tobacco screening and treatment for adult cancer · pdf filetobacco screening and treatment ....
TRANSCRIPT

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
TOBACCO SCREENING AND TREATMENT FOR ADULT CANCER PATIENTS
Effective Date: August, 2016
The recommendations contained in this guideline are a consensus of the Alberta Cancer Prevention Legacy Fund and the Tobacco Reduction Program, and are a synthesis of currently accepted approaches to management, derived
from a review of relevant scientific literature. Clinicians applying these guidelines should, in consultation with the patient, use independent medical judgment in the context of individual clinical circumstances to direct care.

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 BACKGROUND In 2015, an estimated 17,000 Albertans were diagnosed with cancer and 6,500 people died of it.1 By 2030, approximately 27,000 new cancer cases are projected to occur, representing a 65% increase since 2010 and a 240% increase since 1990.2 Smoking is the leading preventable risk factor for cancer and is responsible for an estimated 30% of all cancer-related deaths, as well as the majority of lung (75.6%) and larynx (74.3%) cancers within Alberta.3,4 Tobacco screening and cessation treatment for cancer patients is a key to high-quality oncology care. An estimated 25 - 80% of individuals who smoke will continue smoking following their diagnosis.5 Continued tobacco use following a cancer diagnosis is associated with reduced treatment effectiveness, increased risk of cancer recurrence, greater treatment-related toxicity, increased risk of second primary cancer and mortality.6,7 The 50th anniversary of the Surgeon General's report on smoking reported that tobacco cessation at the time of cancer diagnosis could lower the risk of death by up to 40% with the benefits of cessation being equal to, or even exceeding, the value of the latest cancer therapies. 7 The use of clear, direct advice from healthcare providers to stop smoking continues to be the single most influential way to achieve smoking cessation in most patient populations. Tobacco intervention by health care professionals has been shown to be effective in increasing the abstinence rate in cancer patients.8 The integration of tobacco screening and cessation treatment into oncology care has been recommended by a number of national and international cancer-focused organizations as a best practice intervention.5,8-14 However, tobacco screening and treatment is not consistently or routinely implemented in cancer care across the province.15,16 The Ask, Advise, Refer (AAR) brief intervention model is being adopted by CancerControl Alberta as a practice standard for all its sites. This guideline presents the key recommendations to support the screening and treatment of tobacco use by cancer patients as a provincial standard of care. GUIDELINE QUESTIONS • Are cancer patients who are current tobacco users, compared to those who are never or former
tobacco users, at increased risk for poorer cancer treatment outcomes, prognosis and quality of life? • Is a cancer diagnosis an important ‘window of opportunity’ or ‘teachable moment’ for tobacco cessation
for patients and their families? • Does brief tobacco intervention in cancer care increase tobacco cessation rates? • Does intensive tobacco interventions (multiple sessions that include problem solving and skills training)
in cancer care increase tobacco cessation rates? • Does cessation pharmacotherapy (with or without behavioural support) in cancer care, increase
tobacco cessation rates? • How does concurrent tobacco treatment (behavioural and/or pharmacotherapy support) impact cancer
treatment (e.g. chemotherapy, radiation surgery)? • What are the rates of desire to quit, quit attempts, quit success and relapse for cancer patients who
are identified as tobacco users?
Page 2 of 21
CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 DEVELOPMENT AND REVISION HISTORY The Tobacco Screening and Treatment Guideline was developed to provide guidance to health professionals to support tobacco cessation with oncology patients. This guideline was reviewed and endorsed by a working group representing members from CancerControl Alberta (CCA), the Alberta Cancer Prevention Legacy Fund, and the Tobacco Reduction Program. Membership captured key stakeholders involved in cancer care (medical oncologist, pharmacist, advanced practice nurse, respiratory therapist) as well as Alberta Health Services staff with content expertise in tobacco cessation and/or cancer treatment. Recommendations were initially informed by a thorough evidence review of published and grey literature. (see “Search Strategy” below) but tailored to reflect provincial resource availability and operational realities. A detailed description of the methodology followed during the guideline development process can be found in the Guideline Resource Unit Handbook. This document was first published in October 2015 and was revised in June 2016 to abbreviate the cessation intervention model to best support adoption across all CCA clinics and settings. SEARCH STRATEGY The search strategy was selected and reviewed by members of the guideline working group with support from an Alberta Health Services research librarian. The PubMED, EMBASE, Medline, Cochrane Database of Systematic Reviews, CINAHL, PsycINFO and Pharmacy databases were searched from 2008 to February 2015 for literature on tobacco cessation interventions in a cancer care setting and associated impacts on tobacco use reduction and/or cessation. A variety of separate and combined search terms were used, including but not limited to: cancer patients, caregiver, staff, tobacco intervention, tobacco cessation treatment, cessation pharmacotherapy, cancer, cancer treatment, risk factors, quality of life, windows of opportunity, recurrence, relapse and quit rates. Results were limited to randomized controlled trials, systematic reviews and observational studies published in English. Grey literature (e.g., Google, Google Scholar, ProQuest) as well as the reference lists of key articles were also searched for additional publications. Excluded from the analysis were pediatric cancer patients, tobacco treatment interventions that occur outside of cancer care (e.g. primary care) and non-oncology patients. A total of 74 studies were identified for inclusion. Clinical guidelines databases (e.g. National Institute for Health and Care Excellence, the National Guidelines Clearinghouse, SAGE Directory,) and guideline bodies (i.e., CAN-ADAPTT, US Department of Health and Human Services, National Comprehensive Cancer Network, American Society of Clinical Oncology) were also searched for guidelines on smoking cessation in cancer care settings. The search returned eight guidelines. A full copy of the evidence tables is available upon request by contacting [email protected].
Page 3 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 TARGET POPULATION This guideline applies to all health professionals working with adult cancer patients (aged 18 years and older) at any phase of the cancer care continuum regardless of cancer type, stage (including metastatic) or treatment plan. Components of this guideline are also applicable to the patient’s family and/or caregivers, where indicated. This guideline is intended for use in both inpatient and ambulatory (outpatient) settings. SCOPE AND DEFINITIONS This guideline outlines recommendations to guide CCA health care professionals who have direct contact with patients and families to deliver brief tobacco intervention as a routine standard of care. The standards for more intensive intervention are not included in the guideline at this time. • Tobacco Use includes the use of cigarettes, cigars, cigarillos, pipe, chew/spit, and waterpipe (e.g.,
Hookah). • AAR Brief Tobacco Intervention Model is an established model used in a variety of clinical settings.
It is designed to be implemented in less than 3 minutes and involves the following three steps: Ask about tobacco use, advice to quit and refer to a local resource for more intensive tobacco treatment counselling or pharmacotherapy.
