to backboard or not to backboard? selective spinal ... jhfems apr...or not to backboard? selective...
TRANSCRIPT
To Backboardor Not To Backboard?
Selective Spinal Immobilization
Will Smith, MD, EMT-PMedical Director
Grand Teton National Park andJackson Hole Fire/EMS, Jackson, WY
www.wildmedconsulting.com

ObjectivesDiscuss current standard of care and
protocols regarding spine injuries.Review research on spine injuries and
evaluation/treatment standards.How to implement spine assessment
protocols into your system.
TerminologySpinal ImmobilizationSpine Stabilization(In Line Traction)Spinal Motion RestrictionSpinal Clearance ProtocolsSelective Spinal ImmobilizationFocused Spine Assessment

Spinal Immobilization1960-70’s
EMS standards developedConsensus and Common Sense
Thought to be best practiceNow changing?
MAST Pants, Massive IVF in trauma
Who needs to be immobilized?
Even if they walked away from this?
Spinal ImmobilizationDo we immobilize for:
Mechanism of Injury?
Symptoms and/or Physical findings?

Spinal ImmobilizationLittle research
Never been shown to improve outcomes
Malaysian /New Mexico StudyHauswald, Acad Emerg Med 1998
5 yr retrospective chart review of 2university hospitals
Less neurologic disability inunimmobilized Malaysian patients
Disproves many theories that previouslyjustified widespread spine immobilization
Malaysian /New Mexico StudyC-spine fractures = >2,000-6,000 NL-spine fractures = >4,200 N
Head off the end of stretcher = 40 N
Spinal ImmobilizationBUT - Standard of Care (in U.S.)
One of the most common EMS proceduresMillions of patients immobilized each yearNot necessarily in other parts of the world
Most Current EMS ProtocolsApply spinal immobilization to all
patients with potential for spine injurybased on mechanism of injury
If in doubt - IMMOBILIZE!

