therapeutics treatment of irritable bowel syndrome (ibs) and constipation
TRANSCRIPT

Therapeutics
Treatment of irritable bowel syndrome (IBS) and constipation

Definition
IBS is an idiopathic chronic relapsing disorder characterized by:
1) Abdominal discomfort (pain), bloating or distension
2) Alteration in bowel habits (diarrhea, constipation or both)
• Abdominal pain / discomfort
• Bloating / distension
• Change in bowel habit
Alarm features = investigations
1. Predominant constipation2. age older than 50 years3. symptom duration less than 6 months4. weight loss5. nocturnal symptoms6. family history of colon cancer7. rectal bleeding8. Anemia9. recent antibiotic usage.

Treatment of IBSAims of treatment: 1) Relieve abdominal pain and discomfort:
1. Anticholinergic drugs (commonly used are; dicyclomine and hyoscyamine) MOA: block M receptors
2. Low doses of TCA (e.g. amitriptyline or desipramine). Low doses have no effect on mood.
2) Relieve distension / bloating3) Improve bowel function
1. For patients with predominant diarrhea: anti-diarrheal agents (especially loperamide) and serotonin 5-HT₃-receptor antagonists
2. For patients with predominant constipation: laxatives (bulk-forming or osmotic laxatives especially Mg oxide) and serotonin 5-HT₄-receptor agonist
K
Antispasmodic drugs in IBSAction: relieve smooth muscle spasm →relieve pain and bloating in IBS)
1. Anticholinergic drugs:Mechanism of action:Block muscarinic receptors (M₃ on smooth muscles in case of hyoscine
or presynaptic M₁ in case of dicyclomine)Adverse effects:2. Blurred vision (may lead to glaucoma)3. Dry mouth4. Tachycardia5. Urinary retention6. Constipation7. Heat intolerance8. Confusion
Antispasmodic drugs in IBS
Contraindications of anticholinergic drugs1. Patients with glaucoma2. Prostatic hyperplasia (elderly)Drug interactions of anticholinergic drugs:3. With other drugs having anticholinergic
effects
Antispasmodic drugs in IBS
2. Mebeverine: (less effective than anticholinergic drugs)
Mechanism of action:Not known (? calcium channel blocker or ?
Direct acting)Adverse effects:3. Hypersensitivity reactions4. In high doses: anticholinergic side effects

Antispasmodic drugs in IBS(for bloating/pain)
Anticholinergic drugs Mebeverine
Hyoscine or dicyclomine -
Indications:1. Female or young male patients (no
prostatic enlargement)2. IBS with predominant diarrhea3. Symptoms of pain or bloating
Indications:1. Symptoms of pain or bloating2. IBS with predominant diarrhea or
predominant constipation
Contraindications:1. Glaucoma2. Prostatic enlargement
Contraindications:1. Hypersensitivity to the drug
Which antispasmodic is preferred in patients with IBS with predominant constipation? Which antispasmodic is indicated in patients with IBS with glaucoma or prostatic enlargement?
Tricyclic antidepressantsAction: relieve pain and bloating in IBS
Mechanism of action:Block synaptic amine uptake (both
norepinephrine and serotonin) →↑ presence of serotonin and norepinephrine at their post-synaptic receptors (→ anxiety) followed by down regulation of the receptors →(delayed anxiolytic and antidepressant effect)
Tricyclic antidepressants
Drugs:Amitriptyline or Desipramine (10 – 50 mg/d) . (N.B. the usual
antidepressant dose = 75 – 200 mg)Adverse effects:1. Blurred vision2. Dry mouth3. Constipation4. Retention of urine5. Orthostatic hypotension6. Arrhythmia7. Cardiac conduction disturbances

Tricyclic antidepressants
Contraindications:GlaucomaElderly patientsPatients with cardiac diseases
Selective Serotonin Reuptake Inhibitors (SSRI)
Mechanism of action:Selective block of synaptic uptake of serotonin.Drugs:Cetalopram (less P450 inhibition → less drug interactions)Adverse effects:Mainly GIT including:1. Nausea and vomiting2. Diarrhea or constipation3. Anorexia and weight loss4. Sexual dysfunction

