tissue engineering of heart valves: advances and current ... › mate › pdfs › 10563.pdf ·...
TRANSCRIPT
259
Review
www.expert-reviews.com ISSN 1743-4440© 2009 Expert Reviews Ltd10.1586/ERD.09.12
Heart valve diseasesValvular heart disease represents a major public-health problem causing significant morbidity and mortality worldwide [1,2]. In developing countries, heart valve diseases affect mainly pediatric and young-adult patients as a result of the persistent burden of rheumatic fever [3,4]. In industrialized nations, the most common etiol-ogy of valve disease has shifted from rheumatic towards a degenerative pathology [5,6], affecting predominantly the elderly. Prevalence shows an increasing trend with increasing age and at least one in eight people aged 75 years and older suffer from a form of valve disease. From this perspective, the social and economic burden of valvular heart disease will continue to increase with the continuous growth and aging of the world’s population [1].
The main causes of cardiac valve dysfunction are calcification of the leaflets, endocarditis, rheumatic fever, myxomatous degeneration or congenital malformations, leading to stenosis or insufficiency of the valve. Valve dysfunction may affect each of the four valves in the heart, but the left-sided valves are particularly susceptible to dysfunction due to the harsh hemodynamic conditions of the systemic circulation in which they function. From a clinical point of view, heart valve repair is preferable to replacement,
depending on the nature and progression of the pathology, as well as patient-related factors, such as age and comorbidities [7]. However, despite an assortment of possible restorative maneuvers [8], 70% of diseased valves are not suitable for repair [9]. Approximately 290,000 heart valve replace-ments are performed annually worldwide and the number of patients requiring valve replace-ment is estimated to triple over the upcoming five decades [10,11].
Heart valve replacementsCurrent available heart valve prostheses are cate-gorized into mechanical or bioprosthetic replace-ment valves. Mechanical valves offer excellent structural durability, but are inherently prone to thromboembolic events due to high shear stress, nonphysiological flow profile and blood damage [4]. Therefore, patients receiving a mechanical prosthesis are committed to daily anticoagula-tion therapy, which results in an increased risk of serious hemorrhage complications. Bioprostheses are more susceptible to structural valve degen-eration, and the associated need for reoperation makes them less suitable for middle-aged and younger patients. Current clinical guidelines recommend the use of a bioprosthetic valve in patients aged 65 years and older [12], supported by large, randomized clinical trials [13,14], and
Anita Mol†, Anthal IPM Smits, Carlijn VC Bouten and Frank PT Baaijens†Author for correspondenceDepartment of Biomedical Engineering, Eindhoven University of Technology, PO Box 513, 5600 MB, Eindhoven, The NetherlandsTel.: +31 402 473 048Fax: +31 402 447 [email protected]
It is estimated that the number of patients requiring heart valve replacement will triple over the next five decades. None of the current replacement valves can fully restore native valve function because they lack growth and remodeling capabilities. Heart valve tissue engineering is a promising technology to overcome these limitations. Various approaches are being employed, either aimed at development of the valve substitute in vitro or at the use of the regenerative potential of the body (in situ) for the tissue culture phase. This review provides an overview of the progress within both the in vitro and in situ tissue engineering approaches for trileaflet heart valve tissue engineering. Current challenges with these approaches are discussed, focusing in particular on the use of synthetic scaffold materials.
Keywords: cardiovascular • cells • extracellular • heart valve • in vitro • in vivo • matrix • scaffold • tissue engineering
Tissue engineering of heart valves: advances and current challengesExpert Rev. Med. Devices 6(3), 259–275 (2009)
For reprint orders, please contact [email protected]

Expert Rev. Med. Devices 6(3), (2009)260
Review Mol, Smits, Bouten & Baaijens
studies on the long-term effects of valve prostheses in terms of mortality and valve-related complications [15–17]. Despite these guidelines, recent developments have aroused some controversy regarding the appropriate valve choice for each individual patient. With the development of improved design and conservation meth-ods to enhance the durability of bioprostheses, there has tended to be a shift towards bioprosthetic valves as the preferred substitute valve in middle-aged patients. However, long-term performance of these third-generation bioprostheses is yet to be evaluated, and randomized clinical trials should elucidate whether or not this trend is justified. Bearing in mind the longer lifespan of the gen-eral population, the need for reoperation after bioprosthetic valve replacement seems inevitable in the long run [18,19]. With respect to mechanical valve replacements, the recently suggested patient-specific method for self-management of anticoagulation allows for a substantially lower and more suitable anticoagulation dose. This results in reduced risks of hemorrhage complications without increasing the risk of thromboembolism [20,21], which may render mechanical prostheses the more favorable substitute valves. For the pediatric patient group, in which repeated valve replacements are often necessitated, the diseased aortic valve is often replaced with its native living counterpart, the pulmonary valve. This procedure, referred to as the Ross procedure, has shown great promise in this age group. However, recent studies have indicated possible fail-ure of those valves, associated with tissue composition alterations due to exposure of the valve to increased biomechanical demands [22–25]. In addition, the transferred pulmonary valve still needs to be replaced, and the risks associated with the replacement valve and repeated surgery remain.
Selection of the appropriate heart valve prosthesis should be dependent on individually specified patient characteristics, such as life expectancy, tolerance to the need for reoperative valve replace-ment and the use of anticoagulants with its associated changes in lifestyle [26]. Survival and quality of life after heart valve replace-ment are primarily conditional upon patient-related factors, such as age, ventricular function and potential comorbidities. Although currently applicable heart valve prostheses significantly improve life expectancy, patient longevity after valvular surgery still remains inferior compared with age-matched healthy individu-als [27]. This underlines that the current options for heart valve replacements are suboptimal for a substantial group of patients [10], and that the ideal prosthetic valve has yet to be developed.
Polymeric flexible-leaflet valves have been put forward as an alternative valve replacement to combine the hemodynamic per-formance of a bioprosthetic valve with the durability of a mechan-ical valve. Initially, however, these valve types comprised the worst of both worlds, with a highly thrombogenic surface subjected to high rates of material degradation [4]. The development of innova-tive synthetic materials and optimized prosthesis design has led to enhanced hemodynamic compatibility and fatigue resistance, as well as improved biostability [28–31]. Despite these improvements, even the latest generation of polymeric valves have proven to be liable to some degree of extrinsic calcification in relatively short-term animal studies [28–30], which raises doubts regarding their long-term durability and in vivo functionality.
The native heart valve is a living, dynamic tissue capable of continuous remodeling to adapt to its hemodynamic environment [32]. None of the current replacement valves can fully restore native valve function because they inherently lack these adaptive capa-bilities. This will also ultimately affect cardiac function. Heart valve tissue engineering represents an evolving field of research, which has the potential to overcome these limitations by creating a living autologous valve replacement that prevents an immune response and allows for growth, remodeling and repair during a patient’s lifetime.
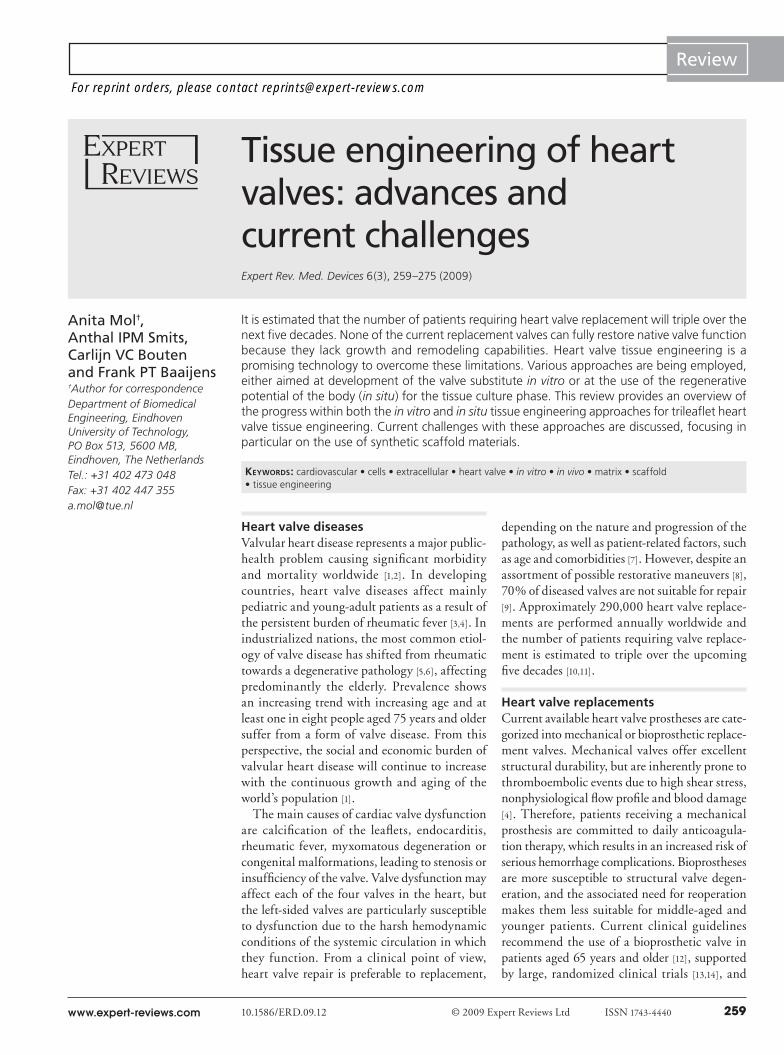
Heart valve tissue engineering paradigmThe first steps towards the development of the intriguing field of cardiovascular tissue engineering were made by cardiovascular sur-geons in the 1970s by studying the use of autologous cells to line the surfaces of cardiovascular prostheses [33,34]. In the early 1990s, lining of biological heart valve replacements was also shown to be feasible [35]. In 1993, Langer and Vacanti defined the term ‘tissue engineering’ as an interdisciplinary field, applying the principles and methods of engineering to the development of biological sub-stitutes that can restore, maintain or improve tissue function [36]. The original tissue engineering paradigm, as defined by Langer and Vacanti, comprises the isolation and expansion of cells from the patient, subsequent seeding onto an appropriate scaffold material, in vitro tissue formation and, finally, implantation into the patient from whom the cells were taken. In this review, only approaches that make use of a porous scaffold material that are the subject of in vivo degradation and/or remodeling are considered within the term tissue engineering. This paradigm, further referred to as the in vitro tissue engineering approach, is being employed for heart valve tissue engineering and is aimed at full development of the tissue substitute in vitro. Adjustments to this paradigm, omitting some of the described steps, are also being employed for heart valve tissue engineering. In general, the adjustments comprise bypassing the in vitro tissue culture phase. Therefore, this approach is further referred to as in situ tissue engineering and is aimed at the use of the regenerative potential of the body for the tissue culture phase. Both approaches are depicted schematically in Figure 1.
This review provides an overview of the progress within both the in vitro and in situ tissue engineering approaches for trileaflet heart valve tissue engineering. Furthermore, current challenges within the approaches are discussed, focusing in particular on the use of synthetic scaffold materials.
In vitro heart valve tissue engineeringIn vitro tissue engineering encompasses the full tissue engineering paradigm and incorporates an in vitro tissue culture phase. Heart valves are being engineered according to this approach using a variety of scaffold materials and cell sources. The most obvious choice for a scaffold material in heart valve tissue engineering is a xenograft or homograft, depleted of cells and cellular components, possessing a native-like geometry and structure with mechanical and physiological hemodynamics equal to its native counterpart. Conventional glutaraldehyde fixation, which is used to mask immunogenic epitopes, blocks cellular ingrowth, rendering these
www.expert-reviews.com 261
ReviewTissue engineering of heart valves: advances & current challenges
Cells ScaffoldBioreactor conditioning
Tissue formation ImplantationA
Scaffold ImplantationC
Cells Scaffold ImplantationB
Figure 1. In vitro and in situ heart valve tissue engineering approaches. (A) The in vitro tissue engineering approach encompasses the full tissue engineering paradigm and is aimed at development of the valve replacement in vitro, always incorporating an in vitro tissue culture phase. (B & C) The in situ tissue engineering approach encompasses just some of the aspects of the tissue engineering paradigm, bypassing the in vitro tissue culture phase. The in situ heart valve tissue engineering approach is aimed at the use of the regenerative potential of the body for the tissue culture phase.

