thoracic trauma - ucsf medical education€¦ · 5/27/10 1 arun nagdev, md department of emergency...
TRANSCRIPT

5/27/10
1
Arun Nagdev, MD Department of Emergency Medicine
Highland General Hospital Director, Emergency Ultrasound
Thoracic Trauma
Overview
• Overview
• Penetrating Thoracic Trauma
• Blunt Thoracic Trauma
• Bedside Ultrasound for Thoracic Trauma
Chest Trauma
Severe Hypoxia
Massive Blood Loss
Reduced Cariac Output
5/27/10
2
ED Goal - Trauma
• Stabilize the Very Sick (thorocostomy, ED thorocotomy, etc.)
• Image the Sick
• Send home the Well
go over basic ATLS including slide on the sick vs not sick slide transition for sick with thorocostomy or edt
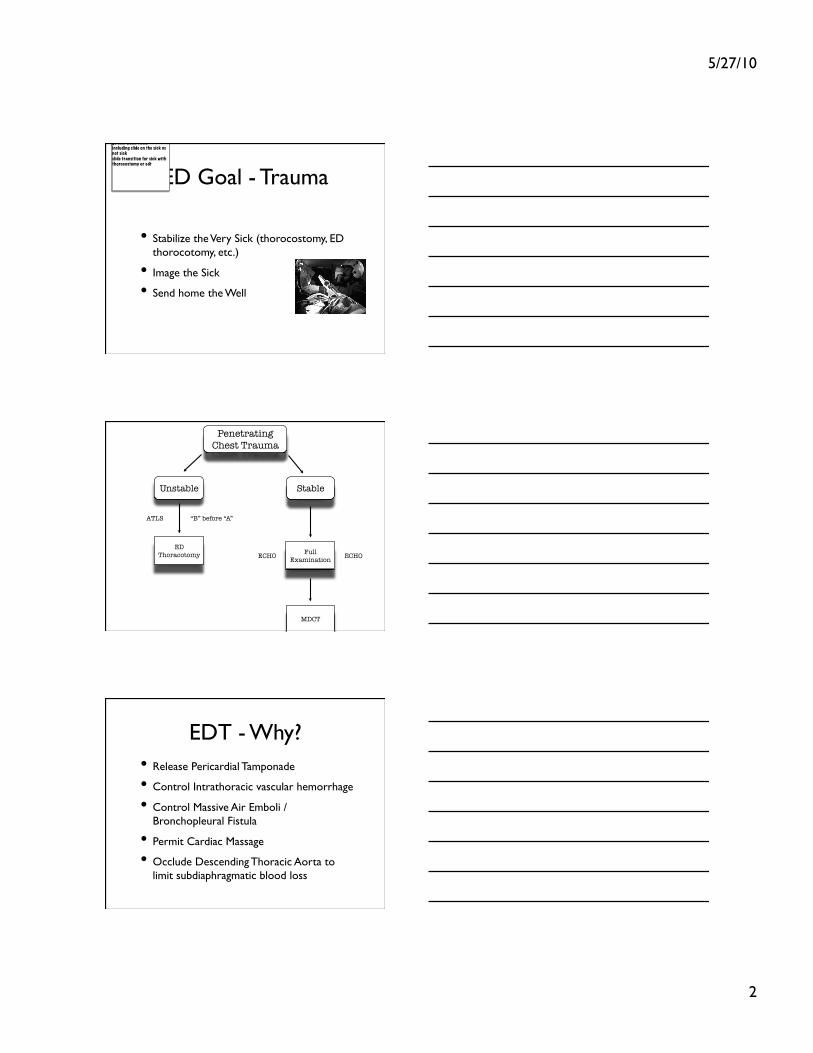
Penetrating Chest Trauma
Unstable Stable
ATLS
ECHO ED
Thoracotomy
MDCT
Full Examination ECHO
“B” before “A”
EDT - Why? • Release Pericardial Tamponade
• Control Intrathoracic vascular hemorrhage
• Control Massive Air Emboli / Bronchopleural Fistula
• Permit Cardiac Massage
• Occlude Descending Thoracic Aorta to limit subdiaphragmatic blood loss

