tienam h-a-30-1187 opinion - european...
TRANSCRIPT

Annex I
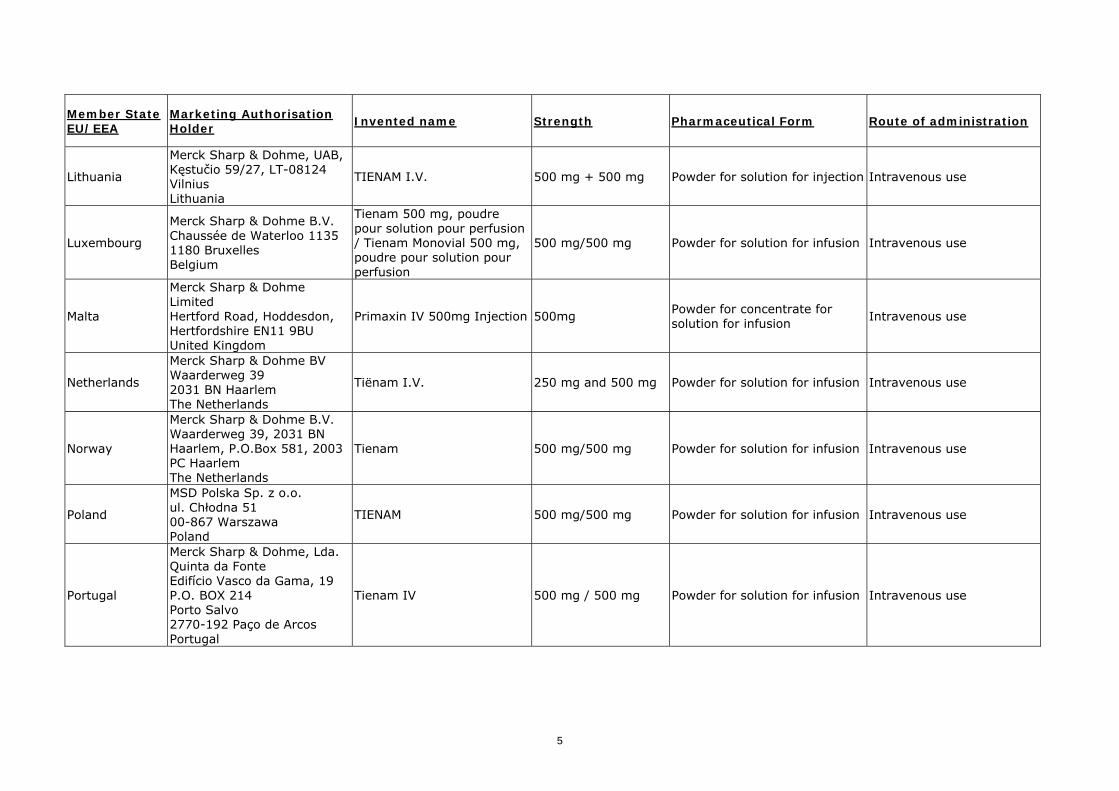
List of the names, pharmaceutical forms, strengths of the medicinal products, routes of administration, marketing authorisation holders in the Member States
1

Member State EU/EEA
Marketing Authorisation Holder
Invented name Strength Pharmaceutical Form Route of administration
Austria
Merck Sharp & Dohme Ges.m.b.H. Am Euro Platz 2 1120 Wien Austria
Zienam 500 mg Trockensubstanz zur Infusionsbereitung
500 mg Powder for solution for infusion Intravenous use
Belgium
Merck Sharp & Dohme B.V. Chaussée de Waterloo 1135 1180 Bruxelles Belgium
Tienam 500 mg, poudre pour solution pour perfusion / Tienam Monovial 500 mg, poudre pour solution pour perfusion
500 mg/500 mg Powder for solution for infusion Intravenous use
Bulgaria
Merck Sharp & Dohme Bulgaria EOOD 55, Nikola Vaptzarov Blvd., Expo 2000 Sofia 1407 Bulgaria
Tienam 500/500 mg powder for solution for infusion Тиенам 500/500 mg прах за инфузионен разтвор
500/500mg Powder for solution for infusion Intravenous use
Czech Republic
Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, The Netherlands
Tienam i.v. 500mg /500mg i.v.
500 mg/500 mg Powder for solution for infusion Intravenous use
Estonia
Merck Sharp & Dohme OÜ Peterburi St 46, 11415 Tallinn Estonia
TIENAM I.V. 500 MG/500 MG 500 mg/500 mg Powder for solution for infusion Intravenous use
Finland
Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, The Netherlands
TIENAM
500 mg/ 500 mg
Powder for solution for infusion Intravenous use
France
Merck Sharp & Dohme Chibret 3 avenue Hoche 75114 Paris cedex 08 France
TIENAM 500 mg/500 mg, poudre pour perfusion avec système de transfert pour poche
500 mg/500 mg Powder for infusion Intravenous use
France
Merck Sharp & Dohme Chibret 3 avenue Hoche 75114 Paris cedex 08 France
TIENAM 250 mg/250 mg, poudre pour perfusion 250 mg/250 mg Powder for infusion Intravenous use
2

Member State EU/EEA
Marketing Authorisation Holder
Invented name Strength Pharmaceutical Form Route of administration
France
Merck Sharp & Dohme Chibret 3 avenue Hoche 75114 Paris cedex 08 France
TIENAM 500 mg/500 mg, poudre pour perfusion 500 mg/500 mg Powder for infusion Intravenous use
France
Merck Sharp & Dohme Chibret 3 avenue Hoche 75114 Paris cedex 08 France
TIENAM 500 mg/500 mg, poudre et solution pour usage parentéral (IM)
500 mg/500 mg Powder for suspension for parenteral use (IM) Intramuscular use
Germany
MSD SHARP & DOHME GMBH Lindenplatz 1 D-85540 Haar Germany
ZIENAM° 500 mg Pulver zur Herstellung einer Infusionslösung
500 mg/500 mg Powder for solution for infusion Intravenous use
Greece
Vianex S.A Tatoiou str. 18th Km Athens-Lamia National Road 14671 Nea Erythrea Greece
Primaxin DR.PD.INJ (500+500)mg/Vial (IV) 500 mg Dry Powder for injection Intravenous use
Greece
Vianex S.A Tatoiou str. 18th Km Athens-Lamia National Road 14671 Nea Erythrea Greece
Primaxin DR.PD.INJ (250+250mg/Vial (IV) 250mg Dry Powder for injection Intravenous use
Hungary
MSD Hungary Ltd. 1123 Budapest, Alkotás u. 50. Hungary
Tienam 500 mg Powder for solution for infusion Intravenous infusion
Iceland
Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, P.O.Box 581, 2003 PC Haarlem The Netherlands
Tienam 500 mg/500 mg Powder for solution for infusion Intravenous infusion
3

Member State EU/EEA
Marketing Authorisation Holder
Invented name Strength Pharmaceutical Form Route of administration
Ireland
Merck Sharp & Dohme Ireland (Human Health) Limited Pelham House South County Business Park Leopardstown Dublin 18 Ireland
Primaxin IV 500mg/500mg Powder for Solution for Infusion
500 mg/500 mg Powder for solution for infusion Intravenous infusion
Italy
Merck Sharp & Dohme (Italia) S.p.A. Via Vitorchiano, 151 – 00189 Roma Italy
TIENAM (20 ml) 500 mg/500 mg Powder for solution for infusion Intravenous infusion
Italy
Merck Sharp & Dohme (Italia) S.p.A. Via Vitorchiano, 151 – 00189 Roma Italy
IMIPEM (20 ml) 500 mg/500 mg Powder for solution for infusion Intravenous infusion
Italy
Sigma-Tau Industrie Farmaceutiche Riunite S.p.A, Viale Shakespeare, 47 00144 Roma Italy
TENACID (20 ml) 500 mg/500 mg Powder for solution for infusion Intravenous infusion
Latvia
SIA "Merck Sharp & Dohme Latvija", Skanstes 13, Riga, LV-1013 Latvia
TIENAM I.V. 500 mg/500 mg Powder for solution for infusion Intravenous use
4
Member State EU/EEA
Marketing Authorisation Holder
Invented name Strength Pharmaceutical Form Route of administration
Lithuania
Merck Sharp & Dohme, UAB, Kęstučio 59/27, LT-08124 Vilnius Lithuania
TIENAM I.V. 500 mg + 500 mg Powder for solution for injection Intravenous use
Luxembourg
Merck Sharp & Dohme B.V. Chaussée de Waterloo 1135 1180 Bruxelles Belgium
Tienam 500 mg, poudre pour solution pour perfusion / Tienam Monovial 500 mg, poudre pour solution pour perfusion
500 mg/500 mg Powder for solution for infusion Intravenous use
Malta
Merck Sharp & Dohme Limited Hertford Road, Hoddesdon, Hertfordshire EN11 9BU United Kingdom
Primaxin IV 500mg Injection 500mg Powder for concentrate for solution for infusion
Intravenous use
Netherlands
Merck Sharp & Dohme BV Waarderweg 39 2031 BN Haarlem The Netherlands
Tiënam I.V. 250 mg and 500 mg Powder for solution for infusion Intravenous use
Norway
Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, P.O.Box 581, 2003 PC Haarlem The Netherlands
Tienam 500 mg/500 mg Powder for solution for infusion Intravenous use
Poland
MSD Polska Sp. z o.o. ul. Chłodna 51 00-867 Warszawa Poland
TIENAM 500 mg/500 mg Powder for solution for infusion Intravenous use
Portugal
Merck Sharp & Dohme, Lda. Quinta da Fonte Edifício Vasco da Gama, 19 P.O. BOX 214 Porto Salvo 2770-192 Paço de Arcos Portugal
Tienam IV 500 mg / 500 mg Powder for solution for infusion Intravenous use
5

