theoretical foundation of nursing
DESCRIPTION
This presentation comprises of the different concepts of nursing theories and their uses.TRANSCRIPT

Theoretical Foundation of Theoretical Foundation of Nursing Nursing
CONCEPTCONCEPT
A mental idea of a phenomenon A comprehensive idea or generalization An idea that brings diverse elements into a
basic relationship A unit of knowledge abstracted from a set of
characteristics attributed to a class of objects, relations or entities.

A unit of thought A general idea formed in the mind Something understood or retained in
the mind.
Concepts are basically vehicles of thought that involve images. Concepts are words that describe objects, properties, or events & are basic components of theory.
Conceptual Framework/ Conceptual Framework/ ModelModel
Framework is a basic structure supporting anything.
A set of interrelated concepts that symbolically represents and conveys a mental image of phenomenon. Conceptual models of nursing identify concepts and describe their relationships to a phenomena of central concern to the discipline
(Power & Knapp)

A group of related concepts. It provides an overall view to focus our thoughts. It can be visualized as an umbrella under which many theories can exist.(Creasia & Parker)

TheoryTheory
A set of statements that tentatively describe, explain, or predict relationships among concepts that have been systematically selected and organized as an abstract representation of some phenomenon (power & Knapp)
Theory serves as guides for nursing action in administration, education, research, and practice.
Nursing Theory is a group of related concepts that derived from the nursing models.
A body of knowledge that describes or explains nursing and is used to support nursing practice.
Nursing TheoryNursing Theory
PrinciplePrinciple
A basic generalization that is accepted as true and that can be used as a basis for reasoning or conduct.
Characteristics of a TheoryCharacteristics of a Theory

Interrelating concepts in such a way as to create a different way of looking at a particular phenomenon.
Logical in nature.Generalizable.Basis for hypotheses that can be
tested.
Increasing the general body of knowledge within the discipline through the research implemented to validate them.
Used by the practitioners to guide and improve their practice.
Consistent with other validated theories, laws, and principles but will leave open unanswered Q that need to be investigated.

Components of a TheoryComponents of a Theory

ConceptsDefinitionsAssumptionsPhenomenon

A nursing theory is a set of concepts, definitions, relationships, and assumptions or propositions derived from nursing models or from other disciplines and project a purposive, systematic view of phenomena by designing specific interrelationships among concepts for the purposes of describing, explaining, predicting, and /or prescribing..

ConceptConcept
A theory is composed of interrelated concepts
Ex: Levine’s Conservation Model3 Major concepts: Conservation
Adaptation Wholeness
King’s Theory of Goal Attainment
Critical concepts to goal attainment in nrsg practice:Personal systemsInterpersonal systemsSocial systems

DefinitionsDefinitions
The definitions within the description of a theory convey the general meaning of the concepts in a manner that fits the theory.

AssumptionsAssumptions
Are statements that describe concepts or connect two concepts that are factual. They are the “taken for Granted” statements that determine the nature of the concepts, definitions, purpose, relationships and structure of the theory.
Ex: People & environment are open systems

PhenomenonPhenomenon
Is an aspect of reality that can be consciously sensed or experienced.
Ex: caring, self-care, client responses to stress

Types of TheoriesTypes of Theories

MetatheoriesMetatheories
are theories whose subject matters are some other theories. These are theories about theories.

Grand TheoriesGrand Theories
Are broad in scope and complex and therefore require further specification through research before they can be fully tested.These are intended to provide structural framework for broad, abstract ideas about nursing.

Middle- Range TheoriesMiddle- Range Theories
Have more limited scope, less abstraction, address specific phenomena or concepts and reflect practice.
Descriptive TheoriesDescriptive Theories
Are the first level of theory development. They describe phenomena, speculate on why phenomena occur, and describe the consequences. Have the ability to explain & relate some situations.
Ex: Theories of Growth & development
Prescriptive TheoryPrescriptive Theory
Address nursing interventions and predict the consequence of a specific nursing intervention. It is an action oriented which test the validity and predictability of a nursing intervention.
Importance of Nursing Importance of Nursing TheoriesTheories
1. Nursing theory aims to describe, predict and explain the phenomenon of nursing (Chinn and Jacobs1978).
2. It should provide the foundations of nursing practice, help to generate further knowledge and indicate in which direction nursing should develop in the future (Brown 1964).
3. It helps to distinguish what should form the basis of practice by explicitly
describing nursing.4. The main exponent of nursing –
caring – cannot be measured, it is vital to have the theory to analyze and explain what nurses do.
5. The benefits of having a defined body of theory in nursing include better patient care, enhanced professional status for nurses, improved communication between nurses, and guidance for research and education(Nolan 1996).

7. As medicine tries to make a move towards adopting a more multidisciplinary approach to health care, nursing continues to strive to establish a unique body of knowledge.

8. This can be seen as an attempt by the nursing profession to maintain its
professional boundaries.

Evolution of Nursing Evolution of Nursing TheoriesTheories
Within Types of Works

PhilosophiesPhilosophies
NightingaleWiedenbachHendersonAbdellah
HallWatsonBenner

Grand TheoriesGrand Theories
NeumanKing
Roper, Logan, and Tierney OremLevineRogersJohnson
Roy

Middle- Range TheoriesMiddle- Range Theories
Peplau Orlando LeiningerTravelbee ParseKolcaba PenderErickson, Tomlin, and Swain NewmanMercer Adam
Purposes of TheoriesPurposes of Theories

In PracticeIn Practice
Assist nurses to describe, explain, and predict everyday experiences.
Serve to guide assessment, intervention, and evaluation of nursing care.