picture
The ResearchNo RCT to asses spinal immobilization
on trauma patient mortality, neurologicinjury, spinal stability, or adverse effectssustainedKwan, Cochrane Database 2001/2007 #2803
The ResearchNEXUS
Hoffman, et. al. - NEJM, July 2000
Canadian C-Spine RuleStiell, et. al. - JAMA, Oct 2001
NEXUSMoves to a standard of clinical spine
clearance in emergency departmentsDecreased imaging in 12.6 % (4,309 pts)
N=34,069 patients
NEXUS All 5 criteria met = No Xray
1. No midline cervical tenderness2. No focal neurological defect3. Normal alertness4. No intoxication5. No painful distracting injury
Canadian C-Spine RuleProvides another clinical spine clearance
pathwaySlightly different protocol - more if/then
Age listed as a factor (>65)Mechanism still plays a roleRange of motion of neck final test
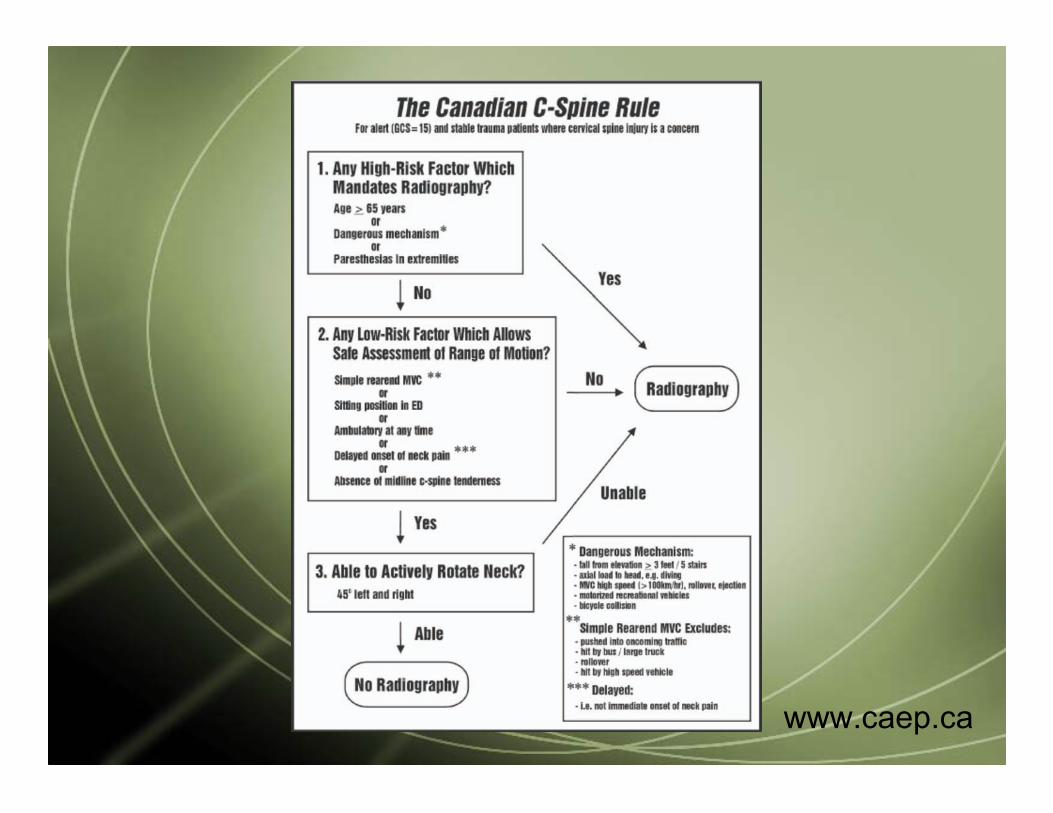
www.caep.ca
Taking this to the field…Wilderness EMS