6
Member State EU/EEA
Marketing Authorisation Holder
Invented name Strength Pharmaceutical Form Route of administration
Romania
Merck Sharp & Dohme Romania S.R.L. Bucharest Business Park, Şos. Bucureşti-Ploieşti Nr.1A, Clădirea C1, Etaj 3, Sector 1, Bucureşti Romania
TIENAM I.V., pulbere pentru soluţie perfuzabilă 500 mg/500 mg Powder for solution for infusion Intravenous use
Slovak Republic
Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem P.O. Box 581, 2003 PC Haarlem The Netherlands
TIENAM i.v. 500 mg/500 mg Powder for solution for infusion Intravenous use
Slovenia
Merck Sharp & Dohme, inovativna zdravila d.o.o. Šmartinska cesta 140, 1000 Ljubljana, Slovenia
CONET 500 mg/500 mg prašek za raztopino za infundiranje
500 mg/500 mg Powder for solution for infusion Intravenous use
Spain
Merck Sharp & Dohme de España, S.A. C/ Josefa Valcárcel, 38 28027 Madrid Spain
TIENAM I.V. 500 mg powder for solution for infusion 500 mg/500 mg Powder for solution for infusion Intravenous use
Sweden
Merck Sharp & Dohme B.V. Waarderweg 39, Haarlem, P.O.Box 581, 2003 PC Haarlem The Netherlands
Tienam 500 mg/ 500 mg Powder for solution for infusion Intravenous use
United Kingdom
Merck Sharp & Dohme Limited, Hertford Road, Hoddesdon, Herts, EN11 9BU United Kingdom
PrimaxinIV 500mg Injection 500mg Powder for concentrate for solution for infusion Intravenous use

Annex II
Scientific conclusions and grounds for amendment of the summary of product characteristics, labelling and package leaflet presented by the European Medicines Agency
7
Scientific conclusions
Overall summary of the scientific evaluation of Tienam and associated names (see Annex I)
A referral under Article 30 of Directive 2001/83, as amended, was started in May 2009 for Tienam and associated names. During the course of the procedure, a Drafting Group meeting was convened by the CHMP. Tienam is a broad spectrum antibacterial agent that belongs to the group of carbapenems and consists of a fixed combination (1:1 ratio) of imipenem (a carbapenem antibiotic which is a derivative of thienamycin) and cilastatin (an inhibitor of dehydropeptidase I, a renal enzyme which metabolizes and inactivates imipenem). Imipenem has activity against a wide variety of bacteria, including Gram-positive aerobic cocci, Gram-positive aerobic bacilli, Gram-negative aerobic bacteria, and anaerobes. In particular, four divergent indications (i.e., gynaecological infections, septicaemia, bone and joint infections, and endocarditis) and the use in paediatric patients less than 3 years of age were discussed. Tienam was approved in the EU in 1985 and is currently authorised in 28 European countries (Norway, Iceland and all EU countries with the exception of Denmark). Tienam is approved as an intravenous (IV) formulation: Powder for solution for infusion, 250 mg/250mg and 500 mg/500 mg. Section 4.1 - Therapeutic indications 4.1.1 Intra-abdominal infections The CHMP considered that the data provided by the MAH included sufficient evidence that imipenem/cilastatin is efficacious in most studies in treating complicated intra-abdominal infections including e.g., intra-abdominal abscesses, peritonitis, complicated appendicitis, gall bladder empyema. The CHMP also noted the additional information in the form of abstracts or brief publications and considered that an indication for complicated intra-abdominal infections was supported. In conclusion, the CHMP adopted the following harmonised indication: “complicated intra-abdominal infections” 4.1.2 Lower respiratory tract infections The CHMP noted the proposed indication “lower respiratory tract infections” but considered the indication to be non-specific and therefore no longer appropriate, according to the Guideline on Antibacterial agents. The MAH discussed a number of specific indications, including community acquired pneumonia (CAP), cystic fibrosis, nosocomial pneumonia or ventilator associated pneumonia. In conclusion, the CHMP adopted the following harmonised indication: “severe pneumonia including hospital and ventilator-associated pneumonia” 4.1.3 Gynaecological infections The CHMP noted the proposed indication “gynaecological infections” but commented that the discussion of the available documentation focused primarily on intra- and post-partum infections. The MAH acknowledged that the spectrum of imipenem/cilatstatin does not cover Chlamydia trachomatis, and that there is insufficient evidence that Neisseria gonorrhoeae is a good target for therapy with this agent. Although data supporting this indication is limited, the CHMP considered the following harmonised indication to be acceptable: “intra- and post-partum infections
4.1.4 Septicaemia The CHMP noted the proposed the indication “septicaemia” but remarked on the limited and old clinical trial data available. There were no useful comparator-controlled clinical trials conducted and published in the peer-review literature from 2000 through 2010 in this indication and the epidemiological studies were of questionable quality and not sufficiently informative, in particular with regards to the used imipenem/cilastatin dosage. However, the CHMP acknowledged that high clinical cure rates were
8
reported in a large number of patients with bacteraemia associated with the approved indications. In conclusion, based on the presented data, the CHMP considered the indication to be acceptable and adopted the following harmonised indication: “Tienam may be used in the management of neutropenic patients with fever that is suspected to be due to a bacterial infection.” 4.1.5 Genitourinary infections The CHMP noted the proposed indication “genitourinary infections” but stated that imipenem/cilastatin should be used only in severe bacterial infections suspected or due to pathogens resistant to other beta-lactams and susceptible to imipenem/cilastatin. In addition, the term “genitourinary tract infections” was considered outdated. Although most studies were outdated and/or of poor quality, the CHMP was of the opinion that a restricted indication would be justified and in conclusion, adopted the following harmonised indication: “complicated urinary tract infections” 4.1.6 Bone and joint infections The CHMP noted the proposed indication “bone and joint infections” but considered the data submitted to be insufficient. The CHMP also assessed the limited data from literature sources and concluded that the claimed broad indication in the treatment of bone and joint infections could not be supported. The CHMP also discussed the possibility of limiting the indication to “Osteomyelitis” however there were not enough data to support this indication. In addition, potential failure of Tienam therapy might lead to surgical interventions or amputations which should be considered as serious adverse outcomes. In conclusion, the CHMP was of the opinion that this indication was inadequately substantiated, and therefore deleted the indication. 4.1.7 Skin and soft tissue infections The CHMP noted the proposed indication “skin and soft tissue infections” (SSTI). These infections are mostly caused by Gram-positive bacteria, S. aureus being the most important. Imipenem/cilastatin is not considered to be the best anti-staphylococcal agent, as other agents like semi-synthetic penicillins are generally considered to be more effective. Furthermore imipenem/cilastatin has no activity against MRSA and is therefore not considered to be an appropriate antibiotic for the empiric treatment of SSTIs caused by staphylococci since the risk of selecting for MRSA is quite high. The CHMP noted and assessed the available clinical trial and publication data showing that imipenem/cilastatin is effective and well tolerated in the treatment of “Complicated Skin and soft-tissue infections”. In conclusion, the CHMP adopted the following harmonised indication: “complicated skin and soft-tissue infections” 4.1.8 Endocarditis The CHMP noted the proposed indication “endocarditis” but considered that the claimed indication in the treatment of endocarditis was insufficiently substantiated. The presented data were very scarce and imipenem/cilastatin is not considered one of the most effective agents against staphylococci and methicillin-resistant staphylococci are known to be resistant to imipenem/cilastatin. Moreover, the use of imipenem in the management of any type of endocarditis has not been mentioned in the EU endocarditis Guideline, 2004. Therefore, the CHMP did not consider imipenem/cilastatin to be an appropriate antibiotic for the empiric treatment of this life-threatening infection as the risk of selecting for MRSA is especially high. In conclusion, the CHMP therefore deleted the indication. 4.1.9 Prophylaxis The CHMP noted the proposed indication “prevention of certain post-operative infections in patients undergoing contaminated or potentially contaminated surgical procedures or where the occurrence of post-operative infection could be especially serious” and the data provided to support the indication, including several published studies evaluating imipenem or imipenem/cilastatin as prophylaxis antibiotic therapy to prevent post-surgical infections as a result of colorectal surgery, appendectomy, and endoscopic sclerotherapy. The CHMP considered that imipenem/cilastatin is a broad spectrum antibiotic which should be used in the treatment of severe/life-threatening infections accompanying
9
with microbial resistance and/or when microbial resistance is demonstrated. Unjustified and non-substantiated prophylactic use is not acceptable. The CHMP therefore deleted this indication. 4.1.10 Management of bacterial infections in patients with febrile neutropenia The CHMP noted that, overall, although no high quality, double blind studies were submitted together with data from a substantial number of randomised, comparative open-labelled studies and concluded that imipenem/cilastatin appears to be suitable for the management of neutropenic patients. The issue of seizures in paediatric patients with systemic malignancies during therapy with imipenem/cilastatin was also discussed and the CHMP was reassured by the absence of evidence in support of an increased risk of seizures in this population. In conclusion, the CHMP adopted the following harmonised indication: “Tienam may be used in the management of neutropenic patients with fever that is suspected to be due to a bacterial infection.” 4.1.11 Mixed infections The CHMP noted the proposed indication “mixed infections” but was of the opinion that this wording is not in line with the current antimicrobial guidelines and recent European regulatory decisions, which require a site of infection to be specified. The CHMP therefore deleted this indication. 4.1.12 Non-indication in the treatment of meningitis. The CHMP did not consider this to be an indication and removed this information from section 4.1. 4.1.13 Paediatric use The CHMP assessed the available data regarding use in children, in particular taking into account 2 large efficacy/safety paediatric studies (Paediatric Study 1 and Paediatric Study 2/3) and the available peer-review medical literature. The overall clinical efficacy of imipenem/cilastatin was high and evaluable patients and the used dosage was effective and safe. The MAH provided a categorised summary of the enrolled patients, according to age groups to provide a basis for a discussion on the need for limiting the use of imipenem/cilastatin to children above 1 year of age for safety reasons. The MAH provided a cumulative review of adverse event reports received for imipenem/cilastatin in paediatric patients between 3 months to 3 years of age, which identified a total of 163 events in 82 reports. The CHMP considered that the frequency of seizures in the paediatric population < 1 year was unacceptably high and that this risk was confirmed by spontaneous adverse event reports. The CHMP therefore considered that the benefit-risk for imipenem/cilastatin in children under 1 year of age is negative and inserted a statement that the clinical data are insufficient to recommend dosing for children under the age of 1 year. With regards to safety, the CHMP considered that the available documentation supports a similar safety profile of imipenem/cilastatin in children compared to adults. 4.2 Posology and method of administration Adults and adolescents. The CHMP was of the opinion that in light of the present clinical and PK/PD data, a standard dose of 500 mg every 6 hours or 1g every 8 hours can be accepted, provided that a recommendation is inserted in the SPC stating that for infections suspected or proven to be due to less susceptible organisms (e.g. P. aeruginosa) and for very severe infections (e.g. in neutropenic patients with a fever), the 1000 mg q.i.d should be used. Paediatric patients above 1 year of age The CHMP was of the opinion that in light of the present clinical and PK/PD data, for paediatric patients ≥1 year of age, a standard dose of 15 or 25 mg/kg/dose administered every 6 hours is recommended. Advice to physicians was provided regarding infections suspected or proven to be due to less susceptible bacterial species (e.g. Pseudomonas aeruginosa) and very severe infections (e.g. in neutropenic patients with a fever), recommending treatment with 25 mg/kg every 6 hours. Elderly population Based on information from the submitted studies, the CHMP considered that no dose adjustment is required in elderly patients, except in cases of moderate to severe renal impairment.
10