Provide a rationale for collecting reliable and valid data about the health status of clients, which are essential for effective decision making and implementation.
Help to establish criteria to measure the quality of nursing care
Help build a common nursing terminology to use in communicating with other health professionals. Ideas are developed and words defined.
Enhance autonomy (independence and self-governance) of nursing by defining its own independent functions.

In EducationIn Education
Provide a general focus for curriculum design.
Guide curricular decision making.

In ResearchIn Research
Offer a framework for generating knowledge and new ideas.
Assist in discovering knowledge gaps in specific field of study.
Offer a systematic approach to identify questions for study, select variables, interpret findings, and validate nursing interventions.
Nursing ParadigmNursing Paradigm
It has a model or paradigm that explains the linkages of science, philosophy, and theory that is accepted and applied by the discipline.

4 major concepts of nursing 4 major concepts of nursing theoriestheories
Four concepts common in nursing theory that influence and determine nursing practice are
--- The person( patient) .--- The environment--- Health--- Nursing (goals, roles, functions)

Each of these concepts is usually defined and described by a nursing theorist.
Of the four concepts , the most important is that of the PERSON. The focus of nursing , regardless of definition or theory.
PersonPerson
Refers to all human beings. They are the recipients of nursing care
Individuals, families, communities and groups

EnvironmentEnvironment
Includes factors that affect individuals internally and externally, not only everyday surroundings but also settings where nursing care is provided.

HealthHealth
Addresses the person’s state of well-being.
Degree of wellness or illness experienced by the person

NursingNursing
Actions, characteristics and attributes of person giving care
Describe what Nursing is, what nurses do, and how nurses interact with clients.
It is the Diagnosis and Treatment of human responses to actual or potential Health Problems.
NON- NURSING THEORIESNON- NURSING THEORIESUSED IN NURSING

General Systems TheoryGeneral Systems Theory
It describes how to break whole things into parts & then to learn how the parts work together in “systems”. These concepts may be applied to different kinds of systems
e.g. Molecules in chemistry, cultures in sociology, and organs in Anatomy & Health in Nursing.
Nursing ModelsNursing Models
Imogene King’s Systems Interaction Model
Betty Neuman’s Health Care System Model
Dorothy Johnson’s Behavioral System Model
Change Theory Change Theory Kurt Lewin (1962)Kurt Lewin (1962)
People grow and change throughout their lives. This growth and change are evident in the dynamic nature of basic human needs and how they are met.
3 states of change3 states of change
1. Unfreezing- is the recognition of the need for change and the dissolution of previously held patterns of behavior.
2. Movement- is the shift of behavior toward a new and more healthful pattern.
3. Refreezing- is the long-term solidification of the new pattern of behavior.

Developmental TheoryDevelopmental Theory
Human Growth and Development is an orderly predictive process that begins with conception and continues through death.

4 Main Areas of 4 Main Areas of Developmental TheoryDevelopmental Theory
A. Biophysical developmentB. Psychoanalytic/ Psychosocial Development
C. Cognitive DevelopmentD. Moral Development
Biophysical DevelopmentBiophysical Development
Attempts to describe the way our physical bodies grow & change.
Ex: Geselle’s Theory of Development

Psychosocial DevelopmentPsychosocial Development
Attempts to describe the development of the human personality, behavior and emotions.
Ex: Sigmund Freud’s Psychoanalytic Model of Personality Development
5 Psychosexual Developmental Stages
Sigmund Freud’s
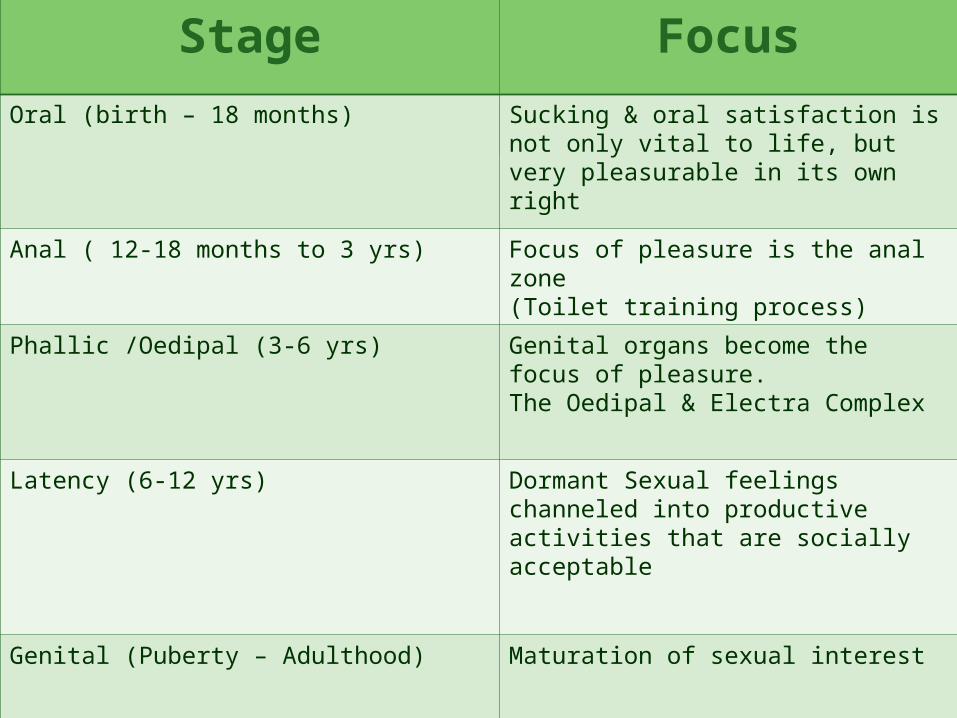
Stage Focus
Oral (birth – 18 months) Sucking & oral satisfaction is not only vital to life, but very pleasurable in its own right
Anal ( 12-18 months to 3 yrs) Focus of pleasure is the anal zone(Toilet training process)
Phallic /Oedipal (3-6 yrs) Genital organs become the focus of pleasure.The Oedipal & Electra Complex
Latency (6-12 yrs) Dormant Sexual feelings channeled into productive activities that are socially acceptable
Genital (Puberty – Adulthood) Maturation of sexual interest

