timothy duerlers 2013 african journey
TRANSCRIPT

Timothy Duerler’s 2013 African Journey
In May of 2013 I embarked on a short trip to South Africa and Swaziland on behalf of our newly formed Mango Foundation, to understand more about the locations and people that we are supporting.
Monday:
! I arrived through Johannesburg airport after a 40 hours travel time from Kailua-Kona via Los Angeles and London. I rented a small SUV, proceeded to head out of the airport and immediately starting driving on the right side of the road, which is the wrong side to drive on in South Africa. I also managed to get lost in some not so nice parts of Johannesburg due to a not functioning GPS and was shooting myself for renting the less expensive manual transmission vehicle, which I am okay driving but not used to shifting with my left hand and sitting on right hand side drivers seat. Nonetheless I survived and headed to my first destination the Acts HIV/AIDs clinic near White River in the Mpumalunga District of South Africa. I arrived later than planned and was shown my hostel accommodations on the campus of the clinic.
! The Acts Clinic is a set in a picturesque hilly setting in the northeast part of South Africa close to several popular tourist areas such as Kruger National Park, the oldest and largest game reserve in southern Africa. It was founded in 2000 by a local doctor that was tired of seeing HIV patients continuously dying and started with a hospice program. This clinic has grown over the years to now include all kinds of services from home and community based care and outreach, outpatient primary care services, mother and child services, maternity care, cancer screening services such as pap smears and even colposcopies and treatment of cervical dysplasia and HIV and TB treatment. It currently counts 12,000 patients with at least 7,000 of them actively following up for care and treatment. The sad part is that there is a local hospital 15km away that sees just as many or more HIV(+) patients and it continues like this around the country.
! The Acts Clinic works as a regional referral center for the surrounding government clinics for those complicated patients that they cannot manage. In South Africa, especially in rural areas there are not enough doctors and they work exclusively in the local hospitals. The clinics are staffed by nurses at best and are often not trained to handle the complex cases caused by HIV/AIDs and also often concurrent tuberculosis. There were several community-based counselors there receiving training that will then go back to their communities in the surrounding regions. They conduct rapid HIV testing and then counsel those that are positive. I was speaking to one gentlemen and he recalls one particularly difficult day where he tested 8 people and 6 of

them were positive. This echoes the official statistics by the South African government that now places this province, Mpumalunga, with the highest incidence of HIV, 52% of the entire population.
Tuesday:
! I spent one day with Dr. Ravital Kahlon as she made her rounds and worked with the patients. She assured me my experience was a typical day for her as she averages
40-50patients/day in the clinics plus inpatient and short-stay calls and various other duties. She was originally from Israel but moved at a young age to South Africa and completed her medical school training there. She had made a decision to work in the rural areas with the HIV population. She admitted to taking a pay cut to work with an NGO like Acts Clinic but was happy with her decision and was extremely frustrated with the government run clinics and hospitals. She felt they were poorly organized, understaffed, and the doctors were run ragged in
the system with little ability to change it. She states as a doctor in a rural South African hospital you worked exclusively in the hospital with 1-2days a week where you were on call for 30hours straight. During this time, you were busy nonstop from emergency calls, surgeries, general anesthesia and more and more, it never stopped. The rest of the time you were busy as well trying to work in an understaffed, overcrowded, poorly organized hospital and manage a large surrounding areas community clinics.