Expert Rev. Med. Devices 6(3), (2009)262
Review Mol, Smits, Bouten & Baaijens
grafts unsuitable for in vitro or in situ tissue engineering [32]. As an alternative, various decellularization techniques are being studied extensively in an effort to suppress the immunogenic potential of such biological matrices. It is crucial to remove all cellular compo-nents, and the decellularization treatment should not harm or alter the matrix properties. Efficiency of cell removal, as well as preserva-tion of the matrix integrity, is highly dependent on the decellular-ization method used [37]. Nonenzymatic detergent-based methods, such as sodium deoxycholate- or sodium dodecyl sulfate-based treatments, have been reported to result in much more efficient cell removal, while maintaining matrix integrity when compared with decellularization with more aggressive agents, such as trypsin/eth-ylenediaminetetraacetic acid (EDTA) [37,38]. For either decellular-ization method, disruptions in the matrix microstructure may lead to changes in leaflet mechanical properties despite preservation of gross fiber architecture [39]. While such decellularized matrices are used mainly in the in situ tissue engineering approach, as described later in this review, they can also be repopulated with cells and cultured in vitro according to the full tissue engineering paradigm to induce autologous tissue formation before implantation [40–43].
Implantation of decellularized valves repopulated with autologous vascular cells as pulmonary valve replacement in sheep has shown promising results, although thickening of the leaflets was apparent [44]. Similarly, such decellularized valves repopulated with autologous bone marrow-derived cells and implanted as aortic valve replacement in dogs have demonstrated partly repopulated and endothelialized tissues after 3 weeks [45]. The originally seeded cells were still pres-ent in all cases after explantation, indicating the contribution of the seeded cells to the tissue regeneration process. Despite the fact that decellularized xenografts or homografts may be the most obvious choice as a scaffold for heart valve tissue engineering, there are major drawbacks in the use of such matrices as a scaffold material. When the matrices are of xenogeneic origin, the risks of zoonoses exist, although it is argued that these risks are minimal [46]. When using homografts for human use, the limited availability of donor valves is still an unsolved problem. In addition, the use of homografts in tissue engineering approaches may raise ethical concerns as these are functional valve replacements. Furthermore, remodeling and growth have not yet been demonstrated when using such valves, which is a prerequisite for future use in children and young adults.
To increase the potential for growth and remodeling, synthetic scaffolds are most commonly used in the in vitro heart valve tis-sue engineering approach. Synthetic biodegradable materials, such as polyglycolic acid (PGA), polylactic acid (PLA), poly-4-hydroxybutyrate (P4HB) and polycaprolactone (PCL) are the main materials of choice. These are all biocompatible materials that vary in their rates of degradation and manufacturing possibilities. PGA degrades at the fastest rate, in weeks, while PCL degrades over years. The first successful replacement of a single pulmonary valve leaflet with an in vitro tissue-engineered equivalent, based on a syn-thetic scaffold, was demonstrated in lambs in 1995 [47–49]. A couple of years later, full trileaflet valve replacements were fabricated based on synthetic scaffolds. These were shown to be fully remodeled in sheep into native-like tissue structures with proper functioning up to 8 months [50–52]. In that time, mechanical conditioning as
a strategy to improve and accelerate the in vitro culture phase was developed for trileaflet tissue-engineered valves by exposure of the growing tissues to increasing amounts of pulsatile flows and stretch [53]. These valves, cultured using mechanical conditioning, have shown great potential in animal studies [54]. Growth of the engi-neered tissues has not yet been proven for these valves, but has been demonstrated in a 2-year follow-up study in juvenile sheep for large blood vessel substitutes, engineered in a comparable manner [55].
The in vitro tissue engineering approach, based on synthetic scaf-folds, has not only been proven successful in animal studies, it also holds promise for clinical application. Tissue-engineered patches based on a synthetic scaffold, seeded with autologous saphenous vein cells, have been successfully used for pulmonary artery recon-struction in humans [56,57]. The feasibility of the in vitro heart valve tissue engineering approach has to be demonstrated with human cells for future clinical application. Various cell sources can be chosen, ranging from prenatally derived stem cells [58–62] to adult stem cells [52,63]. As the challenge of obtaining sufficient amounts of extracellular matrix remains when using human cells, a novel bioreactor system has been developed using solely stretch [64] in contrast to others applying a combination of pulsatile stretch and flow [53,65–67]. Using this bioreactor system in combination with fully differentiated vascular-derived cells and a rapid-degrading scaffold, human replacement valves for application in the systemic application were developed [68]. Future animal studies should elu-cidate the short- and long-term functionality of such valves in the systemic circulation. To ensure physiological hemodynamics in the systemic circulation, scaffold geometry and design are of utmost importance. The commonly used PGA is commercially available as nonwoven fiber sheet, representing a ready-to-use scaffold, but limits the possibilities with respect to complicated geometries. PCL, P4HB and PLA are excellent candidates for various manufacturing and scaffold design technologies to enable the development of more complex geometries. Examples herein include the use of knitting, electrospinning and stereolithography, as demonstrated for heart valve scaffolds using PCL [69–71].
Both the use of synthetic scaffolds and decellularized matrices rely on in vitro cell invasion to achieve cellularity. When using a suitable (hydro) gel, cellularity is improved by entrapment of the cells within the gel. This concept is being applied for valves using a fibrin gel as a scaffold material [72,73], but these valves lack the mechanical strength required to be used as replacement valve [74]. Induction of commissural alignment of the gel fibers by cell-induced compaction holds promise for pulmonary application [75]. When combining the use of fibrin, for improved cellularity, and a synthetic scaffold, for mechanical strength [76], applications in the systemic circulation are feasible [68].
Challenges for the in vitro heart valve tissue engineering approachIn vitro tissue engineering using synthetic scaffold materials rep-resents a safe approach in terms of long-term graft survival to be applied in clinical studies. For translation of the use of such valves into clinics, several challenges remain to be addressed as discussed later in the article.

www.expert-reviews.com 263
ReviewTissue engineering of heart valves: advances & current challenges
The missing elastic networkThe role of elastin in the biomechanical behavior of the valve has long been underestimated owing to its relatively small abun-dance, but its importance in its action in interplay with collagen has now been acknowledged [77,78]. Disturbances in the elastin homeostasis are believed to represent an underlying cause of valve replacement failure and the formation of aneurysms [24,79,80]. Therefore, elastin formation has been recognized as a missing link in tissue-engineered cardiovascular substitutes for proper biomechanical function [81], which is certainly accounted for with trileaflet heart valves. Efforts within in vitro human heart valve tissue engineering have, until now, always focused on col-lagen formation to increase the mechanical strength of the valves. Therefore, it remains a challenge to generate an elastic network in the valves to further mimic native biomechanical behavior and to increase the chance of lifelong functionality of these valves after implantation. Elastin production has been reported using animal-derived cells [82] and human neonatal cells [82–84]. However, elastin formation using adult human cells is a chal-lenging task, although some elastin production by adult human cells is reported [85,86]. It may be worth investigating different cell sources for their capacity to generate components of the elastic networks, as fibroblasts may be more suitable, compared with smooth muscle cells, for this purpose. Several biochemical and biomechanical triggers are known to enhance or inhibit elastin formation by cells from several cell sources; the presence of fibrin [82,83], the use of vitamin A [85], growth factors supplemented to the culture medium [82] and the use of static and dynamic strains during culturing [87] are known enhancers of elastin formation. By contrast, the presence of scaffold degradation products [75], the use of vitamin C [88] and the presence of collagen [82,83] are known inhibitors. The feasibility of the formation of the compo-nents of the elastic network, and the network as a whole, should be studied to eventually be implemented into the in vitro heart valve tissue engineering protocol.
Conditioning as a tool for tissue composition & organizationMimicking native biomechanical behavior remains of the utmost importance to provide valve replacements that hold promise for long-term graft survival. Similar to native tissues, the biome-chanical behavior of tissue-engineered valves depends on the composition, organization and quality of the extracellular matrix. Not only the extracellular matrix composition, but, in particular, collagen cross-link density, has also demonstrated a direct cor-relation to the biomechanical tissue behavior [89]. Biochemical conditioning of the growing tissue during the in vitro culture phase, by means of the addition of growth factors, represents a promising strategy to influence tissue quality [90,91]. However, caution is desired in the translation of the use of growth factors to clinical application, as the pathways of the used growth fac-tors are often not yet fully elucidated. Mechanical conditioning is another commonly used strategy and may represent a safer approach to influence extracellular matrix production [92–94]. Various conditioning strategies are being employed and their
influence on tissue formation and extracellular matrix proper-ties in model systems using fast-degrading scaffolds and human adult vascular-derived cells studied. As the vascular-derived human cells belong to the myofibroblast phenotype, they pro-duce a continuous isometric tension on their environment [95]. Constraining the tissues during growth, thereby allowing the myofibroblasts to develop tension, has been proven beneficial for tissue formation and organization [96]. In addition to constrain-ing the growing tissues, continuous long-term dynamic straining has been demonstrated to further increase collagen cross-link densities and tissue organization, but large straining magnitudes deteriorated the biomechanical properties [97,98]. Intermittent dynamic straining, in addition to constraining the growing tis-sues, providing a delicate balance between periods of mechanical stimulation alternated with periods of rest, has proven a safe approach to accelerate tissue formation and organization without the risk of tissue deterioration [99]. Next to mechanical condition-ing, culturing the tissues under hypoxic conditions represents a promising approach towards the development of native-like tissue properties of engineered heart valves [100]. By unraveling the influences of various mechanical and hypoxic stimuli on extracellular matrix formation and properties, the biomechani-cal behavior of tissue-engineered valves may be fine-tuned and controlled towards future clinical application.
Heart valve bioreactors for more than just monitoringIn most heart valve tissue engineering studies using bioreactor systems, the conditioning regime is focusing on mimicking the physiological environment of these valves [53,65–67]. From studies unraveling mechanical conditioning as a tool for tissue organi-zation and orientation, as described in the previous paragraph, a novel conditioning strategy was developed. This conditioning strategy focuses on mimicking solely the diastolic phase of the cardiac cycle, the phase in which the leaflet tissues are being cyclically strained [64]. This approach has rendered human tis-sue-engineered valves that may sustain the systemic circulation [68]. In this bioreactor system, referred to as the Diastolic Pulse Duplicator, a pressure difference is applied across the growing leaflets, inducing local cyclic strains. The pressure difference is monitored, but cannot be translated into applied straining mag-nitudes, as this translation is directly dependent on the properties of the leaflets. Afterwards, having measured the biomechanical properties of the engineered tissues, the applied straining magni-tude can be estimated, based on the applied pressure difference, using numerical modeling [64]. In order to translate the use of such a bioreactor system to routine clinical use to culture valves, the applied deformations during culture should be monitored and controlled. Ideally, the bioreactor should be designed such that it serves as a quality control system next to a controllable culture environment, being able to determine the biomechanical properties of the growing valves and subsequently adjusting the conditioning magnitude to further improve tissue properties. Measuring volumetric deformations, next to the pressure differ-ence, has proven to be a valuable tool to assess applied local tissue strains in the leaflets using numerical modeling in a real-time,

Expert Rev. Med. Devices 6(3), (2009)264
Review Mol, Smits, Bouten & Baaijens
noninvasive manner [101]. In addition, it has proven feasible to assess the overall biomechanical properties of the growing leaflets during culture in a real-time and noninvasive manner, based on an inverse experimental–numerical estimation method [102]. Current studies are ongoing to use these developed features and to translate them into a feedback control loop to control tissue deformation and resulting tissue properties. Such a bioreactor system will provide a fully controlled culture environment for tissue engineering of heart valves and will be a major step towards the clinical application of such valves.
