therapeutic drug monitoring (tdm): practical questions ...nid... · therapeutic drug monitoring...
TRANSCRIPT

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 1
Therapeutic Drug Monitoring ( TDM ):Practical Questions and Answers
Charles A. Peloquin, Pharm. D.Professor, and Director Infectious Disease Pharmacokinetics LaboratoryCollege of Pharmacy and The Emerging Pathogens InstituteUniversity of Florida
Drugs FDA Approved for TB
Aminosalicylate sodium (PAS)
Bedaquiline
Capreomycin, Streptomycin
Cycloserine
Ethionamide
Ethambutol
Isoniazid
Pyrazinamide
Rifampin, Rifapentine
Drugs not FDA approved for TB
Other Aminoglycosides:
Amikacin
Kanamycin
Fluoroquinolones:
Moxifloxacin
Levofloxacin

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 2
Drugs not FDA approved for TB
Macrolides - generally poor TB drugs:
Azithromycin
Clarithromycin
( indicated for, and primarily useful for, MAC )
Amoxicillin - clavulanate ( role not established )
Clofazimine ( role being re - evaluated )
Rifabutin ( used for TB and MAC )
Linezolid , newer agents Sutezolid and AZD-5847
Outside US: prothionamide, thiacetazone, viomycin
A drug must enter the organism,
bind to a specific target,
and produce an inhibitory or lethal effect.
Unless the drug is delivered to the site of
infection ( PK ), nothing happens ( PD ).
How Do Antibiotics Work ?
PK and PD

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 3
Pharmacodynamics ( PD )
role: primary drug, along with INH
action: DNA - dependent RNA polymerase
dosage: oral, I.V.
dose: 600 mg QD // 10-20 mg / Kg for kidsmuch higher doses being studied
cleared: liver >> kidneys
toxicity: hepatotoxicity, flu - like syndrome
Rifampin ( RIF )
Rifamycin Comparison
CYP 3A4 * Uniqueinduction features
Rifampin 1.00 flu - like syndrome
Rifapentine 0.85 to 1.00+ 99% protein bound
Rifabutin 0.40 uveitis, neutropenia
• Liver enzyme induction speeds up clearance of other drugs

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 4
Rifamycin Comparison
MIC * Cmax ^ Ratio t ½( µg / ml ) ( µg / ml ) ( hr )
Rifampin 0.25 12 48 3
Rifapentine 0.06 12 200 15
Rifabutin 0.06 0.6 10 36
• 7H12 broth minimal inhibitory concentration
• ^ total Rx ( free and bound )
Rifamycin Comparison
MIC * Cmax # Ratio t ½( µg / ml ) ( µg / ml ) ( hr )
Rifampin 0.25 1.8 7.2 3
Rifapentine 0.06 0.12 2.0 15
Rifabutin 0.06 0.09 1.5 36
* 7H12 broth # free Rx ( only free is active )
The study of the movement of drugs
through the body.
Most commonly based on the study of
serum concentrations in relation to dose,
with interpretation and dose adjustment.
Pharmacokinetics ( PK )

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 5
PK: Plasma Elimination Half - Life
t 1/2 is defined as the time for concentrations
( in plasma ) to decline by 50 %.
After 7 t 1/2’s, nearly all of the drug is gone,
regardless of the starting concentration.
t 1/2 is independent of dose and concentration.
PK: Clearance
t 1/2 is inversely proportional to
the clearance of a drug ( Cl ).
Clearance can be thought of as the size
of the drain in the bathtub.
A big drain will empty the tub faster.

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 6
PK: Clearance
Clearance organs:
Kidneys : especially water soluble drugs
– creatinine clearance might predict
Liver : metabolize drugs to make water sol.
– AST, ALT usually do not predict
[ minor: lungs, skin, saliva… ]
PK: Volume of Distribution
t 1/2 is directly proportional to
the volume of distribution ( V ).
V can be viewed as the size of the bathtub.
Big tubs take a longer time to drain.
t 1/2 is viewed as a proportionality constant,
dependent upon Cl and V.
PK: Volume of Distribution
Large volumes of distribution typically
reflect drug penetration into tissues which
return the drug to the plasma space
only slowly.
Drug molecules inside of tissues are
unavailable to the organs of clearance.

