thrombosis of the cranial vena cava in a cow with ... · 1 1 thrombosis of the cranial vena cava in...
TRANSCRIPT

Zurich Open Repository andArchiveUniversity of ZurichMain LibraryStrickhofstrasse 39CH-8057 Zurichwww.zora.uzh.ch
Year: 2011
Thrombosis of the cranial vena cava in a cow with bronchopneumonia andtraumatic reticuloperitonitis
Gerspach, Christian; Wirz, Mirjam; Knubben-Schweizer, Gabriela; Braun, Ueli
Abstract: This paper reports the clinical findings, surgical and medical management, and necropsy ofa 6 year old cow with thrombosis of the cranial vena cava and thrombo embolic pneumonia followingtraumatic reticuloperitonitis. The clinical diagnosis was confirmed by necropsy. Thrombosis of the caudalvena cava is a well known disorder of cattle, whereas thrombosis of the cranial vena cava is relativelyuncommon (1-7). Liver abscesses that break into the caudal vena cava are the most common cause ofthrombosis of the vessel (3,8). Thrombosis of the cranial vena cava is usually attributable to embolismof a jugular vein thrombus and is less often due to haematogenous spread of infection (6). Thrombosisof the vena cava is often associated with metastatic bronchopneumonia with characteristic clinical signs.Wyssmann (1), Breeze (9) and Bueno (10) described respiratory syndrome and signs of congestion incattle with thrombosis of the cranial vena cava. This case report describes the clinical findings in asix-year-old Swiss Braunvieh cow with thrombosis of the cranial vena cava.
Posted at the Zurich Open Repository and Archive, University of ZurichZORA URL: https://doi.org/10.5167/uzh-56078Journal ArticleAccepted Version
Originally published at:Gerspach, Christian; Wirz, Mirjam; Knubben-Schweizer, Gabriela; Braun, Ueli (2011). Thrombosis ofthe cranial vena cava in a cow with bronchopneumonia and traumatic reticuloperitonitis. CanadianVeterinary Journal, 52(11):1228-1231.

1
Thrombosis of the cranial vena cava in a cow with 1 bronchopneumonia and traumatic reticuloperitonitis 2 3 C. Gerspach, M. Wirz, G. Schweizer-Knubben, U. Braun 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
C. Gerspach, DrMedVet., G. Schweizer-Knubben, DrMedVet., U. 36
Braun, DrMedVet., Department of Farm Animals, M. Wirz, MedVet, 37
Institute of Veterinary Pathology, University of Zurich, 38
Winterthurerstrasse 260, CH-8057 Zurich 39
2
Abstract 40
This paper reports the clinical findings, surgical and medical management, and 41
necropsy of a 6 year old cow with thrombosis of the cranial vena cava and thrombo-42
embolic pneumonia following traumatic reticuloperitonitis. The clinical diagnosis was 43
confirmed by necropsy. 44
45
Thrombosis of the caudal vena cava is a well known disorder of cattle, whereas 46
thrombosis of the cranial vena cava is relatively uncommon (1-7). Liver abscesses 47
that break into the caudal vena cava are the most common cause of thrombosis of 48
the vessel (3,8). Thrombosis of the cranial vena cava is usually attributable to 49
embolism of a jugular vein thrombus and is less often due to haematogenous spread 50
of infection (6). Thrombosis of the vena cava is often associated with metastatic 51
bronchopneumonia with characteristic clinical signs. Wyssmann (1), Breeze (9) and 52
Bueno (10) described respiratory syndrome and signs of congestion in cattle with 53
thrombosis of the cranial vena cava. 54
This case report describes the clinical findings in a six-year-old Swiss Braunvieh cow 55
with thrombosis of the cranial vena cava. 56
