tm 1 vaccine doses administered: overview of data collection and reporting pandemic influenza...
TRANSCRIPT

TM1
Vaccine Doses Administered: Overview of Data Collection and
Reporting Pandemic Influenza Vaccine:
Doses Administered And Safety Training ConferenceAtlanta, GA
Joint Presentation August 21, 2008 by:Immunization Services Division
National Center for Immunization and Respiratory Diseases
andDivision of Emergency Preparedness and Response
National Center for Public Health Informatics
TM2
Talk Outline
• Background• 2007 Vaccine Doses
Administered Pilot Results; Lessons Learned
• 2008 Vaccine Doses Administered Exercise
• CRA New Features• Interactive Session
TM3
Background
• The National Strategy for Pandemic Influenza: Implementation Plan calls for monitoring appropriate use of scarce pre-pandemic/pandemic influenza vaccine
• To accomplish this, Project Areas are expected to track pandemic influenza (PI) vaccine doses administered at the individual patient level and then send a subset of data (minimum data set) on a weekly basis to the CDC; Project Areas are the 50 states, 4 large cities and 8 territories
• CDC’s CRA system has been modified to provide flexible ways for Project Areas to report vaccine doses administered
TM4
PI Vaccine Doses Administered Minimum Data Set for Reporting
to CDC • Project Area ID• Reporting Period Start and End Dates• Vaccine Type (CVX code)• HHS Pandemic Priority Groups
• Homeland and Nations Security• Health Care and Community Support Services• Critical Infrastructure• General Population
• Dose #• Count of Doses Administered per Priority
Group and Dose #
TM5
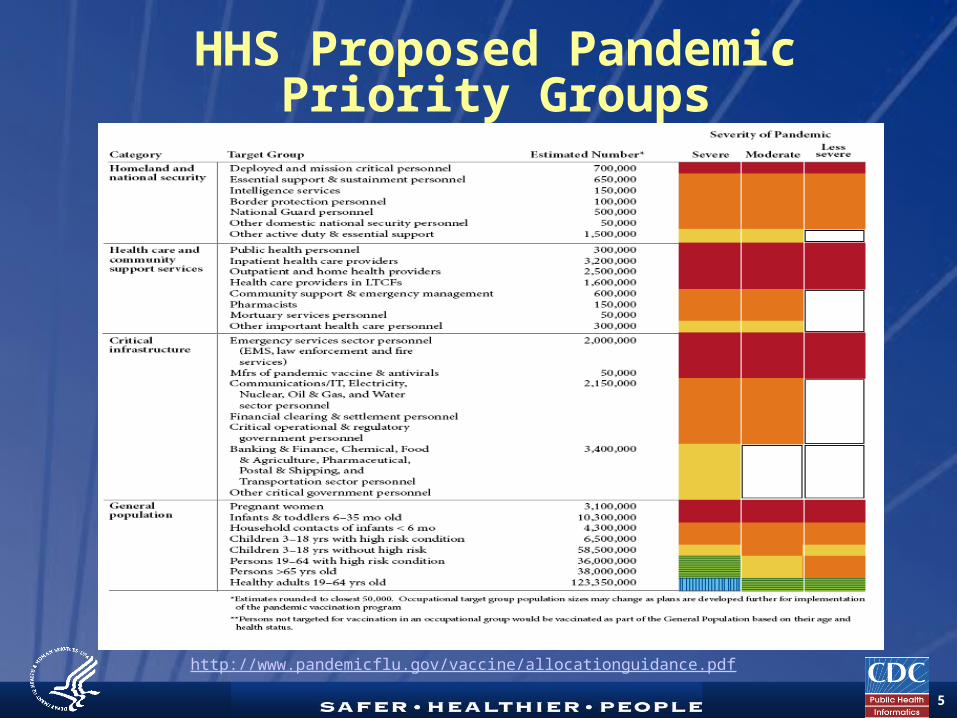
HHS Proposed Pandemic Priority Groups
http://www.pandemicflu.gov/vaccine/allocationguidance.pdf
TM6
Current Thinking on Data Collection and Aggregation
Strategies• The proposed HHS prioritization format
lists: 4 Categories, 14 Tier Groups and numerous Target Groups
• Data collection and aggregation will be:• by Category, • by each Tier Group (1, 2, 3 …) within each
Category, and • by each Tier Group across all Categories
• Data collection and aggregation will not be done at the individual Target Groups
• Examples next slide