Doses ≥ 4 gm/day The CHMP requested the MAH to carry out a relevant safety analysis across dose levels to confirm that the reason for not recommending the higher dose of 1 g q6h in several indications was not driven by safety aspects. The CHMP observed that no new safety issues or increased ADRs were observed with the use of imipenem/cilastatin doses of ≥ 4 gm/day as compared to doses of <4 gm/day, based on the review of clinical trial data in the original WMA, PMS data and the literature. The CHMP also deleted the low doses of 250 mg every 6 hours as mild infections should not be treated with imipenem/cilastatin. In conclusion, the CHMP adopted a harmonised wording for section 4.2, including the following dose recommendations: “Adults and adolescents For patients with normal renal function (creatinine clearance of >70 ml/min/1.73 m2), the recommended dose regimens are: 500 mg every 6 hours OR 1000 mg every 8 hours OR every 6 hours It is recommended that infections suspected or proven to be due to less susceptible bacterial species (such as Pseudomonas aeruginosa) and very severe infections (e.g. in neutropenic patients with a fever) should be treated with 1000 mg administered every 6 hours. The maximum total daily dose should not exceed 4000 mg/day. Paediatric population ≥1 year of age For paediatric patients ≥1 year of age, the recommended dose is 15 or 25 mg/kg/dose administered every 6 hours. It is recommended that infections suspected or proven to be due to less susceptible bacterial species (such as Pseudomonas aeruginosa) and very severe infections (e.g. in neutropenic patients with a fever) should be treated with 25 mg/kg administered every 6 hours. Paediatric population <1 year of age Clinical data are insufficient to recommend dosing for children less than 1 year of age.” Section 4.4 - Special warnings and precautions for use The CHMP noted the MAH proposal for this section and made a number of revisions. The CHMP adopted a harmonised wording for section 4.4 and in particular, the following statement concerning the limited susceptibility of specific pathogens and the concomitant use of an appropriate anti-MRSA agent or of an aminoglycoside was included: “The antibacterial spectrum of imipenem/cilastatin should be taken into account especially in life-threatening conditions before embarking on any empiric treatment. Furthermore, due to the limited susceptibility of specific pathogens associated with e.g. bacterial skin and soft-tissue infections, to imipenem/cilastatin, caution should be exercised. The use of imipenem/cilastatin is not suitable for treatment of these types of infections unless the pathogen is already documented and known to be susceptible or there is a very high suspicion that the most likely pathogen(s) would be suitable for treatment. Concomitant use of an appropriate anti-MRSA agent may be indicated when MRSA infections are suspected or proven to be involved in the approved indications. Concomitant use of an aminoglycoside may be indicated when Pseudomonas aeruginosa infections are suspected or proven to be involved in the approved indications (see section 4.1).” Sections 4.3 – Contraindications, 4.5 - Interaction with other medicinal products and other forms of interaction, 4.6 – Fertility, Pregnancy and Lactation, 4.7 - Effects on ability to drive and use machines, 4.8 - Undesirable effects, 4.9 – Overdose, 5.1 - Pharmacodynamic properties, 5.2 - Pharmacokinetic properties and 5.3 - Preclinical safety data The CHMP adopted a harmonised wording for these sections.
11

SECTION 6 – PHARMACEUTICAL PARTICULARS In sections 6.3 and 6.6, a warning was added to state that diluted solutions should be used immediately and that the interval between beginning of reconstitution and the end of intravenous infusion should not exceed two hours. In addition, the recommended solutions were specified as being 0.9% sodium chloride solution and water for injection, while the use of 5% glucose was restricted to exceptional circumstances where 0.9% sodium chloride cannot be used for clinical reasons.
Grounds for amendment of the summary of product characteristics, labelling and package leaflet
Whereas
the scope of the referral was the harmonisation of the summary of products characteristics,
labelling and package leaflet
the summary of products characteristic, labelling and package leaflet proposed by the marketing
authorisation holders have been assessed based on the documentation submitted and the scientific
discussion within the Committee
the CHMP has recommended the amendment of the marketing authorisations for which the summary
of product characteristics, labelling and package leaflet are set out in Annex III for Tienam and
associated names (see Annex I).
12

Annex III
Summary of product characteristics, labelling and package leaflet
Note: This SPC, labelling and packages leaflet is the version valid at the time of Commission decision.
After the Commission decision the Member State competent authorities, in liaison with the reference
Member State, will update the product information as required. Therefore, this SPC, labelling and
package leaflet may not necessarily represent the current text.
13

SUMMARY OF PRODUCT CHARACTERISTICS
14

1. NAME OF THE MEDICINAL PRODUCT TIENAM and associated names (see Annex I) 500 mg/500 mg powder for solution for infusion [See Annex I – To be completed nationally] 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains imipenem monohydrate equivalent to 500 mg imipenem anhydrate and cilastatin sodium equivalent to 500 mg cilastatin. Each vial contains sodium bicarbonate equivalent to approximately 1.6 mEq of sodium (approximately 37.6 mg). For a full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Powder for solution for infusion. White to light yellow powder. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications TIENAM is indicated for the treatment of the following infections in adults and children 1 year of age and above (see sections 4.4 and 5.1): complicated intra-abdominal infections severe pneumonia including hospital and ventilator-associated pneumonia intra- and post-partum infections complicated urinary tract infections complicated skin and soft-tissue infections TIENAM may be used in the management of neutropenic patients with fever that is suspected to be due to a bacterial infection. Treatment of patients with bacteraemia that occurs in association with, or is suspected to be associated with, any of the infections listed above. Consideration should be given to official guidance on the appropriate use of antibacterial agents. 4.2 Posology and method of administration Posology The dose recommendations for TIENAM represent the quantity of imipenem/cilastatin to be administered. The daily dose of TIENAM should be based on the type and severity of infection, the pathogen(s) isolated, the patient's renal function and body weight (see also section 4.4 and 5.1). Adults and adolescents For patients with normal renal function (creatinine clearance of >70 ml/min/1.73 m2), the recommended dose regimens are:
15

