thumbs up/thumbs down – feb 2003 allhat allhat: optimal first-step therapy for hypertension eric j...
TRANSCRIPT

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT: Optimal first-step therapy for hypertension
Eric J Topol MDProvost and Chief Academic OfficerChairman, Department of Cardiovascular MedicineThe Cleveland Clinic FoundationCleveland, OH
Robert M Califf MDProfessor of MedicineAssociate Vice Chancellor for Clinical ResearchDirector, Duke Clinical Research InstituteDuke University Medical CenterDurham, NC

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Randomized designof ALLHAT
High-risk hypertensive patients
Consent / Randomize
(42 418)
AmlodipineChlorthalidoneDoxazosinLisinopril
Eligible for lipid-lowering
Not eligible for lipid-lowering
Consent / Randomize (10 355)
Pravastatin Usual care
Follow for CHD and other outcomes until death or end of study (up to 8 yrs).

Thumbs up/Thumbs down – Feb 2003
ALLHAT
A horse race
Each class of antihypertensive is represented by a drug, and the losers drop out as events are accrued
Primary end point: fatal CHD or nonfatal MI
All major clinical end points were measured in minimal detail
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Secondary drug protocol
Step 2 agents: Dose 1* Dose 2* Dose 3*
Reserpine 0.05 qdor 0.1 qod
0.1 qd 0.2 qd
Clonidine (oral) 0.1 bid 0.2 bid 0.3 bid
Atenolol 25 qd 50 qd 100 qd
Step 3 agent:
Hydralazine 25 bid 50 bid 100 bid
*All doses in mg

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT: Trial design
•42 418 patients age >55 with hypertension and 1 additional risk factor
•623 sites:
United States
Canada
Puerto Rico
US Virgin Islands
Thumbs up/Thumbs down – Feb 2003
ALLHAT
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0 1 2 3 4
Cu
mu
lati
ve e
ve
nt
rate
Years of Follow-up
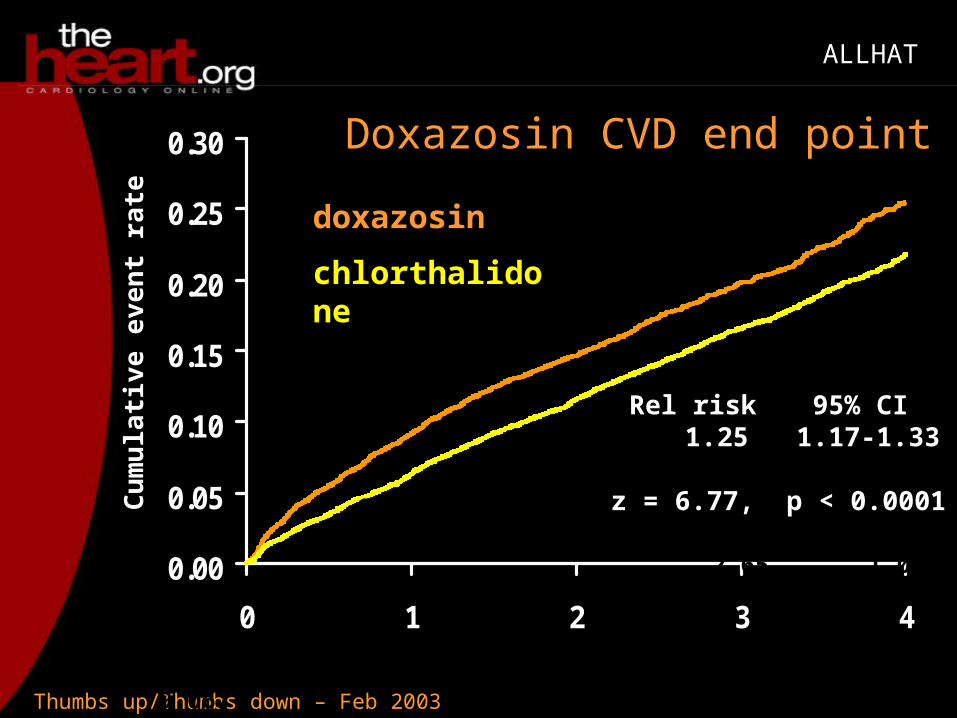
doxazosin
chlorthalidone
C: 15,268D: 9,067
12,990 7,382
9,4435,285
4,8272,654
2,0101,083
Rel risk 1.25
z = 6.77, p < 0.0001
95% CI1.17-1.33
JAMA. 2000;283:1967-1975
Doxazosin CVD end point

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
ALLHAT: Primary end point
0.0
2.0
4.0
6.0
8.0
10.0
12.0
Events
(%
)
Chlorthalidone Lisinopril Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
Lisinopril secondary end points
0
1
2
3
4
5
6
7
8
9
6-y
ear
even
t ra
te
(per
10
0 p
ers
on
s)
Heart failure Stroke
Chlorthalidone Lisinopril