TM7
Overall Proposed Doses Administered Category and
Tiers for Data ReportingHomeland and Nations
SecurityTier 1 (HNSt1) Tier 2 (HNSt2) Tier 3 (HNSt3)
Health Care and Community Support ServicesTier 1 (HCCSSt1)Tier 2 (HCCSSt2)Tier 3 (HCCSSt3)
Critical Infrastructure Tier 1 (CIt1) Tier 2 (CIt2) Tier 3 (CIt3)
General PopulationTier 1 (GPt1) Tier 2 (GPt2) Tier 3 (GPt3) Tier 4 (GPt4) Tier 5 (GPt5)

TM8
Countermeasure and Response Administration
(CRA)• Genesis in Pre-Event Vaccination System
(PVS) for national smallpox vaccination campaign
• Supports mass tracking during an event• Evolved to support any countermeasure,
any event (medical interventions such as vaccines, pharmaceuticals; non-medical such as patient isolation and quarantine, scarce medical equipment and social distancing measures)
• Tracks both detail (person level) and aggregate counts of countermeasures

TM9
Aggregate Reporting of Pandemic Vaccine Doses
Administered• Data Exchange (Option 1): Project Area
has own system (IIS or other CRA); may send using: pipe delimited, XML file, HL7
• Web Entry Aggregate (Option 2): Project Area collects/aggregates data manually or electronically; enters via aggregate reporting screen
• Web Entry Detail (Option 3): Project Area collects individual data via CRA; minimum data set is automatically aggregated
TM10
2007 Seasonal Influenza Pilot Test
• To test the capability to monitor vaccines doses, a pilot using seasonal influenza vaccine as proxy for pandemic was developed
• Priority areas to be assessed:• Project areas on ability to collect and report
to CDC; access aggregate reports • CDC on technical capability of CRA to accept
and aggregate data • Exercise was designed to be minimally
invasive to normal operations• Time frame: November 1 – December 31,
2007• Frequency: Repeatable; at minimum - twice

TM11
2007 Pilot Minimum Data Set
• Project Area ID• Vaccination Dates• Age Groups
• 6 – 23 months• 2 – 18 years• 19 – 49 years• 50 – 64 years• 65+ years

