there is no perfect hemodyypnamic parameter perfect.pdf · there is no perfect hemodyypnamic...
TRANSCRIPT

1
There is no perfect There is no perfect hemodynamic parameterhemodynamic parametery py p
Azriel Perel
Professor and ChairmanProfessor and ChairmanDepartment of Anesthesiology and Intensive CareSheba Medical Center, Tel Aviv University, Israel
Rome 2009
Disclosure
Th k t ith th f ll i iThe speaker cooperates with the following companies
BMeye
Drager-Siemens
Pulsion
2
Hemodynamic monitoring Hemodynamic monitoring is essential for proper is essential for proper
decisiondecision--making in critically ill making in critically ill and highand high risk surgical patientsrisk surgical patientsand highand high--risk surgical patients. risk surgical patients.
And yet, each and every And yet, each and every hemodynamic variable that we hemodynamic variable that we measure has limitations and measure has limitations and
confounding factors.confounding factors.
Knowing the limitations of Knowing the limitations of hemodynamic parameters is ashemodynamic parameters is ashemodynamic parameters is as hemodynamic parameters is as
important as knowing their important as knowing their potential value.potential value.

3
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation
Clinical evaluation compared to PAC in the hemodynamic assessment of critically ill patients
Eisenberg PR et al. Crit Care Med 1984; 12: 349
Physicians correctly predict the cardiac output, Physicians correctly predict the cardiac output, PCWP and SVR in only PCWP and SVR in only 5050% of the cases% of the cases
Prediction of hemodynamics in critically ill patients by Prediction of hemodynamics in critically ill patients by clinical evaluation alone is inaccurate and unreliable.clinical evaluation alone is inaccurate and unreliable.
Assessing hemodynamic status in critically ill patients: Do physicians use clinical information optimally?
Connors AF et al. J Crit Care 1987; 2: 174
Therapeutic impact of PAC in the ICUSteingrub et al. Chest 1991; 99: 1451
PAC in critically ill patients: A prospective analysis of outcome changes associated with catheter-prompted changes in therapy
Mimoz O et al. Crit Care Med 1994; 22: 573
Hemodynamic and pulmonary fluid status in the trauma patient: are we slipping?
Veale WN Jr et al. Am Surg. 2005; 71: 621

4
In patients with ALI there is a high probability that physical examination findings of ineffective
i l ti ( ill fill ti >2 kcirculation (capillary refill time >2 secs, knee mottling, or cool extremities) are not useful for predicting low cardiac index or mixed venous oxygen saturation.
In high-risk, hemodynamically stable surgical patients, there were no significant differences in mean BP, HR, urine output, and arterial oxygenation at any time between survivors and non-survivors, although non-survivors had higher lactate levels than survivors.
Adequate resuscitation cannot be based Adequate resuscitation cannot be based only on normalization of vital signs.only on normalization of vital signs.

5
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation

6
“Estimates of intravascular volume based on any given level of filling pressure do not reliably predict a
Crit Care Med 2006;34:1333
pressure do not reliably predict a patient’s response to fluid administration.”
We do not recommend the routine use of the PAC for patients in shockPAC for patients in shock.
We recommend that preload measurement alone not be used to predict fluid responsiveness.

7
CCM 2007 35:64-8
Occult hypoperfusion! Fluid
overload!

8
This systematic review demonstrated a very poor relationship between CVP and blood volume as well as the inability of CVP / ΔCVP to predict the hemodynamic response to ato predict the hemodynamic response to a fluid challenge.
CVP should not be used to make clinical decisions regarding fluid management.
Intravascular volume depletion in a Intravascular volume depletion in a 2424--hour porcine model of hour porcine model of intraintra--abdominal hypertensionabdominal hypertension
Schachtrupp A et al, J Trauma. Schachtrupp A et al, J Trauma. 5555: : 734734--740740, , 20032003
Traditional CVP cannot b d t t lbe used to accurately direct resuscitation of the critically ill patients with elevations in IAP or ITP. To do so places the patient at risk for under-resuscitation
Cheatham ML. CCM 2007; 35:1629
under-resuscitation with resultant organ dysfunction, failure, and increased mortality.