! Our day started out at 7:30am with everyone gathering in the central courtyard at the Acts Clinic and singing praise and worship songs and then scripture readings in both English and Siswati. We ducked out a bit early to go do morning rounds at the IPU (inpatient unit). This was a short drive away from the Acts clinic itself in a surrounding neighborhood of small cinder block homes and dirt roads. There were 11 beds in the small cinder block building with 7 of them currently occupied. Ailments ranged from severe cases of herpes zoster to active concurrent TB and AIDs to unknown diagnoses of severe headaches and concern for TB meningitis. The rooms were small with 3-6 patients in each room. For TB control they used the open air ventilation method meaning you kept the windows open and didn’t shut them. There were no masks or isolation wards. The one lady whose name was Promise, who was complaining of severe headache and neck stiffness Dr. Ravi wanted to do a lumbar puncture on but
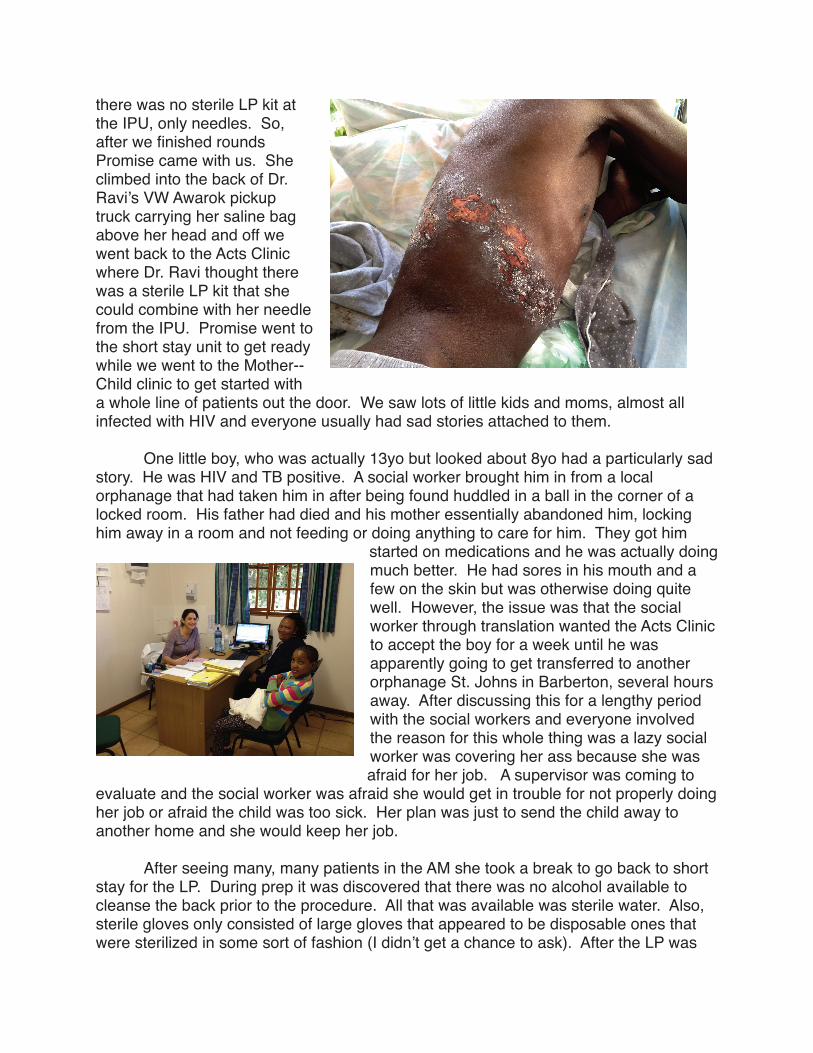
there was no sterile LP kit at the IPU, only needles. So, after we finished rounds Promise came with us. She climbed into the back of Dr. Ravi’s VW Awarok pickup truck carrying her saline bag above her head and off we went back to the Acts Clinic where Dr. Ravi thought there was a sterile LP kit that she could combine with her needle from the IPU. Promise went to the short stay unit to get ready while we went to the Mother--Child clinic to get started with a whole line of patients out the door. We saw lots of little kids and moms, almost all infected with HIV and everyone usually had sad stories attached to them.