57
Case description 58
The cow had calved three months ago. Three weeks ago she had a reduced appetite 59
and was treated by the referring veterinarian with a magnet and procaine penicillin 60
because of suspected traumatic reticuloperitonitis. There was a transient response to 61
treatment, but two weeks later milk production decreased and rumination ceased. 62
She was then referred to the Department of Farm Animals, University of Zurich, for 63
further diagnostic work-up. 64

3
The general condition and mental status of the cow were markedly abnormal, the 65
cow was depressed. The cow had a body condition score of 3/5. The rectal 66
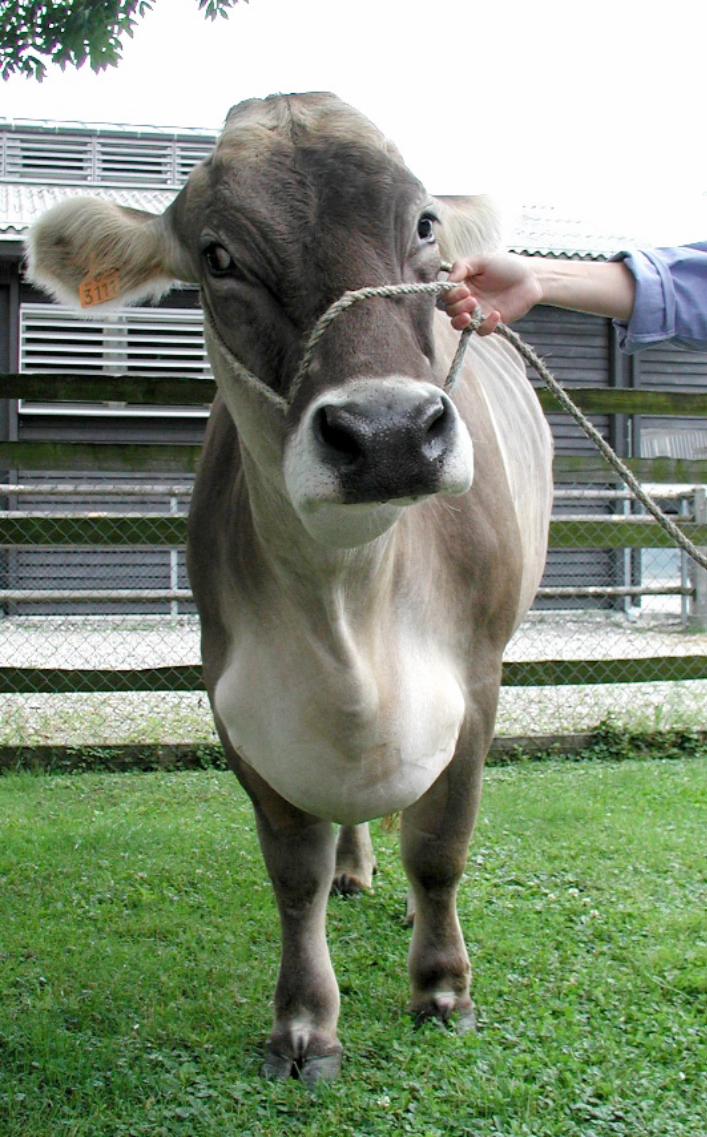
temperature was 38.7 °C, and the heart rate was 108 bpm. Both jugular veins were 67
distended and there was brisket edema (Fig. 1). The respiratory rate was 48 68
breaths/minute, and the cow had abdominal breathing and coughed spontaneously. 69
Auscultation of the lungs revealed increased breath sounds. Ruminal motility was 70
slightly decreased with two contractions per three minutes, and there was a reduced 71
amount of ruminal content. The withers’ pinch, pole test and deep palpation of the 72
cranio-ventral abdomen were consistently positive, and the glutaraldehyde test was 73
shorter than normal at 3 minutes (normal > 10 minutes). 74
Further diagnostic work-up included haematological and biochemical analyses and 75
ultrasonographic examination of the lungs (11), heart (12), reticulum (13), liver (14) 76
and abdomen (15). Radiographs of the lungs and reticulum were also taken (16). 77
The most important haematological and biochemical findings were an increase in the 78
concentrations of total protein at 84 g/l (normal 60-80 g/l) and fibrinogen at 8 g/l 79
(normal 4-7 g/l) and increased activities of glutamate dehydrogenase at 39.1 U/l 80
(normal 0-25 U/l), sorbit dehydrogenase at 37.2 U/l (normal 0-20 U/l) and γ-glutamyl 81
transferase at 41 U/l (normal 0-20 U/l). The albumin concentration was normal (29 82
g/l; normal 21-36 g/l). 83
Ultrasonographic examination of the reticulum (13) showed one weak incomplete 84
contraction per 3-minute period (normal, 3 complete biphasic contractions per 3-85
minute period). Echogenic fibrin deposits containing pockets of hypoechogenic fluid 86
were seen on the reticular wall and extended from the left to right side of the 87
abdomen and from the ventral abdomen to the level of the elbows. An 11-cm 88
abscess with a hypoechogenic centre surrounded by an echogenic capsule was 89

4
seen caudal to the reticulum. Fibrin deposits were seen on the ventral margin of the 90
liver. The pleura had comet-tail artefacts on both sides of the thorax, and a layer of 91
anechoic fluid with a diameter of 1 cm was seen between the visceral and parietal 92
pleura on the right side. The heart valves, liver parenchyma, caudal vena cava, 93
portal vein and gallbladder were unremarkable. Transcutaneous, ultrasound-guided 94
biopsy of the liver was done because of the elevation in liver enzyme activity; 95
histological evaluation of the sample did not reveal pathologic changes. 96
On laterolateral radiographs of the thorax the lungs, caudal cardiac silhouette and 97
caudal vena cava were clearly seen. A non-delineated soft-tissue opacity was seen 98
in the caudoventral lung field, and the dorsal lung area appeared normal. This finding 99
was interpreted as localised pneumonia. Radiographs of the reticulum revealed two 100