• Health Professional means an individual who is a member of a regulated health discipline, as defined by the Alberta Health Disciplines Act or Health Professions Act, and who provides promotional, preventive, curative, or rehabilitative care as per their defined scope or role.
• Putting Patient First (PPF) Form is a self-report tool completed by the patient to support completion
of the provincially standardized Screening for Distress Intervention. The form consists of the revised Edmonton Symptom Assessment System (ESASr), a version of the Canadian Problem Checklist, and questions designed to satisfy CCA operational and accreditation requirements.
RECOMMENDATIONS 1. CCA Inpatient and Outpatient Procedure for Tobacco Treatment
• Brief Tobacco Intervention using the ASK, ADVISE, REFER model is implemented and documented
on the Putting Patient First (PPF) Form. Documentation can occur electronically in the PPF questionnaire within ARIA or on the paper version of the form and attached to the patient’s chart. Refer to Appendix A for the Algorithm for the Screening and Treatment of Tobacco Use.
• In compliance with the AHS Level 1 Tobacco and Smoke Free Environment Policy, patients, family member(s), or those accompanying the patient should be advised that AHS facilities and grounds are tobacco free.
Page 4 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 2. Responsibilities of the Nurse or other Health Care Provider
2.1 Tobacco Use Screening (ASK)
o Screen for tobacco use at clinical encounters where the PPF Form is used. Document tobacco use status on PPF within ARIA or on the paper version of the form. Screen should capture: tobacco use within past 30 days (high relapse risk)
tobacco use within the past year
o Where able and/or appropriate, accompanying caregivers or family members should also
be asked about their tobacco use with appropriate follow-up advice or referral to available cessation supports including but not limited to the Tobacco Treatment and Support Clinic(s). Refer to Appendix B for a screen shot of the Tobacco Treatment and Support Clinic Referral Form; this form can be accessed through the AHS Policy and Forms page on the Insite intranet.
o If the patient is not a tobacco user, STOP THE INTERVENTION.
Note about e-cigarette use: At this time, Health Canada has not fully evaluated e-cigarettes for safety, quality and efficacy, and advises Canadians against the purchase or use of e-cigarettes/vaping products.
2.2 Education and Assessment (ADVISE)
o Patients who self-identify as using tobacco should be advised to stop or reduce use. Advice should be personalized to the patient’s cancer type, stage and treatment plan and broadly address:
health effects of continued tobacco in context of cancer treatment.
benefits of cessation and/or reduction.
benefit of counselling and medication as most effective treatment.
o Advise patients’ and/or their family members of available cessation services including but not limited to the Cancer Treatment and Support Clinic. Assess patient interest in receiving a referral to such services for counselling and/or pharmacotherapy support.
o Document advice given in paper or electronic PPF form under ‘Actions Taken’.
o If appropriate, patients should be advised on importance of reducing exposure to second-hand-smoke with message of cessation to accompanying caregivers/family members who identify as tobacco users.
o A longer tobacco cessation intervention following the five A’s (Ask, Advise, Assess, Assist, Arrange) approach can occur when staff knowledge and time enables them to do so.
Page 5 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
Please reference the resource ‘The 5A’s Approach: A Continuum of Brief and Intensive Settings”, accessed through the Alberta Quits Website > Health Care Providers > Tools and Resources > Downloadable Resources.
2.3 Referral (REFER)
o For patients and family members interested in quitting:
Refer to one of the two CCA Cancer Treatment and Support Clinics as per patient preference or by geographic proximity.
Provide self-help resources.
Document in paper or electronic PPF Form under ‘Referrals’ > ‘Referral to Cessation Clinic’.
Referral Process: For CCA centres that are electronic, referrals will be automated and triggered by a positive tobacco screen and acceptance of referral to ‘cessation clinic’ as documented on the PPF Questionnaire in ARIA. For centres/clinics that are paper-based, the most appropriate health professional can phone in or fax a referral using the Tobacco Treatment and Support Clinic Referral Form (Appendix B). Copies of the form can be accessed internally through the AHS Policy and Forms page on the Insite intranet.
o For patients not interested in quitting:
Provide the appropriate self-help resources.
Document patient refusal of referral in the ‘comment’ box of the electronic PPF form, on the paper version of the PPF form, or elsewhere in the patient’s chart.
Advise patients that they can self-refer to the clinic at any time by calling the clinic directly. Provide patient with clinic contact information.
3. Nicotine Withdrawal and Cessation Pharmacotherapy
3.1 Patients Admitted to Hospital
o Inpatients that self-identify as using tobacco products should be assessed for nicotine withdrawal symptoms and offered the most appropriate Nicotine Replacement Therapy (NRT) (patch, gum, inhaler). Pharmacotherapy can be ordered using the Tobacco Cessation Order Sets in ARIA under ‘favorites’. Refer to Appendix C and Appendix D for a Summary of Cessation Pharmacotherapy and Drug Interactions with Tobacco Smoke, respectively.
3.2. Outpatient Visits
o Where outpatients express interest in stopping or reducing tobacco use and where time or scope of practice allow, pharmacologic assistance can be offered/ initiated by an available
Page 6 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
authorized prescriber at point of care. Pharmacotherapy can be ordered using the Tobacco Cessation Order Sets in ARIA under ‘favorites’.
o Outpatients receiving day care treatment(s) for an extended period of time should be encouraged to bring a personal supply of cessation medication to manage withdrawal, if required.