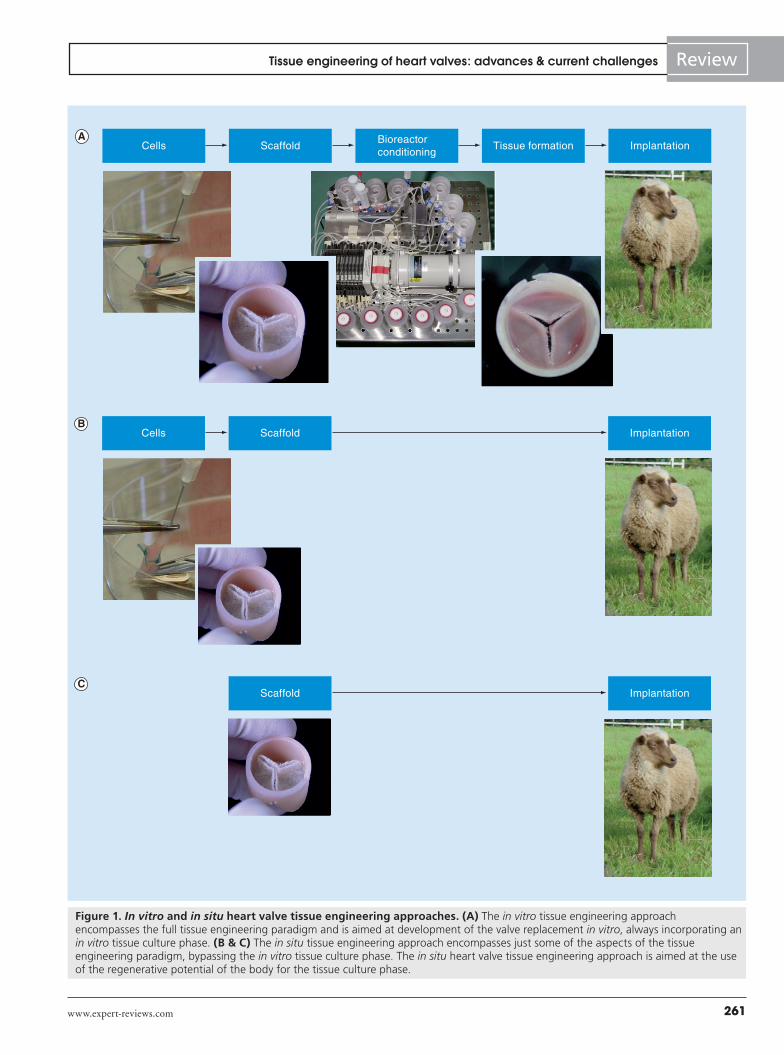
Translation from human cells to animal-derived cells & vice versaMany groups have started their work in heart valve tissue engi-neering using animal-derived cells as they are easier to obtain and directly implementable into animal studies. When using human adult vascular-derived cells, mechanical conditioning is a pre-requisite to obtain tissue formation of such quality that it may serve to withstand the systemic loads [64,68,92]. The next step is to obtain proof of concept in animal studies. Such animal studies require translation of the techniques developed for in vitro human heart valve tissue engineering to the use of animal cells. When culturing ovine vascular-derived cells, it was noted that these cells were much smaller than their human equivalents, as shown in Figure 2. Heart valves were engineered from ovine cells according to the techniques used for human heart valve tissue engineering. Vascular-derived cells were seeded onto PGA/P4HB scaffolds using fibrin as a cell carrier and the valves were conditioned in the Diastolic Pulse Duplicator, as described earlier [68]. Strikingly, the outcome of the ovine tissue-engineered valves was dramati-cally different from their human equivalents, as demonstrated in Figure 2, necessitating a study into the effects of various tissue engineering parameters on tissue formation using ovine cells. The influence of conditioning, the amount of P4HB in the scaf-fold, the culture period and the culture medium composition were the studied parameters [Mol A, Unpublished Data]. Ovine cells reacted more profoundly to mechanical conditioning compared with human cells. The contractile forces exerted on the scaffold by the ovine cells were higher, requiring an increase in P4HB con-centration for coating of the scaffold. Thick surface tissue layers were observed, indicating high proliferative activity of the cells. Decreasing the culture period, as well as changing the medium composition to contain lower amounts of serum, enabled a more homogeneous tissue formation. Optimization of all parameters has resulted in functional ovine heart valves with an outcome comparable to their tissue-engineered human counterparts, as shown in Figure 3, and ready for use in animal studies. This study shows that translation of in vitro human heart valve tissue engi-neering experience to animal studies requires, once again, full optimization of many of the tissue engineering parameters. The observed differences are most likely due to both the age of the cells and species differences. This has large implications for all areas of tissue engineering and raises a fundamental question: what is awaiting us at the translation step from animal studies to clinical practice? Perhaps new tools, other than the current
animal models, to test the longevity of tissue-engineered valves should be developed. As such, valves cannot undergo a process of accelerated testing, as performed for artificial valves; Sir Magdi Yacoub suggests moderate accelerated in vitro testing for 2 weeks [103]. He emphasized that the most important proof for longevity of tissue-engineered valves is the absence of rejection by the body. Another alternative is numerical modeling, which provides valu-able information to assess and evaluate the mechanical behavior of engineered valve leaflets [104]. In addition, the use of animal-based culture products will have to be omitted to allow future safe clinical use of such valves. Development and testing of alternatives for the use of animal-derived serum in culture, such as the use of human serum and/or platelet lysates, is promising, and the topic of many studies [105–107].
Minimally invasive approach & tissue-engineered valvesConventional valve replacement encompasses invasive open-heart surgery with substantial morbidity and mortality risks, par-ticularly in the case of repeated valve replacements. Minimally invasive valve replacement techniques have evolved rapidly as an alternative treatment option. Various transvascular, catheter-based techniques, as well as alternative minimally invasive sur-gical techniques, such as the transapical approach, have been developed and proven safe in clinical routine [108–110]. A challenge for the heart valve tissue engineering field is to demonstrate the feasibility of the use of tissue-engineered valves in minimally invasive valve replacement techniques. For minimally invasive delivery, the valves need to be crimped. In the case of transapi-cal implantation, the crimping ratio, compared with its original diameter, should be in the order of 2.5, which is similar to the crimping ratio used clinically for delivery of stented bioprosthetic valves [110]. To allow for crimping of the valve and subsequent deployment, the valve needs to be incorporated into a stent. Tissue damage may be easily induced by the stent struts dur-ing crimping and deployment, which may be prevented by the incorporation of a protective layer in between the valve and the stent [111]. Animal studies, as well as more fundamental studies into the influence of crimping on cell behavior and subsequent tissue remodeling, will provide insights into the possible future clinical application of such valves in minimally invasive surgical and catheter-based implantation techniques.
In situ heart valve tissue engineeringThe in situ tissue engineering approach has the potential to yield a more clinically attractive alternative compared with in vitro tissue engineering, offering off-the-shelf availability. This approach of in situ tissue engineering, or ‘guided tissue regeneration’, relies on the natural regenerative potential of the body and allows for a simplified regulatory process prior to implantation. Key to the process of in situ tissue engineering is the use of a nonthrombo-genic and nonimmunogenic, functional scaffold, capable of host cell repopulation and subsequent remodeling in situ.
Decellularized xenografts or homografts represent an obvious and attractive option as scaffold material, particularly for guided tissue regeneration of heart valves. Signaling components present

www.expert-reviews.com 265
ReviewTissue engineering of heart valves: advances & current challenges
in the matrix provide natural cues to dictate cell adhesion, prolif-eration and growth. Various studies have demonstrated successful in situ recellularization of decellularized homografts and xeno-grafts in animal models [112–119]. The success rate was dependent on the decellularization method used and the use of a xenograft or homograft. Up to 80% repopulation of SynerGraft®-treated homografts and porcine xenografts in sheep, in both pulmonary and systemic circulation, was reported 11 months after implanta-tion [112,113]. When trypsin/EDTA decellularized porcine xeno-grafts were used in the pulmonary position in an ovine model, recellularization with valve-specific cells was only observed in xenografts and not in homografts, due to severe calcifications [114]. The decellularized xenografts were not only repopulated in the pulmonary position in sheep, but in the systemic circulation in dogs as well [115]. Successful host cell repopulation of porcine xenografts has also been reported when using varying sodium dodecyl sulfate-based decellularization methods in goats [116] and dogs [117]. Additionally, various studies have indicated not
only recellularization, but also adaptive matrix remodeling and growth potential of decellularized xenografts in juvenile sheep models [118,119].
Uncertainty remains as to whether or not these prosperous results with decellularized xenografts and homografts, as seen in animal models, can be translated to human counterparts. While initial promising results were obtained in adults [112], implantation of porcine xenografts treated with the SynerGraft process has led to severe immunogenic response and early graft failure in children [120]. These observations triggered a series of studies targeting rem-nant immunogenicity of decellularized grafts. It became evident that porcine xenografts particularly, completely devoid of cells, still hold significant residual immunogenic potential in contrast to homografts [121]. In vitro studies have indicated that recruitment of monocyte and lymphocyte subpopulations could be dimin-ished by decellularization, but not the recruitment of granulocytes [122], which are known to be strongly involved in early inflamma-tory reactions. Recently, it was suggested that inhibitory factors,
A B
C D
200 µm 200 µm
Figure 2. Translation of the developed techniques for in vitro human heart valve tissue engineering to the use of ovine cells. When culturing the cells, it was observed that (A) the human cells were much larger than (B) their ovine equivalents. (C) While the valves cultured with the human vascular cells were functional valves, (D) the valves cultured with the ovine vascular cells, according to the exact same protocol, demonstrated thickened, retracted and nonfunctional leaflets.
Expert Rev. Med. Devices 6(3), (2009)266
Review Mol, Smits, Bouten & Baaijens
naturally present in the extracellular matrix, are lost due to decel-lularization treatment, which might account for the activation of human granulocytes by porcine valve tissue [123]. Further studies should elucidate the exact, underlying mechanisms of remnant immunogenicity in decellularized xenografts to evaluate whether or not safe clinical use can be ensured. The chance of success for clinical use of decellularized xenograft matrices may benefit from revised decellularization techniques. In vitro studies have demon-strated that the repopulation potential of porcine xenografts by human cells is dependent on the decellularization method used. Specifically, a treatment with combined Triton X-100/sodium deoxycholate detergents rendered the most favorable scaffold for repopulation with human cells [124]. Indeed, preliminary results of an ongoing clinical study using deoxycholic acid-treated por-cine xenografts as pulmonary replacement, during a Ross pro-cedure, revealed repopulation with host cells in the vessel wall and leaflets, as well as endothelial coverage of the valve intimal surface, 10 months after implantation [118]. Thereafter, promis-ing results were obtained in human application of these decellu-larized xenografts as pulmonary valve replacements [125,126]. To further decrease the susceptibility of decellularized matrices to an inflammatory response, the matrices can be impregnated within a biodegradable polymer solution. This has been demonstrated to be essential during the early postimplantation phase until the matrix is repopulated with host cells [127,128]. Another option to decrease the inflammatory response is endothelialization of the matrices before implantation, using autologous endothelial cells. However, this encompasses an in vitro cell culture and expansion phase, next to a flow conditioning culture phase, to prevent the cells from being washed off after exposure to
in situ conditions [129,130]. This is beyond the scope of in situ tissue engineering as this aims to prevent the in vitro tissue culture phase. In general, the feasibility of spontaneous in situ recellularization of acellular xenografts within the human body remains somewhat speculative [131].
