tobacco cessation - jackson county health … · result of cigarette smoking. ... patients smoking...
TRANSCRIPT
TOBACCO CESSATION
HEALTHCARE
PROVIDER TOOLKIT
November 2012, Version 2.0

2
TABLE OF CONTENTS
LETTER TO PROVIDERS 3
IT’S WORTH IT TALK TO YOUR PATIENTS 4
GETTING STARTED IN YOUR PRACTICE 5
PATIENT COMMUNICATION
MOTIVATIONAL INTERVIEWING 6
KEYS TO MOTIVATIONAL INTERVIEWING 7-8
MOTIVATIONAL INTERVIEWING: THE BASICS 9-10
THE FIVE Rs 11
CASE STUDIES 12-13
THE 5 A’S 14-16
THE 2 A’s +R 17
STAGES OF CHANGE 18
OFFICE TOOLS
PATIENT ENCOUNTER DOCUMENTATION 19
PATIENT INTAKE SURVEY 20
“PREPARING TO QUIT” HANDOUT 21
“BARRIERS & BENEFITS TO QUITTING” HANDOUT 22
PATIENT EDUCATION MATERIALS RESOURCE LIST 23
LOCAL RESOURCES
ILLINOIS TOBACCO QUITLINE 24-27
JACKSON COUNTY RESOURCES 28
NATIONAL RESOURCES 29-30
CONTINUING EDUCATION 31
TOBACCO CODING AND BILLING 32-35
MEDICARE BENEFITS 36
ACKNOWLEDGEMENTS 37-38

3
November 2012 Dear Healthcare Provider, According to the Illinois Department of Public Health each year more than 20,000 Illinoisans will die as a result of cigarette smoking. Overall, smoking is the single most important preventable cause of morbidity and mortality in the United States today. It is known that smoking cessation has many benefits, even for those who have smoked for years. As a provider you have an integral role in helping your patients achieve optimal health. By utilizing your skills, along with the resources in this toolkit, you can help to change the lives of your patients as you assist them in their journey to smoke-free living. This toolkit will provide you information on using the stages of change model to assess your patients smoking behaviors and readiness to quit smoking. It also includes tips for using motivational interviewing techniques and implementing the evidence-based 5 As model to enhance your smoking cessation messages. Finally, you will find that we have also included office aids and patient resources to further reinforce your message. We thank you for your interest in using this toolkit in your practice. If you have any questions or would like further information please contact Angie Bailey of Jackson County Health Department at 616-684-3143 ext. 134. Sincerely,
Miriam Link-Mullison
Miriam Link-Mullison Administrator Jackson County Health Department
4
IT’S WORTH IT: TALK TO YOUR PATIENTS
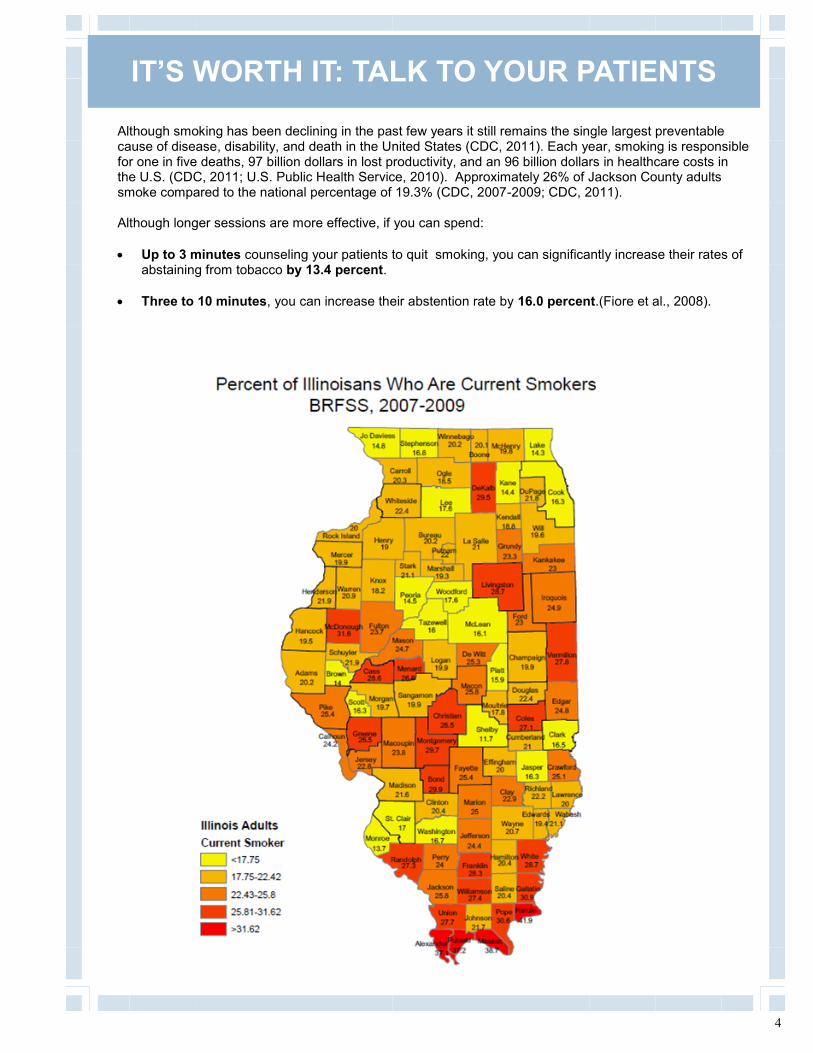
Although smoking has been declining in the past few years it still remains the single largest preventable cause of disease, disability, and death in the United States (CDC, 2011). Each year, smoking is responsible for one in five deaths, 97 billion dollars in lost productivity, and an 96 billion dollars in healthcare costs in the U.S. (CDC, 2011; U.S. Public Health Service, 2010). Approximately 26% of Jackson County adults smoke compared to the national percentage of 19.3% (CDC, 2007-2009; CDC, 2011). Although longer sessions are more effective, if you can spend:
Up to 3 minutes counseling your patients to quit smoking, you can significantly increase their rates of abstaining from tobacco by 13.4 percent.
Three to 10 minutes, you can increase their abstention rate by 16.0 percent.(Fiore et al., 2008).

5
1. Engage staff in a discussion about their own behaviors and their cessation experiences with patients.
What were the results? Were there techniques that were especially helpful that staff have used to talk with patients about smoking habits? What do the staff feel are areas for improvement in addressing patient smoking? 2. Consider the office environment. Are there messages that your office sends out related to healthy behaviors and smoking? Promoting smoking cessation can be as simple as a well placed poster or modeling positive behaviors. 3. Screen for smoking status and use a consistent method to track it on patient charts. Make it part of the patient’s normal intake forms and the part of the patient’s electronic health record. 4. Talk with patients. Motivational interviewing techniques can be used to increase patients’ belief in the importance of quitting and their belief in their ability to quit. 5. Connect to the community Patients can also be referred to various resources such as the Illinois Tobacco Quitline (1-866-QUIT-YES).
GETTING STARTED IN YOUR PRACTICE
As a healthcare provider you have a unique opportunity to help patients who may be interested in quitting or influence those who have not yet thought about quitting. Studies have shown that patient adherence to recommendations are more likely to be successful if suggested and encouraged by an individual’s physician (Stead, Bergson, & Lancaster, 2008). Here are some easy ways to get started in your practice.