magnets on the ventral aspect of the reticulum. One magnet had two linear foreign 101
bodies, one of which appeared to be at an angle to the magnet and possibly 102
penetrating the reticular wall. There was localised loss of detail in the region of the 103
caudal reticular contour. 104
Traumatic reticuloperitonitis and bronchopneumonia were diagnosed based on all 105
the findings. The cause of distension of both jugular veins was suspected to be 106
obstruction of the cranial vena cava by a thrombus or compression of the vein by a 107
mass. Cardiac insufficiency was ruled out based on echocardiography. 108
The albumin concentration was normal, therefore a low oncotic pressure as a cause 109
of edema could be ruled out. 110
The owner requested a laparotomy, since the cow was valuable. 111
A laparorumenotomy was performed using a standart laparotomy incision in the left 112
paralumbar fossa. Anesthesia of the paralumbar fossa and abdominal wall was 113

5
achieved by a proximal paravertebral nerve block. Prior to the rumenotomy an 114
abdominal exploratory was performed. 115
The ruminotomy was performed using a Weingarth’s ring. 116
The exploratory revealed massive adhesions involving the spleen, reticulum, cranial 117
blind sac of the rumen, omasum and those parts of the liver that could be palpated 118
from the left flank incision. Two magnets with a 7.5-cm nail and loop of wire were 119
removed from the reticulum. An abscess, which was palpated on the caudomedial 120
wall of the reticulum, was lanced and drained into the reticulum and lavaged with an 121
iodine solution (Betadine). 122
Postoperative treatment consisted of 10 litres of 0.9 % saline with 5 % glucose 123
administered intravenously daily, 1.2 x 106 IU/100 kg procaine penicillin (Procacillin) 124
administered IM every eight hours and 1.1 mg/kg flunixin meglumine (Fluniximine) 125
administered intravenously every 24 hours for 3 days. 126
Four days postoperatively, there was marked worsening of the brisket oedema (Fig 127
2) and development of mandibular oedema and swelling of the nose. In order to rule 128
out an allergic etiology of the swelling of the nose, the cow was given 2.5 mg 129
flumethasone (Cortival) IV every 24 hours and 50 mg/100 kg tripelenamine 130
(Vetibenzamin) IM once. Oedema of the front limbs and ventral abdomen (Fig 3) 131
developed seven days postoperatively. Ultrasonographic examination of the thorax 132
revealed severe pleural and pericardial effusion. Thoracocentesis yielded a 133
transudate with a specific gravity of 1.010 and no measurable protein. 134
Based on these findings, thrombosis of the cranial vena cava was suspected and the 135
cow was given 45,000 IU heparin IV every eight hours and 1 mg/kg furosemide 136
(Dimazon) intravenously for three days. However, over the following three days, the 137
oedema worsened, breathing became laboured when the cow was recumbent, and 138
6
there was intermittent mouth breathing. Because of a poor prognosis and failure to 139
respond to treatment, the cow was euthanased. A postmortem examination was 140
carried out. 141
Postmortem examination confirmed the ultrasonographic diagnosis of massive 142
adhesions involving the reticulum. A friable, beige, rough, 8 cm x 3 cm thrombus was 143
fully occluding the lumen of the cranial vena cava (Fig 3). Histopathology of the 144
thrombus revealed gram positive (Brown-Brenn staining) coccoid bacteria. Culture 145
of the thrombus has not been performed. 146
