quarterly 79(2) 281ndash303
Gilman M Adams E K Hockenberry J M Milstein A S Wilson I B amp Becker E R (2015) Safety-net hospitals more likely than other hospitals to fare poorly under Medicarersquos value-based purchasing Health Affairs 34(3) 398ndash405
Gustafson S Beaubien J Salas E amp Barach P (2005) Medical teamwork and patient safety
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
417
value-baseD aPProacHes In HealtHcare
The evidence-based relation Rockville MD Agency for Healthcare Research and Quality
Halm E A Lee C amp Chassin M R (2002) Is volume related to outcome in health care A systematic review and method-ological critique of the literature Annals of Internal Medicine 137(6) 511ndash520
Heikkinen K Salanterauml S Suomi R Lindblom A amp Leino-Kilpi H (2011) Ambulatory orthopaedic surgery patient education and cost of care Orthopaedic Nursing 30(1) 20ndash28
Hysong S J Teal C R Khan M J amp Haidet P (2012) Improving quality of care through improved audit and feedback Implementation Science 7(45) 1ndash22
Kahn C N Ault T Isenstein H Potetz L amp Van Gelder S (2006) Snapshot of hospital quality reporting and pay-for-performance under Medicare Health Affairs 25(1) 148ndash162
Kaplan A L Klein M P Tan H J Setlur N P Agarwal N Steinberg K amp Saigal C S (2014) Use of patient ethnography to support quality improvement in benign prostatic hyperplasia Healthcare 2(4) 263ndash267
Kim Y A Loucks A Yokoyama G Light-wood J Rascati K amp Serxner S A (2011) Evaluation of value-based insur-ance design with a large retail employer American Journal of Managed Care 17(10) 682ndash690
Kirkpatrick J R Smith B M Zapas J L amp Thomas W L (2013) Clinical impact of a value-based decision A surgical case study Journal of the American College of Surgeons 216(4) 800ndash811
Koenig L Dall T M Ruiz D Jr Saavoss J amp Tongue J (2014) Can value-based insurance impose societal costs Value in Health 17(6) 749ndash751
Leichter S B (2006) Pay-for-performance contracts in diabetes care Clinical Diabetes 24(2) 56ndash59
Lohr K N (1988) Outcome measurement Concepts and questions Inquiry 25(1) 37ndash50
McHugh M Neimeyer J Powell E Khare R K amp Adams J G (2013) An early look at performance on the emergency care measures included in Medicarersquos hospital inpatient value-based purchasing program Annals of Emergency Medicine 61(6) 515ndash623
Miller H D (2009) From volume to value Better ways to pay for health care Health Affairs 28(5) 1418ndash1428
Porter M E (2010) What is value in health care New England Journal of Medicine 363(26) 2477ndash2481
Porter M E amp Lee T H (2013) The strategy that will fix health care Harvard Business Review 91(10) 50ndash70
Reid P P Compton W D Grossman J H amp Fanjiang G (2005) Building a better delivery system A new engineeringhealth care partnership Washington DC The National Academies Press
Rosenthal M B Landon B E Normand S L T Frank R G amp Epstein A M (2006) Pay for performance in commer-cial HMOs New England Journal of Medicine 355(18) 1895ndash1902
Ryan A M Burgess J F Pesko M F Borden W B amp Dimick J B (2015) The early effects of Medicarersquos mandatory hospital pay-for-performance program Health Services Research 50(1) 81ndash97
Scanlon D P Chernew M amp Doty H E (2002) Evaluating the impact of value-based purchasing A guide for purchasers Rockville MD Agency for Healthcare Research and Quality Retrieved from httparchiveahrqgovprofessionalsquality-patient -safetyquality-resourcesvaluevalue basedevalvbp2html
Scanlon D P Darby C Rolph E amp Doty H E (2001) The role of performance measures for improving quality in managed care organizations Health Services Research 36(3) 619ndash641
Shelton J B amp Saigal C S (2011) The crossroads of evidence-based medicine and health policy Implications for urology World Journal of Urology 29(3) 283ndash289
Spaulding A Zhao M amp Haley D R (2014) Value-based purchasing and hospital acquired conditions Are we seeing improvement Health Policy 118(3) 413ndash421
Teckie S McCloskey S A amp Steinberg M L (2014) Value A framework for radiation oncology Journal of Clinical Oncology 32(26) 2864ndash2870
Tompkins C P Altman S H amp Eilat E (2006) The precarious pricing system for hospital services Health Affairs 25(1) 45ndash56
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

418
Journal of HealtHcare ManageMent 616 noveMberDeceMber 2016