For human application, the use of decellularized homografts may be beneficial over the use of decellularized xenografts, as homografts have proven to be less thrombogenic with lower infec-tion risk [132]. Histopathologic findings in a human pulmonary homograft decellularized with the SynerGraft treatment showed infiltration of the neointima by neutrophils and CD68-positive macrophages, but no valve-specific cell types, 5 weeks after implantation [133]. Recipient cell colonization, as well as differen-tiation into endothelial and smooth muscle phenotypes, was found in a SynerGraft-treated aortic homograft, which was recovered upon reoperation 2 years after implantation [134]. Further promis-ing results with SynerGraft-treated homografts as pulmonary valve replacements and as aortic valve replacements in humans were reported [135,136]. Yet, when compared with the results of conven-tional cryopreserved homografts, no clear benefits in functionality were observed at 1-year follow-up [137,138].
The use of synthetic matrices has several advantages over the described decellularized matrices. The chemical and mate-rial properties are well defined and immunogenic potential is reduced. The choice of the synthetic scaffold material is of high importance and factors such as degradation rate and mechanism, biocompatibility, mechanical properties and ease of handling for surgical intervention should be taken into account. Implantation of a plain scaffold has been shown to render immature cellulariza-tion and thrombus formation in dogs [139]. Pretreatment of the
A B
Figure 3. In vitro heart valve tissue engineering protocol for use with ovine vascular cells was optimized such that the outcome of (A) the ovine valves was similar to (B) their human tissue-engineered equivalents. Optimization of the culture protocol involved a decrease in culture time as well as changes in medium composition containing lower amounts of serum.

www.expert-reviews.com 267
ReviewTissue engineering of heart valves: advances & current challenges
scaffolds with collagen before implantation renders promising results in animal studies for use in vessel wall reconstruction of both the pulmonary artery and the aorta [140,141]. Even tubu-lar grafts used as aorta replacements were shown to function properly for up to 1 year in a porcine model [142], as did carotid artery replacements in a dog model [143]. Another approach is to combine the use of such synthetic scaffolds with freshly isolated autologous cells, obtained via a single biopsy on the day of sur-gery. By using biopsies as a same-day source of cells, arterial and venous reconstruction has been successfully performed in both animal and clinical studies [57,144–146]. Recently, even evidence of growth using this interesting approach was demonstrated in a juvenile sheep model [147]. Small-scale cell culture facilities are necessary, but an extensive in vitro cell expansion and tissue cul-ture phase is still omitted. The challenge of such an approach remains the development of an appropriate scaffold for in situ heart valve tissue engineering.
In situ tissue engineering is also implemented by using the peritoneal cavity as a bioreactor. In this way, in situ cellularization is achieved via the foreign body reaction. After tissue is formed, the scaffolds are removed and implanted at the requested site, where they can serve as replacements. Intraperitoneally cellular-ized valves, created from bovine pericardium, have demonstrated promising results in a sheep model [148,149]. It is still question-able whether this approach renders the correct cell types [150] and studies are ongoing to determine the origin of the attracted cell types and the consequences on valve remodeling and tissue formation [151].
Challenges of the in situ heart valve tissue engineering approachIn situ tissue engineering represents a quick, cheap and on-demand approach. While decellularized matrices are mostly used in this approach, the use of synthetic scaffolds for in situ heart valve tissue engineering is very attractive. Such scaffolds, either containing or not containing incorporated biological cues and/or combined with the use of freshly isolated autologous cells, hold great promise for future application and commercialization. For demonstration of the feasibility of this approach, and for the translation of such valves into clinics, several challenges remain to be addressed, as discussed later in the article.
Grasping the principles of host cell repopulationThe exact mechanism behind repopulation of heart valve replace-ments with host cells remains elusive. Preclinical and a few clinical studies on the characterization of cell populations and mapping of recellularization profiles, in both biological and synthetic grafts, have managed to shed some light upon the possible principles involved in host cell repopulation. The presence of circulating endothelial progenitor cells in the blood originating from the bone marrow has been well established [152,153]. Accordingly, experi-ments in mice have shown that smooth muscle cells, present in the intima of aortic implants, originate at least partly from donor bone marrow [154]. It is suggested that repopulation of these aortic grafts occurs via neovascularization and not via direct binding of
the circulating cells onto the lumina due to the high shear forces in the aorta. This role of neovascularization is in line with the findings in decellularized pulmonary xenografts in a juvenile sheep model, which displayed a pattern of repopulation with host mono-nuclear cells being highly dependent on the development of the vasa vasorum [118]. Studies assessing the recellularization poten-tial of decellularized matrices in animal models have proposed that host cells are indeed derived from neovascularization in the implant or from tissue adjacent to the graft [113,116]. A pattern of cellular migration was observed from the conduit wall onto the valve leaflets, starting at the base towards the free margin of the leaflet. Caution is required when interpreting the results of animal studies with respect to host cell repopulation, as indicated by Zilla et al. [155]. Most animal models may be inappropriate for study-ing this phenomenon as transanastomotic rather than transmural or blood-borne repopulation is being studied, which is not clini-cally relevant. Findings in a human aortic homograft, 2 years after implantation, confirmed repopulation with the recipient’s cells, as seen in animal models [134]. Also, a centrifugal propagation of cells, extending from the lumen outward, was suggested to be congruent with theories on circulating progenitor cells present in the adult human heart valve [156].
An additional process involved in cell recruitment is represented by the foreign body response. Subcutaneous and intraperitoneal implantations of biomaterial patches have demonstrated a major role of Sca-1+ cells during early phases of the foreign body response, the capability of these cells to form hematopoietic or mesenchymal colonies, and their subsequent differentiation into multiple cell lines [151,157]. Analysis of cytokine, chemokine and growth factor concentrations during the foreign body response, as provoked by various biomaterials, has led to the suggestion that the foreign body response is similar for all inert implanted materials [158].
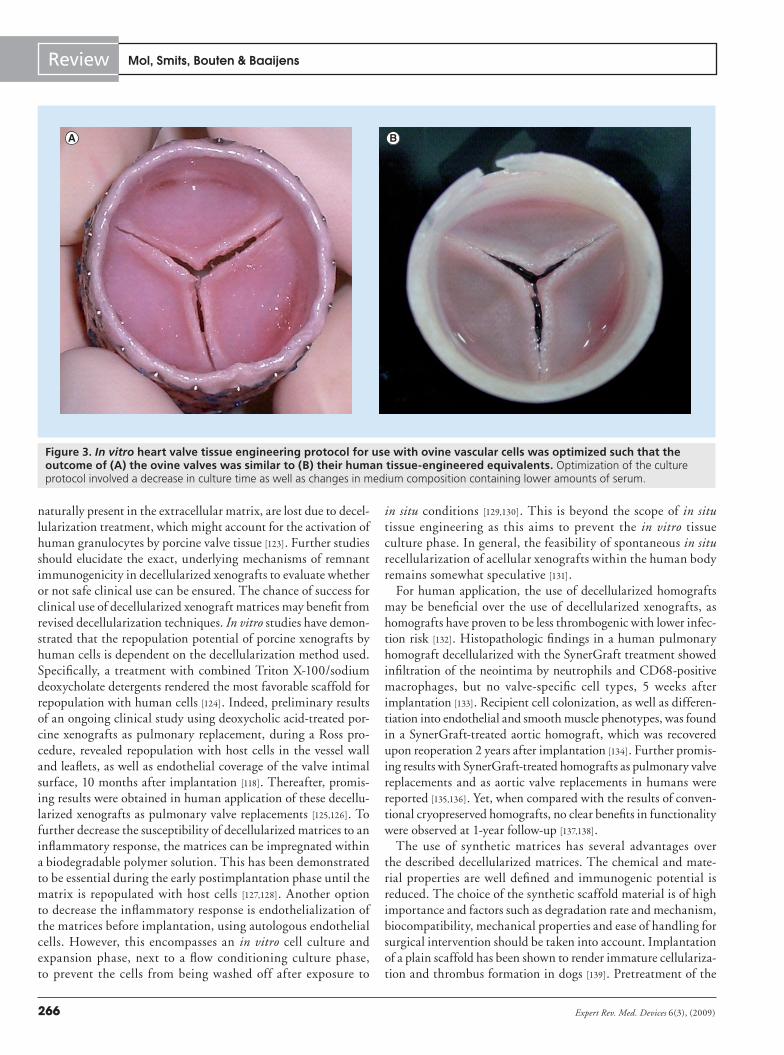
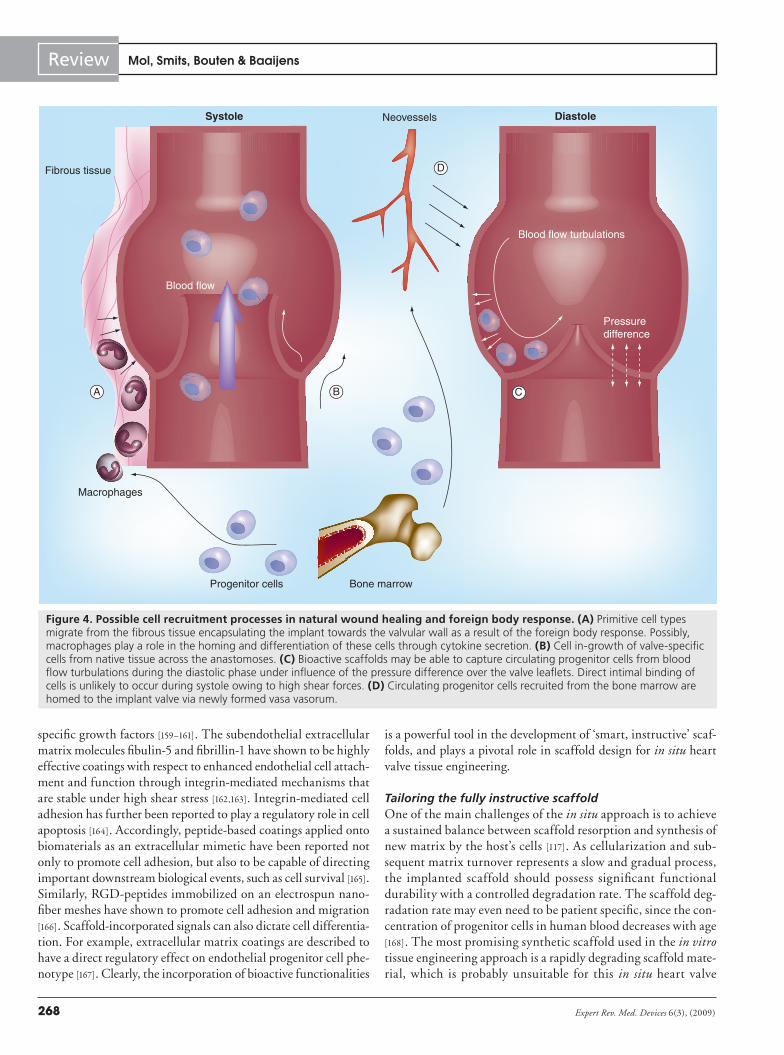
Overall, it can be hypothesized that the process of cell recruit-ment comprises a range of pathophysiological reactions. It was proposed that recellularization may involve binding of circulating progenitor cells to the luminal surface of the graft in combination with stromal cells migrating from the periadventitial granulation tissue or across the anastomosis site [117]. Such a combined effect of the natural wound healing response and foreign body reaction, as depicted in Figure 4, holds great promise for the cellularization potential of heart valve scaffolds, conforming to the guided tissue regeneration concept.