The walls of the right atrium and ventricle of the heart were thicker than normal at 1 147
cm. The pericardial sac contained 100 ml of light red watery fluid. On cut surface, the 148
pulmonary vessels contained several friable rough structures, up to 2 cm in length 149
(Fig 4). The pulmonary parenchyma surrounding these areas was yellow. Culture of 150
these lung lesions revealed Streptococcus ssp. 151
The hepatic bile ducts contained massive numbers of small liver flukes. Specimens 152
of the lungs, kidneys and thrombus in the cranial vena cava were examined 153
histologically. Based on the findings, the cow was diagnosed with thrombosis of the 154
cranial vena cava, severe multifocal necrotising pneumonia with multiple pulmonary 155
thrombi, ischemic renal infarction, Dicrocoelium dentriticum infestation and localised 156
peritonitis in the region of the reticulum. 157
158
Discussion 159
Our patient had signs of thrombosis of the cranial vena cava. The differential 160
diagnosis for sudden distension of both jugular veins includes obstruction of the 161
cranial vena cava by a thrombus, compression of the vein by a mass and cardiac 162
insufficiency. Because the cow had an elevated heart rate, echocardiography was 163

7
carried out and pericarditis, cardiomyopathy and endocarditis were ruled out. 164
However, it was not possible to determine clinically whether there was obstruction or 165
compression of the cranial vena cava. Radiography and ultrasonography showed no 166
evidence of compression of the vein by a space-occupying lesion. Thus, obstruction 167
of the cranial vena cava with a thrombus, which has been described in cattle 168
(1,9,10), was diagnosed by exclusion of the other differential diagnoses. 169
In principle, thrombi, which result from increased coagulation or reduced blood 170
flow, are differentiated from thrombi, which are attributable to suppurative 171
inflammation. Wyssmann (1) described a thrombus, which was determined to be 172
associated with a reticular abscess based on histological evaluation. In the present 173
case, the thrombus causing distension of both jugular veins and impaired venous 174
return with resultant oedema of the head and neck region was suspected to be 175
septic based on histopathology. 176
The most common cause of thrombosis of the cranial vena cava is 177
thrombophlebitis of the jugular vein (6). Septic emboli may also originate from other 178
foci of infection, including mastitis, endometritis and claw disease (6,17). The most 179
common pathogens are Fusobacterium necrophorum and Actinomyces pyogenes, 180
but staphylococcus spp., streptococcus spp. and Escherichia coli may also be 181
cultured from thrombi in the vena cava (18). No abnormalities were found on 182
ultrasonographic examination of the jugular veins in our patient. The most likely 183
source of infection was traumatic reticuloperitonitis with abscessation of the reticular 184
wall. Peritonitis, mainly in the reticular region, in conjunction with thrombosis of the 185
cranial vena cava was also described by Bueno (10) and Wyssmann (1). It is 186
plausible that bacteria from the traumatic reticuloperitonitis were transported via the 187
cranial epigastric and internal thoracic veins to the cranial vena cava. 188

8
The cow also had severe multifocal necrotising pneumonia with formation of multiple 189
pulmonary thrombi. Metastatic bronchopneumonia caused by embolisation of part of 190
a thrombus in the vena cava has been described (2,3,5,6,9). The clinical signs of 191