6
Image adapted from Systems Training and Outreach Program. What to Do With a Patient Who Is Not Ready to Quit. Arkansas Department of Health. Used with permission. Retrieved from http://tinyurl.com/9ccg9sf
MOTIVATIONAL INTERVIEWING
Motivational Interviewing (MI) is a patient-centered counseling technique that focuses on “exploring a tobacco user’s feelings, beliefs, ideas, and values regarding tobacco use in an effort to uncover any ambivalence about using tobacco. Once ambivalence is uncovered, the clinician selectively elicits, supports, and strengthens the patient’s ‘change talk’ (e.g., reasons, ideas, needs for eliminating tobacco use) and ‘commitment language ‘ (e.g., intentions to take action to change smoking behavior, such as not smoking in the home). MI researchers have found that having patients use their own words to commit to change is more effective than clinician exhortations, lectures, for arguments for quitting, which tend to increase rather than lessen patient resistance to change.” (Fiore et al., 2008; p. 58). Meta-analyses of controlled clinical trials have found that MI is significantly more effective than comparison treatments in helping people to quit tobacco use (Hettema & Hendricks, 2010; Lai et al., 2010). Studies have found that MI was effective when delivered by primary care physicians and by counselors (Lai et al., 2010), as well as nurses (Karatay, Kublay, & Emiroglu, 2009; Borrelli et al., 2005). Longer sessions (> 20 minutes) are more effective, and multiple sessions are slightly more effective than single sessions (Lai et al., 2010). MI is based on four key principles: (1) express empathy, (2) develop discrepancy, (3) roll with resistance, and (4) support self-efficacy.

7
Express Empathy Develop Discrepancy
Keys to Motivational Interviewing
MOTIVATIONAL INTERVIEWING
Voice discrepancy between present behavior and expressed priorities: “It sounds like you are very devoted to
your family. How do you think your smoking is affecting your children?”
Reinforce and support “change talk” and “commitment” language: “So, you realize how smoking is affecting
your breathing and making it hard to keep up with your kids.”
“It’s great that you are going to quit when you get through this busy time at work.”
Build and deepen commitment to change: “There are effective treatments that will
ease the pain of quitting, including counseling and many medication options.”
“We would like to help you avoid a stroke like the one your father had.”
Open ended questions: “How important do you think it is for
you to quit smoking?” “What might happen if you quit?”
Reflective listening: “So you think smoking helps you
maintain your weight.” – Summarize
(“What I have heard so far is that smoking is something you enjoy. On the other hand, your boyfriend hates your smoking, and you are worried you might develop a serious disease.”)
Normalize feelings: “Many people worry about managing
without cigarettes.” Support right to choose or reject change: “I hear you saying you are not ready
to quit smoking right now. I’m here to help you when you are ready.”

8
Keys to Motivational Interviewing
Back off and use reflection when the pa-tient expresses resistance: “Sounds like you are feeling pressured
about your smoking.” Express empathy: “You are worried about how you would
manage withdrawal symptoms.” Ask permission to provide information: “Would you like to hear about some
strategies that can help you address that concern when you quit?”
Roll with Resistance Support Self-efficacy
Help the patient to identify and build on past successes: ”So you were fairly successful the last
time you tried to quit.” Offer options for achievable small steps toward change: Call the Illinois Tobacco Quitline (1-866-
QUIT-YES) for advice and information. Read about quitting benefits and
strategies. Change smoking patterns (e.g., no
smoking in the home). Ask the patient to share his or her ideas
about quitting strategies.
MOTIVATIONAL INTERVIEWING

9
MOTIVATIONAL INTERVIEWING: THE BASICS
ELICITING CHANGE TALK (Adapted from handouts by David Rosengren and from Miller WR, Rollnick S. (2002). Motivational
interviewing: Preparing people for change. (2nd ed.) New York, NY: Guilford Press.)
Eliciting Change Talk
Eliciting change talk is the consciously directive strategy on the part of the counselor for resolving ambivalence. If OARS (open questions, affirmations, reflective listening, and summarizing) were the only skills used by the counselor, it would be quite possible for the client to remain stuck in ambivalence. Instead of the counselor advocating for change, which often puts the clients in the position of defending against it, motivational interviewing takes a different approach. The idea is to have the counselor facilitate the client’s expression of change talk, that is, for the client to present the arguments for change.
Four Categories of Change Talk
Recognizing disadvantages of the status quo: “This is more serious than I thought.”
Recognizing advantages of change: “I’d probably feel a lot better.”
Expressing optimism about change: “I think I could do that if I decided to.”
Expressing intention to change: “I’ve got to do something.”
Methods for Evoking Change Talk
Asking evocative questions: “What worries you about your current situation?”
Using the importance ruler (also use this regarding a client’s confidence to change): “How important would you say it is for you to ____? On a scale of zero to ten, where zero is not at all important and ten is extremely important, where would you say you are?”
0 1 2 3 4 5 6 7 8 9 10 Not at all Extremely important Important
Exploring the decisional balance: “What do you like about your present pattern?” “What concerns you about it?”
Elaborating: “What else?”
Querying extremes: “What concerns you most about ___? “What are the best results you could imagine if you made a change?"
Looking back: “What were things like before you ___? What has changed?”
Looking forward: “How would you like things to be different a year from now?”
Exploring goals and values: “What things are most important to you?”

10
MOTIVATIONAL INTERVIEWING: THE BASICS
GIVING ADVICE
Giving Advice Intent of advice-giving in Motivational Interviewing
Not an attempt to convince the person of the folly of his or her ways
An opportunity to express concerns and help the individual make an initial commitment to the process of change
Can be thought of as helping with decision-making
Advice-giving: a few thoughts
It’s okay to express concerns
There are many ways people change
Help the person to evaluate options
Offer advice, don’t impose it
If the person is not ready for change, set the stage for when she or he might be
Suggested Methods
Ask permission: “Is it okay if I share something with you?”
Then make a statement of concern: “Your situation concerns me and here’s why…”
List concerns in a non-judgmental manner
“You’ve told me that you’ve been drinking a half gallon of vodka a day. The doctor has informed you that your liver is in trouble and you’ve noticed the physical changes. You also told me your partner is pretty frustrated with your drinking.”
Recognize and affirm that it is the individual’s decision to make. “Of course, it really doesn’t matter what I think, because this is your decision to make.”
Inquire about the client’s thoughts. “I wonder what you think.”
Emphasize change statements, provide affirmations and statements of hope. Source: Homelessness Resource Center, Substance Abuse and Mental Health Services Admini-stration. (2007). Motivational interviewing, the basics, eliciting change talk and giving ad-vice. Rockville, MD: SAMHSA. Retrieved from http://homeless.samhsa.gov/Resource/Motivational-Interviewing-Eliciting-Change-Talk-and-Giving-Advice-32841.aspx

11
THE 5 R’s OF MOTIVATIONAL INTERVIEWING
During Motivational Interviewing keep the 5 R’s in mind: Relevance, Risks,
Rewards, Roadblocks, and Repetition. (Fiore et al., 2008).
1. Relevance: Identify motivational factors and encourage the patient to
consider why quitting is personally important.
2. Risks: Discuss side-effects and dangers of tobacco use. Help iden-
tify the consequences of continued smoking such as personal and family health risks, financial costs, and example setting for chil-dren.
3. Rewards: Discuss the benefits of stopping. Help patient to identify
what the benefits to themselves and their family could include.
4. Roadblocks: Identify barriers to quitting. Address barriers that led to
relapse in past quit attempts and offer suggestions for coping ( see benefits and barriers page)
5. Repetition: Talk about tobacco cessation (in an abbreviated form) at
every visit for patients who smoke.