4. Staff Education
o CCA health care professionals who have direct contact with patients and families are encouraged to participate in professional education and training opportunities pertaining to tobacco cessation or treatment as offered. Additional supports and training include:
The AlbertaQuits Learning Series, accessed through the Alberta Quits Website > Learning
Alberta Quits Tools and Resources for Healthcare Providers, accessed through the Alberta Quits Website > Helping Others > Healthcare Providers > Tools & Resources
DISCUSSION Impact of Continued Tobacco Use on Cancer Outcomes Current evidence strongly supports quitting smoking following a cancer diagnosis. The 2014 Surgeon General’s Report concluded that there is sufficient causal evidence between smoking and increased all-cause mortality, increased cancer-specific mortality and increased risk of developing second primary cancers.7 Smoking was further associated with an increased risk of cancer recurrence, poorer response to treatment and increased treatment-related toxicity.7 Indeed, estimates suggest that quitting smoking at the time of diagnosis could lower the risk of dying by up to 40% with the benefits of cessation being equal to or exceeding the value of new cancer therapies for some cancer diagnoses.7 The benefits of cessation go beyond cancers known to be caused by tobacco use, with increased mortality rates associated with continued smoking after diagnosis reported across cancer types and stages of diagnosis.14,17-19 Results of a meta-analysis with early stage non-small cell lung cancer (NSCLC) and limited stage small cell lung cancer (SCLC) showed continued smoking increased the risk of all-cause mortality, recurrence and development of a second primary tumour. 20 In patients with NSCLC, quitting smoking was associated with an estimated five-year survival rate of 70% compared to 33% in those who continued to smoke. Survival rates were comparable for patients with SCLC at 63% and 29% in quitters and those who continued to smoke, respectively.20
There is consistent evidence that tobacco use, namely smoking, reduces the efficacy of radiation therapy and some chemotherapy agents7,21-23 and increases the risk for treatment-induced complications including surgical site infections, pulmonary function and return to operating room.14,24-26 Studies further report an association between smoking and increased risk of recurrence following cancer treatment (radiation, chemotherapy, surgery) among patients with head and neck cancers,17,22,27,28 prostate cancer,29 urothelial cancer,30 and gastrointestinal cancers.31
Page 7 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 Impact of Tobacco Use on Cancer Treatment: Chemotherapy Considerations Tobacco smoke can interfere with the pharmacokinetic mechanisms of several chemotherapy drugs potentially causing an altered pharmacologic response. 23,32 Tobacco smoke increases the amount of drug binding protein (AAG) resulting in induction of cytochrome-450 enzymes (primarily CYP1A2) and UGT isoenzymes which metabolize several chemotherapy drugs. Nicotine replacement therapy does not impact CYP1A2 activity or reduce cancer drug efficacy. Erlotinib: Commonly used in the treatment of non-small-cell lung and pancreatic cancers, erlotinib is primarily metabolized by CYPs 3A4 and 1A2. Cigarette smoking has been shown to cause induction of several CYP enzymes primarily by CYP3A4 but also by CYP1A2, resulting in more rapid metabolism and decreased systemic exposure to the drug.32 Data analyzed from seven clinical trials that administered the standard dose of erlotinib (150 mg once daily) found that smoking status was a significant covariate affecting drug clearance.23 Patients who smoked and who were treated with erlotinib experienced a 23.5% increase in clearance and had lower (nearly half) median steady-state trough plasma concentrations compared to never and former smokers.23,33 An increased dose of erlotinib may benefit patients with NSCLC who continue to smoke following diagnosis. Dosing consideration should also be given to patients exposed to secondhand smoke.33 Irinotecan: Smoking is known to alter the pharmacokinetics of irinotecan (CPT-11), a topoisomerase-I inhibitor used to treat a variety of cancers (e.g., colon, rectum, lung, bone). While not definitive, a study of cancer patients treated with irinotecan (n=190) found those who smoked experienced 40% lower systemic exposure to the active metabolite SN-38 (median, 0.54 v 0.87 ng x h/mL/mg; P < .001); 18% faster clearance (median, 34.8 versus 29.5 l/hour, p = 0.001); and less neutropenia (6% in smokers versus 38% in nonsmokers) (odds ratio [OR], 0.10; 95% CI, 0.02 to 0.43; P < .001) compared to non-smokers.33 The effects of smoking on irinotecan pharmacokinetics may be attributed to induction and modulation of the CYP3A and UGT1A1 enzymes involved in the drug’s metabolism.23,34 The personalization of irinotecan therapy by increasing dosing in patients who smoke has been proposed.32 Quit Behaviours and Efficacy of Tobacco Cessation among Cancer Patients Long-term abstinence is an important performance measure and clinical outcome for cessation interventions.35 In the United States, an estimated 62% of patients recently diagnosed with cancer identified as current smokers, recent quitters (quit within the last 12 months),or former smokers.36 In the short-term, cancer patients experience high cessation rates, relapse is common and higher among those experiencing comorbid mental health and/or addiction issues.37-39
A longitudinal study examining smoking behaviours among lung, head and neck cancer patients (n=154) following surgical treatment found that those who smoked the week before surgery experiences a 60% relapse rate at 12 months following their surgery compared to 13% of patients who were abstinent pre-surgery. 40 Using backward regression analysis, low quitting self-efficacy (p=.029), higher depression proneness (p=.037), and fear over cancer recurrence (p=.028) were cited reasons for relapse.40
Tobacco Screening and Treatment in Healthcare Settings Clinical practice guidelines from leading national and international health and cancer organizations recommend that all healthcare providers screen for and offer tobacco cessation treatment. The 5 A’s model (Ask, Advise, Assess, Assist, Arrange) is a recognized gold standard to support tobacco cessation across different health-care settings and populations.11,16,35,41-43 Several published reports have highlighted
Page 8 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
the utility and efficacy of the abbreviated ‘Ask-Advice-Refer’ (AAR) model to promote cessation intervention where time constraints, lack of expertise or resources make it hard for clinicians to deliver a more intensive intervention.44,45 Integrating the first two steps of the 5A’s approach, this model concludes with a referral to available cessation support services for more intensive tobacco treatment and counselling. The provision of physician-delivered advice to quit is a critical component of tobacco cessation treatment. The results of a 2015 systematic review and meta-analysis comparing advice to quit to the offer of assistance found that advice to quit on medical grounds increased long-term abstinence by 47% (RR 1.47, 95% CI: 1.24–1.75]. The findings concluded, however, that offering assistance in the form of behavioural counselling or provision of NRT generated more quit attempts than simply giving advice to quit on medical grounds (RR 1.69, 95% CI: 1.24–2.31 for behavioural support and 1.39, 95% CI: 1.25–1.54 for offering medication).46 While few studies have addressed the optimal intensity of tobacco interventions with cancer patients and their families, evidence conducted within other clinical settings report a dose-response relationship between intervention time and quit success.44 The clinical practice guidelines from the US Public Health Service report abstinence rate increases from 14.4% with brief counselling (< 3 minutes) to 18.8% for interventions lasting 4-30 minutes. Optimal total contact time was estimated to be 91–300 minutes, resulting in abstinence rates of roughly 28%.44