5/27/10
3
When - Selective
• Signs of life* in the ED
• No obvious Non-survivable Injuries
• very low survival rates
• Signs of life in the field or ED
• SW (10%)
• GSW (1-5%)
Blunt Penetrating
J Trauma. 1993 May;34(5):711-5; discussion 715-6.
Cardiac stapling in the management of penetrating injuries of the heart: rapid control of hemorrhage and decreased risk of personal contamination. Macho JR, Markison RE, Schecter WP.
Department of Surgery, University of California, San Francisco.
EDT - Why? • Release Pericardial Tamponade
• Control Intrathoracic vascular hemorrhage
• Control Massive Air Emboli / Bronchopleural Fistula
• Permit Cardiac Massage
• Occlude Descending Thoracic Aorta to limit subdiaphragmatic blood loss
Release Pericardial Tamponade
5/27/10
4
ED ECHO
• A needed tool for ALL EM physicians managing Thoracoabdominal Trauma
• Not difficult to determine Pos vs Neg pericardial Effusion
• Game Changer
Oakland 911
• 23 ym s/p left sided SW
• Hypotensive in the field, cool, clammy, diaphoretic but GCS 15
• ABC intact, BG 111
• BP?
5/27/10
5
Dispo?
• Pressures + trauma surgeon = OR
• PEA and/or no trauma surgeon = volume + ED thoracotomy
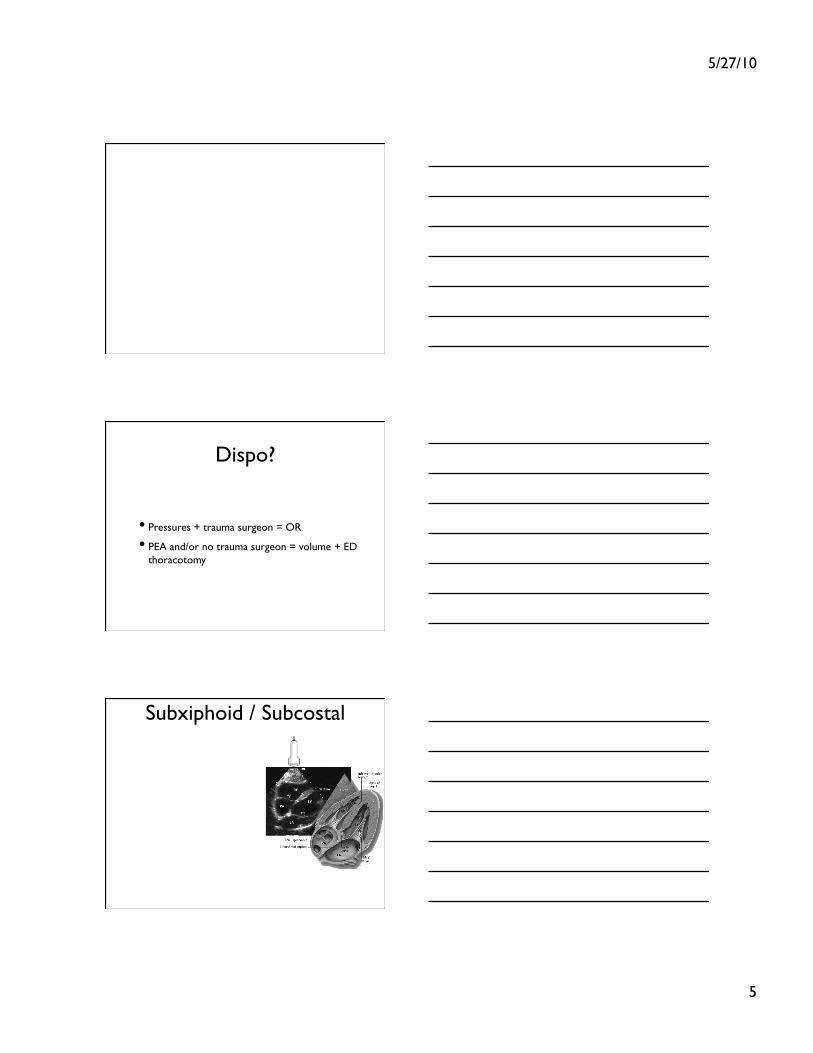
Subxiphoid / Subcostal

5/27/10
6
RV
LV RA
LA
Liver COPD

5/27/10
7
Parasternal Long
LV
RV Mitral Valve
Ao
Pericardium
Young and Healthy
DTA

5/27/10
8
• Residents and Attendings
• 1h didactic and 4 h hands-on
• N=515
• Sens = 96%
• Spec 98%
• Accuracy = 97.5%
Quick Penetrating Chest Trauma Points
• Below the Nipple = think about the abdomen
• Chest tube with lots of blood (>1-1.5L) think OR
• Air leak from Chest Tube w/ continued pneumo = tracheobronchial injury
• Bedside ECHO mandatory
Blunt Thoracic Injury

