thursday, january 11, 2018 adhd: facts and myths · thursday, january 11, 2018. title goes here ......
TRANSCRIPT

ADHD: Facts and MythsPanelists:
Cheryl Chase, Ph.D.
Stephen Grcevich, M.D.
Moderator: Kelly M. Christian, Ph.D.
Thursday, January 11, 2018

Title Goes Here
ADHD: Facts and Myths
Part II
Ethan D. Schafer Center
at
Lawrence School
January 11,2018
2

Cheryl Ann Chase, PhDClinical PsychologistIndependence, Ohio
ChasingYourPotential.com
Facebook: https://business.facebook.com/ChasingYourPotential/
Twitter: @DrCherylChase
3

ADHD
Attention-Deficit/Hyperactivity Disorder
Diagnostic criteria from the
Diagnostic and Statistical manual of Mental Disorders
– 5th edition (DMS-5)
© 2013
4

INATTENTIVE SYMPTOMS
1) Six (or more) of the following have persisted for at least 6 months to a degree that is inconsistent with developmental level and negatively impacts directly on social and academic/occupational activities:
a. Fails to give close attention to details or makes careless mistakes.
b. Has difficulty sustaining attention.
c. Does not appear to listen.
d. Struggles to follow through on instructions.
e. Has difficulty with organization.
f. Avoids or dislikes tasks requiring a lot of thinking.
g. Loses things.
h. Is easily distracted.
i. Is forgetful in daily activities.
5

HYPERACTIVE/IMPULSIVE SYMPTOMS
2) Six (or more) of the following have persisted for at least 6 months to a degree that is inconsistent with developmental level and negatively impacts directly on social and academic/occupational activities:
a. Fidgets with hands or feet or squirms in chair.
b. Has difficulty remaining seated.
c. Runs about or climbs excessively in children; extreme restlessness in adults.
d. Difficulty engaging in activities quietly.
e. Acts as if driven by a motor; adults will often feel inside like they were driven by a motor.
f. Talks excessively.
g. Blurts out answers before questions have been completed.
h. Difficulty waiting or taking turns.
i. Interrupts or intrudes upon others.
6

Developmental considerations
Always think: relative to same-age peers!
• Preschool – normal is very broad. What else could be
going on?? Need a good developmental assessment.
Rule out sensory issues, language delays, etc. But it IS
possible to diagnose in preschool.
• Elementary – early years – what are the demands? Are
they realistic and developmentally appropriate?
• High-School – Can be complicated by other things.
Don’t overlook mood issues – not everything is ADHD!
Watch for more inattentive, more restless. For individuals
17 and above only 5 or more symptoms are needed.
• Adulthood – executive skills, restless. Yes, it persists in the
majority of cases, but the functional impact may be
less.7

2 Big things to remember when teaching a
child who contends with ADHD
8

1) Reduce cognitive load !!!!!!!
• Oral instructions simple and short
• Lessons brief
• Allow time for processing and rehearsal
• One task at a time (not notetaking and listening)
• Quiet environment
• Direct instruction with repetition. Repetition. Repeat
• Nonessential, irrelevant or confusing info omitted
• Present steps just before they are needed
• Present visually and verbally
• Be organized and clear.
9

2) Externalize everything and post
at the point of performance!!!!!
10

• Use mnemonics and strategies and post them
• Visual reminders
• Frequently misspelled words
• Classroom rules
• Letter formations
• Steps in a process
• Number line
• Have a strategy wall
11

Classroom Accommodations
Barkley’s 9 principles
1. Rules and instructions provided to children with ADHD must
be clear, brief, and often delivered through more visible and
external modes of presentation than is required for the
management of non-ADHD children.
2. Consequences used to manage the behavior of children
with ADHD must be delivered swiftly and more immediately
than is needed for non-ADHD children.
3. Consequences must be delivered more frequently, not just
more immediately, to children with ADHD in view of their
motivational deficits.
4. The type of consequences used with children with ADHD
must be of a higher magnitude, or more powerful, than that needed to manage the behavior of non-ADHD children
12