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 7
PK: Data Handling
The most common parameters clinically are
are Cmax ( peak ), Cmin ( trough ), Tmax, & t1/2
Simple kinetics can be done with a calculator,
or with a spreadsheet.
The most common calculations involve
linear regression ( fitting a straight line to data ).
Example: Amikacin Kinetics
the study of the relationships betweendrug concentrations and responses
Methods
• in vitro models• animal models• human clinical trials with dose escalation
Pharmacodynamics ( PD )

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 8
Evans, 1986
Minimal inhibitory concentration ( MIC )
The concentration of the drug required
to inhibit the growth of an organism
in the laboratory.
From this: “ susceptible ” or “ resistant ”
[ This test cannot be done within the patient. ]
Antibiotic Terms
ID: Usual PK - PD Response Parameters
• Cmax / MIC
• Time > MIC
• AUC > MIC

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 9
MIC
Cmax
AUC > MIC
10
8
6
4
2
0
Cmax = 9 mcg / ml
MIC = 3 mcg / ml
Cmax / MIC = 3
T > MIC = 8 h
AUC ( mcg * h / ml )
PD: Response Parameters
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
0 4 8 12 16 20 24
CO
NC
TIME
ISONIAZID
slow
fast
MIC
0.0
0.5
1.0
1.5
2.0
2.5
0 4 8 12 16 20 24
CO
NC
TIME
ETHIONAMIDE
eta
MIC

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 10
Pharmacodynamics ( PD )
Killing of TB by most TB drugs can be
described very well using AUC / MIC,
and more AUC is better.
This has been known for many years,
and has been widely published.
PD: Response Parameters
“Concentration - dependent” antimicrobials
best given as large ( daily ) doses
• aminoglycosides, quinolones, RIFAMYCINS
( based on in vitro, animal and human data )
• target a Cmax / M I C of at least 10 - 12
Rifampin has profoundconcentration – dependent killing
Week 5 mg/kg 10 mg/kg 20 mg/kg 40 mg/kg
Lung CFUweek 1
100,000,000 100,000,000 100,000,000 100,000,000
Lung CFUweek 10
10,000 100 10 0
% reduction 99.99000% 99.99990% 99.99999% 100.00000%
Verbist L. Acta Tuberculosa et Phneumolgia Belgica1969 ; number 3 - 4: 397 - 412.;
Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 11
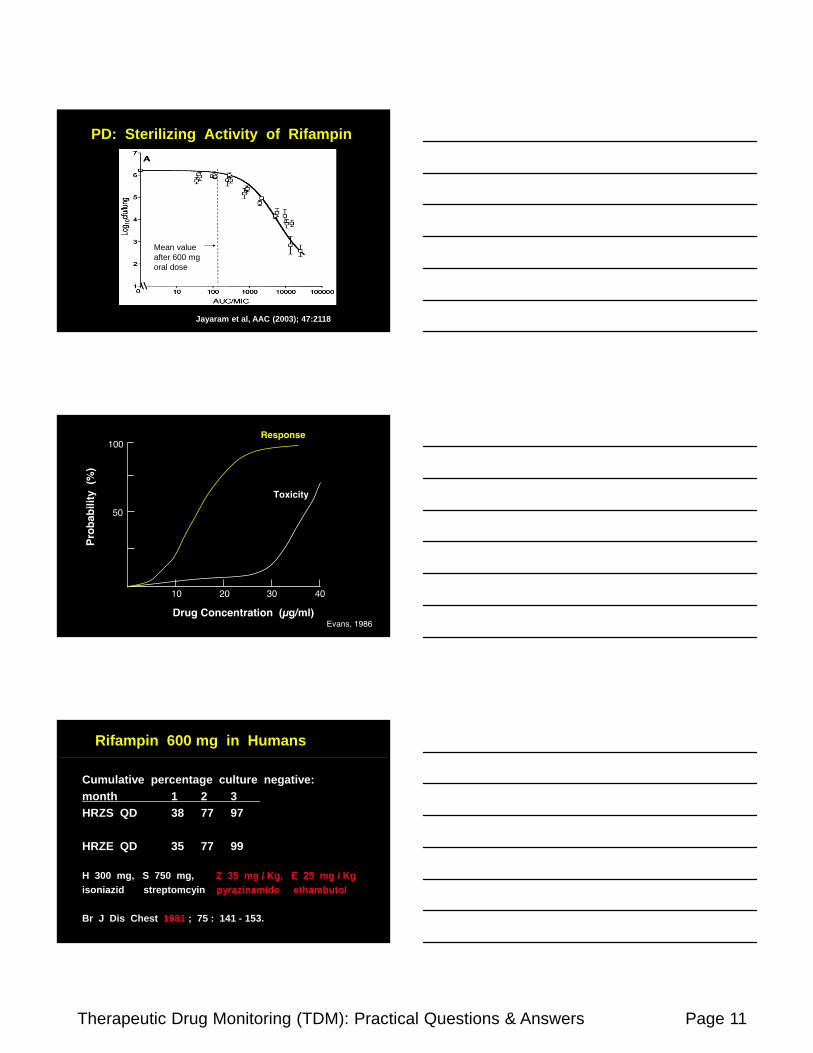
PD: Sterilizing Activity of Rifampin
Jayaram et al, AAC (2003); 47:2118
Mean value after 600 mg oral dose
Evans, 1986
Rifampin 600 mg in Humans
Cumulative percentage culture negative:
month 1 2 3
HRZS QD 38 77 97
HRZE QD 35 77 99
H 300 mg, S 750 mg, Z 35 mg / Kg, E 25 mg / Kg
isoniazid streptomcyin pyrazinamide ethambutol
Br J Dis Chest 1981 ; 75 : 141 - 153.