500 mg/500 mg every 6 hours OR 1000 mg/1000 mg every 8 hours OR every 6 hours It is recommended that infections suspected or proven to be due to less susceptible bacterial species (such as Pseudomonas aeruginosa) and very severe infections (e.g. in neutropenic patients with a fever) should be treated with 1000 mg/1000 mg administered every 6 hours. A reduction in dose is necessary when: creatinine clearance is ≤ 70 ml/min/l.73 m2 (see Table 1) or body weight is < 70 kg. The proportionate dose for patients < 70 kg would be calculated using the
following formula: Actual body weight (kg) X standard dose 70 (kg)
The maximum total daily dose should not exceed 4000 mg/4000 mg per day. Renal impairment To determine the reduced dose for adults with impaired renal function: 1. The total daily dose (i.e. 2000/2000, 3000/3000 or 4000/4000 mg) that would usually be applicable
to patients with normal renal function should be selected. 2. From table 1 the appropriate reduced dose regimen is selected according to the patient's creatinine
clearance. For infusion times see Method of administration. Table 1: Reduced dose in adults with impaired renal function and body weight 70 kg*
Creatinine clearance (ml/min/1.73 m2) 41-70 21-40 6-20
Total daily dose for patients with normal renal function (mg/day)
dose in mg (interval hrs) 2000/2000 500/500 (8) 250/250 (6) 250/250 (12) 3000/3000 500/500 (6) 500/500 (8) 500/500 (12)** 4000/4000 750/750 (8) 500/500 (6) 500/500 (12)**
* A further proportionate reduction in dose administered must be made for patients with a body weight <70 kg. The proportionate dose for patients <70 kg would be calculated by dividing the patient's actual body weight (in kg) by 70 kg multiplied by the respective dose recommended in Table 1. ** When the 500 mg/500 mg dose is used in patients with creatinine clearances of 6 to 20 ml/min/l.73 m2, there may be an increased risk of seizures. Patients with a creatinine clearance of ≤5 ml/min/1.73 m2 These patients should not receive TIENAM unless haemodialysis is instituted within 48 hours. Patients on haemodialysis When treating patients with creatinine clearances of 5 ml/min/1.73 m2 who are undergoing dialysis use the dose recommendation for patients with creatinine clearances of 6 to 20 ml/min/1.73 m2 (see table 1). Both imipenem and cilastatin are cleared from the circulation during haemodialysis. The patient should receive TIENAM after haemodialysis and at 12 hour intervals timed from the end of that haemodialysis session. Dialysis patients, especially those with background central nervous system (CNS) disease, should be carefully monitored; for patients on haemodialysis, TIENAM is recommended only when the benefit outweighs the potential risk of seizures (see section 4.4). Currently there are inadequate data to recommend use of TIENAM for patients on peritoneal dialysis.
16
Hepatic impairment No dose adjustment is recommended in patients with impaired hepatic function (see section 5.2). Elderly population No dose adjustment is required for the elderly patients with normal renal function (see section 5.2). Paediatric population ≥1 year of age For paediatric patients ≥1 year of age, the recommended dose is 15/15 or 25/25 mg/kg/dose administered every 6 hours. It is recommended that infections suspected or proven to be due to less susceptible bacterial species (such as Pseudomonas aeruginosa) and very severe infections (e.g. in neutropenic patients with a fever) should be treated with 25/25 mg/kg administered every 6 hours. Paediatric population <1 year of age Clinical data are insufficient to recommend dosing for children less than 1 year of age Paediatric population with renal impairment Clinical data are insufficient to recommend dosing for paediatric patients with renal impairment (serum creatinine > 2 mg/dl). See section 4.4. Method of administration TIENAM is to be reconstituted and further diluted (see section 6.2, 6.3 and 6.6) prior to administration. Each dose of 500 mg/500 mg should be given by intravenous infusion over 20 to 30 minutes. Each dose >500 mg/500 mg should be infused over 40 to 60 minutes. In patients who develop nausea during the infusion, the rate of infusion may be slowed. 4.3 Contraindications Hypersensitivity to the active substances or to any of the excipients Hypersensitivity to any other carbapenem antibacterial agent Severe hypersensitivity (e.g. anaphylactic reaction, severe skin reaction) to any other type of beta-
lactam antibacterial agent (e.g. penicillins or cephalosporins). 4.4 Special warnings and precautions for use General The selection of imipenem/cilastatin to treat an individual patient should take into account the appropriateness of using a carbapenem antibacterial agent based on factors such as severity of the infection, the prevalence of resistance to other suitable antibacterial agents and the risk of selecting for carbapenem-resistant bacteria. Hypersensitivity Serious and occasionally fatal hypersensitivity (anaphylactic) reactions have been reported in patients receiving therapy with beta-lactams. These reactions are more likely to occur in individuals with a history of sensitivity to multiple allergens. Before initiating therapy with TIENAM, careful inquiry should be made concerning previous hypersensitivity reactions to carbapenems, penicillins, cephalosporins, other beta-lactams and other allergens (see section 4.3). If an allergic reaction to TIENAM occurs, discontinue the therapy immediately. Serious anaphylactic reactions require immediate emergency treatment. Hepatic Hepatic function should be closely monitored during treatment with imipenem/cilastatin due to the risk of hepatic toxicity (such as increase in transaminases, hepatic failure and fulminant hepatitis).
17

Use in patients with liver disease: patients with pre-existing liver disorders should have liver function monitored during treatment with imipenem/cilastatin. There is no dose adjustment necessary (see section 4.2). Haematology A positive direct or indirect Coombs test may develop during treatment with imipenem/cilastatin. Antibacterial spectrum The antibacterial spectrum of imipenem/cilastatin should be taken into account especially in life-threatening conditions before embarking on any empiric treatment. Furthermore, due to the limited susceptibility of specific pathogens associated with e.g. bacterial skin and soft-tissue infections, to imipenem/cilastatin, caution should be exercised. The use of imipenem/cilastatin is not suitable for treatment of these types of infections unless the pathogen is already documented and known to be susceptible or there is a very high suspicion that the most likely pathogen(s) would be suitable for treatment. Concomitant use of an appropriate anti-MRSA agent may be indicated when MRSA infections are suspected or proven to be involved in the approved indications. Concomitant use of an aminoglycoside may be indicated when Pseudomonas aeruginosa infections are suspected or proven to be involved in the approved indications (see section 4.1). Interaction with valproic acid The concomitant use of imipenem/cilastatin and valproic acid/sodium valproate is not recommended (see section 4.5). Clostridium difficile Antibiotic-associated colitis and pseudomembranous colitis have been reported with imipenem/cilastatin and with nearly all other anti-bacterial agents and may range from mild to life-threatening in severity. It is important to consider this diagnosis in patients who develop diarrhoea during or after the use of imipenem/cilastatin (see section 4.8). Discontinuation of therapy with imipenem/cilastatin and the administration of specific treatment for Clostridium difficile should be considered. Medicinal products that inhibit peristalsis should not be given. Meningitis TIENAM is not recommended for the therapy of meningitis. Central nervous system CNS adverse reactions such as myoclonic activity, confusional states, or seizures have been reported, especially when recommended doses based on renal function and body weight were exceeded. These experiences have been reported most commonly in patients with CNS disorders (e.g. brain lesions or history of seizures) and/or compromised renal function in whom accumulation of the administered entities could occur. Hence close adherence to recommended dose schedules is urged especially in these patients (see section 4.2). Anticonvulsant therapy should be continued in patients with a known seizure disorder. Special awareness should be made to neurological symptoms or convulsions in children with known risk factors for seizures, or on concomitant treatment with medicinal products lowering the seizures threshold. If focal tremors, myoclonus, or seizures occur, patients should be evaluated neurologically and placed on anticonvulsant therapy if not already instituted. If CNS symptoms continue, the dose of TIENAM should be decreased or discontinued. Patients with creatinine clearances of 5 ml/min/1.73 m2 should not receive TIENAM unless haemodialysis is instituted within 48 hours. For patients on haemodialysis, TIENAM is recommended only when the benefit outweighs the potential risk of seizures (see section 4.2).
18