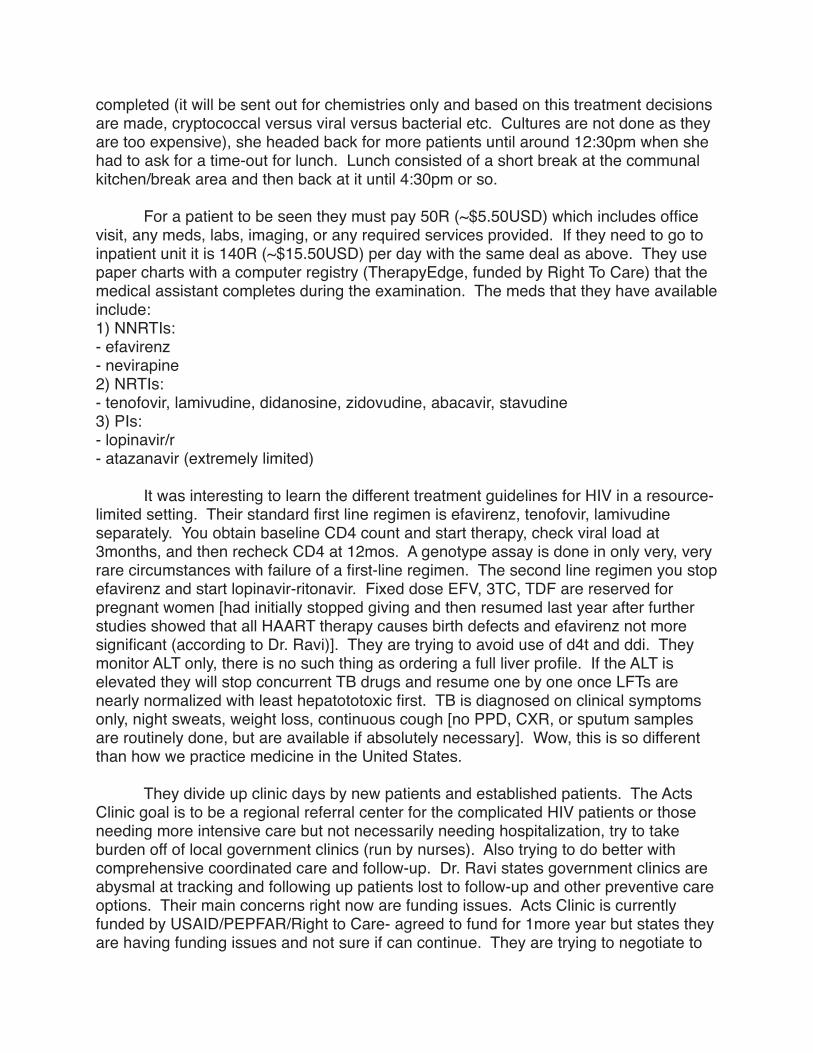
! One little boy, who was actually 13yo but looked about 8yo had a particularly sad story. He was HIV and TB positive. A social worker brought him in from a local orphanage that had taken him in after being found huddled in a ball in the corner of a locked room. His father had died and his mother essentially abandoned him, locking him away in a room and not feeding or doing anything to care for him. They got him
started on medications and he was actually doing much better. He had sores in his mouth and a few on the skin but was otherwise doing quite well. However, the issue was that the social worker through translation wanted the Acts Clinic to accept the boy for a week until he was apparently going to get transferred to another orphanage St. Johns in Barberton, several hours away. After discussing this for a lengthy period with the social workers and everyone involved the reason for this whole thing was a lazy social worker was covering her ass because she was afraid for her job. A supervisor was coming to
evaluate and the social worker was afraid she would get in trouble for not properly doing her job or afraid the child was too sick. Her plan was just to send the child away to another home and she would keep her job.
! After seeing many, many patients in the AM she took a break to go back to short stay for the LP. During prep it was discovered that there was no alcohol available to cleanse the back prior to the procedure. All that was available was sterile water. Also, sterile gloves only consisted of large gloves that appeared to be disposable ones that were sterilized in some sort of fashion (I didn’t get a chance to ask). After the LP was
completed (it will be sent out for chemistries only and based on this treatment decisions are made, cryptococcal versus viral versus bacterial etc. Cultures are not done as they are too expensive), she headed back for more patients until around 12:30pm when she had to ask for a time-out for lunch. Lunch consisted of a short break at the communal kitchen/break area and then back at it until 4:30pm or so.
! For a patient to be seen they must pay 50R (~$5.50USD) which includes office visit, any meds, labs, imaging, or any required services provided. If they need to go to inpatient unit it is 140R (~$15.50USD) per day with the same deal as above. They use paper charts with a computer registry (TherapyEdge, funded by Right To Care) that the medical assistant completes during the examination. The meds that they have available include:1) NNRTIs:- efavirenz- nevirapine2) NRTIs:- tenofovir, lamivudine, didanosine, zidovudine, abacavir, stavudine3) PIs:- lopinavir/r- atazanavir (extremely limited)
! It was interesting to learn the different treatment guidelines for HIV in a resource-limited setting. Their standard first line regimen is efavirenz, tenofovir, lamivudine separately. You obtain baseline CD4 count and start therapy, check viral load at 3months, and then recheck CD4 at 12mos. A genotype assay is done in only very, very rare circumstances with failure of a first-line regimen. The second line regimen you stop efavirenz and start lopinavir-ritonavir. Fixed dose EFV, 3TC, TDF are reserved for pregnant women [had initially stopped giving and then resumed last year after further studies showed that all HAART therapy causes birth defects and efavirenz not more significant (according to Dr. Ravi)]. They are trying to avoid use of d4t and ddi. They monitor ALT only, there is no such thing as ordering a full liver profile. If the ALT is elevated they will stop concurrent TB drugs and resume one by one once LFTs are nearly normalized with least hepatototoxic first. TB is diagnosed on clinical symptoms only, night sweats, weight loss, continuous cough [no PPD, CXR, or sputum samples are routinely done, but are available if absolutely necessary]. Wow, this is so different than how we practice medicine in the United States.