9
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation
Global End-Diastolic Volume as an Indicator of Cardiac Preload in Patients With Septic Shock
F Michard et al, Chest. 2003;124:1900-1908
% of fluid-responders
720
740
760
780
800PrePre--infusioninfusionGEDViGEDVi(mL/m(mL/m22))
600
620
640
660
680
700
Responders Non-responders

10
ITBV and its changes correlates to CI and its changes ITBV and its changes correlates to CI and its changes significantly better than the CVPsignificantly better than the CVP
Crit Care Med 2008; 36: 2348

11
Static ‘preload’ parameters cannot Static ‘preload’ parameters cannot accurately predict the response of the accurately predict the response of the
CO to fluid loadingCO to fluid loading
F Michard et al, Chest 2003
Should we monitor preload andShould we monitor preload and fluid responsiveness in shock?

12
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation
Functional hemodynamic parameters Functional hemodynamic parameters (SPV, PPV, SVV) are the most sensitive (SPV, PPV, SVV) are the most sensitive
parameters for the assessment of parameters for the assessment of
SPV PPV SVVSPV PPV SVV
Responder Non-responder
ppfluid responsiveness in mechanically fluid responsiveness in mechanically
ventilated patientsventilated patients

13
Limitations and confounding factors of functional hemodynamic parameters
1. Sinus rhythm
2. Spontaneous breathing
3. Tidal volume / airway P.
4. Use in ARDS
5. SPV vs. PPV and SVV
6. The neglected dUp
7. New algorithms
14
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation
Unreliability of blood pressure and heart rate to evaluate cardiac output in emergency resuscitation
and critical illness.
Wo CCJ, et al. CCM 1993;21: 218
Blood flow (cardiac output) cannot li bl b i f d f t i lreliably be inferred from arterial
pressure and heart rate measurements until extreme hypotension occurs.

15
A Perel, M Maggiorini, M Malbrain, JL Teboul, J Belda, E Fernández-Mondéjar, M Kirov, J Wendon
The PiCClin StudyThe PiCClin Study
206 206 critically ill patients were evaluated by critically ill patients were evaluated by 166 166 id t did t d 146146 i li ti li tresidents and residents and 146 146 specialists.specialists.
EVLWiGEDViSVRCO
124 (40.8%)
154 (49%)
107 (34.3%)
110 (34.9%)Within ± 20%
83 (27.3%)
97 (30.9%)
46 (14.7%)
170 (54%)
Under-estimation
>20%
The main reason to measure CO is to identify patients that have low (or high) CO values that is not evident clinically, and to assess response to diagnostic and therapeutic interventions.

16
Th i iti l h f SAH iThe initial phase of SAH is characterized by a high CI (5.3 L/min/m2) and a low GEDVi (555 mL/m2).
CI progressivelyCI progressively decreased and GEDVi was normalized by fluid administration aimed at normovolemia.
Cardiac output in and by itself is not
enough!
Cardiac output 6.77 L/min
ScvO2 is 60%!
Is this CO adequate???

17
ScvOScvO22==7474CO
Patient is given dobutamine
ScvOScvO22==6363ScvOScvO22==7676
22
CO was high, but not high enough!CO was high, but not high enough!
The limitations of cardiac output
The optimal CO for an individual patient is difficult to assess.
A low CO does not tell us WHAT to do.
A ‘normal’ or even high CO does preclude the presence of inadequate regional and microcirculatory flow.

18
Clinical examinationClinical examinationBlood pressure, Heart rateBlood pressure, Heart rate
Urine outputUrine outputCVP PAOPCVP PAOPCVP, PAOPCVP, PAOPGEDV, EDAGEDV, EDA
SPV, PPV, SVVSPV, PPV, SVVCOCO
ScvOScvO22
PetCOPetCO22
SaOSaO22
EVLWEVLWMicrocirculationMicrocirculation

19
wns
trea
mLactate
Organ function
SvO ScvO
Upstream
CO
Hgb
CaO2
Venous oximetry Bloos, Reinhart Intensive Care Med 2005; 31:911-3
DoSvO2, ScvO2
PcvCO2
m
2

20
It is useful to measure SvO2 because if cardiac output becomes inadequate, SvO2 will decrease.
A low SvO2 should prompt rapid intervention to increase oxygen delivery to the tissues.
“Clearly, SvO2 is the gold standard for defining global adequacy of
Crit Care Med 2005; 33:1119-22
g g q ycardiovascular performance.”