Paediatric use Clinical data are insufficient to recommend the use of TIENAM in children under 1 year of age or paediatric patients with impaired renal function (serum creatinine >2 mg/dl). See also above under Central nervous system. TIENAM 500 mg/500 mg contains 37.6 mg of sodium (1.6 mEq) which should be taken into consideration by patients on a controlled sodium diet. 4.5 Interaction with other medicinal products and other forms of interaction Generalized seizures have been reported in patients who received ganciclovir and TIENAM. These medicinal products should not be used concomitantly unless the potential benefit outweighs the risks. Decreases in valproic acid levels that may fall below the therapeutic range have been reported when valproic acid was co-administered with carbapenem agents. The lowered valproic acid levels can lead to inadequate seizure control; therefore, concomitant use of imipenem and valproic acid/sodium valproate is not recommended and alternative antibacterial or anti-convulsant therapies should be considered (see section 4.4). Oral anti-coagulants Simultaneous administration of antibiotics with warfarin may augment its anti-coagulant effects. There have been many reports of increases in the anti-coagulant effects of orally administered anti-coagulant agents, including warfarin in patients who are concomitantly receiving antibacterial agents. The risk may vary with the underlying infection, age and general status of the patient so that the contribution of the antibiotic to the increase in INR (international normalised ratio) is difficult to assess. It is recommended that the INR should be monitored frequently during and shortly after co-administration of antibiotics with an oral anti-coagulant agent. Concomitant administration of TIENAM and probenecid resulted in minimal increases in the plasma levels and plasma half-life of imipenem. The urinary recovery of active (non-metabolized) imipenem decreased to approximately 60% of the dose when TIENAM was administered with probenecid. Concomitant administration of TIENAM and probenecid doubled the plasma level and half-life of cilastatin, but had no effect on urine recovery of cilastatin. 4.6 Fertility, pregnancy and lactation Pregnancy There are no adequate and well-controlled studies for the use of imipenem/cilastatin in pregnant women. Studies in pregnant monkeys have shown reproductive toxicity (see section 5.3). The potential risk for humans is unknown. TIENAM should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus. Breast-feeding Imipenem and cilastatin are excreted into the mother’s milk in small quantities. Little absorption of either compound occurs following oral administration. Therefore it is unlikely that the suckling infant will be exposed to significant quantities. If the use of TIENAM is deemed necessary, the benefit of breast feeding for the child should be weighed against the possible risk for the child. Fertility There are no data available regarding potential effects of imipenem/cilastatin treatment on male or female fertility.
19
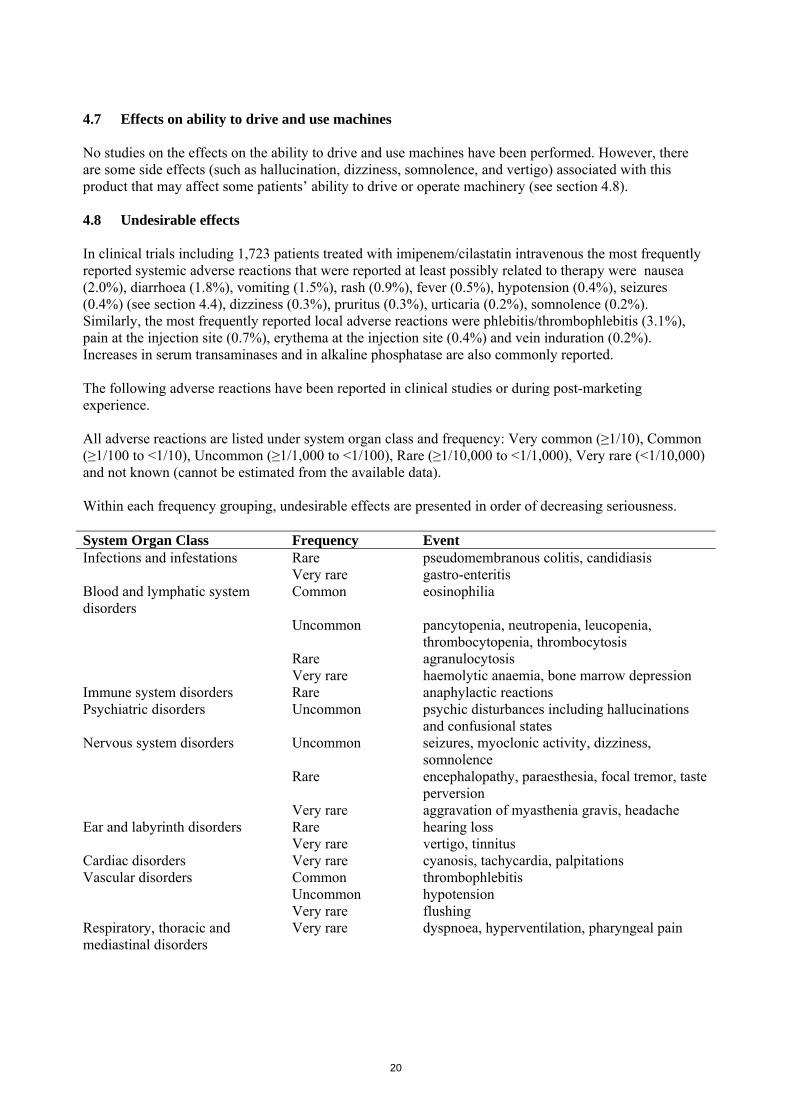
4.7 Effects on ability to drive and use machines No studies on the effects on the ability to drive and use machines have been performed. However, there are some side effects (such as hallucination, dizziness, somnolence, and vertigo) associated with this product that may affect some patients’ ability to drive or operate machinery (see section 4.8). 4.8 Undesirable effects In clinical trials including 1,723 patients treated with imipenem/cilastatin intravenous the most frequently reported systemic adverse reactions that were reported at least possibly related to therapy were nausea (2.0%), diarrhoea (1.8%), vomiting (1.5%), rash (0.9%), fever (0.5%), hypotension (0.4%), seizures (0.4%) (see section 4.4), dizziness (0.3%), pruritus (0.3%), urticaria (0.2%), somnolence (0.2%). Similarly, the most frequently reported local adverse reactions were phlebitis/thrombophlebitis (3.1%), pain at the injection site (0.7%), erythema at the injection site (0.4%) and vein induration (0.2%). Increases in serum transaminases and in alkaline phosphatase are also commonly reported. The following adverse reactions have been reported in clinical studies or during post-marketing experience. All adverse reactions are listed under system organ class and frequency: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. System Organ Class Frequency Event Infections and infestations Rare pseudomembranous colitis, candidiasis Very rare gastro-enteritis Blood and lymphatic system disorders
Common eosinophilia
Uncommon pancytopenia, neutropenia, leucopenia, thrombocytopenia, thrombocytosis
Rare agranulocytosis Very rare haemolytic anaemia, bone marrow depression Immune system disorders Rare anaphylactic reactions Psychiatric disorders Uncommon psychic disturbances including hallucinations
and confusional states Nervous system disorders Uncommon seizures, myoclonic activity, dizziness,
somnolence Rare encephalopathy, paraesthesia, focal tremor, taste
perversion Very rare aggravation of myasthenia gravis, headache Ear and labyrinth disorders Rare hearing loss Very rare vertigo, tinnitus Cardiac disorders Very rare cyanosis, tachycardia, palpitations Vascular disorders Common thrombophlebitis Uncommon hypotension Very rare flushing Respiratory, thoracic and mediastinal disorders
Very rare dyspnoea, hyperventilation, pharyngeal pain
20
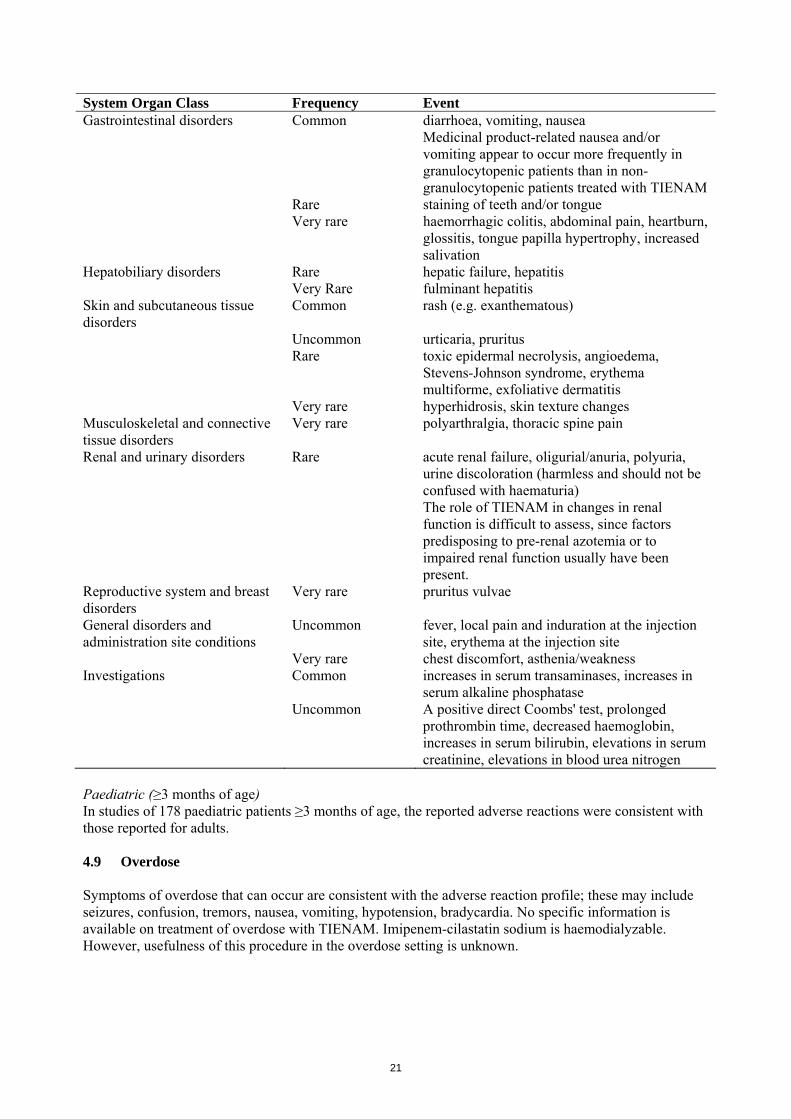
System Organ Class Frequency Event Gastrointestinal disorders Common diarrhoea, vomiting, nausea
Medicinal product-related nausea and/or vomiting appear to occur more frequently in granulocytopenic patients than in non-granulocytopenic patients treated with TIENAM
Rare staining of teeth and/or tongue Very rare haemorrhagic colitis, abdominal pain, heartburn,
glossitis, tongue papilla hypertrophy, increased salivation
Hepatobiliary disorders Rare hepatic failure, hepatitis Very Rare fulminant hepatitis Skin and subcutaneous tissue disorders
Common rash (e.g. exanthematous)
Uncommon urticaria, pruritus Rare toxic epidermal necrolysis, angioedema,
Stevens-Johnson syndrome, erythema multiforme, exfoliative dermatitis
Very rare hyperhidrosis, skin texture changes Musculoskeletal and connective tissue disorders
Very rare polyarthralgia, thoracic spine pain
Renal and urinary disorders Rare acute renal failure, oligurial/anuria, polyuria, urine discoloration (harmless and should not be confused with haematuria) The role of TIENAM in changes in renal function is difficult to assess, since factors predisposing to pre-renal azotemia or to impaired renal function usually have been present.
Reproductive system and breast disorders
Very rare pruritus vulvae
General disorders and administration site conditions
Uncommon fever, local pain and induration at the injection site, erythema at the injection site
Very rare chest discomfort, asthenia/weakness Investigations Common increases in serum transaminases, increases in
serum alkaline phosphatase Uncommon A positive direct Coombs' test, prolonged
prothrombin time, decreased haemoglobin, increases in serum bilirubin, elevations in serum creatinine, elevations in blood urea nitrogen
Paediatric (≥3 months of age) In studies of 178 paediatric patients ≥3 months of age, the reported adverse reactions were consistent with those reported for adults. 4.9 Overdose Symptoms of overdose that can occur are consistent with the adverse reaction profile; these may include seizures, confusion, tremors, nausea, vomiting, hypotension, bradycardia. No specific information is available on treatment of overdose with TIENAM. Imipenem-cilastatin sodium is haemodialyzable. However, usefulness of this procedure in the overdose setting is unknown.
21
5. PHARMACOLOGICAL PROPERTIES 5.1 Pharmacodynamic properties Pharmacotherapeutic group: Antibacterials for systemic use, carbapenems, ATC code: J01D H51 Mode of action TIENAM consists of two components: imipenem and cilastatin sodium in a 1:1 ratio by weight. Imipenem, also referred to as N-formimidoyl-thienamycin, is a semi-synthetic derivative of thienamycin, the parent compound produced by the filamentous bacterium Streptomyces cattleya. Imipenem exerts its bactericidal activity by inhibiting bacterial cell wall synthesis in Gram-positive and Gram-negative bacteria through binding to penicillin-binding proteins (PBPs). Cilastatin sodium is a competitive, reversible and specific inhibitor of dehydropeptidase-I, the renal enzyme which metabolizes and inactivates imipenem. It is devoid of intrinsic antibacterial activity and does not affect the antibacterial activity of imipenem. Pharmacokinetic/Pharmacodynamic (PK/PD) relationship Similar to other beta-lactam antibacterial agents, the time that imipenem concentrations exceed the MIC (T>MIC) has been shown to best correlate with efficacy. Mechanism of resistance Resistance to imipenem may be due to the following: Decreased permeability of the outer membrane of Gram-negative bacteria (due to diminished
production of porins) Imipenem may be actively removed from the cell with an efflux pump. Reduced affinity of PBPs to imipenem Imipenem is stable to hydrolysis by most beta-lactamases, including penicillinases and
cephalosporinases produced by gram-positive and gram-negative bacteria, with the exception of relatively rare carbapenem hydrolysing beta-lactamases. Species resistant to other carbapenems do generally express co-resistance to imipenem. There is no target-based cross-resistance between imipenem and agents of the quinolone, aminoglycoside, macrolide and tetracycline classes.
Breakpoints EUCAST MIC breakpoints for imipenem to separate susceptible (S) pathogens from resistant (R) pathogens are as follows (v 1,1 2010-04-27): Enterobacteriaceae 1: S ≤2 mg/l, R >8 mg/l Pseudomonas spp. 2: S ≤4 mg/l, R >8 mg/l Acinetobacter spp.: S ≤2 mg/l, R >8 mg/l Staphylococcus spp. 3: Inferred from cefoxitin susceptibility Enterococcus spp.: S ≤4 mg/l, R >8 mg/l Streptococcus A, B, C, G: The beta-lactam susceptibility of beta-haemolytic streptococcus groups A,
B, C and G is inferred from the penicillin susceptibility. Streptococcus pneumoniae 4: S ≤2 mg/l, R >2 mg/l Other streptococci 4: S ≤2 mg/l, R >2 mg/l Haemophilus influenzae 4: S ≤2 mg/l, R >2 mg/l Moraxalla catarrhalis 4: S ≤2 mg/l, R >2 mg/l Neisseria gonorrhoeae: There is insufficient evidence that Neisseria gonorrhoeae is a good target
for therapy with imipenem. Gram-positive anaerobes: S ≤2 mg/l, R >8 mg/l
22