! They divide up clinic days by new patients and established patients. The Acts Clinic goal is to be a regional referral center for the complicated HIV patients or those needing more intensive care but not necessarily needing hospitalization, try to take burden off of local government clinics (run by nurses). Also trying to do better with comprehensive coordinated care and follow-up. Dr. Ravi states government clinics are abysmal at tracking and following up patients lost to follow-up and other preventive care options. Their main concerns right now are funding issues. Acts Clinic is currently funded by USAID/PEPFAR/Right to Care- agreed to fund for 1more year but states they are having funding issues and not sure if can continue. They are trying to negotiate to
get funding from South African government but a long and lengthy process and so far no commitments.
Swaziland and Acts II
! Next, I traveled from the Acts Clinic near White River in South Africa through Nelspruit to Badplaas and then through Osheok to Swaziland. It is a scenic drive through wide sweeping valleys with large orchards of oranges and steep winding roads up and down mountain passes. It is not unlike many other places around the world except by a few sights that punctuate the reminder that you are in Africa. The man standing at the street corner in the middle of a shopping district in White River with his arms outstretched in front of him walking between cars with 2 large snakes extending 2 feet further beyond his clenched hands. I still haven’t found out what this story is about and I didn’t stop to take a picture. Part of the road traveled was a nice toll highway with very modern rest stops. I would give it my favorite restroom award because as you stand in front of the urinal you are able to look out through the large eye level windows to the field stretched out in front of you filled with ostrich, springbok, impala, wildebeest, and rhinos.
! I had to make two stops, the first one at a local college to pickup some vitamins for the children at the New Hope Centre orphanage. I had five large boxes but was informed multiple times it was much better if I did not declare these at the border entering Swaziland. So I neatly tucked these into the back of my rented Hyundai SUV and placed my duffel bags on top and neatly went on my way. “Just on holiday” at the border and within 10minutes whisked right into Swaziland with nary a word of the vitamins. The other stop was in the town of Badplaas close to the border with Swaziland. This stop was rather uneventful as I was just picking up a large suitcase filled with children’s clothes from a retired missionary nurse named Jane, however she did have a rather interesting story.
! Originally I was supposed to pick her up and we would travel on together into Swaziland. However, she had to stay behind as she was trying to recover her stolen Land Rover. She relayed the dangers with crime, murder, theft, rape in the area and this unfortunately was repeated across my travels. Her Land Rover was stolen nearly a year prior and she knew exactly where it was, right down the road in the hands of a local machine shop owner who also rented vehicles to unsuspecting tourists going into the nearby game parks, one being a very nice Land Rover. Despite this knowledge, which the local police also knew, it had taken a year and still was slowly, ever so slowly winding its way through the court system and at least part of the delay was a poor overworked solo police detective for a large region where these sorts of thefts were so commonplace. I saw this again and again during my travels and couldn’t help but notice
the bars on windows, doors, manned gates, and security patrols 24/7 that were necessary if you didn’t want to be a victim of petty crimes or worse.
! So I drove onward into Swaziland on the very nice paved tar road that wound itself up into the hills of Mbabane and then down again into the valleys and onto Matsapha which was to be my stop for the night as I was staying at the New Hope Centre. Unfortunately the two stops and construction delays had caused me to be quite late and I found myself arriving after dark. This worried me as I had never been here before and my directions for arrival were “exit at Matsapha, take 3rd left off of roundabout, cross the stream with the hippo in it and continue for 4km until you see sign on right for New Hope Centre. Turn right onto unpaved road, continue for 2km until splits and continue left and then left again, honk twice when you get to gate. Note if it is raining road may not be accessible.” Nonetheless, somehow I found the gate and sure enough it opened with 2 honks of a horn. A few children emerged from the building and then they called for Samuel. Samuel was my sponsoree and I immediately recognized him from the pictures. To sponsor a child fully is to provide $120USD/month that provides for almost all basic needs for that child. It covers food, clothing, shelter, education, and others for that child. As I was soon to discover the education is top notch as we are seeing the older children now going off to become lawyers, doctors, pilots and several other professions. They instill a desire within the children to learn and a belief that they can do whatever they desire and find a way to make that dream happen. This is often difficult as education, especially in neighboring countries such as South Africa or other places abroad can be quite expensive. However, they trust that God will provide and “He always has” says the founder Dr. Elizabeth Hynd, either with donations or other unexpected ways that funds become available.