Initiating tobacco screening and intervention at the time of diagnosis and/or during the preoperative period is consistently recommended as best practice regardless of cancer type or level of intervention.11,16,35 Tobacco Treatment Options with Cancer Patients Similar to the general population, first-line pharmacotherapy for tobacco cessation with cancer patients include all forms of nicotine replacement therapy (NRT), bupropion and varenicline.10,11,15,16 Compared to placebo, varenicline is the most effective monotherapy for successful long-term smoking cessation (see Table 2). Table 2: Effectiveness of Cessation Mono and Combination Therapies Pharmacotherapy Abstinence Rate at 6 months (Odds Ratio) Nicotine Gum 19% (1.5) Nicotine Patch 23.7% (1.9) Nicotine Inhaler 24.8% (2.1) Nicotine Lozenge 19.9% (1.96) Bupropion SR 24.2% (2.0) Varenicline 33.2% (3.1) Patch + Gum or Spray 36.5% (3.6) Patch + Bupropion 28.9% (2.5) Patch + Inhaler 25.8% (2.2)
Combination therapies improve efficacy over monotherapies alone (Table 2).44 Systematic reviews show that combining bupropion or varenicline with NRT is more efficacious than either varenicline or bupropion alone.47,48 Compared to NRT monotherapy, bupropion combined with NRT was not found to be more
Page 9 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
efficacious.49 Two recent randomized control trials suggest that varenicline combined with bupropion may be more effective than either monotherapy, however more research is needed.50,51 Treatment with pharmacotherapy combined with behavioural counseling is more effective than pharmacotherapy or counselling alone in both cancer and non-cancer patients. A 2013 meta-analysis comparing smoking cessation interventions with usual care in cancer patients found that the combined use of pharmacological (NRT and varenicline) and behavioural therapy were most effective at improving quit rates.35
Clinical Considerations and Contraindications for Cancer Patients Nicotine Replace Therapy (NRT): Oral products, including gum, lozenges, spray and inhalers, may be irritating to the oral mucosa and therefore may not be appropriate for use for individuals with oral cancer, or with head and neck cancer who are undergoing radiation and/or receiving chemotherapy with high incidence of stomatitis.52 Some forms of NRT may be contraindicated in the immediate pre- and/or post-operative period in patients who undergo tissue reconstruction where revascularization is a concern. These cases should be discussed on an individual basis with the surgeon and health-care team. In such cases, non-nicotine treatments for smoking cessation are alternate options (e.g., varenicline, bupropion).53 Bupropion: In cancer patients experiencing depression symptoms, bupropion has been shown to increase abstinence rates, decrease withdrawal symptoms and increase quality of life compared to those with no depression symptoms.54 Bupropion is contraindicated in patients with a history of seizures or those with a predisposition to seizures, such as patients with CNS tumours.44 The drug should also be avoided breast cancer patients taking tamoxifen as bupropion impacts the metabolism of tamoxifen by inhibiting conversion to its active metabolites.55 In the general population, bupropion can reduce appetite and prevent weight gain and may warrant monitoring if prescribing in patients who may experience weight loss related to their cancer treatments.52 Bupropion may be associated with neuropsychiatric symptoms, including suicidal ideation, suicide attempts, depressed mood, hostility, and agitation. Patients taking bupropion should be closely monitored for adverse effects and should stop taking the drug immediately if any of these side effects develop.
Varenicline: To date, there are no reported studies of interactions between varenicline and commonly used lung cancer therapies.23 A small study testing the effectiveness of varenicline and behavioural support in a cohort of cancer patients reported nausea as the most common side effect, similar to rates reported within general population which has about a 30% incidence.8 Drug titration and dosing can reduce nausea and should be considered with cancer patients experiencing cancer-treatment induced nausea.52 Varenicline should be used cautiously in patients with a history of seizures or conditions that lower seizure threshold.56 Close monitoring is required for neuropsychiatric symptoms with consideration of nicotine replacement therapy as an alternate treatment option.56 Due to the psychological and medical vulnerability of cancer patients, varenicline is encouraged to be used along with intensive behavioural counselling to support cessation.8 While there have been studies of adverse cardiovascular events in patients taking varenicline,57-59 overall data suggest that the benefit of varenicline as the most effective cessation drug in clinical trials outweighs the low risk of adverse events associated with its use.60 Personalization of varenicline and close monitoring are still encouraged if prescribing in patients with cardiovascular disease.
Page 10 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 E-cigarettes: There is currently insufficient evidence to support the recommendation of e-cigarettes or smokeless tobacco in tobacco cessation with cancer patients due to lack of evidence of their safety, quality or efficacy.6
GLOSSARY OF ABBREVIATIONS Acronym Description AAG alpha 1-acid glycoprotein AAR Ask, Advise, Refer AHS Alberta Health Services CAN-ADAPTT Canadian Action Network for the Advancement, Dissemination and
Adoption of Practice-informed Tobacco Treatment CCA CancerControl Alberta NRT Nicotine replacement therapy NSCLC Non-small cell lung cancer PPF Putting Patients First SHS Second hand smoke UGT (isoenzyme) uridine diphosphate glucuronosyltransferase
DISSEMINATION • Present the guideline at the local and provincial tumour team meetings and weekly rounds. • Present guideline to the Cancer Strategic Clinical Network (SCN) and other relevant meetings. • Post the guideline on the Alberta Health Services website and Alberta Prevents Cancer website. • Conduct trainings with health-care professionals, including allied health, on implementing the
guideline. • Send electronic notification of the updated guideline to all members of CancerControl Alberta. MAINTENANCE A formal review of the guideline will be conducted in 2018 by the Alberta Provincial Tumour Team Council, with additional input from identified members of the guideline working group, if needed. If critical new evidence is brought forward before that time, the guideline working group will revise and update the document accordingly. CONFLICT OF INTEREST Participation of the guideline working group members in the development of this guideline has been voluntary and the authors have not been remunerated for their contributions. There was no direct industry involvement in the development or dissemination of this guideline. CancerControl Alberta recognizes that although industry support of research, education and other areas is necessary in order to advance patient care, such support may lead to potential conflicts of interest. While some members of the working group are involved in research funded by industry or have other such potential conflicts of interest, the developers of this guideline are satisfied it was developed in an unbiased manner.
Page 11 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 ADDITIONAL RESOURCES Alberta Quits: Tools and Resources for Healthcare Providers ASCO Policy Statement Update: Tobacco Cessation and Control National Comprehensive Cancer Network (NCCN): Tobacco Cessation Guidelines (requires free registration) REFERENCES 1. Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2015. 2015. 2. Grundy A, Poirier AE, Khandwala F, Friedenreich CM, Brenner DR. Cancer incidence attributable to modifiable risk factors in
Alberta, Canada in 2012. Department of Cancer Epidemiology and Prevention Research for the Alberta Cancer Prevention Legacy Fund. 2015.
3. Alberta Cancer Board. Briefing Note: Evidence Supporting Tobacco Control Policies. 2007. 4. Alberta Health Services. Preliminary findings of the Population Attributable Risk (PAR) project.Department of Cancer
Epidemiology and Prevention Research. 2015. 5. Cancer Care Manitoba. Practice Guideline: Smoking Cessation in Oncology Care. 2015. 6. Hanna N, Mulshine J, Wollins DS, Tyne C, Dresler C. Tobacco cessation and control a decade later: American society of
clinical oncology policy statement update. J Clin Oncol 2013 Sep 1;31(25):3147-3157 PubMed ID 23897958. 7. United States Department of Health and Human Services (USDHHS). The health consequences of smoking-50 years of
progress. A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. 2014; Available at: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/. Accessed Sept 1, 2015.