12
Case Study: Patient Not Willing to Quit Ron is a 22 year-old African American male who has been smoking for 4 years and is currently smoking 16-20 cigarettes per day. He has come into the office today for a chronic cough with difficulty breathing (bronchitis) and has recently been diagnosed with acid reflux and is taking Prilosec. Although his girlfriend (a non-smoker) wants him to quit, he has no desire to quit smoking and says he is tired of people nagging him about his smoking.
Using the spirit of Brief Motivational Interviewing: Asking, Listening, Informing Asking: Clinician: Tell me, what brings you into the office today?
Patient: I have had this cough for two weeks and I cannot get rid of it. I cough all night and cannot get any sleep.
Listening: Clinician: That must be wearing you out (empathy/reflection). How are you feeling right now?
Patient: Tired and weak. I’ve missed several days of work and I need the money. What can you give me?
Clinician: It is so hard to feel good if you aren’t sleeping well and even harder when you are under stress (Empathy/reflection). I see in your chart that you had a similar illness 5 months ago. Looks like you may have another episode of bronchitis.
Asking: Clinician: Do you have any sense what may be causing another round of infection?
Patient: Well I work in a restaurant and figure I am surrounded with sick people and germs.
Listening: Clinician: Silence – let the person reflect. Depending on what is said, this could be a follow-up question.
Asking: Clinician: How are you feeling about your smoking right now (elicit, open ended)?
Patient: I know I should quit or at least cut back (change talk) but I’m under a lot of stress right now and don’t even want to think it. I am so tired of people trying to get me to quit! All I want is something to make me feel better so I can get back to work.
Informing: Clinician: Even thinking about quitting while you are sick can be overwhelming for most people (empathy). Unfortunately, your immune system is weak from the toxins in the cigarette smoke and your body is having a hard time fighting the infection. (STOP – listen, silence; elicit change talk.)
Patient: I tried to quit last year but since I’m under so much stress, I have been smoking even more. My girlfriend wants me to quit – she nags me all of the time.
Clinician: Though you don’t want to quit right now and you are tired of people hassling you about it, you also think it would be good to quit or cut down. (Roll with resistance – not a question. State it as fact. Silence.).
Patient: Well, I guess I know that smoking is no good for me (change talk) but I didn’t know it breaks down my immune system. Can’t I just take an antibiotic like the last time? Clinician: Actually, the antibiotic is only a short term solution. Like you said, smoking isn’t any good for you and in all likelihood, you will develop another lung infection in the future. (Silence. Resist the urge to educate.)
Patient: I am not sure I can quit on my own – it didn’t work before. Do you have anything that can help me?
This is where MI stops and assisting the patient create a quit plan starts. By allowing the patient to self-discover through small pieces of information and a lot of self-reflection, real change can occur – within the patient.

13
Case Study: Patient Not Willing to Quit Elizabeth is a 69 year-old white female has been smoking for 52 years. She is currently smoking
16-20 cigarettes per day. She had a stroke two years ago. In addition to high blood pressure, she
has diabetes. She came in today to get her lipid levels checked. She does not want to quit at this
time because she says her life is too stressful. She is not interested in a Chronic Disease
Self-Management Program at this time.
Using Brief Motivational Interviewing techniques: How would you begin the conversation / establish rapport (OARS)? ______________________________________________________________________________________________________________________________________________________________ How would you express empathy and convey understanding to Elizabeth? ______________________________________________________________________________________________________________________________________________________________ How would you evoke change talk with Elizabeth? ______________________________________________________________________________________________________________________________________________________________ How would you roll with expressed resistance? ______________________________________________________________________________________________________________________________________________________________ How can you handle discrepancies between Elizabeth’s current behaviors and her expressed priori-ties, values, and goals? ______________________________________________________________________________________________________________________________________________________________ How you can support Elizabeth’s self-efficacy? ______________________________________________________________________________________________________________________________________________________________ For each aspect of Motivational Interviewing below, give an example of what you might say to Elizabeth: Encourage Elizabeth to verbally state why quitting is relevant to her. _______________________________________________________________________________ Ask Elizabeth to identify the negative consequences of tobacco use. _______________________________________________________________________________ Ask Elizabeth to identify benefits of stopping smoking. _______________________________________________________________________________ Ask Elizabeth to identify barriers to quitting. _______________________________________________________________________________

14
Starting a conversation about tobacco use can sometimes be difficult or may leave you feeling discouraged by patient response, but remember, as a healthcare provider you have the unique opportunity to influence patient behavior for the better. You can advocate for healthy behaviors, advise patients to quit smoking, support patients as they attempt to quit, and refer patients to medical and community resources that may help them. The Public Health Services’ 2008 Clinical Practice Guideline recommends using the 5 A’s model (Fiore et al., 2008).
PATIENT COMMUNICATION
The 5 A’s Model for Brief Tobacco-Use Treatment in Healthcare
Ask
Implement a system to ensure that every patient’s tobacco-use status (i.e., current, former, or never) is identified and documented at every visit.
Advise
Provide each patient who uses tobacco with a clear, strong, and personalized recommendation to quit.
Assess
Determine the patient’s willingness to make a quit attempt at this time (e.g., within the next 30 days).
Assist
Help the patient create a quit plan; provide brief practical counseling (problem solving and skills training), intra-treatment social support, and supplementary patient education materials as appropriate; and offer medication unless contraindicated. Provide or refer to more intensive treatment if the patient is interested. For patients not ready to make a quit attempt, provide brief counseling using the 5R’s, which is designed to promote the motivation to quit, as well as motivational interviewing techniques. (See p. 9)
Arrange
Schedule follow-up contact with the patient (either in person or by telephone), preferably within the first week after the quit date, and provide or refer to more intensive treatment if tobacco use has occurred after the quit date. This follow-up can also be done through the Illinois Tobacco Quitline (1-866-QUIT-YES).

15
Ask every tobacco user if he/she is willing to quit at this time. Use clear and strong language: “I think you should
quit smoking or chewing tobacco now.” Personalize the message, relating it to the patient's
symptoms, or to economic and social costs, or the impact on family members, e.g. “Your child may have fewer ear infections if you quit smoking.” “Continuing to smoke will make your asthma
worse.”
If willing to quit, provide resources and assistance (see Assist section). If unwilling to quit at this time, help motivate the patient:
Identify reasons to quit in a supportive manner. Build patient’s confidence about quitting.
Identify reasons for quitting and benefits of quitting
Set a quit date, ideally within 2 weeks. Assist tobacco users with a quit plan.
Suggest they remove tobacco products from their environment.
Suggest they get support from family, friends, and coworkers.
Review past quit attempts—what helped, what led to relapse.
Anticipate challenges, particularly during the critical first few weeks, including nicotine withdrawal.
Encourage use of medications such as nicotine patch, gum, or lozenge or give prescription for varenicline, bupropion SR, nicotine inhaler, or nasal spray, unless contraindicated.
Recommend toll free 1-866-QUIT–YES (1-866-784-8937), the Illinois Tobacco Quitline.
Refer to Web sites for free materials: NIH: http://www.smokefree.gov/ American Cancer Society: http://tinyurl.com/2fz7mvv
If the person has recently quit, help them determine ways to prevent relapse.
THE 5 A’S MODEL
Assess
Assist to Quit
Ask/Advise to Quit

16
THE 5 A’S MODEL
Schedule followup visits to review progress toward quitting. If a relapse occurs, encourage repeat quit attempts. Review the circumstances that caused relapse. Use relapse as a learning experience. Review medication use and problems. Refer patients to the Illinois QuitLine: 1-866-QUIT-YES (1-866-784-8937).
Flow chart from Fiore et al., 2009. (public domain)
Arrange Follow-up