5/27/10
9
Stable
1. Lost Pulses - EDT 2. Pneumo - Needle vs Thorocostomy 3. Hemo - Thorocostomy 4. Pericardial Effusion -Pericardiocentesis vs EDT
ABC
Persistent Hypo or Blood Loss
OR Thoracotomy
MDCT
Secondary Survey CXR?
“B” before “A”
Done
No
MDCT
Improved
????
Yes
• N=492 patients
• 31/492 had injury
• Palpable Chest Tenderness or Hypoxia identified all SIGNIFICANT injuries
• Potential = 46% reduction of CXR
• No f/u after D/C
Ann EM 2006
• Retro Trauma Registry = 1989 (2.7%) to 2004 (28.7%) - N=1873
• Normal CXR then MDCT = sig number of occult injuries (hemo/pneumo, rib fractures, etc.)
• 6 BAI w/ normal CXR
• ? Need for all Thoracic Trauma to get MDCT
J Trauma 2007
5/27/10
10
Non-trauma Centers
• EM Docs = highly sensitivity
• Large trauma center is very different than a single coverage ED
• Goal = Emergent Intervention vs Further Imaging vs nothing
• Associations - for the “in between” group�
EMS Questions / Pretest
• Vehicle Speed ? High Speed (>40mph)
• Restraints? (seat belts and airbag deployment)
• Extensive vehicle damage with intrusion?
• Steering Wheel Deformity
H&P
• Obvious injuries = imaging
• Vital Signs
• Patient’s complaints / clinical appearance

5/27/10
11
Imaging
• CXR vs Chest CT
• Low risk (no tenderness or hypoxia) - as per Rodriguez, we may not even need a CXR
• Really Sick / High Mechanism = Stabilize and CT
• In Between - look for Associated Injuries
Blunt Thoracic Trauma
CXR
• AP vs PA
• Sensitivity, Specificity
• No need?
• Done after CXR
5/27/10
12
CRX : Bad • Wide Mediastinum
• Obscured Aortic Knob
• Left Apical Cap
• Large Left hemothorax
• Deviation of NGT
• Deviation of trachea rightward and/or right mainstem bronchus downward
• Wide Paravertebral Stripe
Chest CT
• Gold Standard
• Radiation?
• All Blunt Thoracic Injuries?
Difficult Injuries • Occult Hemothorax
• Occult Pneumothorax
• Aortic Injury
• Cardiac Contusion
• Pulmonary Contusion
• Diaphragmatic Injury
• Multiple Rib Fracture / Sternal Fracture
label Easy, Med, Difficult
Concept - Need to know they exist and how your tests sens/spec to pick one up
Example - bowel injury Ovarian Torsion
5/27/10
13
Occult Hemothorax
• defined - missed by supine CXR
• 300 cc on upright CXR
• 20-30% not identified on Supine CXR
• What to do with them?
• Association with other thoracic injuries?
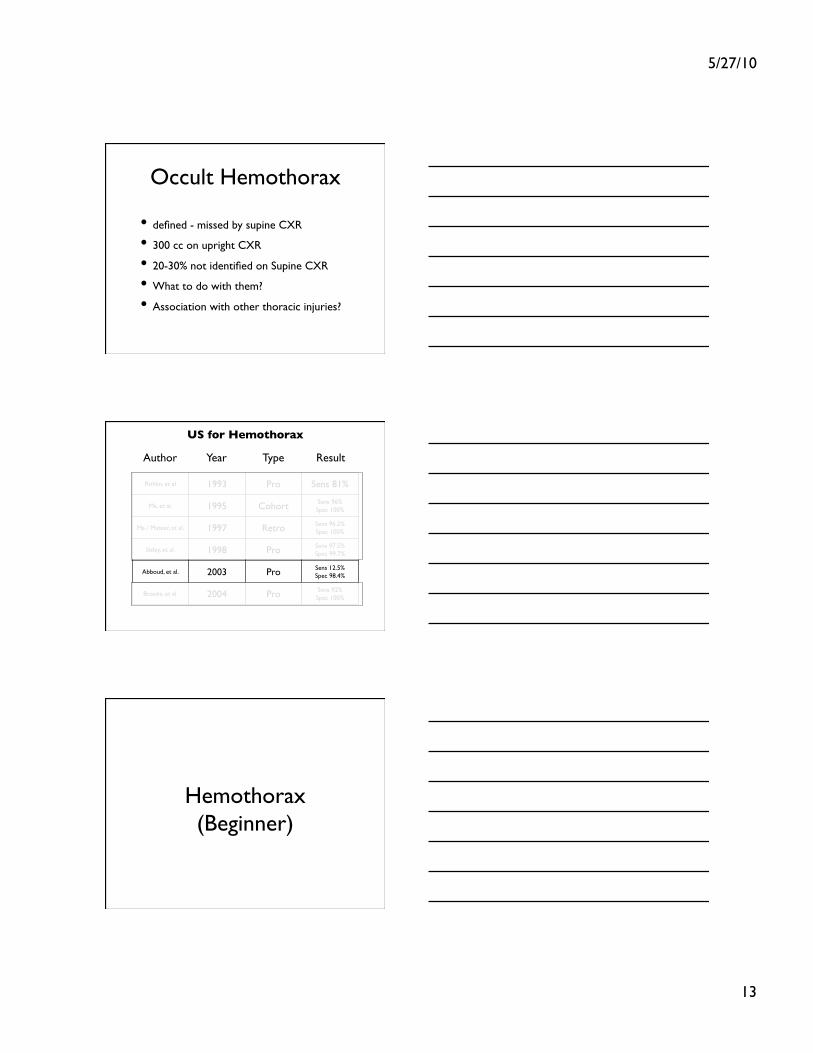
Rithlin, et al 1993 Pro Sens 81%
Ma, et al. 1995 Cohort Sens 96% Spec 100%
Ma / Mateer, et al. 1997 Retro Sens 96.2% Spec 100%
Sisley, et al. 1998 Pro Sens 97.5% Spec 99.7%
Abboud, et al. 2003 Pro Sens 12.5% Spec 98.4%
Brooks, et al. 2004 Pro Sens 92% Spec 100%
Author Year Type Result
US for Hemothorax
Hemothorax�(Beginner)