8. Park ER, Japuntich S, Temel J, Lanuti M, Pandiscio J, Hilgenberg J, et al. A smoking cessation intervention for thoracic surgery and oncology clinics: a pilot trial. J Thorac Oncol 2011 Jun;6(6):1059-1065 PubMed ID 21512406.
9. Ung YC, Souter LH, Darling G, Dobranowski J, Donohue L,Leighl N et al. Follow-up and surveillance of curatively treated lung cancer patients. 2014;26-3.
10. National Cancer Institute. Smoking in Cancer Care–for health professionals (PDQ®). 2014; Available at: http://www.cancer.gov/about-cancer/causes-prevention/risk/tobacco/smoking-cessation-hp-pdq.
11. NCCN Clinical Practice Guidelines in Oncology. 2015; Available at: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive.
12. Leone FT, Evers-Casey S, Toll BA, Vachani A. Treatment of tobacco use in lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013 May;143(5 Suppl):e61S-77S PubMed ID 23649454.
13. Lung Cancer Overview. 2015; Available at: http://pathways.nice.org.uk/pathways/lung-cancer. 14. Parsons A, Daley A, Begh R, Aveyard P. Influence of smoking cessation after diagnosis of early stage lung cancer on
prognosis: systematic review of observational studies with meta-analysis. BMJ 2010 Jan 21;340:b5569 PubMed ID 20093278.
15. Alberta Health Services. Tobacco Free Futures Guidelines. 2014. 16. CAN-ADAPTT. Canadian Smoking Cessation Clinical Practice Guideline. 2011. 17. Al-Mamgani A, van Rooij PH, Mehilal R, Verduijn GM, Tans L, Kwa SL. Radiotherapy for T1a glottic cancer: the influence of
smoking cessation and fractionation schedule of radiotherapy. Eur Arch Otorhinolaryngol 2014 Jan;271(1):125-132 PubMed ID 23797970.
18. Chen AM, Chen LM, Vaughan A, Farwell DG, Luu Q, Purdy JA, et al. Head and neck cancer among lifelong never-smokers and ever-smokers: matched-pair analysis of outcomes after radiation therapy. Am J Clin Oncol 2011 Jun;34(3):270-275 PubMed ID 20622648.
19. Moreira DM, Aronson WJ, Terris MK, Kane CJ, Amling CL, Cooperberg MR. Cigarette smoking is associated with an increased risk of biochemical disease recurrence, metastasis, castration-resistant prostate cancer, and mortality after radical prostatectomy: Results from the SEARCH database. Cancer 2014;120(2):197-204. PubMed ID 24127391.
20. Braithwaite D, Izano M, Moore DH, Kwan ML, Tammemagi MC, Hiatt RA, et al. Smoking and survival after breast cancer diagnosis: a prospective observational study and systematic review. Breast Cancer Res Treat 2012 Nov;136(2):521-533 PubMed ID 23053660.
Page 12 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 21. Hoff CM, Grau C, Overgaard J. Effect of smoking on oxygen delivery and outcome in patients treated with radiotherapy for
head and neck squamous cell carcinoma--a prospective study. Radiother Oncol 2012 Apr;103(1):38-44 PubMed ID 22385797.
22. Meyer F, Bairati I, Fortin A, Gelinas M, Nabid A, Brochet F, et al. Interaction between antioxidant vitamin supplementation and cigarette smoking during radiation therapy in relation to long-term effects on recurrence and mortality: a randomized trial among head and neck cancer patients. Int J Cancer 2008 Apr 1;122(7):1679-1683 PubMed ID 18059031.
23. O'Malley M, King AN, Conte M, Ellingrod VL, Ramnath N. Effects of cigarette smoking on metabolism and effectiveness of systemic therapy for lung cancer. J Thorac Oncol 2014 Jul;9(7):917-926 PubMed ID 24926542.
24. Mason DP, Subramanian S, Nowicki ER, Grab JD, Murthy SC, Rice TW, et al. Impact of smoking cessation before resection of lung cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database study. Ann Thorac Surg 2009 Aug;88(2):362-70; discussion 370-1 PubMed ID 19632374.
25. Zevallos JP, Mallen MJ, Lam CY, Karam-Hage M, Blalock J, Wetter DW, et al. Complications of radiotherapy in laryngopharyngeal cancer: effects of a prospective smoking cessation program. Cancer 2009 Oct 1;115(19):4636-4644 PubMed ID 19569250.
26. Gajdos C, Hawn MT, Campagna EJ, Henderson WG, Singh JA, Houston T. Adverse effects of smoking on postoperative outcomes in cancer patients. Ann Surg Oncol 2012 May;19(5):1430-1438 PubMed ID 22065194.
27. Guo SS, Huang PY, Chen QY, Liu H, Tang LQ, Zhang L, et al. The impact of smoking on the clinical outcome of locoregionally advanced nasopharyngeal carcinoma after chemoradiotherapy. Radiat Oncol 2014 Nov 26;9:246-014-0246-y PubMed ID 25424191.
28. Ouyang PY, Su Z, Mao YP, Liang XX, Liu Q, Deng W, et al. Prognostic impact of cigarette smoking on the survival of patients with established nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers Prev 2013 Dec;22(12):2285-2294 PubMed ID 24252872.
29. Joshu CE, Mondul AM, Meinhold CL, Humphreys EB, Han M, Walsh PC, et al. Cigarette smoking and prostate cancer recurrence after prostatectomy. J Natl Cancer Inst 2011 May 18;103(10):835-838 PubMed ID 21498781.
30. Rink M, Zabor EC, Furberg H, Xylinas E, Ehdaie B, Novara G, et al. Impact of smoking and smoking cessation on outcomes in bladder cancer patients treated with radical cystectomy. Eur Urol 2013 Sep;64(3):456-464 PubMed ID 23206854.
31. Han MA, Kim YW, Choi IJ, Oh MG, Kim CG, Lee JY, et al. Association of smoking history with cancer recurrence and survival in stage III-IV male gastric cancer patients. Cancer Epidemiol Biomarkers Prev 2013 Oct;22(10):1805-1812 PubMed ID 23904463.
32. Petros WP, Younis IR, Ford JN, Weed SA. Effects of tobacco smoking and nicotine on cancer treatment. Pharmacotherapy 2012 Oct;32(10):920-931 PubMed ID 23033231.
33. Hamilton M, Wolf JL, Rusk J, Beard SE, Clark GM, Witt K, et al. Effects of smoking on the pharmacokinetics of erlotinib. Clin Cancer Res 2006 Apr 1;12(7 Pt 1):2166-2171 PubMed ID 16609030.
34. van der Bol JM, Mathijssen RH, Loos WJ, Friberg LE, van Schaik RH, de Jonge MJ, et al. Cigarette smoking and irinotecan treatment: pharmacokinetic interaction and effects on neutropenia. J Clin Oncol 2007 Jul 1;25(19):2719-2726 PubMed ID 17563393.