Psychosocial TheoryPsychosocial Theory
Erik Erickson’sErik Erickson’s

Individuals need to accomplish a particular task before successfully completing the stage.
Each task is framed with opposing conflicts, such as the adolescent’s need to develop a sense identity challenged by many confusing choices.
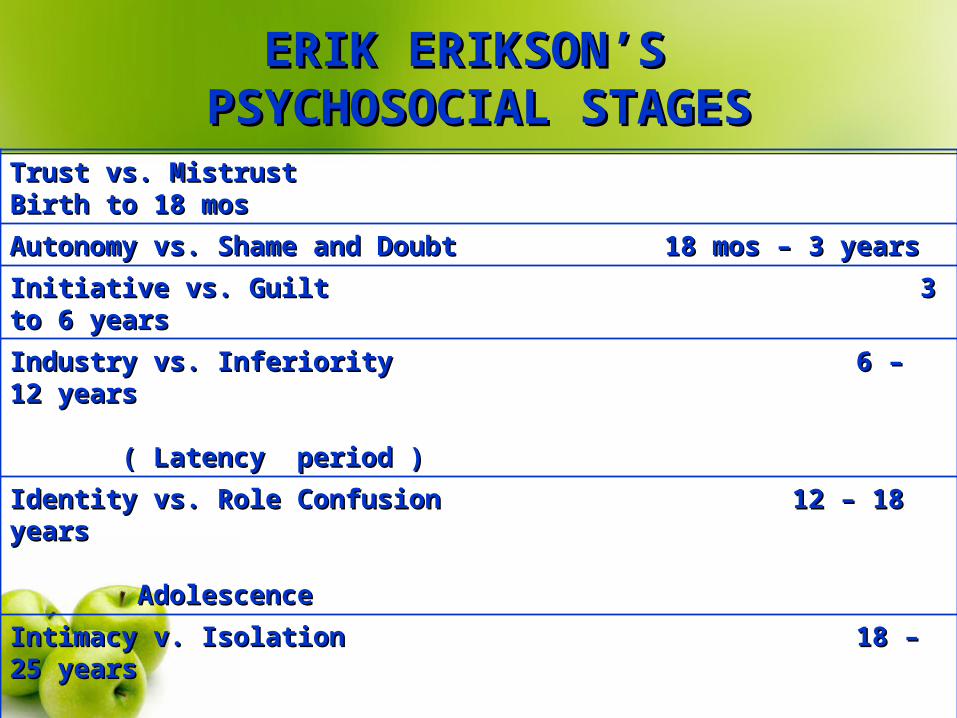
ERIK ERIKSON’S ERIK ERIKSON’S PSYCHOSOCIAL STAGESPSYCHOSOCIAL STAGES
Trust vs. Mistrust Birth to 18 mosTrust vs. Mistrust Birth to 18 mos
Autonomy vs. Shame and Doubt 18 mos – 3 years Autonomy vs. Shame and Doubt 18 mos – 3 years
Initiative vs. Guilt 3 to 6 yearsInitiative vs. Guilt 3 to 6 years
Industry vs. Inferiority 6 – 12 yearsIndustry vs. Inferiority 6 – 12 years ( Latency period ) ( Latency period )
Identity vs. Role Confusion 12 – 18 yearsIdentity vs. Role Confusion 12 – 18 years AdolescenceAdolescence
Intimacy v. Isolation 18 – 25 yearsIntimacy v. Isolation 18 – 25 years (Early Adulthood)(Early Adulthood)
Generativity vs. Stagnation 25 – 65 years Generativity vs. Stagnation 25 – 65 years (Adulthood)(Adulthood)
Ego Integrity vs. Despair 65 years and olderEgo Integrity vs. Despair 65 years and older