17
IF YOU HAVE LESS THAN 3 MINUTES
Ask every patient if they use tobacco.
“Have you used tobacco in the past 30 days?”
If no: “Congratulations, quitting tobacco is one of the best things you can do for your health.
If yes:
Advise patients to quit.
“Quitting tobacco is one of the best things you can do for your health. I strongly
encourage you to quit.”
Refer patients to a resource for additional support.
Ready to Quit Provide direct referral to a support resource that will complete the “Assess, Assist and Arrange” steps, e.g., the Illinois Tobacco Quitline.
“Congratulations on your decision to quit tobacco. This is a resource that I
recommend. They will provide you with support, help you create a quit plan,
and help you overcome urges.”
Not Ready to Quit Provide self-help materials and let patients know you are available for future support.
“When you are ready to quit, I am here to support you and have resources that can assist you.”
If you have less than 3 minutes to counsel a patient, use this procedure based on the
5 A’s model:
Chart adapted from: Systems Training and Outreach Program. 2 As + R Tobacco Intervention Pocket Card. Arkansas Department of
Health. Retrieved from http://tinyurl.com/c7z272d Used with permission.

18
STAGES OF CHANGE
Stages of Change: Characteristics and Appropriate Actions
Stage Characteristics Appropriate Action
Pre-contemplation
• Reasons to continue smoking dominate • Limited interest in change
• Discuss personalized health benefits of quitting
Contemplation • Aware of problem • Conflicted about behavior • Considering change
• Consider small changes • Ask patient to build commitment
Preparation • Realizes benefit of making changes • Building a commitment to change
• Begin teaching behavior modification • Help patient plan for tempting situations • Help to set a quit date
Action • Taking active steps toward change
• Provide guidance and support • Consider pharmacotherapy
Maintenance • Initial treatment goals reached • Control relapse and monitor abstinence

19
PATIENT ENCOUNTER DOCUMENTATION
Ask (in person or use survey) Advise Assess Date: Initial: # of cigarettes per day: # of years smoked: # of quit attempts:
Smoke w/in 30 min of wake up
Relapsed
Other tobacco use: Smoking Location:
In home Outside home
In car Other
Discussed:
Relevance
Rewards
Risks
Roadblocks
Other:
No interest
Quit later
Ready to quit
Set quit date:
Maintain > 6 months
Quit < 6 months
Prevent relapse
Assist Arrange
Counsel
Handouts
Support
Pharmacotherapy
Outline
Referral
Follow-up appointment Quit date:
Ask (in person or use survey) Advise Assess Date: Initial: # of cigarettes per day: # of years smoked: # of quit attempts:
Smoke w/in 30 min of wake up
Relapsed
Other tobacco use: Smoking Location:
In home Outside home
In car Other
Discussed:
Relevance
Rewards
Risks
Roadblocks
Other:
No interest
Quit later
Ready to quit
Set quit date:
Maintain > 6 months
Quit < 6 months
Prevent relapse
Assist Arrange
Counsel
Handouts
Support
Pharmacotherapy
Outline
Referral
Follow-up appointment Quit date:

20
PATIENT INTAKE SURVEY
1. Have you ever smoked or used any tobacco? Yes ______ No ______ 2. Are you currently smoking or using tobacco? Yes ______ No ______ 3. Approximately how many cigarettes (or amount of smokeless) do you smoke in a day? Yes ______ No ______ 4. How soon after waking do you smoke your first cigarette or use your first tobacco? ______ 5. At what age did you start smoking or using tobacco? ______ 6. How many years have you smoked/ used tobacco? ______ 7. Do you use any other tobacco products? Yes ______ No ______ Check all that apply: Pipe ______ Cigars ______ Chew/Spit Tobacco ______ Water Pipe/Hookah ______ Bidis ______ Other ______ 8. On a scale of 1-10 how willing are you to quit smoking (10 is very willing)? 1 2 3 4 5 6 7 8 9 10 9. Have you tried to quit smoking/using tobacco in the past? Yes ______ No ______
About how many times? ______
What did you use to help you quit (Check all that apply)?
Patches ______ Lozenges ______ Nicotine Gum ______ Counseling ______ Pills_____ Other ______ No aids ______
10. Have you been diagnosed with any of the following (check all the apply): Asthma ______ Emphysema ______ Heart Disease ______ Diabetes ______ Stroke ______ Cancer ______ 11. Do other people currently smoke/use tobacco around you? Yes ______ No ______

21
PREPARING TO QUIT
Reasons I smoke: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— Times I usually smoke: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— My reasons to quit: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— Things I can do instead of smoking: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— Family & friends I can count on to help me: ——————————————————————————————————————————————————————————————————————————————————————————————————————————————————–————————————————— Others who can help me: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— Ways to handle others smoking around me: ———————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————————— Ways I can handle “slips”:
——————————————————————————————————————————————————————
——————————————————————————————————————————————————————
My Quit Date:
—————————————————————————-

22
Barrier
Coping Strategies
Negative Mood - Take part in some sort of physical activity. - Try deep breathing or another form of relaxation. - Talk to a trusted friend or family member. - Keep a journal.
Being Around Other Smokers - Ask others not to smoke around you. - Establish “smoke-free” zones in your home and car. - Walk away from others if they are smoking. - Remind yourself that you are a non-smoker.
Time Pressures - Take part in a physical activity to reduce stress in your life.
BARRIERS & BENEFITS TO QUITTING
Remember, the urge to smoke and other withdrawal symptoms will only last a few weeks at most and the benefits will be well worth it!
Benefits like:
You will be around longer to see children and grandchildren grow up. You will have more money that you can spend on other things. Your food will taste better. You will feel good about yourself and your accomplishment in quitting smoking. You will have more energy. You will be able to breathe easier. Your clothes, hair, home, and car will smell better. You won’t have any more yellow teeth or fingers. You won’t have inconvenient cigarette cravings. You will be less likely to develop heart disease, stroke,
lung cancer, emphysema, and other smoking-related diseases!

23
PATIENT EDUCATION MATERIALS
A variety of evidence-based patient education materials can be found online at:
AAFP Office Resources and Patient Education Materials http://www.aafp.org/online/en/home/clinical/publichealth/tobacco/resources.html
American Cancer Society: Guide to Quitting Smoking http://www.cancer.org/healthy/stayawayfromtobacco/guidetoquittingsmoking/index American Heart Association: Quitting Smoking http://tinyurl.com/492x5pj
HealthFinder.gov: Guide to Quitting Smoking http://healthfinder.gov/prevention/ViewTopic.aspx?topicId=24
MouthHealthy™: Smoking and Tobacco Videos (American Dental Association) http://www.mouthhealthy.org/en/az-topics/s/smoking-and-tobacco.aspx Use the pull down menu to see different videos.
Resources for Smokers (Smoking Cessation Leadership Center) http://smokingcessationleadership.ucsf.edu/FSStopSmoking.htm
Smokefree.gov http://www.smokefree.gov/Default.aspx Includes a Quit Guide, a text messaging support program, mobile phone apps, and more tools for patients.
Tobacco Publications Catalog (CDC) http://apps.nccd.cdc.gov/osh_pub_catalog/PublicationList.aspx Features free brochures, posters, flyers and other media materials about smoking that can be given to patients or used in an office setting.
Treating Tobacco Use and Dependence: 2008 Update (AHRQ) http://www.ahrq.gov/path/tobacco.htm Includes brochures that you can print and give to patients.