Active cell captureIn order to benefit from the body’s natural regenerative ability, an implanted heart valve scaffold should trigger appropriate signal-ing cascades for cell recruitment. Traditional synthetic scaffolds have the disadvantage of lacking such signaling molecules and cannot offer cell matrix interactions as naturally present in the extracellular matrix. Consequently, the functional integration of bioactivity into biomaterials has been the scope of a broad field of research. With respect to heart valve tissue engineering, various types of bioactive moieties in the scaffold may optimize cell cap-ture, as well as active recruitment and differentiation guidance, such as CD34 antibodies and high-affinity aptamers, as well as
Expert Rev. Med. Devices 6(3), (2009)268
Review Mol, Smits, Bouten & Baaijens
specific growth factors [159–161]. The subendothelial extracellular matrix molecules fibulin-5 and fibrillin-1 have shown to be highly effective coatings with respect to enhanced endothelial cell attach-ment and function through integrin-mediated mechanisms that are stable under high shear stress [162,163]. Integrin-mediated cell adhesion has further been reported to play a regulatory role in cell apoptosis [164]. Accordingly, peptide-based coatings applied onto biomaterials as an extracellular mimetic have been reported not only to promote cell adhesion, but also to be capable of directing important downstream biological events, such as cell survival [165]. Similarly, RGD-peptides immobilized on an electrospun nano-fiber meshes have shown to promote cell adhesion and migration [166]. Scaffold-incorporated signals can also dictate cell differentia-tion. For example, extracellular matrix coatings are described to have a direct regulatory effect on endothelial progenitor cell phe-notype [167]. Clearly, the incorporation of bioactive functionalities
is a powerful tool in the development of ‘smart, instructive’ scaf-folds, and plays a pivotal role in scaffold design for in situ heart valve tissue engineering.
Tailoring the fully instructive scaffoldOne of the main challenges of the in situ approach is to achieve a sustained balance between scaffold resorption and synthesis of new matrix by the host’s cells [117]. As cellularization and sub-sequent matrix turnover represents a slow and gradual process, the implanted scaffold should possess significant functional durability with a controlled degradation rate. The scaffold deg-radation rate may even need to be patient specific, since the con-centration of progenitor cells in human blood decreases with age [168]. The most promising synthetic scaffold used in the in vitro tissue engineering approach is a rapidly degrading scaffold mate-rial, which is probably unsuitable for this in situ heart valve
Bone marrowProgenitor cells
Macrophages
Blood flow
Fibrous tissue
Blood flow turbulations
Pressuredifference
Systole DiastoleNeovessels
B C
D
A
Figure 4. Possible cell recruitment processes in natural wound healing and foreign body response. (A) Primitive cell types migrate from the fibrous tissue encapsulating the implant towards the valvular wall as a result of the foreign body response. Possibly, macrophages play a role in the homing and differentiation of these cells through cytokine secretion. (B) Cell in-growth of valve-specific cells from native tissue across the anastomoses. (C) Bioactive scaffolds may be able to capture circulating progenitor cells from blood flow turbulations during the diastolic phase under influence of the pressure difference over the valve leaflets. Direct intimal binding of cells is unlikely to occur during systole owing to high shear forces. (D) Circulating progenitor cells recruited from the bone marrow are homed to the implant valve via newly formed vasa vasorum.

www.expert-reviews.com 269
ReviewTissue engineering of heart valves: advances & current challenges
tissue engineering approach. As an alternative, a three-layered graft has been suggested, in which a fast-degrading interior of knitted PGA with collagen is reinforced with an exterior of slow-degrading woven poly-l-lactic acid [142]. Both scaffold layers are linked via a PCL film. This three-layered scaffold has shown excellent in vivo durability as a vascular graft for up to 12 months in animal models [142,143]. PCL in itself may also represent a promising scaffold material for use in in situ tissue engineering. Being a slow-degrading scaffold material, it has shown excellent in vivo stability [169] and the mechanical proper-ties of PCL-based polymers can be elegantly tailored by using supra molecular filler materials incorporated into the material hard block [170]. Implantation of electrospun PCL tubular grafts replacing the abdominal aorta in rats has demonstrated promis-ing results in terms of healing characteristics when compared with expanded polytetraflouroethylene grafts [171]. Interestingly, it appears that chondroid metaplasia is the major drawback of using these PCL grafts. This finding emphasizes the need for a more instructive scaffold with appropriate cell-signaling molecules to direct the differentiation of migrated and captured cells, as also suggested by others [32].
Expert commentary & five-year viewIn vitro tissue engineering represents a safe approach in terms of long-term graft survival. Despite the decellularized xenograft or homograft being the most obvious choice as a heart valve scaffold, the approach using fast-degrading scaffold materials holds significantly more promise with respect to the growth capacity of the valve. The challenge, when using synthetic scaffold materials in the in vitro heart valve tissue engineering approach, of obtaining sufficient and high-quality tissue that mimicks native valve biomechanics remains. Incorporation of an elastic network, unraveling the use of mechanical condition-ing as a tool to guide tissue composition and organization, and the development of a bioreactor system to monitor and control
applied conditioning strategies, are prerequisites towards clini-cal implementation of such in vitro tissue-engineered valves. The ovine model is the recommended animal model for test-ing heart valves. It remains questionable whether this is the correct test model as it was demonstrated that the outcomes of in vitro engineered valves based on ovine and human cells were remarkably different. With this in mind, one may ask oneself to what extent the results obtained from animal studies may be translated into future clinical outcome and vice versa. Therefore, alternative test systems and guidelines should be developed to demonstrate proof of principle. Furthermore, the use of animal-based culture products will have to be omitted and reproducibility issues and interpatient variability will have to be elucidated for future routine clinical use of such valves. Despite the fact that the risk of infection is high during the process of cell harvesting and subsequent tissue culture, and the process being expensive and time consuming, the 5-year view for the in vitro heart valve tissue engineering approach holds great promise. It may very well be feasible to have performed the first human implantations with in vitro tissue-engineered heart valves, at least as pulmonary valve replacements, but maybe even as aortic valve replacements based on the use of a synthetic scaffold material and autologous cells.
In situ tissue engineering represents a quick, cheap and on-demand approach, making it an attractive approach for com-mercialization. Most studies focusing on in situ tissue engineer-ing make use of decellularized valves, which, in itself, represents a promising approach as the valve matrix is representative for its native counterpart. However, the use of decellularized xenografts in human applications renders controversial results, and the use of decellularized homografts does not solve the problem of limited donor valve availability and may raise ethical concerns. The use of synthetic scaffolds offers an elegant approach, which holds great promise for future clinical application, either inde-pendently or in combination with freshly isolated autologous
Key issues
• The number of patients requiring valve replacement is estimated to triple over the coming five decades.
• None of the current replacement valves can fully restore native valve function because they inherently lack growth and remodeling capabilities.
• Heart valve tissue engineering is an evolving field of research that enables the development of the ideal replacement valve, which is autologous, living and capable of adaptive remodeling.
• In vitro heart valve tissue engineering aims at full development of the tissue substitute in vitro.
• Promising results have been obtained in the in vitro heart valve tissue engineering approach using synthetic scaffolds and mechanical conditioning, demonstrating functionality and remodeling into native-like tissues in the pulmonary position in animal studies.
• In vitro tissue engineering of human heart valves, based on a synthetic scaffold and cultured using a strain-based conditioning approach, holds promise for use in both the pulmonary and systemic circulation.
• In situ tissue engineering aims at using the regenerative potential of the body for the tissue culture phase.
• Promising results have been obtained using the in situ heart valve tissue engineering approach using decellularized homografts, but the use of such scaffolds does not solve the limited availability of donor valves and may raise ethical concerns.
• Repopulation of scaffolds in situ is most likely to occur as a combination of cell migration from adjacent tissues and cell capture from the blood, guided by the foreign body response.
• In situ tissue engineering using synthetic scaffolds, either containing or not containing incorporated biological cues, either independently or in combination with freshly isolated autologous cells, may represent the heart valve tissue engineering paradigm of the future.

Expert Rev. Med. Devices 6(3), (2009)270
Review Mol, Smits, Bouten & Baaijens
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet 368, 1005–1011 (2006).
2 Rosamond W, Flegal K, Furie K et al. Heart disease and stroke statistics – 2008 update: a report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation 117, E25–E146 (2008).
3 Nkomo VT. Epidemiology and prevention of valvular heart diseases and infective endocarditis in Africa. Heart 93, 1510–1019 (2007).
4 Zilla P, Brink J, Human P, Bezuidenhout D. Prosthetic heart valves: catering for the few. Biomaterials 29, 385–406 (2008).
5 Iung B, Baron G, Butchart EG et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on valvular heart disease. Eur. Heart J. 24, 1231–1243 (2003).
6 Goldbarg SH, Elmariah S, Miller MA, Fuster V. Insights into degenerative aortic valve disease. J. Am. Coll. Cardiol. 50, 1205–1213 (2007).
7 Yacoub MH, Cohn LH. Novel approaches to cardiac valve repair: from structure to function: part I. Circulation 109, 942–950 (2004).
8 Yacoub MH, Cohn LH. Novel approaches to cardiac valve repair: from structure to function: part II. Circulation 109, 1064–1072 (2004).
9 Friedewald VE, Bonow RO, Borer JS et al. The editor’s roundtable: cardiac valve surgery. Am. J. Cardiol. 99, 1269–1278 (2007).
10 Yacoub MH, Takkenberg JJM. Will heart valve tissue engineering change the world? Nat. Clin. Pract. Cardiovasc. Med. 2, 60–61 (2005).
11 Mikos AG, Herring SW, Ochareon P et al. Engineering complex tissues. Tissue Eng. 12, 3307–3339 (2006).
12 Bonow RO, Carabello BA, Chatterjee K et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 114, E84–E231 (2006).
13 Hammermeister K, Sethi GK, Henderson WG, Grover FL, Oprian C, Rahimtoola SH. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the Veterans Affairs randomized trial. J. Am. Coll. Cardiol. 36, 1152–1158 (2000).
14 Oxenham H, Bloomfield P, Wheatley DJ et al. Twenty year comparison of a Bjork-Shiley mechanical heart valve with porcine bioprostheses. Heart 89, 715–721 (2003).
15 Jamieson WRE, Von Lipinski O, Miyagishima RT et al. Performance of bioprostheses and mechanical prostheses
assessed by composites of valve-related complications to 15 years after mitral valve replacement. J. Thorac. Cardiovasc. Surg. 129, 1301–1308 (2005).
16 Chan V, Jamieson WRE, Germann E et al. Performance of bioprostheses and mechanical prostheses assessed by composites of valve-related complications to 15 years after aortic valve replacement. J. Thorac. Cardiovasc. Surg. 131, 1267–1273 (2006).
17 Eichinger WB, Hettich IM, Ruzicka DJ et al. Twenty-year experience with the St. Jude Medical Biocor bioprosthesis in the aortic position. Ann. Thorac. Surg. 86, 1204–1211 (2008).
18 Lund O, Bland M. Risk-corrected impact of mechanical versus bioprosthetic valves on long-term mortality after aortic valve replacement. J. Thorac. Cardiovasc. Surg. 132, 20–26 (2006).
19 Brown ML, Schaff HV, Lahr BD et al. Aortic valve replacement in patients aged 50 to 70 years: improved outcome with mechanical versus biologic prostheses. J. Thorac. Cardiovasc. Surg. 135, 878–884 (2008).
20 Koertke H, Minami K, Boethig D et al. INR self-management permits lower anticoagulation levels after mechanical heart valve replacement. Circulation 108(Suppl. II), II75–II78 (2003).
21 Koertke H, Zittermann A, Tenderich G et al. Low-dose oral anticoagulation in patients with mechanical heart valve prostheses: final report from the Self-Management Anticoagulation trial II. Eur. Heart J. 28, 2479–2484 (2007).