PhilosophiesPhilosophies
Florence Nightingale
Florence Nightingale’s work is closely related to her philosophical orientation of the patient environment interaction and the principles and rules on which nursing practice was founded. Nightingale believed that disease was a reparative process. Patient’s surroundings-ventilation, warmth, light, diet, cleanliness and noise-would contribute to the reparative process and the health of the patient. Notes on Nursing: What it is and what it is not.
Ernestine Wiedenbach concentrated on the art of nursing and focused on the needs of the patient. It guides the nurse’s action in the art of nursing.
Four Elements:
1. Philosophy 3. Practice
2. Purpose 4. Art
Postulated that clinical nursing is directed toward meeting the patient’s perceived need-for-help. Clinical Nursing: A Helping Art.
Virginia Henderson viewed the patient as an individual requiring help toward achieving independence. She envisioned the practice of nursing as independent from the practice of the physicians and acknowledges her interpretation of the nurse’s function as a synthesis of many influences. Henderson emphasized the art of nursing and identified the 14 basic human needs on which nursing care is based. Her definition of nursing first appeared in 1995 in the fifth edition of Textbook of the Principles and Practice of Nursing by Harmer and Henderson.
Henderson stated, “The unique function of the nurse is to assist the individual sick or well, in the performance of those activities contributing to health or its recovery (or to peaceful death)” that he would perform unaided if he had the necessary strength. She identified the following 14 basic needs of patients that comprise the components of nursing care:
1. Breathing
2. Eating and drinking
3. Elimination
4. Movement
5. Rest and sleep
6. Suitable clothing
7. Body temperature
1. Clean body and protected integument
2. Safe environment
3. Communication
4. Worship
5. Work
6. Play
7. Learning
She identified three levels of nurse-patient relationships in which the nurse is a:
1. Substitute for the patient
2. Helper to the patient
3. Partner with the patient.
She supports empathetic understanding and states that the nurse must “get inside the skin of each of her patients in order to know what he needs.”
Major AssumptionsNursing
The nurse has a unique function to help sick or well individuals
The nurse functions as a member of a medical teamThe nurse functions independently of the physician,
but promotes his or her plan if there is physician in attendance
The nurse is knowledgeable in both biological and social sciences.
The nurse can assess basic human needsThe 14 components of nursing care encompass all
possible functions of nursing
PersonThe person must maintain physiological and
emotional balanceThe mind and body of the person are inseparableThe patient requires help toward independenceThe patient and his and her family are a unit
HealthHealth is a quality of lifeHealth is basic to human functioningHealth requires independence and interdependencePromotion of health is more important than care of
the sickIndividuals will achieve or maintain health if they
have the necessary strength, will, or knowledge.
EnvironmentHealthy individuals may be able to control their
environment, but illness may interfere with that abilityNurses should have safety educationNurses should protect patients from mechanical injuryNurses should minimize the chances of injury through
recommendations regarding construction of buildings, purchase of equipment, and maintenance
Doctor’s use nurses observations and judgments as the base of their prescriptions for protective devices.
Nurses must know about social customs and religious practices to assess dangers.
Theoretical AssertionsThe nurse- patient relationship
1. The nurse as a substitute for the patient2. The nurse as a helper to the patient3. The nurse as a partner to the patient
The nurse-physician relationshipThe nurse have a unique
function that is distinct from the physician’s function.

The nurse as a member of the health care team
The nurse works independence with other healthcare professionals.

Logical FormHenderson appeared to use the
deductive form of logical reasoning to develop her definition of nursing.
Acceptance by the nursing communityPractice
The nurse must make every effort to understand the patient when he or she lacks will, knowledge, or strength.

Education
The nurse’s education demands universal understanding of diverse human beings.
Research
Nurse’s should base their practice on research findings and acquire the habit of looking for research.
Further Development
Henderson’s last revision of her nursing definition was in 1966. She continued to write and reflect on the practice of nursing through out her life.
Critique“My interpretation of the nurse’s function is
the synthesis of many influences, some positive and negative…I should first made clear that I do not expect everyone to agree with me. Rather, I would urge every nurse to develop her own concept.”
Simplicity
Henderson’s concept of nursing is complex rather than simplistic.

GeneralityGenerality is present in Henderson’s definition
because it is broad is scope. It attempts to include the function of all nurses and all patients in their various interrelationships and interdependencies.
Derivable Consequences
His perspective has been useful in promoting new ideas and furthering conceptual development of emerging theorists.
Faye Glenn Abdellah’s work is based on the problem-solving method and had a great impact on nursing curriculum development. Abdellah’ viewed nursing as both an art and a science that molds the attitude, intellectual competencies and technical skills of the individual nurse into the desire and ability to help people cope with their health needs whether they are ill or well. She formulated 21 nursing problems based on a review of nursing research studies. The typology of her 21 nursing problems first appeared in the 1960 edition of Patient Centered approaches to nursing Abdellah’s work is considered a philosophy of nursing
Jean Watson began publishing in the mid 1970s. Her book, Nursing: the Philosophy and Science of Caring was published in 1979. She presented Nursing: Human Science and Human Care. In 1985, with another edition in 1988, and published Post-modern nursing and Beyond in 1999. In an effort to reduce the dichotomy between theory and practice. She identified the following 10 carative factors:
1. The formation of a humanistic altruistic system of values
2. The instillation of faith-hope;
3. The cultivation of sensitivity to self and to others
4. The development of a helping-trust relationship
5. The promotion and acceptance of the expression of positive and negative;
6. The systematic use of the scientific problem-solving method for decision making
7. The promotion of interpersonal teaching-learning;
8. The provision for a supportive, protective, or corrective mental, physical, socio-cultural and spiritual environment;
9.Assistance with the gratification of human needs; and
10. The allowance for existential-phenomenological forces.

Patricia Benner. The Dreyfus Model of Skills Acquisition was developed in reached about pilot’s performance in emergency situation. She validated the Dreyfus Model of Skill Acquisition in nursing practice with her systematic description of the five stages (novice, advanced beginner, competent, proficient, and expert).