5. An appropriate and often richer degree of incentives must be provided within a setting or task to reinforce appropriate behavior before punishment can be implemented.
6. Those reinforces or particular rewards which are employed must be changed or rotated more frequently with children with ADHD than with non-ADHD children given the penchant of the former for more rapid habituation or satiation to response consequences, apparently rewards in particular.
7. Anticipation is the key with children with ADHD.
8. Children with ADHD must be held more ‘publicly’ accountable for their behavior and goal-attainment than non-ADHD children.
9. Behavioral interventions, while successful, only work while they are being implemented and, even then, require continued monitoring and modification over time for maximal effectiveness.
13

Behavior Management
• Behavior modification; NOT traditional talk therapy
or play therapy
• Goal is to get child doing more desired behavior
and less undesired behavior – but do NOT use to
bully the child
• Use rewards and punishments – but mostly rewards
• Put in terms of ABC’s
– Antecedents – things that happen before
– Behaviors – things the child does
– Consequences – things that happen after the behavior
• Adults learn to change A’s and C’s
14
• Parent and teacher interventions should be carried
out at the same time with communication between
the two
• Five points to incorporate into both components:
– Start with goals that the child can achieve in small steps
– Keep it simple – don’t try to change too much at once
– Be consistent – across times of day, settings, people
(specials teachers, too)
– Implement behavior interventions over the long haul – not just a few months
– Expect to have to freshen-it-up regularly
15

• Target behaviors can be either negative behaviors
that need to stop OR new skills that need to be
developed
• The areas targeted will typically not be the
symptoms of ADHD – but rather the specific
problems that those symptoms cause in every-day
life
– “completes assigned work with 80% accuracy”
– “plays well with siblings”
– “does what he is told first of second time told it”
16

Conclusions
“The treatment of ADHD requires a comprehensive behavioral, psychological, educational, and sometimes
medical evaluation followed by education of the individual or their family members as to the nature of the
disorder and the methods proven to assist with its management. Treatment is likely to be multidisciplinary,
requiring the assistance of the mental health, educational, and medical professions at various points in its course. Treatment must be provided over long time periods to assist those with ADHD in the ongoing management of
their disorder. In doing so, many with the disorder can lead satisfactory, reasonably adjusted, and productive lives.”
-russellbarkley.org/content/adhd-facts.pdf
17

ADHD Facts and Myths
An Interactive Discussion for Parents and Professionals
Stephen Grcevich, MD
President, Family Center by the Falls, Chagrin Falls OH
Clinical Associate Professor of Psychiatry, NEOMED
President and Founder, Key Ministry
The Ethan D. Schafer Center at Lawrence School
January 11, 201818

Is the need to treat a product of cultural expectations?
“It is our culture that disables.”
“When one is disabled, the problem is not
really that they have impairments and social
skill deficits. The issue at stake is that they
live in an ‘ableist’ culture that rarely affords
them the space or opportunity to make their
unique contribution to society”
Ben Conner - Amplifying Our Witness (2012)
19
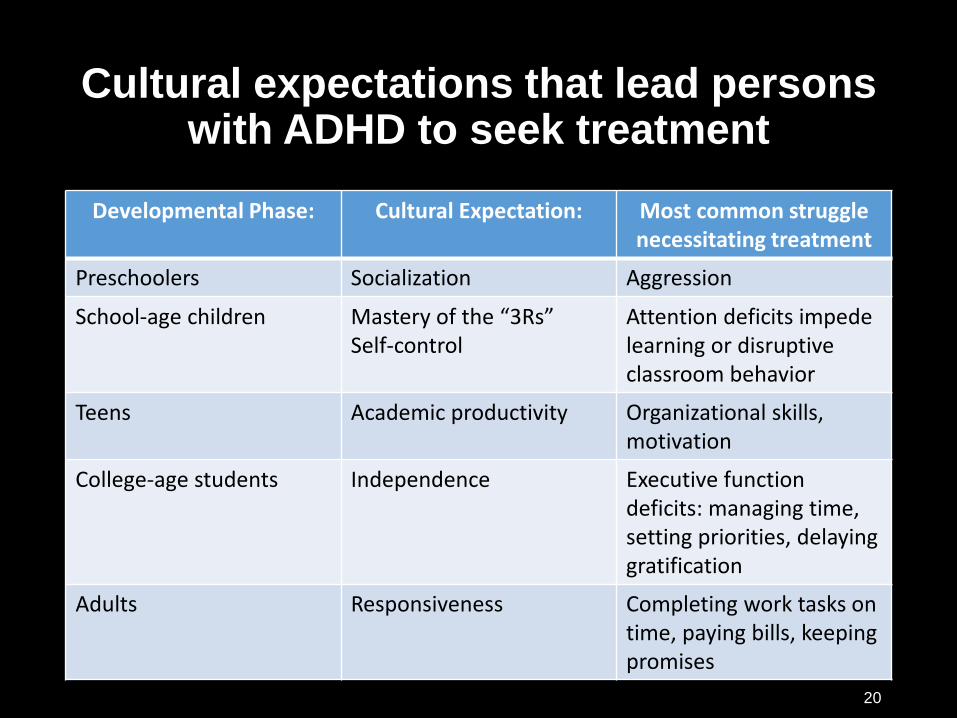
Cultural expectations that lead persons with ADHD to seek treatment
Developmental Phase: Cultural Expectation: Most common struggle necessitating treatment
Preschoolers Socialization Aggression
School-age children Mastery of the “3Rs”Self-control
Attention deficits impede learning or disruptive classroom behavior
Teens Academic productivity Organizational skills, motivation
College-age students Independence Executive function deficits: managing time, setting priorities, delaying gratification
Adults Responsiveness Completing work tasks on time, paying bills, keeping promises
20