22 Koolbergen DR, Hazekamp MG, de Heer E et al. Structural degeneration of pulmonary homografts used as aortic valve
cells. The scaffold can be fully characterized and tailored to its functional demands. Furthermore, biological cues may be incorporated to guide cellularization and tissue regeneration. In situ tissue engineering using synthetic scaffold materials for heart valve tissue engineering is still in its infancy and efforts are ongoing to study all aspects related to this approach. The main challenge is to get a grasp on the repopulation process with autologous cells, which have to differentiate into the appropriate phenotype to maintain valve function, and providing a non-thrombogenic surface. Repopulation of the scaffold will most likely involve cell migration from adjacent tissue combined with cell capture from the blood flow, guided by the foreign body response. The in situ tissue engineering approach is hard to fully explore in an in vitro setting, because the foreign body response and cell migration capacity is not incorporated, and so in vivo
studies will have to elucidate feasibility of the approach. The most easily tested model is a tubular graft and promising results are expected within the next 5 years using synthetic scaffolds containing incorporated biological cues. However, the develop-ment of synthetic scaffolds that are suitable for the in situ heart valve tissue engineering approach represents a challenging task that holds great promise for future valve replacement therapy.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
www.expert-reviews.com 271
ReviewTissue engineering of heart valves: advances & current challenges
substitute underlines early graft failure. Eur. J. Cardiothorac. Surg. 22, 802–807 (2002).
23 Jennings LM, Butterfield M, Booth C, Watterson KG, Fisher J. The pulmonary bioprosthetic heart valve: its unsuitability as an aortic valve replacement. J. Heart Valve Dis. 11, 668–678 (2002).
24 Schoof PH, Takkenberg JJM, van Suylen R et al. Degeneration of the pulmonary autograft: an explant study. J. Thorac. Cardiovasc. Surg. 132, 1426–1432 (2006).
25 Klieverik LMA, Takkenberg JJM, Bekkers JA, Roos-Hesselink JW, Witsenburg M, Bogers AJJC. The Ross operation: a Trojan horse? Eur. Heart J. 28, 1993–2000 (2007).
26 El Oakley R, Kleine P, Bach DS. Choice of prosthetic heart valve in today’s practice. Circulation 117, 253–256 (2008).
27 Puvimanasinghe JP, Steyerberg EW, Takkenberg JJ et al. Prognosis after aortic valve replacement with a bioprosthesis: predictions based on meta-analysis and microsimulation. Circulation 103, 1535–1541 (2001).
28 Wheatley DJ, Raco L, Bernacca GM, Sim I, Belcher PR, Boyd JS. Polyurethane: material for the next generation of heart valve prostheses? Eur. J. Cardiothorac. Surg. 17, 440–448 (2000).
29 Daebritz SH, Sachweh JS, Hermanns B et al. Introduction of a flexible polymeric heart valve prosthesis with special design for mitral position. Circulation 108(Suppl. II), II134–II139 (2003).
30 Daebritz SH, Fausten B, Hermanns B et al. Introduction of a flexible polymeric heart valve prosthesis with special design for aortic position. Eur. J. Cardiothorac. Surg. 25, 946–952 (2004).
31 Gallocher SL, Aguirre AF, Kasyanov V, Pinchuk L, Schoephoerster RT. A novel polymer for potential use in a trileaflet heart valve. J. Biomed. Mater. Res. Part B Appl. Biomaterials 79(2), 325–334 (2006).
32 Schoen FJ. Evolving concepts of cardiac valve dynamics. The continuum of development, functional structure, pathobiology, and tissue engineering. Circulation 118, 1864–1880 (2008).
•• Recentreviewdiscussingtheinteractionofvalvebiologyandbiomechanics,mechanismsofvalvedisease,considerationsinvalverepairandreplacement,andthepotentialfortissueengineering.
33 Adachi M, Suzuki M, Kennedy JH. Neointimas cultured for circulatory assist devices: comparison of cultured cells derived from autologous tissues of various organs. J. Surg. Res. 11, 483–491 (1971).
34 Mansfield PB, Wechezak AR, Sauvage LR. Preventing thrombus on artificial vascular surfaces: true endothelial cell linings. Trans. Am. Soc. Artif. Intern. Organs 21, 264–272 (1975).
35 Eberl T, Siedler S, Schumacher B, Zilla P, Schlaudraff K, Fasol R. Experimental in vitro endothelialization of cardiac valve leaflets. Ann. Thorac. Surg. 53, 487–492 (1992).
36 Langer R, Vacanti JP. Tissue engineering. Science 260, 920–926 (1993).
37 Kasimir MT, Rieder E, Seebacher G et al. Comparison of different decellularization procedures of porcine heart valves. Int. J. Artif. Organs 26, 421–427 (2003).
38 Tudorache I, Cebotari S, Sturz G et al. Tissue engineering of heart valves: biomechanical and morphological properties of decellularized heart valves. J. Heart Valve Dis. 16, 567–573 (2007).
39 Liao J, Joyce EM, Sacks MS. Effects of decellularization on the mechanical and structural properties of the porcine aortic valve leaflet. Biomaterials 29, 1065–1074 (2008).
40 Curtil A, Pegg DE, Wilson A. Repopulation of freeze-dried porcine valves with human fibroblasts and endothelial cells. J. Heart Valve Dis. 6, 296–306 (1997).
41 Schenke-Layland K, Opitz F, Gross M et al. Complete dynamic repopulation of decellularized heart valves by application of defined physical signals – an in vitro study. Cardiovasc. Res. 60, 497–509 (2003).
42 Cushing MC, Jaeggli MP, Masters KS, Leinwand LA, Anseth KS. Serum deprivation improves seeding and repopulation of acellular matriced with valvular interstitial cells. J. Biomed. Mater. Res. A 75, 232–241 (2005).
43 Knight RL, Booth C, Wilcox HE, Fisher J, Ingham E. Tissue engineering of cardiac valves: re-seeding of acellular porcine aortic valve matrices with human mesenchymal progenitor cells. J. Heart Valve Dis. 14, 806–813 (2005).
44 Steinhoff G, Stock U, Karim N et al. Tissue engineering of pulmonary heart valves on allogenic acellular matrix conduits. Circulation 102(Suppl. 3), III150–III155 (2000).
45 Kim S, Lim S, Hong Y et al. Tissue engineering of heart valves in vivo using bone-marrow derived cells. Artif. Organs 30, 554–567 (2006).
46 Walles T, Lichtenberg A, Puschmann C et al. In vivo model for cross-species porcine endogenous retrovirus transmission using tissue engineered pulmonary arteries. Eur. J. Cardiothorac. Surg. 24, 358–363 (2003).
47 Shinoka T, Breuer CK, Tanel RE et al. Tissue engineering of heart valves: valve replacement study in a lamb model. Ann. Thorac. Surg. 60, S513–S516 (1995).
48 Shinoka T, Ma PX, Shum-Tim D et al. Tissue engineered heart valves: autologous valve replacement study in a lamb model. Circulation 94(Suppl. 3), III64–III68 (1996).
49 Kim WG, Cho SK, Kang MC, Lee TY, Park JK. Tissue-engineered heart valve leaflets: an animal study. Int. J. Artif. Organs 24, 642–648 (2001).
50 Sodian R, Hoerstrup SP, Sperling et al. Early in vivo experience with tissue-engineered trileaflet heart valves. Circulation 102(Suppl. 3), III22–III29 (2000).
51 Stock UA, Nagashima M, Khalil PN et al. Tissue-engineered valved conduits in the pulmonary circulation. J. Thorac. Cardiovasc. Surg. 119, 732–740 (2000).
52 Sutherland FWH, Perry TE, Yu Y et al. From stem cells to viable semilunar autologous heart valve. Circulation 111, 2783–2791 (2005).
53 Hoerstrup SP, Sodian R, Sperling JS, Vacanti JP, Mayer JE. New pulsatile bioreactor for in vitro formation of tissue engineered valves. Tissue Eng. 6, 75–79 (2000).
54 Hoerstrup SP, Sodian R, Daebritz S et al. Functional living trileaflet heart valves grown in vitro. Circulation 102(Suppl. 3), III44–III49 (2000).
•• Firststudytodemonstratefunctionalovinetissue-engineeredtrileafletheartvalves,basedonasyntheticscaffoldseededwithvascular-derivedcellsandculturedinabiomimeticenvironment,upto20weeksinapulmonaryposition.
55 Hoerstrup SP, Cummings I, Lachat M et al. Functional growth in tissue-engineered vascular grafts: follow-up at 100 weeks in a large animal model. Circulation 114(Suppl.), I159–I166 (2006).
56 Shinoka T, Imai Y. Transplantation of a tissue-engineered pulmonary artery. N. Engl. J. Med. 344, 532–533 (2001).

Expert Rev. Med. Devices 6(3), (2009)272
Review Mol, Smits, Bouten & Baaijens
57 Matsumura G, Hibino N, Ikada Y, Kurosawa H, Shinoka T. Successful application of tissue engineered vascular autografts: clinical experience. Biomaterials 24, 2303–2308 (2003).
58 Schmidt D, Mol A, Breymann C et al. Living autologous heart valves engineered from human prenatally harvested progenitors. Circulation 114(Suppl.), I125–I131 (2006).
59 Schmidt D, Mol A, Odermatt B et al. Engineering of biologically active living heart valve leaflets using umbilical cord-derived progenitor cells. Tissue Eng. 12, 3223–3232 (2006).
60 Sodian R, Lueders C, Kraemer L et al. Tissue engineering of autologous human heart valves using cryopreserved vascular umbilical cord cells. Ann. Thorac. Surg. 81, 2207–2216 (2006).
61 Schmidt D, Achermann J, Odermatt B et al. Prenatally fabricated autologous human living heart valves based on amniotic fluid derived progenitor cells as a single cell source. Circulation 116(Suppl.), I64–I70 (2007).
62 Schmidt D, Achermann J, Odermatt B, Genoni M, Zund G, Hoerstrup SP. Cryopreserved amniotic fluid-derived cells: a lifelong autologous fetal stem cell source for heart valve tissue engineering. J. Heart Valve Dis. 17, 446–455 (2008).
63 Hoerstrup SP, Kadner A, Melnitchouk S et al. Tissue engineering of functional trileaflet heart valves from human marrow stromal cells. Circulation 106(Suppl.), I143–I150 (2002).
64 Mol A, Driessen NJB, Rutten MCM, Hoerstrup SP, Bouten CVC, Baaijens FPT. Tissue engineering of human heart valve leaflets: a novel bioreactor for a strain-based conditioning approach. Ann. Biomed. Eng. 33, 1778–1788 (2005).
65 Dumont K, Yperman J, Verbeken E et al. Design of a new pulsatile bioreactor for tissue engineered aortic heart valve formation. Artif. Organs 26, 710–714 (2002).
66 Hildebrand DK, Wu ZJ, Mayer JE, Sacks MS. Design and hydrodynamic evaluation of a novel pulsatile bioreactor for biologically active heart valves. Ann. Biomed. Eng. 32, 1039–1049 (2004).
67 Morsi YS, Yang WW, Owida A, Wong CS. Development of a novel pulsatile bioreactor for tissue culture. J. Artif. Organs 10, 109–114 (2007).
68 Mol A, Rutten MCM, Driessen NJB, Bouten CVC, Baaijens FPT, Hoerstrup SP. Autologous human tissue-engineered heart
valves: prospects for systemic application. Circulation 114(Suppl.), I152–I158 (2006).
•• Firststudytodemonstratethefeasibilityofengineeringtrileaflethumanheartvalves,basedonasyntheticscaffoldseededwithvascular-derivedcellsandculturedaccordingtoastrain-basedconditioningapproach,whicharecapableoffunctioninginthesystemiccirculation.