5/27/10
14
Probe Selection
Low Freq
Curvilinear
Supine Chest
Air
Blood

5/27/10
15
Rationale
Hemothorax - Landmarks
• Always Identify the Diaphragm
• Look Above and Below the Diaphragm
• Practice on Normal
• Black / Anechoic stripe = Blood
5/27/10
16
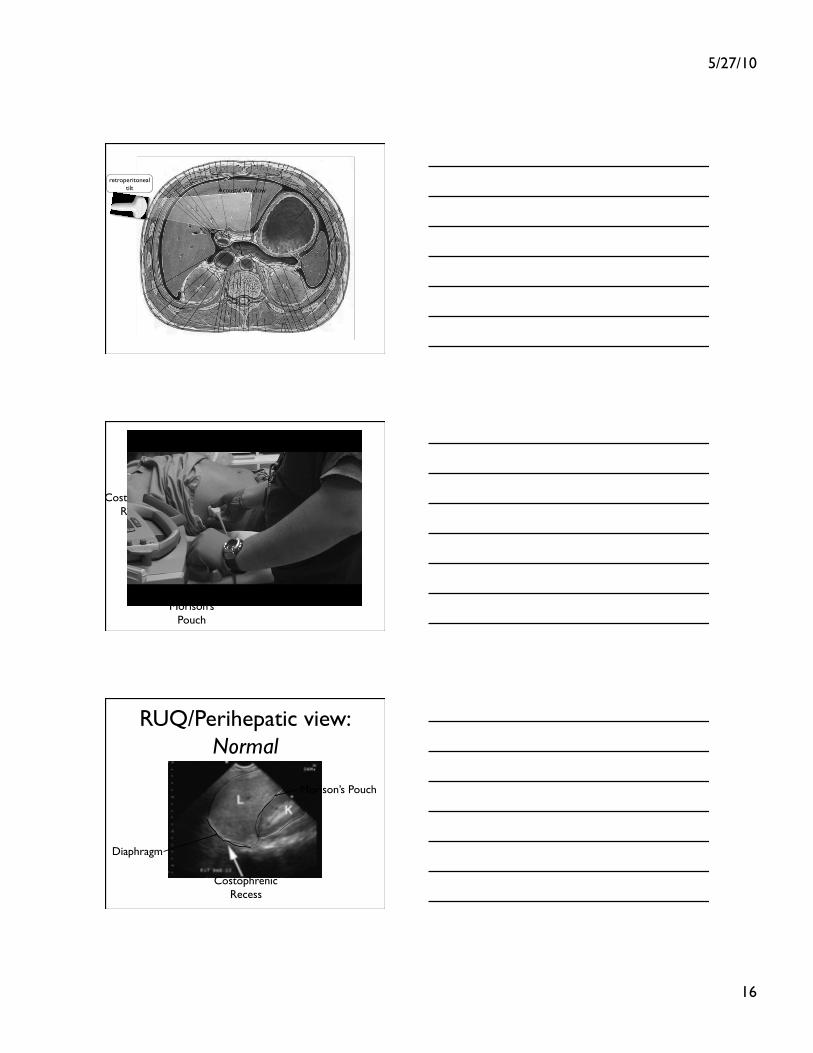
Acoustic Window
retroperitoneal tilt
Morison’s Pouch
Costophrenic Recess
RUQ/Perihepatic view:�Normal
Morison’s Pouch
Costophrenic Recess
Diaphragm

5/27/10
17
Hemothorax Data
• Ma, Mateer, et al. Trauma Ultrasound Examination Versus Chest Radiography in the Detection of Hemothorax. Ann Emerg Med 1997
• Abboud et al. Emergency Department Ultrasound For Hemothorax After Blunt Traumatic Injury. JEM 2003
• Brooks et al. Emergency Ultrasound in the Acute Assesment of Haemothorax. EMJ 2004
Poor Sensitivity for Small Volumes?