Dorothea E Orem has been publishing about nursing practice and education SINCE THE 1950s. Orem explicated self-care as a human need and nursing as human service; she emphasized nursing’s special concern for a person’s need for self-care actions on a continuous basis to sustain life and malized the Self-Care deficit Theory of nursing as a general theory composed of the following three related theories:

1. The theory of self-care
2. The theory of self-care deficit
3. The theory of nursing systems
Her work identifies three types of nursing systems:
1. Wholly compensatory (doing for the patient)
2. Partly compensatory (helping the patient do for himself or herself)
Supportive-educative (helping the patient learn to do for himself or herself and emphasizing the important role of the nurse in designing nursing care).
Myra Estrin Levine started publishing in the mid 1960s. By contributing to the nursing literature, she facilitated the development of theory, she wrote Introduction to Clinical Nursing, a textbook to teach medical-surgical nursing to beginning students. She proposed that nurses use the principles of conservation of:
1. Energy
2. Structural integrity
3. Personal integrity
4. Social integrity to keep the holism of the individual balanced.

Levine specified four levels of organismic response:
Fear
Inflammatory response
Response to stress
Sensory response
Martha E. Rogers has publishes widely since the early 1960s and is considered one of the most creative thinkers in nursing. Her work regarding unitary human beings appears in An Introduction to the Theoretical Basis of Nursing.

Dorothy E. Johnson published from the mid 1940s to the early 1970s. Johnson presented the Behavioral System Model in Riehl and Roy’s books, Conceptual Mode for Nursing Practice. Her behavioral system also includes the subsystems of dependency, achievement, aggressive, ingestive, eliminative and sexual. In Johnson’s words, “Nursing problems arise because there are disturbances in the structure or functions o of the subsystems of the system, or because the level of behavioral functioning is less than desirable.”
Sister Callista Roy proposed that humans are biopsychosocial beings who exist within an environment. Environment and self provide three classes of stimuli:
1. Focal
2. Residual
3. Contextual
Sister Callista RoySister Callista Roy
Betty Neuman developed her first teaching practice model for mental health consultation in the late 1960s. She designed the Systems Model in 1970 to help graduate students evaluate nursing problems. It was first published in Nursing Research in 1972 and further refined in the Neuman Systems Model in 1982, 1989 and 1995. Major concepts include: total persons approach, holism, open system, stressors, energy resources, lines of resistance, lines of defense, intervention, levels of prevention and reconstitution.
Betty NeumanBetty Neuman

has been publishing since the mid1960s. Toward a Theory for Nursing was published in 1971 and a Theory for Nursing was published in 1981. King’s conceptual; framework specifies the following interacting systems: personal system, interpersonal system and social system. The concepts of the personal systems are perception, self, body image, growth and development and time and space. The concepts of interpersonal system are role, interaction, communication and transaction and stress.
Imogene King
Nancy Roper, Winifred W. Logan, and Alison J. Tierney, The Elements of Nursing: A Model for Nursing based of a Model for Living. The 12 activities of living (ALs) include maintaining a safe environment, communicating, breathing, eating and drinking, eliminating, personal cleansing and dressing, controlling body temperature, mobilizing, working and playing, expressing sexuality, sleeping and dying. The five groups of factors influencing the Als are biological, psychological, socio-cultural, and environmental and politico economic.

Hildegard E. Peplau’s contributions to nursing in general and to the specialty of psychiatric nursing in particular have been enormous since1950s. Interpersonal Relations in Nursing. She identified four phases of the nurse-patient relationship:
1. Orientation
2. Identification
3. Exploitation
4. Resolution

Peplau proposed and described six nursing roles:
1. Stranger
2. Resource person
3. Teacher
4. Leader
5. Surrogate
6. Counselor

In 1961, Ida Jean Orlando (Pelltier) first describe her discipline’s Professinal Response Theory in The Dynamic Nurse-patient Relationship which was reissued by the National League for Nursing in 1991. She reported related research in the Discipline and Teaching of Nursing Process. Orlando used the interpersonal nurse-patient relationship in response to the patient’s needs as the basis for her work. Three elements comprise a nursing situation:
1. Patient behaviors
2. Nurse Reactions
3. Nursing actions
Joyce Travelbee published predominantly in the mid1960s. She died in 1973 at a relatively young age. Travelbee proposed her Human-to-Human Relationship Theory in Her book, Interpersonal Aspects of Nursing about illness, suffering, pain, hope, communication, interaction, empathy, sympathy, rapport, and therapeutic use of self. She proposed that nursing was accomplished through human-to-human relationships that begin with:

1. The original encounter and then progressed through stages of
2. emerging identities
3. developing feelings of empathy and later,
4. sympathy, until
5. the nurse and patient attained rapport in the final stage.
Travelbee’s emphasis on caring stressed empathy, sympathy, rapport, and the emotional aspects of nursing. The work is categorized as a nursing theory.

Katharine Kolcaba defies healthcare needs as those needs for comfort including physical, psycho-spiritual, social and environmental needs. Comfort measures include physiological, social, financial, psychological, spiritual, environmental and physical measures.
Types of comfort
•a sense of ease
•calm or contentment and
•transcendence when a person rises above problems of pain.
Ramona T. Mercer has researched and published 1970s. Researched the field of maternal role attainment and developed a complex theory about factors influencing maternal role development over time her 1986 book, First-Time Motherhood: Experiences from Teens to Forties.

Kathryn E. Barnard is an active researcher who has published extensively about infants and children since the mid 1960s. She began by studying the activities of the well child and then expanded her work to include methods of evaluating the growth and development of children and mother-infant relationships.