Adults with
ADHD
Adolescents
with ADHD
ADHD: A Lifelong Disorder
Children
with ADHD
Prevalence in juvenile population
6%-11%
Prevalence in adult
population 3%-5%
40-50%
persists
into
adulthood
75%
persists
into
adolescence
Wilens TE. Psychiatr Clin North Am. 2004;27:283-301. 21

Preschool
School-age
Adolescence
College-age
Adult
• Disruptive behavior
• Academic failure
• Poor socialization
• Self-esteem issues
• Injuries
• Low self-esteem
• Smoking
• Substance use
• Crime
• Car accidents
• Academic failure
• Occupational failure
• Substance abuse
• Relationship failures
• Poor work history
• Chronic substance
abuse and dependence
• Incarceration
ADHD impairment across the lifespan…
Slide courtesy of Joseph Biederman, MD. 22

ADHD in College
• High school very difficult for kids with ADHD• Many classes irrelevant, uninteresting
• Duration of school day/time for activities
• Need to study in evening
• College classes/major selected on basis of interest
• Shorter duration of time in class, fewer classes
• Most colleges will accommodate
• Biggest challenges: • Too much free time
• Self-discipline to study
• Need to self-advocate
23

Executive functioning-the fundamental difference in persons with ADHD?
• Executive functions…cognitive abilities involved in controlling and regulating other abilities and behaviors
• Necessary in initiating goal-directed behavior, regulating emotions, delaying gratification, planning future behavior
• Children with weaknesses in executive functioning have more difficulty foreseeing outcomes of behavior, adapting to new situations.
Hathaway WL, Barkley RA. J Psychol Christianity 2003, 22(2) 101-114
24

Key executive functions:
• Behavioral inhibition
• Verbal working memory
• Non-verbal working memory
• Emotional self-regulation
• Reconstitution
Hathaway WL, Barkley RA. J Psychol Christianity 2003, 22(2) 101-11425
What I’m looking at in an evaluation…
• Interview with parent(s), caregivers
• Interview with child
• Report cards, online grades
• Standardized testing
• School records (MFE/ETR, IEP, correspondence)
• Screening for common comorbid conditions
• Rating scales for ADHD, other conditions
26