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 12
Rifampin 1200 mg in Humans
Cumulative percentage culture negative
month 1 2 3
HRS QD 72 94 98
HRS QOD 70 93 100
H 900 mg, S 1000 mg QD both regimens
isoniazid streptomycin
Kreis B et al. Bull Int Union Tuber 1976 ; 51 : 71 - 75.
Rifampin 600 mg vs. 1200 mg
Cumulative percentage culture negative
month 1 2 3
HRZS QD 38 77 97
R 600 mg, with Z
HRS QD 72 94 98
R 1200 mg, NO Z
INH 900 mg
Rifampin 1200 mg
Flu - like syndrome was NOT reported
by Kreis et al ( 3 months of treatment )
Even with highly - intermittent RIF,
syndrome usually appears after 3 to 6 months.
Kreis B et al. Bull Int Union Tuber 1976 ; 51 : 71 - 75.
Peloquin C. Int J Tuberc Lung Dis 2003; 7: 3 - 5.

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 13
Evans, 1986
PD: Response Data
Association between Acquired Rifamycin Resistance and the Pharmacokinetics of Rifabutin and Isoniazid among Patients with HIV and TB [ Study 23A ].
Weiner M, Benator D, Burman W, Peloquin CA, Khan A, Vernon A, Jones B S, Silva-Trigo C, Zhao Z, Hodge T and the Tuberculosis Trials Consortium
Clinical Infectious Diseases 2005; 40: 1481 - 1491.
Lower rifabutin AUC associated with failure, relapse, and ARR
• P for RBT AUC ARR vs. cure, Mann-Whitney• Odds ratio for CD4 count 1.01• Odds ratio for RBN AUC 23
0.045.1
(4.0 - 7.4)
4.8
(4.2 – 6.2)
82CURE
3.1
(2.0 - 3.8)
4.6
(3.5 - 5.7)
6ARR
P-Value*
AUC0-24
Med (IQC)
Dose mg/kg
Med (IQC)
No.Group

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 14
Rifampin has profoundconcentration – dependent killing
Week 5 mg/kg 10 mg/kg 20 mg/kg 40 mg/kg
Lung CFUweek 1
100,000,000 100,000,000 100,000,000 100,000,000
Lung CFUweek 10
10,000 100 10 0
% reduction 99.99000% 99.99990% 99.99999% 100.00000%
Verbist L. Acta Tuberculosa et Phneumolgia Belgica1969 ; number 3 - 4: 397 - 412.;
Rifampin PD
Rifampin PD clearly is linked to AUC / MIC
and somewhat less to Cmax / MIC.
It is not linked to % Time > MIC.
Therefore, what is the rationale for
a long half – life version of rifampin ?
Rifampin 600, 1200, 1500, 1800, 2100 mg
RIF log cfu TTP Cmax AUC ( mg / kg ) ( / ml / d )
10 0.18 0.02 7 2620 0.15 0.03 26 11325 0.16 0.03 25 13530 0.25 0.04 33 18935 0.25 0.04
Boeree M. et al, CROI 2013; Paper #148LB