24
Illinois Tobacco Quitline Facts
ILLINOIS TOBACCO QUITLINE
Educational materials available in Spanish, Chinese, Khmer, Vietnamese and Polish
Access to more than 200 other languages
TDD for the Deaf and Hard of Hearing: 1-800-501-1068
Website: www.quityes.org; access to our chat line, talk with a quitline staff member live
The services are unlimited—clients can call as often as they need to.
Phone - 1-866-QUIT-YES (1-866-784-8937)
It’s Free
All services are completely confidential
Convenient hours of operation: DAILY— 7 a.m. to 11 p.m. (Central Time)
Staffed by registered nurses, respiratory therapists, and certified tobacco treatment specialists
Spanish-speaking staff members on-site
The Illinois Tobacco Quitline (ITQL) is funded by the state of Illinois to provide tobacco cessation services, free of charge, over the telephone. ITQL services are available to all residents of Illinois regardless of location. Counseling is the backbone of the Illinois Tobacco Quitline program. Clients are educated and counseled in tobacco cessation to create a solid basis for a plan tailored to each individual’s needs. The use of nicotine replacement therapies and medications are integrated into the cessation program, with a special emphasis on behavioral modification. Throughout the counseling process the client and counselor will discuss the “ins and outs” of physical addiction and withdrawal, behavior patterns and triggers as obstacles to quitting, distracters and coping strategies. Calls to the Illinois Tobacco Quitline are not limited: we accept calls from clients for as long as they feel they need our support and assistance. Our staff of registered nurses, respiratory therapists and certified tobacco treatment specialists attend accredited Nicotine Dependence training programs at renowned medical research and education centers, to become skilled in smoking cessation therapies. Each of our nurses and therapists has at least 20 years of medical experience and is qualified to answer questions regarding lung health and disease, in addition to providing guidance in tobacco cessation. The Illinois Tobacco Quitline functions under the direction of a Medical Advisory Board, comprised of physicians who are board certified allergists and pulmonologists, to ensure that the information shared is timely, accurate, and consistent with current accepted clinical practice. The Illinois Tobacco Quitline’s performance is reviewed on an ongoing basis so that the best possible service can be provided. All aspects of the Quitline service are evaluated by clients and partners ensure quality control.

25
To order these and other Quitline materials please fill out the provided
materials order form or you may download additional order forms at www.quityes.org
ILLINOIS TOBACCO QUITLINE MATERIALS

26
FAX REFERRAL INFORMATION
Illinois Tobacco Quitline Electronic Fax Referral/Electronic Medical Record Program
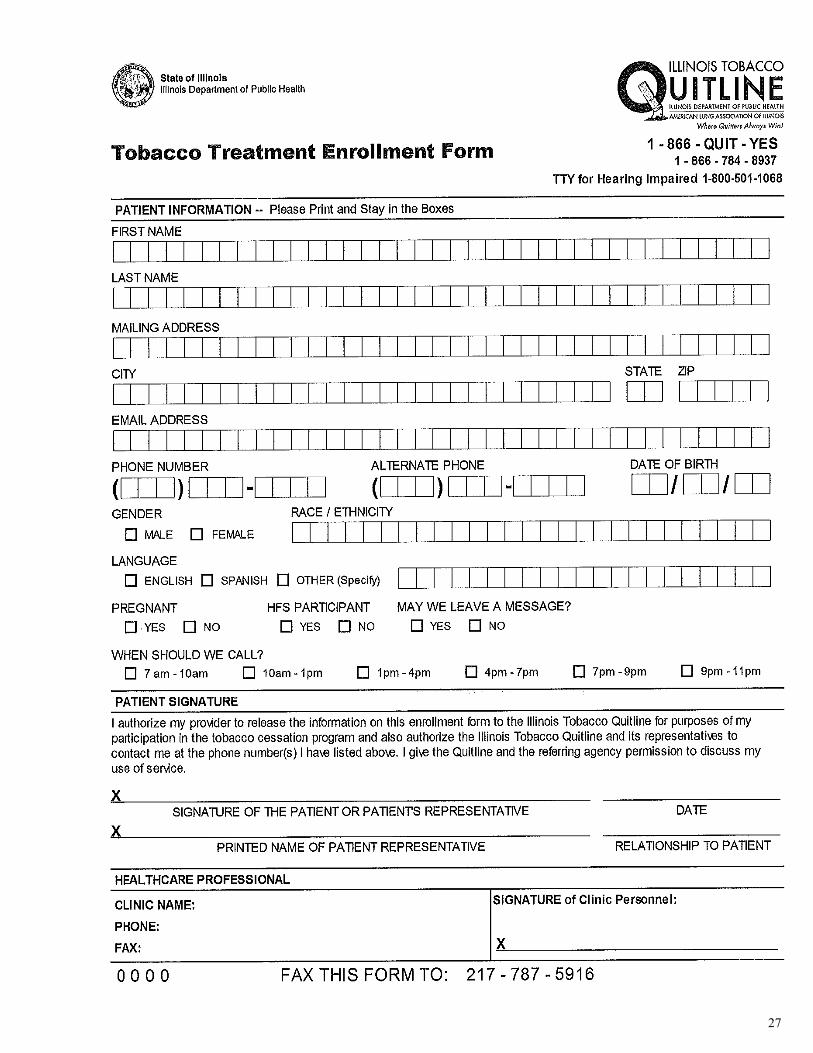
Tobacco users who receive advice and resources to quit from their health care provider have higher satisfaction rates yet, only 33% of tobacco users report being advised to quit and referred to a program by a doctor. In addition, providers and clinic staff often do not have the time in their busy schedules or the necessary counseling skills to effectively counsel patients on tobacco cessation. The growing implementation of Fax Referral/ Electronic Fax Referral and Electronic Medical Records (EMR) in primary care may provide an opportunity to more systematically identify and refer smokers to the Illinois Tobacco Quitline (ITQL), thereby increasing the number of smokers who receive help for tobacco dependence. If a health care provider recommends quitting and makes a treatment referral, clients are more likely to make a quit attempt and ultimately stop smoking. Fax Referrals give providers an additional opportunity to easily, quickly, and effectively connect clients with individualized tobacco cessation help. Simply, print of copy the referral form and type, stamp or write in your Provider Information to personalize the form for your use if you so choose. Once client consents to being contacted by the Illinois Tobacco Quitline, have the client complete
contact information and sign the form. Please fill in the form completely, also filling in Assessment and Assistance checkboxes. Be sure to get the Patient or Patient Representative Signature.
Please use the 5A’s (Ask, Advise, Assess, Assist, Arrange) to assess clients readiness and assistance to quit sections. Once the fax referral is completed, fax it to 217-787-5916. It’s that easy! The ITQL will call the client and begin the tobacco cessation counseling protocol. Provider Follow-Up: Providers are encouraged to arrange follow-up appointments to discuss the client’s progress towards cessation. Important things to know: Fax Referrals may ONLY be used if the client gives their written consent. In order to use Fax Referrals your practice must be a HIPAA Covered Entity (e.g., doctor’s office,
dentist’s office, hospital, clinic or agency site) Important things to know: Fax Referrals may ONLY be used if the client gives their written consent. In order to use Fax Referrals your practice must be a HIPAA Covered Entity (e.g., doctor’s office, dentist’s office, hospital, clinic or agency site)
27
28
Illinois Tobacco Quitline American Lung Association Phone: 1-866-QUIT-YES (1-866-784-8937) Website: www.quityes.org Hours: Sun-Sat 7am– 11 pm
Personalized, over the phone smoking cessation for FREE. There is no limit on the number of calls. If you can’t get through or are placed on hold, leave a message with your contact information and you will be called back.
SIUC Student Wellness Center Southern Illinois University-Carbondale 374 East Grand Avenue Carbondale, IL 62901 Phone: 618-536-4441 Website: shc.siu.edu Hours: Mon-Fri 8:00a-4:30p
One on one smoking cessation counselors are available to SIUC students by appointment. Appointments can be made at the Wellness Center located on the first floor of the Student Health Center.
Memorial Hospital of Carbondale Deb Newbolds 405 West Jackson Carbondale, IL 62901 Phone: 618-549-0721 ext. 65616
Individual consultations and counseling for patients who get a physicians order to receive services. FREE handouts available.
SIUC Dental Hygiene Clinic Joan Davis Southern Illinois University- Carbondale 1365 Douglas Drive Carbondale, IL 62901 Phone: 618-453-8826 Website: www.sah.siu.edu/DH/clinic.htm Hours: Vary by semester. See website for details.
Chair-side cessation intervention, referrals, quit kits and pamphlets available to SIUC students, faculty and community residents.
St. Joseph Memorial Hospital Diane Moore 2 South Hospital Drive Murphysboro, IL 62966 Phone: 618-684-3156 ext. 55381
Individual consultations and counseling for patients who get a physicians order to receive services. Handouts and phone follow-ups available for FREE.
Jackson County Health Department Angie Bailey 415 Health Department Road Murphysboro, IL 62966 Phone: 618-453-3143 ext. 134 Website: www.jchdonline.org/
Offers FREE educational materials and serves as a source of information and referral to further services.
JACKSON COUNTY RESOURCES
29
HEALTHCARE PROVIDER RESOURCES
AAFP: Treating Tobacco Dependence Practice Manual: Build a Better Office System http://bit.ly/V6Eq7s Focuses on creating an office climate and systems that promote tobacco cessation.
Alliance for the Prevention and Treatment of Nicotine Addiction http://www.aptna.org Links to healthcare provider toolkits, patient resources, and online training resources.
CDC: Primary Care and Public Health Initiative: Tobacco Cessation http://www.cdc.gov/primarycare/materials/smokingcessation/index.html Includes a materials from a teleconference course (slides, transcript, audio) plus links to additional resources for providers. From the Office for State, Tribal, Local and Territorial Support (OSTLTS).
Center for Tobacco Research and Intervention (University of Wisconsin) http://www.ctri.wisc.edu Resources and training materials healthcare providers, researchers, insurers, employers, advocates, and consumers.
Reports for Health Care Professionals (U.S. Surgeon General’s Initiative on Tobacco) http://www.surgeongeneral.gov/initiatives/tobacco/
Smoking and Tobacco Use (Centers for Disease Control and Prevention) http://www.cdc.gov/tobacco/ Cessation program materials for consumers and healthcare providers. The CDC has resources specifically for state tobacco control program managers and staff in state health departments, as well as partner organizations at the Cessation Resource Center (https://nccd.cdc.gov/CRC/index.aspx).
Tobacco Cessation Leadership Network http://www.tcln.org Resources and tools for health plans, health professionals, purchasers, state agencies, and tobacco control advocates.
Tobacco Technical Assistance Consortium (Emory University) http://www.ttac.org General information, technical assistance, and training to state and community organizations involved in tobacco control.