Madeleine Leininger has published extensively about many nursing topics since 1960. Transcultural Care Theory is found in her 1984 book, Care: The Essence of Nursing and Health. Caring includes assistive, supportive, or facilitative acts toward an individual or group with evident or anticipated need.

Rosemarie Rizzo Parse derives her theory form Roger’s principles and concepts and from Heidegger, first book of her theory, Man-Living-Health: A Theory of Nursing in 1981. Major concepts include imaging, valuing, languaging , revealing-concealing, enabling-limiting, connecting-separating, powering, originating and transforming.
Merle Mishel used qualitative and quantitative findings to conceptualize uncertainty in illness.
Margaret A. Newman began publishing in the mid 1960s. She has drawn from several fields of inquiry. Her model appeared in Theory Development in Nursing. Newman’s theory of health is derived from Roger’s model. According to Newman, the goal of nursing is not to promote wellness or to prevent illness, but to help people use the power within them as they evolve toward a higher level of consciousness.
Evelyn Adam is a Canadian nurse who started publishing in the mid1970s.
Nola J. Pender defines the goal of nursing care as the optimal health of the individual. She began to build the foundation for studying how individuals make decisions about their own healthcare in her article.
Florence Nightingale, the matriarch of modern nursing, was born on May 12, 1820. At the time of her birth, her parents were on extended European tour. Her parents, Edward and Frances Nightingale, named their daughter after her birthplace Florence, Italy. The Nightingales were a well-educated, affluent, aristocratic Victorian family who maintained residences. After she understood that she was called to become a nurse, she was finally able to complete her training in 1851 at Kaiserworth, Germany, a Protestant religious community with a hospital facility.

She was called “The lady of the Lamp”, as immortalized in the poem “Santa Filomena” by Henry Wadsworth Longfellow, because she made ward rounds during the night. Florence Nightingale’s reputation as the founder of modern nursing was establish. Her writings, Notes on matters Affecting the Health, Efficiency and Hospital Administration of the Bristish Army, Notes on Hospitals and Report on Measures Adopted for Sanitary Improvements in India from June 1869 to June 1870.
In her lifetime, Nightingale’s work was recognized through the many awards she received from her own country and many other countries. She was able to work into her eighties and died in her sleep on August 13, 1910 at age 90.
MAJOR ASSUMPTIONSMAJOR ASSUMPTIONS
Nursing
Nightingale believed that every woman, at one time in her life, would be a nurse in the sense that nursing is having the responsibility for someone else’s health. Nightingale wrote Notes on Nursing to provide women with guidelines fro providing nursing care and to give advice on how to “think like a nurse”.
Person
Nightingale referred to the person as a patient. Nurses performed tasks to and for the patient and controlled the patient’s environment to enhance recovery.
Health
Health as being well and using every power that the person has to the fullest extent. Envisioned the maintenance of health through the prevention of disease via environmental control; what she described is modern public health nursing and the more modern concept of health promotion.

Environment
Fitzpatrick and Whall describe Nightingale’s concept of environment as “those elements external person” and included “everything from the patient’s food and flowers to the patient’s verbal and nonverbal interactions with the patient.” She believed that nurses could be instrumental in changing the social status of the poor by improving their living conditions.
THEORETICAL ASSERTIONSTHEORETICAL ASSERTIONS
Nightingale was totally committed to nursing education (training). Although she wrote Notes on Nursing that nurses needed to be excellent at the observation of their patients and the environment. She believed that nurses needed to use common sense in their nursing practice, coupled with their observation, perseverance and ingenuity. She believed that persons desired good health and that they would cooperate with the nurse and nature to allow the reparative process.

ACCEPTANCE BY THE NURSING COMMUNITYACCEPTANCE BY THE NURSING COMMUNITY
Practice
The environmental aspects of her theory (ventilation, warmth, quiet, diet and cleanliness) remain integral components of current nursing care.
Education
Nightingale’s principles of nursing training (instruction in scientific principles and practical experience for the mastery of skills) provided a universal template for early nurse training schools beginning with St. Thomas Hospital and King’s College Hospital in London.

Research
Nightingale’s interest in scientific inquiry and statistics continues to define the scientific inquiry used in nursing research.

THE HELPING ART OF CLINICAL NURSINGTHE HELPING ART OF CLINICAL NURSING
Ernestine Wiedenbach’s affluent family immigrated from Germany. Her interest in nursing began with her childhood experiences with nurses. She greatly admired the private duty nurse who cared for her ailing grandmother. She wrote family-Centered Maternity Nursing a text on clinical nursing that was published in 1958.

MAJOR ASSUMPTIIONSMAJOR ASSUMPTIIONS
Nursing
Nurses ascribe to an explicit philosophy. Basic to this philosophy of nursing are:
1. reverence for the gift of life
2. respect for the dignity, worth, autonomy, and individuality of each human being
3. resolution to act dynamically in relation to one’s beliefs
Weidenbach identifies five essential attributes of a professional person:
1. Clarity of purpose
2. Mastery of skill and knowledge essential for fulfilling the purpose
3. Ability to establish and sustain purposeful working relationships with other (both professional and nonprofessional individuals)
4. Interest in advancing knowledge in the area of interest and in creating new knowledge
5. Dedication to furthering the goal of humankind rather than supporting self-aggrandizement.