thrombosis of the caudal vena cava and its sequelae are described as respiratory 192
syndrome attributable to metastatic pneumonia, pulmonary thromboembolism or 193
embolic pulmonary aneurysm (17). Selman (2) and Breeze (9) described respiratory 194
syndrome due to thrombosis of the caudal vena cava and cranial vena cava, 195
respectively. Pulmonary thrombi may lead to aneurysm and rupture of the vessel 196
with subsequent epistaxis and sudden death. The lung lesions in the present case 197
were consistent with thromboembolism. The most likely source for septic emboli 198
traveling to the lungs was the septic thrombus in the cranial vena cava. A similar 199
organism cultured from different lesions could prove that these lesions were related. 200
Streptococcus ssp. could be cultured from the lung lesions, but no culture was 201
performed from the thrombus in this case. However, histopathology of the thrombus 202
revealed gram positive coccoid bacteria. 203
The clinical signs in our patient were attributable to oedema of the head and 204
neck. Bueno (10) and Wyssmann (1) also described brisket and mandibular edema 205
and bilateral jugular vein distension in cattle with thrombosis of the cranial vena 206
cava. Oedema was not a clinical feature in the patient described by Breeze (9). 207
However, all affected cattle had respiratory signs (1,9,10). 208
In human medicine, congestion of the cranial vena cava is usually the result of 209
compression of the vessel, which in more than 80 per cent of patients is attributable 210
to a malignant tumour (65% bronchial carcinoma). The lead sign in human patients is 211
oedema of the head and neck (19). To the authors’ knowledge, compression of the 212
cranial vena cava causing congestion has not been reported in cattle. 213
9
Ultrasonography is an important diagnostic tool for assessment of the vena 214
cava. Diagnosis of thrombosis of the vena cava directly by visualisation of the 215
thrombus (7,20) or indirectly by identification of dilatation of the caudal vena cava in 216
the region of the liver (5,21) is rare. A definitive diagnosis of thrombosis of the cranial 217
vena cava can only be achieved by direct visualisation of the thrombus via 218
ultrasonography. Bueno et al. (10) detected a thrombus visible within the right atrial 219
lumen, extending into the cranial vena cava. However, we were not able to detect a 220
thrombus in our patient. This was probably due to insufficient penetration into the 221
thorax and lack of access to the cranial thorax because the examination area is 222
delimited by the caudal margin of the thoracic limb. The cranial vena cava originates 223
from the right atrium, traveling through the mediastinum to the thoracic inlet, where it 224
bifurcates into the jugular veins. The cranial vena cava is covered by the lung lobes 225
cranial to the heart. The vein can only be imaged adjacent to the heart. 226
227
228
229
230
231
Authors’ contributions 232
Drs. Gerspach, Schweizer-Knubben, and Braun were the clinicians responsible for 233
the case and described clinical and ultrasonographic findings and Dr. Wirz 234
performed the necropsy and described the pathological findings. 235

10
236
237
238
239
240
References 241
1. Wyssmann E. Thrombose der vorderen Hohlvene mit enormem Stauungsödem 242 beim Rind. Schweizer Archiv für Tierheilkunde 1932;74:285-290. 243
244 2. Selman IE, Wiseman A, Petrie L, Pirie HM, Breeze RG. Respiratory syndrome in 245