5/27/10
18
What to do with Occult Hemo?
• Bllello, et al. “Occult Traumatic Hemothorax: when can sleeping dogs lie?” AM J Surg 2005
• Stafford, et al. “Incidence and management of occult hemothoraces” AM J Surg 2006
• Small = leave alone
• Large (>1.5cm) = drain
• ABX for Thorocostomy- ?
Clinical Relevance
• Like FAST, large/clinically significant should be clearly visible*
• Does a small hemothorax warrant further CT imaging?
• Associations
5/27/10
19
Associations
• No prospective data regarding associations between hemothorax and other more serious Intrthoracic injuries
• Further imaging may be warranted
• You know your next step

5/27/10
20
Pneumothorax
sens of AP cxr sens of us when do you place a chest tube abx for chest tube
easy
Pneumothorax�(Intermediate)

5/27/10
21
86-98%
97-100%
CXR US
Sens
Spec
AEM Jan 2010
4 prospective observational studies
Supine Chest
Air

5/27/10
22
Hilum B A
V
V
L
1980
Lams et al. 1982 Radiology;142:309-312
Inferior Pulmonary Ligament
Pleural Space
Mediastinum
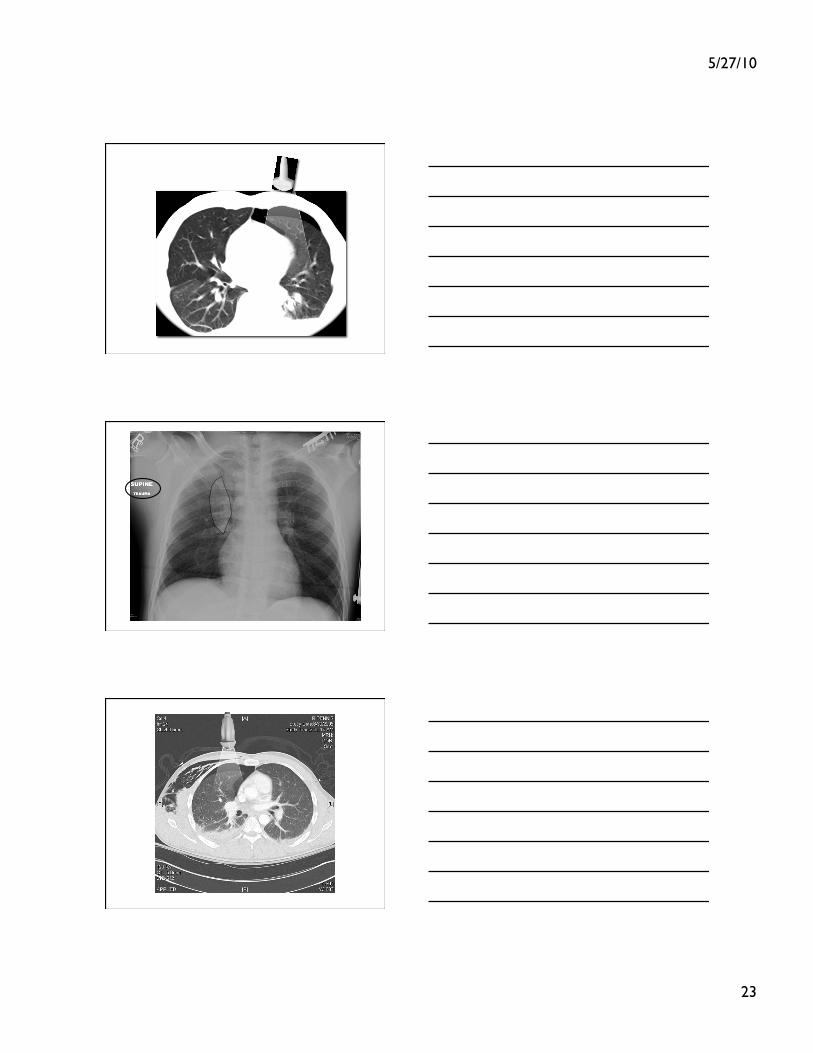
5/27/10
23
5/27/10
24
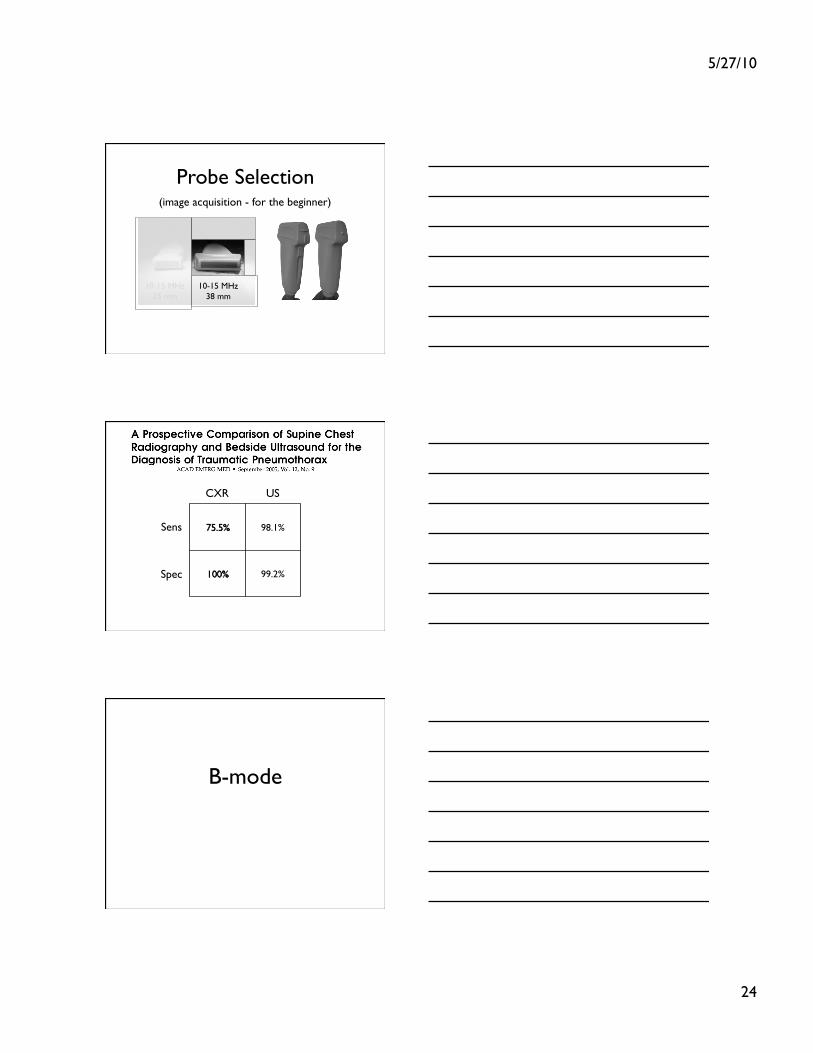
Probe Selection
10-15 MHz 38 mm
10-15 MHz 25 mm
(image acquisition - for the beginner)
98.1%
99.2%
CXR US
Sens
Spec
B-mode
5/27/10
25
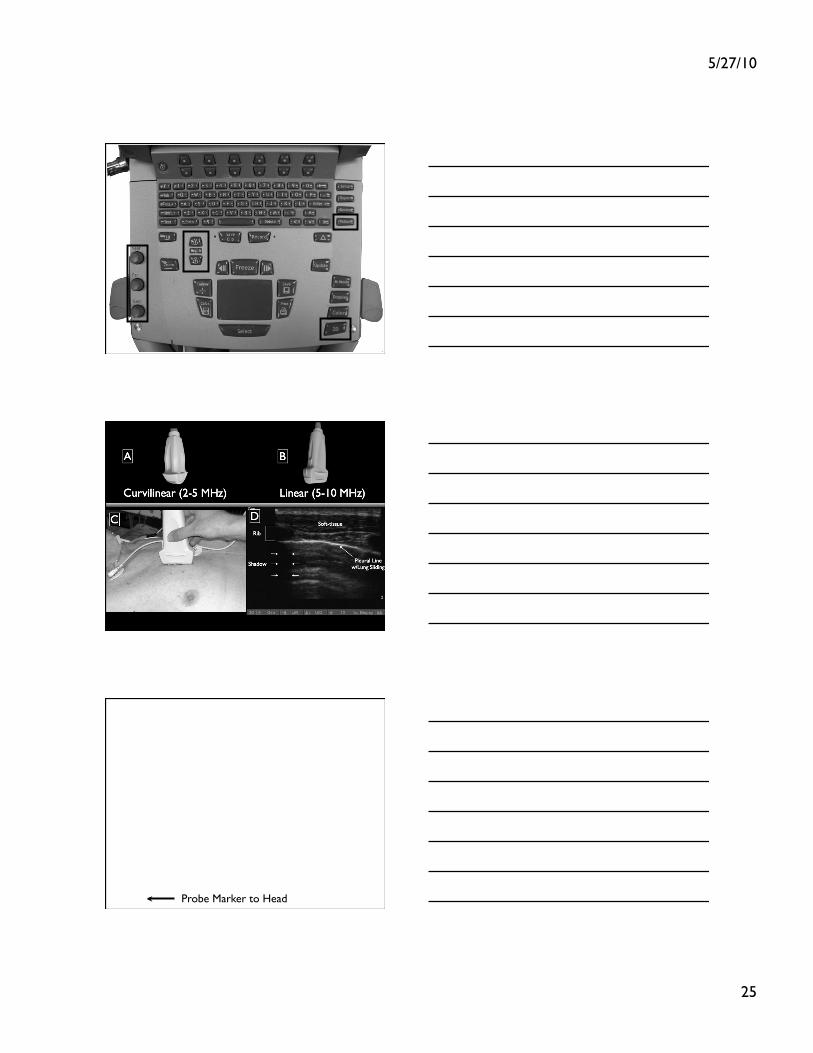
Probe Marker to Head