Rural EMS
Urban EMS
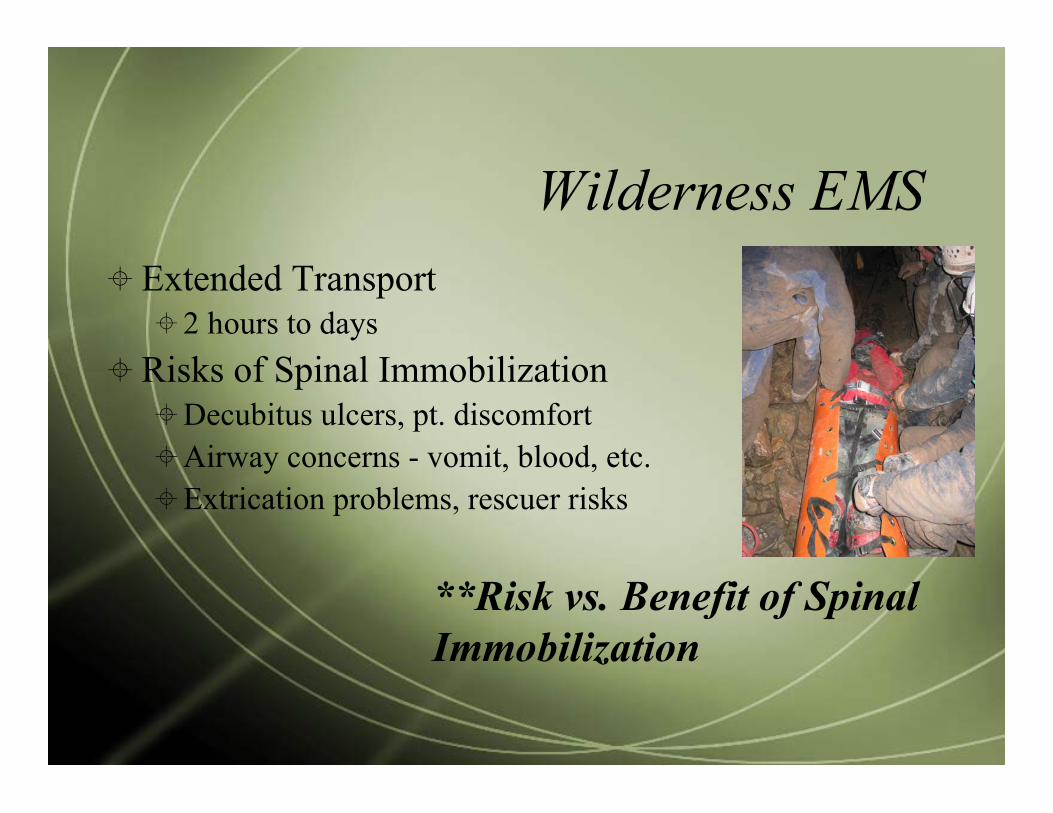
Wilderness EMS Extended Transport
2 hours to days Risks of Spinal Immobilization
Decubitus ulcers, pt. discomfortAirway concerns - vomit, blood, etc.Extrication problems, rescuer risks
**Risk vs. Benefit of SpinalImmobilization
Wilderness EMS
Wilderness EMSFocused Spine AssessmentAccepted protocol for Wilderness First
Responders (WFR)WMA, NOLS/WMI, SOLO
Rural EMSProlonged Transport
15 minutes to 1-2 hours
Pt. uncomfortableNo provider risk
Rural EMSSeveral Devices to Increase Comfort
Urban EMSRapid Transport
Less than 15 minutesPresent to emergency departments
Spine clearing protocolsNEXUS, Canadian C-Spine Rule
Xrays or CTs
Little risk to patients or EMS providers
Flight EMSPatient’s cleared in referral ED’s by CT
and board certified EM physicians placedback on boards for transfer to traumacenters.