21
A low ScvOA low ScvO22 in the perioperative period is in the perioperative period is associated with increased risk of associated with increased risk of
postoperative complicationspostoperative complications
Mixed venous oxygen saturation in critically ill septic shock patients.Krafft P, et al. Chest 1993; 103:900
Fluid resuscitation in severe sepsis and septic shock: An evidence-based review.
Vincent JL, Gerlach H. CCM 2004; 32[Suppl.]:S451
The SvOThe SvO22 of septic shock patients isof septic shock patients is mainly mainly normal or even supranormal or even supra--normal due to reduced normal due to reduced oxygen extraction.oxygen extraction.
ce t J , Ge ac CC 00 ; 3 [Supp ] S 5
Therefore, a normal or high SvOTherefore, a normal or high SvO22 does not does not necessarily indicate adequate tissue necessarily indicate adequate tissue oxygenation.oxygenation.
22
Kortgen A, et al: Implementation of an evidence-based
The ScvO2 values of patients in septic shock are significantly higher than those
reported by Rivers et al (~50%)
‘standard operating procedure’ and outcome in septic shock. Crit Care Med 2006, 34:943-949.
Shapiro NI, et al: Implementation and outcomes of the Multiple Urgent Sepsis Therapies (MUST) protocol. Crit Care Med 2006, 34:1025-1032.
van Beest P, et al: The incidence of low venous oxygen saturation on admission in the ICU: a multicenter observational study in the Netherlands. Crit Care 2008, 12:R33Out of Out of 125 125 patients in septic shock only patients in septic shock only 8 8 patients (patients (66%) %) had ScvOhad ScvO22 < < 6060%, and only %, and only 1 1 ((11%) < %) < 5050%.%.
, et al,
In ICU-resuscitated patients, targeting only ScvO2 may not be sufficient to guide therapy.
When the 70% ScvO2 goal-value is reached, the presence of a P(cv-a)CO2 larger than 6 mmHg might be a useful tool to identify patients who still remain inadequately resuscitated.
23
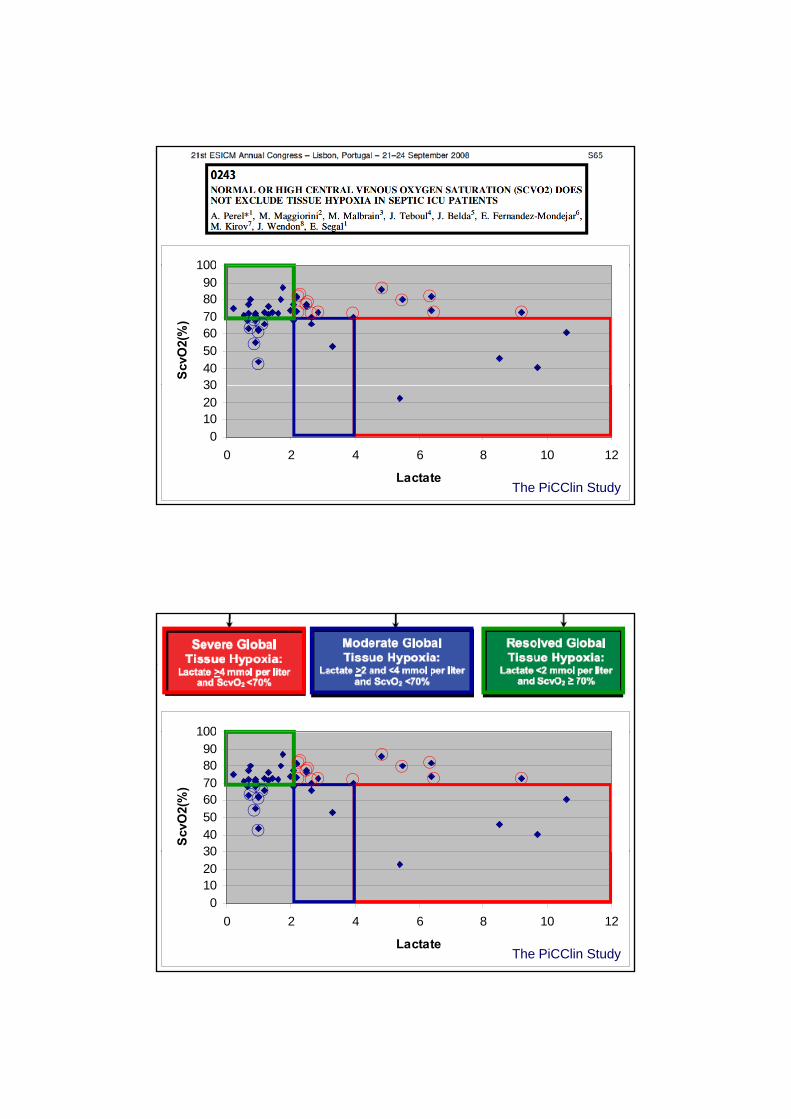
100
30405060708090
100
ScvO
2(%
)
0102030
0 2 4 6 8 10 12
LactateThe PiCClin Study
100
30405060708090
100
ScvO
2(%
)
0102030
0 2 4 6 8 10 12
LactateThe PiCClin Study