Laxatives
Classification:1. Bulk-forming2. Osmotic laxatives3. Stimulant laxatives4. Fecal softeners / emollients (little role in
chronic constipation)

Laxatives
1. Bulk-forming laxatives:Containing more soluble fibers (more flatulence)
Containing more insoluble fibers (less flatulence)
1. Methylcellulose2. Psyllium
1. Bran
Precautions:Adequate fluid intake to avoid intestinal obstructionAdverse effects:
1. Abdominal distension (due to fermentation).2. Intestinal obstruction when not consumed with
sufficient fluid
Laxatives
2. Osmotic laxatives:a.Saline laxatives (e.g. Mg oxide)b.Non-digestible sugars or alcohols (e.g. lactulose)c.Polyethylene glycold.Glycerin
Mg oxide is preferred because it is less expensive and it causes less distensionAdverse effects of Mg oxide:
1. Flatulence, abdominal cramps, diarrhea2. Intravascular volume depletion3. Electrolyte disturbances

Laxatives
Contraindications of Mg oxide1.Renal insufficiency2.Severe cardiac disease3.Preexisting electrolyte abnormalities4.Patients on diuretic therapy

Treatment of diarrhea:Antimotility agents (opioids)
Opioids agonists:Action in the GIT (mediated by binding to opioid receptors)1. Increase segmentation and a decrease propulsive
movement → ↑ intestinal transit time → ↑ absorption of water and electrolyte → feces become more solid
2. Antisecretory3. ↑ tone of the internal anal sphincter 4. ↓ response to the stimulus of a full rectum (by their
central action)
Antimotility agents (cont)
Mechanism of opioid action:Inhibition of presynaptic cholinergic nerves in
the submucosal and myenteric plexuses

Opioiods - Diphenoxylate Opioid agonist that has no analgesic properties in standard doses. Higher doses have central opioid actions. Used in combination with a sub-therapeutic dose of atropine (to prevent abuse)Contraindications:1. Children below 2 y (toxicity at lower doses than
adults) 2. Obstructive jaundice

Opioiods - Diphenoxylate
Drug interactions:1. Potentiate the effects of CNS depressants2. Co-administration with MAO inhibitors→
hypertensive crisesAdverse effects:3. Caused by the atropine in the preparation and
include anorexia, nausea, pruritus, dizziness, and numbness of the extremities.
4. Prolonged use of high doses may cause dependence
Opioids - Loperamide
Opioid agonist that does not cross the blood-brain barrier and has no analgesic properties and no potential for addictionAdverse effects: Abdominal pain and distention, constipation, dry
mouth, hypersensitivity, and nausea and vomiting.
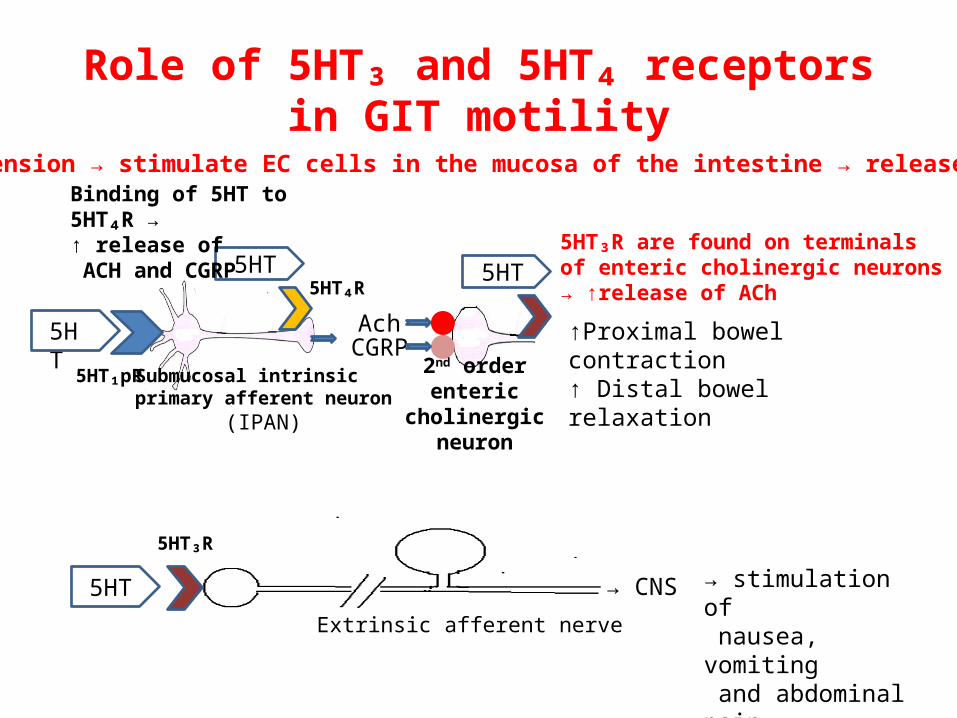
Role of 5HT₃ and 5HT₄ receptors in GIT motility
GIT distension → stimulate EC cells in the mucosa of the intestine → release of 5HT →
5HT
5HT₁pR
AchCGRP
Submucosal intrinsic primary afferent neuron
(IPAN)
2nd order enteric cholinergic
neuron
↑Proximal bowel contraction↑ Distal bowel relaxation
5HT₄R
5HT
Binding of 5HT to 5HT₄R → ↑ release of ACH and CGRP
5HT
5HT₃R
→ CNS
Extrinsic afferent nerve
→ stimulation of nausea, vomiting and abdominal pain
5HT₃R are found on terminals of enteric cholinergic neurons → ↑release of ACh
5HT

