thyroidectomy- operative surgery
TRANSCRIPT

THYROIDECTOMY
DR.B.Selvaraj MS; Mch; FICS;
Professor of Surgery
Melaka Manipal Medical College
Melaka 75150 Malaysia
OPERATIVE SURGERY

THYROIDECTOMY
• INDICATIONS:
- Thyroid malignancies
- Multinodular goiter
- Graves’ disease
• ANESTHESIA:
- GA-(ET)
• POSITION:
- Semi-fowler’s position with neck hyperextension
• Pre-op preparation for surgery:
- Investigations like TFT, FNAC, USG thyroid, Thyroid scintigraphy and bone scan
- Never use iodine containing contrasts
- If patient is hyperthyroid bring to euthyroid state with anti-thyroid drugs and propranolol
- Give Lugol’s iodine from 10 days prior to surgery to diminish vascularity
- Exclude MEN sydromes

THYROIDECTOMY
• POSITIONING
- Semi-fowler’s position
- Pillow in between scapulae to hyperextend neck on a headrest
- Protect eyes
• DRAPPING- Double towel for head
-Expose cranially mandible,
caudally suprasternal notch, laterally
sternomastoid muscles
-Silk thread to imprint incision

THYROIDECTOMY
• Skin incision & division of platysma
- Kocher’s low collar incision
- Subdermal platysma muscle incision
• Mobilisation of upper & lower flaps- Skin with platysma flaps mobilised
cranially upto thyroid cartilage- upper flap
- Lower flap mobilised caudally upto
suprasternal notch

THYROIDECTOMY
• Ligation of anterior jugular veins
- The superficial anterior jugular veins are suture ligated and divided
• Division of strap muscles &
pretracheal fascia- Divide the strap muscles in the middle
- Incise the pre tracheal fascia
- Dissect laterally in between the
pretracheal fascia(false capsule) and true
capsule of thyroid gland

THYROIDECTOMY
• Mobilisation of lateral lobe and ligation of middle thyroid vein
- Mobilise the lateral part of a lobe
- Ligate and divide middle thyroid vein
• Exposure of superior pedicle & it’s
division- Clamp, divide and transfix the superior
pedicle as close to the gland as possible
- Nowadays Harmonic scalpel has been
used
THYROIDECTOMY
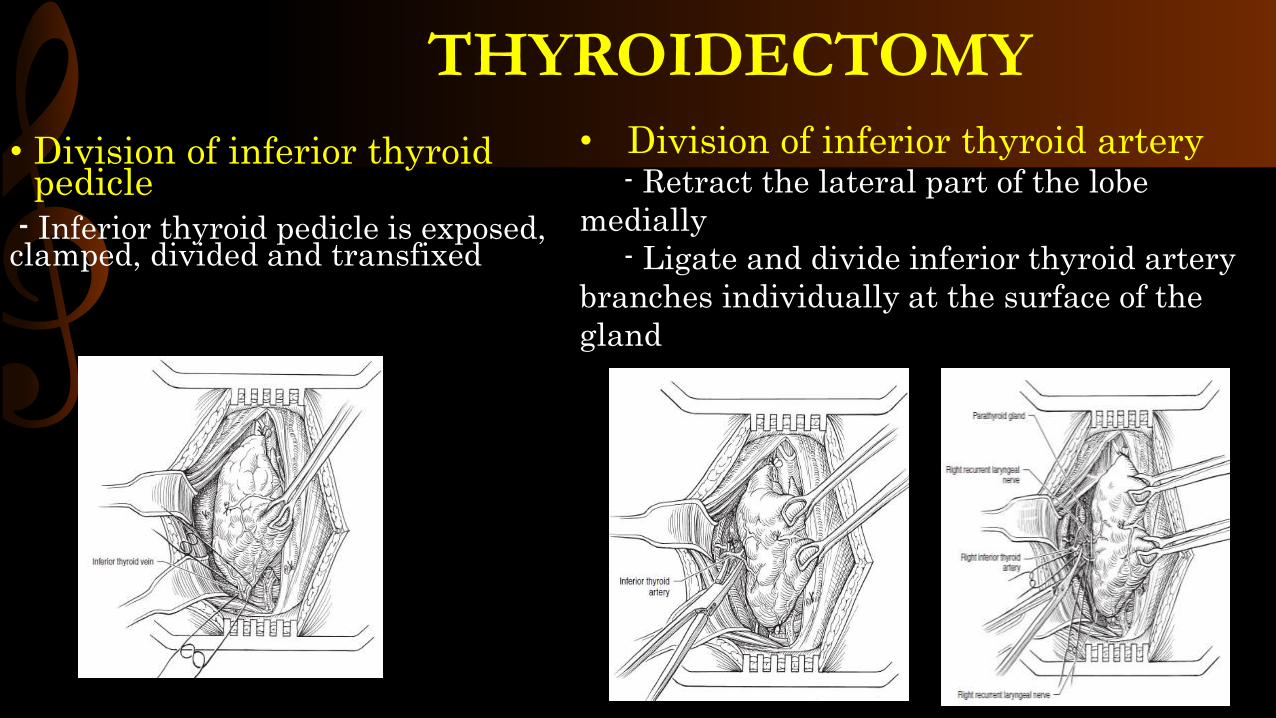
• Division of inferior thyroid pedicle
- Inferior thyroid pedicle is exposed, clamped, divided and transfixed
• Division of inferior thyroid artery- Retract the lateral part of the lobe
medially
- Ligate and divide inferior thyroid artery
branches individually at the surface of the
gland

THYROIDECTOMY• Separation from anterior
tracheal aspect
- Division of Berry’s ligament allows the thyroid to be mobilized medially
- Dissection of the thyroid from the trachea can then be performed with the electrocautery
• For Hemithyroidectomy- If lobectomy is indicated, then the
isthmus is clamped using a Kocher or
tonsil clamp, divided, and oversewn with
an interlocking continuous 3-0 Vicryl
suture

THYROIDECTOMY• For Total Thyroidectomy
- If total thyroidectomy is indicated, the operation is continued in a similar fashion on the other side to remove the thyroid gland in toto
- Preserve parathyroids and recurrent laryngeal nerves
• For Subtotal Thyroidectomy- Perform a subtotal resection if operating
for benign disease, thus preserving the
parathyroid glands and not dissecting in
the area of the recurrent laryngeal nerves.
-The line of resection on the thyroid lobe to
preserve this rim of thyroid tissue overlying
the parathyroid glands is shown in Fig

THYROIDECTOMY
- Once resection is completed and hemostasis is ensured, closure is performed by first reapproximatingthe strap muscles at the midline using interrupted 3-0 Vicrylsutures
CLOSURE OF INCISION
-The platysma muscle is
likewise reapproximated
using interrupted 3-0
Vicryl sutures
-Finally, the skin is
reapproximated with a
subcuticular stitch of
4-0 Monocryl suture
- Keeping a suction
drain is surgeon’s
option

THYROIDECTOMY
• COMPLICATIONS
- Tension hematoma
- Recurrent laryngeal nerve injury
- Superior laryngeal nerve injury
- Hypoparathyroidism
- Hypothyroidism
- Wound infection
- Hypertrophied scar or keloid
• Recent Advances- Endoscopic Thyroidectomy: Bilateral
Axillo-Breast Approach (BABA)
- Axillary port insertion and sharp
dissection with Harmonic. A 12-mm port is
made on the right axilla (marked by star )