TM12
Parameters for Participation in 2007 Pilot
• Identify Point of Contact (POC)• Select option choice• Identify minimum of two clinic
dates• Send data for both clinics within 48
hours – “fully successful”
TM13
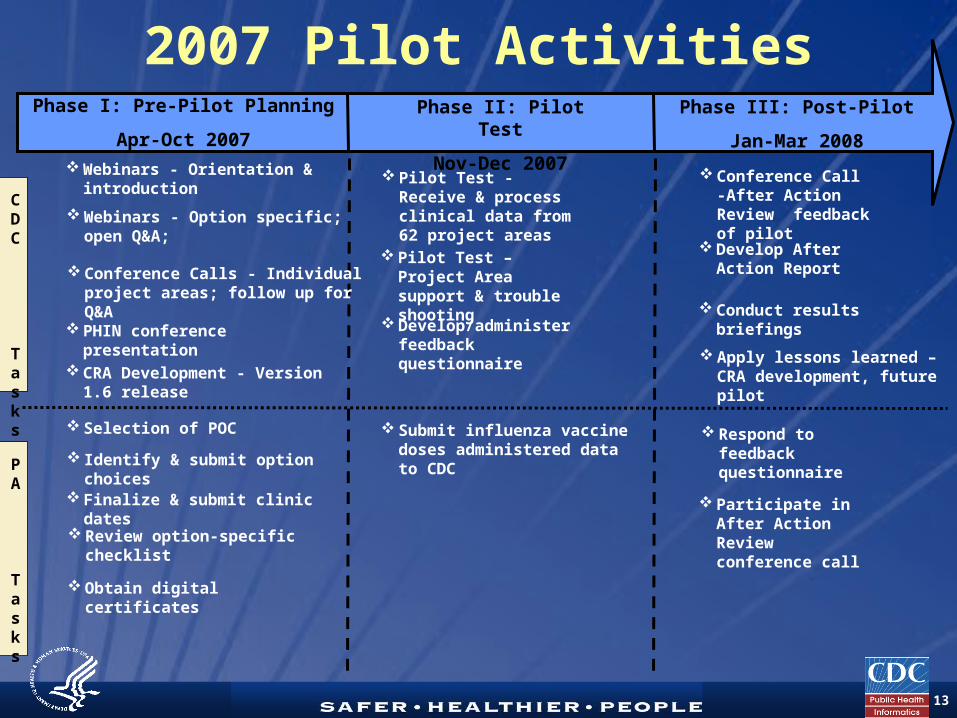
Phase I: Pre-Pilot Planning
Apr-Oct 2007
CDC
Tasks
2007 Pilot ActivitiesPhase II: Pilot Test
Nov-Dec 2007
Phase III: Post-Pilot
Jan-Mar 2008 Webinars - Orientation &
introduction
Webinars - Option specific; open Q&A;
Selection of POC
Conference Calls - Individual project areas; follow up for Q&A
PHIN conference presentation
Identify & submit option choices
CRA Development - Version 1.6 release
Pilot Test - Receive & process clinical data from 62 project areas
Finalize & submit clinic dates
Review option-specific checklist
Develop/administer feedback questionnaire
Respond to feedback questionnaire
Develop After Action Report
Conference Call -After Action Review feedback of pilot
Obtain digital certificates
Conduct results briefings
Participate in After Action Review conference call
Submit influenza vaccine doses administered data to CDC
Pilot Test – Project Area support & trouble shooting
PA
Tasks
Apply lessons learned – CRA development, future pilot

TM14
2007 Option Choices by Project Area
Web Entry aggregate
Web Entry Detail
Data Exchange
LA county
DC
NY City
Chicago
Marshall Islands
Guam
Mariana Islands
Virgin Islands
Puerto Rico
Palau
FS Micronesia
American Samoa

TM15
2007 Summary Results• Pre-Planning
• 100% (62/62) identified a POC• 100% (62/62) selected an Option• 85% (53/62) submitted both clinic dates
• Pilot • 89% (55/62) submitted some data • 11% (7/62) did not submit any data• 64% (35/55) fully successful
• Post-Pilot• 55 Respondents completed on-line feedback
questionnaire • 61% (38/62) participated in After Action
Review call

TM16
Kansas Governor, Kathleen Sebelius, getting influenza vaccination in a Pilot Influenza Clinic, Kansas

TM17
The Kansas Bee Mascot says:“Be wise, get immunized!”

TM18
Timeliness Among All Options by Aggregation Method
11 11
5
21
6
23
3
0
5
10
15
20
25
30
Data Exchange Web Form Aggregation Individual Pt Data
Num
ber o
f Pro
ject
Are
as Yes (Within 48 hrs)
No( >48 hrs)
Did not report

TM19
Data Submission Timeline All Options
55
24
95
15 16
0
10
20
30
40
50
60
24 hrs 48 hrs 72 hrs 96 hrs >120 hrs Data notreported
Timeline of Data Submission (Hrs)
Nu
mb
er
of
Cli
nic
Da
tes
Note: N= 124 clinic dates

TM20
Aggregation Method Among Web Entry
Aggregate Users (Option 2)
• IIS or other system : 23.5% 8/34• Spreadsheet : 41.2% 14/34• Paper based (reported) : 17.6% 6/34• Paper based (did not report) : 17.6% 6/34