30
RESOURCES FOR CONSUMERS American Cancer Society
Set Yourself Free: Deciding How to Quit: A Smoker’s Guide http://tinyurl.com/cg2kg38
Excellent resource for helping consumers prepare to quit
Stay Away from Tobacco http://www.cancer.org/Healthy/StayAwayfromTobacco/ Includes guides for quitting smoking and smokeless tobacco products, suggestions for family and friends, information about tobacco and cancer, and more. Smoking Cost Calculator http://tinyurl.com/2gygbeh Consumers can find out how much money they are spending on cigarettes over time.
American Heart Association Quit Smoking http://tinyurl.com/492x5pj Tips to control weight gain, information for friends and family, smoking cost calculator.
HealthFinder.gov
Guide to Quitting Smoking http://healthfinder.gov/prevention/ViewTopic.aspx?topicId=24 Another excellent resource that includes suggested action steps as well as an overview of why it is important to quit.
National Cancer Institute Clearing the Air: Quit Smoking Today http://www.smokefree.gov/pubs/clearing_the_air.pdf This booklet helps tobacco users create an action plan for quitting.
Smokefree.gov
http://www.smokefree.gov/ This website includes several resources for consumers, including free cell phone apps and texting support services, as well as links to sites tailored for teens and women. There is a Spanish language version of the site.
National Institute of Dental and Craniofacial Research
Smokeless Tobacco: A Guide for Quitting http://tinyurl.com/as4du3l

31
CONTINUING EDUCATION
Both fee-based and no-cost clinician training resources are listed on many of the Web sites noted in this toolkit. The following are examples of tobacco-use treatment training resources that are available at no cost if continuing education credits are not needed:
Adolescent Tobacco Use—Prevention and Cessation: Strategies for Primary Care Providers http://www.idph.state.il.us/TobaccoWebSite/factsheets/SC_12UP.PDF A consensus statement from an expert panel sponsored by the Illinois Chapter of the American Academy of Pediatrics. Includes stages of change theory and the 5 As.
APTNA: Online Provider Education Courses http://www.aptna.org/APTNA_Online_Courses_General.html
CDC: Primary Care and Public Health Initiative: Smoking Cessation (OSTLTS) http://www.cdc.gov/primarycare/materials/smokingcessation/index.html Materials from the Office for State, Tribal, Local and Territorial Support’s 2012 teleconference course, includ-ing audio, transcript, presentation slides, and links to additional resources.
Center for Tobacco Research and Intervention (University of Wisconsin) http://www.ctri.wisc.edu/HC.Providers/healthcare.htm Offers training manuals (including Treating Tobacco Use and Dependence: Practical Strategies to Help Your Patient Quit), presentations, an online continuing medical and nursing education activities, webinars, videos (including examples of motivational interviewing), billing codes, and other training resources.
Rx for Change: Clinician-Assisted Tobacco Cessation (University of California-San Francisco School of Pharmacy) http://rxforchange.ucsf.edu Offers a comprehensive training program for clinicians who want to better assist patients with quitting, includ-ing teaching materials, case scenarios, short videos, and extensive continuing education materials.
Tobacco Cessation Online Learning Center (University of Arizona HealthCare Partnership) http://www.aztreattobacco.org Includes links for additional resources and training for tobacco treatment specialists. Requires registration (at no charge) for full access.
U.S. Surgeon General Initiatives: Tobacco http://www.surgeongeneral.gov/initiatives/tobacco/ Provides access to reports on smoking, including Preventing Tobacco Use Among Youth and Young Adults (2012).
General Motivational Interviewing Video Resources (YouTube)
Ineffective Interaction: http://www.youtube.com/watch?v=80XyNE89eCs&feature=related
Effective Interaction: http://www.youtube.com/watch?v=URiKA7CKtfc&feature=related
Elicit Change: http://www.youtube.com/watch?v=dm-rJJPCuTE
Rollnick: Roll w/ Resistance : http://www.youtube.com/watch?v=KTj4VncnE5g&feature=related
Australian Heart Association Motivational Interviewing (each video is 8-10 min)
Part 2 (Concept Overview) http://www.youtube.com/watch?v=-aTe4LpGz_E&feature=relmfu
Part 3 (MI Spirit) http://www.youtube.com/watch?v=nim62l1oaN4&feature=channel&list=UL
Part 4 (Change Talk) http://www.youtube.com/watch?v=Pwu99NIGiXU&feature=relmfu
Part 5 (OARS) http://www.youtube.com/watch?v=-zEpwxJlRQI&feature=relmfu
Part 6 (Summary ) http://www.youtube.com/watch?v=se7gJCjNo2Q&feature=relmfu