Serotonin 5HT₃ receptor antagonists
1. Inhibition of 5HT₃ receptors in the GIT→ inhibit nausea, bloating and pain
2. Inhibition of 5HT₃ receptors in the brain→ inhibit central response to afferent visceral stimuli
3. Inhibition of 5HT₃ receptors on terminals of enteric cholinergic neurons → ↓motility in the left colon and ↑colon transit time
Serotonin 5HT₃ receptor antagonistsAlosetron
Action: relieves lower abdominal pain, urgency and diarrhea (no effect on stomach)
Mechanism of action: 5HT₃ receptor antagonistUses: Female patients with severe IBS with
diarrhea with no response to other therapies

Serotonin 5HT₃ receptor antagonistsAlosetron
Pharmacokinetics: Rapidly absorbed after oral administration Plasma t½ = 1.5 h. Long duration of action (dissociates slowly from 5HT₃
receptor) Extensive hepatic metabolism (P450) with renal
excretion of metabolitesAdverse effects: Constipation Ischemic colitis (may be fatal)
Serotonin 5HT₄ receptor partial agonist:Tegaserod
Action:1. ↑gastric emptying and enhance small and large bowel transit (no
effect on esophagus)2. ↑ stool liquidityMechanism of action of tegaserod: Serotonin 5HT₄ partial agonist. Binding to 5HT₄ receptors on the terminals of the 2nd order enteric neuron
→↑ release of Ach and CGRP →↑gastric emptying and enhance small and large bowel transit (no effect on esophagus)
→↑ Cl secretion from the colon →↑ stool liquidity

Tegaserod
Pharmacokinetics:Low bioavailability (further reduced by food)→
should be taken before mealsMetabolized in liver (by glucuronidation)Excreted in feces (unchanged) and in urine
(metabolites)Contraindications:Severe renal or hepatic impairment