Person
Four explicit assumptions are stated in relation to human nature:
1. Each human being is endowed with the unique potential to develop-within self-resources that enable them to maintain and sustain himself
3. The human being basically strives toward self-direction and relative independence and desires not only to make best use of his capabilities and potentialities, but also to fulfill his responsibilities.
4. Self-awareness and self-acceptance are essential to the individual’s sense of integrity and self-worth.
5. Whatever the individual does represents his or her best judgment at the moment of his doing.
Health
The definitions of nursing, patient, and need-for-help, and the relationships among these concepts, imply health related concerns in the nurse-patient situation.
Environment
She recognized the potential effects of the environment. It is implied the environment may produce obstacles resulting in the person experiencing a need-for-help.

Faye Glenn Abdellah was born in New York City in 1919. She graduated magna cum laude from Fitkin Memorial Hospital School of Nursing (now Ann May School of Nursing) in 1942. Abdellah received her B.S. in 1945, her M.A. in 1947 and her Ed.D in 1955 from Teachers College at Columbia University.
Abdellah’s Typology of 21 Nursing Problems
1. To maintain good hygiene and physical comfort
2. To promote optimal activity: exercise, rest and sleep
3. To promote safety through prevention of accident, injury or other trauma and through the prevention of the spread of infection
4. To maintain good body mechanics and prevent and correct deformity

5. To facilitate the maintenance of the supply of oxygen to all body cells
6. To facilitate the maintenance of nutrition of all body cells
7. To facilitate the maintenance of elimination8. To facilitate the maintenance of fluid and
electrolyte balance.9. To recognize the physiological responses of the
body to disease conditions-pathological, physiological and compensatory
10. To facilitate the maintenance of regulatory mechanisms and functions
11. To facilitate the maintenance of sensory function12. To identify and accept positive and negative
expressions, feelings and reactions13. To identify and accept interrelatedness of
emotions and organic illness14. To facilitate the maintenance of effective verbal
and nonverbal communication15. To promote the development of productive
interpersonal relationships

16.To facilitate progress toward achievement and personal spiritual goals.
17. To create or maintain a therapeutic environment18. To facilitate awareness of self as an individual
with varying physical, emotional and developmental needs.
19. To accept the optimum possible goals in the light of limitations, physical and emotional
20. To use community resources as an ald in resolving problems arising from illness
21. To understand the role of social problems as influencing factors in the cause of illness.

Lydia Hall began her prestigious career in nursing as a graduate of the York Hospital School of Nursing in York, Pennsylvania. She then earned her B.S. and M.A. degrees from Teachers College, Columbia University, in New York. Hall’s career interests revolved around public health nursing, cardiovascular nursing, pediatric cardiology and nursing of long-term illnesses.

The PersonSocial sciences Therapeutic
use of self-aspects of nursing
“The Core”
The BodyNatural and biological
sciencesIntimate bodily
care-aspects of nursing“The Care”
The DiseasePathological and
therapeutic sciencesSeeing the patient and
family through the medical care-aspects
of nursing“The Cure”

Philosophy and Science of CaringPhilosophy and Science of Caring
Margaret jean Harman Watson was born in southern West Virginia and grew up during the 1940s and 1950s in the small town of Welch, West Virginia in the Appalachian Mountains.
10 Carative Factors
1. Formation of a Humanistic-Altruistic System of Values
2. Instillation of faith-Hope
3. Cultivation of Sensitivity to Self and to Others
4. Development of a Helping-Trust Relationship

5. Promotion and Acceptance of the Expression of Positive and negative Feelings
6. Systematic Use of the Scientific Problem-Solving Method for Decision-Making
7. Promotion of Interpersonal Teaching-Learning
8. Provision for Supportive, Protective and Corrective Mental, Physical, Socio-cultural, and Environmental
9. Assistant with gratification of Human Needs
10. Allowance for Existential-Phenomenological Forces

Patricia Benner was born in Hampton, Virginia and spent her childhood in California, where she received her early and professional education. Majoring in nursing, she obtained a Bachelor of Arts degree from Pasadena College in 1964. In 1970, she earned a master’s degree in nursing, with her major emphasis in medical-surgical nursing from the University of California, San Francisco School of nursing.
Novice
In the novice stage of skill acquisition in the Dreyfus model, the person has no background experience of the situation in which he or she is involved.
Advanced Beginner
Advanced beginner stage in the Dreyfus model develops when the person can demonstrate marginally acceptable performance having coped with enough real situations to note, or to have pointed out by a mentor, the recurring meaningful components of the situation.

Competent
Through learning from actual practice situations and by following the actions of others, the advanced beginner moves to the competent level.
Proficient
Performer perceives the situation as a whole (the total picture) rather than in terms of aspects and the performance is guided by maxims. The proficient level is qualitative leap beyond the competent. Nurses at this level demonstrate a new ability to see changing relevance in a situation including the recognition and the implementation of skilled responses to the situations as it evolves.

Expert
The fifth stage of the Dreyfus model is achieved when “the expert performer no longer relies on analytical principle (rule, guideline, maxim) to connect her or his understanding of the situation to an appropriate action.”

Dorothea Elizabeth Orem, one of America’s foremost nursing theorists, was born in Baltimore, Maryland. Her early nursing experiences included operating room nursing, private duty nursing (home and hospital), hospital staff nursing on pediatric and adult medical and surgical units, evening supervisor in the emergency room, and biological science teaching. Labels her self-care deficit theory of nursing as a general theory composed of three related theories:
1. the theory f self-care, which describes why and how people care for themselves
2. the theory of self-care deficit, which describes and explains why people can be helped through nursing
3. the theory of nursing systems, which describes and explains relationships that must be brought about and maintained for nursing to be produced.