69 Sodian R, Loebe M, Hein A et al. Application of stereolithography for scaffold fabrication for tissue engineered heart valves. ASAIO J. 48, 12–16 (2002).
70 van Lieshout MI, Vaz CM, Rutten MCM, Peters GW, Baaijens FPT. Electrospinning versus knitting: two scaffolds for tissue engineering of the aortic valve. J. Biomaterials Sci. Polym. Ed. 17, 77–89 (2006).
71 Morsi YS, Wong CS. Current developments and future challenges for the creation of aortic heart valve. J. Mech. Med. Biol. 8, 1–15 (2008).
72 Jockenhoevel S, Chalabi K, Sachweh JS et al. Tissue engineering: complete autologous valve conduit – a new moulding technique. Thorac. Cardiovasc. Surg. 49, 287–290 (2001).
73 Flanagan TC, Cornelissen C, Koch S et al. The in vitro development of autologous fibrin-based tissue-engineered heart valves through optimised dynamic conditioning. Biomaterials 28, 3388–3397 (2007).
74 Jockenhoevel S, Zund G, Hoerstrup SP et al. Fibrin gel—advantages of a new scaffold in cardiovascular tissue engineering. Eur. J. Cardiothorac. Surg. 19, 424–430 (2001).
75 Neidert MR, Tranquillo RT. Tissue-engineered valves with commissural alignment. Tissue Eng. 12, 891–903 (2006).
76 Mol A, Lieshout van MI, Dam-de Veen CG et al. Fibrin as a cell carrier in cardiovascular tissue engineering aaplications. Biomaterials 26, 3113–3121 (2005).
77 Scott M, Vesely I. Aortic valve cusp microstructure : the role of elastin. Ann. Thorac. Surg. 60, S391–S394 (1995).
78 Vesely I. The role of elastin in aortic valve mechanics. J. Biomech. 31, 115–123 (1998).
79 Lee TC, Midura RJ, Hascall VC, Vesely I. The effect of elastin damage on the mechanics of the aortic valve. J. Biomech. 34, 203–210 (2001).
80 Anidjar S, Salzmann JL, Gentric D, Lagneau P, Camilleri JP, Michel JB. Elastase-induced experimental aneurysms in rats. Circulation 82, 973–981 (1990).
81 Patel A, Fine B, Sandig M, Mequanint K. Elastin biosynthesis: the missing link in tissue-engineered blood vessels. Cardiovasc. Res. 71, 40–49 (2006).
82 Long JL, Tranquillo RT. Elastic fiber production in cardiovascular tissue-equivalents. Matrix Biol. 22, 339–350 (2003).
83 Williams C, Johnson SL, Robinson PS, Tranquillo RT. Cell sourcing and culture conditions for fibrin-based valve constructs. Tissue Eng. 12, 1489–1502 (2006).
84 Yang C, Sodian R, Fu P et al. In vitro fabrication of a tissue engineered human cardiovascular patch for future use in cardiovascular surgery. Ann. Thorac. Surg. 81, 57–64 (2006).
85 Ogle BM, Mooradian DL. Manipulation of remodelling pathways to enhance the mechanical properties of a tissue engineered blood vessel. J. Biomech. Eng. 124, 724–733 (2002).
86 Luo Y, Kobler JB, Zeitels SM, Langer R. Effects of growth factors on extracellular matrix production by vocal cord fibroblasts in 3-dimensional culture. Tissue Eng. 12, 3365–3374 (2006).
87 Gupta V, Grande-Allen J. Effects of static and cyclic loading in regulating extracellular matrix synthesis by cardiovascular cells. Cardiovasc. Res. 72, 375–383 (2006).
88 Rosenbloom J, Abrams WR, Mecham R. Extracellular matrix 4: the elastic fiber. FASEB J. 7, 1208–1218 (1993).
89 Balguid A, Rubbens MP, Mol A et al. The role of collagen cross-links in biomechanical behavior of human aortic heart valve leaflets – relevance for tissue engineering. Tissue Eng. 13, 1501–1511 (2007).
90 Huang SD, Liu XH, Bai CG et al. Synergistic effect of fibronectin and hepatocyte growth factor on stable cell-matrix adhesion, re-endothelialization, and reconstitution in developing tissue-engineered heart valves. Heart Vessels 22, 116–122 (2007).
91 Robinson PS, Johnson SL, Evans MC, Barocas VH, Tranquillo RT. Functional tissue-engineered valves from cell-remodeled fibrin with commissural alignment of cell-produced collagen. Tissue Eng. Part A 14, 83–95 (2008).

www.expert-reviews.com 273
ReviewTissue engineering of heart valves: advances & current challenges
92 Mol A, Bouten CV, Zund G et al. The relevance of large strains in functional tissue engineering of heart valves. Thorac. Cardiovasc. Surg. 51, 78–83 (2003).
93 Isenberg BC, Tranquillo RT. Long-term cyclic distention enhances the mechanical properties of collagen based media-equivalents. Ann. Biomed. Eng. 31, 937–949 (2003).
94 Seliktar D, Nerem RM, Galis ZS. Mechanical strain stimulated remodeling of tissue-engineered blood vessel constructs. Tissue Eng. 9, 657–666 (2003).
95 Hinz B, Gabbiani G. Mechanisms of force generation and transmission by myofibroblasts. Curr. Opinion. Biotechnol. 14, 538–546 (2003).
96 Grenier G, Rémy-Zolghadri M, Larouche D et al. Tissue reorganization in response to mechanical load increases functionality. Tissue Eng. 11, 90–100 (2005).
97 Boerboom RA, Rubbens MP, Driessen NJB, Bouten CVC, Baaijens FPT. Effect of strain magnitude on the tissue properties of engineered cardiovascular constructs. Ann. Biomed. Eng. 36, 244–253 (2008).
98 Rubbens MP, Mol A, Marion van MH et al. Straining-mode dependent collagen remodeling in engineered cardiovascular tissues. Tissue Eng. DOI: 10.1089/ten.tea.2008.0185 (2008) (Epub ahead of print).
99 Rubbens MP, Mol A, Boerboom RA, Bank RA, Baaijens FPT, Bouten CVC. Intermittent straining accelerates the development of tissue properties in engineered heart valve tissue. Tissue Eng. DOI: 10.1089/ten.tea.2007.0396 (2008) (Epub ahead of print).
100 Balguid A, Mol A, Vlimmeren MA, Baaijens FPT, Bouten CVC. Hypoxia induces near-native mechanical properties in engineered heart valve tissue. Circulation 119, 290–297 (2009).
101 Kortsmit J, Driessen NJB, Rutten MCM, Baaijens FPT. Real-time non-invasive assessment of leaflet deformation in heart valve tissue engineering. Ann. Biomed. Eng. 37(3), 532–541 (2009).
102 Kortsmit J, Driessen NJB, Rutten MCM, Baaijens FPT. Nondestructive and noninvasive assessment of mechanical properties in heart valve tissue engineering. Tissue Eng. Part A DOI: 10.1089/ten.tea.2008.0197 (2009) (Epub ahead of print).
103 Yacoub M. Viewpoint: heart valve engineering. Interview by James Butcher. Circulation 116, F44–F46 (2007).
104 Driessen NJB, Mol A, Bouten CVC, Baaijens FPT. Modeling the mechanics of tissue-engineered human heart valve leaflets. J. Biomech. 40, 325–334 (2007).
105 Stute N, Holtz K, Bubenheim A, Lange C, Blake F, Zander AR. Autologous serum for isolation and expansion of human mesenchymal stem cells for clinical use. Exp. Hematol. 32, 1212–1225 (2004).
106 Bernardo ME, Avanzini MA, Perotti C et al. Optimization of in vitro expansion of human multipotent mesenchymal stromal cells for cell-therapy approaches: further insights into the search for a fetal calf serum substitute. J. Cell. Physiol. 211, 121–130 (2007).
107 Kocaoemer A, Kern S, Klüter H, Bieback K. Human AB serum and thrombin-activated platelet-rich plasma are suitable alternatives to fetal calf serum for the expansion of mesenchymal stem cells from adipose tissue. Stem Cells 25, 1270–1278 (2007).
108 Lutter G, Ardehali R, Cremer J, Bonhoeffer P. Percutaneous valve replacement: current state and future prospects. Ann. Thorac. Surg. 78, 2199–2206 (2004).
109 Lichtenstein SV, Cheung A, Ye J et al. Transapical transcatheter aortic valve implantation in humans. Initial clinical experience. Circulation 114, 591–596 (2006).
110 Walther T, Simon P, Dewey T et al. Transapical minimally invasive aortic valve implantation: multicenter experience. Circulation 116(Suppl.), I240–I245 (2007).
111 Stock UA, Degenkolbe I, Atmann T, Schenke-Layland K, Freitag S, Lutter G. Prevention of device-related tissue damage during percutaneous deployement of tissue-engineered heart valves. J. Thorac. Cardiovasc. Surg. 131, 1323–1330 (2006).
112 Goldstein S, Clarke DR, Walsh SP, Black KS, O’Brien MF. Transpecies heart valve transplant: advanced studies of a bioengineered xeno-autograft. Ann. Thorac. Surg. 70, 1962–1969 (2000).
113 Elkins RC, Goldstein S, Hewitt CW et al. Recellularization of heart valve grafts by a process of adaptive remodeling. Semin. Thorac. Cardiovasc. Surg. 13(Suppl. 1), I87–I92 (2001).
114 Leyh RG, Wilhelmi M, Rebe P et al. In vivo repopulation of xenogeneic and allogeneic acellular valvular matrix conduits in the pulmonary circulation. Ann. Thorac. Surg. 75, 1457–1463 (2003).
115 Takagi K, Fukunaga S, Nishi A et al. In vivo recellularization of plain decellularized xenografts with specific cell characterization in the systemic circulation: histological and immunohistochemical study. Artif. Organs 30, 233–241 (2006).
116 Kim WG, Huh JH. Time related histopathological changes of acellularized xenogeneic pulmonary valved conduits. ASAIO J. 50, 601–605.
117 Iwai S, Torikai K, Coppin CM, Sawa Y. Minimally immunogenic decellularized porcine valve provides in situ recellularization as a stentless bioprosthetic valve. J. Artif. Organs 10, 29–35 (2007).
118 Erdbrügger W, Konertz W, Dohmen PM et al. Decellularized xenogenic heart valves reveal remodeling and growth potential in vivo. Tissue Eng. 12, 2059–2068 (2006).
119 Dohmen PM, da Costa F, Holonski S et al. Is there a possibility for a glutaraldehyde-free porcine heart valve to grow? Eur. Surg. Res. 38, 54–61 (2006).
120 Simon P, Kasimir MT, Seebacher G et al. Early failure of the tissue engineered porcine heart valve SYNERGRAFT in pediatric patients. Eur. J. Cardiothorac. Surg. 23, 1002–1006 (2003).
• Reportingonthestructuralfailureandrapiddegenerationofdecellularizedporcinexenograftsinahumanstudy,representingthedifficultiesintranslatingpromisingresultsfromanimalstudiesintoclinics.
121 Kasimir MT, Rieder E, Seebacher G et al. Decellularization does not eliminate thrombogenicity and inflammatory stimulation in tissue-engineered porcine heart valves. J. Heart Valve Dis. 15, 278–286 (2006).
122 Rieder E, Nigisch A, Dekan B et al. Granulocyte-based immune response against decellularized or glutaraldehyde cross-linked vascular tissue. Biomaterials 27, 5634–5642 (2006).
123 Bastian F, Stelzmüller ME, Kratochwill K, Kasimir MT, Simon P, Weigel G. IgG deposition and activation of the classical complement pathway involved in the activation of human granulocytes by decellularized porcine heart valve tissue. Biomaterials 29, 1824–1832 (2008).