Tegaserod
Uses:Short term treatment (up to 12 weeks) of women with
moderate/severe IBS with predominant constipation who have failed to fiber supplementation and laxatives (reduce pain and bloating - ↑ bowel movements and ↓ hardness of stools)
Other uses:Chronic constipation in patients not responsive or intolerant to
other less expensive therapiesAdverse reactions (rare):1. Diarrhea2. Headache
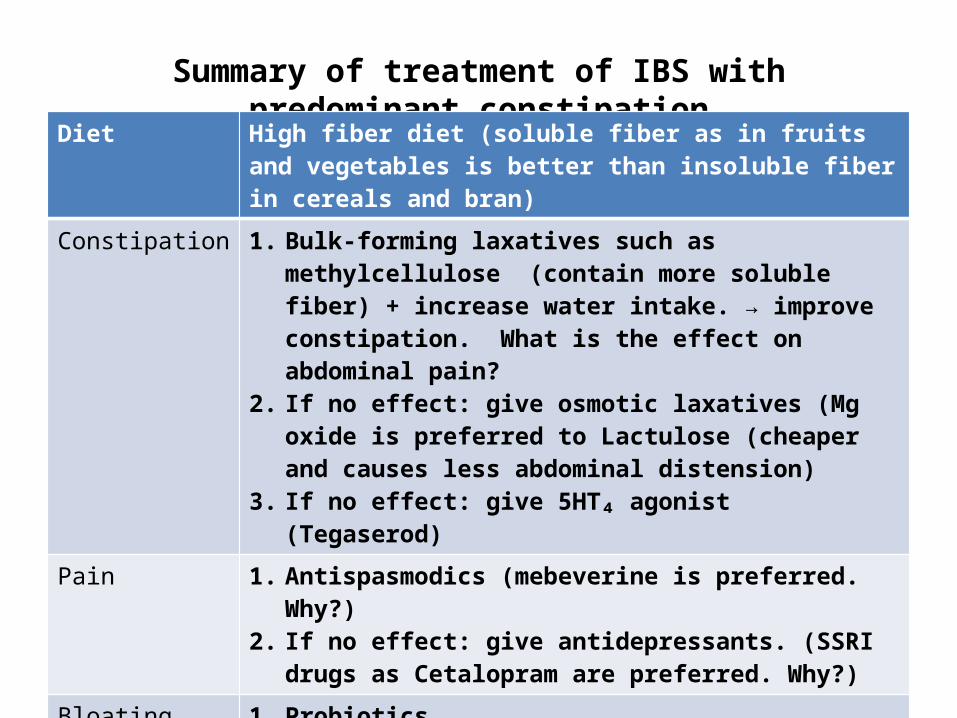
Summary of treatment of IBS with predominant constipationDiet High fiber diet (soluble fiber as in fruits and vegetables is better
than insoluble fiber in cereals and bran)
Constipation 1. Bulk-forming laxatives such as methylcellulose (contain more soluble fiber) + increase water intake. → improve constipation. What is the effect on abdominal pain?
2. If no effect: give osmotic laxatives (Mg oxide is preferred to Lactulose (cheaper and causes less abdominal distension)
3. If no effect: give 5HT₄ agonist (Tegaserod)
Pain 1. Antispasmodics (mebeverine is preferred. Why?)2. If no effect: give antidepressants. (SSRI drugs as Cetalopram
are preferred. Why?)
Bloating with distension
1. Probiotics2. If no effect: give 5HT₄ agonist (Tegaserod)
Bloating without distension
1. Probiotics2. Tricyclic antidepressants
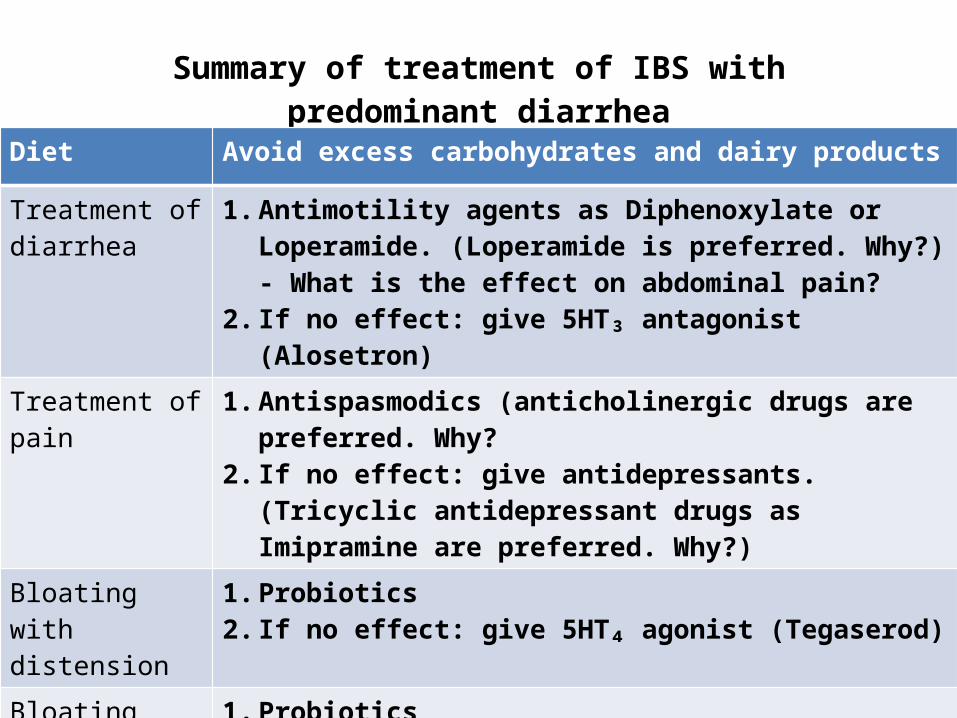
Summary of treatment of IBS with predominant diarrhea
Diet Avoid excess carbohydrates and dairy products
Treatment of diarrhea
1. Antimotility agents as Diphenoxylate or Loperamide. (Loperamide is preferred. Why?) - What is the effect on abdominal pain?
2. If no effect: give 5HT₃ antagonist (Alosetron)
Treatment of pain 1. Antispasmodics (anticholinergic drugs are preferred. Why?2. If no effect: give antidepressants. (Tricyclic antidepressant
drugs as Imipramine are preferred. Why?)
Bloating with distension
1. Probiotics2. If no effect: give 5HT₄ agonist (Tegaserod)
Bloating without distension
1. Probiotics2. Tricyclic antidepressants
Case (1)
A 34-year-old woman presents with a 6-month history of abdominal pain, bloating, distension, decrease in the number of bowel movements per week (<3 times) and difficulty when passing stools. She also states that the abdominal pain and bloating almost occur continuously throughout the day although her symptoms are alleviated by passing stool. She also states that the symptoms are worse when she has midterm or final examinations.