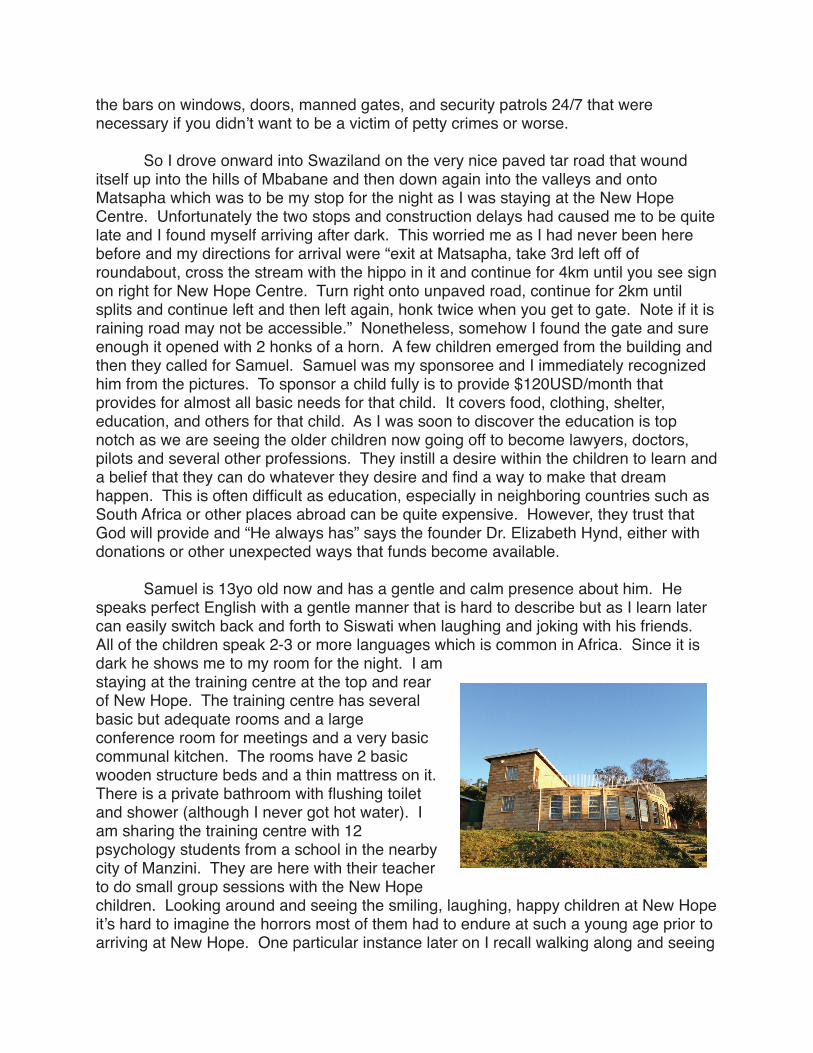
! Samuel is 13yo old now and has a gentle and calm presence about him. He speaks perfect English with a gentle manner that is hard to describe but as I learn later can easily switch back and forth to Siswati when laughing and joking with his friends. All of the children speak 2-3 or more languages which is common in Africa. Since it is dark he shows me to my room for the night. I am staying at the training centre at the top and rear of New Hope. The training centre has several basic but adequate rooms and a large conference room for meetings and a very basic communal kitchen. The rooms have 2 basic wooden structure beds and a thin mattress on it. There is a private bathroom with flushing toilet and shower (although I never got hot water). I am sharing the training centre with 12 psychology students from a school in the nearby city of Manzini. They are here with their teacher to do small group sessions with the New Hope children. Looking around and seeing the smiling, laughing, happy children at New Hope it’s hard to imagine the horrors most of them had to endure at such a young age prior to arriving at New Hope. One particular instance later on I recall walking along and seeing