Gram-negative anaerobes: S ≤2 mg/l, R >8 mg/l Non-species related breakpoints 5: S ≤2 mg/l, R >8 mg/l
1 Proteus and Morganella species are considered poor targets for imipenem. 2 The breakpoints for Pseudomonas relate to high dose frequent therapy (1g every 6 hours). 3 Susceptibility of staphylococci to carbapenems is inferred from the cefoxitin susceptibility. 4 Strains with MIC values above the susceptible breakpoint are very rare or not yet reported. The
identification and antimicrobial susceptibility tests on any such isolate must be repeated and if the result is confirmed the isolate must be sent to a reference laboratory. Until there is evidence regarding clinical response for confirmed isolates with MIC above the current resistant breakpoint they should be reported resistant.
5 Non-species related breakpoint have been determined mainly on the basis of PK/PD data and are independent of MIC distributions of specific species. They are for use only for species not mentioned in the overview of species-related breakpoints or footnotes.
Susceptibility The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable. Commonly susceptible species: Gram-positive aerobes:
Enterococcus faecalis Staphylococcus aureus (Methicillin-susceptible)* Staphylococcus coagulase negative (Methicillin-susceptible) Streptococcus agalactiae Streptococcus pneumoniae Streptococcus pyogenes Streptococcus viridans group
Gram-negative aerobes: Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzae Klebsiella oxytoca Klebsiella pneumoniae Moraxella catarrhalis Serratia marcescens
Gram-positive anaerobes: Clostridium perfringens** Peptostreptococcus spp.**
Gram-negative anaerobes: Bacteroides fragilis Bacteroides fragilis group Fusobacterium spp. Porphyromonas asaccharolytica Prevotella spp. Veillonella spp.
23
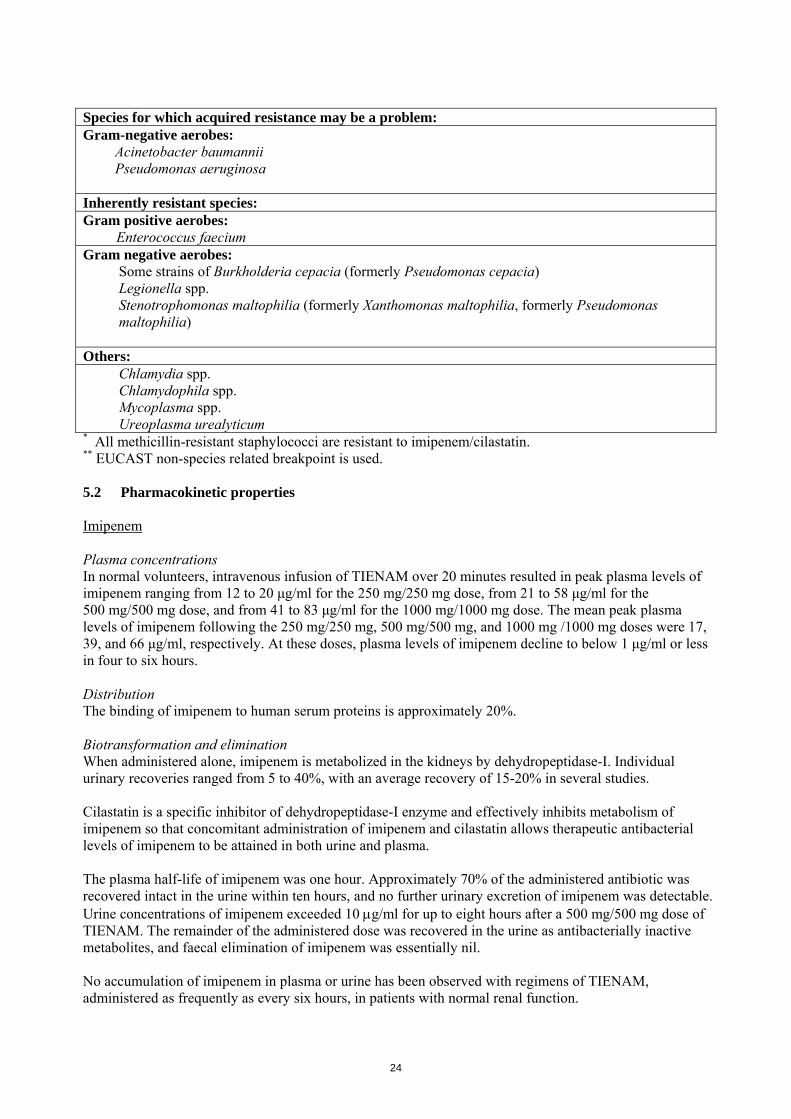
Species for which acquired resistance may be a problem: Gram-negative aerobes:
Acinetobacter baumannii Pseudomonas aeruginosa
Inherently resistant species: Gram positive aerobes:
Enterococcus faecium Gram negative aerobes:
Some strains of Burkholderia cepacia (formerly Pseudomonas cepacia) Legionella spp. Stenotrophomonas maltophilia (formerly Xanthomonas maltophilia, formerly Pseudomonas maltophilia)
Others:
Chlamydia spp. Chlamydophila spp. Mycoplasma spp. Ureoplasma urealyticum
* All methicillin-resistant staphylococci are resistant to imipenem/cilastatin. ** EUCAST non-species related breakpoint is used. 5.2 Pharmacokinetic properties Imipenem Plasma concentrations In normal volunteers, intravenous infusion of TIENAM over 20 minutes resulted in peak plasma levels of imipenem ranging from 12 to 20 μg/ml for the 250 mg/250 mg dose, from 21 to 58 μg/ml for the 500 mg/500 mg dose, and from 41 to 83 μg/ml for the 1000 mg/1000 mg dose. The mean peak plasma levels of imipenem following the 250 mg/250 mg, 500 mg/500 mg, and 1000 mg /1000 mg doses were 17, 39, and 66 μg/ml, respectively. At these doses, plasma levels of imipenem decline to below 1 μg/ml or less in four to six hours. Distribution The binding of imipenem to human serum proteins is approximately 20%. Biotransformation and elimination When administered alone, imipenem is metabolized in the kidneys by dehydropeptidase-I. Individual urinary recoveries ranged from 5 to 40%, with an average recovery of 15-20% in several studies. Cilastatin is a specific inhibitor of dehydropeptidase-I enzyme and effectively inhibits metabolism of imipenem so that concomitant administration of imipenem and cilastatin allows therapeutic antibacterial levels of imipenem to be attained in both urine and plasma. The plasma half-life of imipenem was one hour. Approximately 70% of the administered antibiotic was recovered intact in the urine within ten hours, and no further urinary excretion of imipenem was detectable. Urine concentrations of imipenem exceeded 10 g/ml for up to eight hours after a 500 mg/500 mg dose of TIENAM. The remainder of the administered dose was recovered in the urine as antibacterially inactive metabolites, and faecal elimination of imipenem was essentially nil. No accumulation of imipenem in plasma or urine has been observed with regimens of TIENAM, administered as frequently as every six hours, in patients with normal renal function.
24

Cilastatin Plasma concentrations Peak plasma levels of cilastatin, following a 20 minute intravenous infusion of TIENAM, ranged from 21 to 26 μg/ml for the 250 mg/250 mg dose, from 21 to 55 μg/ml for the 500 mg/500 mg dose and from 56 to 88 μg/ml for the 1000 mg/1000 mg dose. The mean peak plasma levels of cilastatin following the 250 mg/250 mg, 500 mg/500 mg, and 1000 mg/1000 mg doses were 22, 42, and 72 µg/ml respectively. Distribution The binding of cilastatin to human serum proteins is approximately 40%. Biotransformation and elimination The plasma half-life of cilastatin is approximately one hour. Approximately 70-80% of the dose of cilastatin was recovered unchanged in the urine as cilastatin within 10 hours of administration of TIENAM. No further cilastatin appeared in the urine thereafter. Approximately 10% was found as the N-acetyl metabolite, which has inhibitory activity against dehydropeptidase comparable to that of cilastatin. Activity of dehydropeptidase-I in the kidney returned to normal levels shortly after the elimination of cilastatin from the blood stream. Renal insufficiency Following a single 250 mg/250 mg intravenous dose of TIENAM, the area under the curve (AUCs) for imipenem increased 1.1-fold, 1.9-fold, and 2.7-fold in subjects with mild (Creatinine Clearance (CrCL) 50-80 ml/min/1.73 m2), moderate (CrCL 30-<50 ml/min/1.73 m2), and severe (CrCL <30 ml/min/1.73 m2) renal impairment, respectively, compared to subjects with normal renal function (CrCL >80 ml/min/1.73 m2), and AUCs for cilastatin increased 1.6-fold, 2.0-fold, and 6.2-fold in subjects with mild, moderate, and severe renal impairment, respectively, compared to subjects with normal renal function. Following a single 250 mg/250 mg intravenous dose of TIENAM given 24 hours after haemodialysis, AUCs for imipenem and cilastatin were 3.7-fold and 16.4-fold higher, respectively, as compared to subjects with normal renal function. Urinary recovery, renal clearance and plasma clearance of imipenem and cilastatin decrease with decreasing renal function following intravenous administration of TIENAM. Dose adjustment is necessary for patients with impaired renal function (see section 4.2). Hepatic insufficiency The pharmacokinetics of imipenem in patients with hepatic insufficiency have not been established. Due to the limited extent of hepatic metabolism of imipenem, its pharmacokinetics are not expected to be affected by hepatic impairment. Therefore, no dose adjustment is recommended in patients with hepatic impairment (see section 4.2). Paediatric patients The average clearance (CL) and volume of distribution (Vdss) for imipenem were approximately 45% higher in paediatric patients (3 months to 14 years) as compared to adults. The AUC for imipenem following administration of 15/15 mg/kg per body weight of imipenem/cilastatin to paediatric patients was approximately 30% higher than the exposure in adults receiving a 500 mg/500 mg dose. At the higher dose, the exposure following administration of 25/25 mg/kg imipenem/cilastatin to children was 9% higher as compared to the exposure in adults receiving a 1000 mg/1000 mg dose. Elderly In healthy elderly volunteers (65 to 75 years of age with normal renal function for their age), the pharmacokinetics of a single dose of TIENAM 500 mg/500 mg administered intravenously over 20 minutes were consistent with those expected in subjects with slight renal impairment for which no dose alteration is considered necessary. The mean plasma half-lives of imipenem and cilastatin were 91 ± 7.0 minutes and 69 ± 15 minutes, respectively. Multiple dosing has no effect on the pharmacokinetics of either imipenem or cilastatin, and no accumulation of imipenem/cilastatin was observed (see section 4.2).
25