124 Rieder E, Kasimir MT, Silberhumer G et al. Decellularization protocols of porcine heart valves differ importantly in efficiency of cell removal and susceptibility of the matrix to recellularization with human vascular cells. J. Thorac. Cardiovasc. Surg. 127, 399–405 (2004).
Expert Rev. Med. Devices 6(3), (2009)274
Review Mol, Smits, Bouten & Baaijens
125 Dohmen PM, Konertz W. Results with decellularized xenografts. Circ. Res. 99, E10 (2006).
126 Dohmen PM, Hauptmann S, Terytze A, Konertz W. In vivo repopulation of a tissue-engineered heart valve in a human subject. J. Heart Valve Dis. 16, 447–449 (2007).
127 Stamm C, Khosravi A, Grabow N et al. Biomatrix/polymer composite material for heart valve tissue engineering. Ann. Thorac Surg. 78, 2084–2092 (2004).
128 Stamm C, Steinhoff G. When less is more: go slowly when repopulating a valve in vivo. J. Thorac. Cardiovasc. Surg. 132, 735–737 (2007).
129 Lichtenberg A, Cebotari S, Tudorache I et al. Flow-dependent re-endothelialization of tissue-engineered heart valves. J. Heart Valve Dis. 15, 287–293 (2006).
130 Lichtenberg A, Tudorache I, Cebotari et al. In vitro re-endothelialization of detergent decellularized heart valves under simulated physiological dynamic conditions. Biomaterials 27, 4221–4229 (2006).
131 Stock UA, Schenke-Layland K. Performance of decellularized xenogeneic tissue in heart valve replacement. Biomaterials 27, 1–2 (2006).
132 Rieder E, Seebacher G, Kasimir MT et al. Tissue engineering of heart valves: decellularized porcine and human valve scaffolds differ importantly in residual potential to attract monocytic cells. Circulation 111, 2792–2797 (2005).
133 Sayk F, Bos I, Schubert U, Wedel T, Sievers HH. Histopathologic findings in a novel decellularized pulmonary homograft: an autopsy study. Ann. Thorac. Surg. 79, 1755–1758 (2005).
134 Miller DV, Edwards WD, Zehr KJ. Endothelial and smooth muscle cell populations in a decellularized cryopreserved aortic homograft (SynerGraft) 2 years after implantation. J. Thorac. Cardiovasc. Surg. 132, 175–176 (2006).
135 Elkins RC, Dawson PE, Goldstein S, Walsh SP, Black SP. Decellularized human valve allografts. Ann. Thorac. Surg. 71, S428–S432.
136 Zehr KJ, Yagubyan M, Connolly HM, Nelson, Schaff HV. Aortic root replacement with a novel decellularized cryopreserved aortic homograft: postoperative immunoreactivity and early results. J. Thorac. Cardiovasc. Surg. 130, 1010–1015 (2005).
137 Bechtel JF, Müller-Steinhardt M, Schmidtke C, Brunswik A, Stierle U, Sievers HH. Evaluation of the decellularized valve homograft (SynerGraft®). J. Heart Valve Dis. 12, 734–739 (2003).
138 Bechtel JF, Stierle U, Sievers HH. Fifty-two months’ mean follow up of decellularized SynerGraft-treated pulmonary valve allografts. J. Heart Valve Dis. 17, 98–104 (2008).
139 Shinoka T, Shum-Tim D, Ma PX et al. Creation of viable pulmonary autografts through tissue engineering. J. Thorac. Cardiovasc. Surg. 115, 536–545 (1998).
140 Iwai S, Sawa Y, Ichikawa H et al. Biodegradable polymer with collagen microsponge serves as new bioengineered cardiovascular prosthesis. J. Thorac. Cardiovasc. Surg. 128, 472–479 (2004).
141 Iwai S, Sawa Y, Taketani S, Torikai K, Hirakawa K, Matsuda H. Novel tissue-engineered biodegradable material for reconstruction of vascular wall. Ann. Thorac. Surg. 80, 1821–1827 (2005).
142 Torikai K, Ichikawa H, Hirakawa K et al. A self-renewing, tissue-engineered vascular graft for arterial reconstruction. J. Thorac. Cardiovasc. Surg. 136, 37–45 (2008).
143 Yokota T, Ichikawa H, Matsumiya G et al. In situ tissue regeneration using a novel tissue-engineered, small-caliber vascular graft without cell seeding. J. Thorac. Cardiovasc. Surg. 136, 900–907 (2008).
144 Hibino N, Shinoka T, Matsumura G, Ikada Y, Kurosawa H. The tissue-engineered vascular graft using bone marrow without culture. J. Thorac. Cardiovasc. Surg. 129, 1064–1070 (2005).
145 Shinoka T, Matsumura G, Hibino N et al. Midterm clinical result of tissue-engineered vascular autografts seeded with autologous bone marrow cells. J. Thorac. Cardiovasc. Surg. 129, 1330–1338 (2005).
146 Matsumura G, Ishihara Y, Miyagawa-Tomita S et al. Evaluation of tissue-engineered vascular autografts. Tissue Eng. 12, 3075–3083 (2006).
147 Brennan MP, Dardik A, Hibino N et al. Tissue-engineered vascular grafts demonstrate evidence of growth and development when implanted in a juvenile animal model. Ann. Surg. 248, 370–377 (2008).
• Promisingstudycombiningtheuseofasyntheticscaffoldmaterialandfreshlyisolatedautologouscellsforin situtissueengineeringofavenacavareplacementinajuvenilesheepmodel,demonstratingevidenceforgrowth.
148 De Visscher G, Vranken I, Lebacq A et al. In vivo cellularization of a cross-linked matrix by intraperitoneal implantation: a new tool in heart valve tissue engineering. Eur. Heart J. 28, 1389–1396 (2007).
149 De Visscher G, Blockx H, Meuris B et al. Functional and biomechanical evaluation of a completely recellularized stentless pulmonary bioprostheses in sheep. J. Thorac. Cardiovasc. Surg. 135, 395–404 (2008).
150 Sievers HH. In vivo tissue engineering an autologous semilunar biovalve: can we get what we want? J. Thorac. Cardiovasc. Surg. 134, 20–22 (2007).
151 Vranken I, De Visscher G, Lebacq A, Verbeken E, Flameng W. The recruitment of primitive Lin(-), Sca-1(+), CD34(+), c-kit(+) and CD271(+) cells during the early intraperitoneal foreign body reaction. Biomaterials 29, 797–808 (2008).
152 Shi Q, Rafii S, Wu MH et al. Evidence for circulating bone marrow-derived endothelial cells. Blood 92, 362–367 (1998).
153 Asahara T, Masuda H, Takahashi T et al. Bone marrow origin of endothelial progenitor cells responsible for postnatal vasculogenesis in physiological and pathological neovascularization. Circ. Res. 85, 221–228 (1999).
154 Shimizu K, Sugiyma S, Aikawa M et al. Host bone-marrow cell are a source of donor intimal smooth-muscle-like cells in murine aortic transplant arteriopathy. Nat. Med. 7, 738–741 (2001).
155 Zilla P, Bezuidenhout D, Human P. Prosthetic vascular grafts: wrong models, wrong questions and no healing. Biomaterials 28, 5009–5027 (2007).
156 Deb A, Wang SH, Skelding K, Miller D, Simper D, Caplice N. Bone marrow-derived myofibroblasts are present in adult human heart valves. J. Heart Valve Dis. 14, 674–678 (2005).
157 Lee SJ, Van Dyke M, Atala A, Yoo JJ. Host cell mobilization for in situ tissue regeneration. Rejuvenation Res. 11, 747–756 (2008).
158 Schutte RJ, Xie L, Klitzman B, Reichert WM. In vivo cytokine-associated responses to biomaterials. Biomaterials 30, 160–168 (2009).
159 Aoki J, Serruys PW, Van Beusekom H et al. Endothelial progenitor cell capture by stents coated with antibody against CD34: the HEALING-FIM (Healthy Endothelial Accelerated Lining Inhibits

www.expert-reviews.com 275
ReviewTissue engineering of heart valves: advances & current challenges
Neointimal Growth-First In Man) Registry. J. Am. Coll. Cardiol. 45, 1574–1579 (2005).
160 Avci-Adali M, Paul A, Ziemer G, Wendel HP. New strategies for in vivo tissue engineering by mimicry of homing factors for self-endothelialisation of blood contacting materials. Biomaterials 29, 3936–3945 (2008).
161 Ota T, Sawa Y, Iwai S et al. Fibronectin-hepatocyte growth factor enhances reendothelialization in tissue-engineered heart valve. Ann. Thorac. Surg. 80, 1801–1802 (2005).
162 Stephan S, Ball SG, Williamson M et al. Cell-matrix biology in vascular tissue engineering. J. Anat. 209, 495–502 (2006).
163 Williamson MR, Shuttleworth A, Canfield AE, Black RA, Kielty CM. The role of endothelial cell attachment to elastic fibre molecules in the enhancement of monolayer formation and retention, and the inhibition of smooth muscle cell recruitment. Biomaterials 28, 5307–5318 (2007).
164 Damsky CH, Ilic D. Integrin signaling: it’s where the action is. Curr. Opin. Cell Biol. 14, 594–602 (2002).
165 Meyers SR, Khoo X, Huang X, Walsh EB, Grinstaff MW, Kenan DJ. The development of peptide-based interfacial biomaterials for generating biological functionality on the surface of bioinert materials. Biomaterials 30, 277–286 (2009).
166 Kim TG, Park TG. Biomimicking extracellular matrix: cell adhesive RGD peptide modified electrospun poly(d,l-lactic-co-glycolic acid) nanofiber mesh. Tissue Eng. 15, 221–233 (2006).
167 Sales VL, Engelmayr GC Jr, Johnson JA Jr et al. Protein precoating of elastomeric tissue-engineering scaffolds increased cellularity, enhanced extracellular matrix protein production, and differentially regulated the phenotypes of circulating endothelial progenitor cells. Circulation 116(Suppl.), I55–I63 (2007).
168 Schmidt-Lucke C, Rössig L, Fichtlscherer S et al. Reduced number of circulating endothelial progenitor cells predicts future cardiovascular events: proof of concept for the clinical importance of endogenous vascular repair. Circulation 111, 2981–2987 (2005).
169 Tillman BW, Yazdani SK, Lee SJ, Geary RL, Atala A, Yoo JJ. The in vivo stability of electrospun polycaprolactone-collagen scaffolds in vascular reconstruction. Biomaterials 30, 583–588 (2009).
170 Wisse E, Govaert LE, Meijer HEH, Meijer EW. Unusual tuning of mechanical properties of thermoplastic elastomers using supramolecular fillers. Macromolecules 39, 7425–7432 (2006).
171 Pektok E, Nottelet B, Tille J et al. Degradation and healing characteristics of small-diameter poly(e-caprolactone) vascular grafts in the rat systemic arterial circulation. Circulation 118, 2563–2570 (2008).
•• Interestingstudydemonstratingthefeasibilityandadvantagesofimplantingaplainscaffoldcomparedwithconventionalgraftsinthesystemiccirculationofrats.
Affiliations• Anita Mol, PhD
Department of Biomedical Engineering, Eindhoven University of Technology, PO Box 513, 5600 MB, Eindhoven, The Netherlands Tel.: +31 402 473 048 Fax: +31 402 447 355 [email protected]
• Anthal IPM Smits, MSc Department of Biomedical Engineering, Eindhoven University of Technology, PO Box 513, 5600 MB, Eindhoven, The Netherlands
• Carlijn VC Bouten, PhD Department of Biomedical Engineering, Eindhoven University of Technology, PO Box 513, 5600 MB, Eindhoven, The Netherlands
• Frank PT Baaijens, PhD Department of Biomedical Engineering, Eindhoven University of Technology, PO Box 513, 5600 MB, Eindhoven, The Netherlands