Case (1) cont.
She was taking bran till 3 months ago but could not stand the taste and wasn’t sure how much it was helping. She switched to psyllium powder but she felt that distension increased. She was also treated with sorbitol solution but it has some side effects and she resumed taking psyllium again.
Medical examination and investigations were unremarkable apart from slight abdominal distension and slight tenderness over the lower abdomen.

Case (1) Questions
1. Why did Psyllium caused abdominal distension?
2. What are the most probable side effects of lactulose in this patient?
3. Mention the drugs required for the patient?4. What are the side effects of each drug
prescribed?

Case (1) answer
A case of IBS with:1. Predominant constipation2. Abdominal pain 3. Bloating

Case (1) answer
Psyllium increased abdominal distension because it contain insoluble fiber which is fermented by colonic bacteria.
Side effects of lactulose:1. Diarrhea 2. Abdominal distension3. Taste may be objectionable

Case (1) answer
Treatment:1. Diet: High fiber diet consisting mainly of fruits and vegetables2. Laxatives:Bulk-forming laxatives such as methylcellulose with increasing
drinking of water3. Antispasmodics:Mebeverine or Hyoscine (Mebeverine is preferred because
Hyoscine may increase constipation)4. Probiotics 5. Tegaserod

Case (2)
• A 40-year-old man presents for the evaluation of abdominal pain and diarrhea. He states that for about 8 months he has had progressively worsening cramping pains, bloating and diarrhea (3 times/day). with loose stools. However, stools never contained blood. He has tried over-the-counter antidiarrheal medications but diarrhea often recurs. He is on no medication regularly and has no significant medical history. Examination of his abdomen revealed it to be distended and diffusely tender with no palpable masses. Otherwise, the patient is normal.
• What medications could be prescribed to that patient. What are their side effects? Comment on the diet that should be followed by the patient.