Catecholamine Mechanisms in ADHD
Posterior Parietal Cortex
Prefrontal Cortex
Striatum
Sensoryinput
Cerebellum
LocusCoeruleus
VTA
SubstantiaNigra
NE enhances relevant signal
NE enhances relevant signal
DA suppresses irrelevant signal
Posner MI, et al. Images of Mind. 1st ed. New York, NY: Scientific American Library; 1997. 27
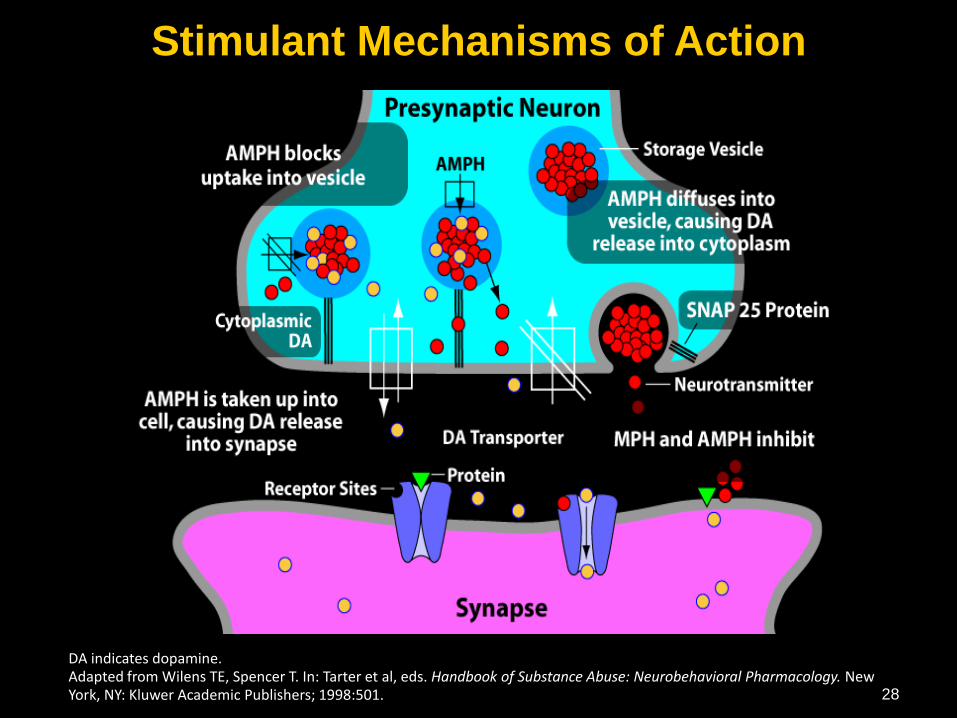
DA indicates dopamine.Adapted from Wilens TE, Spencer T. In: Tarter et al, eds. Handbook of Substance Abuse: Neurobehavioral Pharmacology. New York, NY: Kluwer Academic Publishers; 1998:501.
Stimulant Mechanisms of Action
28

Do stimulants cause long term changes in brain function?
Wang G-J, Volkow ND, Wigal T, Kollins SH, Newcorn JH, et al. (2013) PLoS ONE 8(5): e63023. doi:10.1371/journal.pone.0063023
29

Implication of long-term stimulant use
• Up-regulation of DA transporter protein in caudate, putamen, ventral striatum
• Decreased DA signaling could lead to worsening of ADHD symptoms when patients aren’t taking medication
• Why we don’t generally see tolerance to stimulants used to treat ADHD
30

Presynaptic Neuron
Synapse
Atomoxetine (Strattera®)Mechanism of Action
NE Receptors
Dopamine
Norepinephrine (NE)
NE Transporter
Postsynaptic Neuron
Atomoxetine
Kratochvil CJ et al. Expert Opin Pharmacother. 2003;4(7):1165-74
31

35
25
29 28
33
21
811 11
66
32
15
0
10
20
30
40
50
60
70
%
Comorbidity in Pediatric ADHD
Lifetime Prevalence of Comorbid Conditions in
Pediatric Population With ADHD
Biederman J. J Clin Psychiatry. 2004;65(suppl 3):3-7.
Boys (N = 140)Girls (N = 140)
ODD EnuresisMajor
Depression
Multiple(>2)
Anxiety
Conduct Disorder
Bipolar Disorder
32
Treatment considerations in ADHD…
• Medication is most effective stand-alone treatment
• Evidence stronger for parent or teacher administered behavior therapy in school-age children than in teens
• Appropriate school-based accommodations, special education services as indicated
• Need to address other comorbid conditions
• Behavior therapy recommended as initial treatment in preschoolers
33