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 15
Dose Ranging Trial to Optimize the Dose of Rifampin
Maximum tolerated dose study :RIF 10, 15, 20, 25, 30, 35 mg / kg for 14 daysin patients with drug – susceptible TB[ 70 kg * 35 mg / kg = 2,450 mg, round to 2,400 mg ]
More – than proportional increases in Cmaxand AUC occurred as doses increased.
Am J Respir Crit Care Med 2015; 191: 1058 - 1065.
Dose Ranging Trial to Optimize the Dose of Rifampin
Maximum tolerated dose study :High inter –individual variability in Cmax and AUC within any given dose ( an argument for TDM ).
Greatest reduction in sputum colony countsof Mtb were seen with the highest AUC.
Am J Respir Crit Care Med 2015; 191: 1058 - 1065.
High RPNT exposures (AUC) were associated
with high levels of sputum sterilization at
the completion of 8 weeks of treatment
( end of intensive phase )
Less – than proportional increases in Cmaxand AUC occurred as doses increased.
Am J Respir Crit Care Med 2015; 191: 333 - 343.
Daily Rifapentine for Treatmentof Pulmonary Tuberculosis

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 16
Where Does TB Drug PK Data Come From ?
Data were compiled from all available sources
( both healthy volunteers and TB patients ) by :
Mack Holdiness Clin Pharmacokinet. 1984; 9 (6) : 511 - 44
Charles Peloquin ( 1991 and later )
Global Alliance for TB Drug DevelopmentHandbook of Anti - Tuberculosis Agents 2008
among others …
Where Does TB Drug PK Data Come From ?
CHAPTER 2ANTITUBERCULOSIS DRUGS: PHARMACOKINETICSCharles A. Peloquin, Pharm.D.
In Heifets L , ed. Drug Susceptibility in theChemotherapy of Mycobacterial Infections. CRC Press, Boca Raton, 1991, p 59 - 88.
191 references
The drug must access the organism and bind to a target to produce an inhibitory or lethal effect.
Access requires absorption and delivery by the blood to the site of infection.
By Analogy: Gravity – not just a good idea - it’s the law
Antibiotic Essentials

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 17
Malabsorption, or lack of blood flow to the site of infection, lead to treatment failures and to the selection of resistance.
The question : Standardized treatment for everyone,and if they don’t respond, continue the same tx,
Or
See why this is happening, adapt, and overcome.
Antibiotic Essentials
Slow responses to TB treatment are common, as shown on the next slide.
While many of these slow responses are dueto treatment interruptions ( adverse drug reactions, patients leaving treatment programs, etc. ), in our experience, a substantial portionof these are due to poor drug absorption.
Role for Therapeutic drug monitoring
aims to promote optimum drug treatment
by maintaining serum drug concentrations
within a "normal range," or preferably
a "therapeutic range”
How can we apply this ?
Therapeutic Drug Monitoring ( TDM )

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 18
Completion of TB Therapy,United States, 1993 – 2010*
* Updated as of June 10, 2013. Data available through 2010 only.
Note: Includes persons alive at diagnosis, with initial drug regimen of one or more drugs prescribed, who did not die during therapy. Excludes persons with initial isolate rifampin resistant, or patient with meningeal disease, or pediatric patient (aged <15) with miliary disease or positive blood culture.
Pe
rce
nta
ge
0
20
40
60
80
100
Completed in 1 year or less Completed
Completion of TB Therapy,United States, 1993 – 2010*
• Updated as of June 10, 2013.
• Data available through 2010 only.
Note: Includes persons alive at diagnosis, with initial drug regimen of one or more drugs prescribed, who did not die during therapy.
Excludes: rifampin resistant TB, meningeal disease, or pediatric patients (aged <15) with miliary disease or positive blood culture.
TB Treatment Is Guideline - Driven
The standard claim is that TB can be treated
with a 6 – month regimen that has roughly
98 % success, followed by about 3 % relapses,
for about a 95 % overall cure.

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 19
Completion of TB Therapy,United States, 1993 – 2010*
• So, what percentage of US TB patients
complete the 6-month regimen in 6 months?
Length of Treatment in the US
Remember, this is supposed to be a 6 – month
“short – course” therapy.
If it takes 12 to 18 months,
it is no longer “short – course” therapy…
and you pay for every month.
So what ?
12 / 6 = 2

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 20
“ In theory, there is no difference between theory
and practice. In practice, there is.”
Yogi Berra
So what ?
The average weight of the patients, predominantly male, in the BMRC Hong Kong and East Africa trials was 48 kg.
600 mg / 48 kg = 12.5 mg / kg
600 mg / 90 kg = 6.7 mg / kg
For many patients, we give a lot less drug thanwas studied originally …
And another thing …
And this is what it looks like …
48 kg 96 kg
600 mg in 600 mg inOriginal patients
Current patients
Full Not Full