Myra Estrin Levine obtained a diploma from Cook Country School of Nursing in 1944, an S.B. from the University of Chicago in1949, an M.S.N. from Wayne State University in 1962, and she has taken postgraduate course at the University of Chicago. Hutchins’ curriculum was being taught to undergraduate students at the University of Chicago.

Three major concepts of the Conservation Model are wholeness, adaptation and conservation.
1. Wholeness (HOLISM)
- “Whole, health, hale is all derivations of Anglo-Saxon word hal.” “Wholeness emphasizes a sound, organic, progressive, mutuality between diversified functions and parts within an entirety, the boundaries of which are open and fluent.”
2. Adaptation
- “Adaptation is a process of change whereby the individual retains his integrity within the realities of his internal and external environment.”
3. Environment
- Environment is “where we are constantly and actively involved.” The person and his or her relationship to the environment is what count.

Conservation PrinciplesConservation Principles
Conservation of Energy The individual requires a balance of energy and a constant renewal of energy to maintain life activities. Processes such as healing and aging challenge that energy.
Conservation of Structural Integrity Healing is a process of restoring structural and functional integrity in defense of wholeness.
Conservation of Personal Integrity Self-worth and a sense of identity are important. The most vulnerable become patients. This begins with the erosion of privacy and the creation of anxiety. Nurses can show patients respect by calling them by name, respecting their wishes, valuing personal possessions, providing privacy during procedures, supporting their defenses and teaching them.

Conservation of Social Integrity Life gains meaning through social communities and health is socially determined. Nurses fulfill professional roles, provide for family members, assist with religious needs, and use interpersonal relationships to conserve social integrity.
Moral TheoriesMoral Theories
Freud (1961)Freud (1961)
Believed that the mechanism for right and wrong within the individual is the superego, or conscience. He hypothesized that a child internalizes and adopts the moral standards and character traits of the model parent through the process of identification.

The strength of the superego depends on the intensity of the child’s feelings of aggression or attachment toward the model parent rather than on the actual standards of his parent.
Erikson (1964)Erikson (1964)
Erikson’s theory on the development of virtues or unifying strengths of the “good man” suggests that moral continues throughout life. He believed that if the conflicts of each psychosocial development stages are favorably resolved then an “ego-strength” or virtues emerges.

KohlbergKohlberg
Suggested three levels of moral development. He focused on the reasons for the making of a decision, not on the morality of the decision itself. At first level called the premoral or the preconventional level, children are responsive to cultural rules and labels of good and bad, right and wrong.

However, children interpret these in terms of the physical consequences of their actions, i.e., punishment or reward. At the second level, the conventional level, the individual is concerned about maintaining the expectations of the family, groups or nation and sees these as right.
At the third level called the postconventional, autonomous, or principled level. At this level, people make an effort to define valid values and principles without regard to outside authority or to the expectations of others. These involve respect for other humans and belief that relationships are based on mutual trust.

PetersPeters Proposed a concept of rational morality
based on principles. Moral development is usually considered to involve three separate components: moral emotion (what one feels), moral judgment (how one reasons), and moral behavior (how one acts). In addition, Peters believed that the development of character traits or virtues is an essential aspect of moral development.
And that virtues or character traits can be learned from others and encouraged by the example of others. Also, Peters believed that some virtues can be described as habits because they are in some sense automatic and therefore are performed habitually, such as politeness, chastity, tidiness, thrift and honesty.
Schulman and Mekler Schulman and Mekler (1985)(1985)
Believed that morality is a measure of how people treat fellow humans and that a moral child is one who strives to be kind and just. They believed that morality has two components, namely:
1. The intention of the person acting must be good in the sense that the goal of the act is the well being of one or more people;
2. The person acting must be fair or just in the sense that the person considers the rights of others without prejudice or favoritism.

Furthermore, the aforementioned authors asserted that the theory of moral development is based on three foundations, which they believed can be taught, as follows:
a. Internalizing parental standards of right and wrong
b. Developing emphatic reactionsc. Acquiring personal standards
Gilligan (1982)Gilligan (1982)Included the concepts of caring and
responsibility. She describe three stages in the process of developing an “Ethic of Care” which are as follow:
a. Caring for oneselfb. Caring for othersc. Caring for self and others.

She believed that women see morality in the integrity of relationship and caring. For women, what is right is taking responsibility for others as self-chosen decision. On the other hand, men consider what is right to be what is just.
Spiritual TheoriesSpiritual Theories

Fowler (1979)Fowler (1979)
Described the development of faith. He believed that faith, or the spiritual dimenston is a force that gives meaning to person’s life. He used the term “faith” as a form of knowing, a way of being in relation “to an ultimate environment.”
To Fowler, faith is a relation phenomenon: it is “ an active made-of-being-in-relation to another or others in which invest commitment belief, love, risk and hope.”

WesterhoffWesterhoff
Proposed that faith is a way of behaving. He developed a four-stage theory of faith development based largely on his life experiences and the interpretation of those experiences. These stages as follows:

a. Experienced faith (infancy to early adolescence): experiences faith through interactions with others who are living a particular faith
b. Affiliative faith (late adolescence): actively participates in activities that characterize a particular faith tradition
c. Searching faith (young Adulthood): through a process of questioning ad doubting own faith, acquires a cognitive as well as effective faith.
d. Owned faith (middle adulthood): puts faith into personal and social action and is willing to stand up for what he/she believes even against the nurturing community.

The EndThe End