Evidence for non-traditional treatments for ADHD
• Omega-3s: statistically significant, but modest effects
• Restrictive diets: helpful for subset of kids with ADHD and food allergies
• Iron deficiency correlated to AMP dose
• Neurofeedback: difficult to create true “placebo” group
• Vision therapy: not substantiated
• CogMed: ineffective in one randomized trial
34

The MTA Study(Multimodal Treatment Study of ADHD)
• NIMH sponsored, multi-site
• 579 children (ages 7 – 9.9)
• 4 treatment groups:
• State-of-the-art medication
• Intensive behavioral intervention
• Combination medication + behavioral
• Community treatment (usual care)
MTA Cooperative Group. Arch Gen Psychiatry. 1999;56:1073-1086.35

Long-Term Outcomes of Therapies for ADHD in the MTA Study
Hyperactive Impulsive Symptoms
(Teacher Reports)
0
10
20
30
40
50
60
70
Medication
Management
Combination
Therapy
(medication +
behavior therapy)
Behavior
Therapy
Community-based
Therapy
Imp
rove
me
nt
at
14
mo
nth
s (
%)
65
55
45
35
15
5
56%60%
45%
36%
25
MTA Cooperative Group. Arch Gen Psychiatry. 1999;56:1073-1086.36

1.5
1
0.5
0
Composite Index
ADHD-only
w/DBD w/Both
w/Anxiety
Behavior Medication Combination
DBD=disruptive behavioral disorder
Jensen et al. J Am Acad Child Adolesc Psychiatry 2001: 40:147.
Comorbidity in the MTA:Response to TreatmentE
ffect
siz
e
37

Factors to consider in selecting medication for ADHD patients:
• What will be the right drug?
• In the right dose?
• With the right duration of action?
• And the right delivery system?
Other Considerations: • Side effect and safety issues
• Cost/availability
Grcevich S. Future Neurology 2006; 1(5) 525-534 38

41.2
78.2
15.6
3.70.9 1.8
0
20
40
60
80
1 1-3 4-6 7-9 10-11 12+
27.4
53.3
19.3
12
6.29.1
0
20
40
60
80
1 1-3 4-6 7-9 10-11 12+
Pat
ien
ts (
%)
Prescriptions FilledOffice Visits
Rate of Office Visits and Prescription Fills Over 12-Month Study Period:
A B
Data shown are the rate (%) of patients with the indicated number of office visits or prescriptions filled over the 12-month study period.
Pat
ien
ts (
%)
Grcevich S et al. Presented at American Academy of Child and Adolescent Psychiatry Annual Meeting, San Diego, October 200639

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sep-03 Oct-03 Nov-03 Dec-03 Jan-04 Feb-04 Mar-04 Apr-04 May-04 Jun-04 Jul-04 Aug-04
OROS-MPH CategoryCapone N, et al. Presented at the CHADD International Conference (2005) Dallas, TX.
Monthly Persistence With OROS-MPH (N=2398)%
of
Pati
en
ts
40

Capone N, et al. Presented at the CHADD International Conference (2005) Dallas, TX.
Monthly Persistence With MAS-XR (N=1626)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sep-03 Oct-03 Nov-03 Dec-03
MAS-XR Category
Jan-04 Feb-04 Mar-04 Apr-04 May-04 Jun-04 Jul-04 Aug-04
% o
f P
ati
en
ts
41

Revised TMAP algorithm for ADHD pharmacotherapy…
• Consensus conference of academic clinicians and researchers, practicing clinicians, administrators, consumers, families
• Revised algorithms based upon new research developed for treatment of ADHD, with and without common comorbid conditions
• Children treated according to earlier algorithms achieved better outcomes and were exposed to less polypharmacy than controls
Pliszka SR et al. J Am Acad Child Adolesc Psychiatry 2006; 45(6) 642-657Pliszka SR et al. J Am Acad Child Adolesc Psychiatry 2003; 42 279-287 42

TMAP algorithm for pharmacologic management of ADHD:
Pliszka SR et al. J Am Acad Child Adolesc Psychiatry 2006: 45(6) 642-65743