TM21
Timeliness by System Reporting Technique –
Options 1 and 2
21
0
24
10
65 40
63
0
5
10
15
20
25
30
Nu
mb
er
of
Clin
ic D
ate
s
Yes-48 hours
No-48 hours

TM22
Need for More Than Systems!
26 27
4
16
0
5
10
15
20
25
30
35
40
System Manual
Data Aggregation Method
Num
ber
of C
linic
Dat
es
Yes-48 hours
No-48 hours

TM23
Option Choice Switching
5 Project Areas (PA) switched from original option choice to other choice when data reporting began• Option 3 to Option 1: 1 PA• Option 2 to Option 1: 2 PA• Option 3 to Option 2: 1 PA• Option 1 to Option 2: 1 PA

TM24
Feedback Questionnaire
• Project Areas requested to complete anonymous, on-line feedback questionnaire
• Nine questions highlighting:• Efficiency of communication from
CDC• Benefits of pilot test• Issues/barriers encountered• Feedback to improve future
exercises
TM25
Question: How beneficial was this pilot test to you in preparing for a pandemic influenza event in the future?
• 14 respondents : Very Beneficial
• 38 respondents : Somewhat Beneficial
• 3 respondents : Not Beneficial

TM26
Question: What issues, if any, did you encounter while transmitting data to CDC?
• 18 respondents : digital certificate • 12 respondents : file format • 12 respondents : SDN (timing out);
technical issues
• 9 respondents : Coordination with their local health departments

TM27
After Action Review Call Feedback
• Confirmed findings from Feedback Questionnaire• SDN timing out affected efficiency• Digital certificate process was a concern
• Supplemented findings from Feedback Questionnaire• CRA was easy to use• CDC/CRA support was good (technical and project)• Need consistent communication by CDC
• Distribution lists• Requesting all information at once• Leading implementer information
• Support for expanded pilot for 2008 - 2009 influenza season

TM28
Strategies for Addressing Challenges
• Digital certificates: two parallel approaches• System design to allow lower level of
security; expected late FY2009 • Internal decision memorandum of
understanding• Timing-out user sessions: immediate
issue corrected; reviewing configuration to avoid in future
• Communications:• Training conference• Communication consistency• Small group calls

TM29
2007 Pilot Total Doses Administered
• 56,667 doses administered across all project areas
• Doses administered by age group:• 6 – 23 Months: 6.4% (3,618)• 2 – 19 Years: 23.0% (12,999)• 20 – 49 Years: 22.6% (12,836)• 50 – 64 Years : 24.4% (13,847)• 65 Years +: 19.6% (11,119)• Not identified 4.0% (2,248)

TM30
Conclusions• Excellent willingness to participate across
project areas• Vast majority (89%) of Project Areas able to
collect, transmit, retrieve data• Nearly 2/3 of Project Areas submitted data
within 48 hour time period• Challenges do exist, technical issues are
being addressed • CRA able to accept, aggregate data submitted
doses • Issues/barriers identified will assist in
improving Pandemic Influenza preparedness• Project Areas supportive of broader/deeper
testing during 2008 influenza season

TM31
2008 - 2009 Seasonal Influenza Exercise Objectives• Timeframe: October 1 - December 31,
2008• Increase volume: to test system and
operational capacities, Project Areas send data from a minimum of eight clinics during the four weeks
• Track prioritization: to test tracking priority groups, Project Areas use proposed prioritization framework
• Weekly reporting: to test weekly reporting capability, Project Areas send data for a minimum of four consecutive weeks
• Tied to 2009 CDC PHEP continuation guidance biosurveillance requirement

TM32
Priority Groups for 2008 Exercise
Focus on General Population Category and its Tier Groups
• General population, Tier 1 (GPt1) contains• "Pregnant women“• “Infants and toddlers 6 - 35 months old"
• General population, Tier 2 (GPt2) contains• “Household contacts of infants < 6 months“• “Children 3 - 18 years with high risk conditions"
• General population, Tier 3 (GPt3) contains • “Children 3 - 18 years without high risk conditions"
• General population, Tier 4 (GPt4) contains • “Persons 19 - 64 with high risk conditions“• “Persons > 65 years old"
• General population, Tier 5 (GPt5) contains• “Healthy adults 19 - 64 years old“
Build Other 9 “Tier Groups” (Not planning to collect data on these for the 2008 exercise)