35. Nayan S, Gupta MK, Strychowsky JE, Sommer DD. Smoking cessation interventions and cessation rates in the oncology population: an updated systematic review and meta-analysis. Otolaryngol Head Neck Surg 2013 Aug;149(2):200-211 PubMed ID 23715685.
36. Warren GW, Kasza KA, Reid ME, Cummings KM, Marshall JR. Smoking at diagnosis and survival in cancer patients. Int J Cancer 2013 Jan 15;132(2):401-410 PubMed ID 22539012.
37. Toll BA, Brandon TH, Gritz ER, Warren GW, Herbst RS, AACR Subcommittee on Tobacco and Cancer. Assessing tobacco use by cancer patients and facilitating cessation: an American Association for Cancer Research policy statement. Clin Cancer Res 2013 Apr 15;19(8):1941-1948 PubMed ID 23570694.
38. Schnoll RA, Martinez E, Langer C, Miyamoto C, Leone F. Predictors of smoking cessation among cancer patients enrolled in a smoking cessation program. Acta Oncol 2011 Jun;50(5):678-684 PubMed ID 21534846.
39. Hopenhayn C, Christian WJ, Christian A, Studts J, Mullet T. Factors associated with smoking abstinence after diagnosis of early stage lung cancer. Lung Cancer 2013 Apr;80(1):55-61 PubMed ID 23290222.
40. Simmons VN, Litvin EB, Jacobsen PB, Patel RD, McCaffrey JC, Oliver JA, et al. Predictors of smoking relapse in patients with thoracic cancer or head and neck cancer. Cancer 2013 Apr 1;119(7):1420-1427 PubMed ID 23280005.
41. Tang MW, Oakley R, Dale C, Purushotham A, Moller H, Gallagher JE. A surgeon led smoking cessation intervention in a head and neck cancer centre. BMC Health Serv Res 2014 Dec 20;14:636-014-0636-8 PubMed ID 25527115.
42. Thomsen T, Tonnesen H, Okholm M, Kroman N, Maibom A, Sauerberg ML, et al. Brief smoking cessation intervention in relation to breast cancer surgery: a randomized controlled trial. Nicotine Tob Res 2010 Nov;12(11):1118-1124 PubMed ID 20855414.
43. de Bruin-Visser JC, Ackerstaff AH, Rehorst H, Retel VP, Hilgers FJ. Integration of a smoking cessation program in the treatment protocol for patients with head and neck and lung cancer. Eur Arch Otorhinolaryngol 2012 Feb;269(2):659-665 PubMed ID 21698416.
Page 13 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 44. Fiore MC, Jaén CR, Baker TB. Treating Tobacco Use and Dependence: 2008 Update: Clinical Practice Guideline. Rockville,
MD: Diane Publishing Co; 2008. 45. Schroeder SA. What to do with a patient who smokes. JAMA 2005 Jul 27;294(4):482-487 PubMed ID 16046655. 46. Aveyard P, Begh R, Parsons A, West R. Brief opportunistic smoking cessation interventions: a systematic review and meta-
analysis to compare advice to quit and offer of assistance. Addiction 2012 Jun;107(6):1066-1073 PubMed ID 22175545. 47. Chang PH, Chiang CH, Ho WC, Wu PZ, Tsai JS, Guo FR. Combination therapy of varenicline with nicotine replacement
therapy is better than varenicline alone: a systematic review and meta-analysis of randomized controlled trials. BMC Public Health 2015 Jul 22;15:689-015-2055-0 PubMed ID 26198192.
48. Stead LF, Perera R, Bullen C, Mant D, Hartmann-Boyce J, Cahill K, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2012 Nov 14;11:CD000146 PubMed ID 23152200.
49. Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev 2013 May 31;5:CD009329 PubMed ID 23728690.
50. Ebbert JO, Hatsukami DK, Croghan IT, Schroeder DR, Allen SS, Hays JT, et al. Combination varenicline and bupropion SR for tobacco-dependence treatment in cigarette smokers: a randomized trial. JAMA 2014 Jan 8;311(2):155-163 PubMed ID 24399554.
51. Rose JE, Behm FM. Combination treatment with varenicline and bupropion in an adaptive smoking cessation paradigm. Am J Psychiatry 2014 Nov 1;171(11):1199-1205 PubMed ID 24934962.
52. Karam-Hage M, Cinciripini PM, Gritz ER. Tobacco use and cessation for cancer survivors: an overview for clinicians. CA Cancer J Clin 2014 Jul-Aug;64(4):272-290 PubMed ID 24817674.
53. Winnipeg Regional Health Authority. Management of Tobacco Use and Dependence: Regional Clinical Practice Guideline. 2013.
54. Schnoll RA, Martinez E, Tatum KL, Weber DM, Kuzla N, Glass M, et al. A bupropion smoking cessation clinical trial for cancer patients. Cancer Causes Control 2010 Jun;21(6):811-820 PubMed ID 20087643.
55. Desmarais JE, Looper KJ. Interactions between tamoxifen and antidepressants via cytochrome P450 2D6. J Clin Psychiatry 2009 Dec;70(12):1688-1697 PubMed ID 20141708.
56. Pfizer Canada Inc. Product Monograph: Champix ® (varenicline tartrate tablets) Smoking –Cessation Aid. 2015. 57. Singh S, Loke YK, Spangler JG, Furberg CD. Risk of serious adverse cardiovascular events associated with varenicline: a
systematic review and meta-analysis. CMAJ 2011 Sep 6;183(12):1359-1366 PubMed ID 21727225. 58. Prochaska JJ, Hilton JF. Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation:
systematic review and meta-analysis. BMJ 2012 May 4;344:e2856 PubMed ID 22563098. 59. Ware JH, Vetrovec GW, Miller AB, Van Tosh A, Gaffney M, Yunis C, et al. Cardiovascular safety of varenicline: patient-level
meta-analysis of randomized, blinded, placebo-controlled trials. Am J Ther 2013 May-Jun;20(3):235-246 PubMed ID 23615317.
60. Sharma A, Thakar S, Lavie CJ, Garg J, Krishnamoorthy P, Sochor O, et al. Cardiovascular adverse events associated with smoking-cessation pharmacotherapies. Curr Cardiol Rep 2015 Jan;17(1):554-014-0554-8 PubMed ID 25410148.
Page 14 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 APPENDIX A: ALGORITHM FOR THE SCREENING AND TREATMENT OF TOBACCO USE
Page 15 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 APPENDIX B: TOBACCO TREATMENT AND SUPPORT CLINIC REFERRAL FORM
Page 16 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 APPENDIX C: SUMMARY OF CESSATION PHARMACOTHERAPY Drug Administration Common Side Effects
Nicotine Patch
7mg (5-10 cigarettes/day); 14mg (11-15 cigarettes/day) and 21mg (16-25 cigarettes/day) per 24 hour sustained release transdermal patches. Take as directed.