5.3 Preclinical safety data Non-clinical data reveal no special hazard for humans based on repeated dose toxicity and genotoxicity studies. Animal studies showed that the toxicity produced by imipenem, as a single entity, was limited to the kidney. Co-administration of cilastatin with imipenem in a 1:1 ratio prevented the nephrotoxic effects of imipenem in rabbits and monkeys. Available evidence suggests that cilastatin prevents the nephrotoxicity by preventing entry of imipenem into the tubular cells. A teratology study in pregnant cynomolgus monkeys given imipenem-cilastatin sodium at doses of 40/40 mg/kg/day (bolus intravenous injection) resulted in maternal toxicity including emesis, inappetence, body weight loss, diarrhoea, abortion, and death in some cases. When doses of imipenem-cilastatin sodium (approximately 100/100 mg/kg/day or approximately 3 times the usual recommended daily human intravenous dose) were administered to pregnant cynomolgus monkeys at an intravenous infusion rate which mimics human clinical use, there was minimal maternal intolerance (occasional emesis), no maternal deaths, no evidence of teratogenicity, but an increase in embryonic loss relative to control groups (see section 4.6). Long term studies in animals have not been performed to evaluate carcinogenic potential of imipenem-cilastatin. 6. PHARMACEUTICAL PARTICULARS 6.1 List of excipients Sodium bicarbonate 6.2 Incompatibilities This medicinal product is chemically incompatible with lactate and should not be reconstituted in diluents containing lactate. However, it can be administered into an I.V. system through which a lactate solution is being infused. This medicinal product must not be mixed with other medicinal products except those mentioned in section 6.6. 6.3 Shelf life 2 years. After reconstitution: Diluted solutions should be used immediately. The time interval between the beginning of reconstitution and the end of intravenous infusion should not exceed two hours. 6.4 Special precautions for storage Do not store above 25 °C. Do not freeze the reconstituted solution. For storage conditions of the reconstituted medicinal product, see section 6.3.
26
6.5 Nature and contents of container 20 ml Type I glass vials. The medicinal product is supplied in packs of 1 vial, 10 vials and 25 vials. Not all pack sizes may be marketed. 6.6 Special precautions for disposal and other handling Each vial is for single use only. Reconstitution: Contents of each vial must be transferred to 100 ml of an appropriate infusion solution (see section 6.2 and 6.3): 0.9% sodium chloride. In exceptional circumstances where 0.9% sodium chloride cannot be used for clinical reasons 5% glucose may be used instead. A suggested procedure is to add approximately 10 ml of the appropriate infusion solution to the vial. Shake well and transfer the resulting mixture to the infusion solution container. CAUTION: THE MIXTURE IS NOT FOR DIRECT INFUSION. Repeat with an additional 10 ml of infusion solution to ensure complete transfer of vial contents to the infusion solution. The resulting mixture should be agitated until clear. The concentration of the reconstituted solution following the above procedure is approximately 5 mg/ml for both imipenem and cilastatin. Variations of colour, from colourless to yellow, do not affect the potency of the product. Any unused product or waste material should be disposed of in accordance with local requirements. 7. MARKETING AUTHORISATION HOLDER [See Annex I – To be completed nationally] {Name and address} <{tel}> <{fax}> <{e-mail}>
27
8. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION [To be completed nationally] 10. DATE OF REVISION OF THE TEXT [To be completed nationally]
28

LABELLING
29

PARTICULARS TO APPEAR ON THE OUTER PACKAGING OUTER CARTON 1. NAME OF THE MEDICINAL PRODUCT TIENAM and associated names (see Annex I) 500 mg/500 mg powder for solution for infusion [See Annex I - To be completed nationally] Imipenem/Cilastatin 2. STATEMENT OF ACTIVE SUBSTANCE(S) Each vial contains: imipenem monohydrate equivalent to 500 mg imipenem anhydrate and cilastatin sodium equivalent to 500 mg cilastatin 3. LIST OF EXCIPIENTS Sodium bicarbonate (E500) 4. PHARMACEUTICAL FORM AND CONTENTS Powder for solution for infusion 1 vial 10 vials 25 vials 5. METHOD AND ROUTE(S) OF ADMINISTRATION Read the package leaflet before use. Intravenous use after reconstitution. For single use only. 6. SPECIAL WARNING THAT THE MEDICINAL PRODUCT MUST BE STORED OUT OF
THE REACH AND SIGHT OF CHILDREN Keep out of the reach and sight of children. 7. OTHER SPECIAL WARNING(S), IF NECESSARY 8. EXPIRY DATE EXP
30
9. SPECIAL STORAGE CONDITIONS Do not store above 25C After reconstitution: Diluted solutions should be used immediately. The time interval between the beginning of reconstitution and the end of intravenous infusion should not exceed two hours. 10. SPECIAL PRECAUTIONS FOR DISPOSAL OF UNUSED MEDICINAL PRODUCTS OR
WASTE MATERIALS DERIVED FROM SUCH MEDICINAL PRODUCTS, IF APPROPRIATE
11. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and Address} <{tel}> <{fax}> <{e-mail}> 12. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 13. BATCH NUMBER Lot 14. GENERAL CLASSIFICATION FOR SUPPLY [To be completed nationally] 15. INSTRUCTIONS ON USE 16. INFORMATION IN BRAILLE
31

PARTICULARS TO APPEAR ON THE IMMEDIATE PACKAGING VIAL 1. NAME OF THE MEDICINAL PRODUCT AND ROUTE(S) OF ADMINISTRATION TIENAM and associated names (see Annex I) 500 mg/500 mg powder for solution for infusion [See Annex I - To be completed nationally] Imipenem/Cilastatin Intravenous use 2. STATEMENT OF ACTIVE SUBSTANCE(S) Each vial contains: imipenem 500 mg and cilastatin 500 mg. 3. LIST OF EXCIPIENTS Sodium bicarbonate (E500) 4. PHARMACEUTICAL FORM AND CONTENTS Powder for solution for infusion 5. METHOD AND ROUTE(S) OF ADMINISTRATION Read the package leaflet before use. IV. Single use. 6. SPECIAL WARNING THAT THE MEDICINAL PRODUCT MUST BE STORED OUT OF
THE REACH AND SIGHT OF CHILDREN Keep out of the reach and sight of children. 7. OTHER SPECIAL WARNING(S), IF NECESSARY 8. EXPIRY DATE EXP
32

9. SPECIAL STORAGE CONDITIONS Do not store above 25C After reconstitution: Use within 2 hours. Do not freeze. 10. SPECIAL PRECAUTIONS FOR DISPOSAL OF UNUSED MEDICINAL PRODUCTS OR
WASTE MATERIALS DERIVED FROM SUCH MEDICINAL PRODUCTS, IF APPROPRIATE
11. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and Address} <{tel}> <{fax}> <{e-mail}> 12. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 13. BATCH NUMBER Lot 14. GENERAL CLASSIFICATION FOR SUPPLY [To be completed nationally] 15. INSTRUCTIONS ON USE 16. INFORMATION IN BRAILLE
33

PACKAGE LEAFLET
34
PACKAGE LEAFLET: INFORMATION TO THE USER
TIENAM and associated names (see Annex I) 500 mg/500 mg powder for solution for infusion
[See Annex I - To be completed nationally]
imipenem/cilastatin
Read all of this leaflet carefully before you start using this medicine. - Keep this leaflet. You may need to read it again. - If you have further questions, ask your doctor or pharmacist. - This medicine has been prescribed for you. Do not pass it on to others. It may harm them, even if
their symptoms are the same as yours. - If any of the side effects gets serious, or if you notice any side effects not listed in this leaflet, please
tell your doctor or pharmacist. In this leaflet: 1. What TIENAM is and what it is used for 2. Before you use TIENAM 3. How to use TIENAM 4. Possible side effects 5. How to store TIENAM 6. Further information 1. WHAT TIENAM IS AND WHAT IT IS USED FOR TIENAM belongs to a group of medicines called carbapenem antibiotics. It kills a wide range of bacteria (germs) that cause infections in various parts of the body in adults and children one year of age and above. Treatment Your doctor has prescribed TIENAM because you have one (or more) of the following types of infection: Complicated infections in the abdomen Infection affecting the lungs (pneumonia) Infections that you can catch during or after the delivery Complicated urinary tract infections Complicated skin and soft tissue infections TIENAM may be used in the management of patients with low white blood cell counts, who have fever that is suspected to be due to a bacterial infection. TIENAM may be used to treat bacterial infection of the blood which might be associated with a type of infection mentioned above. 2. BEFORE YOU USE TIENAM Do not use TIENAM - if you are allergic (hypersensitive) to imipenem, cilastatin or any of the other ingredients of
TIENAM - if you are allergic (hypersensitive) to other antibiotics such as penicillins, cephalosporins, or
carbapenems
35