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
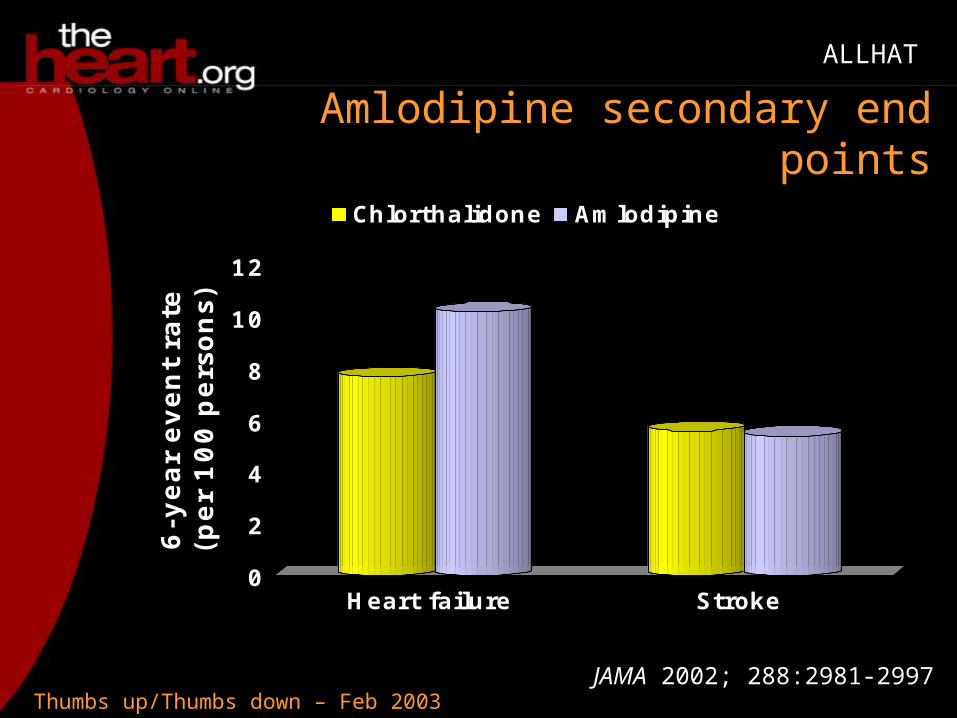
Amlodipine secondary end points
0
2
4
6
8
10
12
6-y
ear
even
t ra
te
(per
10
0 p
ers
on
s)
Heart failure Stroke
Chlorthalidone Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
ALLHAT: Fasting glucose levels
0
5
10
15
20
25
30
35
Fasti
ng g
lucose >
126 m
g/dL (
%)
Baseline 2 years 4 years
Chlorthalidone Lisinopril Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Stroke risk: Lisinopril vs chlorthalidone
Subgroup Relative risk 95% CI
Nonblack 1.00 0.85-1.17
Black 1.40 1.17-1.68
JAMA 2002; 288:2981-2997

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
ALLHAT: Glomerular filtration rate
60626466687072747678
Fil
trati
on r
ate
m
L/
min
per
1.7
3
sq m
Baseline 2 years 4 years
Chlorthalidone Lisinopril Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT-LLT: Primary results
0
2
4
6
8
10
12
14
16
6-y
ear
even
t ra
te/
100 p
ati
en
ts
Mortality CHD and nonfatal MI
Pravastatin Usual care
JAMA 2002; 288:2998-3007

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT-LLT: Disappointing
Second largest statin trial after HPS
"[It's] disappointing that it didn't provide true consistency and only with this bouillabaisse pooling stuff do you get the same relative effect."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT: Points of contention
Why did lisinopril increase heart failure and stroke?
This is directly opposite of the results from HOPE
PEACE and EUROPA are looking at ACE inhibitors as a key preventive tactic
"This backfired terribly in ALLHAT."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Active control trial
The other drugs were only less effective than the diuretic, not increasing risks for the patients
The "soft underbelly" of HOPE was whether the patients were being adequately treated with regard to their other risk factors
If EUROPA and PEACE are negative, either HOPE was wrong or ramipril is "a magic potion"
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Using less ramipril
I've gone from requiring ramipril use to making it optional
"I think we have to say this is a piece of data that moves back toward less radical enthusiasm about the ACE-inhibitor class."
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
ALLHAT: Blood pressure
125
130
135
140
145
150
0 1 2 3 4 5
Years
Systo
lic B
P (
mm
Hg
)Chlorthalidone Lisinopril Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Genetics of hypertension
Studies suggest the genetic defect of essential hypertension alpha —adducin Gly460Trp would be particularly responsive to thiazide diuretic
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Stroke risk: Lisinopril vs chlorthalidone
Subgroup Relative risk 95% CI
Nonblack 1.00 0.85-1.17
Black 1.40 1.17-1.68
JAMA 2002; 288:2981-2997

Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
ALLHAT: Blood pressure
125
130
135
140
145
150
0 1 2 3 4 5
Years
Systo
lic B
P (
mm
Hg
)Chlorthalidone Lisinopril Amlodipine
Thumbs up/Thumbs down – Feb 2003
ALLHAT
JAMA 2002; 288:2981-2997
Amlodipine secondary end points
0
2
4
6
8
10
12
6-y
ear
even
t ra
te
(per
10
0 p
ers
on
s)
Heart failure Stroke
Chlorthalidone Amlodipine

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Edema or heart failure?
There was no objective measure of function to diagnose heart failure
A substudy was commissioned to have records independently reviewed
All the results are not in, but so far the substudy suggests that there is more than just edema going on
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Surprising increase in heart failure
The increase in heart failure for both classes of drugs (ACE inhibitor and CCB) was a very surprising finding
• Lisinopril 19% increased risk
• Amlodipine 38% increased risk
"You would have thought both drugs would not have done this."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Bad choice of second drug
Critics say the second drug after ACE inhibitor would be a diuretic, forbidden by the trial
Most doctors in the US probably don't use a diuretic as the second drug
"I think no matter how you slice the loaf here the answer is that the underused diuretics, which are a lot cheaper, are at least as good and almost certainly better."
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
A class effect?
Most doctors use hydrochlorothiazide as a diuretic
This could be a chlorthalidone-specific result, you can't be sure
"We have examples where drugs in the same class don't get the same results."
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Striking secondary outcomes
The media loved that a cheaper drug came out better
I wasn't enthusiastic about the trial when I was on the NIH advisory committee reviewing the trial
"The secondary outcomes made for all the spice here. If you were
to just go by the primary outcome, though, you wouldn't be able to differentiate the treatments."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Public health
Why not use a cheaper drug that is just as good? It's a dominant treatment
A company trying to get labelling with this primary outcome might have trouble getting approval from the FDA
"We have examples where drugs in the same class don't get the same results."
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
An easy choice
There is a value judgment being made among the secondary outcomes
"I think the majority of people, if you said, 'Look, I can give you this thing for 2 cents a day, or I can give you this thing for a buck and a half a day, and here are the expected outcomes, which would you buy?' I don't think that's a hard choice."
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Inadequate treatment
"None of these drugs are very good, they all have some untoward effects, unfortunately. You're picking your poison in some respects."
This study reinforces that there is inadequate treatment of blood pressure.
"A lot of people are walking around with very high blood pressure still, despite therapy." Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Lowering blood pressure
"I think that people that are most critical of doctors trying to lower blood pressure are people that have never actually worked in a clinic trying to get blood pressure down."
It takes the doctor and patient working together to get blood pressure down
We usually need more than 2 drugs
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Genomics approach to hypertension
Genomics will allow us to move past the trial and error approach
"$37 billion a year it costs to treat hypertension and we're not
even doing a very good job of doing it. We've got to have a better strategy and almost any strategy would be better than what we have today."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Interpersonal approach
People will round numbers down for patients who are frustrated at not getting hypertension under control to avoid adding more drugs drugs
Lowering blood pressure is very complicated and interpersonal
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Two thumbs up
Topol: "Don't you think this is as good as it gets for hypertension and clinical trials?"
• Two thumbs up
Califf: "I think it's as good as it gets."
• Two thumbs up

Thumbs up/Thumbs down – Feb 2003
ALLHAT
A new approach
"The system we have now, where companies not only fund trials but decide what the questions are is not the right way to do it"
Doctors and patients want to know which is the best choice among the treatments that work?
Most companies avoid head-to-head trials and try to game them even when they agree
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Honest broker
NIH or other agencies as an honest broker is the model to pursue in the future
"If a drug is a winner it ought to prevail in a direct comparison without the type of
engineering that can occur with interested sponsors."
Topol

Thumbs up/Thumbs down – Feb 2003
ALLHAT
Pricing
The price of a drug should be a function of how much it contributes
"The way it is now, people are having to decide what to take and what to buy without any knowledge in many fields of which one is really better."
In multiple sclerosis, for example, there are 4 drugs and no one knows which is really better
Califf

Thumbs up/Thumbs down – Feb 2003
ALLHAT
ALLHAT: Optimal first-step therapy for hypertension
Eric J Topol MDProvost and Chief Academic OfficerChairman, Department of Cardiovascular MedicineThe Cleveland Clinic FoundationCleveland, OH
Robert M Califf MDProfessor of MedicineAssociate Vice Chancellor for Clinical ResearchDirector, Duke Clinical Research InstituteDuke University Medical CenterDurham, NC