• apply to a clean, dry, hairless area • remove old patch prior to application of new one change sites daily to
prevent skin irritation • patient/client is normally advised not to use tobacco while using the
patch; however, continued use is generally not considered • dangerous and does not imply treatment failure • if insomnia and vivid dreams are a concern, patch should be removed
prior to bedtime
• skin irritation • vivid dreams • insomnia • headache • nausea
Nicotine Gum
2mg - One Piece as instructed every 1-2 hour(s) as needed. 4mg - One Piece as instructed every 1-2 hour(s) as needed. • absorbed through the lining in the mouth • do not eat or drink for 15 minutes before or during use • the term “gum” is misleading, as proper use is bite, bite, park, repeat • bite gum until a peppery taste or tingling occurs; park gum • between cheek and gums; repeat when sensation goes away • do not swallow
• mouth or throat soreness • jaw ache • hiccups • flatulence • upset stomach • insomnia • headache • nausea
Nicotine Lozenge
1mg (<20 cigarettes/day); 2mg (Take every 1 - 2 hour(s) as needed.
2mg nicotine bitartrate dehydrate
2mg and 4mg as nicotine polacrilex
• absorbed through the lining of the mouth • do not eat or drink for 15 minutes before taking the lozenge • do not chew or swallow the lozenge • slowly suck until there is a strong taste, then rest the lozenge in the
cheek, wait 1 minute or until taste fades and then repeat. • may be useful for those who cannot chew gum • sugar-free and safe for use by people with diabetes
• mouth or throat soreness • hiccups • upset stomach • insomnia • headache • nausea
Nicotine Inhaler
10 mg cartridge that delivers 4 mg of nicotine through about 80 inhalations (over 20 minutes of active puffing)
• hand-mouth activity from using the inhaler is preferred by some quitters the inhaler is useful for those with poor oral health or dentures, and for those who cannot chew gum
• similar in appearance to a cigarette: designed to be puffed on • not a true inhaler; the nicotine is delivered and absorbed through the
lining in the mouth • allows fine tuning of how much and how often the user consumes
nicotine
• mild local irritation of mouth,
• sinus or throat • cough • dry mouth • hiccups • insomnia • headache • nausea
Nicotine Mouth Spray
Available in a dispenser that contains 150 sprays; each spray delivers 1 mg of nicotine.
• absorbed through the lining in the mouth • do not eat or drink for 15 minutes before using the spray • if using the spray for the first time, or if the spray has not been used for
two days, load the spray pump by pressing on the dispenser several times until a fine spray is released into a tissue
• hiccups • throat irritation • increased salivation • tingling sensation of the • mouth/lips • insomnia • headache
Page 17 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 Drug Administration Common Side Effects
• point the spray nozzle towards the open mouth and hold as close as possible to the mouth, avoiding the lips
• press down on the dispenser to release a spray into the mouth • do not inhale while spraying and avoid swallowing for a few seconds
afterwards • expect a strong mint taste in the mouth
• nausea
Bupropion
150 mg orally daily x 3 days, then 150 mg orally two times daily for 12 weeks
• If insomnia is bothersome, the afternoon dose can be taken early in the
evening or late afternoon (as long as it is 8 hours after the morning dose).
• insomnia • dry mouth • headache • weight loss • agitation
Varenicline
0.5mg, 1mg tablets
• To reduce nausea, take on a full stomach and with a full glass of water. • To reduce insomnia, take second dose at supper rather than bedtime.
• Nausea • insomnia • vivid dreams • headache • constipation • agitation, depression, • suicidal thoughts
** Formatted from Alberta Quits Summary of Cessation Pharmacology resource.
Page 18 of 21
CLINICAL PRACTICE GUIDELINE SUPP-002
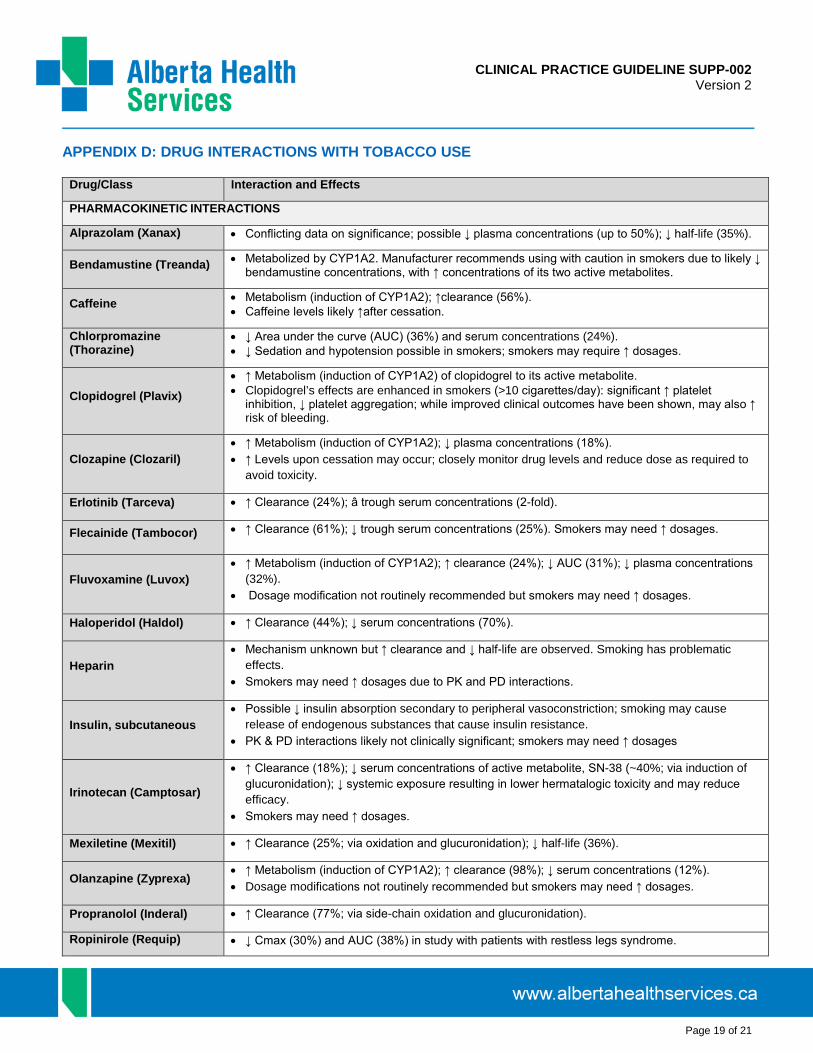
Version 2 APPENDIX D: DRUG INTERACTIONS WITH TOBACCO USE
Drug/Class Interaction and Effects
PHARMACOKINETIC INTERACTIONS
Alprazolam (Xanax) • Conflicting data on significance; possible ↓ plasma concentrations (up to 50%); ↓ half-life (35%).