32
CODING & BILLING Here are some resources that may help you with reimbursement and coding questions. ***Please also see the American Lung Association handout on State of Illinois reimbursement policies (http://www.lungusa2.org/cessation2/statedetail.php?stateId=17) See the Medicare.gov site for up-to-date information about coverage (http://www.medicare.gov/coverage/smoking-and-tobacco-use-cessation.html). AAFP: Treating Tobacco Dependence Practice Manual: Build a Better Office System http://bit.ly/V6Eq7s The manual focuses on creating an office climate and systems that promotes tobacco cessation.
Build a Financial Infrastructure: Health Plan Benefits and Provider Reimbursement for the Treatment of Tobacco Dependence. (Tobacco Cessation Leadership Conference) http://www.tcln.org/cessation/PCHT.html
Coding Information Regarding the Diagnosis of and Billing for Tobacco Dependence Treatment http://www.ahrq.gov/path/tobacco.htm This is Appendix C of USPHS’s Treating Tobacco Use and Dependence—2008 Update: A Clinical Practice Guideline.
Current Procedural Terminology Codes for Tobacco-Use Screening and Counseling http://www.businessgrouphealth.org/benefitstopics/topics/purchasers/fullguide.pdf (Page 97 of A Purchaser’s Guide to Clinical Preventive Services: Moving Science into Coverage)
Helping Smokers Quit: Tobacco Cessation Coverage 2011. (American Lung Association) http://www.lung.org/assets/documents/publications/smoking-cessation/helping-smokers-quit-2011.pdf Discusses the impact of the Affordable Care Act on tobacco cessation treatment coverage.
Reimbursement for Smoking Cessation Therapy: A Healthcare Practitioner’s Guide (PACT) http://www.endsmoking.org/resources/reimbursementguide/pdf/reimbursementguide-3rd-edition.pdf
Reimbursement/Payment for Tobacco-Use Treatment (AAFP) http://www.aafp.org/online/en/home/clinical/publichealth/tobacco/reimbursement.html Includes many resources, including a list of HCPCS, CPT, & ICD-9 Codes related to tobacco cessa-tion counseling.
Smoking and Tobacco-Use Cessation Counseling Services (Medicare) http://www.cms.hhs.gov/MLNproducts/downloads/smoking.pdf Medicare Learning Network brochure. Also see http://www.medicare.gov/coverage/smoking-and-tobacco-use-cessation.html for additional information about Medicare coverage.)
Tips on Getting Paid for Smoking Cessation Treatment (Amer. Medical Association) http://www.ama-assn.org/amednews/2011/06/06/bica0606.htm An article by VA Elliott in the Amednews.com newsletter.

33
CODING & BILLING ICD-9 Diagnosis Codes (All codes with .x or .xx require fourth and fifth digits. See the ICD-9 manual for complete descriptions.):
140.x Malignant neoplasm, lip 141.x Malignant neoplasm, tongue 143.x Malignant neoplasm, gum 144.x Malignant neoplasm, floor of mouth 145.x Malignant neoplasm, other parts mouth 146.x Malignant neoplasm, oropharynx 147.x Malignant neoplasm, nasopharynx 148.x Malignant neoplasm, hypopharynx 149.x Malignant neoplasm, other and ill-defined sites within the lip, oral cavity, and pharynx 150.x Malignant neoplasm, esophagus 151.x Malignant neoplasm, stomach 157.x Malignant neoplasm, pancreas 161.x Malignant neoplasm, larynx 162.x Malignant neoplasm, trachea, bronchus and lung 180.x Malignant neoplasm, cervix uteri 188.x Malignant neoplasm, bladder 189.0 Malignant neoplasm, kidney except pelvis 205.xx Acute myeloid leukemia 231.x Carcinoma in situ respiratory system 250.xx Diabetes mellitus 296.xx Episodic mood disorders 300.4 Dysthymic disorder 311 Depressive disorder, not elsewhere classified 366.xx Cataract 401.x Essential hypertension 402.xx Hypertensive heart disease 403.xx Hypertensive chronic kidney disease 404.xx Hypertensive chronic heart and kidney disease 405.xx Secondary hypertension 410.xx Acute myocardial infarction 411.xx Other acute and subacute ischemic heart disease 412 Old myocardial infarction 413.x Angina pectoris 414.0x Coronary atherosclerosis 415.0 Acute cor pulmonale 415.1x Pulmonary embolism and infarction 416.x Chronic pulmonary heart disease 420.xx Acute pericarditis 421.x Acute and subacute endocarditis 422.xx Acute myocarditis 425.x Cardiomyopathy 423.x Other diseases of the pericardium 424.xx Other diseases of the endocardium 425.x Cardiomyopathy 426.xx Conduction disorders 427.xx Cardiac dysrhythmias

34
CODING & BILLING ICD-9 Diagnosis Codes Continued
428.xx1 Heart failure 1 If heart failure is due to hypertension, code first 402.0-402.9 with fifth digit 1 or code 404.0-404.9 with fifth digit 1 or 3. 429.xx Other ill-defined heart disease 430 Subarachnoid hemorrhage 431 Intracerebral hemorrhage 432.x Other and unspecified intracranial bleeding 433.xx Occlusion and stenosis of precerebral arteries 434.xx Occlusion of cerebral arteries 435.x Transient cerebral ischemia 436 Acute, but ill-defined, cerebrovascular disease 437.x Other and ill-defined cerebrovascular disease 438.xx Late effects of cerebrovascular disease 440.xx Atherosclerosis 441.xx Aortic aneurysm and dissection 442.xx Other aneurysm 443.xx Other peripheral vascular disease 444.xx Arterial embolism and thrombosis 445.xx Atheroembolism 461.x Acute sinusitis 462 Acute pharyngitis 463 Acute tonsillitis 464.xx Acute laryngitis and tracheitis 465.x Acute upper respiratory infections of multiple or unspecified sites 466.xx Acute bronchitis and bronchiolitis 472.x Chronic pharyngitis and nasopharyngitis 473.x Chronic sinusitis 474.xx Chronic disease of tonsils and adenoids 476.x Chronic laryngitis and laryngotracheitis 477.x Allergic rhinitis 478.xx Other diseases of upper respiratory tract 480.x Viral pneumonia 481 Pneumococcal pneumonia 482.xx Other bacterial pneumonia 483.x Pneumonia due to other specified organism 484.x Pneumonia in infectious diseases classified elsewhere 485 Bronchopneumonia, organism unspecified 486 Pneumonia, organism unspecified 487.0 Influenza with pneumonia 490 Bronchitis, not specified as acute or chronic 491.xx Chronic bronchitis 492.x Emphysema 493.xx Asthma 496 Chronic airway obstruction, not elsewhere classified 523.3x Aggressive and acute periodontitis 523.4x Chronic periodontitis