Medication Treatment for ADHD
Approved Not Approved
Non-Stimulant
Intuniv
Kapvay
Strattera
IR Clonidine
IR Guanfacine (Tenex)
Nuvigil/Provigil
Tricyclics
Venlafaxine (Effexor)
Wellbutrin
Stimulants
Amphetamine
Short Acting Long ActingIntermediate
Adderall
Desoxyn
Dexedrine
Dextrostat
Evekeo
Zenzedi
Dexedrine Spansule†
Adderall‡
Adderall XR
Adzenys XR ODT
Dexedrine Spansules
Dynavel XR
Vyvanse
Methylphenidate
Short Acting Long ActingIntermediate
Ritalin
Focalin
Methylin
Ritalin SR
Metadate ER
Aptenzio XR
Concerta
Daytrana (patch)
Focalin XR
Metadate CD/ER
Methylin ER
Quillivant/Quillichew
Ritalin LA/SR
44

Meta-analysis of ADHD Medications
Drug Effect Size
Amphetamine 0.92
Methylphenidate 0.80
Atomoxetine 0.73
Modafinil 0.49
Buproprion 0.32
Faraone SV, Spencer TJ: American Psychiatric Association, Toronto, Canada, May 2006.
(29 controlled studies over 25 years, 4465 children, adolescents)
45

Differential Response to Stimulants
Arnold LE. J Atten Disord. 2000;3:200-211.
0
10
20
30
40
50
Be
st re
sp
on
se
(%)
Meta-Analysis of Within-subject Comparative Trials
Evaluating Response to Stimulant Medications
AMP=amphetamine MPH=methylphenidate
AMP MPH Equal response to either stimulant
28%
16%
41%
46

Implications of Arnold Study:
• Patients with uncomplicated ADHD should try another stimulant from the alternate category if they fail an initial trial.
• Sub-optimal responders (improved, but not normalized) to a stimulant may also benefit from a trial of a different stimulant from the alternate category.
47

Dosing issues:
• Start with small doses, increase in small, weekly increments
• One week sufficient to assess response
• Poor ”community care” response in MTA often attributed to insufficient dosing
• Beneficial effects, side effects are dose-dependent
• Differences in response common with generics considered “equivalent” by FDA
• Stimulants aren’t dosed on the basis of weight…non-stimulants are.
• Response to stimulants is highly individualized
48

The right drug delivery system:
• Pills, patches, liquids, chewables
• How soon does the product work?
• When during the day does maximum benefit occur?
• How often does the patient need to take it?
49

Analog classroom study of Focalin XR: Impact upon math performance
Turnbow JM et al. US Psychiatric and Mental Health Conference; 2005; Las Vegas, NV
Change From Predose in Number of Math Problems Correctly Solved
-30
-20
-10
0
10
20
30
40
50
60
70
0 0.5 1 2 3 4 5 6 7 8 9 10 11 12
Focalin XR Placebo
-30
-20
-10
0
10
20
30
40
50
60
70
0 0.5 1 2 3 4 5 6 7 8 9 10 11 12
Me
an
Ch
an
ge F
rom
Pre
do
se
,M
ath
Co
rre
ct
Hours Postdose
*
**
**
** *
**
*
**
Imp
rove
me
nt
50

Analog classroom study of OROS MPH:Impact upon math performance
0
5
10
15
20
25
30
35
40
45
50
8:15 9:20 10:30 12:30 14:05 16:00 17:15 18:20 19:10
Placebo
OROS MPH (all doses)
TID MPH (all doses)
Class period
Change in number of math problems completed
Pelham WE et al. Pediatrics 2001; 107(6) e105.51

Laboratory Classroom Mean Change from Pre-Dose in Number of
Math Problems Correct
Analog classroom study of Transdermal MPH: Impact upon math performance
-20
-15
-10
-5
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5 6 7 8 9 10 11 12
Time (hr)
Mean
Ch
an
ge S
co
re
Placebo
Transdermal MPH
Patch applied Patch removed
Wigal et al. Poster presented at the AACAP Annual Meeting, Toronto. October 21, 2005.
Imp
rove
me
nt
* P < .001 Transdermal MPH vs placebo at all measured post-dose time points.
*
*
**
* *
**
N=79
52