5/27/10
26
Rib Rib Normal
Lung
Rib
Alveoli
Rib Shadow
Normal Lung: Sliding Visceral Pleura
Normal Lung
5/27/10
27
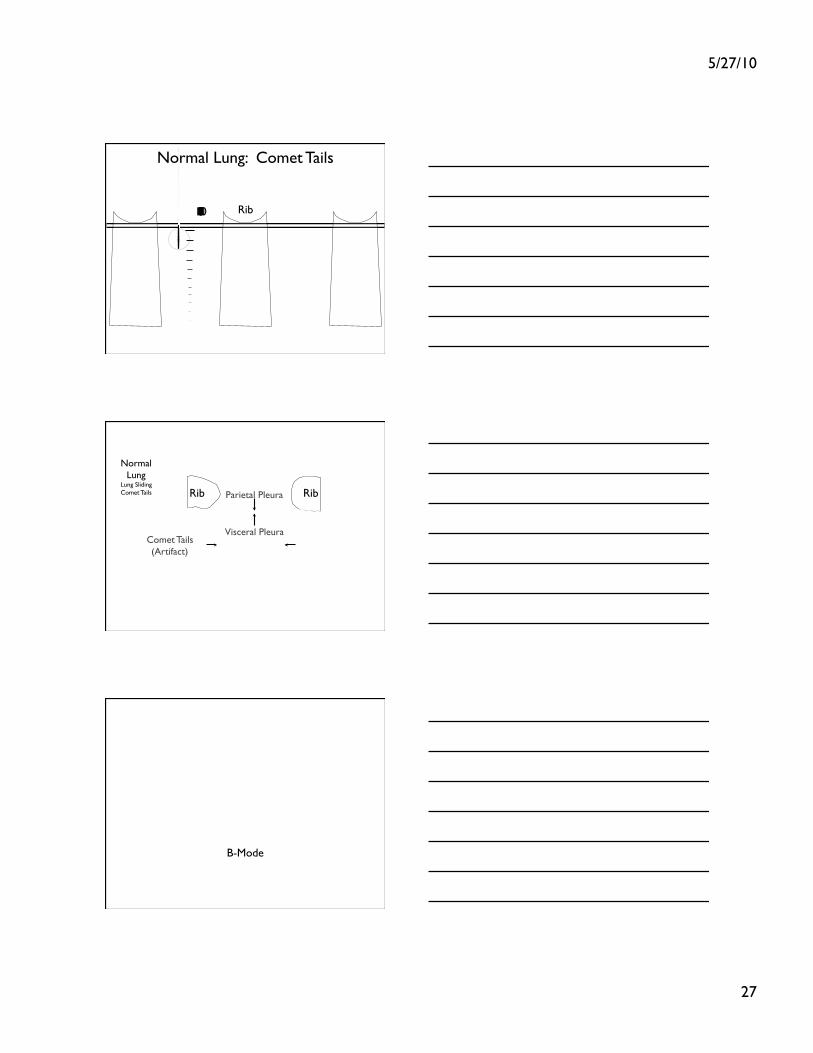
Rib 1 2 3 4 5 6 7 8 9 10 11
Normal Lung: Comet Tails
Rib Rib Parietal Pleura
Visceral Pleura Comet Tails (Artifact)
Normal Lung
Lung Sliding Comet Tails
B-Mode

5/27/10
28
Rib
AIR
Rib
Abnormal Lung: Pneumothorax
Parietal Pleura
Visceral Pleura
Parietal Pleura
Air (Scatter)
5/27/10
29
Normal Abnormal
REVIEW
Back to our CASE

5/27/10
30
Pneumo - No lung Sliding Normal
What to do?
2009
Much Debate - positive and negative data in small studies
Watch all non-ventilated patients
Intubation = Chest Tube

5/27/10
31
US for Occult Pneumo
• Practice on Normals
• Look for Lung Sliding
• Supine CXR does not R/O a Pneumo
• Associated Injuries with ? need for further imaging
Sternal Fracture • Mech - Hig energy, rapid decel with chest
hitting steering column
• AP CXR = 50% sensitive
• CT Chest - much more sensitive, but no definitive studies
• Again - standard imaging Not Sens
US?