Bendamustine (Treanda) • Metabolized by CYP1A2. Manufacturer recommends using with caution in smokers due to likely ↓ bendamustine concentrations, with ↑ concentrations of its two active metabolites.
Caffeine • Metabolism (induction of CYP1A2); ↑clearance (56%). • Caffeine levels likely ↑after cessation.
Chlorpromazine (Thorazine)
• ↓ Area under the curve (AUC) (36%) and serum concentrations (24%). • ↓ Sedation and hypotension possible in smokers; smokers may require ↑ dosages.
Clopidogrel (Plavix) • ↑ Metabolism (induction of CYP1A2) of clopidogrel to its active metabolite. • Clopidogrel’s effects are enhanced in smokers (>10 cigarettes/day): significant ↑ platelet
inhibition, ↓ platelet aggregation; while improved clinical outcomes have been shown, may also ↑ risk of bleeding.
Clozapine (Clozaril) • ↑ Metabolism (induction of CYP1A2); ↓ plasma concentrations (18%). • ↑ Levels upon cessation may occur; closely monitor drug levels and reduce dose as required to
avoid toxicity.
Erlotinib (Tarceva) • ↑ Clearance (24%); â trough serum concentrations (2-fold).
Flecainide (Tambocor) • ↑ Clearance (61%); ↓ trough serum concentrations (25%). Smokers may need ↑ dosages.
Fluvoxamine (Luvox) • ↑ Metabolism (induction of CYP1A2); ↑ clearance (24%); ↓ AUC (31%); ↓ plasma concentrations
(32%). • Dosage modification not routinely recommended but smokers may need ↑ dosages.
Haloperidol (Haldol) • ↑ Clearance (44%); ↓ serum concentrations (70%).
Heparin • Mechanism unknown but ↑ clearance and ↓ half-life are observed. Smoking has problematic
effects. • Smokers may need ↑ dosages due to PK and PD interactions.
Insulin, subcutaneous • Possible ↓ insulin absorption secondary to peripheral vasoconstriction; smoking may cause
release of endogenous substances that cause insulin resistance. • PK & PD interactions likely not clinically significant; smokers may need ↑ dosages
Irinotecan (Camptosar)
• ↑ Clearance (18%); ↓ serum concentrations of active metabolite, SN-38 (~40%; via induction of glucuronidation); ↓ systemic exposure resulting in lower hermatalogic toxicity and may reduce efficacy.
• Smokers may need ↑ dosages.
Mexiletine (Mexitil) • ↑ Clearance (25%; via oxidation and glucuronidation); ↓ half-life (36%).
Olanzapine (Zyprexa) • ↑ Metabolism (induction of CYP1A2); ↑ clearance (98%); ↓ serum concentrations (12%). • Dosage modifications not routinely recommended but smokers may need ↑ dosages.
Propranolol (Inderal) • ↑ Clearance (77%; via side-chain oxidation and glucuronidation).
Ropinirole (Requip) • ↓ Cmax (30%) and AUC (38%) in study with patients with restless legs syndrome.
Page 19 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2
• Smokers may need ↑ dosage
Tacrine (Cognex) • ↓ Metabolism (induction of CYP1A2); ↓ half-life (50%); serum concentrations 3-fold lower. • • Smokers may need ↑ dosages.
Theophylline (Theo Dur, etc.)
• ↑ Metabolism (induction of CYP1A2); ↑ clearance (58–100%); ↓ half-life (63%). • Levels should be monitored if smoking is initiated, discontinued, or changed. Maintenance doses
are considerably higher in smokers. • ↓ Clearance with second-hand smoke exposure.
Tricyclic antidepressants (e.g., imipramine, nortriptyline)
• Possible interaction with tricyclic antidepressants in the direction of ↓ blood levels, but clinical significance is not established,
Tizanidine (Zanaex) • ↓ AUC (30-40%) and ↓ half-life (10%) observed in male smokers.
Warfarin • ↑ Metabolism (induction of CYP1A2) of R-enantiomer; however, S-enantiomer is more potent and
effect on INR is inconclusive. • Consider monitoring INR upon smoking cessation.
PHARMACODYNAMIC INTERACTIONS
Benzodiazepines (diazepam, chlordiazepoxide)
• ↓ Sedation and drowsiness, possibly caused by nicotine stimulation of central nervous system.
Beta-blockers • Less effective antihypertensive and heart rate control effects; possibly caused by nicotine-
mediated sympathetic activation. • Smokers may need ↑ dosages.
Corticosteroids, inhaled • Smokers with asthma may have less of a response to inhaled corticosteroids.
Hormonal contraceptives
• ↑ Risk of cardiovascular adverse effects (e.g., stroke, myocardial infarction, thromboembolism) in women who smoke and use oral contraceptives. Ortho Evra patch users shown to have 2-fold
• ↑ Risk of venous thromboembolism compared to oral contraceptive users, likely due to ↑ estrogen exposure (60% higher levels).
• ↑ Risk with age and with heavy smoking (_15 cigarettes per day) and is quite marked in women >/ 35 years old.
Opioids (propoxyphene, pentazocine)
• ↓ Analgesic effect; smoking may ↑ the metabolism of propoxyphene (15–20%) and pentazocine (40%). Mechanism unknown.
• Smokers may need ↑ opioid dosages for pain relief.
** Adapted from Alberta Quits Drug Interactions with Tobacco Smoke resource. Adapted and updated from Zevin S, Benowitz NL. Drug interactions with tobacco smoking. Clin Pharmacokinet 1999;36:425–438.
Page 20 of 21

CLINICAL PRACTICE GUIDELINE SUPP-002
Version 2 COPYRIGHT DISCLOSURE Copyright © (2016) Alberta Health Services. This material is protected by Canadian and other international copyright laws. All rights reserved. This material may not be copied, published, distributed or reproduced in any way in whole or in part without the express written permission of Alberta Health Services (please contact the Guideline Resource Unit Manager at CancerControl Alberta at [email protected]). This material is intended for general information only and is provided on an "as is", "where is" basis. Although reasonable efforts were made to confirm the accuracy of the information, Alberta Health Services does not make any representation or warranty, express, implied or statutory, as to the accuracy, reliability, completeness, applicability or fitness for a particular purpose of such information. This material is not a substitute for the advice of a qualified health professional. Alberta Health Services expressly disclaims all liability for the use of these materials, and for any claims, actions, demands or suits arising from such use.
Page 21 of 21