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 21
Kind of like putting 10 gallons of gas in each of these vehicles …
Full Not Full
PD: Sterilizing Activity of Rifampin
Jayaram et al, AAC (2003); 47:2118
Mean value after 600 mg oral dose
PD: Sterilizing Activity of Rifampin
Jayaram et al, AAC (2003); 47:2118
most useful when there is a direct
relationship between serum concentrations
and therapeutic response,
and when serum concentrations serve as a
surrogate for drug concentrations
at the site of action
TDM

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 22
most important when there is a narrow range
of concentrations that are effective and safe,
and when toxicity or lack of effectiveness
puts the patient at great risk
TDM
in conjunction with other clinical data,
allows for an assessment of
the patient's status,
and for timely therapeutic interventions
TDM
Spruill WJ, Wade WE, DiPiro JT, Blouin RA, Pruemer JM,
Concepts in Clinical Pharmacokinetics, 6th Ed.
American Society of Health - System Pharmacists 2014.
TDM

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 23
Jelliffe R.
Goal - oriented, model - based drug
regimens: setting individualized goals for
each patient.
Ther Drug Monit 2000; 22: 325 – 329.
TDM
Roger Jelliffe’s Key Points:
“ Therapeutic ” concentrations vary by patient
Once a drug is chosen, a goal should be set for the desired serum concentrations.
This goal should be achieved with thegreatest precision possible.
TDM
Roger Jelliffe’s Key Points:
In other words, if you are relying on drugs
to cure the patient, you may as well
give the right amount to EACH patient.
TDM

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 24
Evans, 1986
TDM with Oral TB Drugs
Two hour post dose blood draws generally
capture the “peak” concentration.
Six hour post dose blood draws generally
separate delayed absorption from malabsorption.
Peloquin CA. Therapeutic Drug Monitoring in the Treatment of Tuberculosis. Drugs 2002; 62: 2169 - 2183.
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0
Conc
entra
tion
( m
cg /
ml )
Time ( hour )
NIH A
NIH B
AACTG
Vols
Rifampin Plasma Concentrations

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 25
The decision to use TDM is the same as
the decision to check a CBC with diff. ,
or the decision to get a CT or MRI.
None of these guarantees the outcome of Tx.
However, all of these inform the clinician
prior to making clinical decisions.
TDM
Role for TDM
TDM allows you to individualize therapy.
TDM allows you to optimize the
pharmacodynamically - linked variable
[ typically Cmax or AUC ].
Role for TDM
TDM may allow you to shorten treatment,
or to avoid concentration - related toxicities.
TDM allows you to unravel complicatedmulti - drug interactions

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 26
In the end, knowing is better than guessing.
So what is the big idea, anyway ?
Any patient in whom you wish to control
drug exposure.
In what populations should TDM be used?
In our lab, a single test is $80.
A pair of tests ( i.e., 2 and 6 hour samples ) per drug are $70 each ( $20 discount ).
Shipping costs vary.
How much does TDM cost ?

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 27
Same as a chemistry panel : plain red top tube.
Time the observed dose.
Time the blood draw (s).
Record the information on the form.
Process the sample promptly.
What are specimen collection Requirements ?
Several labs offer some testing.
Two labs offer most testing.
One lab includes PK consultations with each sample for each patient at noextra charge.
Where is testing done ?
Process the sample within 1 hour if possible.
If not, collect in a green top tube, invert x 3,and place on ice chips until processed.
Given INH stability is questionable…

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 28
No.
Each drug is absorbed independently.
You can have good absorption of one,but not of the other.
Can rifampin be used as a surrogate for INH absorption ?
No.
Each drug is absorbed independently.
Ex. Posaconazole is poorly absorbed and requires high fat food for absorption –just the opposite of RIPE.
Should we use another surrogate marker of absorption ?
As a general population, they appear to have
lower serum concentrations of TB drugs.
See next slide…
What about DM patients…

Therapeutic Drug Monitoring (TDM): Practical Questions & Answers Page 29
BMC Infect Dis. 2017; 17: 125
Early interventions for diabetes related tuberculosis associate with hastened sputum microbiological clearance in Virginia, USA.
Alkabab Y, Keller S, Dodge D, Houpt E, Staley D, Heysell S.
Thanks
• Thanks to Eric Nuermberger, MD and William Burman, MD for providing several slides
• The IDP Lab Team: TJ Zagurski, Kyung Mee Kim, Roger Sedlacek,Emily Graham, Yasuhiro Horita
http://idpl.pharmacy.ufl.edu
http://idpl.cop.ufl.edu/