Why change what we’re doing?Patient ComfortAirway Compromise
Vomit, Blood, PositionBreathing CompromiseSkin CompromisePatient/Provider safety in technical
settings
Some places have…MaineMichiganCaliforniaNational Park Service
Malaysia (by default)

Selective Spinal ImmobilizationProtocol Implementation
Review ResearchReferences are a startDo your own search as well!
Medical Director / Medical ControlSupportCritical for success
Selective Spinal ImmobilizationProtocol Implementation
Review Established ProtocolsState of MaineNational Park ServiceOthers
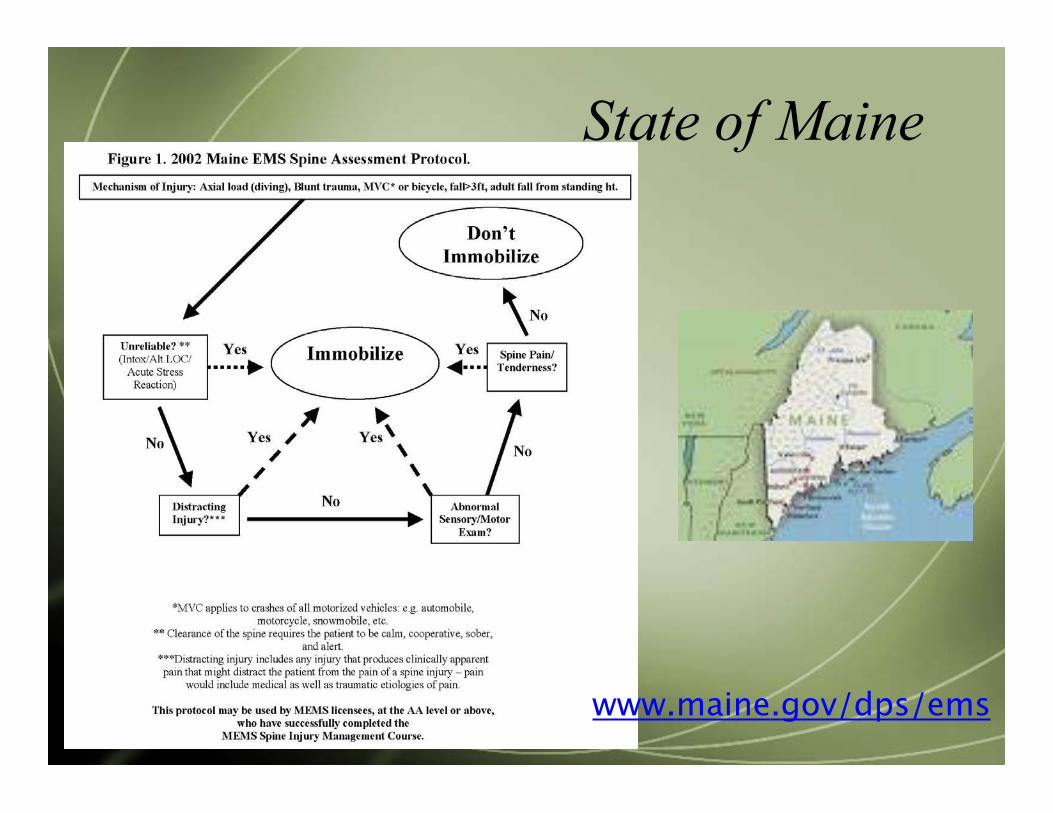
State of Maine
www.maine.gov/dps/ems
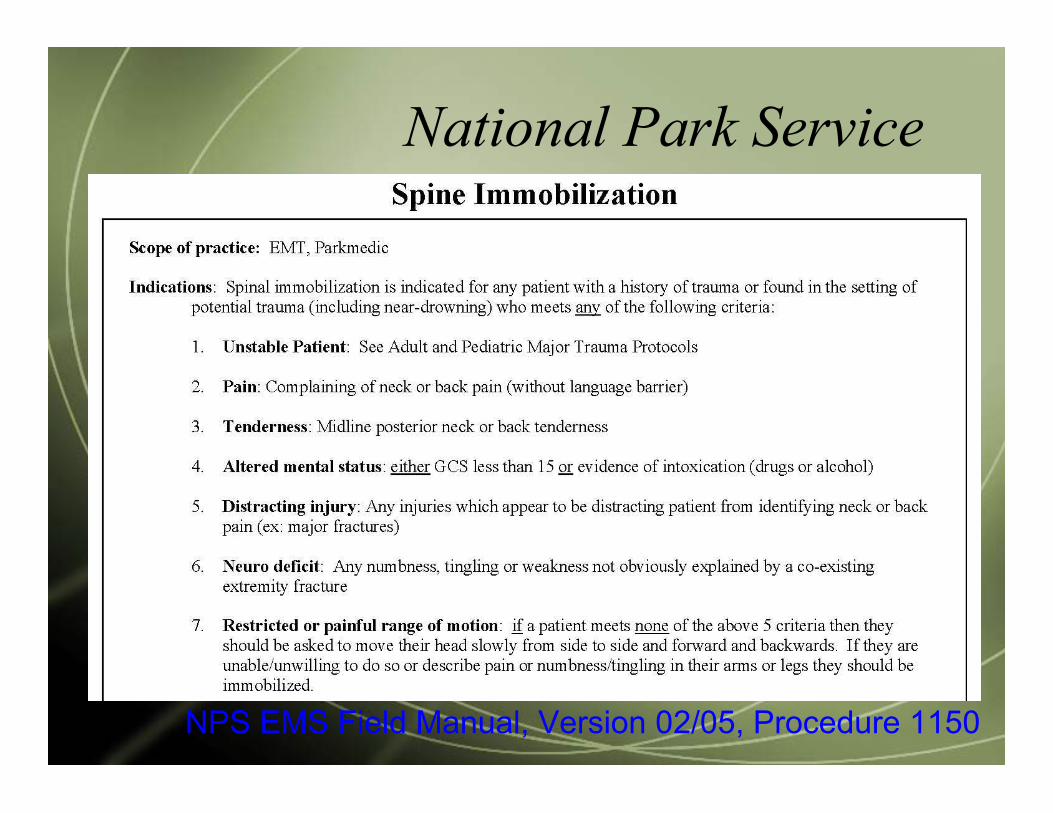
National Park Service
NPS EMS Field Manual, Version 02/05, Procedure 1150

Wilderness Medical Associates
www.wildmed.com
Selective Spinal ImmobilizationProtocol Implementation
Develop Protocol that works for yoursystemAge >65 get collar? Backboard?Peds excluded?
Selective Spinal ImmobilizationProtocol Implementation
Good QA/QI programEducation of EMS ProvidersOngoing Review of Decisions and
Outcomes
SummaryNot everyone with blunt trauma needs
spinal immobilization in the ED or in thefield
Selective spinal immobilization can andshould be done by prehospital providers
Questions???
Copy of lecture noteswww.wildmedconsulting.com
Questions?
Lecture Notes: www.wildmedconsulting.com