TM33
Exercise Next Steps• Exercise timeframe is 10/01 – 12/31/2008• CRA version 1.8 to be released 09/15/2008• Training scheduled for 09/17/2008 and
monthly thereafter to support Project Area timeframes
• Expect to follow procedures similar to 2007 pilot compile and report results:• Activities requirements• Webinars/teleconference calls• Exercise poll• After action call• Presentations• After Action Report
TM34
CRA New Feature:Upload Confirmation
• What is it?• Allows Project Area to verify and confirm
counts entered by local health departments• Why is it needed?
• Support growing technical and operations capacity of Project Areas
• Support Project Areas ability to choose multiple options to report DA
• Ensure counts are verified by each Project Area• When is it available?
• Incorporated with in CRA Version 1.8 schedule for release 09/15/2008
• Component of DAX 2008 influenza season exercise
TM35
Confirmation Procedures Option 1: Data Exchange
• Same as 2007 exercise• Personnel at local health departments
enter vaccine administrations using the Project Area’s IIS or other electronic system
• The Project Area POC uploads or messages Project Area-level aggregate file
• Aggregate counts are automatically confirmed when aggregate file is accepted into the CRA system

TM36
Confirmation Procedures Option 2: Web Entry
Aggregate• New process using CRA confirmation
screen• Data Entry Specialist (DES) at the local health
department enters clinic-level aggregate counts of vaccine doses administered
• Clinic-level doses administered are aggregated and displayed on confirmation screen
• Project Area POC confirms aggregate counts and reports counts to the CDC
• A report listing the aggregate counts for each clinic/POD can be generated
TM37
Confirmation Procedures Option 3: Web Entry Detail
• Similar to Option 2• DES at local health department or
clinic enters person-level vaccine doses administered
• Clinic-level doses administered are aggregated and displayed on screen
• Project Area POC confirms aggregate counts and reports counts to the CDC
• A listing of the aggregate counts for each clinic can be generated

TM38
Confirmation Procedures Mixed Options
• Project Areas may now use multiple options to report doses administered data• Clinic-level and person-level doses
administered entered by the local health departments are aggregated and displayed on the screen
• Project Area POC confirms and reports the aggregate counts for the Project Area to the CDC
• A report listing of the aggregate counts for each clinic can be generated
• Extensive coordination of the entire PA is needed

TM39
Interactive Dialog
• Feedback topics 1. What are the best thoughts and
practices on screening for priority groupings?
2. How do Doses Administered (DA) data collection efforts help with overall preparedness efforts?
3. Does the testing and work help promote automation efforts?
4. Does pilot help/hurt collection of routine seasonal data?
5. Future role for increase private vaccination administration efforts?
TM40
1. What are the best practices on screening for
priority groupings?Sample form
Comments on tools such as forms to the bucket classifications

TM41
2. How do Doses Administered (DA) data collection efforts help with overall preparedness efforts?
• Feedback on communication and collaboration bridge between immunization and preparedness?
• Resources sharing?• Opportunities for future projects?

TM42
3. Does the testing and work help promote automation efforts?
• Increasing use of techniques to capture data?
• Use of PHIN MS transport standards?• Opportunities for IIS improvement?• What are the barriers to increase
automation?• Does more automation equal better?

TM43
4. Do exercises (2007 pilot) improve collection of
routine seasonal data?• Do clinics pay better attention to
details during exercises, impact other data collection efforts?
• Any noticeable trends (good or not so good) in reporting of seasonal influenza data from last year’s exercise?

TM44
5. Future role for increase in private vaccination
administration efforts?• What would be the impact and
challenges of targeting industry clinics or occupational groups to collect DA data?
• What are the system roll out and trainability issues?
TM45
Thank you!
Lunch Time