Duration of action:
• Extracurricular activities, homework, driving renders concept of school or work day coverage obsolete
• Why do patients tell you extended-release stimulants don’t last as long as they should?
• Needs may be different for college students, adults.
53

40
50
60
70
80
90
100
110
120
130
140
0 1.5 3 4.5 6 7.5 9 10.5 12
Adderall XR
Academic Productivity:
Time post dose (hr)
Placebo Adderall™ 10 mg ADD XR 30 mgADD XR 10 mg ADD XR 20 mg
McCracken et al. Presented at AACAP; October 26, 2000; New York.
Number of Math Problems Completed Correctly
54

Medication controversies in ADHD
55

Side effect, safety issues:
• Cardiovascular safety: sudden death, heart rate, BP
• Effects upon growth
• Relationship to substance abuse risk
• Other long-term consequences?
• Management of effects upon appetite, sleep
56

Sudden Death Overview in Children and Adolescents on
Stimulants:• Rate in children, adolescents:
AMP: 0.36/1,000,000 RX
MPH: 0.16/1,000,000 RX (difference is non-significant)
• Background rate in pediatric population: 1.3-8.5/100,000 patient years (more common in males than females)
• FDA Pediatric Advisory Committee recommended against boxed warnings for stimulants
Liberthson RR. New England Journal of Medicine 1996:(334) 1039-1044Meeting of the FDA Pediatric Advisory Committee, Washington DC, March 22, 2006
57

Sudden death overview in adults on stimulants:
• Rate in adults:
AMP: 0.53/1,000,000 RX
MPH: 0.07/1,000,000 RX (difference is non-significant)
• Background rate in adult population: 1-2/1000 patient years
• 3 of 5 deaths in adult patients occurred in individuals over 40 with preexisting HTN (coronary artery disease and dysrhythmia was a pre-existing condition in one case)
• More data needed to evaluate risk in patients over 40 with HTN, preexisting cardiovascular disease, obesity
Janse MJ. Pharmacol and Therapeutics 2003(100) 89-99Cardiovascular Safety Review, Office of Drug Safety , February 9, 2006 (www.fda.gov)
58

Screening for Cardiac Risk: American Heart Association Guidelines
• Medical history
• History of congenital or acquired cardiac disease
• Family history of or premature cardiac disease (<30 years of
age)
• Palpitations, chest pain, syncope, seizures, post-exercise
symptoms
• Ask about other medications (including OTC)
• Routine medical exam
• Monitor blood pressure & pulse at baseline and follow-up
• No need for baseline ECG, Holter, ECHO in children
• Adults: Work-up as medically indicated
• Suspicion of CV defect (e.g., idiopathic hypertrophic sub-aortic
stenosis): work-up as indicated
Gutgesell H et al. Circulation. 1999:99:979-982. 59

Hypertension and ADHD medication in adults
• Cardiovascular data from five controlled studies (MPH, MAS-XR, pemoline, buproprion, desipramine)
• Stimulants and non-stimulants associated with increases in heart rate, blood pressure
• Also common on placebo
• New-onset systolic or diastolic hypertension (BP>140/90)
• 10% of patients on active drug• 8% on placebo
• Baseline HR and BP measurement, along with periodic monitoring is recommended in adults
Wilens TE, Hammerness PG, Biederman J et al. J Clin Psychiatry 2005:66(2) 253-25960

Cardiovascular effects of stimulants in kids
• Amphetamine, atomoxetine associated with, small, statistically significant changes in heart rate, systolic, diastolic BP
• Methylphenidate associated with significant increase in systolic BP
• No difference in severity of effects between treatments
• Long term significance unclear
Hennissen, L., Bakker, M.J., Banaschewski, T. et al. CNS Drugs (2017) 31: 199. doi:10.1007/s40263-017-0410-7 61

Effects on Stature: MTA
• Statistically, but not clinically significant differences in height, weight
• Effects appear primarily in first 12-18 months
• Kids with ADHD experience growth spurts later than peers
• Group averages at 14 months (end of MTA study):• Gain in height:
• Medical management only: 4.75 cm• Behavioral therapy only: 6.19 cm• Variance: –1.44 cm/14 months (= –1.23 cm/year)
• Gain in weight:• Medical management only: 1.64 kg• Behavioral therapy only: 4.53 kg• Variance: –2.89 kg/14 months (= –2.48 kg/year)
MTA Cooperative Group. Pediatrics. 2004;113:762-769. 62