24
SvOSvO22
ScvOScvO22(CVC)(CVC) Sander M, et al.
(PAC)(PAC)
S O >S O S O <S O
Gutierrez G, et al.
ScvO2>SvO2 ScvO2<SvO2
A low SvO tells you that something is wrong but
The major problems with the interpretation of ScvO2
A low SvO2 tells you that something is wrong, but not what is wrong and what should be done about it (fluids? inotropes?).
However,
When the O2ER is reduced, as is frequently the case 2 , q yin septic patients, a normal or high ScvO2 does not guarantee that perfusion is adequate and that resuscitation is complete.
25
Each and every Each and every yyhemodynamic variable hemodynamic variable that we measure has that we measure has
limitations and limitations and confounding factors.confounding factors.
A number of large, randomized, prospective trials have demonstrated that protocol-based strategies can not only reduce variation and cost of ICU medicine but also improve morbidity and mortality of critically ill patients requiring ICU support.
Pathways to standardize numerous facets of patient care are becoming the most sought-after means of improving patient outcomes and reducing overall ICU expenditures.

26
“Medicine has become complex. Details have become overwhelming for clinicians to process at the bedside…
Surely, we recognize the need to give up some measure of autonomy…yield some decision-making power…
The data certainly suggest that when we surrender this autonomy and standardizesurrender this autonomy and standardize care, patients do better.”
M. Levy, SCCM 2009
38th SCCM Conference Perspectives
27
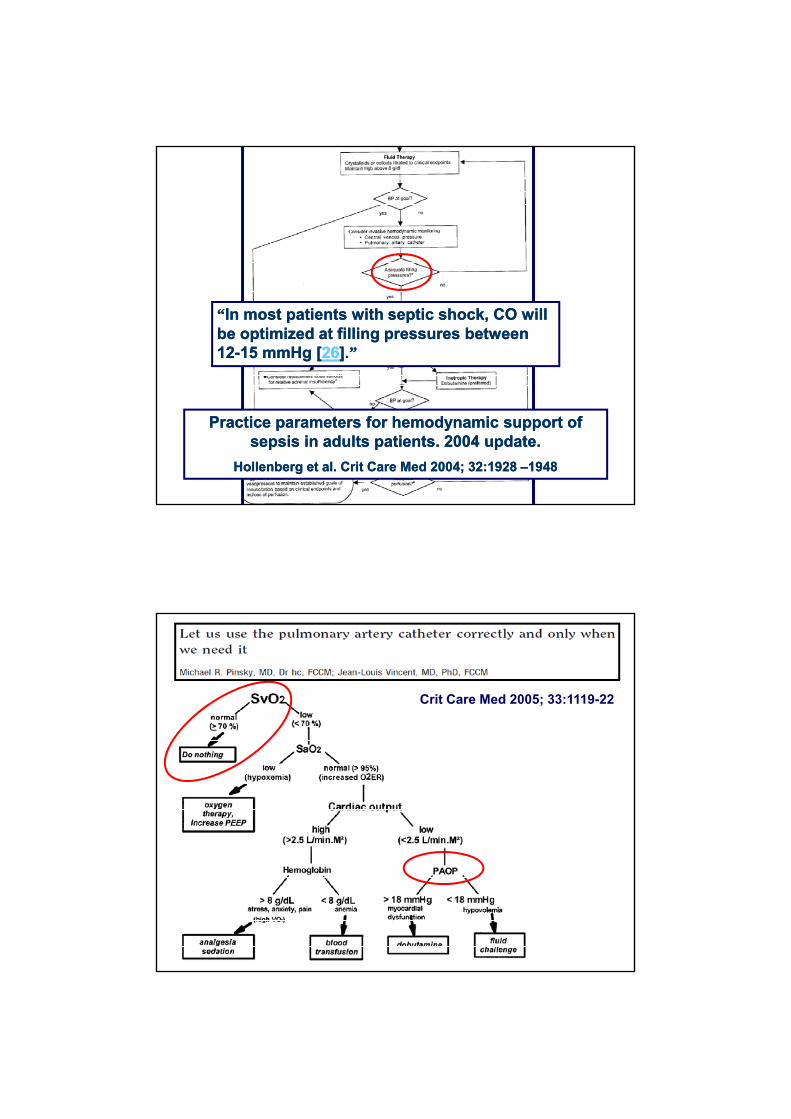
““In most patients with septic shock, CO will In most patients with septic shock, CO will be optimized at filling pressures between be optimized at filling pressures between
””].].2626mmHg [mmHg [15 15 --1212
Practice parameters for hemodynamic support of Practice parameters for hemodynamic support of sepsis in adults patients. sepsis in adults patients. 2004 2004 update.update.
Hollenberg et al. Crit Care Med Hollenberg et al. Crit Care Med 20042004; ; 3232::1928 1928 ––19481948
Crit Care Med 2005; 33:1119-22