Werner R M amp Dudley R A (2009) Making the lsquopayrsquo matter in pay-for-performance Implications for payment strategies Health Affairs 28(5) 1498ndash1508
Wyse J M Joseph L Barkun A N amp Sewitch M J (2011) Accuracy of adminis-trative claims data for polypectomy Canadian Medical Association Journal 183(11) E743ndashE747
Yin R K (2013) Case study research Design and methods Thousand Oaks CA Sage Publications
Yong P L Olsen L A amp McGinnis J M (2010) Value in healthcare Accounting for cost quality safety outcomes and innovation Washington DC The National Academies Press
P R A C T I T I O N E R A P P L I C A T I O N
Elizabeth W Brady MD FACS director Quality Safety and Patient Experience Hartford Health Care Medical Group Hartford Connecticut
Mkanta et al have astutely described the current state of confusion as it pertains to qualitatively and quantitatively assessing the effects of changes in healthcare as
it transitions from volume to value The Affordable Care Act has catalyzed an incred-ible rate of change in healthcare and this report highlights the need for standardiza-tion of measurement and reporting of outcomes in a universally understandable language
The premise that more care does not lead to better care has been well docu-mented by the Dartmouth Atlas and other sources The transition from volume-based to value-based care stems from the fact that US healthcare costs have continued to climb at an unsustainable rate and our outcomes are mediocre at best when com-pared with those in other countries The transition to patient-centered care is in keeping with the need for consumers to become more involved in their healthcare Transparency in costs and outcomes is inevitable and with it comes the need to court the favor of healthcare consumersmdashpayers patients and providers
This article highlights the challenges faced in determining value Although there may be general agreement regarding the definition of value (ie outcomescosts) consensus is lacking in the determinants of costs and the methods used to report outcomes vary greatly The authors put forth an excellent case for agreeing first on the definition and they follow this with examples of qualitative and quantitative meth-ods to determine value
The authors state that the value measure should include all services that address patientsrsquo needs while incorporating relevant costs for a full set of outcomes and adjusting for patient and environmental factors The premise that researchers and ultimately policymakers should agree on the definition of outcomes costs and value as they pertain to healthcare before amassing large volumes of confusing literature on the subject seems obvious
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg
419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg

419
value-baseD aPProacHes In HealtHcare
In our healthcare delivery system in Connecticut we emphasize patient-centered-ness via a defined strategic initiative in patient experience Providersrsquo compensation is tied to patient experience scores We measure patient satisfaction by means of surveys that have been scientifically validated and are used by more than 1000 healthcare entities throughout the United States We are bombarded by the media almost daily with reports comparing our outcomes with those in other healthcare organizations locally regionally and nationally often the methods used to compare performance are indecipherable We are competing in a field in which success can be determined through subjective interpretation and presentation of outcome data along with superior marketing capabilities A system of accurate comparison would pave the way for competition that results in better care and outcomes for patients
Mkanta et al conclude that ldquoa well-defined coordinated research strategy needs to be developed to generate information that will allow researchers to assess the effectiveness of VBP schemesrdquo Eventually policymakers and researchers can effec-tively assess the goals of value-based performance schemes including cost control quality improvement and better outcomes of care How to develop and coordinate this research strategy will be a challenge for researchers and other stakeholders
Photocopying or distributing this PDF is prohibited without the permission of Health Administration Press Chicago IL
For permission please contact the Copyright Clearance Center at wwwcopyrightcom For reprints please contact hapbooksacheorg