cattle resulting from thrombosis of posterior vena-cava. Vet Rec 1974;94:459-246 466. 247
248 3. Rebhun WC, Rendano VT, Dill SG, King JM, Pearson EG Caudal vena-caval 249
thrombosis in 4 cattle with acute dyspnea. J Am Vet Med Assoc 1980;176:1366-250 1369. 251
252 4. Mills L, Pace W. Caudal vena-caval thrombosis in a cow. J Am Vet Med Assoc 253
1990;196:1294-1296. 254 255 5. Braun U, Schefer U, Gerber D, Föhn J. Ultrasonographic Findings in a Cow with 256
Ascites Due to Thrombosis of the Caudal Vena-Cava. Schweiz Arch Tierheilkd 257 1992;134:235-241. 258
259 6. Braun U. Krankheiten der Kreislauforgane und des Blutes In: Innere Medizin und 260
Chirurgie des Rindes. 4th ed. Berlin and Hamburg: Paul Parey Verlag, 2002:194-261 197. 262
263 7. Braun U, Salis F, Gerspach C. Sonographic evidence of an echogenic thrombus 264
in the Vena cava caudalis in a cow. Schweiz Arch Tierheilkd 2003; 145:340-341. 265 266 8. Gudmundson J, Radostits OM, Doige CE. Pulmonary thromboembolism in cattle 267
due to thrombosis of posterior vena-cava associated with hepatic abscessation. 268 Canadian Vet Journal1978;19(11):304-309. 269
270 9. Beeze RG.Thrombosis of Cranial Vena-Cava in a Cow. Vet. Rec. 1977;101:130-271
131. 272 273 10. Bueno AC, Watrous BJ, Parker JE, Hedstrom OR. Ultrasonographic diagnosis: 274
Cranial vena cava thrombosis in a cow. Vet Radiol Ultrasound 2000;41:551-553. 275 276 11. Braun U, Sicher D, Pusterla N. Ultrasonography of the lungs, pleura, and 277
mediastinum in healthy cows. Am J Vet Res1996;57:432-438. 278 279 12. Braun U, Schweizer G, Pusterla N. Echocardiography of the normal bovine heart: 280
technique and ultrasonographic appearance. Vet Rec 2001;148:47-51. 281 282

11
13. Braun U, Goetz M. Ultrasonography of the reticulum in cows. Am J Vet Res 283 1994:55:325-332. 284
285 14. Braun U. Ultrasonographic examination of the liver cows. Am J Vet Res 286
1990;51:1522-1526. 287 288 15. Braun U. Atlas und Lehrbuch der Ultraschalldiagnostik beim Rind. Berlin: Parey 289 Buchverlag; 1997. 290 291 16. Braun U, Flückiger M, Naegeli F. Radiography as an aid in the diagnosis of 292
traumatic reticuloperitonitis in cattle. Vet Rec 1993; 132:103-109. 293 294 17. Smith J. Disorders of the organ systems In: Large Animal Internal Medicine. 4th 295
ed. St. Louis: Mosby, 2009:660-661. 296 297 18. kawa H, Narushima T, Kohno T. Bacteriology of caudal vena-caval thrombosis in 298 slaughter cattle. Vet Rec 1987;120:184-186. 299 300 19. Dempke W. Diagnostisches und therapeuthisches Management der oberen 301
Einflussstauung. Medizinische Klinik 1999;94:681-684. 302 303 20. Mohamed T, Sato H, Kurosawa T, Kawa S. Ultrasonographic localisation of 304
thrombi in the caudal vena cava and hepatic veins in a heifer. Vet J 305 2004;168:103-106. 306
307 21. Braun U, Flückiger M, Feige K. Pospischil A. Diagnosis by ultrasonography of 308
congestion of the caudal vena cava secondary to thrombosis in 12 cows. Vet Rec 309 2002;150:209-213. 310
311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 330 331 332

12
333 334 335 336 337 338 339 340 Figure legents 341
342 Figure 1 343 Physical appearance of the cow with brisket edema. 344 345 346 Figure 2 347 Physical appearance of the cow with distended jugular veins and brisket edema 348 349 Figure 3 350 Anatomical appearance of a friable, beige, rough, 8 cm x 3 cm thrombus from the 351 cranial vena cava, bar = 1 cm. 352 353 Figure 4 354 Anatomical appearance of a thrombus within a pulmonary vessel, bar = 1 cm. 355 356 357