28
During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol:
The application of invasive monitoring data is very complex and is not easily included in therapeutic protocols that are applicable across heterogeneous populations of acutely ill patients.
Hemodynamic management is made complex because adequacy is not synonymous with “normality” and because correct application must integrate several variables…reality may be more complex than initially thought.

29
The large number of critical variables and how they interact
The correct application of monitored cardiopulmonary and other variables in the critically ill is characterized by:
interact.
The importance of initial starting conditions to eventual outcome.
The effects of unexpected events.
The non-linear dynamics: Small things may have i t d t !an enormous impact downstream!
These in fact are the principles of the Complexity Theory which is used for
describing weather, traffic patterns, etc.
A therapeutic approach that targets and attempts to normalize abnormal physiological variables may be hazardous because of
Ignoring the underlying problemInducing harmAblation of physiological benefit Generation of associated errorsTraining effect

30
What should we be doing?What should we be doing?
((4 4 final comments)final comments)
Hemodynamic monitoring Hemodynamic monitoring is essential for proper is essential for proper
decisiondecision--making in critically illmaking in critically illdecisiondecision--making in critically ill making in critically ill and highand high--risk surgical patients. risk surgical patients.
The fact that this statement is not The fact that this statement is not supported by EBM tells us more supported by EBM tells us more pp ypp yabout the shortcomings of EBM about the shortcomings of EBM
than those of hemodynamic than those of hemodynamic monitoring.monitoring.

31
The fact that each and every The fact that each and every h d i i bl th th d i i bl th themodynamic variable that we hemodynamic variable that we measure has limitations and measure has limitations and
confounding factors has to be confounding factors has to be recognized and incorporated intorecognized and incorporated intorecognized and incorporated into recognized and incorporated into
the way we practice and teach.the way we practice and teach.
Since no hemodynamic parameter Since no hemodynamic parameter y py pis perfect, a multiis perfect, a multi--parametric parametric
approach may reduce the chance approach may reduce the chance of erroneous decisions.of erroneous decisions.

32
Attempts to protocolize care in Attempts to protocolize care in critically ill patients have to leave critically ill patients have to leave
room for clinical judgment room for clinical judgment especially during especially during
th ti fli tth ti fli ttherapeutic conflicts.therapeutic conflicts.
If you meet the Buddha on the road, kill him!Sheldon Kopp
Lowe & Brydon (Printers) Ltd. 1974. ISBN 0-85969-022-9.
We must live within the ambiguity of partial We must live within the ambiguity of partial freedom, partial power, and partial knowledge.freedom, partial power, and partial knowledge.
All important decisions must be made on the All important decisions must be made on the basis of insufficient data.basis of insufficient data.
Yet we are responsible for everything we do.Yet we are responsible for everything we do.
No excuses will be accepted.No excuses will be accepted.
[email protected] you!