35
CODING & BILLING ICD-9 Diagnosis Codes Continued
531.xx Gastric ulcer 532.xx Duodenal ulcer 533.xx Peptic ulcer 733.xx Osteoporosis *This list was formulated based on the 2004 Surgeon General’s Report on the Health Consequences of Smoking. It is not an all-inclusive list and may be subject to different interpretation of the report. PRIVATE PAYER SMOKING CESSATION THERAPY BENEFITS Private payer benefits are subject to specific plan policies. Before providing service, benefit eligibility and payer coding requirements should be verified. HCPCS/CPT Codes: 99406: Smoking and tobacco-use cessation counseling visit; intermediate, greater than 3 minutes up to 10 minutes. Short descriptor: Smoke/Tobacco counseling 3-10
99407: Smoking and tobacco-use cessation counseling visit; intensive, greater than 10 minutes. Short descriptor: Smoke/Tobacco counseling greater than 10
S9075: Smoking Cessation Treatment
S9453: Smoking Cessation Classes, non-physician provider, per session
Various Evaluation and Management Services (associated with acute or chronic care). When providing an E/M service, if greater than fifty percent of face-to-face time with patient is spent in counseling, time may be used as a basis for selection of level of service.
99381-99397: Preventive medicine services
96150-96155: Health & Behavior Assessment/Intervention (Non-physician only)
99078: Physician educational services in a group setting ICD-9 diagnosis codes (All codes with .x or .xx require fourth and fifth digits. See the ICD-9 manual for complete descriptions.): 305.1 Tobacco use disorder 649.0x Tobacco use disorder complicating pregnancy, childbirth, or puerperium 989.84 Toxic effect of other substances, chiefly nonmedicinal as to source, tobacco* * List additional code to specify nature of toxic effect, excludes localized toxic effects classified elsewhere and respiratory conditions due to external agents and if applicable, any diagnosis code(s) for condition(s) evaluated and managed in the same encounter. ® CPT is a registered trademark of the American Medical Association. Current Procedural Terminology (CPT®) is copyright 2010 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values, or related listings are included in CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS restrictions apply to government.

36
Type of Benefit Standard Part B Benefit Preventive Service
Qualifying Medicare Patients
1. A patient who uses tobacco and has been diagnosed with a recognized tobacco-related disease or who exhibits symptoms consistent with tobacco-related disease;
2. A patient who uses tobacco and whose treatment is adversely affected by tobacco use;
3. And whose counseling is furnished by a qualified physician or other Medicare recognized practitioner.
1. Patients who use tobacco but are asymptomatic of tobacco-related disease;
2. Who are competent and alert at the time that counseling is provided;
3. And whose counseling is furnished by a qualified physician or other Medicare recognized practitioner.
CPT Codes 99406 - Smoking and tobacco-use cessation counseling visit; intermediate, greater than 3 minutes up to 10 minutes. 99407 - Smoking and tobacco-use cessation counseling visit; intensive, greater than 10 minutes.
G0436 - Smoking and tobacco cessation counseling visit for the asymptomatic patient; intermediate, greater than 3 minutes, up to 10 minutes. G0437 - Smoking and tobacco cessation counseling visit for the asymptomatic patient; intensive, greater than 10 minutes.
ICD-9 Diagnosis Codes
305.1 - non-dependent tobacco use disorder and ICD-9 of condition adversely affected or condition for which treatment is adversely affected by tobacco use.
305.1 - non-dependent tobacco-use disorder, or V15.82, history of tobacco use.
Patient Out-of-Pocket Cost
Patient is responsible for both co-insurance and unmet deductible.
Medicare pays full allowable amount. Patient has no out-of-pocket cost.
Frequency 2 attempts per year, maximum of 4 sessions each attempt.
2 attempts per year, maximum of 4 sessions each attempt.
MEDICARE BENEFITS
Tobacco Cessation Counseling - 2012 Medicare Benefits
Developed by Cindy Hughes, CPC, PCS. Copyright © 2011 American Academy of Family Physicians.
Physicians may photocopy or adapt for use in their practices; all other rights reserved.

37
Special Thanks To: Joan Davis, RDH, CTTS, PhD, Professor in the College of Applied Science and Arts, Southern Illinois University Carbondale Angie Bailey, Director of Health Education, Jackson Co. Health Dept. Heidi Hale, MPH Practicum Student Mary Taylor, MPH Practicum Student Mary Williams, Southern Illinois Healthcare Pam Drew, Jackson County Health Department Funding for the development and distribution of this toolkit provided by the American Cancer Society.
Toolkit compiled from the following sources: American Academy of Family Physicians. Ask and Act Practice Toolkit. Retrieved from
http://www.aafp.org/online/en/home/clinical/publichealth/tobacco/toolkit.html Borrelli B, Novak S, Hecht J, Emmons K, Papandonatos G, Abrams D. (2005). Home health
care nurses as a new channel for smoking cessation treatment: outcomes from project CARES (Community-nurse Assisted Research and Education on Smoking). Preventive Medicine, 41(5-6), 815-821.
CDC. (2007-2009). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, GA:
U.S. Dept. of Health and Human Services, CDC. CDC (2011, September). CDC Vital Signs: Adult Smoking in the US. Retrieved from http://
www.cdc.gov/vitalsigns/AdultSmoking/ Fiore MC, Jaén CR, Baker TB, et al. (2008). Treating tobacco use and dependence: 2008
update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service. Retrieved from http://www.ahrq.gov/clinic/tobacco/treating_tobacco_use08.pdf
ACKNOWLEDGEMENTS

38
ADDITIONAL REFERENCES
ACKNOWLEDGEMENTS continued Fiore MC, Jaén CR, Baker TB, et al. (2009). Treating tobacco use and dependence:
2008 update: Quick reference guide for clinicians. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service. Retrieved from http://www.ahrq.gov/clinic/tobacco/tobaqrg.pdf
Hettema JE, Hendricks PS. (2010). Motivational interviewing for smoking cessation: a
meta-analytic review. Journal of Consulting and Clinical Psychology, 78(6), 868-884.
Illinois Health Connect. Provider education webinars. Retrieved from http://www.illinoishealthconnect.com/provider/providereducation/
providereducationdetails.aspx Karatay G, Kublay G., Emiroğlu ON. (2010). Effect of motivational interviewing on
smoking cessation in pregnant women. Journal of Advanced Nursing 66(6), 1328-1337.
Kwong, J. (2011). Smoking cessation. In U.S. Department of Health and Human
Services, Health Resources and Services Administration, HIV/AIDS Bureau. Guide for HIV/AIDS clinical care. Rockville, MD: DHSS. Retrieved from http://hab.hrsa.gov/deliverhivaidscare/clinicalguide11/cg-308_smoking_cessation.html
Lai DTC, Cahill K, Qin Y, Tang JL. (2010). Motivational interviewing for smoking
cessation. Cochrane Database of Systematic Reviews. Issue 1. Art. No.: CD006936. DOI: 10.1002/14651858.CD006936.pub2.
Massachusetts Dept. of Public Health. QuitWorks: Child and family practitioners.
Retrieved from http://quitworks.makesmokinghistory.org/tools-resources-3/child-and-family-
practitioners.html Miller WR, Rollnick S. (2002). Motivational interviewing: Preparing people for change.
(2nd ed.) New York, NY: Guilford Press. NACCHO. Toolbox: Tobacco. Retrieved from http://naccho.org/toolbox/index.cfm?v=4&id=235&topicname=Tobacco National Cancer Institute. (1994). Tobacco and the clinician: Interventions for medical
and dental practice. Smoking and Control Monographs, #5. Retrieved from http://cancercontrol.cancer.gov/tcrb/monographs/5/index.html U.S. Public Health Service, Office of the Surgeon General. (2010). How tobacco
smoke causes disease: the biology and behavioral basis for smoking-attributable disease: a report of the Surgeon General. Rockville, MD: Dept. of Health and Human Services, Public Health Service, Office of Surgeon General. Retrieved from http://www.surgeongeneral.gov/library/reports/tobaccosmoke/full_report.pdf