Take special care with TIENAM Tell your doctor about any medical condition you have or have had including: - allergies to any medicines including antibiotics (sudden life-threatening allergic reactions require
immediate medical treatment) - colitis or any other gastrointestinal disease - any central nervous system disorders such as localized tremors or epileptic seizures - liver, kidney or urinary problems You may develop a positive test (Coombs test) which indicates the presence of antibodies that may destroy red blood cells. Your doctor will discuss this with you. Tell your doctor if you are taking medicines called valproic acid or sodium valproate (see Using other medicines below). Children TIENAM is not recommended in children less than one year of age or children with kidney problems. Using other medicines Please tell your doctor or pharmacist if you are taking or have recently taken any other medicines, including those obtained without a prescription. Tell your doctor if you are taking ganciclovir which is used to treat some viral infections. Also, tell your doctor if you are taking valproic acid or sodium valproate (used to treat epilepsy, bipolar disorder, migraine, or schizophrenia) or any blood thinners such as warfarin. Your doctor will decide whether you should use TIENAM in combination with these medicines. Pregnancy and breast-feeding It is important that you tell your doctor if you are pregnant or are planning to become pregnant before receiving TIENAM. TIENAM has not been studied in pregnant women. TIENAM should not be used during pregnancy unless your doctor decides the potential benefit justifies the potential risk to the foetus. It is important that you tell your doctor if you are breast-feeding or if you intend to breast-feed before receiving TIENAM. Small amounts of this medicine may pass into breast milk and it may affect the baby. Therefore, your doctor will decide whether you should use TIENAM while breast-feeding. Ask your doctor or pharmacist for advice before taking any medicine. Driving and using machines There are some side effects associated with this product (such as seeing, hearing, or feeling something that is not there, dizziness, sleepiness, and a spinning sensation) that may affect some patients' ability to drive or operate machinery (see section 4). Important information about some of the ingredients of TIENAM This medicinal product contains approximately 1.6 mEq (approximately 37.6 mg) of sodium per 500 mg dose which should be taken into consideration by patients on a controlled sodium diet.
36
3. HOW TO USE TIENAM TIENAM will be prepared and given to you by a doctor or another health care professional. Your doctor will decide how much TIENAM you need. Adults and adolescents The usual dose of TIENAM for adults and adolescents is 500 mg/500 mg every 6 hours or 1,000 mg/1,000 mg every 6 or 8 hours. If you have kidney problems or weigh less than 70 kg, your doctor may lower your dose. Children The usual dose for children one year of age or older is 15/15 or 25/25 mg/kg/dose every 6 hours. TIENAM is not recommended in children under one year of age and children with kidney problems. Method of administration TIENAM is given intravenously (into a vein) over 20-30 minutes for a dose of ≤500 mg/500 mg or 40-60 minutes for a does of >500 mg/500 mg. If you use more TIENAM than you should Symptoms of overdose may include seizures, confusion, tremors, nausea, vomiting, low blood pressure and slow heart rate. If you are concerned that you may have been given too much TIENAM, contact your doctor or another healthcare professional immediately. If you forget to use TIENAM If you are concerned that you may have missed a dose, contact your doctor or another healthcare professional immediately. Do not take a double dose to make up for a forgotten dose. If you stop using TIENAM Do not stop using TIENAM until your doctor tells you to. If you have any further questions on the use of this product, ask your doctor or pharmacist. 4. POSSIBLE SIDE EFFECTS Like all medicines, TIENAM can cause side effects, although not everybody gets them. The frequency of possible side effects listed below is defined using the following convention: very common: affects more than 1 user in 10 common: affects 1 to 10 users in 100 uncommon: affects 1 to 10 users in 1,000 rare: affects 1 to 10 users in 10,000 very rare: affects less than 1 user in 10,000 not known: frequency cannot be estimated from the available data
37
Common Nausea, vomiting, diarrhoea. Nausea and vomiting appear to occur more frequently in patients with
low number of white blood cells Swelling and redness along a vein which is extremely tender when touched Rash Abnormal liver function detected by blood tests Increase in some white blood cells Uncommon Local skin redness Local pain and formation of a firm lump at the injection site Skin itchiness Hives Fever Blood disorders affecting the cell components of the blood and usually detected by blood tests
(symptoms may be tiredness, paleness of skin, and prolonged bruising after injury) Abnormal kidney, liver and blood function detected by blood tests Tremors and uncontrolled twitching of muscles Seizures Psychic disturbances (such as mood swings and impaired judgment) Seeing, hearing or feeling something that is not there (hallucinations) Confusion Dizziness, sleepiness Low blood pressure Rare Allergic reactions including rash, swelling of the face, lips, tongue and/or throat (with difficulty in
breathing or swallowing), and/or low blood pressure. If these side-effects occur while receiving or after receiving TIENAM, the medicine must be stopped and your doctor contacted immediately.
Skin peeling (toxic epidermal necrolysis) Severe skin reactions (Stevens-Johnson syndrome and erythema multiforme) Severe skin rash with loss of skin and hair (exfoliative dermatitis) Fungal infection (candidiasis) Staining of the teeth and/or tongue Inflammation of the colon with severe diarrhoea Disturbances in taste Inability of the liver to perform normal function Inflammation of the liver Inability of the kidney to perform normal function Changes in the amount of urine, changes in urine colour Disease of the brain, tingling sensation (pins and needles), localised tremor Hearing loss Very rare Severe loss of liver function due to inflammation (fulminant hepatitis) Inflammation of stomach or intestine (gastro-enteritis) Inflammation of intestine with bloody diarrhoea (haemorrhagic colitis)
38

Red swollen tongue, overgrowth of the normal projections on the tongue giving it a hairy appearance, heartburn, sore throat, increase in the production of saliva
Stomach pain A spinning sensation (vertigo), headache Ringing in the ears (tinnitus) Pain in several joints, weakness Irregular heartbeat, the heart beating forcefully or rapidly Chest discomfort, difficulty breathing, abnormally fast and superficial breathing, pain in the upper
spine Flushing, bluish discoloration of the face and lips, skin texture changes, excessive sweating Itching of the vulva in women Changes in the amounts of blood cells Worsening of a rare disease associated with muscle weakness (aggravation of myasthenia gravis) If any of the side effects gets serious, or if you notice any side effects not listed in this leaflet, please tell your doctor or pharmacist. 5. HOW TO STORE TIENAM Keep out of the reach and sight of children. Do not use TIENAM after the expiry date stated on the container. The expiry date refers to the last day of that month. Do not store above 25 C. After reconstitution: Diluted solutions should be used immediately. The time interval between the beginning of reconstitution and the end of intravenous infusion should not exceed two hours. Do not freeze the reconstituted solution. Medicines should not be disposed of via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. These measures will help to protect the environment. 6. FURTHER INFORMATION What TIENAM contains - The active substances are imipenem and cilastatin. Each vial contains imipenem monohydrate
equivalent to 500 mg imipenem and cilastatin sodium equivalent to 500 mg cilastatin. - The other ingredient is sodium bicarbonate. What TIENAM looks like and contents of the pack TIENAM is a white to light yellow powder for solution for infusion in a glass vial. Pack sizes of 1, 10 or 25 vials. Not all pack sizes may be marketed. Marketing Authorization Holder and Manufacturer [See Annex I - To be completed nationally]
39
This medicinal product is authorised in the Member States of the EEA under the following names: Austria: Zienam Belgium: Tienam Bulgaria: Tienam Czech Republic: Tienam Estonia: TIENAM I.V. Finland: TIENAM France: TIENAM Germany: ZIENAM Greece: Primaxin Hungary: Tienam Iceland: Tienam Ireland: Primaxin IV Italy: TIENAM (20 ml), IMIPEM (20 ml) and TENACID (20 ml) Latvia: TIENAM I.V. Lithuania: TIENAM I.V. Luxembourg: Tienam Malta: Primaxin IV Netherlands: TIENAM I.V. Norway: Tienam Poland: TIENAM Portugal: Tienam IV Romania: TIENAM IV Slovak Republic: TIENAM i.v. Slovenia: CONET Spain: TIENAM IV Sweden: Tienam United Kingdom: Primaxin IV This leaflet was last approved in {MM/YYYY}. [To be completed nationally] ----------------------------------------------------------------------------------------------------------------------------- The following information is intended for medical or healthcare professionals only: Each vial is for single use only. Reconstitution Contents of each vial must be transferred to 100 ml of an appropriate infusion solution (see Incompatibility and After reconstitution): 0.9% sodium chloride. In exceptional circumstances where 0.9% sodium chloride cannot be used for clinical reasons, 5% glucose may be used instead. A suggested procedure is to add approximately 10 ml of the appropriate infusion solution to the vial. Shake well and transfer the resulting mixture to the infusion solution container. CAUTION: THE MIXTURE IS NOT FOR DIRECT INFUSION. Repeat with an additional 10 ml of infusion solution to ensure complete transfer of vial contents to the infusion solution. The resulting mixture should be agitated until clear.
40

41
The concentration of the reconstituted solution following the above procedure is approximately 5 mg/ml for both imipenem and cilastatin. Variations of colour, from colourless to yellow, do not affect the potency of the product. Incompatibility This medicinal product is chemically incompatible with lactate and should not be reconstituted in diluents containing lactate. However, it can be administered into an I.V. system through which a lactate solution is being infused. This medicinal product must not be mixed with other medicinal products except those mentioned under Reconstitution. After reconstitution Diluted solutions should be used immediately. The time interval between the beginning of reconstitution and the end of intravenous infusion should not exceed two hours. Any unused product or waste material should be disposed of in accordance with local requirements.