5/27/10
32
Association
• High associations with intrathoracic injuries
• CT Chest, ECG, +/- cardiac biomarkers
• No data on ED US
Blunt Cardiac Injury
• No standard definition with unknown incidence
• Mechanism - Same as before
• Presentation - CP, SOB, Sinus tach, cardiac ectopy/dysrythmia, hypotension
Mechanism
• Significant Chest Trauma
• Pain and Tenderness over the Mid-anterior Chest
• Sternal Fracture
• Mech (rollover, high speed, fatality at scene)
Mechanism for Blunt Cardiac Injury?�Physical Findings? Seat Belt Sign?

5/27/10
33
Data?
• Single ECG vs Serial ECGs?
• Troponins? - Biffl vs Rajan
• Biffl - Useless, and screening ECG best test
• Rajan - Elevated Trop at 6h correlated with increased risk for dysrhythmia and low EF
• No clear standard
What to do?
• Screen with ECG = pain or tenderness over anterior Chest, sternal fracture, history of cardiac disease (accident precipitated by cardiac dysfunction, major mechanism)
• ECG - persistent tachycardia, new bundle branch block or dysrhythmia
• Abnormality = ECHO (valvular, septum or ventricular wall injury) for low output
Treatment
• Persistent Tachycardia - Look for other signs of hemorrhage (chest, abdomen, etc.)
• High-grade Dysrhythmia - ECHO and ? treatment via ACLS
• My Case

5/27/10
34
Normal Low EF
Function?
Blunt Cardiac Injury
• Mechanism + pain = screening ECG
• 4-6 hour Trop?
• Bedside ECHO may be useful
• Remember to look for Non-cardiac causes

5/27/10
35
Blunt Diaphragmatic Injuries
• Incidence = low (1%) with increasing rates secondary to more sensitive CT
• Left (80%) > Right (20%)
• Right = 50% liver injury
Mechanism
• High Impact MVC
• Head on collision
• >30cm intrusion
• rapid deceleration >40mph
Other Injuries
• Spleen and Liver
• Clinical - epigastric/abdominal pain, referred shoulder pain, SOB, vomiting, dysphagia, etc
• Least Urgent injury in Multiple Trauma
5/27/10
36
Diagnosis • CXR - 50% sensitive
• Specific = NGT or Viscera in Chest
• Nonspecific = atelectasis, pleural effusion, loss of contour, hemo/pneumo
• MDCT - increasing with coronal and sagittal recons (not 100% sensitive)
• Thoracoscopy/Laproscopy - TOC
CT data for diaphragmatic injury?
Normal
Abnormal
Specific, Not Sensitive!

5/27/10
37
Associations
• Treat - NGT decompression
• Look for other associated injuries
• Very Difficult Diagnosis - Missed Often
Blunt Aortic Injury
• 80% die on scene
• Tear usually at the Isthmus (just distal to left subclavian artery)
• Can be very subtle in those that reach the ED
• Pseudocoarctation - Elevated BP in UE and lower BP in lower extermities
difficult
data any associations? cxr findings? how sensitive? ed treatment - BP control
Mechanism
• Fall 10 feet
• MVC > 40 mph
• Any blunt trauma with rapid deceleration
• Crush Injuries

5/27/10
38
Presentation
• Chest Wall tenderness
• Other Skeletal Injuries
• Mechanism should be the trigger
• Associated Injuries Common
CXR
• Widened Mediastinum
• Deviation of NG Tube
• Apical Capping
• Depressed Left Main Stem Bronchus
• Widened Paratracheal Stripe
• Loss of Aortic Knob Contour
Widened Mediastinum
• No exact Widths (no consensus)
• CXR (especially supine AP) cannot “rule out” the disease
• Mechanism and associated injuries should trigger further investigation

5/27/10
39
Imaging
• Newer generation MDCT = 100% sensitivity
• TEE - useful, but impractical
• TTE - not sensitive (no data)
• Maintain High Clinical Suspicion
• Associated Injuries
Treatment • Prevent propagation of adventitial
dissection by reducing wall stress
• Decrease HR = Esmolol
• Decreasing Blood Pressure = nitroprusside or nitrglycerin
• *diltiazem if beta blocker contraindicated
• Goal = SBP 100mmHg
dose?
Review

5/27/10
40
Penetrating Chest Trauma
Unstable Stable
ED Thoracotomy
MDCT
Full Examination
“B” before “A”
ECHO
ECHO
Blunt
1. Lost Pulses - EDT 2. Pneumo - Needle vs Thorocostomy 3. Hemo - Thorocostomy 4. Pericardial Effusion -Pericardiocentesis vs EDT
ABC
Persistent Hypo or Blood Loss
OR Thoracotomy
MDCT
Secondary Survey CXR?
“B” before “A”
Done
Not Stable
MDCT
Improved
????
Stable
ABC
MDCT
Secondary Survey
Done
Normal CXR Normal US low Mech
High Mechanism Abn US
Diaphragmatic Injuries Cardiac Contusion

5/27/10
41
Summary
• Look for occult Associated Injuries
• Use Ultrasound
• Neg CT does not rule out all disease
END