Case (2) Answer
Diet: Diet should be low in carbohydratesDrugs:The patient had IBS with predominant diarrhea
with pain and distension.Treatment of diarrhea: Loperamide. (why not
diphenoxylate?) What can you prescribe if loperamide fails? What are the side effects of the new drug? (see the table)

Case (2) Answer
Treatment of abdominal pain:1. Antispasmodics as Hyoscine (what are its side
effects and contraindications?). Why hyoscine is preferred to mebeverine in cases of diarrhea?
2. What are the second line drug you can prescribe if Hyoscine fails? What are the side effects of the new drug? (see the table)

Case (2) Answer
Treatment of bloating:Probiotics. (why tegaserod could not be
prescribed in this case?)

Treatment of constipation
Acute constipation1. Glycerine suppositoryIf not effective:2. Oral sorbitol or lactulose or saline laxatives
(e.g., Mg hydroxide)3. Low doses of bisacodyl or senna or cascara

Treatment of constipation
Chronic constipation: 1. Dietary modifications that increase dietary
fiber2. Bulk-forming agents (daily and continued
indefinitely)
Treatment of constipation in special populations
Bed ridden, geriatric or chronic constipation patients:1. First line of treatment is bulk forming laxatives 2. Second line: more potent agents may be required :
a) Osmotic laxatives (Saline laxatives as Mg hydroxide) or poorly absorbed sugars (sorbitol or lactulose).
b) Irritant laxatives (bisacodyl, senna, cascara)• Mineral oil should be avoided, particularly in bed-ridden patients.
Why? (because of the risk of aspiration and lipoid pneumonia).• When other than bulk-forming laxatives are used, they should be
administered in the lowest effective dose and as infrequently as possible to maintain regular bowel function (more than 3 stools per week).

Treatment of constipation in special populations
Fecal impaction. Before oral laxatives can be used, the impaction
needs to be removed using mechanical methods, including tap-water or saline enemas and digital extraction.

Treatment of constipation in special populations
In the hospitalized patient without GI disease:1. If rapid bowel evacuation is required:
Eithera)glycerin suppository orb)oral Mg hydroxideFollowed by: 2.
2. Most orally or rectally administered laxatives may be used in these situations.
Prevention of constipation
1. Prevention of straining during recovery from myocardial infarction or following rectal surgery
2. During pregnancy
1. Bulk-forming laxatives2. Docusate3. Irritant laxatives (mentioned
in some books)

Other uses of laxatives:Evacuation of bowel before surgery or diagnostic procedures involving the
GIT as sigmoidoscopy or barium enema:
Oral forms:Oral bisacodyl, sodium picosulfate, cascara or senna (active after 6 -12 h)
Given the night before operation or procedure)Oral castor oil (active after 1-3 h)Oral Mg hydroxide (active after 2-5h)Rectal suppository:Bisacodyl rectal suppository (active after 30 – 60 min)Enema:Rectal Na sulfate enema (active after 30 min)Polyethylene glycol - electrolyte solution enema

Case (1)
A 35-year-old patient on normal diet and exercise presented with Constipation since 2 weeks. Mention three alternative drugs from different groups that could be used to treat his condition giving the side effect of each.
Answer: 1. Glycerine suppository2. Lactulose3. Bisacodyl
Case (2)
You have been asked to prescribe a drug for prevention of straining for a hospitalized patient treated from myocardial infarction. Mention 2 drugs from 2 different groups giving their side effects.

Case (3)
A patient will undergo sigmoidoscopy in the next morning. Mention drugs which could be given to evacuate his bowel giving the expected time of action and possible adverse effects.
Constipation questions
Mention two pharmacological groups of drug that may cause constipation as a side effect giving the mechanism in each case.
To which category of drugs does lactulose belong? Comment on its mechanism of action.
Comment on the adverse effects which are associated with the use of stimulant laxatives.