ADHD and Substance Abuse
• ADHD is a significant risk factor for substance abuse disorders in teens, adults
• Medication during adolescence may reduce risk, but protective effects disappear by age 25
• Smoking• Adults with ADHD smoke more, experience more
difficulty quitting
• Children with ADHD start younger, smoke more
Biederman et al. Pediatrics. 1999;104:e20. Pomerleau et al. J Subst Abuse. 1995;7:373-378.Milberger et al. J Am Acad Child Adolesc Psychiatry. 1997;36:37-44. 63

Trends in stimulant misuse, abuse
• Rate of stimulant misuse, diversion calculated at 2.0%
• Statistically significant reduction in misuse, diversion of stimulants (p<0.01) between 2002 and 2004
• Reduction in abuse rates corresponds to time period during which use of extended release products was rapidly expanding
• Misuse rates at college proportional to mean SAT scores of incoming freshman class
2004 National Survey on Drug Use and Health, DHHS Publication #SMA 05-4062
McCabe SE et al. Addiction, 99, 96–106 64

Stimulants and rebound effects:
• Rate: 8.6% vs 1.9% on placebo (Adderall XR)
• Possible causes
• Fatigue factor
• Hypoglycemia
• Comorbid anxiety
• Patients with anxiety/OCD often experience more irritability on stimulants-decreased distractibility may intensify anxiety awareness
Biederman J et al. Pediatrics (2002) 110:258-266
Swanson JM et al. J Am Acad Child Adolesc Psychiatry (1998) 37:519-526
Grcevich S. Future Neurology. 2006; 1(5) 525-53465

Do stimulants cause long term changes in brain function?
Wang G-J, Volkow ND, Wigal T, Kollins SH, Newcorn JH, et al. (2013) PLoS ONE 8(5): e63023. doi:10.1371/journal.pone.0063023
• Study examined long-term changes in DA transporter in never-treated adults with ADHD after 12 months on Concerta vs. controls
• 24% increase in DA transporter in caudate and putamen after 12 months (significant)
• Does long term use of ADHD medication make ADHD symptoms worse when medication is stopped?
• More studies needed of other medications, impact upon functional impairment
66

Drug Holidays
• Recommended by many pediatricians, especially during summer months
• Driven by concerns that kids aren’t eating enough, achieving expected growth
• Often driven by difficulty tolerating stimulant-related side effects
• Does ADHD significantly impact functioning in one or more major life domains (school/work, family, friends, community) during weekends, vacation?
67

Managing stimulant-related side effects:
• Appetite/weight: • Eat Breakfast• Encourage small snacks throughout day • Bedtime snacks replace missing lunchtime calories
• Sleep: • Limit access to electronics before bed• Melatonin (3-6 mg, two hours before bedtime)• Consider adjusting duration of medication coverage• Adjunctive clonidine
• Irritability: • Evaluate for comorbid conditions• Consider “dose-sculpting” in late afternoon• Consider alternative medication
• Most stimulant related side effects resolve within three months of treatment initiation
McGough JJ et al. J Am Acad Child Adolesc Psychiatry (2005) 44:530-538 68

Helpful Resources
• AACAP ADHD Resource Center https://www.aacap.org/aacap/families_and_youth/resource_centers/adhd_resource_center/Home.aspx
• Russell Barkley lecture on ADHD and neurodevelopment, UC Davis MIND Institute https://www.youtube.com/watch?v=q3d1SwUXMc0
• How are children and teens with ADHD different? (Article by Stephen Grcevich, MD) http://www.keyministry.org/church4everychild/2016/4/3/how-are-kids-and-teens-with-adhd-different?rq=ADHD
69

Stay in Touch!• Family Center by the Falls:
• Phone (440) 543-3400, Web: http://www.fcbtf.com
• Key Ministry: • Phone: (216) 970-0974, Web: http://www.keyministry.org
https://www.facebook.com/fcbtf/
https://www.facebook.com/keyministry/
https://www.facebook.com/NotAloneParents/
@drgrcevich
@keyministry
70